fournier's gangrene
TRANSCRIPT
Fournier’s Gangrene: A Urologic Emergency
You Don’t Want to Miss!Angela Lou Reu, B.A., M.S., PA-C
Emergency Care Consultants

Chief Complaint: Flu-like Symptoms
HPI: The patient is a 43 y/o male with h/o DM, HTN, HLD, and obesity who presents to the ED with flu-like symptoms. He c/o feeling feverish with chills, diaphoresis, nausea and generalized body aches x 4-5 days. He reports decreased appetite and has not been taking his home meds for the past few days d/t not feeling well. Sugars have been “high”. No temp taken at home. He denies headache, neck pain or stiffness, cough or URI symptoms, sore throat, runny nose, sinus congestion, earache, chest pain, SOB, abdominal pain, vomiting, diarrhea, constipation, urinary symptoms, rashes, recent illness or ill contacts and has no other complaints or concerns at this time.
History cont.
PMH: DM, HTN, HLD, obesity
PSH: None
Home Meds: ASA, Metformin, Lantus, Lipitor, Losartan
Allergies: NKDA
SH: Lives at home with wife. Former smoker. Daily drinker (reports 4 beers daily).
FH: Noncontributory

ROS – pertinent positives and negatives
General: feverish with chills, diaphoresis, decreased appetite
HEENT: no headache, sore throat, runny nose, sinus congestion, earache
CV: no chest pain
Pulm: no cough, sputum, or SOB
GI: nausea without vomiting, no diarrhea or constipation
GU: denies urinary complaints
MS: myalgias, denies neck pain/stiffness
Skin: denies rash

Physical Exam
Vitals: T 102.2 HR 114 BP 104/87 RR 22 Sats 98% on RA
General: lethargic, appears ill, diaphoretic, uncomfortable, mild distress
HEENT: NC/AT, PERRLA, conjunctiva clear, sclera white, EOMI, EACs clear, TMs noninjected with good light reflex, dry mucous membranes, no oropharyngeal edema, erythema, or exudate, uvula midline
Neck: soft, supple, no LAD, no meningeal signs
CV: regular rhythm, tachycardic, no m/r/g

Physical Exam cont.
Pulm: Tachypneic, Lungs CTAB, no wheezing or rales
Abdomen: obese, soft, nondistended, nontender, normal bowel sounds
MS: Extremities warm, well perfused, no cyanosis, clubbing, edema, SILT, MAE
Neuro: lethargic, oriented x 3, CN II-XII grossly intact
Skin: good color, warm to touch, diaphoresis noted
Differential Diagnosis
F/C, diaphoresis, decreased appetite, nausea, myalgias
Influenza or viral illness
Otitis media/externa
Sinusitis
Bacterial or viral pharyngitis
Pneumonia
Gastroenteritis
UTI/pyelonephritis
* Wait! After family leaves the room, the nurse tells you that the patient has something he wants to show you. *
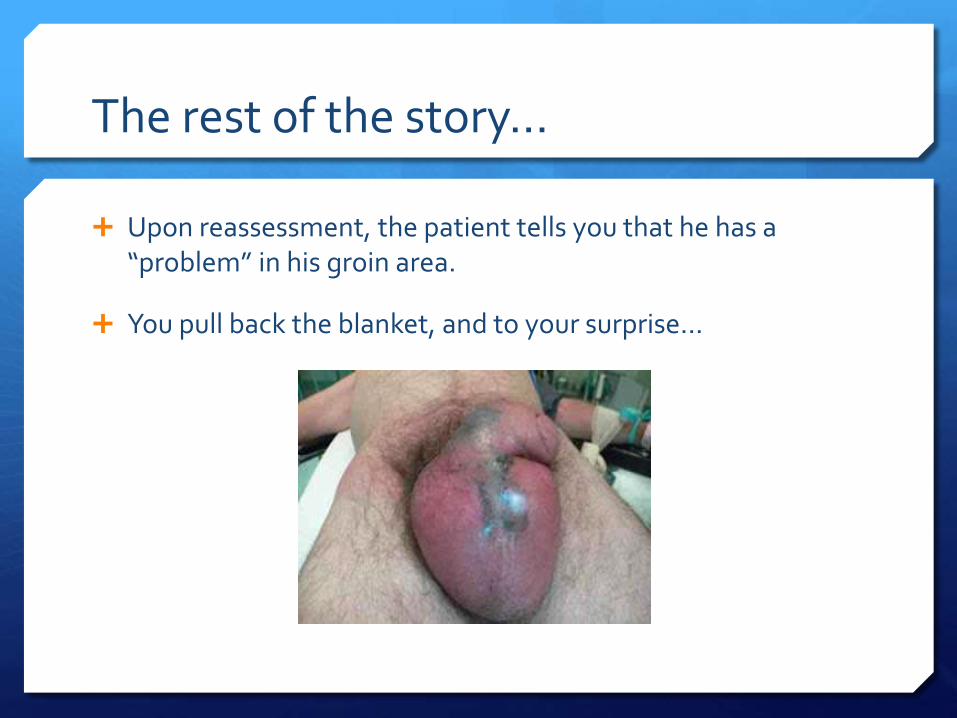
The rest of the story…
Upon reassessment, the patient tells you that he has a “problem” in his groin area.
You pull back the blanket, and to your surprise...

GU Exam
Erythematous, edematous scrotum with warmth and exquisite tenderness on palpation. Malodor noted. Necrotic tissue, midline scrotum and dorsal penile shaft. No open lesions or active drainage. Erythema extending onto abdominal wall, perineum and bilateral proximal thighs with bogginess and crepitus.

Reconsider the Differential
Scrotal pain and swelling
Cellulitis
Gonococcal balanitis
Epididymitis or orchitis
Strangulated hernia
Scrotal abscess
Testicular torsion
Hydrocele or Varicocele
Vascular occlusion syndromes
Polyarteritis nodosa
Warfarin necrosis

Don’t Miss the Obvious!!!
Fever, lethargy, severe scrotal pain and swelling with erythema, crepitus +/- necrotic tissue should raise suspicion of necrotizing fasciitis of the genitalia, or…
Fournier’s Gangrene! Failure to examine the genitals, especially in diabetics or
immunocompromised patients, can result in misdiagnosis and delay in treatment!!!

Labs – Sepsis Workup
CMP: Na 133, K 4.1, Glucose 417, Cr 1.5, bicarb 26
CBC: WBC 15.5, Hgb 12.2, HCT 37.2 PLT 255
UA/UC: pending
INR: 1.2
Lactate: 1.6
Blood cultures x 2: pending
Imaging
Do not delay early surgical debridement for imaging studies. Delay will result in a negative impact on prognosis! 24-hour delay increases mortality rate by 11.5%, 6-day delay by
76%.

Fournier's Gangrene
First described in 1764 by Baurienne. Named after French venereologist, Alfred Jean Fournier, in 1883.
Aggressive, rapidly spreading infection of soft tissue, or necrotizing fasciitis, that affects the genitalia, perineal, and/or perianal regions.
Ten times more common in men, but can affect women and even children.
Rare, but life threatening!
High mortality rate (20-30%, some reports as high as 50%), despite advanced management.
Epidemiology and Etiology
Etiology
Perineal and genital skin infections (scrotal or anorectal abscess)
Urethral stricture
Anorectal, urogenital and perineal trauma (including genital piercing and intracavernosal cocaine injection)
Iatrogenic (indwelling catheter, traumatic catheterization, prostatic or rectal biopsy, anal dilatation, hemorrhoidectomy, vasectomy, penile implant, hydrocele aspiration)
Nidus typically from GI tract (30-50%), GU tract (20-40%), and cutaneous injuries (20%).
Associated Comorbidities:
DM (20-70%), alcoholism (25-50%), immunosuppression (including malnutrition, SLE, Crohn’s, chronic corticosteroid use, chemotherapy, HIV, liver disease, IVDA, and, less likely, bone marrow malignancy)
Onset to presentation, on average, 5 days.

Microbiology
Polymicrobial infections by aerobes and anaerobes: Enterobacter, esp. E coli
Klebsiella
Bacteroides
Streptococci
Staphylocci
Clostridia
Pseudomonas
Most are normal flora in the perineum and genitalia, most common E coli.
On average, at least 3 organisms cultured from each patient.

Pathophysiology
Microvascular thrombosis leading to cutaneous and subcutaneous necrosis, facilitating bacterial proliferation along fascial planes
Virulence in synergy promotes rapid spread and extensive tissue damage
Impaired host cellular immunity = favorable environment to permit infection
Portal of entry of microorganism into perineum/genitalia
Clinical Presentation
Most common presenting complaints: Fever, lethargy – first sign
Intense scrotal pain and tenderness with edema - hallmark
Cellulitis
Fetid odor
Crepitus/Fluctuance (gas producing organisms)
As inflammation worsens, necrotic tissue appears. Fascial necrosis is usually more extensive than visible gangrene suggests.
Infection can spread up the entire anterior abdominal wall, up to the clavicle.
Rapid progression to multi-organ failure secondary to Gm – sepsis, the most common cause of death.
Diagnosis
Primarily clinical (HIGH clinical index of suspicion)
Labs (CBC, CMP, Coag studies, Lactate, Blood cultures, Wound cultures – intraoperative)
Surgical consult
Imaging ???
Early surgical exploration and debridement of all necrotic tissue – definitive diagnosis
Clinical predictive values (LRINEC or FGSI)

Imaging
May be useful in atypical presentation or questionable true extent of disease.
Plain radiographs
May show air in tissue.
Ultrasonography
Differentiate intrascrotal abnormality; shows thickened, swollen scrotal wall containing gas.
CT and MRI
Diagnose or rule out retroperitoneal or intra-abdominal process.
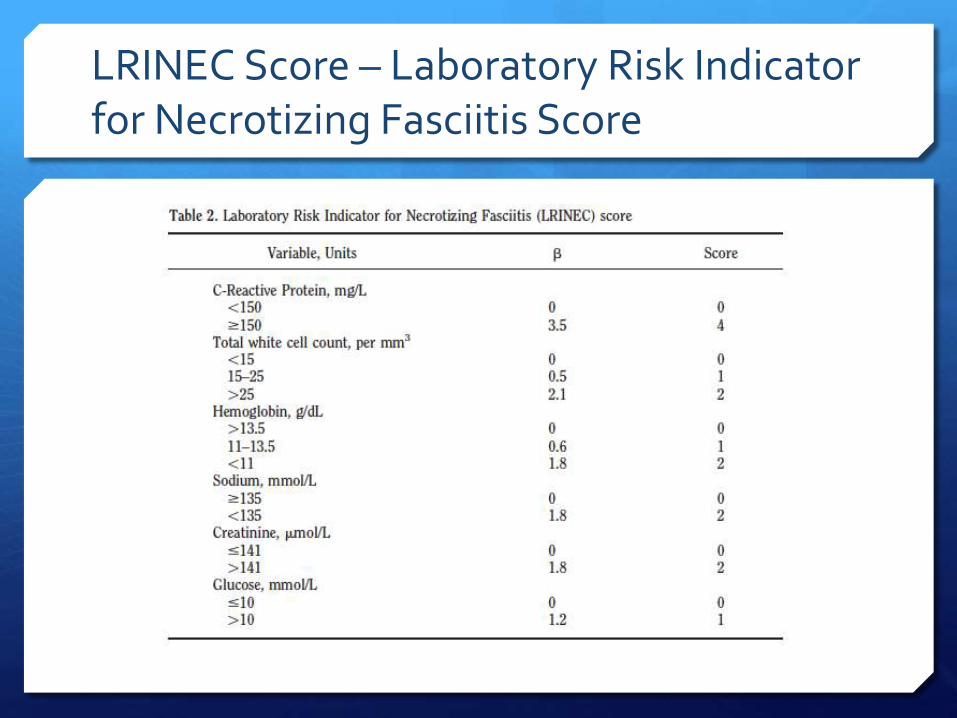
LRINEC Score – Laboratory Risk Indicator for Necrotizing Fasciitis Score

Fournier’s Gangrene Severity Index (FGSI)

Clinical Predictive Scores
LRINEC can be used to risk stratify patients with cellulitis to determine the likelihood of necrotizing fasciitis being present.
A LRINEC score ≥ 6 should raise suspicion of necrotizing fasciitis among patients with severe soft tissue infections.
A LRINEC score ≥ 8 is strongly predictive of this disease.
FGSI is useful to help predict outcome.
A FGSI score > 9 is associated with a 75% death rate.
A FGSI score of < 9 is associated with 78% survival.
One study quoted, a FGSI score of > 10.5 is associated with 96% death and a score of < 10.5 is associated with 96% survival.

Treatment
Aggressive multimodal approach.
Hemodynamic stabilization – aggressive fluid resuscitation.
Broad spectrum triple antibiotics – cover Gm +, Gm – and Anaerobes (Zosyn and Vanco , PLUS Clindamycin for anti-toxin effects against toxin-elaborating strains of strep and staph). Narrowed based on culture and sensitivities.
Early surgical debridement - primary component of treatment (Average 3.5 procedures per patient).
Treatment cont.
Hyperbaric Oxygen – believed to be effective adjunct, though no conclusive evidence regarding effectiveness.
Neutralizes anaerobes, improves neutrophil function, increased fibroblast proliferation, promotes angiogenesis.
Honey ??? – natural antimicrobial, digests necrotic tissue, accelerates healing by stimulating growth and multiplication of epithelial cells.
Wound VAC – minimizes contamination and skin defects, as well as speeds tissue healing.
Plastics Reconstruction – split-thickness graft to repair perineal and scrotal defects.

Fournier’s Gangrene: Report of Thirty-Three Cases and a Review of the Literature
Group 1
21 patients, mean age 57
Broad spectrum antibiotics
Broad debridement (avg 3)
Exhaustive cleaning
Split-thickness skin grafts or delayed closure
Group 2
12 patients, mean age 48
Broad spectrum antibiotics
One debridement per patient
Unprocessed honey daily
Own new scrotal skin (4 patients) or secondary suturing (8 patients)
Results
Group 1
Older, multiple comorbidites, more extensive disease
Longer hospitalization (4.5 weeks)
Three patients died – severe sepsis
Worse clinical and cosmetic results
Group 2
Younger, healthier, more localized disease
Shorter hospitalization (4 weeks)
No deaths
Better clinical and cosmetic results

Back to the Case
Started on Zosyn/Vanc/Clindamycin
2L IVF resuscitation
NPO
To OR for emergent debridement
LRINEC score 7 (intermediate risk for necrotizing fasciitis)
FGIS score 8 (>78% chance of survival)

After Debridement

Plastics Reconstruction
Summary
Fournier's Gangrene is BAD. Mortality rates remain high, despite aggressive management. Long term complications for those who survive (pain, sexual dysfunction, infertility, extensive scarring).
HIGH clinical index of suspicion, especially in diabetics, alcoholics, and patient’s with immunosuppression.
Low threshold for Surgical consult and early operative intervention.
Broad spectrum antibiotics.
+/- Hyperbaric oxygen therapy.
Honey – reduce cost, morbidity and mortality ???
Clinical predictive scores useful to help predict outcome.

Questions ???

References
Burch DM, Barreiro TJ, Vanek VW. Fournier’s gangrene: Be alert for this medical emergency. JAAPA Nov 2007; 20(11):44-47.
Kessler CS, Baum J. Non-Traumatic Urologic Emergencies in Men: A Clinical Review. West J Emerg Med. Nov 2009; 10(4): 281-287.
Mallikarjuna, MN. Vijayakumar, A, Patil, VS, et al. Fournier’s Gangrene: Current Practices. ISRN Surgery, Vol. 2012, Article ID 942437, 8 pages, 2012.
Pastore, et al. A multistep approach to manage Fournier’s gangrene in a patient with unknown type II diabetes: surgery, hyperbaric oxygen, and vacuum-assisted closure therapy: a case report. Journal of Medical Case Reports 2013, 7:1.
References cont.
Rahmaz L, Erdemir R, Kibar Y, et al. Fournier’s gangrene: Report of thirty-three cases and a review of the literature. International Journal of Urology, 12: 960-967.
Stevens, DL, Baddour, LM. (2014). Necrotizing soft tissue infections. In: UpToDate, Sexton DJ, Edwards MS, (Ed), UpToDate, Waltham, MA, 2014.
Thwaini A, Khan A, Malik A, et al. Fournier’s gangrene and it’s emergency management. Postgrad Med J. Aug 2006; 82(970):516-519.