florida cynthia k. davis, rn, fache principal cic … · florida cynthia k. davis, rn, fache...
TRANSCRIPT
FLORIDA
Cynthia K. Davis, RN, FACHE Principal
CIC Advisory Palm Harbor, FL
Many years ago, I was the charge nurse in an extremely busy ICU in New Mexico. A surgical resident called and told me that a young man in for an outpatient procedure now needed a bed. Something had gone terribly wrong in the OR.
This patient was Chris, a paraplegic in for a procedure to reduce his pain. His attending nurse sent his written health history, medications, and allergies into the OR. Tragically, the anesthesiologist administered medication without noticing Chris’s allergies and the monitors failed to alert the team when Chris stopped breathing for nearly five minutes. They were eventually able to resuscitate him and only then learned of his strict DNR order.
Chris left the OR a quadriplegic. He was in constant misery as we cared for him through bladder and lung infections. He could only breathe with a ventilator and a tracheotomy. He was no longer whole in spirit, mind or body.
Finally, it was agreed that we could take Chris off the breathing machine for a day, so that he could go in peace. We got Chris off the ventilator and wheeled him out of ICU after nine long months. Chris lived another three days before he quietly slipped away.
It’s been 30 years since Chris’s death. If he were alive today, informatics would’ve spared him this fate. What befell Chris while he was in the hospital’s care became a life-defining moment of clarity, leading me eventually to a career in nursing informatics.

FLORIDA
Lynn Drummond-Smith MS, RN-BC, CNL James A Haley VA Hospital
Tampa, FL
I began my nursing career in the Veterans Health Administration (VHA) as a Licensed Practical Nurse in 1993. I am working on a psychiatry unit. I returned to school to first obtain my ASN in 1999, Followed by my BSN in 2004. I finally obtained my MS in nursing with a concentration as Clinical Nurse Leader, graduating from University of South Florida in 2008. My role as a Clinical Nurse Leader is a direct care provider. I am the attending nurse, overseeing patient’s nursing care. Because I am not required to take a patient assignment each day I have the opportunity to work on performance improvement projects with other disciplines to improve care at the micro and macro systems. While working to improve our facilities noise levels I collaborated with nursing informatics on this project. During the early phases of TCAB (Transforming Care at the Bedside), staff nurses carried modified PDAs to collect data to determine what percent of time during the shift they spent on tasks away from the beside and conversely, what percent of time was spent in direct patient/family care. It was discovered that the simple task of making and retrieving phone calls were accounting for a large amount of their time spent away from patient care. Over the course of a few years with increased use of the telecommunication devices, we realized significant improvement in several of our nurse sensitive clinical outcomes. The documentation of pain medication effectiveness increased and the occurrence of pressure ulcer skin sores decreased. We are now exceeding the targeted benchmarks for the management of patient pain and hospital acquired pressure ulcer occurrence has been reduced.

GEORGIA
Brittney Wilson, RN, BSN Nurse Blogger
The Nerdy Nurse, LLC TheNerdyNurse.com Villa Rica, GA
When I discovered nursing informatics, it was like a dream come true. I was completing my BSN coursework, and I began researching options to further my education in nursing. I realized fairly quickly that I wasn't interested in most of the education pathways that many of my nursing peers were following. Somewhere in the midst of that research I stumbled onto "Nursing Informatics" and I knew it was for me. The stars aligned, the angels sang, and the fascinating world of healthcare information technology became my goal. For months I researched ways to break into nursing informatics. It became increasingly clear that being a master’s prepared informatics nurse was not a guarantee of employment. However, It seemed that every job posting required informatics experience or at the very least five years in clinical nursing experience. At the time I only had three. I was also struggling with the concept of leaving my home town. When I finally made the decision that I would need to start looking outside of my home town for opportunities the magic started to happen. Updating my resume was key. I tailored my resume to focus on my IT strengths. A friend of mine convinced me to highlight the fact that I was a blogger. Up until that point I had always feared my employers knowing I was a nurse blogger. It was a hard decision that ended up being one of the best I've ever made. I was able to leverage the programming and technical skills I had gained from working with a database powered content management system to my favor. I was energetic and passionate in my interview and was finally given a chance to spread my nerdy nurse wings. Clinical informatics isn't the only place that nurses are flaunting their technology skills. Nurses are going beyond the bedside and connecting online with other nurses, physicians and patients in an effort to promote better healthcare. There are many social networks where nurses are connecting online. However, there are some nurses who decide they need a bigger online footprint, and start a blog or website. Being a nurse blogger has given me an opportunity to have a digital soap box and achieve a level of influence that I would not be able to attain in my local environment. It's been incredibly empowering and has granted me the skills and confidence needed to secure a career in nursing informatics. By utilizing the web to share ideas, express opinions, and highlight information, nurse bloggers have the ability to be change catalysts. Nursing informatics has the potential to step up and utilize the web as a mechanism to educate patients as well as conduct research to

determine the best way to reach the largest audiences to promote better care and healthier communities.

KENTUCKY
Christine L. Corkins MSN, RN, PMP Director Clinical Informatics
Central Baptist Hospital Lexington, KY
When first entering the specialty of nursing informatics, it was a foreign concept to nearly everyone I contacted. Nearly 17 years later, informatics has become such a way of life; it is hard to imagine being a nurse anywhere else. Many things have improved, but a recent implementation of computerized order entry has been especially memorable. Leading up to the implementation, the physicians planned to be the pilot began surprising us by asking to be a part of the testing as opposed to having to enlist them in the process. They began providing input into desired order sets and helping with the training plan. On implementation day, a clinical analyst was in a patient room assisting the physicians with the order entry session. The physician entered a modification to a respiratory order and shortly thereafter the respiratory therapist presented at the door. He told the RT person that he had made some changes to which she replied that she was already aware. Oh to have captured that moment on film! On several other occasions the clinical informatics staff have witnessed turnaround time decrease to nearly zero minutes; pharmacy references to decreases in order processing time related to clarity; and orders in general are more complete. Certainly there are struggles as progress is made; however, the benefit for patients with improved care cannot be measured. Informatics as a profession has room for improvement, but the strides forward in such a short time have clearly demonstrated the great benefits to improve healthcare.

LOUISIANA
Charles A. Seaman RN, MSN Veterans Health Administration
Alexandria, LA VA Healthcare System Pineville, LA
I am a staff nurse working in Occupational Health at the Alexandria, LA VA Healthcare System. I became interested in nursing informatics while I was pursuing my Bachelors in nursing. I soon began working on a national project for the VA in developing an electronic employee medical record (Occupational Health Recordkeeping System). As a subject matter expert in Occupational Health I spent hours in team discussions, reviewing and testing the system. This project has allowed Occupational Health providers throughout the country to move into using (OHRS) electronic medical records for our VA employees. I was so interested in this project that I continued my education and completed my Master’s Degree in Nursing Informatics in 2010. We have been using OHRS for documenting vaccinations, medical clearance and fit testing for several years and we are on the path to completion. Once this project is completed the impact to the VA Occupational Health community will be tremendous. It will allow VA employees to go to any VA across the country and receive treatment if they become ill or injured while working. It will allow the provider to review any occupational health medical history on VA employees. This electronic medical record will also provide a place to document work related injuries, surveillance exams, fit testing, vaccinations along with the ability to generate reports. I have also had the opportunity to create a web page at my local facility for employee health as well as the development of a national web site for Clinical Occupational Health. Both of these web sites have provided Occupational Health providers and nurses the ability to provide and share important information to the VA Occupational Health Community at the Local and National level.

MARYLAND
Chrissy Ruhl, BSN, CCRN Nurse Manager, CVU/Cardiology Services
Western Maryland Health System Cumberland, MD
Karen Howsare, RN MSN
Director of Inpatient Nursing / Dialysis Western Maryland Health System
Cumberland, MD
Western Maryland Health System was formed in 1996 when two Cumberland MD hospitals joined together in an effort to effectively manage local healthcare resources. In November 2009, the two hospitals that were located a few miles apart, moved into one new hospital. Along with that move came the opportunity for new and more innovative technology in both equipment and low voltage systems. During the several years of planning, a strong desire to provide safe and fiscally responsible patient care to our community was very clearly communicated by the Executive Management team. A multidisciplinary team, in which Nursing had an integral role, was developed to evaluate technologies and equipment, select vendors, and later implement these new technologies. The size of the hospital and the Nursing units in particular created a necessity for the integration of technology systems to improve flow and processes. Due to the expense of building this new hospital and purchasing equipment and technologies immediately needed at opening, the replacement of IV pumps was scheduled for 2011. Research and investigation of several “smart pumps” was conducted, including site visits and testing IV pumps in-house with our wireless system, our goal was to utilize our wireless technology to the fullest with all our equipment, including IV pumps, in order to enhance our patient safety initiatives. A vendor was selected and installation of over 400 IV pumps occurred in September 2011. Since that time we have integrated information technology, infusion pumps, and nursing practice to improve medication safety. This entailed the adoption of an eMAR with BCMA, wireless infusion pumps, a software program to monitor our infusions in real-time, and observation of nursing practices to optimize workflow. Since nursing is a primary user of these technologies, our nurses and leadership team were heavily involved in the selection, implementation, and on-going optimization of the integration. For example, we used the real-time monitoring to identify any medications infusing outside of the DERS (dose error reduction software), reviewed weekly override reports to understand dosing trends, and provided direct observation to document compliance and identify barriers. We established targets of 95% across key infusion pump metrics: DERS use with dosed-
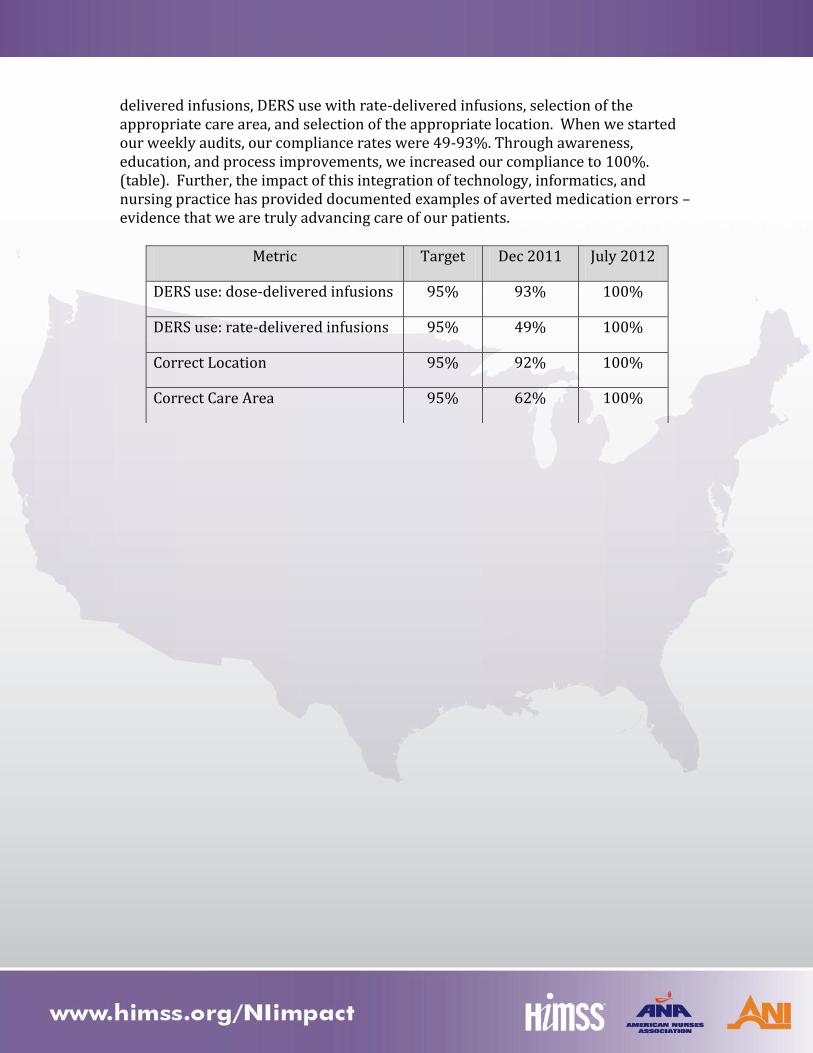
delivered infusions, DERS use with rate-delivered infusions, selection of the appropriate care area, and selection of the appropriate location. When we started our weekly audits, our compliance rates were 49-93%. Through awareness, education, and process improvements, we increased our compliance to 100%. (table). Further, the impact of this integration of technology, informatics, and nursing practice has provided documented examples of averted medication errors – evidence that we are truly advancing care of our patients.
Metric Target Dec 2011 July 2012
DERS use: dose-delivered infusions 95% 93% 100%
DERS use: rate-delivered infusions 95% 49% 100%
Correct Location 95% 92% 100%
Correct Care Area 95% 62% 100%
MISSISSIPPI
Maria Arellano MS, RN Clinical Product Manager
American Healthtech Ridgeland, MS
I was in year 23 of my nursing career when I decided to try a different way to impact lives, including my own. I had spent most of those 20+ years working in different capacities in long term care; direct resident care, nursing administration, and corporate clinical consultant. My goal was to change the public perception of nursing home care and to impact the quality of care provided to the residents I served. However, the harder I tried, the harder it got. I began to be very frustrated with the many organizational obstacles and regulatory pressures. Doing more with less was the mantra. The solution to my conundrum? I needed a different path, the path of higher education. I found excitement in reading about the use of technology to advance health care, so I enrolled in the University of Colorado master’s program in informatics, graduating in 2010. I quickly found a new career with a post-acute care software vendor who strongly believes that nurses are integral in the design of technologies used by nurses. My knowledge of human-computer interface design and usability were quickly put into use, but my true value is my “real world” knowledge of what it means to do the work. I know what nurses need from the technology, and when they need it. In my position as clinical software designer; I work collaboratively with other clinicians incorporating evidence-based nursing practice into our EHR, develop the capability to capture and analyze outcomes measures and design nursing decision support tools. Finally, after all these years, I feel that now I truly am impacting the quality of resident care by providing nurses with tools that help, not hinder them in their work to provide the best care they can, to the population that needs it most.

NORTH CAROLINA
Ellen J Reed, MBA, MSN, APRN, BC Practice Consultant
Encore Health Resources Sanford, NC
From the age of 10 volunteering as a candy striper to the day I proudly accepted my BSN diploma, I knew that I would maintain a level of accountability and responsibility which would ensure excellence in my patient outcomes. Whether it was my personal satisfaction and privilege assisting an individual’s return to improved health; or the challenge of being a change agent, I dedicated myself to quality by graduating from an MSN program, becoming ANCC certified and ultimately completing an MBA in Health Services. It became abundantly clear the only way to prove that patient care represents excellence is through an efficient collection of data. Although often difficult to step away from direct patient care, nurses engaged in clinical informatics serve as guardians to even a larger client system. Establishing electronic documentation is not about hardware and connectivity, but a conduit to vital information. Designing and building a document based on evidence and standardizations in practice, places all clinicians on a level playing field with the expert lending knowledge to the novice. Understanding the parameters of a full assessment and having interprofessional exchange of data, increases the likelihood that the patient will benefit from the watchful eyes of all caregivers. Incorporating quantifiable and retrievable data provides patients, families and communities assistance in making responsible decisions to improve health conditions, and/or respond respectfully when sustaining life is impossible. Reporting trends and creating bench marks perpetuates the goal of nursing science to maintain and promote health along the entire continuum of life.

SOUTH CAROLINA
Ruth Roldan, RN V21 CIS/ARK Clinical Manager
Organization: Nursing Palo Alto Health Care System
York, SC Trailblazing in 2001: Our ICU was finally going live with a clinical information system (CIS) I’d been hired to configure. The RN’s needs were crystal clear to me since I cared for ICU patients myself. A blank slate had been handed over with the instruction: Build. There was no committee, user group, co-worker, or an office partner to share this load. My fingerprints were on every screen, line, category, fluid in/out, and so on. Hours had been spent developing the home screen, creating surveys, brainstorming with blood bank, pharmacy, nurse managers, and CACs. On Go Live, I would be test driving the car myself! My peers, ICU RNs, were not timid with opinions. I’d be working alongside them. How would I feel documenting on my own system? What surprises were in store? There was no turning back the clock. Here I was documenting on both my patients. The CIS was working beyond all my expectations. I had 2 extra hours of patient face time due to the technology at my fingertips. Device data automatically updated every minute. My data was easy to enter and quite manageable. The CIS was intuitive so the stress level was low. I could not have asked for more. My CIS content would later be distributed to other VISNs as their “starter set”. Today, Operating Rooms, PACUs, GI Labs, Pain Centers, Cath Labs, and so on, are using similar configurations. What an honor to help provide the best care for our most deserving patients: Our Veterans.

TENNESSEE
Kelly Aldrich DNP, RN Director, Nursing Informatics HCA Clinical Services Group
Hospital Corporation of America (HCA) Nashville, TN
As an open heart recovery and neuro-trauma intensive care nurse for more than 20 years, I saw many opportunities where patient data for the sickest populations could drive trended information and allow for the best coordinated care with physicians, nurses and others on the care team. When caring for patients, I would often think of innovative solutions that could be utilized to support safe, efficient and effective care only to discover no such information technology solutions existed to support me as a bedside nurse. An example would be a real time voice documentation tool that could capture the ongoing lifesaving steps being done for a patient, such as medications I was administering to sustain my patients’ blood pressure, resulting in more time with the patient and less on documentation. I found it surprising that we did not have such solutions, and I often shared ideas with colleagues, who agreed that they would serve their patients better with seamless, innovative solutions that would give them time back with their patients. We wanted to care for patients, not spend time nursing the paper documents or nursing the machines. I carried this question with me for many years and entered into a graduate program to become a nurse practitioner. As I neared completion of my program, I heard the term “Nursing Informatics.” I was instantly drawn to the combination of data, information, and nursing knowledge and ultimately changed my education path to pursue Healthcare Systems Leadership and Nursing Informatics degrees. I knew that this was the future of nursing: bringing my clinical experiences and operation knowledge in partnership with information technology. Nursing Informatics has the ability to not only affect patient care and outcomes; it advocates for nurses by providing tools and solutions that they can use at the bedside everyday as they seek the best way of caring for the sick. My personal and professional objective as the Director of Nursing Informatics for a healthcare system that includes 166 facilities in 23 states is to implement large-scale informatics solutions that seamlessly integrate technology that is clinically relevant, intuitive and supports bedside nursing workflow. For example, I was asked by the HCA CNO (Chief Nursing Officer) Council to design and implement a solution that would help increase the time medical surgical nurses spent at the patient’s bedside. We worked on implementing a nurse-selected solution to automate the process of recording a patient’s vital signs. Our goal was to automate the information directly from the patient’s bedside into the electronic medical record, giving time back to nurses for patient care. Outcomes of the initiative were:

Proper patient identification through the use of bar code readers Elimination of the time between collection of the patient’s data and keying it into
the electronic medical record, saving 45 minutes in the collection process per set of rounds
Ability for clinical decision support to respond immediately to the aggregation of vital signs, resulting in a Modified Early Warning Scoring System (MEWS) that supports failure to rescue initiatives
Successful adoption in over 150 facilities in less than one year
This is just one example of how nursing knowledge and technology can cooperate to improve patient care; aggregated physiological scoring systems can detect a patient’s clinical deterioration up to 6.6 hours earlier than scenarios where scoring systems were not used. As a direct result of the partnership between nursing, nursing informatics and the information technology staff, a solution was implemented using real-time, effective and immediate information. This directly impacted the quality of care delivered at our facilities and, most importantly, provided clinically relevant solutions at the bedside.

TEXAS
Juliana J. Brixey, PhD, MPH, MSN, RN Assistant Professor
The University of Texas School of Biomedical Informatics Houston, TX
As a professor of informatics and a mentor of informaticists, a vital role for the future of healthcare, I help nurses, nursing informaticists, and others improve the quality and affordability of healthcare, and facilitate the creation of healthier communities. Teaching these students is amazing as they become immersed in the field of health informatics. Many come with little to no knowledge of informatics or technologies used in healthcare. The course curriculum is experiential and actively engages students. Social media is used extensively to create a sense of community as well as teach informatics skills. For some students it is a quantum leap to create an avatar and attend office hours in a Second Life, a virtual online world. By the end of the program students are comfortable participating in online virtual office hours. They become skilled at conducting virtual team meetings using various online software applications and competent with various social medial applications including social bookmarking all while completing health informatics courses to become the new workforce of health informaticists. Many of my students participate in professional and educational informatics activities outside the classroom. Several of my students are members of HIMSS. One recently was elected as web/communication position in local HIMSS chapter. My students successfully presented a poster and a podium talk at the 2012 International Nursing Informatics Congress in Montreal. Other students are active in the AMIA Nursing Informatics Working group as webmasters. Many students from the program have and are assuming leadership positions in health informatics.
TEXAS
Brittany Newman BSN, RN Educator EPIC Clinical Systems/Clinical Informatics
Texas Health Arlington Memorial Hospital Arlington, TX
The patient handoff has always been a crucial point of communication for clinical staff. As clinicians if we get busy or distracted we might forget important information regarding our patient that needs to be passed on. At Texas Health Resources we promote bedside report among nursing staff at change of shift. About 2 years ago when I was a bedside Oncology nurse we were encouraged to do bedside handoff. Computers were put in all the patient’s rooms to help facilitate this. However, much of the nursing staff at the time, including myself, still did not perform bedside report because we didn’t feel it fit into our workflow. When I became an Informatics nurse most of the staff were still not doing bedside report. At Texas Health Resources we have a group titled Nurse Champions which includes about 25 nurses from all of Texas Health Resource’s 13 hospitals. The Nurse Champions consist of bedside nurses from multiple clinical areas as well as Informatics Nurses. The Nurse Champions, as a group, felt it was time to create a handoff tool within our electronic health record to enhance and facilitate bedside reporting. With the input from this group a handoff tool was created to assist nurses in their bedside report, and gives them the information needed to communicate during report. The feedback we received from nursing staff was remarkable and positive. Nursing staff were happy to have a tool that would facilitate bedside report in an effective and efficient way.

TEXAS
Joni S. Padden, MSN, APRN, IN-BC, ACNS-BC Clinical Education Specialist for the Electronic Health Record
Texas Health Resources Harris Fort Worth Fort Worth, TX
#1 As our hospital was preparing to implement our electronic health record, we knew we would need experts in every area to help staff best use the new system. We recruited and trained super users for every area and named the group SUGAR (Super User Group Awesome Responders). These incredible people took ownership of making the transition go smoothly for the staff and safely for the patients. They made the experience fun and a little less stressful with their amazing attitudes and hard work. After implementation, the SUGAR’s continue to help their areas by being the go-to person for questions or help, by training new staff how to best use the system, by advocating for needed changes to the record, by educating their staff on changes or new processes, and by being the voice of informatics in their area. It has been over three years since we ‘went live’ and our SUGAR’s are still a strong, active part of our informatics team. They keep the lines of communication open to the frontline staff and are a valuable resource for trouble shooting and problem solving with the record. They are a vocal and empowered group of professionals who want the record to improve how they care for their patients. The ideas they bring forward often lead to the most successful ways we optimize the record. They are the experts on what needs the patient needs and being a SUGAR gives them a voice to make the record work for them. #2 After implementing our electronic health records the admission questions required to ask the patient grew to over 300. It was taking hours for the nurses to get even the simplest admission information entered into the record. This was frustrating for the patients and the staff. To address the issue, a team of bedside nurses from all disciplines (ER, Med-Surg, ICU, Women’s Services) and informatics nurses came together to hammer out what information really needed to be collected for the best care of the patient. A list of required information was developed as well as better ways to group and display the necessary information. Certain questions only showed when they applied to the patient’s condition, others could be expanded if needed or addressed with a simple yes or no. The system could tell the nurse if all of the required information had been gathered so they could have confidence that the needed information to keep their patient safe was in the record. When the team was done with their project the list was cut by more than half, the layout was much improved; the content matched what they needed to know to best care for their patients, the time to do an admission dropped to a reasonable amount, and the nurses and patients satisfaction improved. The work of the informatics nurses to help the frontline staff was so successful the group was made permanent and now the Nurse Champion group works to improve all facets of the electronic health record.

#3 Care plans are not a popular task for most nurses. The care planning in our electronic health record was cumbersome and doing the care plan was seen as busy work that did not have any impact on patient care. After listening to the staff and getting their ideas on how to improve the care plan, the informatics team developed and implemented changes to the care plan that have been a huge success with the staff. In one easy step in their flow sheets, the nurses can individualize the care plan with the goal for the shift of their patient or family. The care plan topics are being modified by the staff to reflect what they really do for and with their patients to provide the best care. The care plan is now integrated with the record instead of being a separate task. The evaluation of the goals at the end of the shift or procedure lets the nurse tell the patients story and give an accurate picture of how the patient is progressing. The basic goals utilized for all patients, such as safety, hygiene, nutrition, are automatically on the care plan to save the nurse steps. In addition to the patient’s goals, the nurse can add guidelines to help address other issues the patient may have, such as heart failure, pneumonia or a stroke. The guidelines help the nurses utilize best practices for these problems. Informatics helped make the record personal for the patient and meaningful for the nurse.

TEXAS
Jennifer F. Russell, MSN/INF, RN, PMP Sr. Applications Analyst
Methodist Hospital System Houston, TX
I was working as a nurse in the Emergency Department seven years ago when I realized that the decisions regarding software and technology did not make sense to me. I found myself saying “if they would have asked me I would have done it differently”. I realized that I had a unique opportunity to enter health care IT and make a difference for clinicians and patients. I felt like many times IT was making decisions that ultimately affected our patient care, but didn’t understand the impact or the work flow. This was a driver for me to make a difference. Since that time I have been full time in health care IT for the past seven years working to integrate evidence based practices and streamlined workflows into the software that clinicians use while ensuring that the software also meets the needs of the IT organization. I believe that software makes patient care safer and allows for better communication between care providers. This improves the patient’s continuity of care and outcomes. The delivery of health care is my passion and I want everyone to receive the care I would want for my parents, husband, or children, this is why software is so important. It provides us with the ability to standardize care, track metrics and outcomes, and continue to improve in the way we provide care for our patients
VIRGINIA
Natalie C. Drawdy, BA, RNC-MNN, CNIV Clinical Resource Nurse
Bon Secours Memorial Regional Medical Center | Mother Infant Unit Mechanicsville, VA
When you think of nursing informatics; computerized charting, electronic MAR’s, and patient barcode scanning most readily come to mind. These applications have unquestionably prevented errors and saved lives, but informatics also plays another vital role within the nursing profession in the implementation of nursing research and data collection. As a Clinical Resource Nurse on a busy Mother Infant Unit, my role involves utilizing research to promote evidence based clinical practice at the bedside. Our latest project involves changes in our practice related to the care of late preterm infants admitted to the newborn nursery. These changes in practice include more frequent vital sign monitoring and specific interventions such as gestational age exams, feeding assessments, and delayed bathing. With the implementation of new practices, we are obligated to track and measure their related outcomes. Prior to computerized charting, chart review and data collection could be a painstaking process. Information that can now be retrieved in a few minutes could have taken hours to collect. I can audit charts by running reports for specific information and quickly correlate that information to patient outcomes, staff/patient educational needs, or measure required documentation compliance. For instance, I can determine how many babies are receiving delayed bathing and how well they return to and maintain normal body temperature post-bath versus babies that receive baths sooner. For these vulnerable babies, an intervention as simple as a bath can have potential negative consequences. Understanding the positive outcomes of a new clinical practice through data analysis helps nurses see the value and benefits for patients, especially those that cannot speak for themselves.

VIRGINIA
Patricia J. Mook RN, MSN, NEA-BC AVP/CNE
Epic Principal Lead - Clinical Operations Inova Health System
Springfield, VA A year ago I was appointed by Inova’s Chief Nurse Executive to be the clinical lead for development and implementation of Inova’s new electronic medical record (EMR) system. This was an enormous endeavor as Inova’s five hospitals and more than 50 outpatient sites had set a target to complete the EMR design, build and implementation (for more than 16 clinical and revenue cycle applications) in two years’ time. My first priority was to assist in assembling an implementation team of more than 100 people from throughout Inova, 52 of which are registered nurses. This team worked diligently to get certified as analysts/ builders of Epic, the vendor of our new EMR system. Rather quickly, nurses went from bedside to informatics, where they use their experience and knowledge of nursing to improve healthcare delivery. Our goal is simple: enhance the quality of clinical care and nursing practice at Inova through improved communication, documentation and efficiency. Our team is responsible for building and implementing an EMR that will change all aspects of a patient’s nursing care, from admission to discharge. We have come to recognize how technology is drastically altering the ways nurses diagnose, treat, administer, care for and manage their patients. Through this amazing journey I have come to realize how the integration of information technology into nursing can improve access to patient information at the point of care, and enhance our ability as nurses to benchmark, monitor and audit quality measures. This would no longer be a manual process. This EMR implementation project has fueled my passion for nursing informatics, nursing technology and innovation. I see the impact of technology in improving patient outcomes and enabling higher quality patient- nurse interactions. I am excited to be able to lead a remarkable group of clinical nurses that are shaping and improving the technology of nursing practice!

VIRGINIA
Victoria Richardson, RN-BC, Lean Six Sigma Green Belt
Clinical Informatics Manager Bon Secours Health System, Inc. /St. Mary’s Hospital
Richmond, VA
Karen Jones, RN, BSN, CPC, Juran Six Sigma Green Belt Director of Project Management/Clinical Informatics
Bon Secours Memorial Regional Medical Center Richmond, VA
Victoria Richardson and Karen Jones continue picking up steam as they continue their Journey on the Nursing Locomotive Train. Below is a brief history about the both of them which has led them to the Nursing Informatics track and EMR Functionality and Legalities. Victoria Richardson desire has always been to teach. She takes pride and pleasure in sharing knowledge, and creating structures and processes for knowledge transfer. Victoria chose nursing as her venue. She has been a registered nurse since 1986, working in a variety of roles, including M/S, Diabetes Case Management, Home Health, and a variety of management positions. Appointed as project manager for implementation of the electronic medical record, she led teams through a successful go-live and adaption of changed workflows. Now as Clinical Informatics Manager, works for system stabilization and optimization, with the goals of adoption, increased quality care, and decreased organizational liability. Karen Jones loves advocating and caring for people. She pursued her nursing degree and has been in nursing for over 15 years, working in the areas of Case Management, Corrections, Community Health, and Practice Management where advocacy and caring go hand in hand. Currently, Karen is the Clinical Informatics Lead /Director of Project Management for two facilities in Virginia and is pursuing her Masters in Juris Prudence in Health Care Law and Policy. Karen shares information gained from her Master’s Program to bring awareness of policy, procedures, and regulatory standards compliance as it relates to the EMR. Nursing Informatics means Nurturing, Uplifting, Rejuvenating, Supporting, and Educating people with technology. Here is an Informatics journey. April 4, 2010, two of the four Bon Secours Richmond acute care facilities went live with its EMR, converting 880 nurses in addition to providers and others from paper to computer. Shortly thereafter, on November 1, the third and largest hospital transitioned an additional 953 nurses to the electronic system.

Post implementation, the Clinical Informatics Leads, Karen Jones and Victoria Richardson utilized focused group meetings, skill fairs, at elbow (re)training and weekly supplemental huddle entries as a way to provide nursing staff and others with need to know information as this ever changing, fluid system evolved. This month, the C.I. duo, recognizing disconcerting trending results from chart audits, problem tickets logged, direct observations, and conversations with nurses and providers, developed EMR: Functionality and Legalities: What Should You Do? During the summer, every 2 weeks in Huddle, staff is given the opportunity to respond to a question or situation related to the practical use of our EMR. The purpose? Having the experts – front line staff - identify educational and/or policy gaps, which are then addressed to improve care at the bedside and decrease staff and organizational liability due to unawareness and/or lack of updated or communicated policies.