foreign bodies: is removal necessary? william j. byrne … · by william j. byrne, m.d., faap, and...
TRANSCRIPT

DOI: 10.1542/aapnews.20082911-212008;29;21AAP News
William J. Byrne and Arthur R. EulerForeign bodies: Is removal necessary?
http://aapnews.aappublications.org/content/29/11/21the World Wide Web at:
The online version of this article, along with updated information and services, is located on
Copyright © 2008 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.been published continuously since 1948. AAP News is owned, published, and trademarked by the AAP News is the official journal of the American Academy of Pediatrics. A monthly publication, it has
at UNIV OF CHICAGO on May 9, 2013http://aapnews.aappublications.org/Downloaded from
©Copyright 2008 AAP News
Volume 29 • Number 11November 2008www.aapnews.org
FOCUS ON SUBSPECIALTIES
by William J. Byrne, M.D., FAAP, and Arthur R. Euler, M.D., FAAP
Kids like to swallowthings, and almost anyobject fills the bill. Fortoddlers, it is part ofexploring the environ-ment; for older childrenand adolescents, it usu-ally is by accident, on adare, or as part of a neu-
rodevelopmental or psychiatric disorder.Fortunately, most foreign bodies are harm-less and pass through the gastrointestinal(GI) tract without problems.
Following are guide-lines for pediatriciansregarding whom to referpa tients to, when to referand what to do in theinterim. These are just “guidelines” as exceptionsbased on case reports and anecdotal experiencecan always be found.
Who removes the foreign body will be institu-tion specific, but start with a pediatric gastroenterologist. In somecases, esophageal foreign bodies are removed by pediatric surgeonsor otolaryngologists.
Desiccant packages are the single most frequently reported foreignbody ingestion, according to the American Association of PoisonControl Centers. Toxicity is negligible, and referral for removal isnot necessary.
Esophageal foreign bodiesForeign bodies lodged in the esophagus require urgent referral
for removal. On an anteroposterior film, the flat portion of a coin will be seen
if the coin is in the esophagus, in deference to the edge if it is inthe trachea. For sharp edged objects, especially those that are radi-olucent such as bones or toothpicks, computerized tomographymay help document the presence of the object. Fish bones maystick in the hypopharynx or proximal esophagus, and care shouldbe taken that these areas are visualized on imaging studies.
Soluble contrast radiography also may be used, but barium contrast
studies should be avoided. Even ifthe foreign body cannot be visual-ized, a history of ingestion withsymptoms of pharyngeal or chestpain and/or drooling warrants refer-ral for endoscopy.
Disc button batteries lodged inthe esophagus require urgent refer-ral to prevent damage to themucosa. Although coins are con-sidered benign, they should not beallowed to remain in the esophagusfor more than 24 hours. Patientsshould be kept NPO. Sedation orintravenous glucagon may resultin relaxation of the esophagus andpassage of the foreign body intothe stomach.
Gastric foreign bodiesCoins and other similar rounded
radio opaque objects the diameter of a nickel or smaller should passfrom the stomach. The rule of thumb is that if it passes the pylorus,it will pass the anus. Quarters and objects of similar size or largerare not likely to pass. A film should be taken three weeks after theingestion or sooner if the patient develops abdominal pain, nauseaor vomiting. If the coin is still within the stomach, the patientshould be referred for removal.
Button disc batteries in the stomach are the exception. A filmshould be taken 72 hours after the ingestion. If the battery still isin the stomach, the patient should be referred for removal at thattime.
Surprisingly, nails, pins, paper clips and other sharp objects lessthan 1½ inches long usually pass from the stomach and all the waythrough the GI tract without any problems. Their continued presencein the stomach after 72 hours warrants referral for removal. Thesame is true for cylindrical batteries.
Sharp objects that have moved beyond the pylorus should be fol-lowed with serial radiographs every two or three days until theyhave passed the anus. If during this time the patient develops ab -dominal pain, fever or vomiting, or on the abdominal films theobject fails to move, the patient should be referred to a centerurgently.
Foreign bodies: Is removal necessary?
Dr. Byrne
Dr. Euler
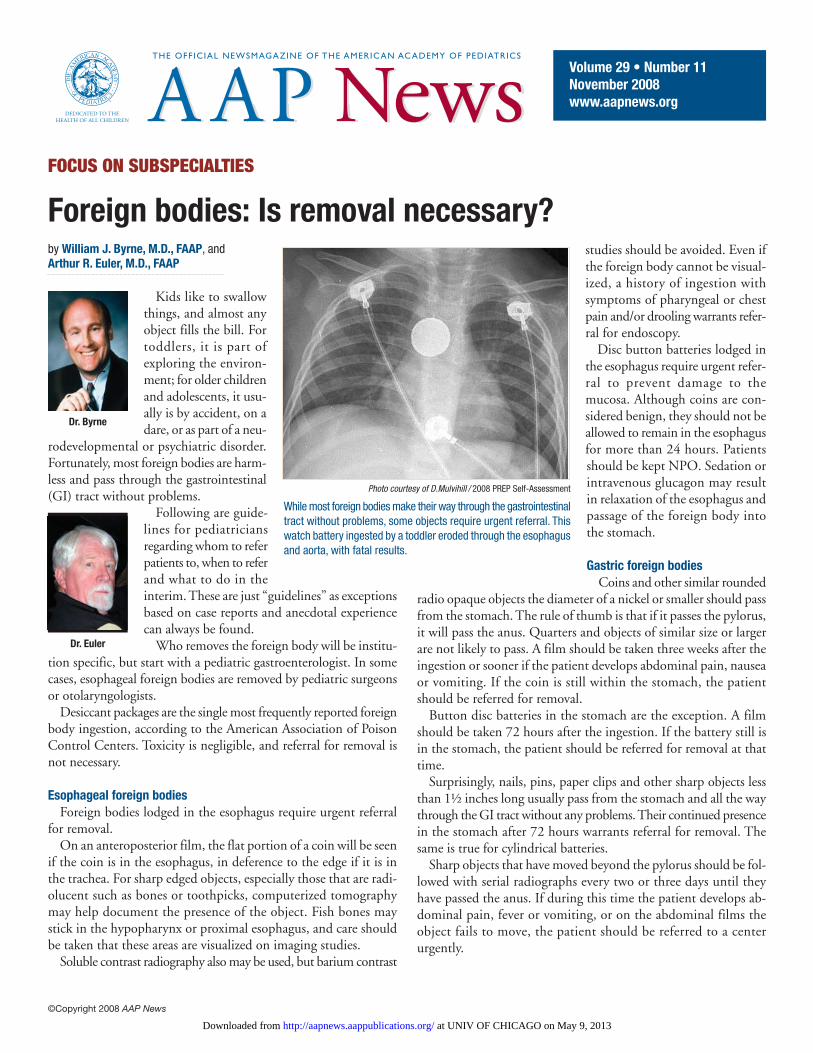
Photo courtesy of D.Mulvihill / 2008 PREP Self-Assessment
While most foreign bodies make their way through the gastrointestinaltract without problems, some objects require urgent referral. Thiswatch battery ingested by a toddler eroded through the esophagusand aorta, with fatal results.
at UNIV OF CHICAGO on May 9, 2013http://aapnews.aappublications.org/Downloaded from

©Copyright 2008 AAP News
Patients who have ingested sharp objects longer than 1½ inches,including hat pins, pens and pencils as well as open safety pins,should be referred im mediately for urgent removal of the object.
Magnets present an interesting challenge. If the child has swallowedtwo or more, referral for urgent removal is warranted regardless ofthe size. In the small intestine, the magnets may stick togethercausing ischemic necrosis between the interposed loops of bowel.
Children with foreign bodies in the stomach or in the intestineshould be kept on a regular diet. The use of prokinetic agents and/or
laxatives has been advocated by some, but no controlled studiessupport their use.
The best treatment for foreign body ingestion is prevention. Atall well-child visits, parents should be reminded to keep small objectsout of the reach of young children.
Drs. Byrne and Euler are members of the AAP Section on Gastroen-terology and Nutrition executive committee.
at UNIV OF CHICAGO on May 9, 2013http://aapnews.aappublications.org/Downloaded from

DOI: 10.1542/aapnews.20082911-212008;29;21AAP News
William J. Byrne and Arthur R. EulerForeign bodies: Is removal necessary?
ServicesUpdated Information &
http://aapnews.aappublications.org/content/29/11/21including high resolution figures, can be found at:
Subspecialty Collections
http://aapnews.aappublications.org/cgi/collection/focusFocus on Subspecialtiesfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
/site/misc/Permissions.xhtmlits entirety can be found online at: Information about reproducing this article in parts (figures, tables) or in
Reprints/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at UNIV OF CHICAGO on May 9, 2013http://aapnews.aappublications.org/Downloaded from