psoriasishus.moh.gov.my/bm/wp-content/uploads/2018/07/psoriasis...how frequently do you expect to...
TRANSCRIPT
PsoriasisDiagnosis and treatment
PsoriasisDiagnosis and treatment
Dr Tang Min MoonMD(UKM) MRCP(UK) AdvMDerm(UKM)
Fellow(NSC, Singapore) Fellow(Bern University Hospital, Switzerland) Department of Dermatology
Hospital Kuala Lumpur21st July 2018
How frequently do you expect to see a patient with psoriasis in your clinic ?How frequently do you expect to see a patient with psoriasis in your clinic ?• Psoriasis 1 ‐ 3% of world population
– prevalence varies greatly among different countries – 0.2% in China ‐ 4.8% in Norway – Ethnicities FREE of psoriasis American Samoa & Mapuche in Chile
• No population‐based prevalence study on psoriasis in Malaysia – 2‐6% of yearly dermatology new clinic attendees in Malaysia– 9.54% of skin clinic attendees in Hospital Kuala Lumpur
Gudjonsson JE et.al, Clin Dermatol.2007;25:535‐546.Tsai TF et.al J Dermatol Sci.2011 63(1):40‐46.
Farber EM et al. Psoriasis. New York: Dekkar 1988. p107‐57Valenzuela F et al. Int J Dermatol 2012;51:1005‐6
Choon SE et.al International J Dermatol.2013Siow KY et al. MJM.2004 59(3):330 ‐ 334.
Heah SK et al. Malaysian J Dermatol 2017;38:19‐24
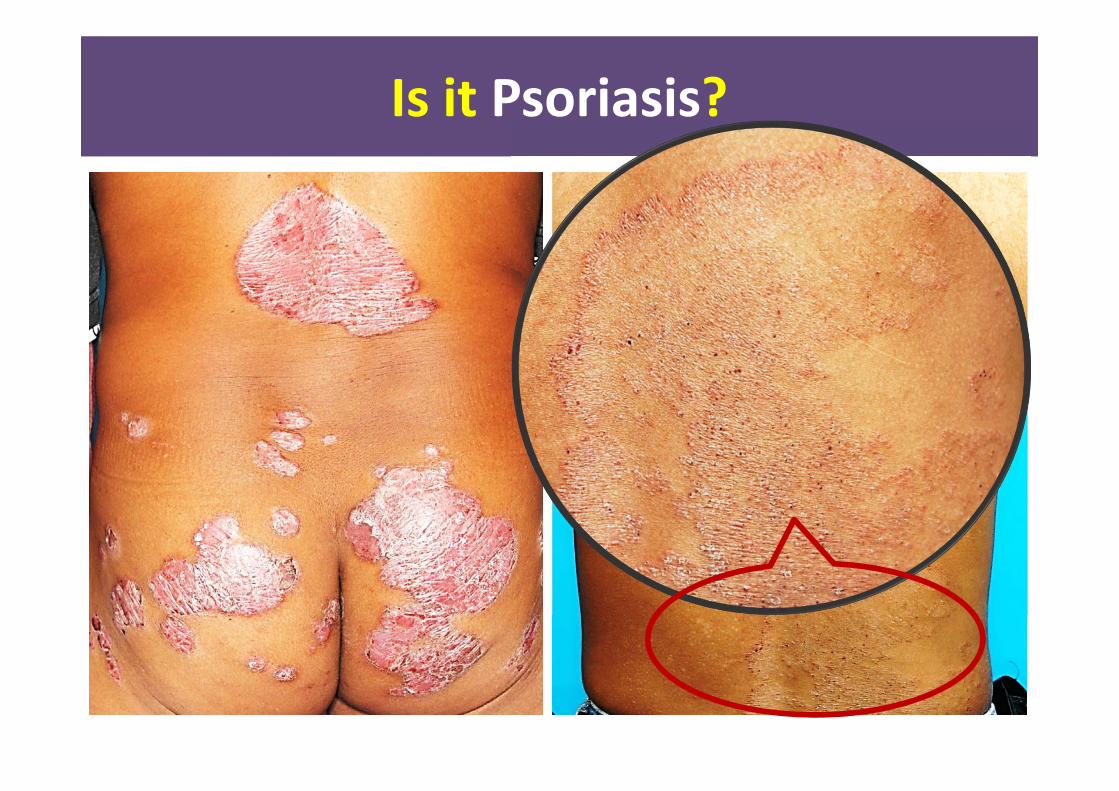
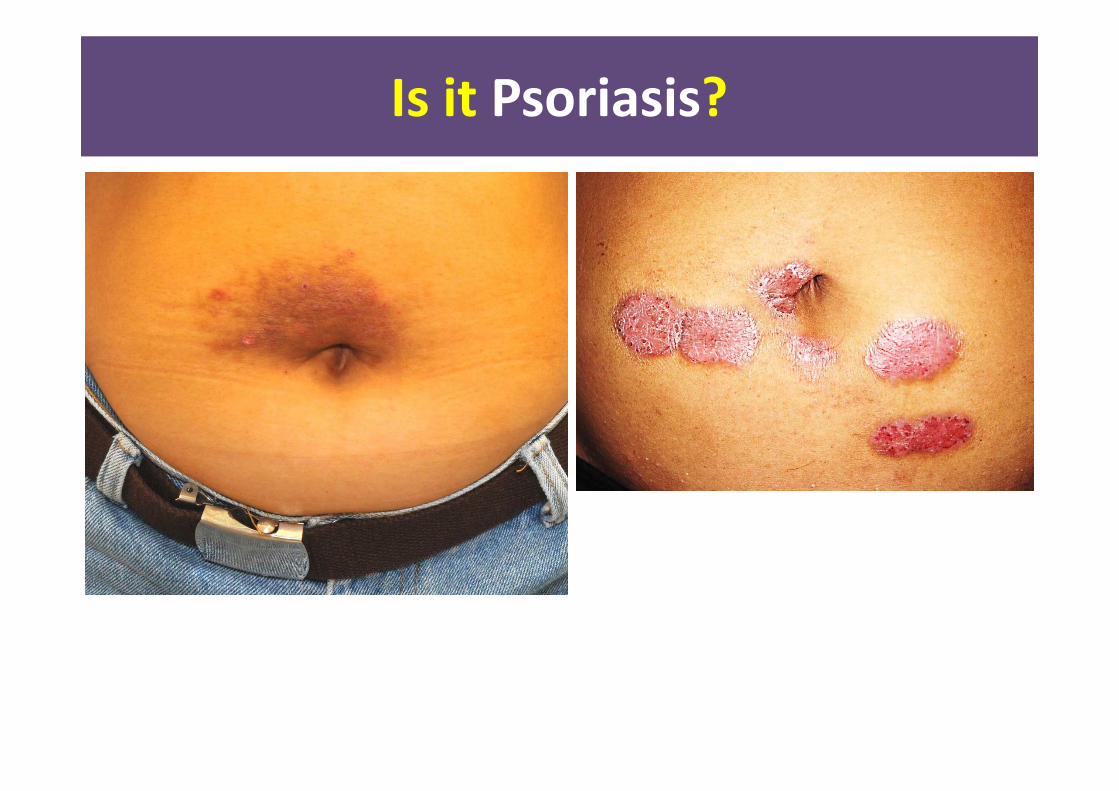
Is it Psoriasis?Is it Psoriasis?

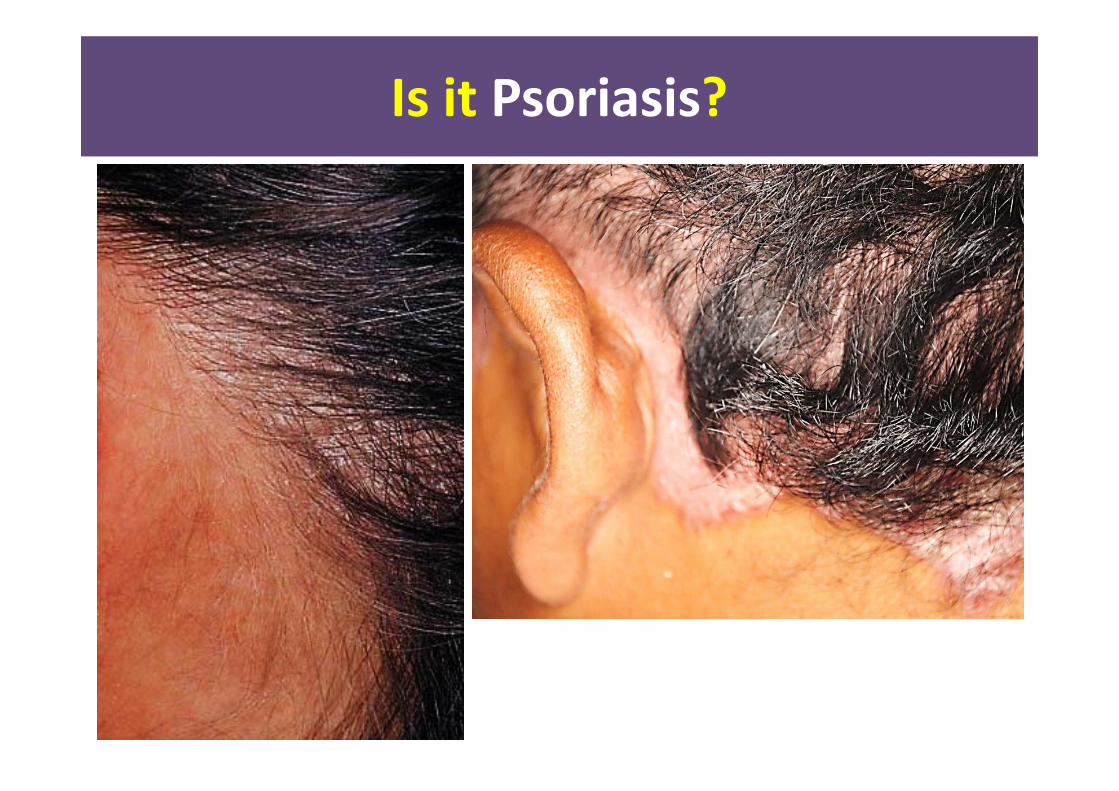
Is it Psoriasis?Is it Psoriasis?

Is it Psoriasis?Is it Psoriasis?
Is it Psoriasis?Is it Psoriasis?
Is it Psoriasis?Is it Psoriasis?

Is it Psoriasis?Is it Psoriasis?

Is it Psoriasis?Is it Psoriasis?

How do you recognize psoriasis??How do you recognize psoriasis??
• Elevated plaques• Scaly erythematous • sharply demarcated • Coarse & thick scales • extend 1‐2 cm beyond the hairline
• Koebner’s phenomenon
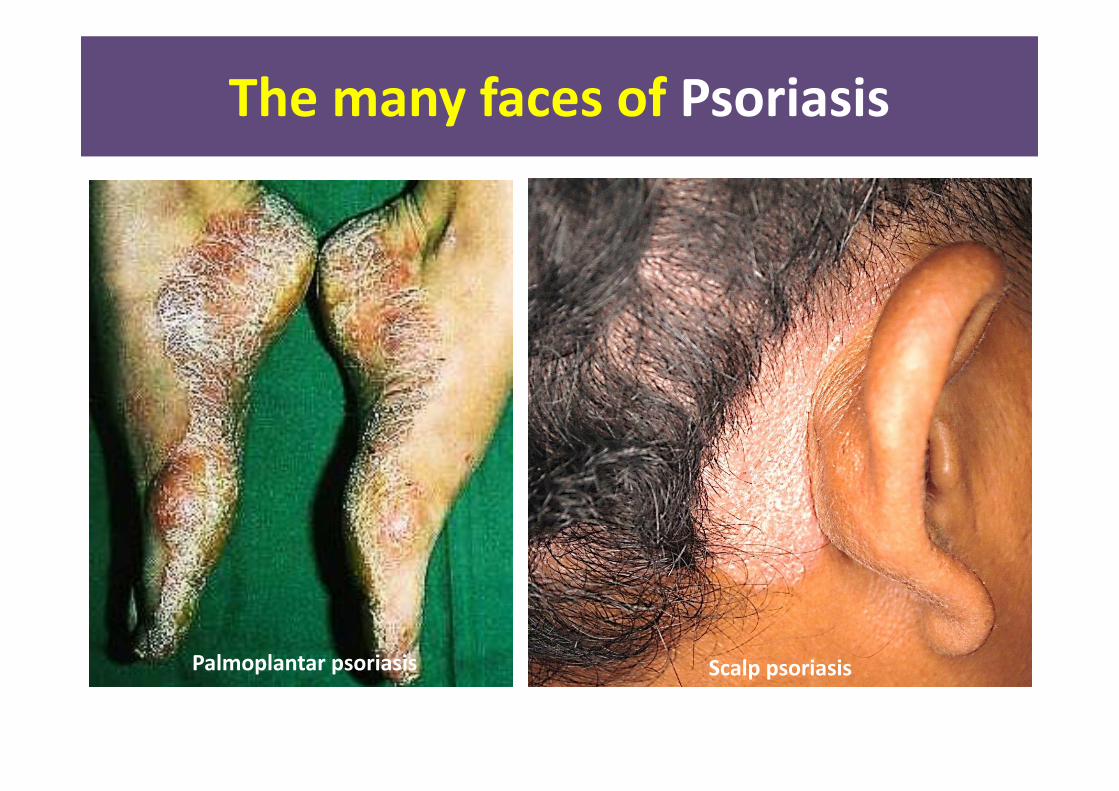
The many faces of PsoriasisThe many faces of Psoriasis
Palmoplantar psoriasis Scalp psoriasis

The many faces of PsoriasisThe many faces of Psoriasis
Guttate psoriasis
Inverse psoriasis

The many faces of PsoriasisThe many faces of Psoriasis
Erythrodermic psoriasis Pustular psoriasis

The many faces of PsoriasisThe many faces of Psoriasis
GPP – annular type GPP – Von Zumbusch
LPP – acrodermatitis continua of Hallopeau
LPP – palmoplantar pustulosis

The many faces of PsoriasisThe many faces of Psoriasis

The many faces of PsoriasisThe many faces of Psoriasis
Patient: Are you sure this is psoriasis? Why me? None of my family has it.
Patient: Are you sure this is psoriasis? Why me? None of my family has it.

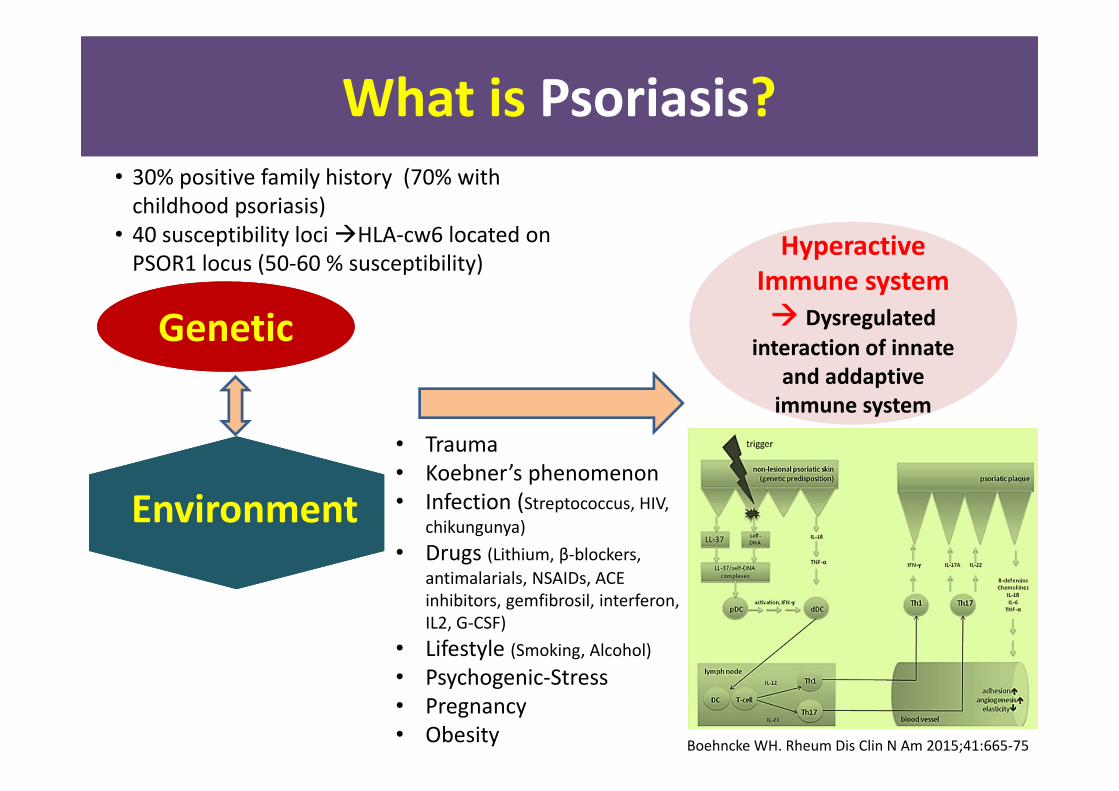
What is Psoriasis?What is Psoriasis?
Environment
GeneticGeneticHyperactive Immunesystem
Hyperactive Immunesystem
Systemic chronic inflammatory disease predominantly affects the skin and joints
What is Psoriasis?What is Psoriasis?
Environment
GeneticGenetic
Hyperactive Immune system Dysregulated
interaction of innate and addaptiveimmune system
Hyperactive Immune system Dysregulated
interaction of innate and addaptiveimmune system
• 30% positive family history (70% with childhood psoriasis)
• 40 susceptibility loci HLA‐cw6 located on PSOR1 locus (50‐60 % susceptibility)
• Trauma• Koebner’s phenomenon• Infection (Streptococcus, HIV,
chikungunya)• Drugs (Lithium, β‐blockers,
antimalarials, NSAIDs, ACE inhibitors, gemfibrosil, interferon, IL2, G‐CSF)
• Lifestyle (Smoking, Alcohol)• Psychogenic‐Stress• Pregnancy• Obesity Boehncke WH. Rheum Dis Clin N Am 2015;41:665‐75
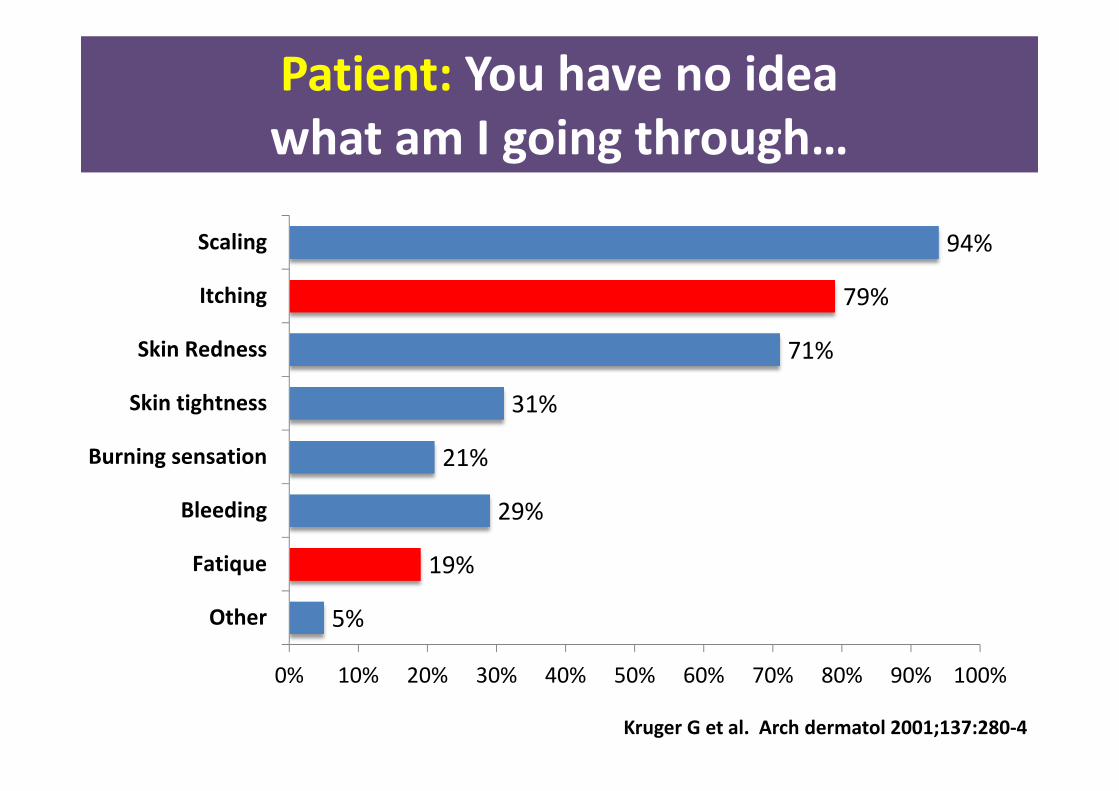
Patient: You have no idea what am I going through…Patient: You have no idea what am I going through…
Physical discomfort1. Pruritus2. Scaling3. Tightness4. Pain5. Bleeding
Patient: You have no idea what am I going through…Patient: You have no idea what am I going through…
5%
19%
29%
21%
31%
71%
79%
94%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Other
Fatique
Bleeding
Burning sensation
Skin tightness
Skin Redness
Itching
Scaling
Kruger G et al. Arch dermatol 2001;137:280‐4
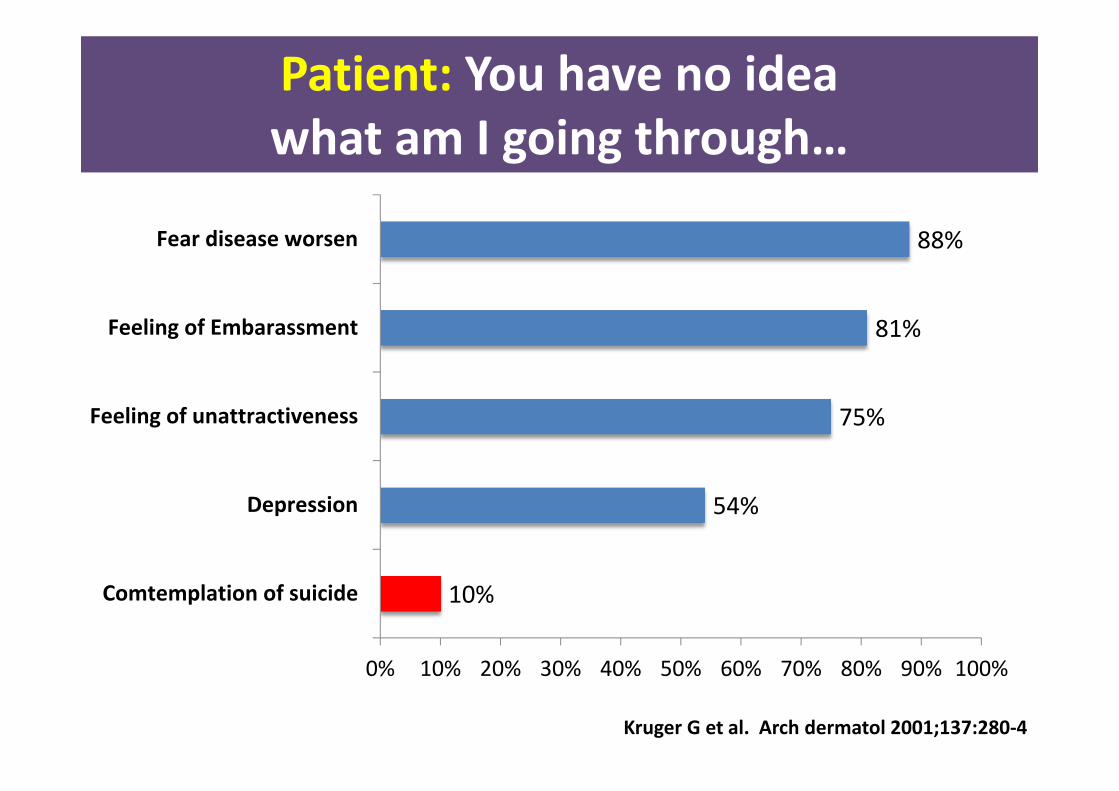
Patient: You have no idea what am I going through…Patient: You have no idea what am I going through…
Kruger G et al. Arch dermatol 2001;137:280‐4
10%
54%
75%
81%
88%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Comtemplation of suicide
Depression
Feeling of unattractiveness
Feeling of Embarassment
Fear disease worsen
Patient: Is it only the skin?Patient: Is it only the skin?
• Higher risk (2‐3x) of metabolic syndrome– Obesity, DM, dyslipidaemia, hypertension
• Severe psoriasis– 3 fold increased risk of developing MI especially young
– 3‐4 year ↓ in life expectancy
• Lymphoma, NMSC

How do you manage Psoriasis?a highly visible disease
How do you manage Psoriasis?a highly visible disease
First, assess the severityFirst, assess the severityPhysical severity1. BSA (% of body surface
involvement)2. PASI (Psoriasis Area and
Severity Index)3. PGA (Physician Global
Assessment)
Quality of Life1. Dermatology Life Quality
Index (DLQI)2. Psoriasis Disability Index
(PDI)3. Short Form 36 (SF36)

First, assess the severityFirst, assess the severityPhysical severity1. BSA (% of body surface
involvement)2. PASI (Psoriasis Area and
Severity Index)3. PGA (Physician Global
Assessment)
Quality of Life1. Dermatology Life Quality
Index (DLQI)2. Psoriasis Disability Index
(PDI)3. Short Form 36 (SF36)
• Area of palm plus 5 fingers ≈ 1% of total BSA– Head and Neck = 10% (10 palms)– Upper extremities = 20% (20 palms)– Trunk (axillae and groin) = 30% (30
palms)– Lower extremities (buttocks) = 40% (40
palms)– Total BSA = 100% (100 palms)
~1% BSA

First, assess the severityFirst, assess the severity
Grade Definition of severityMild BSA ≤ 10% or
PASI ≤ 10 orDLQI ≤ 10
Moderate BSA >10% to 30% orPASI >10 to 20 orDLQI >10 to 20
Severe BSA > 30% orPASI > 20 orDLQI >20
Malaysian Clinical Practice Guideline on the Management of Psoriasis VulgarisDefinition of Psoriasis Severity

Second, set a goal of treatmentSecond, set a goal of treatmentTreatment Minimal targets Time for Evaluation
(Induction phase)(weeks)
Subsequent Evaluation(Maintenance phase)
(months)
Topical therapy ↓ BSA ≥ 50% orPASI ≥ 50 orDLQI ≤ 5
6 6 ‐12
Phototherapy↓BSA ≥ 75% orPASI ≥ 75 orDLQI ≤ 5
6 6 Methotrexate 16
Cyclosporin 16Acitretin 24Infliximab ↓PASI ≥ 75% or
PASI 50 to <75 plus DLQI ≤ 5
10 6
Adalimumab 16Ustekinumab 16Etanercept 24

Third, choose the best available treatment modality
Third, choose the best available treatment modality
• Share decision between patients and cliniciansTopical Rx Phototherapy Systemic Rx BiologicsCoal Tar
Keratolytics
Topical steroids*
Vit D3 analogues
Dithranol(anthralin)
Emollients
NB‐UVB
Oral PUVA
Bath PUVA
Topical PUVA
Methotrexate
Acitretin (Retinoid)
Sulphasalazine
Cyclosporin
Hydroxyurea
Systemic steroids*
Etanercept
Infliximab
Adalimumab
Ustekinumab
Secukinumab
Safe Still safe Potential risk Higher risk

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatment

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatment
Emollient• Moisturizer• Restore normal hydration & epidermal barrier function
• May have steroid‐sparing effect
• Use regularly

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatmentDithranol (Anthralin)• Anti‐proliferative & anti‐inflammatory drugs
• Short contact therapy (20‐30min)
• Apply accurately to affected large thick plaques, remove with liquid paraffin

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatment
Topical tar• Reduce cell turnover, anti‐inflammatorym antikeratotic
• Available as shampoo, bath additives, ointment, lotions, pastes
• Avoid body folds, face & genitalia
• No increase in cancer

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatmentTopical corticosteroids• Anti‐inflammatory, antiproliferative, immunosuppressive, vasoconstrictive
• cream, ointment, gel, spray, lotion• Short term potent/superpotentcorticosteroids rapid clearance of psoriasis with limited plaques• Avoid face, genitalia, body folds• Limit super potent steroid <30g/week• Limit potent steroid <60g/week
• Use on extensive lesions /large areas skin atrophy & systemic absorption

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatmentTopical corticosteroids• Anti‐inflammatory, antiproliferative, immunosuppressive, vasoconstrictive
• cream, ointment, gel, spray, lotion• Short term potent/superpotentcorticosteroids rapid clearance of psoriasis with limited plaques• Avoid face, genitalia, body folds• Limit super potent steroid <30g/week• Limit potent steroid <60g/week
• Use on extensive lesions /large areas skin atrophy & systemic absorption

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Topical treatment
Calcipotriol (Vitamin D analogues)• Enhances normal keratinization, inhibit epidermal proliferation
• Do not >100g/wk to avoid hypercalcemia
• Avoid face
Topical salicylic acid• Keratolytics↓scaling & softening of psoriatic plaques
• Used in combination with topical steroids

Third, choose the best available treatment modality
Third, choose the best available treatment modality
PhototherapyUltraviolet B• Broad band UVB (290‐320nm)
• Narrow band UVB (311nm)
Psoralen + Ultraviolet A• Topical PUVA (320‐400nm)• Oral PUVA• Bath PUVA• Hand & foot PUVA

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Phototherapy

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Phototherapy

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Phototherapy – NBUVB in Psoriasis
Before treatment 10 week6 week

Third, choose the best available treatment modality
Third, choose the best available treatment modality
Phototherapy – Oral PUVA in Psoriasis
Before treatment 6 week (5MOP, 4x/week)

Systemic treatment & BiologicsSystemic treatment & Biologics
……to be continued tomorrow ..…..

Take home messageTake home message
• Psoriasis ~2% of population• Chronic immune‐mediated inflammatory disease involving skin & joint disfiguring
• Treatment should be personalized, tailored to disease severity with a goal set
• Psoriasis higher risk of metabolic syndrome• Young, severe psoriasis higher risk of myocardial infarction
Thank youThank you