folic acid article
TRANSCRIPT

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 1/13
Folic Acid-Based Intervention in Non-ST ElevationAcute Coronary Syndromes
Marcelo Severino B Imasa, MD1, Neil T Gomez, MD2, Jose B Nevado, Jr, MD3
1 Department of Pharmacology, University of the Philippines College of Medicine, Manila2
Philippine Heart Center, Quezon City3
Department of Biochemistry and Molecular Biology, University of the Philippines College of Medicine,Manila
Jose B Nevado, Jr, MD, Tel: +240 301 482 9625, Fax: +(632) 526 4197 301 451 7090,Email: [email protected], 547 Pedro Gil Street, Ermita, Manila, Philippines.
ABSTRACT
Homocysteinemia is a risk factor for cardiovascular diseases. Folic acid combined withvitamins B6 and B12 is effective in lowering homocysteine levels. This randomized placebo-
controlled
study was designed to determine the effect of a folic acid-based
supplement onsecondary prevention of clinical events in non-ST-segment elevation acute coronary syndromes.The study comprised 240 patients with either unstable angina or non-ST-elevationmyocardialinfarction in the previous 2 weeks who were randomized to a folate group (n =116) or a placebo group (n =124). The folate group received 1 mg folic acid, 400 µg vitamin B12, and 10mg vitamin B6 daily. Clinical outcomes within 6 months were assessed. The composite endpointof death, nonfatal acute coronarysyndrome, and serious re-hospitalization was significantlyhigher in the folate group; serious re-hospitalization alone was significantly higher in this group.
Advanced age and diabetes increased susceptibility to the composite outcome. Folic acid-basedsupplementation is not beneficial and may even be harmful in the secondary prevention of cardiovascular events in patients with unstable angina and non-ST-elevation myocardialinfarction. Further studies on the safety of such supplements are suggested. Controlled
Clinical
Trials Registry no. ISRCTN30249553.
INTRODUCTION
A raised plasma homocysteine level is a risk factor for cardiovascular diseases.Extensive systematic reviews summarize the numerous clinical studies and reveal a strongassociation between highhomocysteine levels and coronary heart disease, stroke,and peripheral venous thrombosis. A causative effect of homocysteine was further supported bystudies demonstrating that homocysteinemia can induce endothelial dysfunction inhumans. Considering that homocysteine might be a modifiable risk factor for cardiovascular diseases, clinical trials were initiated to determine the therapeutic effect of lowering homocysteine levels. Almost all of these trials made use of folic acid, which has been
shown to significantly
decrease homocysteine levels. Folic acid serves as a cofactor
in the mainpathway for converting homocysteine to nontoxic methionine. In 1998, a meta-analysisdemonstrated that folic acid supplementation of 0.5 to 5 mg per day reducedhomocysteinelevels by a quarter to a third. In the same study, vitamin B12
was estimated tocontribute a 7% mean reduction in homocysteine levels at 0.5 mg per day. Daily intake of 2 mgfolic acid alsosignificantly reduced homocysteine levels by 1.8 µmol · L ±1 in patients withprevious myocardial infarction (MI) or unstable angina after 6 months of treatment. Bylowering homocysteine levels with folic acid supplementation, usually in combination withvitamins B6 and B12, clinical studies have shown trends toward a parallel decrease in the

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 2/13
occurrence of cardiovascular events such as stroke, MI, and peripheral vascular disease. In2001, a research group in Switzerland observed that folic acid supplementation decreased by athird the rate of coronary artery restenosis in patients who had undergonecoronary angioplasty. Since then, several clinical trials have been initiated to assess thecardiovascular effects of folic acid supplementation. Unfortunately, no significant reduction inmortality or nonfatal cardiac events was noted in any of these studies. A recent meta-analysis of
randomized controlled trials did not find conclusive clinical benefit of using folic acid incardiovascular diseases.
Non-ST-elevation myocardial infarction (NSTEMI) and unstable angina belong to thespectrum of acute coronary syndromes (ACS) that imply partial occlusion of the coronaryarteries, leading to ischemic events. These conditions are significant indicators of impending MIwhich can be fatal or may require intensive hospital care. Unstable angina and NSTEMI havehigh rates of recurrence in ACS and mortality within 6 months after an event.Bloodhomocysteine levels are higher in patients with unstable angina. In addition to being a riskfactor, elevated homocysteine is also implicated in poorer outcomes and greater myocardial injury in unstable angina and NSTEMI. In epidemiologic studies, low homocysteinelevels seemed to confer better long-term outcomes in patients with coronary heart
disease.17 Thus, in view of current evidence, it was hypothesized that loweringhomocysteine levels might reduce subsequent clinical events in patients with recent unstableangina or NSTEMI. As no randomized controlled trial on the use of folic acid-basedsupplementation in this subset was available, this study sought to determine whether suchsupplements could lower the incidence of mortality, nonfatal acute coronary events, serious re-hospitalization, or a composite of these endpoints in such patients, especially in the first 6months after an event.
PATIENTS AND METHODS
Patients with unstable angina or NSTEMI in the previous 2 weeks were screened for inclusion in the study. The study recruited 243 patients from 5 medical centers in the Philippines:
Philippine Heart Center (133), Philippine General Hospital (92), Quirino Memorial MedicalCenter (7), Ospital ng Maynila Medical Center (6), and East Avenue Medical Center (2). TheEthical Review Board of the Research Implementation and Development Office of the Universityof the Philippines College of Medicine approved the protocol.
All patients provided informed consent. However, the number of prospects assessed for eligibility was not routinely recorded, including their reasons for non-participation. Of therecruited patients, 118 were assigned to folic acid supplementation and 125 were assigned tothe placebo group. Exclusion criteria included hemodynamic instability (cardiogenic shock,ongoing chest pain, unresolved and new-onset end-organ damage, and unstablecongestive heart failure in the previous 2 weeks), significant liver disease (classic signs andsymptoms, or liver enzyme levels 3 times the upper limit of normal, or prothrombin time >1.5
times normal), significant renal disease (creatinine >180 µmol · dL ±1 or requiring dialysis),hemoglobin <10 g · dL ±1, high-output failure, inability to provide adequate self-care, malignancyor any terminal illness, age <18 years, pregnancy, and residency outside Metro Manila or theadjacent provinces of Cavite and Rizal. In view of the finding that folic acid-based supplementsincreased the rate of in-stent restenosis, patients who had revascularization procedures wereexcluded.8 Those who joined the study and then had a revascularization procedure wereadvised to discontinue intake of supplements, but were included in the final analysis according

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 3/13
to their original assignment. Baseline characteristics were collected by interview with aquestionnaire.
The study is a double-blind placebo-controlled trial. Patients underwent randomizationusing predetermined randomization provided to the pharmacy by the study statistician. Amember of the pharmacy staff, who had sole knowledge of patient assignment,
randomly allocated and dispensed the treatment. Patients in the folate group were instructed toingest a supplement tablet (1 mg folicacid, 400 µg vitamin B12, and 10 mg vitamin B6) daily for 6months in addition to their prescribed treatment for unstable angina or NSTEMI. The controlgroup received a placebo tablet daily for 6 months with their conventional treatment.Conventional treatment included anticoagulants, platelet inhibitors, beta blockers, andnitrovasodilators. Any suspected serious adverse effect of the supplement resulted intermination of the treatment.
Follow-up was conducted after 1, 3, and 6 months of treatment. The duration of treatment was based on available data that indicated >90% of adverse cardiac events after onset of NSTEMI or unstable angina occur within the first 6 months after an acutecoronary event.14,18 The patients¶ attending physicians also conducted follow-up examinations at
their own discretion. Outcomes beyond6 months after the start of the trial were not included inthe analysis. The primary outcomes consisting of death, nonfatal ACS, and serious re-hospitalization were assessed using a hierarchaldesignation, that is, in decreasing priority.
Accordingly, only 1 clinical endpoint was assigned to each patient. ACS was defined as acuteMI, NSTEMI, or high- or medium-risk unstable angina.Serious re-hospitalization was defined asan emergency admission to hospital, which required airway or circulatory support for at least 1day, as decided by the attending physician.
Homocysteine levels were determined using an Abbott IMx analyzer (AbbottLaboratories, Abbott Park, IL, USA). Dyslipidemia was defined as total cholesterol >190 mg · dL ±
1, low-density lipoprotein >160 mg · dL ±1, or use of a cholesterol-lowering drug.
Analysis was intention-to-treat. Baseline characteristics and clinical endpoints wereanalyzed with appropriate tests, using STATA version 6.0 software (Stata Corp., CollegeStation, TX, USA). Forest graphs were constructed using the software of Clark O, Djulbegovic B.Forest plots in excel software (data sheet), 2001, available at: www.evidencias.com. The samplesize (243) was less than the projected 404 patients expected to be recruited to have a power of 0.80 to detect a 20% reduction in the composite endpoint alone, using the 31.4% incidence inthe PRISM-PLUS study.14Nevertheless, a significant divergence emerged early between the 2groups to warrant termination of the study. Due to the inadequate sample size, adverse eventsare summarized and described without attempting statistical comparison.
RESULTS
The study recruited 243 subjects. However, 3 patients were excluded after recruitment(Figure 1 ): 1 from each group was found to have persistently increased creatinine and requiredchronic renal support, despite a normal creatinine level in the emergency room; another in thefolate group had persistent anemia due to thalassemia, after an initially normal hemoglobin.These patients were excluded during the first 3 days after inclusion as such conditions cantheoretically augment the benefit of folic acid-based supplementation. No adverse outcome wasassessed in these patients upon exclusion, and they did not receive their allocated treatmentbeyond 1 month, the duration for the minimum volume of supplement provided. Three patients

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 4/13
were lost to follow-up, thus using intention-to-treat analysis, 2 in the folate group were assumeddead, while the data of 1 in the placebo group were considered missing. Compliance with thetreatment was also determined (Table 1 ); there was no significant difference between groups.Those taking the folic acid-based supplement tended to have decreased compliance in the earlypart of the study, but the level of compliance became almost equal towards the end, with morepatients in the placebo group sustaining their intake until 6 months. The main reasons for
discontinuing treatment included the occurrence of a possible adverse event (18patients), inability to present for follow-up due to financial constraints (48), failure to comply dueto attending physician¶s advice (2), transfer to areas remote from the follow-up centers (12), andunspecified reasons (2). Thus, data from 240 subjects were available for analysis. Table 2summarizes the baseline characteristics of the participants according to treatment group. There
was no significant difference in patient profiles between groups. The baseline homocysteinelevels did not differ significantly despite an individual in the placebo group having a levelof 159.5 µmol · L ±1(upper normal limit, 16 µmol · L ±1); no significant difference was noted whenthis subject¶s data were excluded.
Figure 1. Flow diagram of the allocation, follow-up, and analysis of subjects included in the study.

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 5/13
Duration of Intake Folate (n = 116) Placebo (n = 124) p Value*
<1 month 14 (12.1%) 14 (11.3%)
1 to <3 months 16 (13.8%) 28 (22.6%)
3 to <6 months 9 (7.8%) 8 (6.5%) 0.0870
Complete compliance 77 (66.4%) 74 (59.7%)
6 months 57 (49.1%) 42 (33.9%)
Until primary endpoint 20 (17.2%) 32 (25.8%)
*Pearson chi2 comparison.
Table 1. Compliance of patients with allocated treatment
Characteristics Folate (n = 116) Placebo (n = 124) pValue*
Mean age (years) 59.1 59.6 0.7124Males 58.6% 57.3% 0.8311Diabetes mellitus 18.1% 25.8% 0.1510Hypertension 66.4% 66.9% 0.9270Smoking habits 0.8220
Nonsmoker 45.7% 40.3%
Ex-smoker 40.5% 42.7%Occasional smoker 3.4% 4.8%
Regular smoker 10.3% 12.1%Dyslipidemia 32.8% 29.3% 0.5320Body mass index (kg · mm ±2) 24.4 24.2 0.6994Previous history of ACS 37.1% 42.7% 0.3700Type of ACS 0.5339
NSTEMI 34.5% 39.5%High-risk unstable angina 16.4% 18.5%
Medium-risk unstable angina 49.1% 41.9%Stroke 13.8% 13.7% 0.9850Medications
Antiplatelet 91.4% 83.9% 0.0Beta blocker 75.9% 68.5% 0.2069
ACE inhibitor/ARB 81.0% 79.8% 0.8155Hypoglycemic 18.1% 20.2% 0.6857Lipid lowering 62.1% 58.9% 0.6127Nitrovasodilator 79.3% 73.4% 0.2812
On open-label vitamins 10.5% 6.7% 0.1450Plasma creatinine (µmol · L ±1) 99.2 96.9 0.5592Plasma homocysteine (µmol · L ±1) 13.0 12.6 0.7760

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 6/13
*Chi2 test uncorrected. For at least 3 months during the study or until a cardiac event. ACE =angiotensin-converting enzyme, ACS = acute coronary syndromes, ARB = angiotensin-receptor antagonist, NSTEMI = non-ST-elevation myocardial infarction.
Table 2. Baseline patient characteristics
The primary outcomes of death, nonfatal ACS, and serious re-hospitalization were
compared between groups (Table 3 ). The composite endpoint of all 3 outcomes was
significantly higher in the folate groupthan the placebo group. There were significantly more
instances of re-hospitalization in the folate group. Most re-hospitalizations were cardiac related
(3 hypertensive emergencies, 3 cases of acute pulmonary edema, and 1 of bradycardia),
implying that cardiac events were increased by use of the supplements. These observations of
possible harm persisted even if all patients lost to follow-up were considered as missing data. To
demonstrate the time-course of the effect of folate supplementation on clinical outcomes,
probability curves for death and the composite outcome were constructed (Figure 2 ). A trend
suggestive of earlier mortality in the folate group was observed. However, after 6 months,
the mortality rates did not differ significantly. In contrast, a marked divergence in the probability
of event-free status wasnoted; this continued to diverge with time, indicating the persistence
of harm in the folate group. Nonfatal outcomes (re-hospitalization and nonfatal MI) increased from
the 5th week onwards in the folate group, implying that supplement intake could be harmful as
early as 5 weeks after administration, and harm continued as long as the supplement was taken.
Again, this finding persisted even if patients lost to follow-up were considered as missing data.
Endpoint Folate (n 116)
Placebo (n 124)
pValue* Risk Ratio (95%CI)
Mortality 22/116 (19.0%) 20/124 (16.1%) 0.5366 1.18 (0.68±2.04)Nonfatal ACS 15/94 (16.0%) 13/104 (12.5%) 0.4857 1.28 (0.64±2.54)
Re-hospitalization 9/80 (11.3%) 2/89 (2.2%) 0.0161 5.11 (1.14±23.00)Compositeendpoint
46/116 (39.7%) 35/124 (28.2%) 0.0444 1.20 (1.00±1.44)
*Chi2 test. ACS = acute coronary syndrome, CI = confidence interval.
Table 3. Occurrence of primary endpoints based on hierarchal assignment

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 7/13
Figure 2. Probability curves for (A) event-free and (B) survival status of patients during the trial. Event-free probability
was significantly decreased in the folate group (log-rank test: p = 0.0492). Survival probability was not significantly
different (log-rank test: p = 0.5650).
A stratified analysis was performed to determine the effect of specific characteristics on
the relationship between folic acid-based supplementation and clinical outcomes. The
relative risks of age, sex, diabetes, hypertension, smoking, dyslipidemia, previous history of
ACS, stroke, and body mass index are summarized in Figure 3 . The advanced aged subgroup
(>45 years in men, >55 years in women) in the folate group was significantly more vulnerable to
the composite outcome, mainly due to more serious non-ACS events. Diabetes mellitus
conferred a poorer prognosis in terms of the composite outcome in the folate group, with a
strong trend towards more nonfatal ACS. On the other hand, folate treatment showed a
significant protective effect against nonfatal ACS in those with a previous stroke.

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 8/13
Figure 3. Relative risk of placebo (dashed line) vs. folate (solid line) in patients with unstable angina, stratifiedaccording to selected clinical characteristics. The supplement was harmful in terms of composite outcome in those
with advanced age, with a strong trend for increased serious non-ACS re-hospitalization. The supplement washarmful to diabetics in terms of composite outcome, with a strong trend for increased nonfatal ACS; but it was
beneficial against nonfatal ACS in patients with previous stroke. * p = 0.0388. p = 0.0606. p = 0.0275. p =0.0694.
p = 0.0318. ACS = acute coronary syndrome, BMI = body mass index.
None of the selected characteristics provided a differential effect between the groups in
terms of death alone or serious non-ACS or re-hospitalization alone. No significant difference in
outcomes was observed between groups stratified according to homocysteine levels, creatinine
levels, or recruitment center. Table 4 summarizes the non-serious adverse events reported
during the study. Combining the serious non-ACS-related events and non-serious adverse
events, more events were noted in the folate group. Dyspnea was the most common adverse
effect, followed by dizziness and rashes. Dizziness was noted in 3 patients, all in the folate
group. Raised blood pressure and rashes were not discriminated as side effects of the
supplement, because they were also observed in the placebo group. Most of these events in the

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 9/13
folate group occurred within 1 month after the onset of the treatment, suggesting a causative
effect of the active ingredients in the treatment.
Non-Serious Serious Total
Adverse Event Folate Placebo Folate Placebo Folate PlaceboDizziness 3 3Palpitations 1 1Rashes/pruritus 2 1 2 1Dyspnea/CHF 1 1 3 4 1Joint pains 1 1Edema 1 1Rise in BP 2 3 1 3 3Hypoglycemia 1 1Bradycardia 1 1
Abdominal pain 1 1 1 1Hypotension 1 1Stroke 1 1Total 8 6 10 2 18 8
ACS = acute coronary syndromes, BP = blood pressure, CHF = congestive heartfailure.
Table 4. Nonfatal and non-ACS-related adverse events
DISCUSSION
The study found that the composite endpoint of death, nonfatal ACS, and serious re-hospitalization was increased by the use of a folic acid-based supplement in patients withmedium- or high-risk unstable angina or NSTEMI. Notably, a consistently harmful trend wasobserved for the other primary endpoints (death and nonfatal ACS), although the small samplesize limited the detection of significance. While the incidence of all primary outcomes was higher in the folate group, the most significant increase was in the number of serious re-hospitalizations. Most of the events were cardiovascular in nature, implying that mostre-hospitalizations were due to cardiac complications, and such additional events could be directeffects of the multivitamin intake. The presence of increased harm in the folate group was highlyprobable. Moreover, the fact that serious re-hospitalizations usually occurred earlier in the folategroup than the placebo group also implies possible harm due to the use of the supplement.
Similar RCTs on the use of folic acid in coronary disease suggest potential harm. In theHOPE 2 trial, an increase in re-hospitalizations, other than those due to nonfatal MI and stroke,is be inferred.9 In fact, the data showed a significantly higher rate of re-hospitalization due tounstable angina in the multivitamin group. The occurrence of heart failure was also higher in thefolate group, although no significant difference was detected. In the NorwegianVitamin (NORVIT) trial, which was carried out in a country without mandatory folic acidsupplementation in the diet, trends towards harm were also observed that could be due to folicacid-based supplements, in terms of mortality, MI, and composite cardiovascular outcomes. Our
8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 10/13
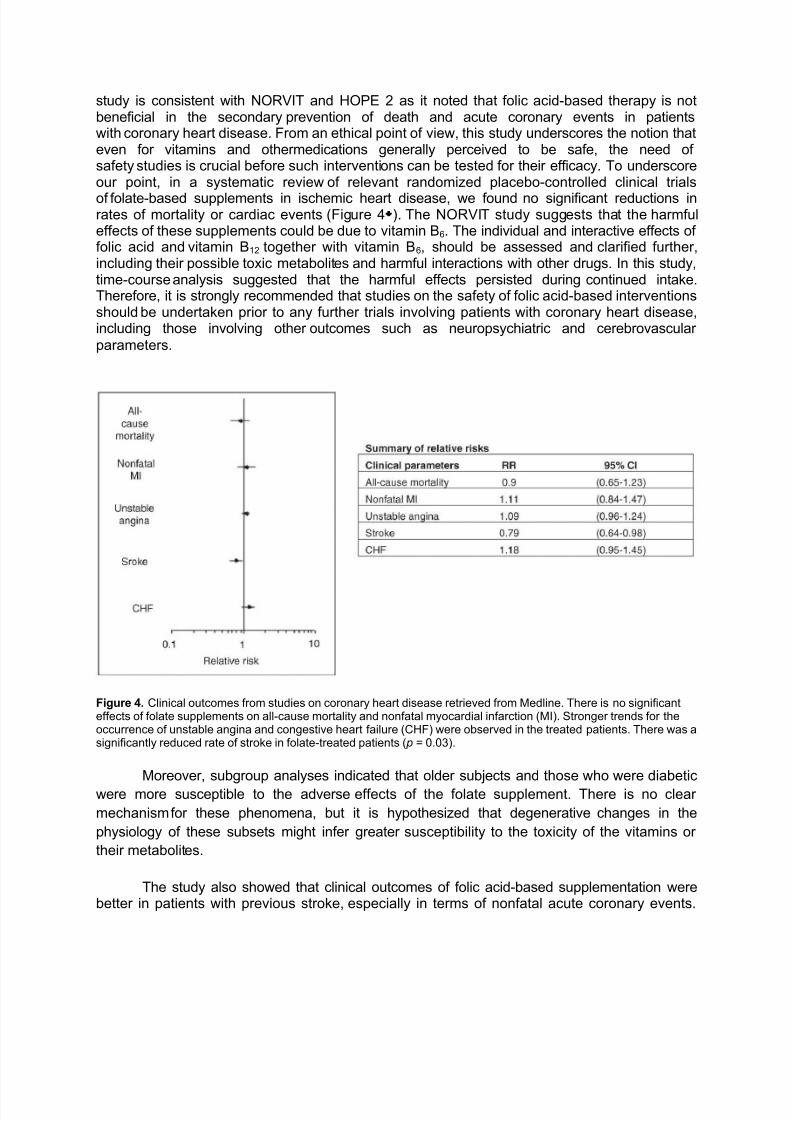
study is consistent with NORVIT and HOPE 2 as it noted that folic acid-based therapy is notbeneficial in the secondary prevention of death and acute coronary events in patientswith coronary heart disease. From an ethical point of view, this study underscores the notion thateven for vitamins and othermedications generally perceived to be safe, the need of safety studies is crucial before such interventions can be tested for their efficacy. To underscoreour point, in a systematic review of relevant randomized placebo-controlled clinical trials
of folate-based supplements in ischemic heart disease, we found no significant reductions inrates of mortality or cardiac events (Figure 4 ). The NORVIT study suggests that the harmfuleffects of these supplements could be due to vitamin B6. The individual and interactive effects of folic acid and vitamin B12 together with vitamin B6, should be assessed and clarified further,including their possible toxic metabolites and harmful interactions with other drugs. In this study,time-course analysis suggested that the harmful effects persisted during continued intake.Therefore, it is strongly recommended that studies on the safety of folic acid-based interventionsshould be undertaken prior to any further trials involving patients with coronary heart disease,including those involving other outcomes such as neuropsychiatric and cerebrovascular parameters.
Figure 4. Clinical outcomes from studies on coronary heart disease retrieved from Medline. There is no significanteffects of folate supplements on all-cause mortality and nonfatal myocardial infarction (MI). Stronger trends for theoccurrence of unstable angina and congestive heart failure (CHF) were observed in the treated patients. There was asignificantly reduced rate of stroke in folate-treated patients ( p = 0.03).
Moreover, subgroup analyses indicated that older subjects and those who were diabetic
were more susceptible to the adverse effects of the folate supplement. There is no clear
mechanism for these phenomena, but it is hypothesized that degenerative changes in the
physiology of these subsets might infer greater susceptibility to the toxicity of the vitamins or
their metabolites.
The study also showed that clinical outcomes of folic acid-based supplementation werebetter in patients with previous stroke, especially in terms of nonfatal acute coronary events.

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 11/13
Although this trial did not assess secondary stroke prevention, other clinical studies have showna significant reduction in the occurrence of stroke. Combined, these findings suggest that themechanism of cerebrovascular disease may not be similar to vasoocclusive disease in other parts of the body, such as the heart. Thus, folic acid supplementation might be selectivelybeneficial to cerebral pathologic lesions by mechanisms not necessarily pertinent toatherosclerosis, or even to the action of homocysteine. This issue could be addressed in
subsequent studies.
It was also observed that there were more non-serious adverse events in the folategroup, including skin irritation and rashes, as previously reported. Dyspnea was more commonin the folate group. Dizziness was noted in the folate group but not in the placebo group; neither are commonly cited side effects of folic acid, vitamin B6 or B12. Hence, it is speculated thatthese could be idiopathic reactions in Filipinos, or more possibly, overlooked side effects. Theseside effects should be considered in subsequent human studies.
It should be noted that the study had significant limitations. The sample size was notlarge enough to detect significant differences in specific clinical outcomes. The compliance rateof approximately 60% probably attenuated the effect of folate treatment. On the other hand,
such a compliance rate may actually reflect the real-life compliance rate that approximatesgenuine harm or benefit. The fact that this study was performed in a developing country such asthe Philippines should also be considered in view of the lack of mandatory folic acidsupplementation in food, and potential ethnical differences. Despite these limitations, it is notrecommended to repeat the study in a larger sample, due to the safety issues. Alternatively,animal or cellular models might be more appropriate. Research on the mechanism of homocysteine-induced injury is clearly needed to direct alternative and more specific therapy for homocysteinemia.
ACKNOWLEDGMENTS
This study was made possible through the funds of the Department of Science andTechnology-Grant-in-Aid of the Republic of the Philippines, under the supervision of thePhilippine Council for Health Research and Development.
We would like to thank the following for their kind support: Senator Ramon MagsaysayJr. for providing the research funds through his initiative; Dr. Felix Eduardo Punzalan for hisadvice, Ms. Marie Jeanne Berroya and Ms. Rosario Hapin for patiently supervising our progress;Pharmacare (Philippines) for supplying the supplements and placebo; Mark Anthony Javelosa,MSc, for the statistical consultation and the Department of Biochemistry and Molecular Biologyof the UP College of Medicine and the Department of Medicine of the UP-Philippine GeneralHospital for administrative support.
Footnotes 4Drs. Imasa and Nevado contributed equally to the study
REFERENCES
1. Ford ES, Smith SJ, Stroup DF, Steinberg KK, Mueller PW, Thacker SB. Homocyst(e)ineand cardiovascular disease: a systematic review of the evidence with special emphasison case-control studies and nested case-control studies. Int J Epidemiol 2002;31:59±70.

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 12/13
2. Homocysteine Studies Collaboration. Homocysteine and risk of ischemic heart diseaseand stroke: a meta-analysis. JAMA 2002;288:2015±22.
3. Chambers JC, Obeid OA, Kooner JS. Physiological increments in plasma homocysteineinduce vascular endothelial dysfunction in normal human subjects. Arterioscler ThrombVasc Biol 1999;19:2922±7.
4. Bellamy MF, McDowell IF, Ramsey MW, Brownlee M, Bones C, Newcombe RG, et al.Hyperhomocysteinemia after an oral methionine load acutely impairs endothelial functionin healthy adults. Circulation 1998;98:1848±52.
5. Lowering blood homocysteine with folic acid based supplements: meta-analysis of randomised trials. Homocysteine Lowering Trialists¶ Collaboration. BMJ 1998;316:894±8.
6. Neal B, MacMahon S, Ohkubo T, Tonkin A, Wilcken D; PACIFIC Study Group. Dose-dependent effects of folic acid on plasma homocysteine in a randomized trial conductedamong 723 individuals with coronary heart disease. Eur Heart J 2002;23:1509±15.
7. Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-loweringtherapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention: the Swiss Heart study: a randomized controlledtrial. JAMA 2002;288:973±9.
8. Lange H, Suryapranata H, De Luca G, Borner C, Dille J, Kallmayer K, et al. Folatetherapy and in-stent restenosis after coronary stenting. N Engl J Med 2004;350:2673±81.
9. Lonn E, Yusuf S, Arnold MJ, Sheridan P, Pogue J, Micks M, et al. Homocysteine
lowering with folic acid and B vitamins in vascular disease. N Engl J Med2006;354:1567±77.
10. Bønaa KH, Njølstad I, Ueland PM, Schirmer H, Tverdal A, Steigen T, et al.Homocysteine lowering and cardiovascular events after acute myocardial infarction. NEngl J Med 2006;354:1578±88.
11. Namazi MH, Motamedi MR, Safi M, Vakili H, Saadat H, Nazari N. Efficacy of folic acidtherapy for prevention of in-stent restenosis: a randomized clinical trial. Arch Iran Med2006;9:108±10.
12. Toole JF, Malinow MR, Chambless LE, Spence JD, Pettigrew LC, Howard VJ, et al.
Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke,myocardial infarction, and death: the Vitamin Intervention for Stroke Prevention (VISP)randomized controlled trial. JAMA 2004; 291:565±75.
13. Bazzano LA, Reynolds K, Holder KN, He J. Effect of folic acid supplementation on risk of cardiovascular diseases: a meta-analysis of randomized controlled trials. JAMA2006;296:2720±6.

8/3/2019 Folic Acid Article
http://slidepdf.com/reader/full/folic-acid-article 13/13
14. Boersma E, Pieper KS, Steyerberg EW, Wilcox RG, Chang WC, Lee KL, et al.Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. The PURSUITInvestigators. Circulation 2000;101:2557±67.
15. Tavares JR, D¶Almeida V, Diniz DC, Terzi CA, Cruz EN, Stefanini E, et al. Analysis of
plasma homocysteine levels in patients with unstable angina. Arq Bras Cardiol2002;79:16±72.
16. Vizzardi E, Nodari S, Fiorina C, Metra M, Dei Cas L. Plasma homocysteine levels andlate outcome in patients with unstable angina. Cardiology 2007;107:354±9.
17. Nygård O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, Vollset SE. Plasmahomocysteine levels and mortality in patients with coronary artery disease. N Engl J Med1997;337:230±6.
18. Januzzi Jr JL, Snapinn SM, DiBattiste PM, Jang IK, Theroux P. Benefits and safety of tirofiban among acute coronary syndrome patients with mild to moderate renalinsufficiency: results from the Platelet Receptor Inhibition in Ischemic SyndromeManagement in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) trial.Circulation 2002; 105:2361±6.
19. Title LM, Cummings PM, Giddens K, Genest Jr JJ, Nassar BA. Effect of folic acid andantioxidant vitamins on endothelial dysfunction in patients with coronary artery disease.J Am Coll Cardiol 2000;36:758±65.