fluid _electrolytes_in_the_surgical_cli
TRANSCRIPT

Paulette Hamner RN,MSNPaulette Hamner RN,MSN
NUR 1213NUR 1213
Fluid & Electrolytes in the Fluid & Electrolytes in the Surgical ClientSurgical Client

F&E Outline/Surgical ClientF&E Outline/Surgical Client
At great risk for F&E imbalancesAt great risk for F&E imbalances Can be prevented or minimized by Can be prevented or minimized by
appropriate interventionappropriate intervention Assessment and management begins in Assessment and management begins in
preoperative periodpreoperative period Continues into postoperative periodContinues into postoperative period

Preoperative Period:Preoperative Period:
Review history and assessment for Review history and assessment for potential problemspotential problems
Review lab dataReview lab data In the Outpatient setting various In the Outpatient setting various
methods usedmethods used Hypokalemia most frequent cause of Hypokalemia most frequent cause of
cancellation of elective surgerycancellation of elective surgery

HypokalemiaHypokalemia
ManifestationsManifestations Most serious are cardiacMost serious are cardiac Skeletal muscle weaknessSkeletal muscle weakness Weakness of respiratory musclesWeakness of respiratory muscles Decreased gastrointestinal motilityDecreased gastrointestinal motility

Preop. Cont.Preop. Cont.
If hypokalemia is caused by diuretics have If hypokalemia is caused by diuretics have a magnesium level checked.a magnesium level checked.
Replace only after adequate urine output is Replace only after adequate urine output is establishedestablished
Fluid RestrictionFluid Restriction NPO after midnightNPO after midnight Permission for unrestricted intake of cl. Permission for unrestricted intake of cl.
Liq. Up to 3 hrs. preop.Liq. Up to 3 hrs. preop. Oral meds with 30ml of H2O 1 hr. preop.Oral meds with 30ml of H2O 1 hr. preop.

Preop. Cont.Preop. Cont.
Use of H2 blockers if have increased risk of Use of H2 blockers if have increased risk of regurgitation and aspiration of gastric regurgitation and aspiration of gastric contents.contents.
If client has predisposing factors such If client has predisposing factors such as chronic illnessas chronic illness
If on chronic corticosteroid therapy If on chronic corticosteroid therapy

Postoperative Period:Postoperative Period:
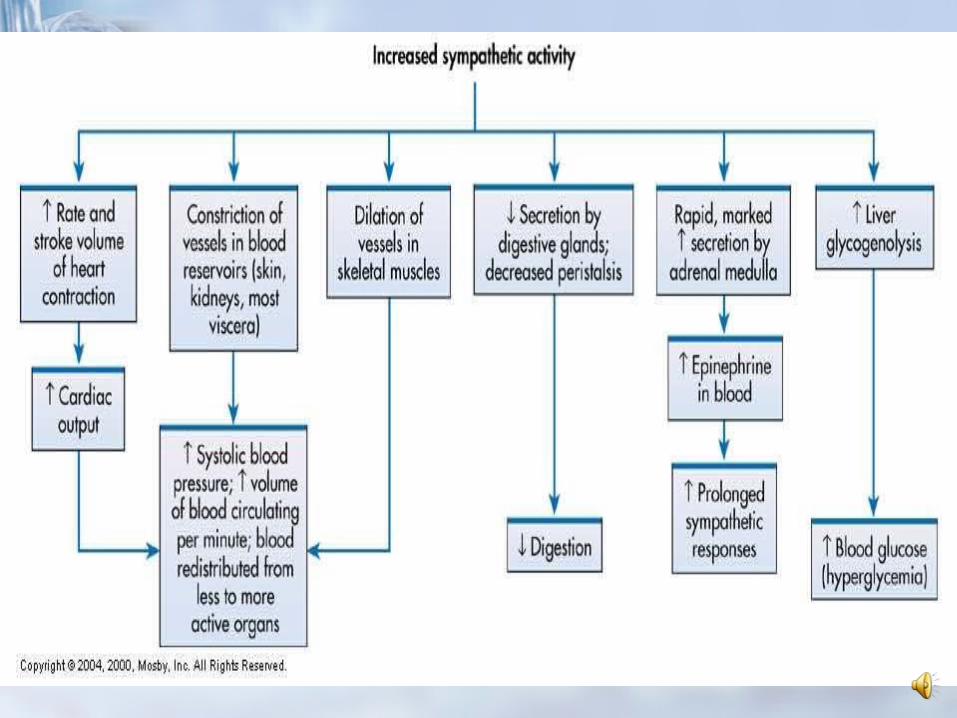
Neuroendocrine response stimulated by Neuroendocrine response stimulated by many anesthetic agentsmany anesthetic agents
Surgical stress by secreting ACTH and Surgical stress by secreting ACTH and cortisol.cortisol.
Many changes happenMany changes happen Circulatory instabilityCirculatory instability
R/T fluid loss during surgery or trauma R/T fluid loss during surgery or trauma that produces decreased renal perfusion.that produces decreased renal perfusion.
This stimulates production of renin, This stimulates production of renin, angiotensis, and aldosteroneangiotensis, and aldosterone

Postop cont.Postop cont.
Causes vasoconstriction and Na and H2O Causes vasoconstriction and Na and H2O conservationconservation
In humans- Isotonic fluid loss (blood)- In humans- Isotonic fluid loss (blood)- most potent stimuli to aldosterone and most potent stimuli to aldosterone and ADH secretion.ADH secretion.
Surgery and trauma can cause the Surgery and trauma can cause the release of aldosterone and ADHrelease of aldosterone and ADH
May last for 12-24 hrs. post-opMay last for 12-24 hrs. post-op Reduced vol. of conc. Urine early post-Reduced vol. of conc. Urine early post-
opop

Postoperative Period cont.:Postoperative Period cont.:
Decreased urine is due to hormonal Decreased urine is due to hormonal changeschanges
Increases the chance of hypokalemia if Increases the chance of hypokalemia if K+ is inadequateK+ is inadequate
In elderly-Neuroendocrine response-In elderly-Neuroendocrine response-increased morbidity especially increased morbidity especially cardiovascular surgery.cardiovascular surgery.
Have a prolonged inadequate secretion Have a prolonged inadequate secretion of ADH-dilutional hyponatremia orof ADH-dilutional hyponatremia or
Suppression of ADH-lg. amt. of diluted Suppression of ADH-lg. amt. of diluted urineurine
Extreme thirst, dehydration, Extreme thirst, dehydration, hypernatremia hypernatremia

Postop cont.:Postop cont.:
Metabolic Changes:Metabolic Changes: First hours post-op=increased blood First hours post-op=increased blood
glucose levelsglucose levels This may result from secretion of growth This may result from secretion of growth
hormone and glucagon and suppression hormone and glucagon and suppression of insulin release.of insulin release.
Hemodynamic Alterations:Hemodynamic Alterations: Increasing catecholamines (epi, norepi)Increasing catecholamines (epi, norepi) Have marked effect on CNS and CVSHave marked effect on CNS and CVS


Postop: Postop: Fluid and Fluid and Electrolyte ImbalanceElectrolyte Imbalance
Most common imbalance is extracellular Most common imbalance is extracellular third spacing-Fluid Volume Deficitthird spacing-Fluid Volume Deficit
““fluid loss” from the vascular space pools fluid loss” from the vascular space pools in another part of the body-surgical site in another part of the body-surgical site or bowel from an ileus. or bowel from an ileus.
Factors-GI fluid loss, cont. fluid shifts, Factors-GI fluid loss, cont. fluid shifts, fever, too many blood samples, fever, too many blood samples, hyperventilation, diuretics.hyperventilation, diuretics.
If FVD is due to third spacing there is no If FVD is due to third spacing there is no decrease in body weight.decrease in body weight.

Fluid Volume Deficit Fluid Volume Deficit (FVD)(FVD)
Decreased U.O. <30ml/hrDecreased U.O. <30ml/hr Postural hypotensionPostural hypotension TachycardiaTachycardia Diminished skin turgorDiminished skin turgor Decreased capillary refill timeDecreased capillary refill time Inc. BUN out of proportion to creatinineInc. BUN out of proportion to creatinine
Treatment:Treatment: Depends on type of fluid lostDepends on type of fluid lost Usually can be done with Isotonic Usually can be done with Isotonic
solutions- NS or LRsolutions- NS or LR
F&E Imbalances Postop F&E Imbalances Postop cont:cont:
Fluid Volume Excess (FVE):Fluid Volume Excess (FVE): Due to seepage of lg volumes of fluid Due to seepage of lg volumes of fluid
from the vascular space into a third from the vascular space into a third space.space.
As fluids are administered to correct As fluids are administered to correct vascular losses=added fluid load.vascular losses=added fluid load.
Most common causes are:Most common causes are: Overcorrection of a previous FVDOvercorrection of a previous FVD Poorly guarded IV linePoorly guarded IV line Treating pain with MorphineTreating pain with Morphine Can occur anytime but usually immediately Can occur anytime but usually immediately
post-oppost-op
F&E Imbalances post-op F&E Imbalances post-op cont.cont.
Hyponatremia R/T:Hyponatremia R/T: Excessive temporary ADH secretionExcessive temporary ADH secretion Nausea without vomitinNausea without vomitin Elevated ADH plasma levelsElevated ADH plasma levels
Avoid using hypotonic solutionsAvoid using hypotonic solutions Avoid excessive use of electrolyte free Avoid excessive use of electrolyte free
solutions during the first 2-4 post-op dayssolutions during the first 2-4 post-op days Serum Na+ should be kept between Serum Na+ should be kept between
130-135 mEq/ml130-135 mEq/ml

F&E Imbalances post-op F&E Imbalances post-op cont:cont:
HypokalemiaHypokalemia Most common K+ imbalance post-opMost common K+ imbalance post-op May be lost through urine or GIMay be lost through urine or GI Usually not present in the first 24 hrs. Usually not present in the first 24 hrs.
post-oppost-op Replacement may be needed after the Replacement may be needed after the
initial 24 hour periodinitial 24 hour period Daily supplement may be 60-100 mEq Daily supplement may be 60-100 mEq
QD.QD.

F&E Imbalances post-op F&E Imbalances post-op cont.cont.
HyperkalemiaHyperkalemia Rare except for the client with acute Rare except for the client with acute
renal failure, tissue necrosis, or renal failure, tissue necrosis, or hemolysishemolysis
If occurs at anytime during the post-op If occurs at anytime during the post-op period, renal function should be period, renal function should be assessed.assessed.
Release of cellular K+ by crush injuries, Release of cellular K+ by crush injuries, electrical injuries or acute renal failure electrical injuries or acute renal failure can lead to lethal hyperkalemia within can lead to lethal hyperkalemia within hours.hours.

F&E Imbalances post-op F&E Imbalances post-op cont.cont.
Hypocalcemia:Hypocalcemia: May be due to a parathyroidectomy, May be due to a parathyroidectomy,
thyroidectomy, or radical neck dissectionthyroidectomy, or radical neck dissection May occur immediately or 1-2 days post-May occur immediately or 1-2 days post-
opop Lasts less than 5 daysLasts less than 5 days Most client remain asymptomaticMost client remain asymptomatic Some develop paesthesias, laryngeal Some develop paesthesias, laryngeal
spasms or tetany.spasms or tetany.
Acid-Base Disorders post-opAcid-Base Disorders post-op
Resp. Acidosis from shallow Resp. Acidosis from shallow respirationsrespirations
Resp. Alkalosis due to pain, hypoxia, Resp. Alkalosis due to pain, hypoxia, CNS injury, and mechanical CNS injury, and mechanical ventilationventilation
Metabolic Alkalosis usually from NG Metabolic Alkalosis usually from NG drainage or vomiting or K+ wasting drainage or vomiting or K+ wasting diuretics.diuretics.

Outpatient Surgery Outpatient Surgery ConsiderationsConsiderations
Seldom have F&E imbalances but do Seldom have F&E imbalances but do require assessment and nursing require assessment and nursing interventions if occursinterventions if occurs
Oral intake is encouraged when gag Oral intake is encouraged when gag reflex returns, no nausea, client is reflex returns, no nausea, client is sufficiently alertsufficiently alert
Assessment of urine output and Assessment of urine output and bladder distentionbladder distention
Thorough post-op instructionsThorough post-op instructions Follow-up call the day after surgeryFollow-up call the day after surgery