fluid metabolism
TRANSCRIPT


FLUID BALANCE MAINLY DEALS WITH METABOLISMS:-
1.Sodium 2.Pottassium3.Chlorine4.Water

ECF- extra cellular fluid it is present outside the cell >> comprises about 50% of body weight >>main cation of ECF – Na >> Cl exists with Na as ECF
ICF – Intra cellular fluid is present inside the cell .>> comprises about 20% of body weight
including :* Plasma * Interstitial fluid
>> main cation of ICF is - K
ECF & ICF

Sodium is the primary cation of ECF.Most of the body’s sodium is located in blood and in the fluid arround the cellsBody obtains Na through food and drink and looses it primarily in sweat and urine .Healthy kidneys maintains constiencyin excretion of urine
SODIUM :

It helps the body to keep fluids in a normal balance
It plays a key role in normal nerve and muscle function
Helps in osmo-regulationHelps in preservation of permeability
of cell
helps to maintain normal blood pressure.
FUNCTIONS:-

It is present mainly in blood serum
Normal serum conc. Of Na–320mg /100ml
Na is also seen in erythrocytes , but very less in conc.
Distribution:

When the conc. Of sodium in blood is too low – HYPO NATREMIA
When the conc. Of Sodium in blood is too high – HYPER NATREMIA
Imbalance of Sodium Ions Causes:

Hyponatremia –true loss of sodium
Poor renal reabsorption
Indicated by excessive vomiting,weightloss
Renal diseases with acidosis
Hyponatremia -due to overhydration
Accumulation of fluid due to odema
Occurs more in cirrhosis of liver
heart failure

• In case of HYPONATREMIA - decrease in its concentration, there is more release of water to store more sodium which the body needs clearly.
• A low sodium level has many causes, including consumption of too many fluids, kidney failure, heart failure, cirrhosis, and use of diuretics.
• At first, people become sluggish and confused, and if hyponatremia worsens, they may have muscle twitches and seizures and become progressively unresponsive.

Increased sodium level in serum
May occur due to ;-
Hyper activity of adrenal cortex Cushing’s Syndrome.
Prolonged administration of cortisone ,ACTH etc.
Hypernatremia:

Cushing’s syndrome

Sources
Mono sodiun glutamate (msg)
Olives
Sources

RDA of sodium – 3,000mg/day
It is to be noted about the difference between Sodium and Salt….
Na – mineral
Table salt contains only 40% of Na….
Increase of intake of salt on other hand causes HYPERTENTION

Most of the potassium is located inside the cells (inter cellular ion).
It is an essential macro nutrient
K+ is one of the most permeable ion across cell membranes and exits the cells mostly via K channels (and in some cells via K-H exchange or via K-Cl co - transport)
Potassium:

Lesser amount of K is present in serum
Normal serum conc. Of K is –19mg/100ml
In erythrocytes is – 440mg/100ml
Distribution:

It is necessary for normal functioning of cells and muscles conduction
Maintains membrane potential
Maintains Fluid balance
Helps in Neuro transmission
Acid – base regulation
Its deficiency conditions
are:-
Functions:

A low potassium level(3.5 mmol/L) has many causes but usually results from vomiting, prolonged diarrhea, adrenal gland disorders(Cushing’s syndrome).
”FAMILIAL PERIODIC PARALYSIS”
A low potassium level can make muscles feel weak, cramp, twitch, or even become paralyzed, and abnormal heart rhythms may develop.
Hypokalemia;

It occurs due to mutation of membranes of electrolyte channels
Symptoms :
>loss of muscle movement due to weakness
> occurs in hips , shoulders
‘’FAMILIAL PERIODIC PARALYSIS”


A high potassium level has many causes, including kidney disorders, drugs that affect kidney function, and consumption of too much supplemental potassium.
Usually, hyperkalemia must be severe before it causes symptoms, mainly abnormal heart rhythms.
Treatment includes reducing consumption of potassium, stopping drugs that may cause hyperkalemia, and using drugs to increase potassium excretion.
Hyperkalemia:

Infants – 0-6 months – 400 mg/day
- 1-3 yrs -- 3000 mg/day
-- 9-13 yrs -- 4500 mg / day
Children older than 13 yrs and adults –4700mg/day
Lactating women – 5100 mg /day
RDA

SourcesSpinach
Apricot

Avacadoes
Broccoli

Chief ECF anion
Present in plasma and expressed as NaCl
Normal plasma conc. 500-550mg/100ml.
Cl conc. Is more in CSF than in plasma
Chlorine:

It is present in plasma - 500-550mg/100ml
But Cl conc. is more in CSF – 600-620mg/100ml
Distribution:

Acid – base balance
Chloride shift
Helps in formation of HCl in gastric juice
Salivary amylase is activated by chlorine
Are its Functions

NaCl- 5-10gms
Dietary req.

Sources

Hypochloremia- a reduction in the serum Chlorine level
Which will occur due to
Vomiting
Diarrhea
respiratory alkalosis
Addison’s disease and excessive sweating
Disease State:

Disorder in which the adrenal glands do not produce sufficient steroid hormones
Addison's disease

An increase in serum chloride level conc.
Which may lead to
Dehydration
respiratory acidosis
Cushing’s syndrome
Hyperchloremia:

Water forms 60-70% of the body weight distributed throughout the body
It is closely associated with electrolyte distribution in body
Intercellular compartment ,comprises fluid present inside the cells
Extracellular compartment ,comprises the fluid present outside the cells.
Water:

Solvent for electrolytes
Regulator of body temperature
Carrier of nutrients
Regulates electrolyte balance
Are its Functions…
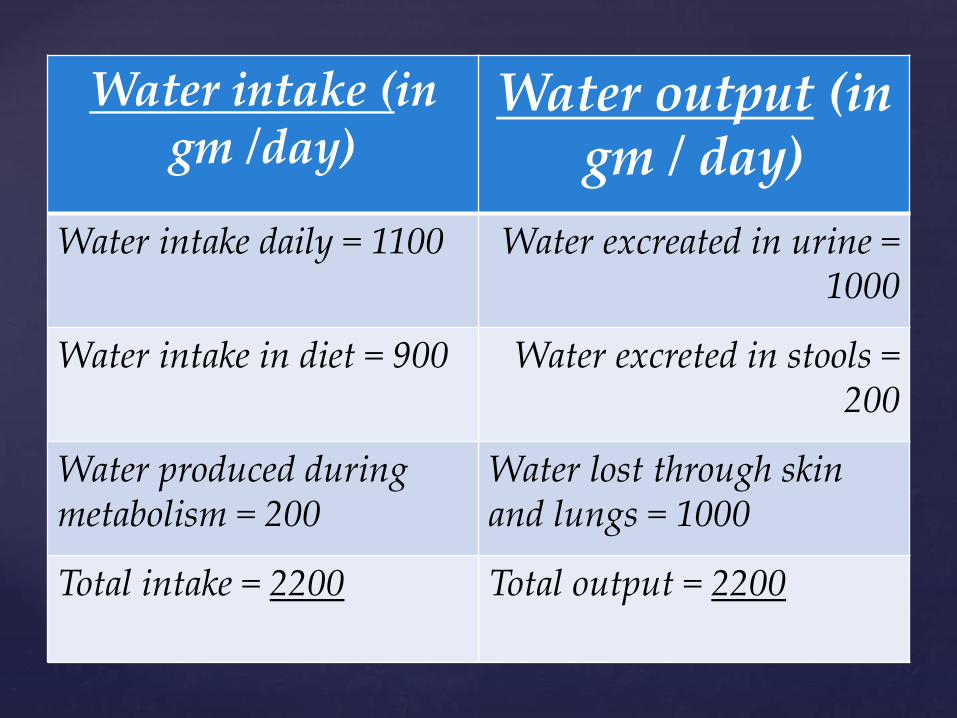
Water intake (in gm /day)
Water output (in gm / day)
Water intake daily = 1100 Water excreated in urine = 1000
Water intake in diet = 900 Water excreted in stools = 200
Water produced during metabolism = 200
Water lost through skin and lungs = 1000
Total intake = 2200 Total output = 2200

• Water gain: water consumed during drinking,in foods, formed during oxidation of foods, metabolic process
Water lost: from skin, sweat etc.


The kidneys stimulate the adrenal glands to secrete the hormone aldosterone.
Aldosterone causes the kidneys to retain sodium and to excrete potassium. When sodium is retained, less urine is produced, eventually causing blood volume to increase.
The pituitary gland secretes antidiuretic hormone. Antidiuretic hormone causes the kidneys to conserve fluid. Then blood volume increases.
Mechanism of Na:

When the conc. of Na increases in body info is passed through:
Sensors in heart
Blood vessels
(finally)
Kidneys detect the increase and stimulates
it to be in normal
Beauty of the body!..

Potassium homeostasis depends on maintenance of external and internal potassium balance
External potassium balance -potassium intake (100 meq/day) and rate of urinary (90 meq/day) and fecal excretion (10 meq/day).
Internal potassium balance - distribution of potassium between muscle, bone, liver, and red blood cells (RBC) and the extracellular fluid (ECF).
Potassium homeostasis

Hyperkalemia :- high level of potassium in blood
The serious consequences of these condition are:- abnormal heart rhythm, cardiac arrest
Hypokalemia :- Low level of potassium in blood

K is consumed in food & drinks that contain electrolytes and lost primarily in urine
Some K is lost through sweat.
Healthy kidneys can adjust the excreation of K to match changes in consumption.
Mechanism how the body maintains …

Body maintains the right level of K by matching the amount of K consumed that of the amount lost….
regulated by alterations in excretion in the distal renal tubule, where mineralocorticoid hormones and Na-K ATPase are the major regulating factors. The distribution of potassium across cell membranes is influenced by changes in acid-base status, by pancreatic hormones and by the autonomic nervous system

Na and Cl metabolism is so much inter related as,
The loss of Na in sweat ,urine is accompanied with more loss of Cl
It results in low level of plasma chloride,andthus there is increase in Bicarbonates with consequent alkalosis
Metabolism of Cl:

Health is wealth!!...
Due to action of ADH
Regulates the excess loss of water by Kidneys
Exception:- in diabetes insipidus
Balancing is seen when
water intake=water output
Balancing of water !!

Finally, FLUID METABOLISM in body is
looked after by our KIDNEYS and our cell membranes which will
help in transportation of ions andmaintains the acid-base balance….
Body has a very good mechanism to manage everything ….