from are to hair: when it isn’t rare - neposeyes.orgneposeyes.org/files/chair_care.pdf · from...
TRANSCRIPT
From Care to Chair: When It Isn’t Rare
Diana Shechtman, O.D., F.A.A.O.
Jeffry Gerson, O.D., F.A.A.O.

Disclosure
• We have both worked for a number of industry companies, and will not be influenced for the purposes of this (or other) lecture
How did we come up with the title?
What do you do?
a. Take care of eyes
b. Whatever insurance companies say I have to
c. prescribe glasses, contacts and eyedrops
d. Whatever you say…
e. None of the above
YOU TAKE CARE OF PEOPLE…NOT JUST EYES!!

Start to look at things from a different perspective…

Start to look at things from a different perspective…

• Most people think that they are going to live forever ….until they develop a cold.
• How does this relate to optometry?

What is this?
A. Choroidal Melanoma
B. Metastatic Carcinoma
C. Retinal Detachment
D. None of the Above
E. Combination of 2 of the above
Quote by Maimonides
• “May I never forget that the patient is a fellow creature in pain. May I never consider him merely a vessel of disease.”
• How does this pertain to the previous slide? (and to the rest of what we do as optometrists)

Lets Try Again: What was this?
A. Incidental finding: At a routine exam by O.D.
B. Bad news: For a calm Husband
C. Life Changing Diagnosis: For a family
D. Mortality: For a person
E. All of the Above
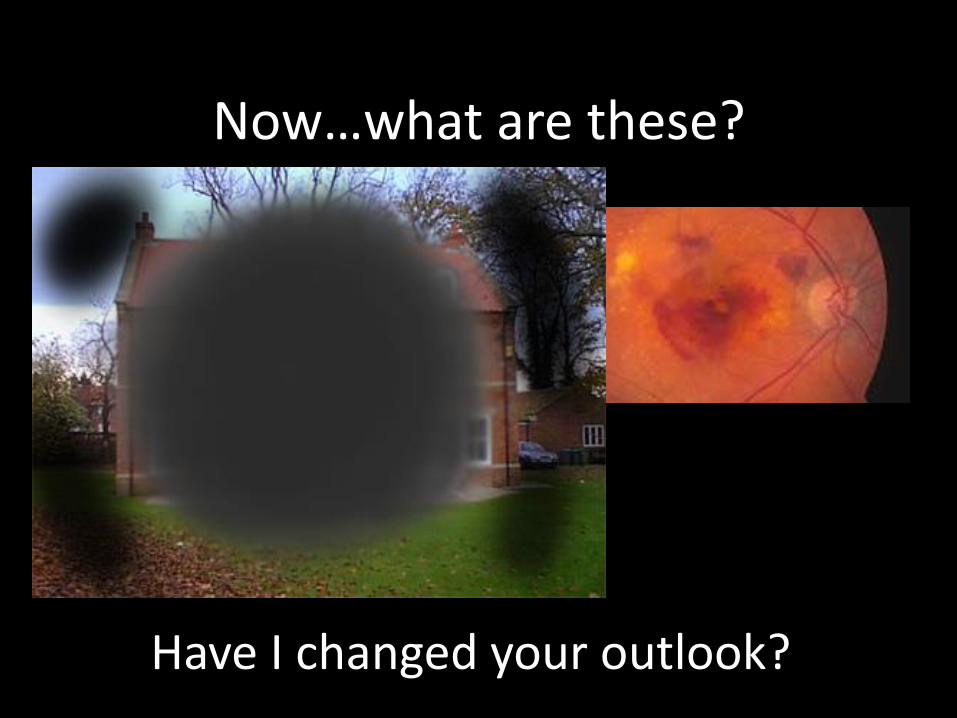
Now…what are these?
• AMD?
• Threat to vision?
• Change in outlook on life?
Have I changed your outlook?

What is YOUR job? (as an O.D.)
• Is it to examine eyes and diagnose eye conditions?
• Help people see better?
• Explain conditions and help treat them?
• “Every time a patient see’s a doctor, they should feel better as a result.”
Treating vs. Healing
• A disease entity is treated
• A person is healed
• Can we do both?
• Often times the goal shifts to treating without regard to healing
– Less regard to comprehensive history taking, chairside manner and overall interaction
A different way to think…
Robin Williams as Path Adams, M.D.
Communication
• Crucial part of every doctor-patient encounter
• Two way street
• Use appropriate terms and tone
– Authority without being dogmatic
– Use understandable terms

When you ask your patient about their chief complaint, how long do you let them
speak?
A. 2 seconds
B. 18 seconds
C. 55 seconds
D. 2 ½ minutes
E. As long as they need
Let the patient speak!
• Good communication starts with listening…
• How long is the average patient allowed to talk when asked of their chief complaint?
– 18 seconds
– 77% never get to complete their opening statement!
– If left uninterrupted, avg. patient would talk 150 sec.
– Avg patient at PCP has 1.2 to 4.9 “chief complaints”
Don’t…
• Use scare tactics
• Knock another doctor
• Fake an answer
• Hide the truth
• Think that everything always can and needs to be fixed.
• Be afraid to admit mistakes or lack of knowledge
Cartoon compliments of Wisconsin Health Freedom Coalition
Words that maim vs words that heal• It’s not what you say, but how you say it
• Language doesn’t carry ideas, it shapes them
• Avoid jargon
• We should never instill uncertainty and dread– Simple mention of cataract can do this!
• Worst case scenario often presented to avoid malpractice (opposite affect)
“Your eye pressure is 25, and you may go blind from glaucoma if we don’t do something about it quickly”
Bedell et al. Words that Harm, words that heal. Arch Intern Med. 2004 Jul 12;164(13).

Words that heal
• Healing words set stage for collaborative decision making
• Verbal and non-verbal language
• Positive “spin”, avoid negativity
• Persuading a patient that nothing is wrong is often a thankless task, if not impossible
“Your eye pressure is slightly elevated, so I’d like to do a few extra tests to insure that everything is just fine”

Speaking of being scared….

Maim or Heal?
• How do you describe a choroidal nevus to a patient?
– Do you mention the chance of conversion to melanoma?
– Do you compare to freckle?
– Do you correlate to skin cancer?
– Do you not mention it to patient?

Breaking Bad News
• How many classes in school discussed this?
• But it comes up every day
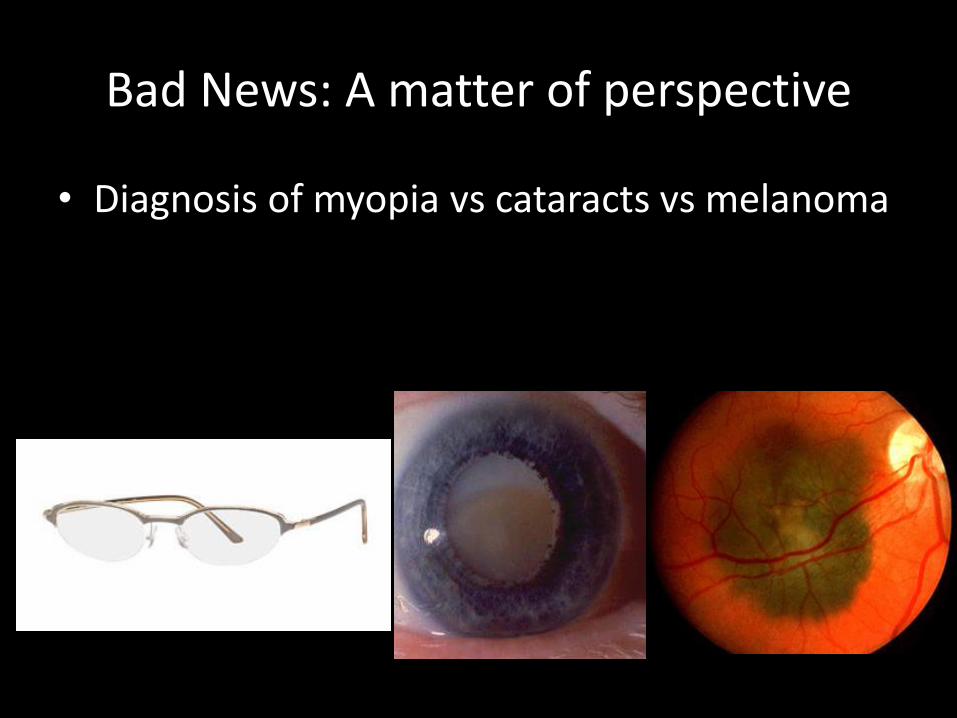
Bad News: A matter of perspective
• Diagnosis of myopia vs cataracts vs melanoma

Bad News
• Definition?– Anything that drastically and/or negatively affects a patient’s view of their
future
– The difference between what a patient expects and what we tell them
• Who needs to break bad news?– We do
• Do we have an ethical obligation to tell truth?– Yes
• Can this “art” be learned?– Yes by experience and researching and understanding
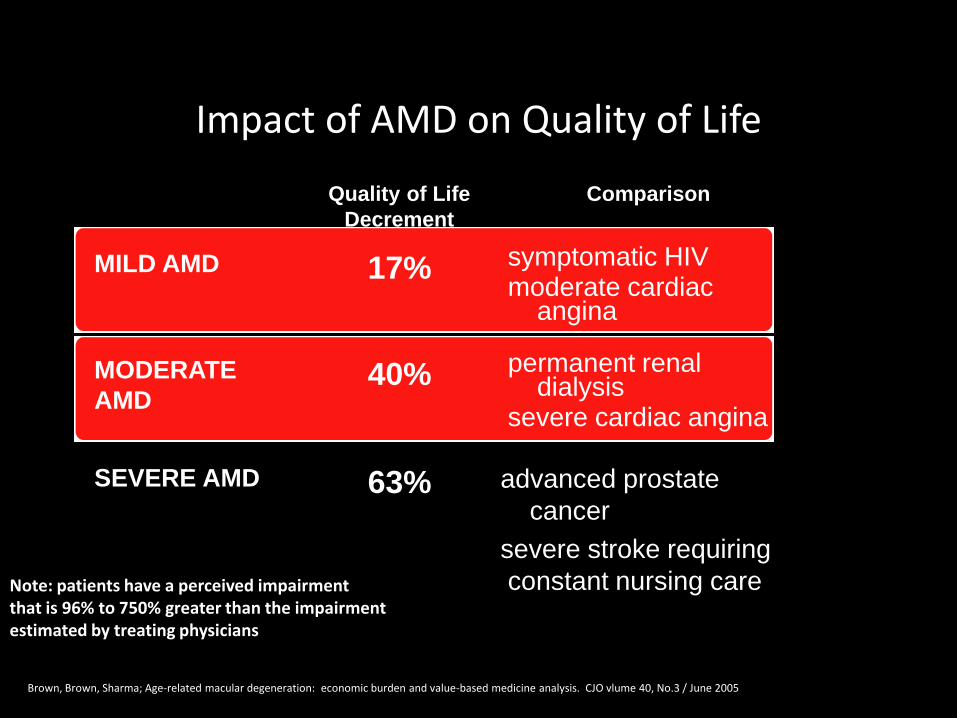
Impact of AMD on Quality of Life
Quality of Life
Decrement
Comparison
MILD AMD 17% symptomatic HIVmoderate cardiac
angina
MODERATE
AMD40% permanent renal
dialysissevere cardiac angina
SEVERE AMD 63% advanced prostate
cancer
severe stroke requiring
constant nursing careNote: patients have a perceived impairment that is 96% to 750% greater than the impairment estimated by treating physicians
Brown, Brown, Sharma; Age-related macular degeneration: economic burden and value-based medicine analysis. CJO vlume 40, No.3 / June 2005
Now to the science (and cases)
Why do we do what we do?
• Clinical intuition
• Case reports
• Case series
• Clinical trials
– Who is the sponsor?
– Who are investigators?
– What is study design?

Clinical Trials
• Often sponsored by NEI/NIH or by industry
• May be for FDA approval or to confirm usefulness of treatment
• Hallmark in determining standard of care
– The basis for science/evidence based medicine

Terms related to clinical trials
• Randomized
• Single vs Double Blind
• Multicenter
• Controlled (Placebo)
• Prospective vs Retrospective
Historic Trials
• DRS / ETDRS
• TAP
• CVOS
• ONTT
• MPS
• COMS
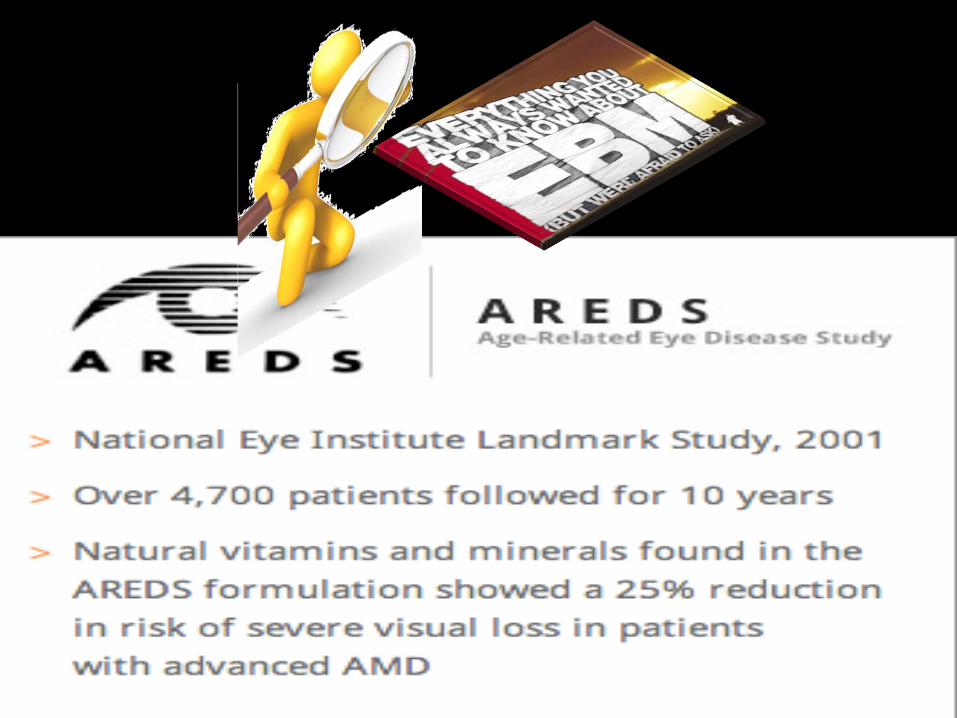
• AREDS
• LAST

Recent Trials and Ongoing
• DRCR.net
• MARINA/ANCHOR/PRONTO
• CATT
• AREDS II
• VEGF Trap: VIEW 1
• COBALT
• VAST
• 100’s of ongoing trials…

OD involvement in Trials
• How many OD’s directly involved in retina clinical trials?
• Indirect involvement crucial
– Find participating centers
– Inform and send patients
Where do we find what we need?
• Sources for Clinically relevant scientific information
– Eye specific: ex: Opthalmology, Review of Optometry, OVS, AJO
– Disease specific: Diabetes, Diabetes Care
– General medicine: JAMA, NEJM, Science
Can you believe everything you read?
• How do we analyze what we read– Size of study
– Prospective vs retrospective
– Double blind vs not
– Randomized?
– Placebo controlled (where pertinent)
– Multi centered unbiased (vs single site company sponsored)
• Statistical analysis and significance

Clinical Trials…not an easy (or cheap process)

Can EBM always apply to pt care?
• EBM derived from GROUPS and now applied to INDIVIDUALS?
• The MAIN benefits or ineffectiveness may be are in the summary but
– What does it really imply? Is there probability that BENEFITS outweigh the RISKS?
• The results are NOT one size fits ALL

Let’s apply it….

Are you high tech or high touch?
• Can we be both?
• What do your patients want?
• What is your first line of defense?

Clinical exam
**BIO best for clinical exam of peripheral retina
Condensing lens at slit lamp ideal for magnified posterior pole views
Dynamic clinical exam
Require examiner to document
Some things best seen clinically, and unable to be seen with imaging devices


New onset floaters
• Healthy 55yo male
• 20/20 OU
• New onset floaters x5days without flashes
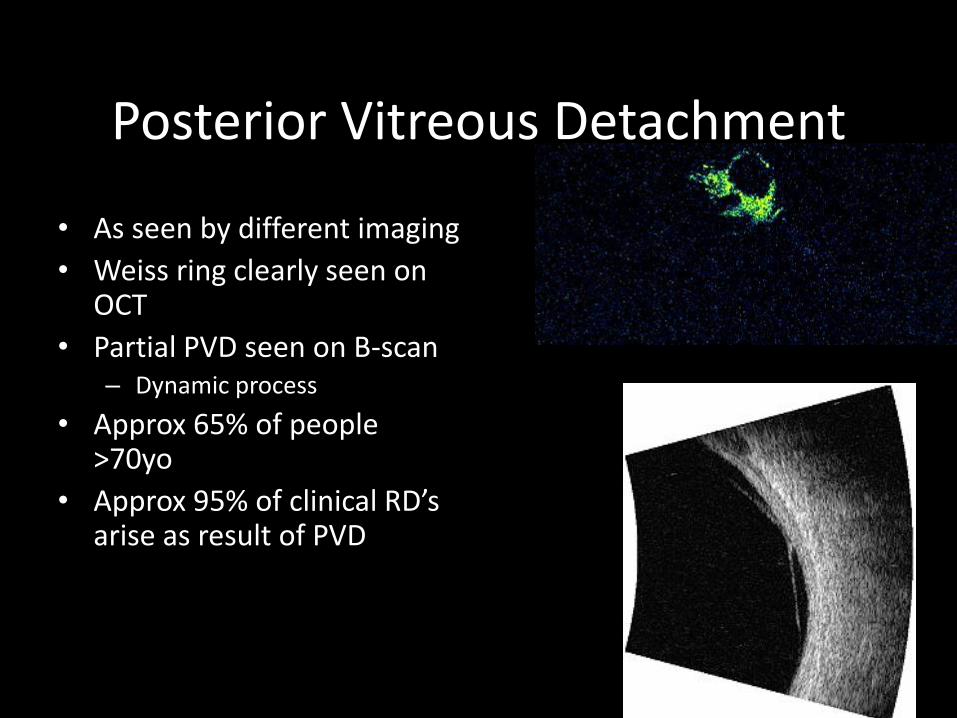
Posterior Vitreous Detachment
• As seen by different imaging
• Weiss ring clearly seen on OCT
• Partial PVD seen on B-scan– Dynamic process
• Approx 65% of people >70yo
• Approx 95% of clinical RD’s arise as result of PVD

Vitreous Hemorrhage
• If PVD with VH, approx 50-70% have tear
• If no tear seen, look harder until find
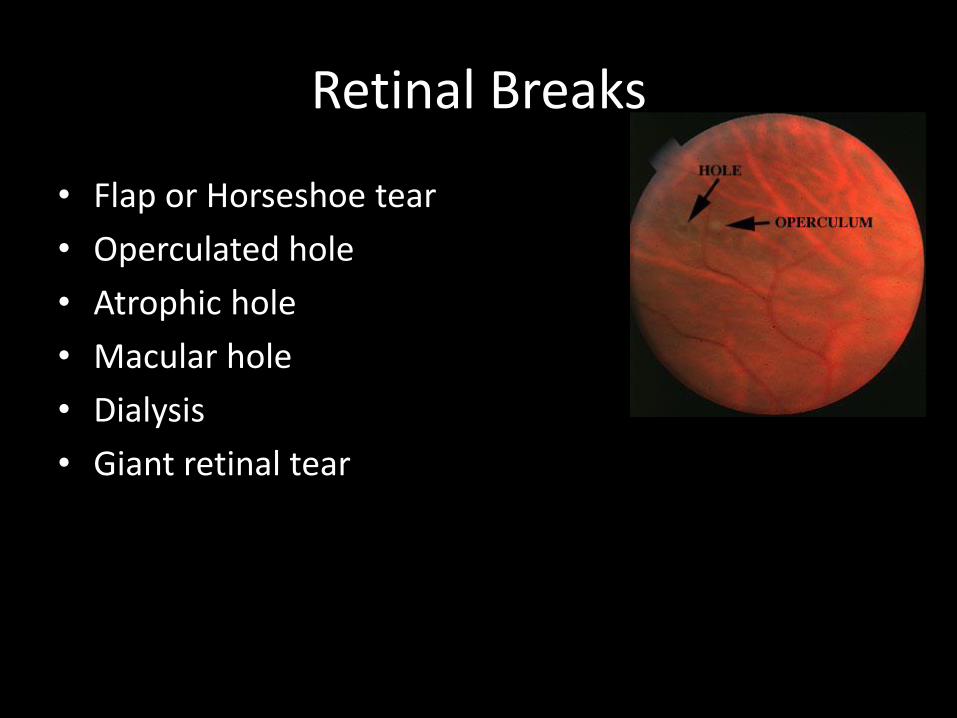
Retinal Breaks
• Flap or Horseshoe tear
• Operculated hole
• Atrophic hole
• Macular hole
• Dialysis
• Giant retinal tear

Retinal Holes
• Can occur anywhere
• Generally no treatment, unless symptomatic
• Rarely progresss to RD
• Pigmentation sign of chronicity
• PVD protective

Retinal Tears
• Up to 15% of symptomatic PVD will develop tear
• **What do you do about symptomatic tear?
• Refer for treatment

Tear Treatment
• Symptomatic tears require laser treatment
• Before and after
• Why treat symptomatic…
– Approx 50% untreated will develop RD
– Approx 5% treated still develop RD
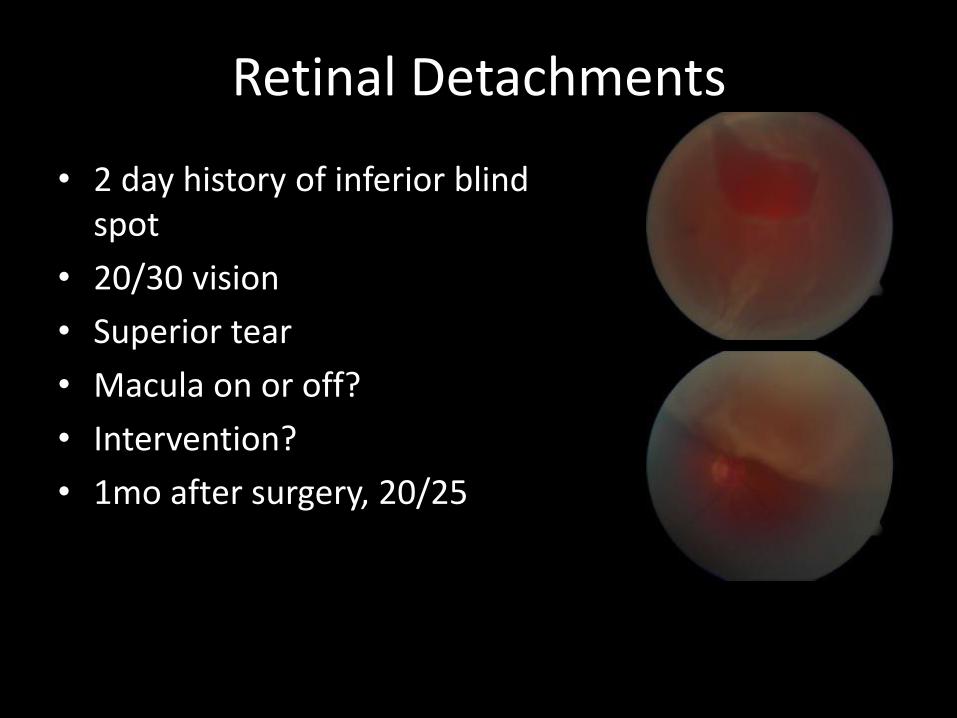
Retinal Detachments
• 2 day history of inferior blind spot
• 20/30 vision
• Superior tear
• Macula on or off?
• Intervention?
• 1mo after surgery, 20/25
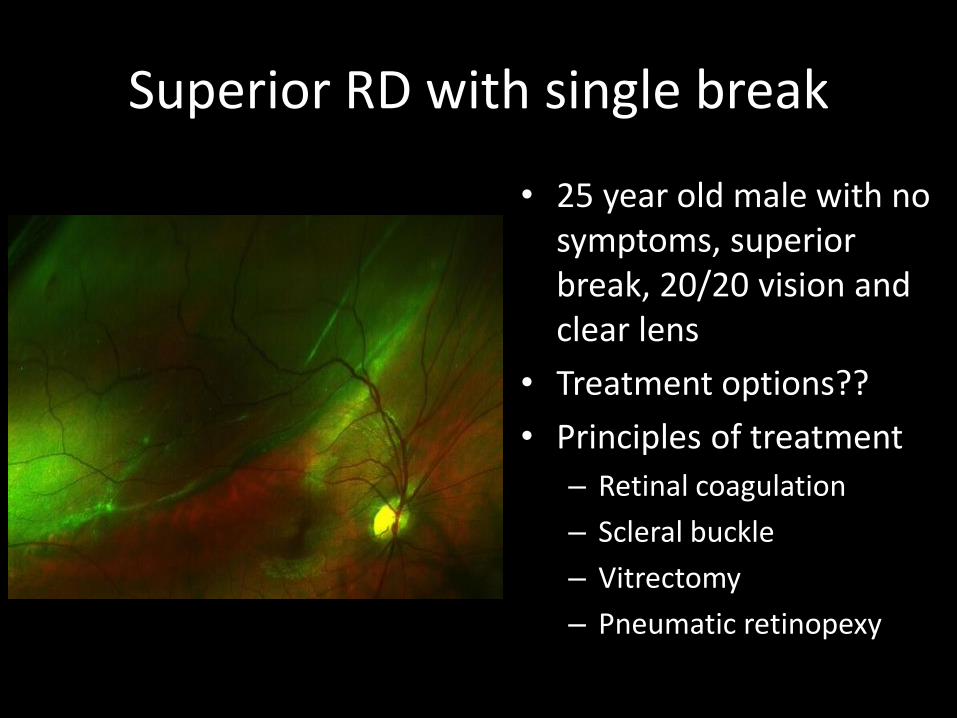
Superior RD with single break
• 25 year old male with no symptoms, superior break, 20/20 vision and clear lens
• Treatment options??
• Principles of treatment
– Retinal coagulation
– Scleral buckle
– Vitrectomy
– Pneumatic retinopexy
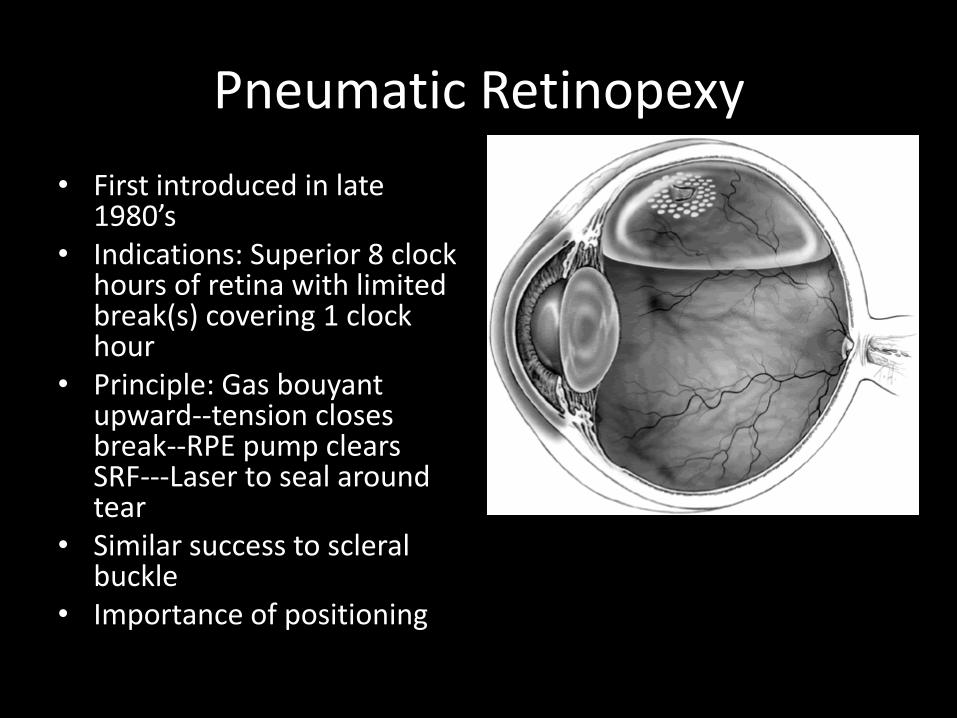
Pneumatic Retinopexy
• First introduced in late 1980’s
• Indications: Superior 8 clock hours of retina with limited break(s) covering 1 clock hour
• Principle: Gas bouyant upward--tension closes break--RPE pump clears SRF---Laser to seal around tear
• Similar success to scleral buckle
• Importance of positioning
What’s This????
• RD with tear at 930 OD
• Gas Injected day before to tamponade
• Returned next (day of photo) to receive successful laser
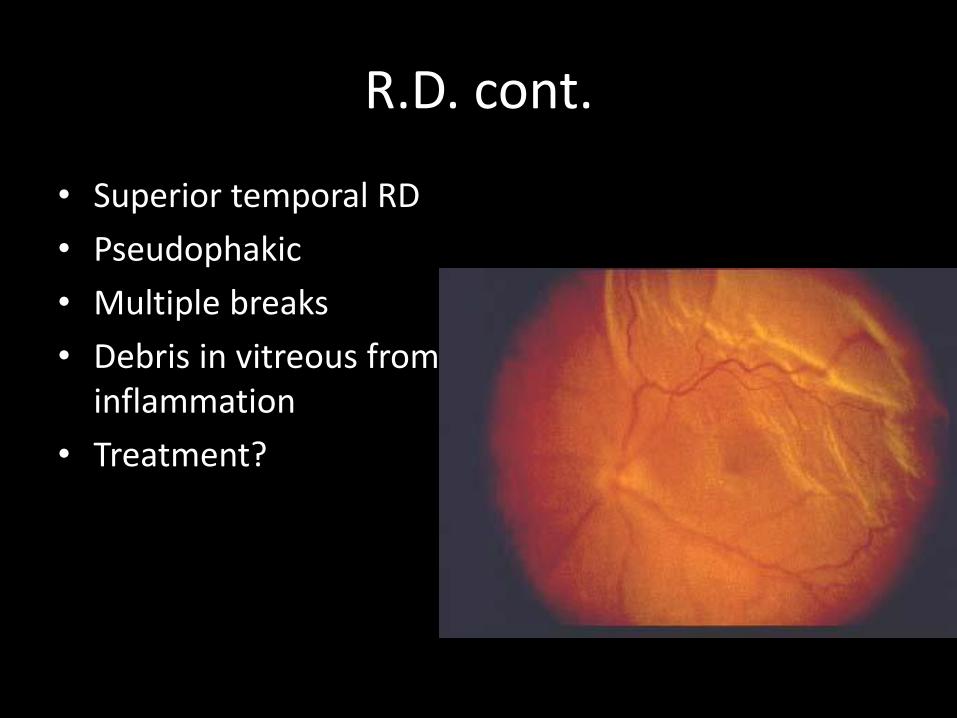
R.D. cont.
• Superior temporal RD
• Pseudophakic
• Multiple breaks
• Debris in vitreous from inflammation
• Treatment?

Primary Vitrectomy
• Better ineroperative sight of peripheral tears
• Controlled removal of vitreous
• Focused endo-laser• Very low occurrence of PVR• Allows for internal drainage• Air/Fluid/Gas exchange for
tamponade• Excellent outcomes
– 25g Vitrectomy
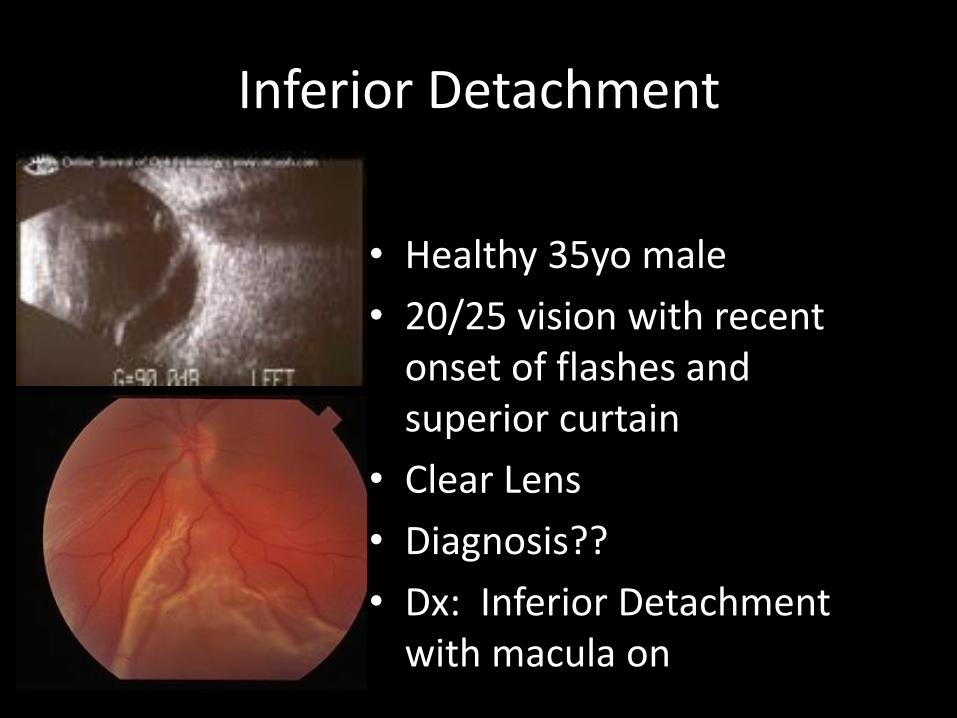
Inferior Detachment
• Healthy 35yo male
• 20/25 vision with recent onset of flashes and superior curtain
• Clear Lens
• Diagnosis??
• Dx: Inferior Detachment with macula on
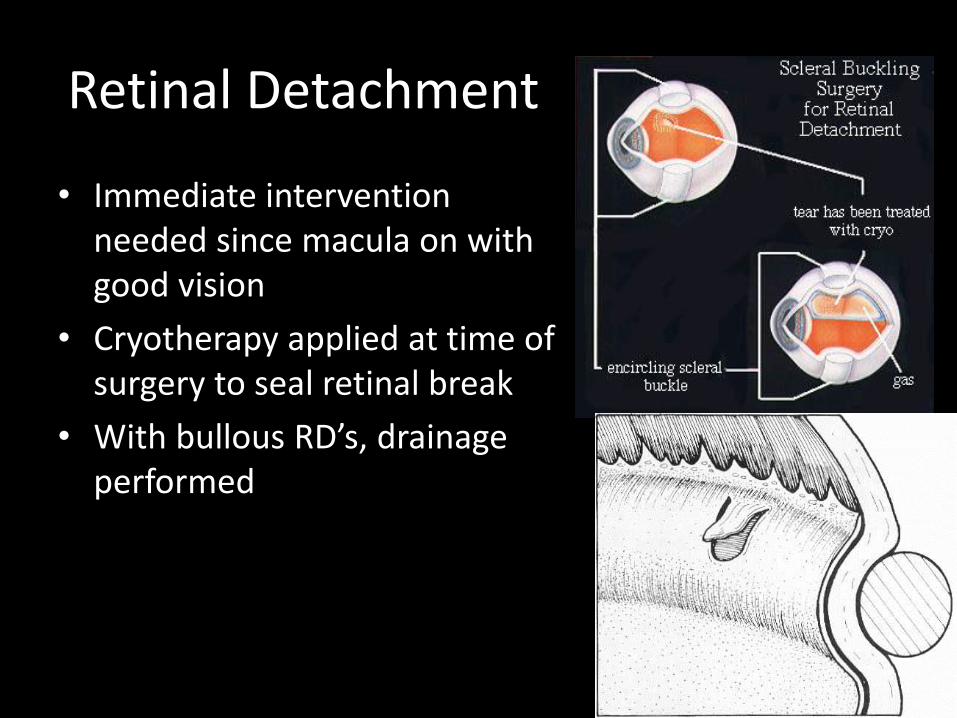
Retinal Detachment
• Immediate intervention needed since macula on with good vision
• Cryotherapy applied at time of surgery to seal retinal break
• With bullous RD’s, drainage performed

Scleral Buckle
• First performed in 1951
• Traction pulls along downslope of buckle to create radial force
• Change in eye contour creates new tangential force to flatten retina
• Different materials can be used for buckle
• Buckle minimally visible externally normally
• Potential complications– PVR
– Buckle related

Scleral Buckle• Unable to use gas
tamponde with inferior break
• Scleral buckle surgery gold standard
• SB alone as effective as SB +PPV in cases of undetected breaks1
• Yellow area is scar from cryotherapy
Salicone et al. Mangement of RD when No Break is found. Ophthalmology. 3/2006

What’s this?
• Scleral Buckle extrusion
• Can cause diplopia, motility problems, changes to retina appearance, endophthalmitis
• Treatment: removal of buckle, culture, antibiotic treatment

To Treat or Not to Treat
• Indications for treatment– Horse-shoe tear almost always
– Dialysis almost always
– Operculated holes sometimes
– Atrophic holes rarely
– Lattice no holes rarely
– Retinal Detachment• Macula On Emergent
• Macla Off Not emergent
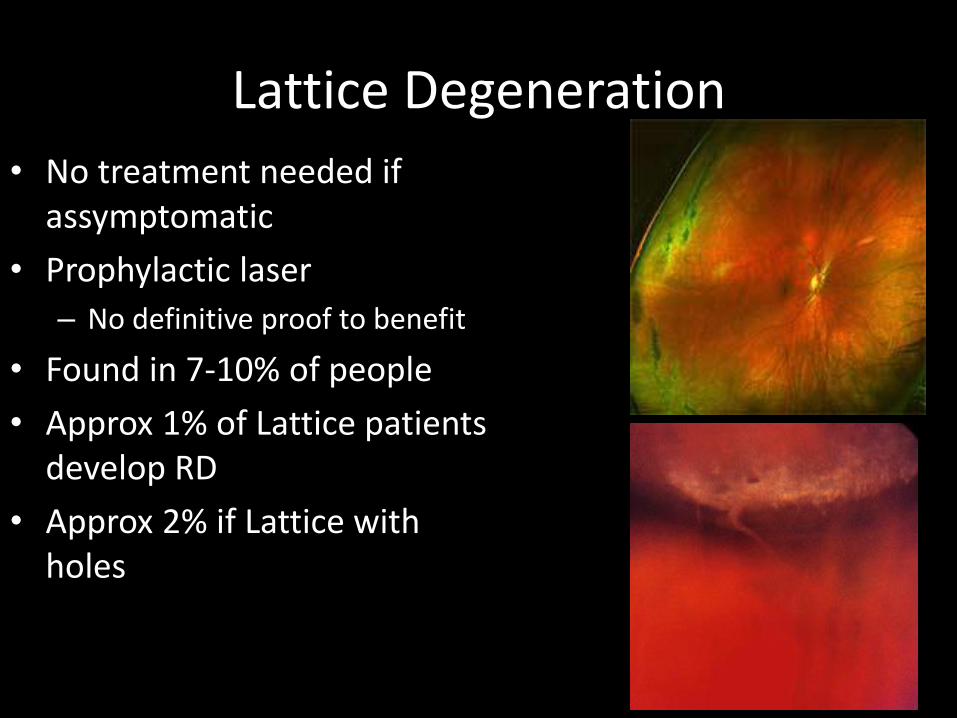
Lattice Degeneration
• No treatment needed if assymptomatic
• Prophylactic laser
– No definitive proof to benefit
• Found in 7-10% of people
• Approx 1% of Lattice patients develop RD
• Approx 2% if Lattice with holes

Why not treat all lattice?
• 20-30% of eyes with RD have Lattice Degen.
• 89% of RD’s from affected eyes occur in areas of normal peripheral retina– So… How can you treat if you don’t know where RD will occur
• Eyes with risk factors don’t seem to have lower incidence of RD if treated– 2-4% of treated eyes still have RD1
• Prophylactic laser did not prevent tear or RD in fellow eyes if no PVD present at time of tx:– 94% still developed tears, 76% developed RD2
“True science teaches us to doubt, and in ignorance to refrain” Claude Bernard
1. Evidence based Prophylactic. Wilkinson C. P. Ophthalmology 1/2000
Editorial by Norman Byer, M.D. in same issue
2. Chauhan et al. Failure of Prophylactic Retinopexy. Arch Ophth. 7/06

Practical approaches to Clinical Nutrition:
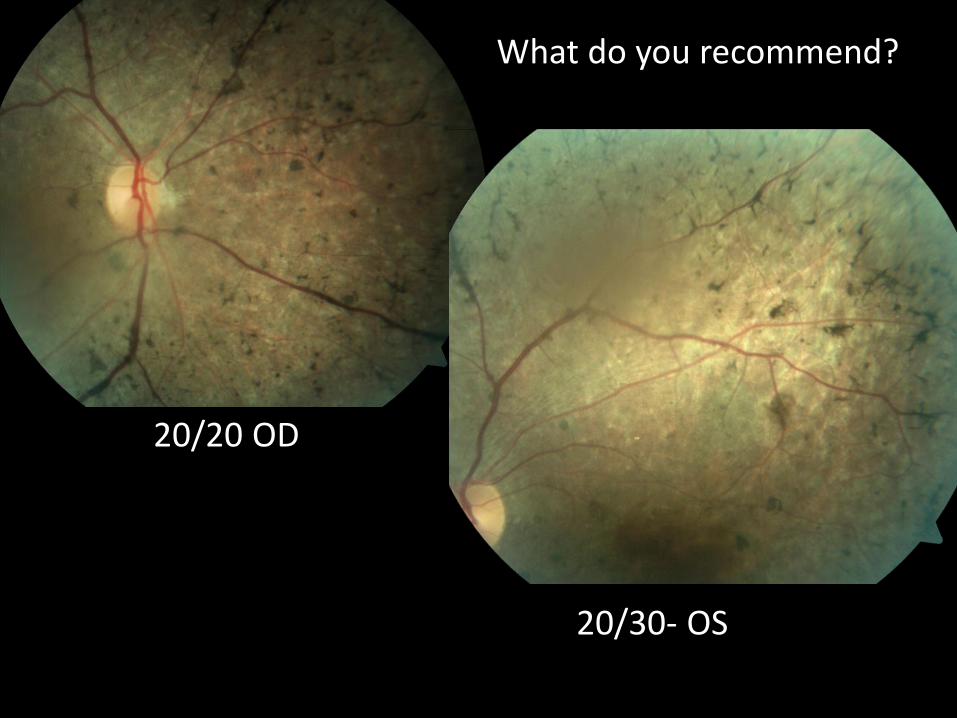
What do you recommend?
20/20 OD
20/30- OS
58 WF• No ocular complaints
• Soc: Previous social smoker…
• FHx: mother has AMD
• Meds: unremarkable
• BCVA: 20/20 OU
• MPOD: 0.24

Nutrition in the Optometric Practice: challenges and obstacles
• “Fringe” medicine?
• “Can’t hurt, might help….and might not”?
• “Downright dangerous”?
• “True Evidence-Based Medicine”?

An example of FRINGE MEDICINEWould this be the next future treatment for wet AMD?
Analysis of 600 cases with exudative central chorioretinopathy (wet AMD) undergoing acupuncture of “Xiangyang” point (index finger pressure) showed
an overall results of cured or improved in 586 cases (97.66%) and unsatisfactory in 14 cases (2.34%) in 7 yrs f/u
Preliminary report from Department of Ophthalmology, The First Hospital, Zhejiang Medical
College Compiled by Ye Linmei
Is vitamin supplementation consider to be Voo-Doo medicine by some Doctors?
The controversy:Does vitamin supplementation really work?
=
=
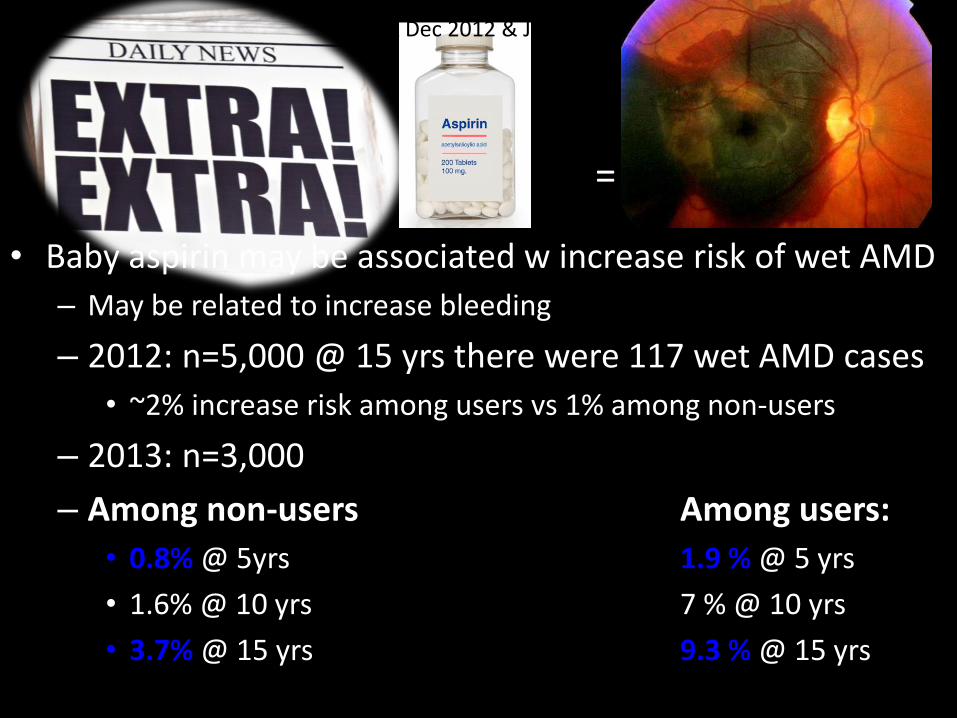
• Baby aspirin may be associated w increase risk of wet AMD
– May be related to increase bleeding
– 2012: n=5,000 @ 15 yrs there were 117 wet AMD cases
• ~2% increase risk among users vs 1% among non-users
– 2013: n=3,000
– Among non-users Among users:
• 0.8% @ 5yrs 1.9 % @ 5 yrs
• 1.6% @ 10 yrs 7 % @ 10 yrs
• 3.7% @ 15 yrs 9.3 % @ 15 yrs
=
JAMA Dec 2012 & Jan 2013

• Other studies stated that the use of ASA had no affect on AMD or may be even protective
• Controversies behind Klein’s study– Show significance but % was relatively small
– Wet AMD is rare; thus any increase is negligible
– Not all risk factors were taken into account
Christen WG. Arch Ophthalmol. 2001Christen WG. Ophthalmology. 2009Wilson HL. Am J Ophthalmol. 2004van Leeuwen R. Ophthalmology. 2004
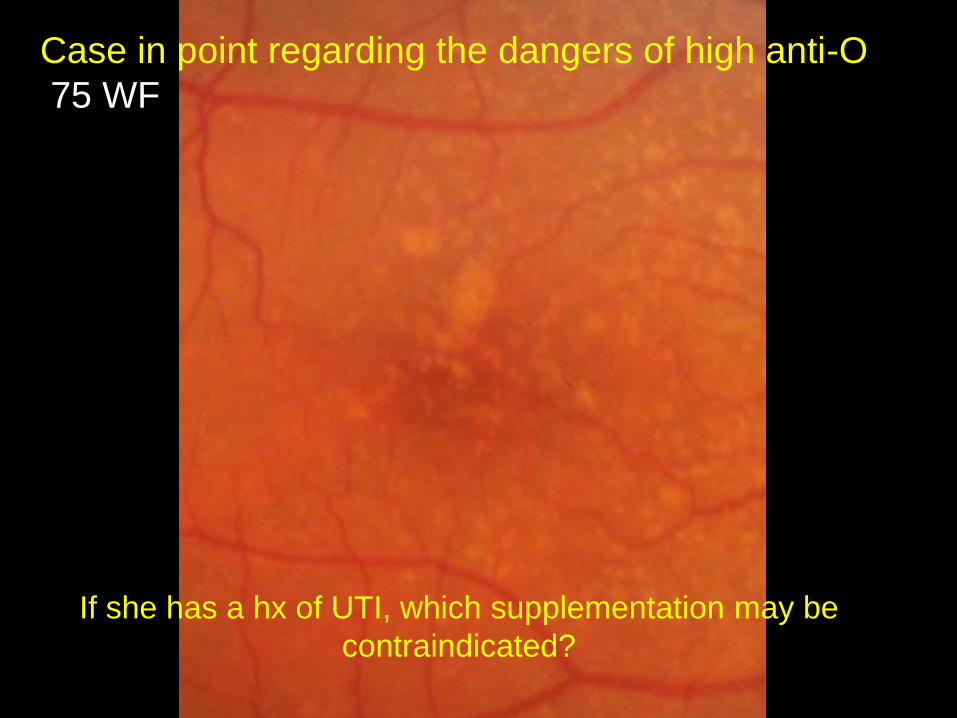
Case in point regarding the dangers of high anti-O
75 WF
If she has a hx of UTI, which supplementation may be
contraindicated?

Benefits according to AREDS 1?Side effects & contraindications according to AREDs 1?
NOTE: AREDS 2 revealed SIMILAR efficacy & safety at HIGH vs LOW dose
Yet, can 80mg of Zn may be TOO much?
Why should you be careful with Coumadin pts?What did meta-analysis revealed?
What was the relationship w mortality rate among AREDS pt taking MV?BOTTOM LINE…

What is the single most important lifestyle
modification to discuss with AMD pts?
• Diet rich in fish• Diet rich in leafy greens• Tighter BP control• Balance meal• Smoking cessation• Taking their MV• Exercise• Maintaining normalhealth BMI
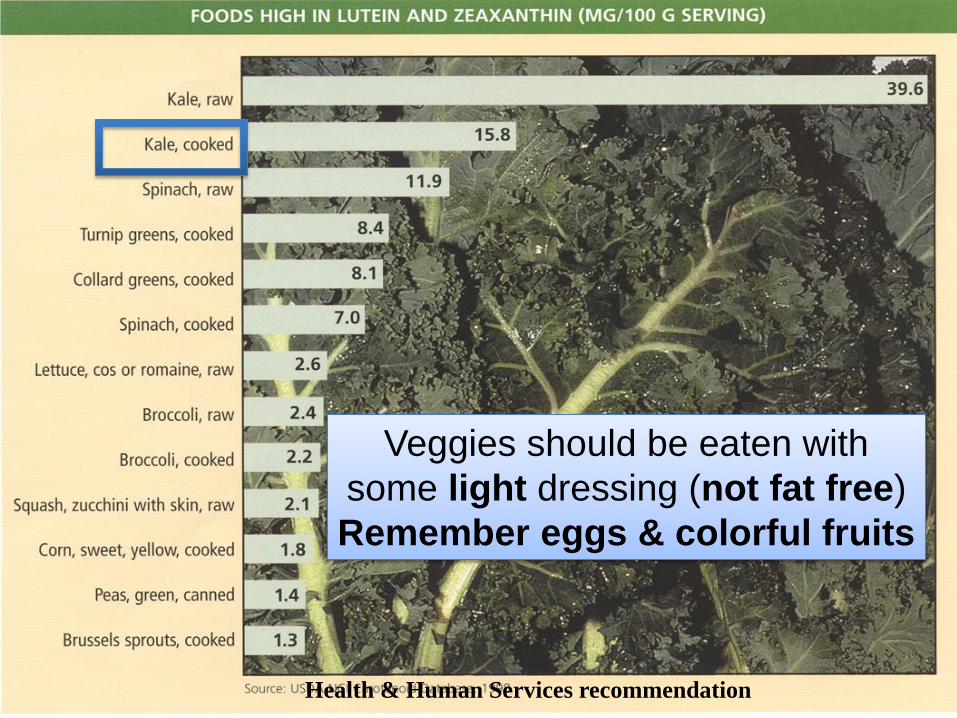
Health & Human Services recommendation
Veggies should be eaten with
some light dressing (not fat free)
Remember eggs & colorful fruits
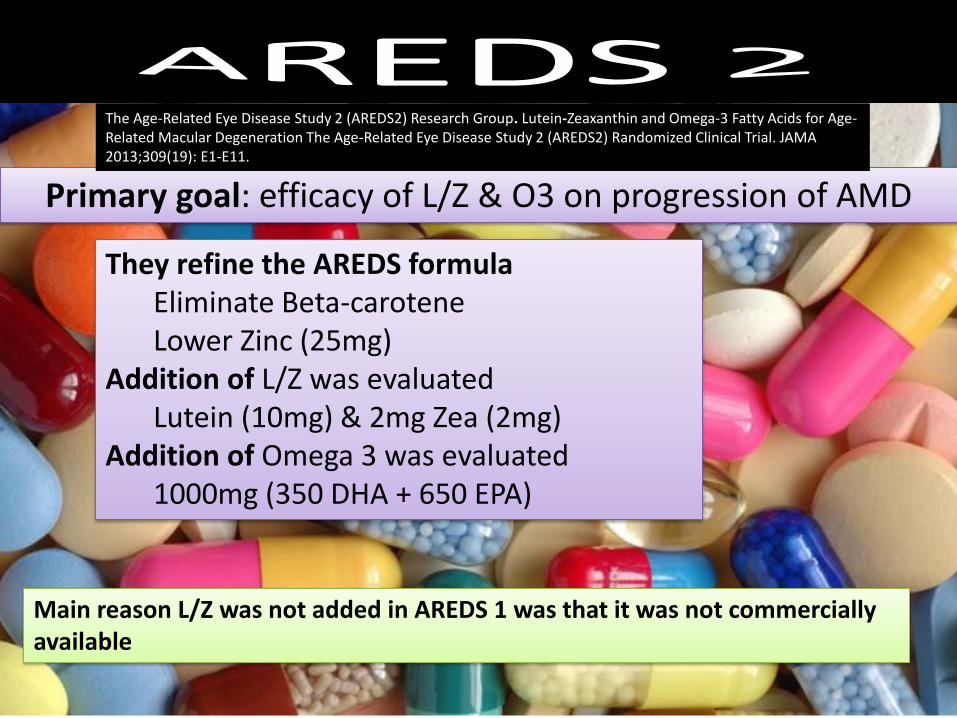
Primary goal: efficacy of L/Z & O3 on progression of AMD
They refine the AREDS formulaEliminate Beta-caroteneLower Zinc (25mg)
Addition of L/Z was evaluatedLutein (10mg) & 2mg Zea (2mg)
Addition of Omega 3 was evaluated1000mg (350 DHA + 650 EPA)
Main reason L/Z was not added in AREDS 1 was that it was not commercially available
The Age-Related Eye Disease Study 2 (AREDS2) Research Group. Lutein-Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration The Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA 2013;309(19): E1-E11.
30%
20%
10%
0%
40%
0Years
1 2 3 4 5
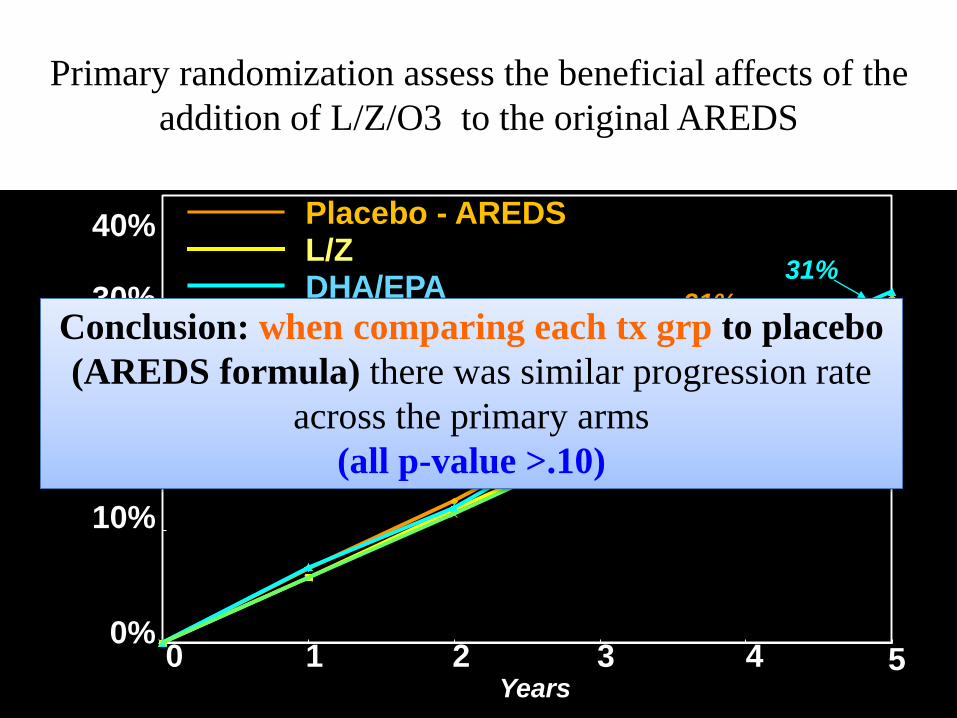
Placebo - AREDS
DHA/EPAL/Z & DHA/EPA
29%
Estimated
Probability
L/Z
30%
31%
31%
Probability of Progression to AAMD
Conclusion: when comparing each tx grp to placebo
(AREDS formula) there was similar progression rate
across the primary arms
(all p-value >.10)
Primary randomization assess the beneficial affects of the
addition of L/Z/O3 to the original AREDS
Evaluating rate towards advanced AMD by 5 years
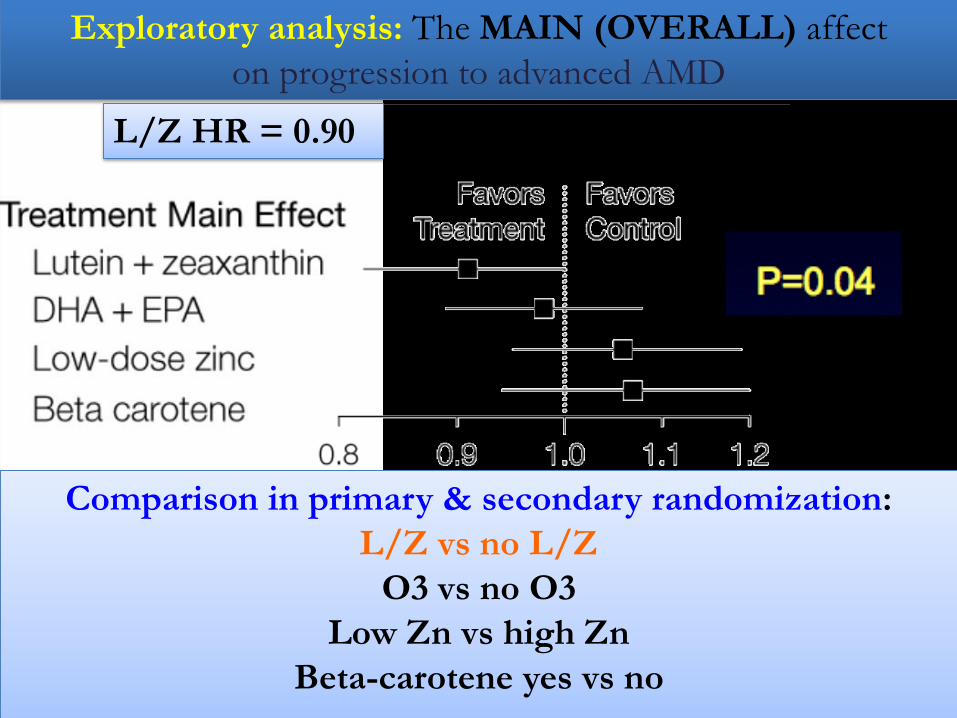
Exploratory analysis: The MAIN (OVERALL) affect
on progression to advanced AMD
L/Z HR = 0.90
Comparison in primary & secondary randomization:
L/Z vs no L/Z
O3 vs no O3
Low Zn vs high Zn
Beta-carotene yes vs no

Which is better
• AREDS1 vs AREDS2

What???
n=1
Vs
n=MANY
What???
n=1
Vs
n=MANY
Dawn of Pharmacogenetics
• Pharmacogenomics is a science that examines the inherited variations in genes that dictate drug response and explores the ways these variations can be used to predict response to treatment
• Is there a difference between pharmacogenomics and pharmacogenetics?
• Pharmacogenetics refers to the study of inherited differences (variation) in drug metabolism and response.
Bottom line:
Genetics
determines resonse
to drugs!
Example:
• What would you recommend for this patient?
Not so fast, don’t
you want to know
genetics?
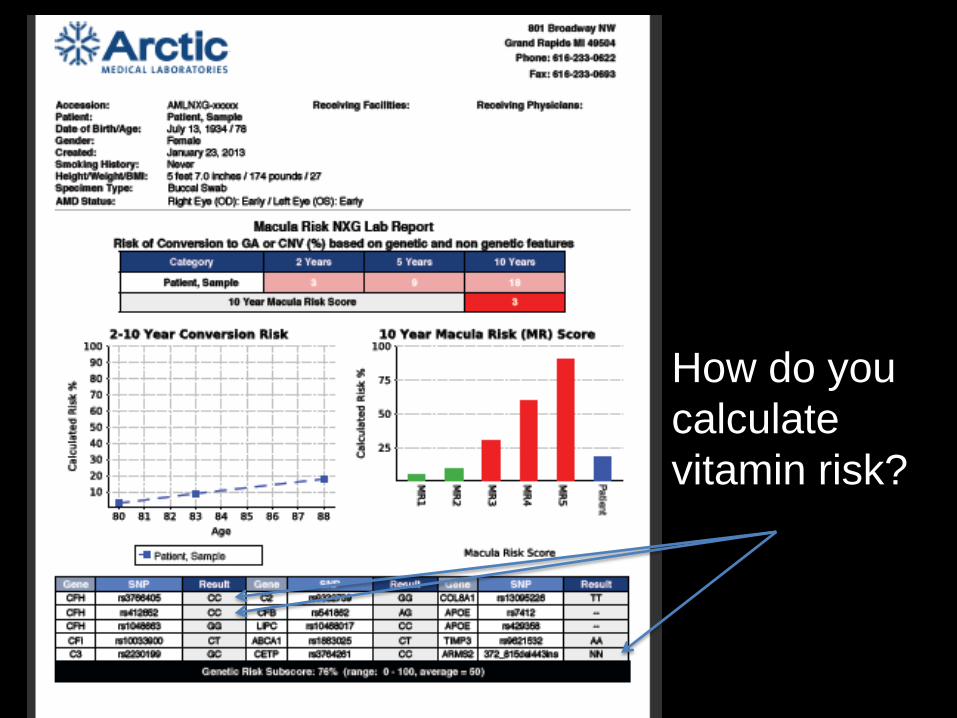
How do you
calculate
vitamin risk?
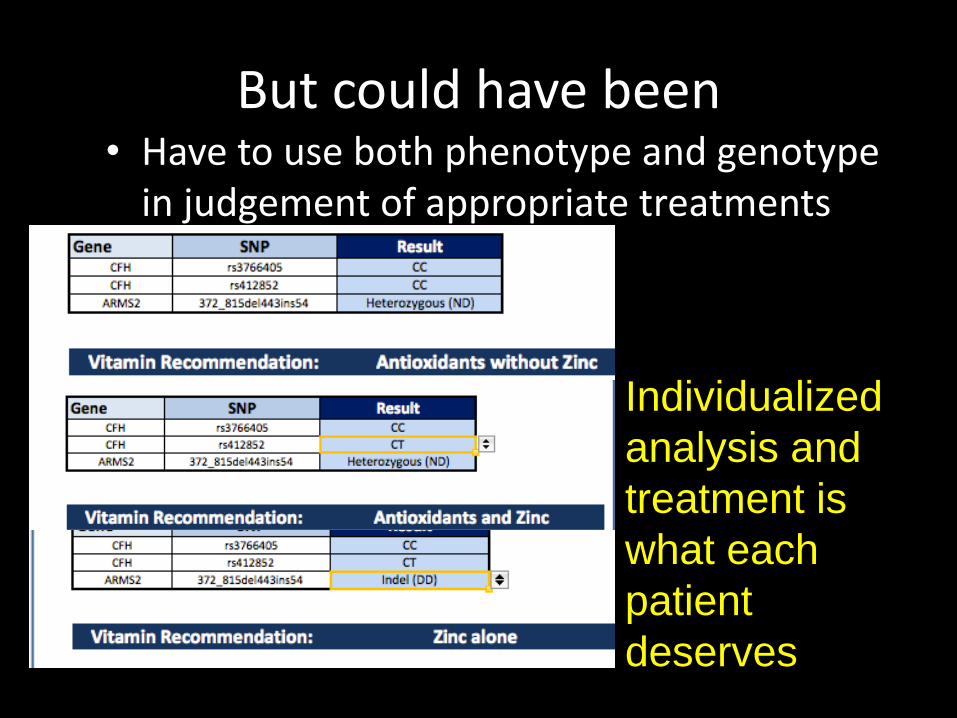
But could have been• Have to use both phenotype and genotype
in judgement of appropriate treatments and f/u
Individualized
analysis and
treatment is
what each
patient
deserves
What is BMI and how is it calculated?
What is the relationship b/t BMI and AMD…How about DM?
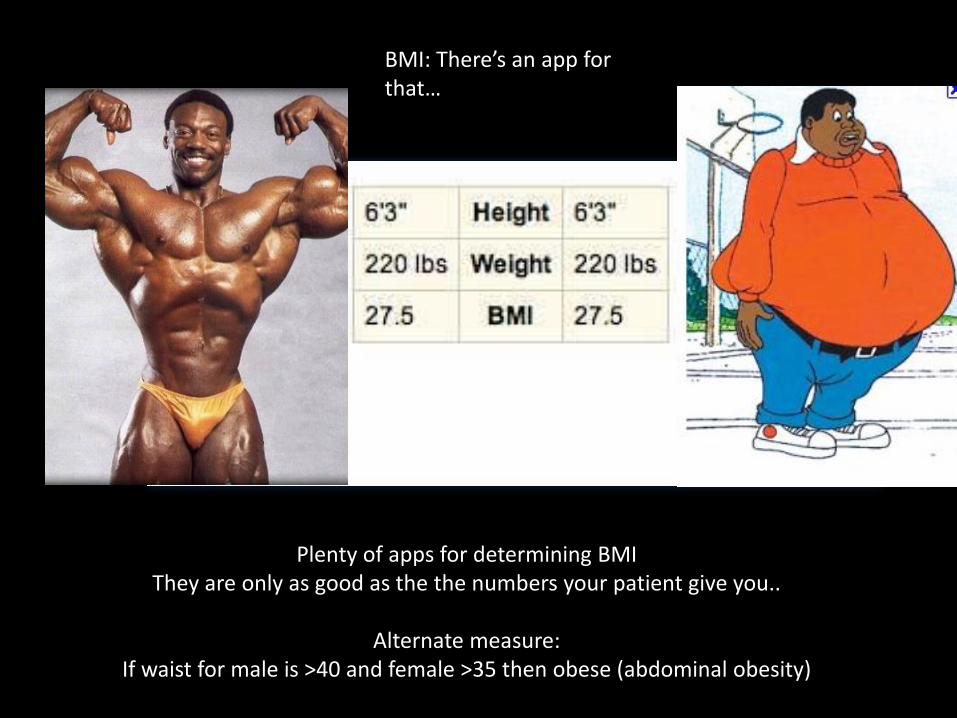
BMI: There’s an app for that…
Plenty of apps for determining BMIThey are only as good as the the numbers your patient give you..
Alternate measure:If waist for male is >40 and female >35 then obese (abdominal obesity)
Exercise – a dirty word Physical Activity is relative to the patient
- small amounts can be very beneficial.
ADA recmd 30min moderate 5x/wk or 20 min vigorous 3x per wk (Sept ‘07)
Each Mile You Walk Increases Life Expectancy by 21 minutes: 5 miles a day = 27 days/year
1 mile = 2,000 steps
2005 American DM Association Meeting
PedometersTake stepsSwim
What does this make you think of with regards to your pts?
What if you just look, can you tell?
Is there a supplement(s) for diabetes?
Is there supplements to prevent or combat diabetic retinopathy?
Is this important in regards to AMD?
What about DM?

Factoid: L/Z make you Smart!
• Xanthophyls (lutein & zeaxanthin) are good for brain health and cognition
• MPOD related to indices that evaluate Processing speed,Accuracy, Completion1
• More L/Z in brain = better cognitive function2
• More AMD and worse VA = worse cognitive function3
• More green veges associated w less cognitive decline w age4
1. Renzi LM et al. FASEB J 22 (abstract 877.5), 2008 2. Miller LS et al. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 17:575-90, 2010. 3. Arch Ophth. 2006 124(4):537-43, 2006 4. Kang, et al. Ann Neurol57:713-720, 2005

The best source of nutrients…
Sorting through it all
• There are SO many different formulations
• Some are found in stores and others in professional offices only
• Beware of formulations and claims
• Multivitamins vs single vitamins vs eye formulations
An ounce of prevention is worth a pound of cure!!
A pound of prevention may be worth the same pound of cure!
Reality….

Controversy: are all sources equivalent
Fish body oil
Fish oil
ALA (alpha-linolenic acid)Short chain FA Primarily Flaxseed, nuts & canola oil
Krill

Not the right way to Rx neutraceuticals
Do you have a favorite or 2??
• Somebody worried with or without family history.
• Somebody with mild dry AMD
• Somebody with advanced dry AMD
• Somebody with Wet AMD
Personalized Medicine
• Each of your patients is an individual with their own potential needs
– “This is the beginning of the end of worshiping at the altar of the large randomized placebo-controlled clinical trial. It introduces the era of personalized medicine based on, among other findings, genetic profile. “ Leo Semes, O.D., F.A.A.O.