foodborne infections - idealprogram.eu · salmonella sp. , yersinia sp. ... •sepsis and...
TRANSCRIPT

FOODBORNE INFECTIONS
Caroline Charlier-Woerther March 2017
LEARNING OBJECTIVES
Know the pathogens involved in diarrheas
Know the basics of management of diarrhea
Know the main patterns of listeriosis and how to diagnose them
Recognize and treat C. difficile
Recognize and treat amoebiasis
FOODBORNE INFECTIONS
• Pathogens
• Clinical patterns
• Complications
• Diagnosis
• Basics of treatment
• Listeriosis, C. diff and amoebiasis

• Infections of food origin
Diarrhea
+/- Other symptoms
• Meningitis, fetal loss
• Bacteremias , neurotransmission blockade
• Single individual/ collective infections
• Frequent : 1/6 US Citizen / year
FOODBORNE INFECTIONS

• Release of a toxin targeting the enterocyte
enhanced water and electrolytes secretion
watery diarrhea
Vibrio cholerae
Enterotoxinogenic E. coli
Staphylococcus aureus
FOODBORNE INFECTIONS PATHOPHYSIOLOGY

FOODBORNE INFECTIONS PATHOPHYSIOLOGY
• Destruction of the enterocytes
Dysentery : pus/ blood/ mucoid diarrhea/ fever/cramps
Shigella sp. , Entamoeba histolytica
• Dissemination beyond the digestive tract
Enterocytes macrophages mesenteric lymph node beyond
Fever, bacteremia
Salmonella sp. , Yersinia sp.
All = entero-invasive mechanism

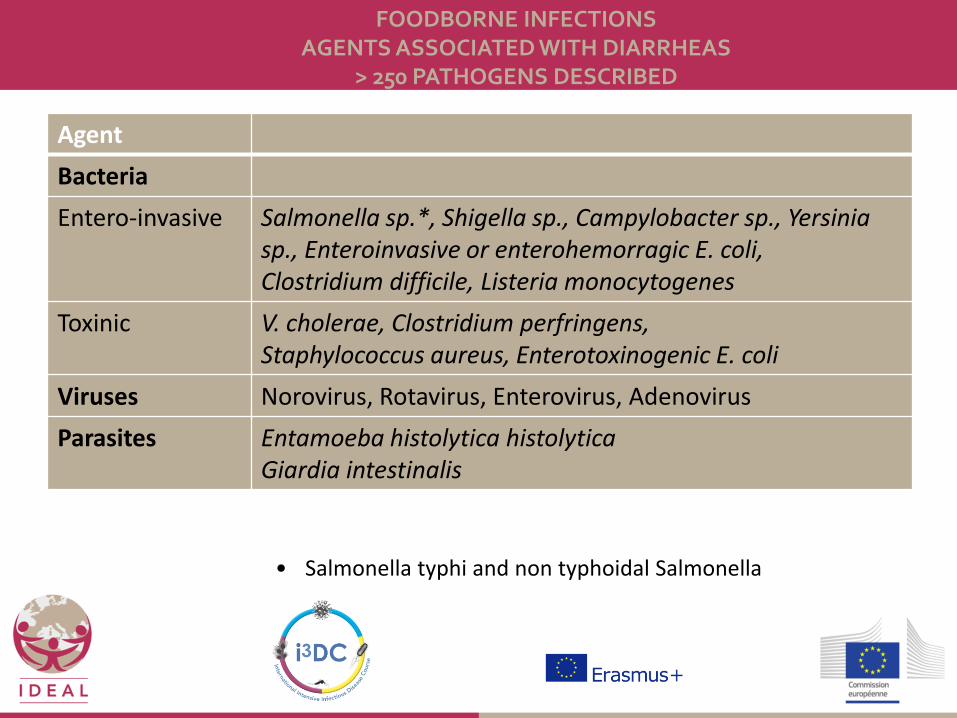
FOODBORNE INFECTIONS AGENTS ASSOCIATED WITH DIARRHEAS
> 250 PATHOGENS DESCRIBED
Agent
Bacteria
Entero-invasive
Salmonella sp.*, Shigella sp., Campylobacter sp., Yersinia sp., Enteroinvasive or enterohemorragic E. coli, Clostridium difficile, Listeria monocytogenes
Toxinic V. cholerae, Clostridium perfringens, Staphylococcus aureus, Enterotoxinogenic E. coli
Viruses Norovirus, Rotavirus, Enterovirus, Adenovirus
Parasites Entamoeba histolytica histolytica Giardia intestinalis
• Salmonella typhi and non typhoidal Salmonella

MOST FREQUENT AGENTS Agent
Bacteria
Entero-invasive
Salmonella sp.*, Shigella sp., Campylobacter sp., Yersinia sp., Enteroinvasive or enterohemorragic E. coli, Clostridium difficile, Listeria monocytogenes
Toxinic V. cholerae, Clostridium perfringens, Staphylococcus aureus, Enterotoxinogenic E. coli
Viruses Norovirus, Rotavirus, Enterovirus, Adenovirus
Parasites Entamoeba histolytica histolytica Giardia intestinalis
USA CDC data Norovirus 5,400,000 cases / year Non typhoidal salmonella 1,000,000 cases / year Clostridium perfringens 950,000 cases / year Campylobacter 850,000 cases / year S. aureus 250,000 cases / year
http://www.cdc.gov/foodborneburden/2011-foodborne-estimates.html

Bacteria
Entero-invasive
Salmonella sp.*, Shigella sp., Campylobacter sp., Yersinia sp., Enteroinvasive or enterohemorragic E. coli, Clostridium difficile, Listeria monocytogenes
Toxinic V. cholerae, Clostridium perfringens, Staphylococcus aureus, Enterotoxinogenic E. coli
Viruses Norovirus, Rotavirus, Enterovirus, Adenovirus
Parasites Entamoeba histolytica histolytica Giardia intestinalis
USA CDC data : Annual deaths Listeriosis : 255 deaths among 650 reported cases > 35% mortality Salmonella : 378 deaths among 1,000,000 cases Norovirus : 150 deaths among 5,000,000 cases
http://www.cdc.gov/foodborneburden/2011-foodborne-estimates.html
MOST SEVERE AGENTS

• Dehydration
• Sepsis and bacteremia
• Occlusion in severe colitis
• Febrile diarrhea in a traveller returning from malaria area always think of malaria
MANAGEMENT
1. Identify emergencies
• Confirm diarrhea ( > stools /day)
• Exclude non infectious diarrhea
• Identify diarrhea associated with non enteric infectious diseases : malaria/ leptospirosis/ pyelonephritis/legionellosis
2. Diagnosis
MANAGEMENT

• Collect clinical data
3 patterns associated with distinct pathogens
– Dysentery : blood, pus, mucoid diarrhea (fever)
– Watery “cholera-like” : diarrhea, usually no fever
– Gastroenteritis-like : diarrhea, vomiting, (fever) : no orientation
2. Diagnosis
MANAGEMENT

• Collect clinical data
3 patterns associated with distinct pathogens
Acute / chronic infection?
Collective infection?
Type of food consumed/ recent antibiotic uptake?
Recent travel in a tropical area?
Background? (pregnancy? IC?)
2. Diagnosis
MANAGEMENT

• Biological tests – 1. stool culture
• If any complication/ dysentery/ collective infection / return from tropical area/ ID patients
– 2. stool test for C. difficile toxin • If recent antibiotic exposure
– 3. virological test in the stool (ELISA) • If complication / ID
– 4. stool samples for parasites • If return from tropical area / ID patients
– 5. blood cultures if fever – 6. (rectosigmoido-/ colonoscopy in case of proctitis / colitis)
2. Diagnosis
MANAGEMENT

• Rehydratation
• Antibiotics in invasive diarrheas
– Fluoroquinolones
– Azithromycine
• Avoid anti-peristaltic drugs like loperamide
3. Principles of treatment
MANAGEMENT

• Wash hands
• Cook food/ peel food
• Water : filtered or boiled or encapsulated
3. Principles of prevention
MANAGEMENT

FOODBORNE INFECTIONS AGENTS ASSOCIATED WITH DIARRHEAS
> 250 PATHOGENS DESCRIBED
Agent
Bacteria
Entero-invasive
Salmonella sp.*, Shigella sp., Campylobacter sp., Yersinia sp., Enteroinvasive or enterohemorragic E. coli, Clostridium difficile, Listeria monocytogenes
Toxinic V. cholerae, Clostridium perfringens, Staphylococcus aureus, Enterotoxinogenic E. coli
Viruses Norovirus, Rotavirus, Enterovirus, Adenovirus
Parasites Entamoeba histolytica histolytica Giardia intestinalis
• Salmonella typhi and non typhoidal Salmonella

CLOSTRIDIUM DIFFICILE
• Asymptomatic carriage of non-toxinogenic
C. difficile : 3% adult population
• Toxinogenic C. difficile
– Antibiotic exposure
– Acquisition of C. difficile
– Secretion of CD toxins
Watery diarrhea / low fever
Pseudomembranous diarrhea

• Watery diarrhea
• Pseudomembranous colitis – Fever, abdominal cramps
– High leukocytes count
– Bloody / mucoid diarrhea
Diagnosis
toxin in the stool in both
membranes on the colic mucosal lining
CLOSTRIDIUM DIFFICILE

• 4 types of complications – Dehydration
– Septic shock
– Colic perforation +++
– Recurrence in 20% of cases
• Treatment – Stop antibiotics if possible
– Metronidazole/ vancomycine PO/ fidaxomycin
CLOSTRIDIUM DIFFICILE

OTHER INVASIVE ENTERIC BACTERIA
• Non typhoidal Salmonella
– Eggs / meats
– Incubation : 36h
– Diarrhea / vomiting / high fever (no blood)
• Campylobacter jejuni
– Poultry
– Incubation 1-3 days
– Bloody stool / cramps / fever

• Yersinia enterocolitica
– Incubation 4-6 days
– Milk/ meat (pork)
– Fever ++ / bloody stool / cramps
– Children may be confused with appendicitis
– 2% reactive arthritis
– Erythema nodosum
OTHER INVASIVE ENTERIC BACTERIA

• Gram positive rod
• Able to multiply at 4°C
• Not killed by freezing
• Hemolysis
• Zoonosis
• Human infections rare but severe
LISTERIOSIS

• 1. Gastro-enteritis – Febrile diarrhea
– Immunocompetent patients
– Incubation 20H
• 2. Septicemia – Mostly immunocompromised (cellular immune defects, alcohol,
corticosteroids, older patients) : 40% mortality
• 3. Neurological infection meningoencephalitis : 30% mortality
• 4. Infection in pregnancy
LISTERIOSIS
CharlierLID 2017

• 4. Infection in pregnancy
• Mother mild disease
– Fever + obstetrical signs > fever alone
• Fetus : not teratogenic but 20% fetal loss, 40% prematurity, 20% abnormal delivery at term
– Placentitis
– Only 5% of pregnancies go on uneventful
LISTERIOSIS
Charlier LID 2017

• 4. Infection in pregnancy
• Diagnosis
– Maternal blood cultures
– Placenta cultures
– Any fetal/ neonatal cultures
• Treatment
– Amoxicillin++ cephalosporins ineffective+++
– Pre-emptive treatment of any unexplained maternal fever
LISTERIOSIS

LISTERIOSIS PREVENTION
• Avoid raw milk
• Avoid soft cheese
• Avoid meat spreads and patés
• Recook ready to eat food until steaming hot
• Wash the refrigerator
• Wash the hands
ENTEROTOXINOGENIC E. COLI
• Leading cause of bacterial diarrhea in tropical areas, leading cause of diarrhea in the returning traveller
• 300,000,000 cases / year
• Watery diarrhea/ vomiting / abdominal cramps
mild or no fever
• Healing in 2-4 days
• Diagnosis based on PCR detection of the toxins
(not routinely done)
es.dreamstime.com

SHIGA TOXIN-PRODUCING ESCHERICHIA COLI
• Various serogroups involved
– O157:H7, O104:H4, O121 etc.
• All produce a toxin similar to the toxin produced by Shigella dysenteriae
• Bloody stool
• Increased risk of hemolytic and uremic syndrom
• Diagnosis : PCR in the stool

STAPHYLOCOCCUS AUREUS
• Short incubation < 4hours
• Heat-stable enterotoxin
• S. aureus transmitted by an asymptomatic carrier or a skin lesion
• Manipulated food
• Vomiting / diarrhea no fever

• Short incubation 6-24 hours
• Abdominal cramps and diarrhea, no vomiting
• Contaminated meat / sauce ++
• Poor storage conditions
• Collective food
CLOSTRIDIUM PERFRINGENS
• Anaerobic gram positive rod
• Nerve toxin
• 3 forms
– Home-canned food foodborne
– Ingestion of spores infant botulism
– Infection of a wound wound botulism
CLOSTRIDIUM BOTULICUM
• Blockade of neurotransmission
• Symptoms
– Double vision, blurred vision, drooping eyelids, slurred speech, difficult swallowing, dry mouth, muscle weakness
– If untreated, progression to paralysis of the respiratory muscles, arms, legs, and trunk.
– Incubated 1-2 days
• Diagnosis : clinical features (toxin in reference centers)
• Treatment : supportive (recuperation within wks/mths)
CLOSTRIDIUM BOTULICUM

• Vibrio cholerae : gram negative bacillus
• Endemic/ epidemic in tropical areas
– India/ Central America/ Africa
– 3-5,000,000 cases / year 150,000 deaths
– Not travellers
– Reservoir = people and aquatic sources like brackish waters and estuaries (global warming!!)
CHOLERA

• Short incubation < 1d
• Clinical presentation – Nothing : 75%
– Among symptomatic cases
• Mild diarrhea = 80%
• Profuse watery diarrhea (10l/d), no fever = 20%
so only <4% of global cases
• Diagnosis : stool examination and culture
• Vaccination confers partial protection
• Antibiotic treatment (cyclines) and rehydratation
CHOLERA
FOODBORNE INFECTIONS AGENTS ASSOCIATED WITH DIARRHEAS
> 250 PATHOGENS DESCRIBED
Agent
Bacteria
Entero-invasive
Salmonella sp.*, Shigella sp., Campylobacter sp., Yersinia sp., Enteroinvasive or enterohemorragic E. coli, Clostridium difficile, Listeria monocytogenes
Toxinic V. cholerae, Clostridium perfringens, Staphylococcus aureus, Enterotoxinogenic E. coli
Viruses Norovirus, Rotavirus, Enterovirus, Adenovirus
Parasites Entamoeba histolytica histolytica Giardia intestinalis
• Salmonella typhi and non typhoidal Salmonella

VIRAL DIARRHEA IMMUNOCOMPETENT
• Children ROTAVIRUS – Spring / summer
– High risk of dehydration if < 2 years
– Vaccine available in France
• Adults NOROVIRUS
• Viral identification possible in the stool
(not routinely performed)
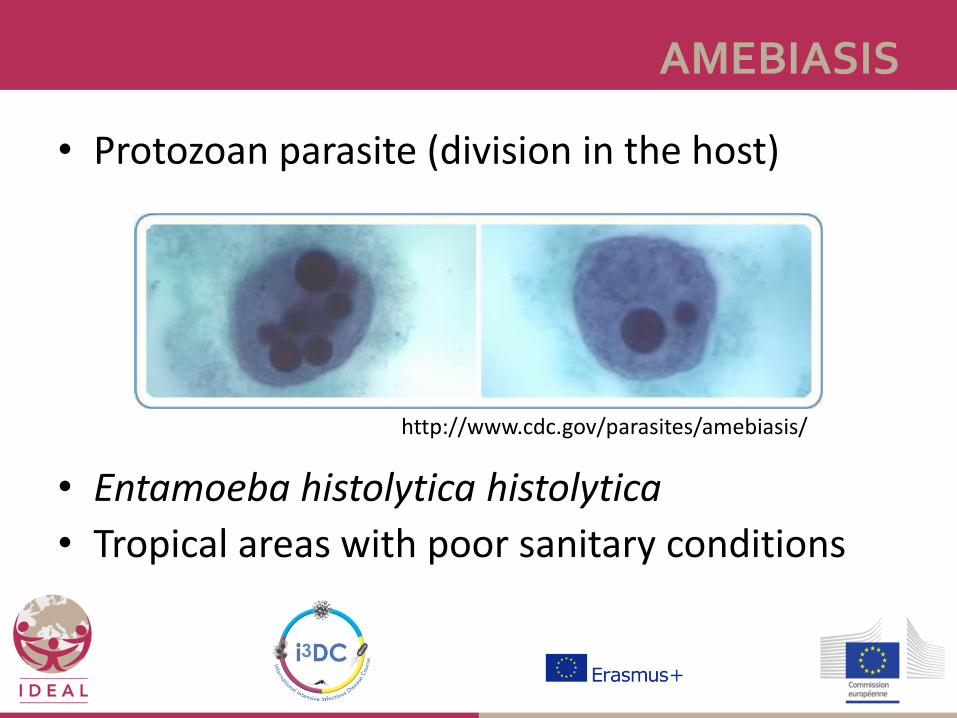
AMEBIASIS
• Protozoan parasite (division in the host)
• Entamoeba histolytica histolytica
• Tropical areas with poor sanitary conditions
http://www.cdc.gov/parasites/amebiasis/
• Orofecal infection : cysts eliminated in the stool ingested trophozoites that invade the mucosal lining
• Human reservoir
• Clinical presentation
– Asymptomatic : 80%
– Loosy stool and abdominal cramps
– +++ Bloody stools and abdominal cramps, no fever colitis
AMEBIASIS

• Extradigestive infection
– Liver+++
– FEVER, enlarged and tender liver
– Unique 2/3 > multiple abcesses
– 80% right lobe
rad-log. blogspot.com -
AMEBIASIS

• Diagnosis
• Colitis : stool samples
– The pathogenic Entamoeba histolytica is characterized by ingested erythrocytes in the trophozoite
AMEBIASIS

• Diagnosis
• Stool samples for colitis
• Serology for liver disease
– False negative < 7 days of fever
– No parasites in the pus/ stool
AMEBIASIS

• Metronidazole 7d (colitis) 10-14d (liver)
against trophozoites
• Tilbroquinol/tiliquinol
against cysts
• Don’t repeat the serology
• Abcesses require 2months -1 year to resolve
AMEBIASIS TREATMENT
• Stomach cramps
• Abdominal cramps
• Diarrhea
• Asymptomatic
• Examination of the stool for parasites
• Treatment : metronidazole or albendazole
GIARDIASIS

• Wikimedia Commons
• CDC
Sources