free vascularized fibula flap - alpha hand...
TRANSCRIPT

FREE VASCULARIZED FIBULA FLAP

HYSTORICAL OVERVIEW - David JB, Taylor AN: muscle pedicle bone grafts: experimental study. Arch Surg 1952
- Degen IL: Modeling and transfer of composite bone autograft in a tubed flap-an experiment. Acta Chir Plast 1970
- Strauch B, Bloomberg AE, Lewin LM:an experimental approach in mandibular replacement:island vascular composite rib grafts. Br J Pl Surg 1971
- Medgyesi S: Observations in pedicle bone grafts in goats. Scand J Plast Surg 1972
- Ostrup LT, Fredrickson JM: distant transfer of a free living bone graft by microvascular anastomoses. PRS 1974

HYSTORICAL OVERVIEW
- Taylor I: The free vascularized bone graft. Plast Reconstr Surg 1975
- Wei, F.C., Chen, H.C., Chuang, C.C., and Noordhoff, M.S. Fibular Osteoseptocutaneous Flap: Anatomic Study and Clinical Application. Plast. Recon. Surg. 1986
- Weiland AJ et al. : Bone grafts: a radiologic, histologic, and biomechanical model comparing autografts, allografts, and free vascularized bone grafts. Plast Reconstr Surg. 1984

REGIONAL ANATOMY ANTERIOR VIEW POSTERIOR VIEW

FLAP ANATOMY
DOMINANT ARTERIAL SUPPLY
Peroneal artery
a) Dominant nutrient endosteal artery (Length 1.5 cm, diameter 1-2mm)
b) Minor periosteal septal and muscular branches

FLAP ANATOMY VENOUS SUPPLY
Venae comitantes of peroneal artery

FLAP ANATOMY
FLAP INNERVATION
Lateral sural nerve

FLAP COMPONENTS
Bone flap
Bone – skin flap
Bone – muscle (Soleus or FHL)
Bone – muscle – skin

ADVANTAGES - Vascularized bone suitable in cases of recipient site wound contamination, scarring, radiation, or poor vascularization
-A long segment of straight, triangular, high density cortical bone (20-26 cm in adults) capable of bridging long osseous defects and resisting angular and rotational stresses
-Fibula size matches the size of the radius and ulna, and snugly fits into the medullary cavity of the humerus, femur, and tibia
-As an osteoseptocutaneous flap, may be readily manipulated allowing greater versatility in wound closure compared to other osteocutaneous flaps (i.e. iliac crest and scapular osteocutaneous flaps)
-Well defined vascular supply allows for multiple osteotomies (2-3 cm bone segments)
-Suitable donor vessels allow for anastomoses to large vessels

DISADVANTAGES
- Obvious donor scar, particularly with skin component greater than 4 cm - Noticeable limitations and discomfort in ankle function and range of motion with aggressive physical activity may result after fibula harvest, particularly if tibio-fibular fusion is performed

PREOPERATIVE EVALUATION
CHECK FOR
MALFORMATIONS
TRAUMA
PERIPHERAL VASCULAR DISEASE
ARTHERITIS
DEEP VEIN THROMBOSIS

PALPABL DORSALIS PEDIS AND TIBIALIS POSTERIOR ARTERY
DUPLEX ULTRASONOGRAPHY ANGIOGRAPHY PERONEAL ARTERY MAGNA
PREOPERATIVE EVALUATION
Disa JJ, Cordeiro PG. The current role of preoperative arteriography in free fibula flaps.Plast Reconstr Surg. 1998 Sep;102(4):1083-8

ANESTHESIA
-GENERAL ANESTHESIA -REGIONAL BLOCK

PATIENT POSITIONING - Patient supine in the operating table - Knee flexed 90° - Pelvis girdle interiorly rotated - Stock of sterile towels under the heel - Tourniquet inflated at 375mmHg

FIBULA FLAP OSSEUS FLAP
OSTEOMUSCULAR FLAP
OSTEOCUTANEOUS FLAP
PEDICLED FLAP:
-ARC OF ROTATION CAN BE UP TO 180° -MEASURE CAREFULLY THE DEFECT LOCATION -THE BONE STOCK IS LOCATED AS DISTAL AS POSSIBLE IN ORDER TO -GAIN PEDICLE LENGTH

FLAP DIMENSIONS
BONE: 16 CM
SKIN ISLAND:
Length: 12CM
Width: 6CM
MUSCLE:
Entire hemi-soleus or part f the FHL

PLANNING
1) Bone
2) Skin paddle
3) Pedicle length
4) Muscle

TECHNIQUE OF FLAP HARVEST

Technique of Flap Harvest
Peroneal muscles
Post. Sup. muscle compartment
Dissection plane

Free Fibula Flap
Anterior Muscle Compartment

F.H.L. muscle
Free Fibula Flap
Posterior tibialis muscle

TECHNIQUE OF FLAP HARVEST

TECHNIQUE OF FLAP HARVEST

TECHNIQUE OF FLAP HARVEST

TECHNIQUE OF FLAP HARVEST

OSSEUS FLAP

OSSEUS FLAP
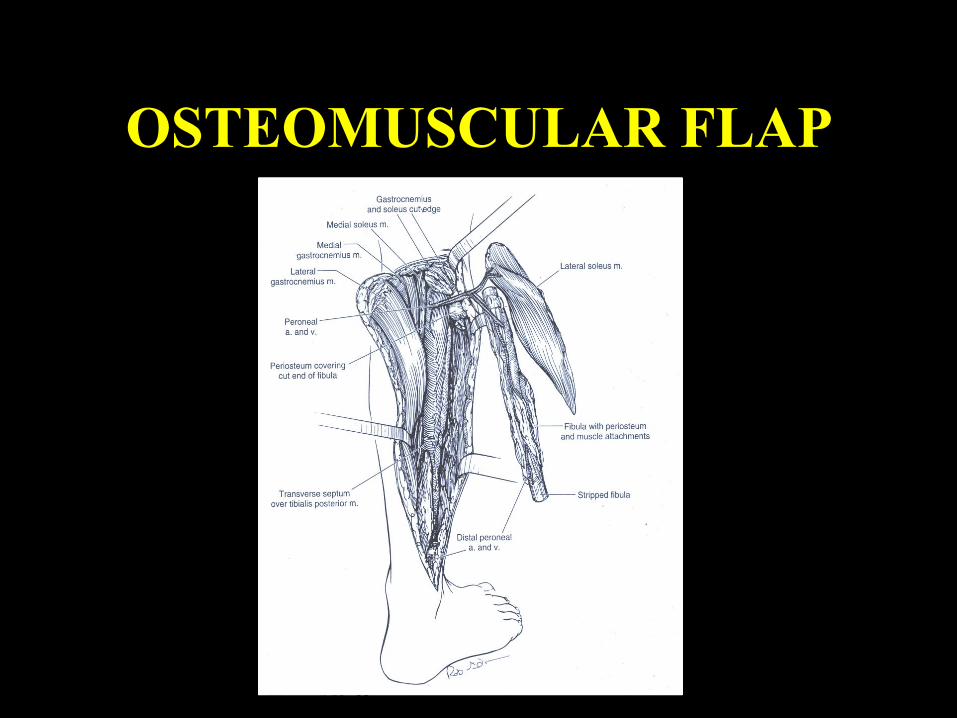
OSTEOMUSCULAR FLAP

BONE CONTOURING

BONE CONTOURING

BONE CONTOURING

PROXIMAL FIBULA

PROXIMAL FIBULA

DONOR SITE CLOSURE - RE-ATTACH FHL TO TIBIALIS POSTERIOR MUSCLE AND INTEROSSEOUS MEMBRANE (?)
- EMOSTASIS
- SUCTION DRAIN
- PRIMARY CLOSURE OR SKIN GRAFT (SKIN ISLAND > 4 CM)
- IF PRIMARY CLOSURE, MONITOR THE LEG POSTOPERATIVELY
- TISSUE EXPENSION

TECHNICAL TIPS
- CT angiogram (8% peroneal arteria magna) - Always include a skin paddle - Include a muscular cuff around the fibula - Subperiosteal dissection in the proximal fibula, until the peroneal nerve is identified

- Maintain distal periosteal cuff around the bony fixation - Verify the presence of the tibialis posterior artery and nerve - Accurate hemostatis - Minimal periosteal stripping at screw insertion site
TECHNICAL TIPS

TYPICAL INDICATIONS
- Segmental loss of long bones or craniofacial skeleton secondary to trauma, infection (osteomyelitis), radiation-induced necrosis (osteoradionecrosis), or after tumor extirpation - Avascular necrosis of the femoral head - Pseudoarthrosis (congenital or acquired) of the tibia, radius, or ulna - Club hand (radial or ulnar) - Penile reconstruction - Bone lengthening

ATYPICAL INDICATIONS
- Vertebral body reconstruction
- Pelvic ring reconstruction
- Proximal fibular head for reconstruction of the distal radius or proximal humerus.

POST-OPERATIVE CARE RECIPIENT SITE
Check every 30 min to 1 h:
flap color
temperature
turgor
capillary refill
Doppler

POST-OPERATIVE CARE RECIPIENT SITE
Monitor for:
- vascular insufficiency
- compartment syndrome
Posterior splint beyond the first toe
No need of bolster dressing, just wrap the leg with a compressive but not tiht dressing
No ambulation for the first two weeks

EXPECTED OUTCOMES
17% refers pain at the donor leg in the immediate post-op
Most of the patients expect to have minimal or no discomfort at 4 o 6 weeks
15-30% refer weakness at ankle and great toe

UNTOWARDS OUTCOMES Wound complication (> with primary closure)
delayed closure infection skin graft loss
Motor weakness of the great toe Contracture FHL Sensory loss Ankle instability or stiffness Donor site pain
Shpitzer T, Neligan P: Ann Plast Surg. 1997 May;38(5):460-4
Anthony JP$: Donor leg morbidity and function after fibula free flap mandible reconstruction. Plast Reconstr Surg. 1995
Bodde EW : Donor-site morbidity after free vascularized autogenous fibular transfer: subjective and quantitative analyses.Plast Reconstr Surg. 2003