from the rsna refresher courses: imaging evaluation for acute
TRANSCRIPT

REFRESHER COURSE 1117
From the RSNARefresher CoursesImaging Evaluation for Acute Pain inthe Right Upper Quadrant1
CME FEATURE
See thequestionnaire onpp 1211–1217.
LEARNINGOBJECTIVESFOR TEST 5After reading thisarticle and takingthe test, the reader
will be able to:
� Discuss the valueof US in assessmentof acute pain in theright upper quadrant.
� Identify the imag-ing features of acutecholecystitis and itscomplications.
� Describe additionalpathologic conditionsthat can cause acutepain in the right up-per quadrant whenthe gallbladder isnormal.
Anthony E. Hanbidge, MB, BCh, FRCPC ● Philip M. Buckler, MDMartin E. O’Malley, MD, FRCPC ● Stephanie R. Wilson, MD, FRCPC
Acute cholecystitis is the most common cause of acute pain in the rightupper quadrant (RUQ), and urgent surgical removal of the gallbladderis the treatment of choice for uncomplicated disease. However, cross-sectional imaging is essential because more than one-third of patientswith acute RUQ pain do not have acute cholecystitis. In addition, pa-tients with complications of acute cholecystitis, such as perforation, areoften best treated with supportive measures initially and elective chole-cystectomy at a later date. Ultrasound (US) is the primary imaging mo-dality for assessment of acute RUQ pain; US is both sensitive and spe-cific in demonstrating gallstones, biliary dilatation, and features thatsuggest acute inflammatory disease. Occasionally, additional imagingmodalities are indicated. Computed tomography is valuable, especiallyfor confirming the extent and nature of the complications of acute cho-lecystitis. Magnetic resonance cholangiopancreatography is helpful incomplicated ductal disease (eg, recurrent pyogenic cholangiohepatitis)when more detailed diagnostic information is required for treatmentplanning, whereas endoscopic retrograde cholangiopancreatography isused when biliary intervention is required (eg, treatment of choled-ocholithiasis). Successful imaging with all modalities requires famil-iarity with both the characteristic and the unusual features of a widevariety of pathologic conditions. In addition, potential pitfalls must berecognized and avoided.©RSNA, 2004
Abbreviation: ERCP � endoscopic retrograde cholangiopancreatography
Index terms: Aneurysm, hepatic, 952.73 ● Bile ducts, calculi, 76.288 ● Bile ducts, hemorrhage, 76.288 ● Cholangitis, 76.288 ● Cholecystitis, 762.285Fistula, biliary, 762.284 ● Gallbladder, perforation, 762.285 ● Liver, abscess, 761.21 ● Liver neoplasms, diagnosis, 761.319, 761.321
RadioGraphics 2004; 24:1117–1135 ● Published online 10.1148/rg.244035149 ● Content Codes:
1From the Department of Medical Imaging, University Health Network and Mount Sinai Hospital, University of Toronto, Ontario, Canada. Pre-sented as a refresher course at the 2002 RSNA scientific assembly. Received June 13, 2003; revision requested July 14 and received September 22; ac-cepted September 23. All authors have no financial relationships to disclose. Address correspondence to A.E.H., Department of Medical Imaging,Toronto General Hospital, NCSB 1C-571, 585 University Ave, Toronto, ON, Canada M5G 2N2 (e-mail: [email protected]).
©RSNA, 2004
Radio
Gra
phic
s

IntroductionPatients presenting to the emergency departmentwith abdominal pain localized to the right upperquadrant constitute a recognized patient populationin whom acute cholecystitis is a prime diagnosticconsideration. Although hepatobiliary disease ingeneral and acute cholecystitis in particular may bethe explanation for the patient’s symptoms, theclinical picture is often confusing and imaging isgenerally indicated early in an effort to reach a spe-cific diagnosis. The primary treatment of acute cho-lecystitis is laparoscopic cholecystectomy. There isevidence that surgery in acute cholecystitis leads tobetter outcomes, and many surgeons prefer earlycholecystectomy. However, more than one-third ofpatients suspected of having acute cholecystitis afterinitial clinical evaluation are ultimately proved tohave a different diagnosis. In one study of 52 pa-tients with acute right upper quadrant pain sus-pected of having acute cholecystitis, the diagnosiswas confirmed in only 34.6%, whereas 32.7% hadchronic cholecystitis and 32.7% had normal gall-bladders (1).
Ultrasound (US) is the primary imaging mo-dality used to evaluate acute right upper quadrantpain. In our experience, it is an accurate, safe,relatively inexpensive, and readily accessible im-aging modality for investigating these patients. Itis highly sensitive and specific for the detection ofgallstones and biliary dilatation. As early as 1982,the accuracy of US (88%) was shown to be simi-lar to that of scintigraphy with hepato-iminodi-acetic acid (HIDA) (85%) in 91 patients sus-pected of having acute cholecystitis (2). In manypractices, US has since replaced scintigraphy forthese patients. Not only will US more easily dem-onstrate complications of acute cholecystitis, suchas gangrenous and emphysematous change, butalso it will frequently demonstrate an alternatediagnosis as the cause of the patient’s symptoms ifthe gallbladder is normal. Finally, scintigraphy istime-consuming, often requiring up to 4 hours fordifferentiation of acute from chronic cholecystitis(3). Many authors therefore suggest that nuclearimaging for the diagnosis of acute cholecystitis bereserved for patients with the rare equivocal sono-gram (1,4,5).
US is also superior to computed tomography(CT) as the initial imaging investigation for assess-ment of biliary disease causing acute right upperquadrant pain. This view is supported by a study byHarvey et al (6) where CT was the initial imagingstudy in 57 patients, and CT findings resulted inunderdiagnosis or misdiagnosis in eight of 11 pa-tients with acute biliary disease. Follow-up US, per-formed within 48 hours of the CT, suggested thecorrect diagnosis and provided additional clinical
information in seven of these eight patients. In addi-tion, US findings resulted in altered clinical man-agement in six of the 11 patients with acute biliarydisease. US was the initial imaging study in 66 pa-tients, and US findings were suggestive of biliarydisease or the correct diagnosis in seven of sevenpatients with acute biliary disease. Follow-up CTwithin 48 hours of the US examination did not re-sult in altered clinical treatment in any of theseseven patients.
Although US is an excellent modality for theinitial evaluation of the patient with acute rightupper quadrant pain and will often suffice to di-rect treatment decisions, there are situationswhere additional imaging may be required. Ingeneral terms, CT is an excellent second choice.It will frequently provide a better overview of thescope and extent of disease where visibility withUS is limited (eg, open wounds, surgical dress-ings, and obesity) and will complement the USfindings in more complex cases. The combinationof US and magnetic resonance (MR) imaging orMR cholangiopancreatography provides excellentpotential for diagnosis of acute biliary ductal dis-ease. On the other hand, endoscopic retrogradecholangiopancreatography (ERCP) with papil-lotomy is the treatment of choice for patientsshown to have choledocholithiasis at US and mayalso be a helpful adjunct to intravenous fluids andantibiotics in treating patients with ascendingcholangitis shown to have biliary dilatation at US.
The spectrum of diseases that may manifest asacute right upper quadrant pain includes acute cho-lecystitis and its complications, gangrene and perfo-ration; gallbladder torsion; mimics of acute chole-cystitis; choledocholithiasis; biliary colic caused byhemobilia; hepatic artery aneurysm; ascendingcholangitis; liver abscess; recurrent pyogeniccholangiohepatitis; and complications of livermasses, such as rupture and hemorrhage. The op-erator must be familiar with the characteristic andunusual appearances of these conditions and mustbe aware of potential pitfalls that can mimic them.
Acute CholecystitisAcute cholecystitis occurs in approximately one-third of patients who have gallstones (7). Ninetypercent to 95% are due to calculous obstructionof the gallbladder neck or cystic duct leading toincreased intraluminal pressure and distention.Inflammation may result from chemical injury ofthe mucosa by bile salts and/or superimposed in-fection. Gallbladder ischemia and transmural ne-crosis may occur if the obstruction persists. Thedifferential diagnosis for acute cholecystitis is ex-tensive and includes choledocholithiasis, pancre-atitis, peptic ulcer disease, acute hepatitis, liverabscess, liver neoplasm with complication, pneu-monia, and heart disease.
1118 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
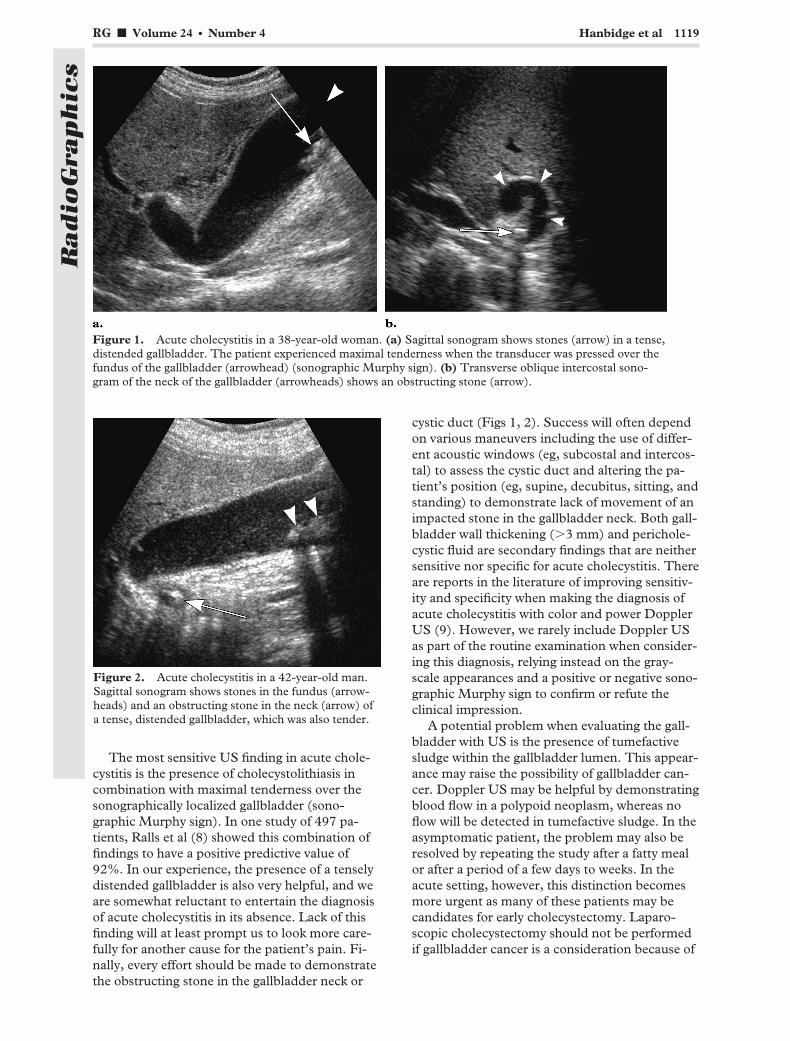
The most sensitive US finding in acute chole-cystitis is the presence of cholecystolithiasis incombination with maximal tenderness over thesonographically localized gallbladder (sono-graphic Murphy sign). In one study of 497 pa-tients, Ralls et al (8) showed this combination offindings to have a positive predictive value of92%. In our experience, the presence of a tenselydistended gallbladder is also very helpful, and weare somewhat reluctant to entertain the diagnosisof acute cholecystitis in its absence. Lack of thisfinding will at least prompt us to look more care-fully for another cause for the patient’s pain. Fi-nally, every effort should be made to demonstratethe obstructing stone in the gallbladder neck or
cystic duct (Figs 1, 2). Success will often dependon various maneuvers including the use of differ-ent acoustic windows (eg, subcostal and intercos-tal) to assess the cystic duct and altering the pa-tient’s position (eg, supine, decubitus, sitting, andstanding) to demonstrate lack of movement of animpacted stone in the gallbladder neck. Both gall-bladder wall thickening (�3 mm) and perichole-cystic fluid are secondary findings that are neithersensitive nor specific for acute cholecystitis. Thereare reports in the literature of improving sensitiv-ity and specificity when making the diagnosis ofacute cholecystitis with color and power DopplerUS (9). However, we rarely include Doppler USas part of the routine examination when consider-ing this diagnosis, relying instead on the gray-scale appearances and a positive or negative sono-graphic Murphy sign to confirm or refute theclinical impression.
A potential problem when evaluating the gall-bladder with US is the presence of tumefactivesludge within the gallbladder lumen. This appear-ance may raise the possibility of gallbladder can-cer. Doppler US may be helpful by demonstratingblood flow in a polypoid neoplasm, whereas noflow will be detected in tumefactive sludge. In theasymptomatic patient, the problem may also beresolved by repeating the study after a fatty mealor after a period of a few days to weeks. In theacute setting, however, this distinction becomesmore urgent as many of these patients may becandidates for early cholecystectomy. Laparo-scopic cholecystectomy should not be performedif gallbladder cancer is a consideration because of
Figure 1. Acute cholecystitis in a 38-year-old woman. (a) Sagittal sonogram shows stones (arrow) in a tense,distended gallbladder. The patient experienced maximal tenderness when the transducer was pressed over thefundus of the gallbladder (arrowhead) (sonographic Murphy sign). (b) Transverse oblique intercostal sono-gram of the neck of the gallbladder (arrowheads) shows an obstructing stone (arrow).
Figure 2. Acute cholecystitis in a 42-year-old man.Sagittal sonogram shows stones in the fundus (arrow-heads) and an obstructing stone in the neck (arrow) ofa tense, distended gallbladder, which was also tender.
RG f Volume 24 ● Number 4 Hanbidge et al 1119
Radio
Gra
phic
s
the high recurrence rates (Fig 3). Open cholecys-tectomy should be performed in this situationwith consideration given to resection of segmentsV and IVB of the liver. Additional imaging withtriphasic CT can therefore be helpful (Fig 4). Theabsence of an enhancing mass at CT suggests thatgallbladder cancer is not present.
Acalculous cholecystitis accounts for 5%–10% ofall cases of acute cholecystitis and occurs most com-monly in patients in the intensive care unit. Predis-posing factors include trauma, mechanical ventila-tion, hyperalimentation, the postoperative state,
diabetes mellitus, vascular insufficiency, prolongedfasting, burns, and the postpartum state. Theseconditions share the propensity to produce gallblad-der ischemia. Acalculous cholecystitis carries highmorbidity and mortality rates partly because of diffi-culty and delay in making the diagnosis. These pa-tients are challenging to assess clinically, and thesonographic features are nonspecific. Scintigraphyhas the propensity to give false-positive results inthis patient population. As a result, image-guidedcholecystostomy tube placement is therefore oftenperformed to decompress the gallbladder if there isa high index of suspicion and the gallbladder is dis-tended at US.
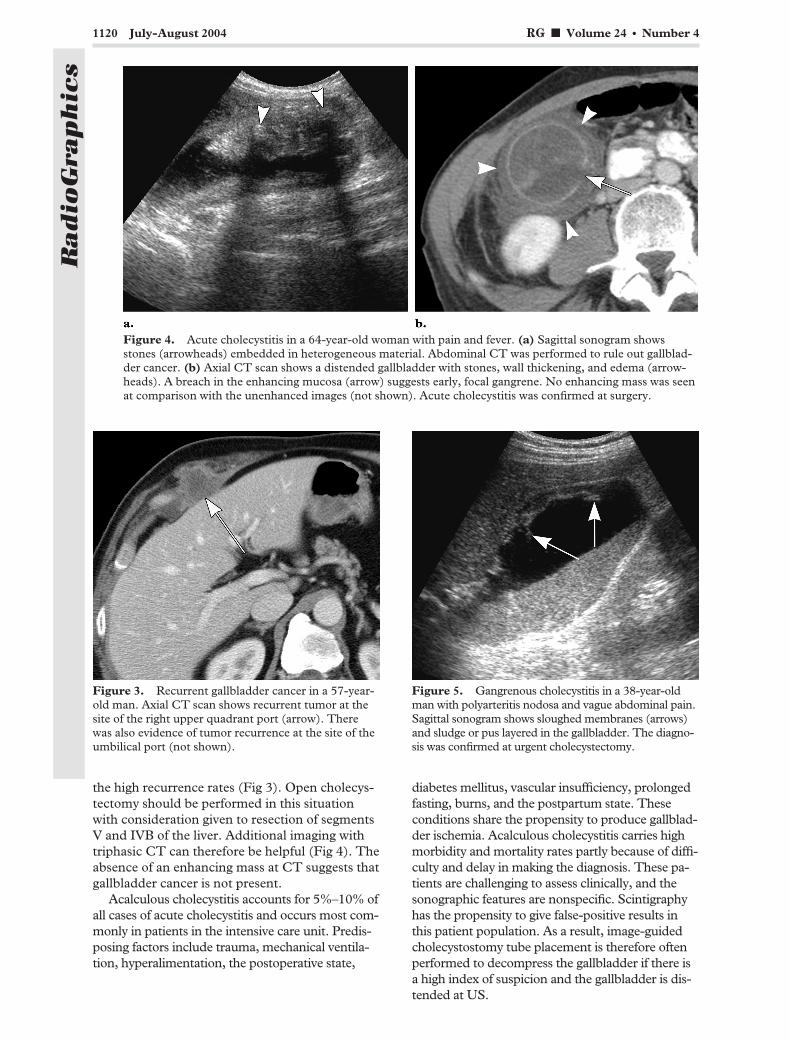
Figure 3. Recurrent gallbladder cancer in a 57-year-old man. Axial CT scan shows recurrent tumor at thesite of the right upper quadrant port (arrow). Therewas also evidence of tumor recurrence at the site of theumbilical port (not shown).
Figure 4. Acute cholecystitis in a 64-year-old woman with pain and fever. (a) Sagittal sonogram showsstones (arrowheads) embedded in heterogeneous material. Abdominal CT was performed to rule out gallblad-der cancer. (b) Axial CT scan shows a distended gallbladder with stones, wall thickening, and edema (arrow-heads). A breach in the enhancing mucosa (arrow) suggests early, focal gangrene. No enhancing mass was seenat comparison with the unenhanced images (not shown). Acute cholecystitis was confirmed at surgery.
Figure 5. Gangrenous cholecystitis in a 38-year-oldman with polyarteritis nodosa and vague abdominal pain.Sagittal sonogram shows sloughed membranes (arrows)and sludge or pus layered in the gallbladder. The diagno-sis was confirmed at urgent cholecystectomy.
1120 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
Complications of Acute Cholecystitis
Gangrenous CholecystitisIncreased intraluminal pressure may producegallbladder wall ischemia and ultimately necrosis,resulting in gangrenous cholecystitis. It compli-cates acute cholecystitis in 2%–38% of cases (10).Perforation is more common than in uncompli-cated cholecystitis, leading to increased morbidityand mortality. As the gallbladder necroses, clini-cal symptoms and signs may become more gener-alized. The abdominal pain may be diffuse in upto 50% of patients (11) possibly because of moregeneralized peritonitis with inflammation of theparietal peritoneum.
In the symptomatic patient, the presence ofasymmetric gallbladder wall thickening or intralu-
minal membranes should be viewed with suspi-cion for gangrenous change (Fig 5). The sono-graphic Murphy sign may be negative in up to66% of cases (11), probably because of dener-vation of the gallbladder wall by gangrenouschanges. At CT, findings with the highest speci-ficity for gangrenous cholecystitis are gas in thewall or lumen (100%), intraluminal membranes(99.5%), irregular or absent wall (97.6%), andabscess (96.6%) (12). Because of the increasedrisk of perforation (up to 10%) (10), early chole-cystectomy should be performed if gangrenouscholecystitis is likely.
Emphysematous CholecystitisEmphysematous cholecystitis is a rare conditionassociated with the presence of gas-forming bac-teria in the gallbladder wall and lumen. Cholecys-tolithiasis is often absent. It is more common inmen than women (7:3) (13), and 40% of the pa-tients are diabetic. There is a fivefold increasedrisk of gangrene and perforation. Emphysematouscholecystitis is a surgical emergency and is treateddefinitively with cholecystectomy. Percutaneouscholecystostomy may be used as a temporizingprocedure in critically ill patients.
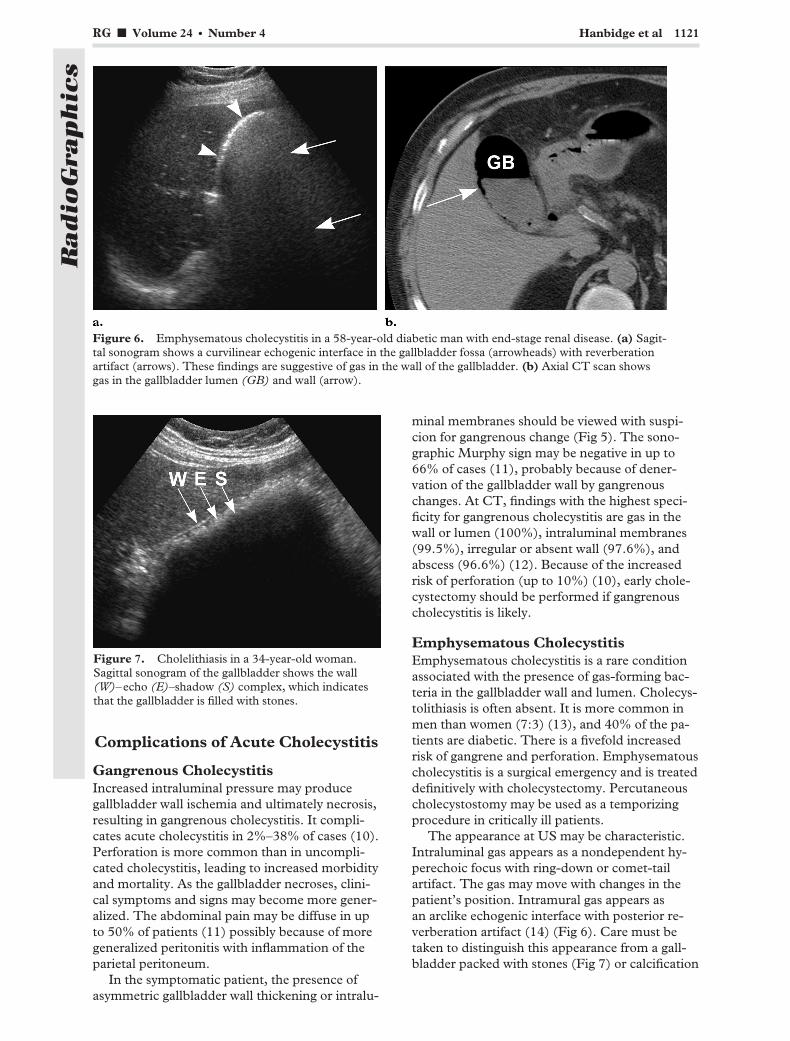
The appearance at US may be characteristic.Intraluminal gas appears as a nondependent hy-perechoic focus with ring-down or comet-tailartifact. The gas may move with changes in thepatient’s position. Intramural gas appears asan arclike echogenic interface with posterior re-verberation artifact (14) (Fig 6). Care must betaken to distinguish this appearance from a gall-bladder packed with stones (Fig 7) or calcification
Figure 6. Emphysematous cholecystitis in a 58-year-old diabetic man with end-stage renal disease. (a) Sagit-tal sonogram shows a curvilinear echogenic interface in the gallbladder fossa (arrowheads) with reverberationartifact (arrows). These findings are suggestive of gas in the wall of the gallbladder. (b) Axial CT scan showsgas in the gallbladder lumen (GB) and wall (arrow).
Figure 7. Cholelithiasis in a 34-year-old woman.Sagittal sonogram of the gallbladder shows the wall(W)–echo (E)–shadow (S) complex, which indicatesthat the gallbladder is filled with stones.
RG f Volume 24 ● Number 4 Hanbidge et al 1121
Radio
Gra
phic
s

in the gallbladder wall (porcelain gallbladder). Indifficult cases, CT is most sensitive for confirminggas in the gallbladder wall or lumen (15). It alsoallows distinction between gas and wall calcifica-
tion, as is seen with porcelain gallbladder. CTshould also be performed in patients with acuteright upper quadrant pain in whom the gallblad-der is not definitely identified at sonography be-cause a gas-filled gallbladder may be mistaken forgas-filled bowel with dire consequences.
Figure 8. Subacute gallbladder perforation in a 72-year-old man. (a) Sagittal sonogram shows a large stone(arrowhead) in the neck of a decompressed gallbladder (GB). There is evidence of a heterogeneous mass in theliver (?). (b) Sagittal sonogram of the liver shows the mass (A), which is complex, located in segment V, andsuggestive of an abscess. (c) Sagittal sonogram obtained in a different plane than in a shows a breach in thegallbladder wall (arrow), which leads into the abscess. (d) Axial CT scan of the abdomen shows the large defect(arrowhead) in the gallbladder (GB) wall. The pericholecystic extent of the abscess is also seen.
1122 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
Gallbladder PerforationGallbladder perforation is a serious complication ofacute cholecystitis and may occur in up to 10% ofcases. There is an associated mortality rate of 19%–24%. Early detection reduces morbidity and mor-tality. There are three categories of gallbladder per-foration as classified by Niemeier (16): acute, sub-acute, and chronic. Acute perforation results ingeneralized peritonitis and has the worst prognosis.Subacute perforation is generally contained, result-ing in pericholecystic abscess. Chronic perforationmay result in an internal biliary fistula, often to theduodenum or common bile duct. Most perforationsare subacute, accounting for 60% of all cases.Chronic perforation accounts for 30%, and acuteperforation accounts for 10%.
Both US and CT are comparable in their abil-ity to show the defect in the gallbladder wall (Fig8). In one study of 23 patients, US helped diag-nose the defect in the gallbladder wall in 16(70%). Eighteen patients in this series underwent
both US and CT, with US demonstrating the de-fect in 11 of these cases (61%) and CT demon-strating the defect in 14 (78%). This differencedid not reach statistical significance (17).
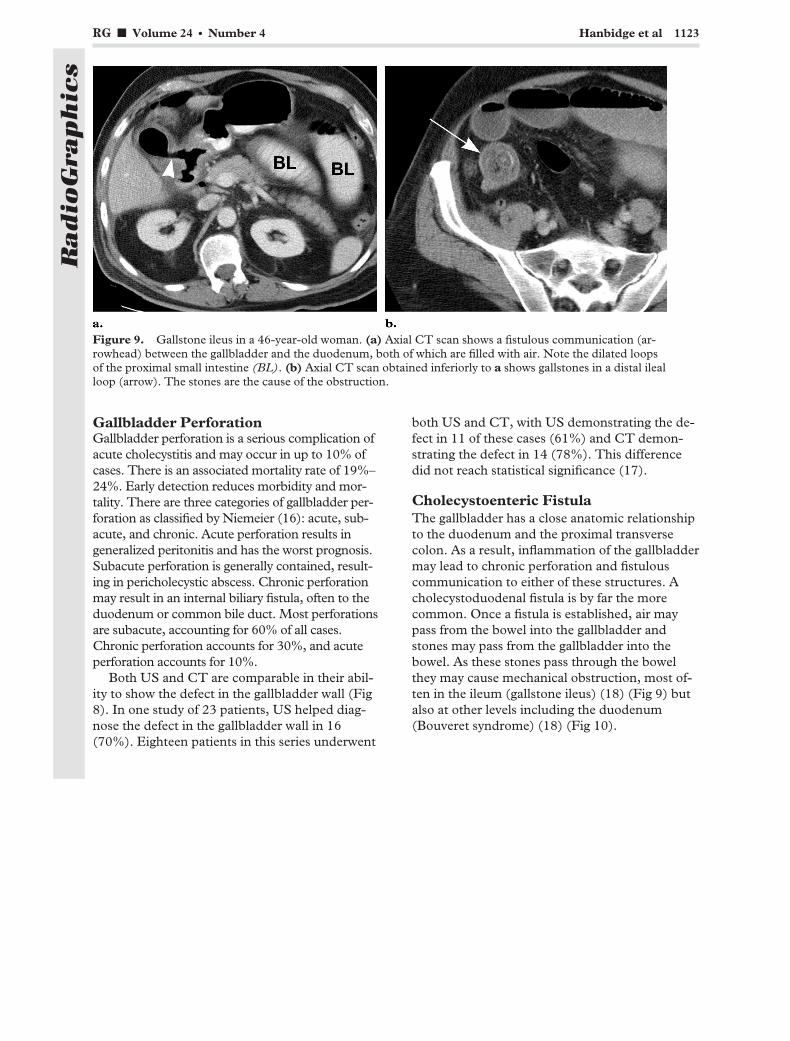
Cholecystoenteric FistulaThe gallbladder has a close anatomic relationshipto the duodenum and the proximal transversecolon. As a result, inflammation of the gallbladdermay lead to chronic perforation and fistulouscommunication to either of these structures. Acholecystoduodenal fistula is by far the morecommon. Once a fistula is established, air maypass from the bowel into the gallbladder andstones may pass from the gallbladder into thebowel. As these stones pass through the bowelthey may cause mechanical obstruction, most of-ten in the ileum (gallstone ileus) (18) (Fig 9) butalso at other levels including the duodenum(Bouveret syndrome) (18) (Fig 10).
Figure 9. Gallstone ileus in a 46-year-old woman. (a) Axial CT scan shows a fistulous communication (ar-rowhead) between the gallbladder and the duodenum, both of which are filled with air. Note the dilated loopsof the proximal small intestine (BL). (b) Axial CT scan obtained inferiorly to a shows gallstones in a distal ilealloop (arrow). The stones are the cause of the obstruction.
RG f Volume 24 ● Number 4 Hanbidge et al 1123
Radio
Gra
phic
s
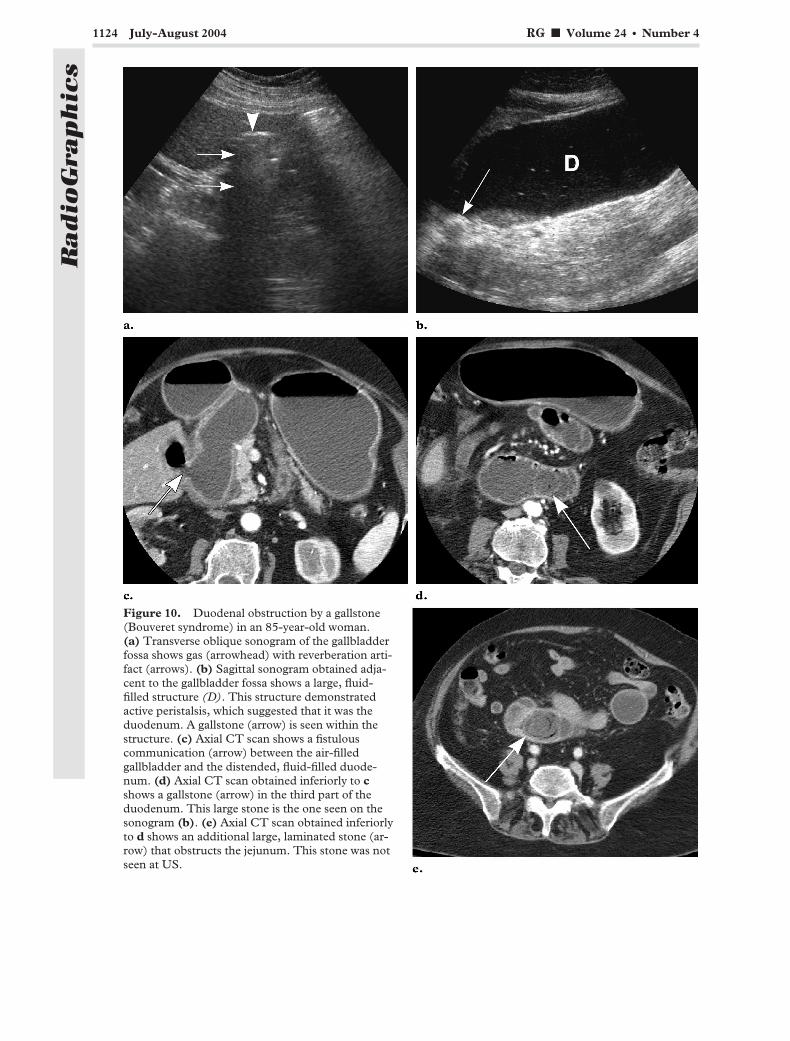
Figure 10. Duodenal obstruction by a gallstone(Bouveret syndrome) in an 85-year-old woman.(a) Transverse oblique sonogram of the gallbladderfossa shows gas (arrowhead) with reverberation arti-fact (arrows). (b) Sagittal sonogram obtained adja-cent to the gallbladder fossa shows a large, fluid-filled structure (D). This structure demonstratedactive peristalsis, which suggested that it was theduodenum. A gallstone (arrow) is seen within thestructure. (c) Axial CT scan shows a fistulouscommunication (arrow) between the air-filledgallbladder and the distended, fluid-filled duode-num. (d) Axial CT scan obtained inferiorly to cshows a gallstone (arrow) in the third part of theduodenum. This large stone is the one seen on thesonogram (b). (e) Axial CT scan obtained inferiorlyto d shows an additional large, laminated stone (ar-row) that obstructs the jejunum. This stone was notseen at US.
1124 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s

There may be difficulty identifying the gall-bladder with US, as it is often air-filled and con-tracted from chronic inflammation. US may showevidence of bowel dilatation and will often dem-onstrate an obstructing stone in the bowel. How-ever, CT will more accurately demonstrate thefistula and the level of bowel obstruction.
Gallbladder TorsionGallbladder torsion is a rare cause of acute abdomi-nal pain with only limited case reports in the litera-ture. It is usually seen in elderly patients, so it maybecome more common as the population ages. Themajority of patients are female (84%). It is mostcommonly acalculous (�67%). Mobility of the gall-bladder because of a long or absent mesentery(“floating gallbladder”) predisposes to torsion,which may be either complete (�180°) or incom-plete (�180°). Complete torsion is likely to result invascular compromise and gangrene of the gallblad-der, whereas incomplete torsion may only obstructthe cystic duct and blood supply to the gallbladderwall may be maintained. A high index of suspicionis required to make this diagnosis preoperatively.US may show a distended, tender gallbladder withan abnormal orientation remote from the gallblad-der fossa (Fig 11). CT and MR imaging may helpconfirm the diagnosis (19) and may show taperingand twisting of the cystic duct.
Mimics of Acute CholecystitisSympathetic thickening of the gallbladder walloccurring secondary to an acute inflammatoryprocess in the right upper quadrant, includingacute pancreatitis, perforated duodenal ulcer,hepatitis, right-sided diverticulitis, and even acuteright-sided pyelonephritis, may cause confusionwhen assessing the gallbladder for acute cholecys-titis (20). Edema of the gallbladder wall from asystemic condition (eg, congestive heart failure,hypoalbuminemia) may also be problematic.
Because many of these diagnoses mimic thepresentation of acute cholecystitis, the diagnosticimager requires a high level of awareness in orderto avoid mistakes (Figs 12–14). Gallstones may ormay not be present. The patient may be tender inthe right upper quadrant; however, an importantpoint is that this tenderness is often remote fromthe sonographically localized gallbladder (Fig 15).We also find lack of tense gallbladder distention auseful “flag” to prompt us to consider an alter-nate diagnosis (Fig 16). Careful assessment of theright upper quadrant may then yield additionalfindings (eg, free air) that facilitate making thecorrect diagnosis.
Figure 11. Incomplete gallbladder torsion in a 94-year-old woman. (a) Sagittal sonogram of the midabdo-men shows a cystic mass (C) with edematous walls anterior to the abdominal aorta (A). (b) Coronal obliquemaximum intensity projection CT scan shows that the mass has a beaked neck (arrow), which extends into thegallbladder fossa.
RG f Volume 24 ● Number 4 Hanbidge et al 1125
Radio
Gra
phic
s
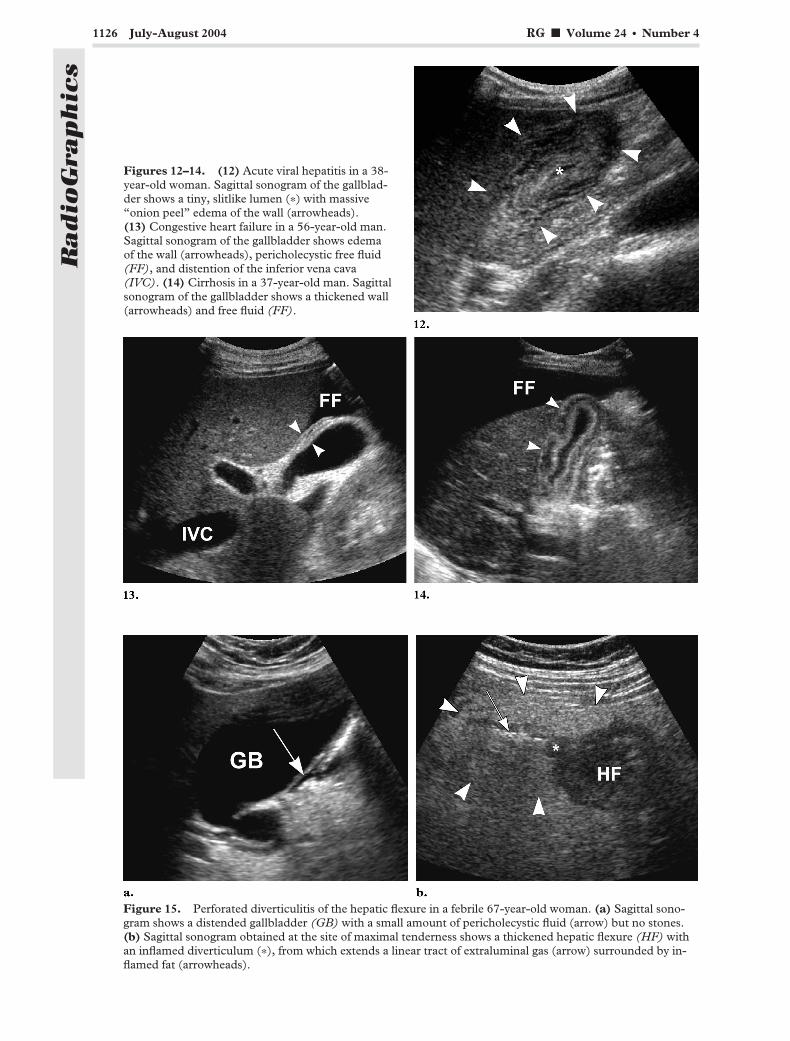
Figures 12–14. (12) Acute viral hepatitis in a 38-year-old woman. Sagittal sonogram of the gallblad-der shows a tiny, slitlike lumen (�) with massive“onion peel” edema of the wall (arrowheads).(13) Congestive heart failure in a 56-year-old man.Sagittal sonogram of the gallbladder shows edemaof the wall (arrowheads), pericholecystic free fluid(FF), and distention of the inferior vena cava(IVC). (14) Cirrhosis in a 37-year-old man. Sagittalsonogram of the gallbladder shows a thickened wall(arrowheads) and free fluid (FF).
Figure 15. Perforated diverticulitis of the hepatic flexure in a febrile 67-year-old woman. (a) Sagittal sono-gram shows a distended gallbladder (GB) with a small amount of pericholecystic fluid (arrow) but no stones.(b) Sagittal sonogram obtained at the site of maximal tenderness shows a thickened hepatic flexure (HF) withan inflamed diverticulum (�), from which extends a linear tract of extraluminal gas (arrow) surrounded by in-flamed fat (arrowheads).
1126 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
It is especially important not to misinterpretgallbladder wall edema secondary to acute hepati-tis as representing acute cholecystitis. Some gen-eral anesthetics, if given to such a patient foremergent cholecystectomy, may have hepatotoxiceffects and can be fatal.
CholedocholithiasisStones in the common bile duct may manifestwith acute right upper quadrant pain and/or jaun-dice. They may also be discovered as a causativefactor in acute pancreatitis or be uncovered inci-dentally at the time of imaging for some otherreason.
US has a sensitivity of 70%–75% for detectionof common bile duct stones (Fig 17). In onestudy, Laing et al (21) found that eight (89%) ofnine proximal and 16 (70%) of 23 distal common
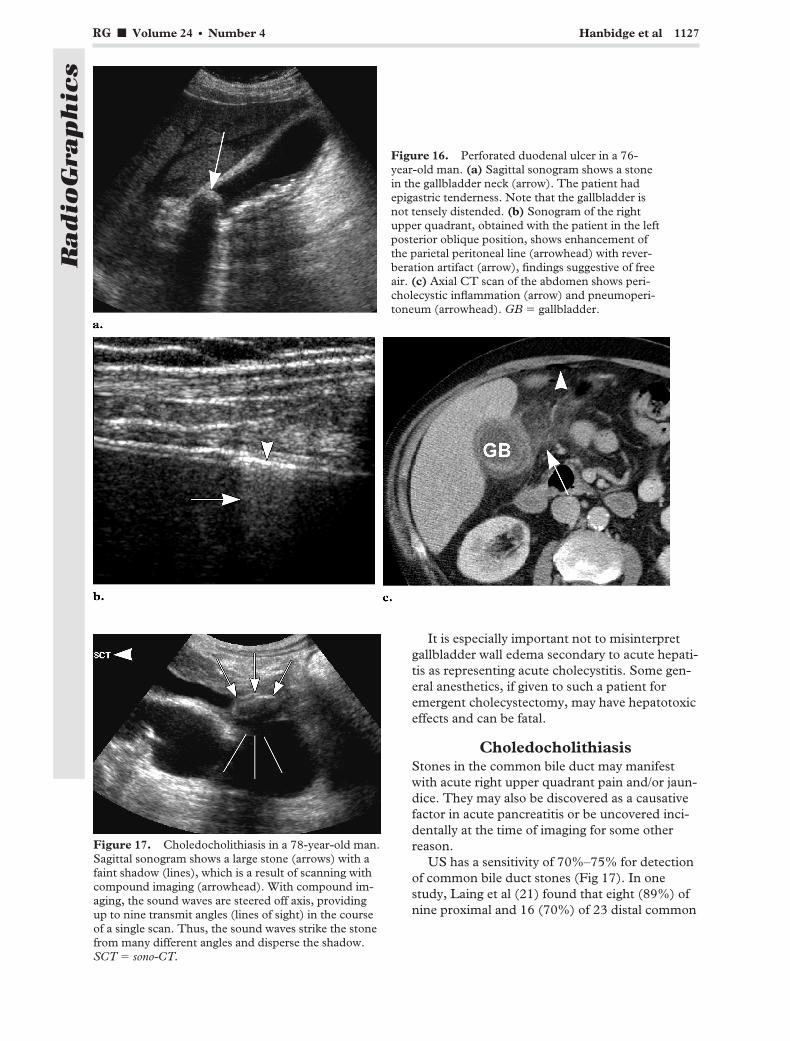
Figure 16. Perforated duodenal ulcer in a 76-year-old man. (a) Sagittal sonogram shows a stonein the gallbladder neck (arrow). The patient hadepigastric tenderness. Note that the gallbladder isnot tensely distended. (b) Sonogram of the rightupper quadrant, obtained with the patient in the leftposterior oblique position, shows enhancement ofthe parietal peritoneal line (arrowhead) with rever-beration artifact (arrow), findings suggestive of freeair. (c) Axial CT scan of the abdomen shows peri-cholecystic inflammation (arrow) and pneumoperi-toneum (arrowhead). GB � gallbladder.
Figure 17. Choledocholithiasis in a 78-year-old man.Sagittal sonogram shows a large stone (arrows) with afaint shadow (lines), which is a result of scanning withcompound imaging (arrowhead). With compound im-aging, the sound waves are steered off axis, providingup to nine transmit angles (lines of sight) in the courseof a single scan. Thus, the sound waves strike the stonefrom many different angles and disperse the shadow.SCT � sono-CT.
RG f Volume 24 ● Number 4 Hanbidge et al 1127
Radio
Gra
phic
s
bile duct stones were visualized with US. Detec-tion of choledocholithiasis can be substantiallyimproved by scanning the proximal and distalcommon bile duct separately. The intrapancreaticportion of the bile duct should be assessed first ina transverse plane with the patient in a semierectright posterior oblique position. The proximalduct is best imaged by obtaining parasagittalscans with the patient in a supine left posterioroblique position (22).
If common bile duct stones are visualized withUS, then the patient should be referred directly toERCP for definitive management (papillotomy).
On the other hand, if choledocholithiasis is sus-pected but cannot be confirmed with US, MRcholangiopancreatography is an excellent choicefor further investigation, with a sensitivity of 95%and specificity of 100% (23) (Fig 18). If immedi-ate access to MR cholangiopancreatography islimited, then CT is an alternative to diagnosticERCP with 80% sensitivity and 100% specificity(24). However, it is mandatory in this scenariothat an unenhanced, thinly collimated seriesthrough the liver and common bile duct be in-cluded in the study to improve detection of stonesand to avoid misinterpretation of a common bileduct stone as an enhancing mass (Fig 19). It isalso advisable in this situation to give water as an
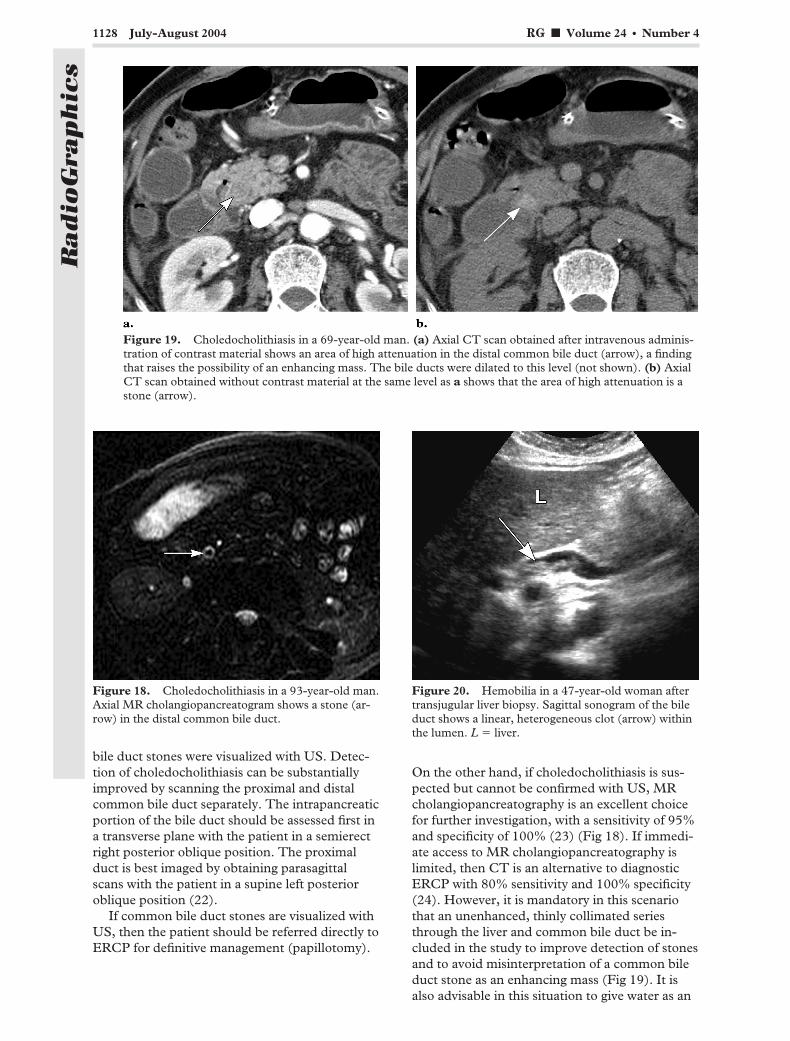
Figure 18. Choledocholithiasis in a 93-year-old man.Axial MR cholangiopancreatogram shows a stone (ar-row) in the distal common bile duct.
Figure 19. Choledocholithiasis in a 69-year-old man. (a) Axial CT scan obtained after intravenous adminis-tration of contrast material shows an area of high attenuation in the distal common bile duct (arrow), a findingthat raises the possibility of an enhancing mass. The bile ducts were dilated to this level (not shown). (b) AxialCT scan obtained without contrast material at the same level as a shows that the area of high attenuation is astone (arrow).
Figure 20. Hemobilia in a 47-year-old woman aftertransjugular liver biopsy. Sagittal sonogram of the bileduct shows a linear, heterogeneous clot (arrow) withinthe lumen. L � liver.
1128 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
oral contrast agent, as positive oral contrastagents may obscure stones in the distal commonbile duct.
HemobiliaThe classical clinical triad for hemobilia consistsof melena, jaundice, and abdominal pain but isseen in less than 50% of patients. Two-thirds ofcases are iatrogenic, whereas trauma accounts for5% (25). It may manifest many weeks after theinitial injury. The diagnosis can be made with US(Fig 20), unenhanced CT (high-attenuation clotwithin the bile ducts), or MR imaging and con-firmed with endoscopy (blood from the ampullaof Vater) or angiography. In one review, 43% of
cases were managed conservatively and 36% weremanaged with transarterial embolization (25).The remainder were managed surgically eitherbecause of failed transarterial embolization or atthe time of laparotomy for other reasons.
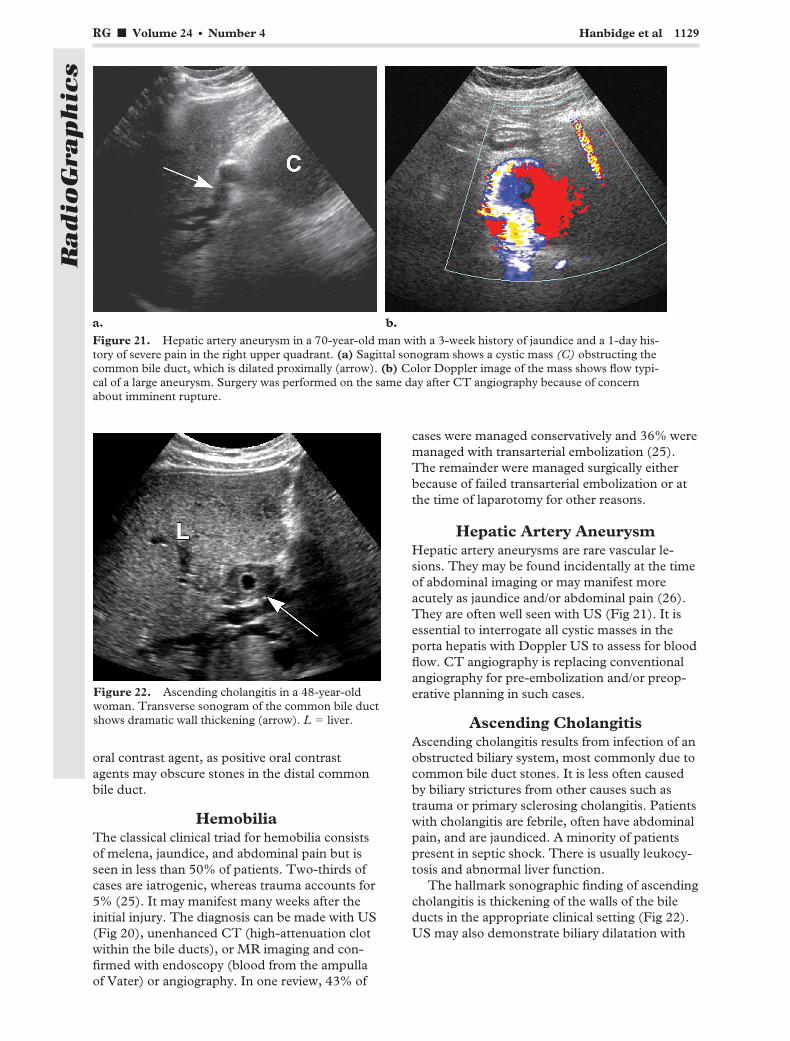
Hepatic Artery AneurysmHepatic artery aneurysms are rare vascular le-sions. They may be found incidentally at the timeof abdominal imaging or may manifest moreacutely as jaundice and/or abdominal pain (26).They are often well seen with US (Fig 21). It isessential to interrogate all cystic masses in theporta hepatis with Doppler US to assess for bloodflow. CT angiography is replacing conventionalangiography for pre-embolization and/or preop-erative planning in such cases.
Ascending CholangitisAscending cholangitis results from infection of anobstructed biliary system, most commonly due tocommon bile duct stones. It is less often causedby biliary strictures from other causes such astrauma or primary sclerosing cholangitis. Patientswith cholangitis are febrile, often have abdominalpain, and are jaundiced. A minority of patientspresent in septic shock. There is usually leukocy-tosis and abnormal liver function.
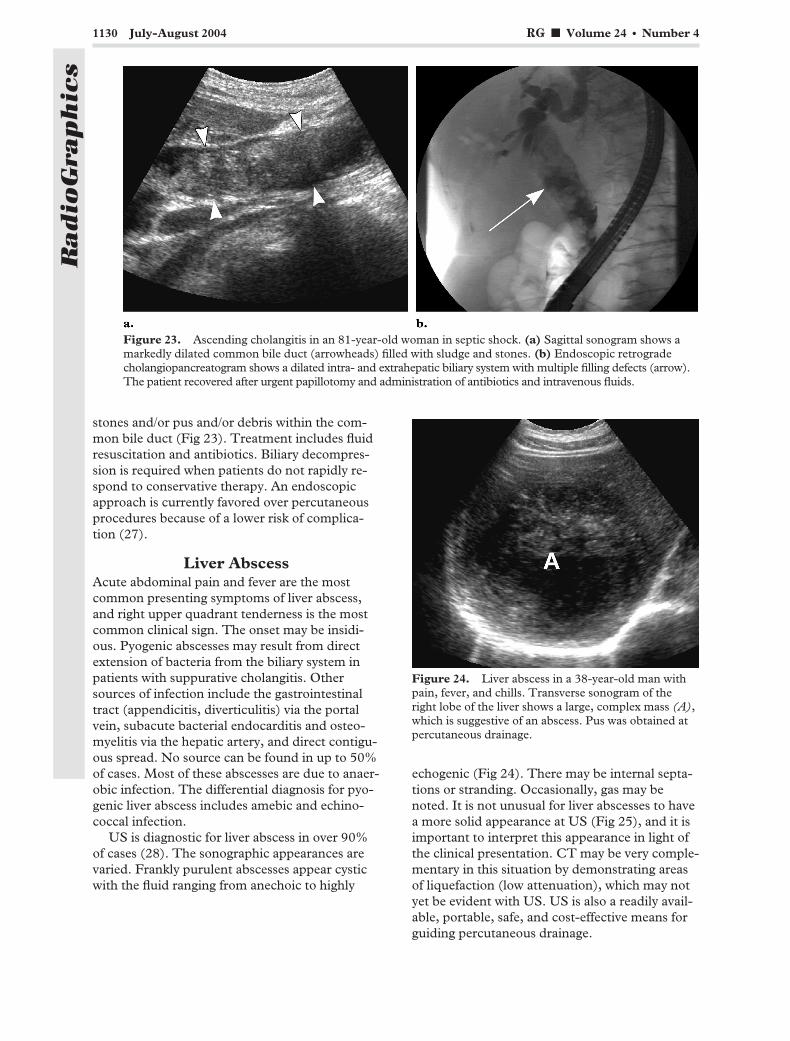
The hallmark sonographic finding of ascendingcholangitis is thickening of the walls of the bileducts in the appropriate clinical setting (Fig 22).US may also demonstrate biliary dilatation with
Figure 21. Hepatic artery aneurysm in a 70-year-old man with a 3-week history of jaundice and a 1-day his-tory of severe pain in the right upper quadrant. (a) Sagittal sonogram shows a cystic mass (C) obstructing thecommon bile duct, which is dilated proximally (arrow). (b) Color Doppler image of the mass shows flow typi-cal of a large aneurysm. Surgery was performed on the same day after CT angiography because of concernabout imminent rupture.
Figure 22. Ascending cholangitis in a 48-year-oldwoman. Transverse sonogram of the common bile ductshows dramatic wall thickening (arrow). L � liver.
RG f Volume 24 ● Number 4 Hanbidge et al 1129
Radio
Gra
phic
s
stones and/or pus and/or debris within the com-mon bile duct (Fig 23). Treatment includes fluidresuscitation and antibiotics. Biliary decompres-sion is required when patients do not rapidly re-spond to conservative therapy. An endoscopicapproach is currently favored over percutaneousprocedures because of a lower risk of complica-tion (27).
Liver AbscessAcute abdominal pain and fever are the mostcommon presenting symptoms of liver abscess,and right upper quadrant tenderness is the mostcommon clinical sign. The onset may be insidi-ous. Pyogenic abscesses may result from directextension of bacteria from the biliary system inpatients with suppurative cholangitis. Othersources of infection include the gastrointestinaltract (appendicitis, diverticulitis) via the portalvein, subacute bacterial endocarditis and osteo-myelitis via the hepatic artery, and direct contigu-ous spread. No source can be found in up to 50%of cases. Most of these abscesses are due to anaer-obic infection. The differential diagnosis for pyo-genic liver abscess includes amebic and echino-coccal infection.
US is diagnostic for liver abscess in over 90%of cases (28). The sonographic appearances arevaried. Frankly purulent abscesses appear cysticwith the fluid ranging from anechoic to highly
echogenic (Fig 24). There may be internal septa-tions or stranding. Occasionally, gas may benoted. It is not unusual for liver abscesses to havea more solid appearance at US (Fig 25), and it isimportant to interpret this appearance in light ofthe clinical presentation. CT may be very comple-mentary in this situation by demonstrating areasof liquefaction (low attenuation), which may notyet be evident with US. US is also a readily avail-able, portable, safe, and cost-effective means forguiding percutaneous drainage.
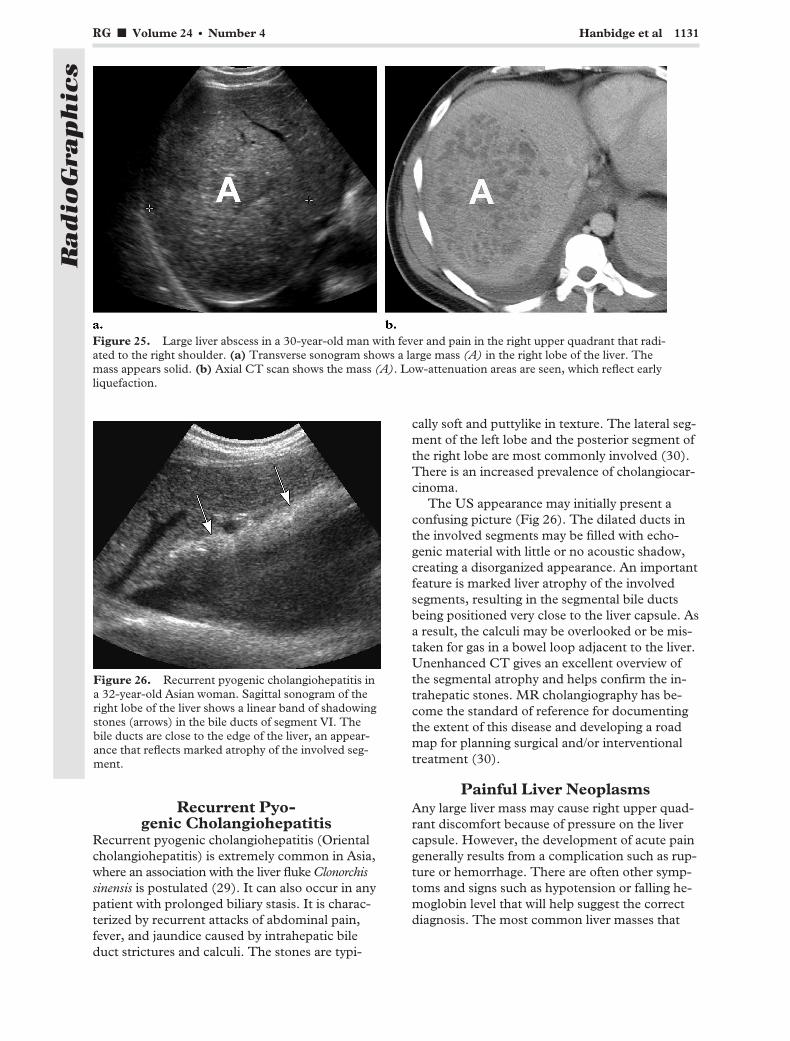
Figure 23. Ascending cholangitis in an 81-year-old woman in septic shock. (a) Sagittal sonogram shows amarkedly dilated common bile duct (arrowheads) filled with sludge and stones. (b) Endoscopic retrogradecholangiopancreatogram shows a dilated intra- and extrahepatic biliary system with multiple filling defects (arrow).The patient recovered after urgent papillotomy and administration of antibiotics and intravenous fluids.
Figure 24. Liver abscess in a 38-year-old man withpain, fever, and chills. Transverse sonogram of theright lobe of the liver shows a large, complex mass (A),which is suggestive of an abscess. Pus was obtained atpercutaneous drainage.
1130 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
Recurrent Pyo-genic Cholangiohepatitis
Recurrent pyogenic cholangiohepatitis (Orientalcholangiohepatitis) is extremely common in Asia,where an association with the liver fluke Clonorchissinensis is postulated (29). It can also occur in anypatient with prolonged biliary stasis. It is charac-terized by recurrent attacks of abdominal pain,fever, and jaundice caused by intrahepatic bileduct strictures and calculi. The stones are typi-
cally soft and puttylike in texture. The lateral seg-ment of the left lobe and the posterior segment ofthe right lobe are most commonly involved (30).There is an increased prevalence of cholangiocar-cinoma.
The US appearance may initially present aconfusing picture (Fig 26). The dilated ducts inthe involved segments may be filled with echo-genic material with little or no acoustic shadow,creating a disorganized appearance. An importantfeature is marked liver atrophy of the involvedsegments, resulting in the segmental bile ductsbeing positioned very close to the liver capsule. Asa result, the calculi may be overlooked or be mis-taken for gas in a bowel loop adjacent to the liver.Unenhanced CT gives an excellent overview ofthe segmental atrophy and helps confirm the in-trahepatic stones. MR cholangiography has be-come the standard of reference for documentingthe extent of this disease and developing a roadmap for planning surgical and/or interventionaltreatment (30).
Painful Liver NeoplasmsAny large liver mass may cause right upper quad-rant discomfort because of pressure on the livercapsule. However, the development of acute paingenerally results from a complication such as rup-ture or hemorrhage. There are often other symp-toms and signs such as hypotension or falling he-moglobin level that will help suggest the correctdiagnosis. The most common liver masses that
Figure 25. Large liver abscess in a 30-year-old man with fever and pain in the right upper quadrant that radi-ated to the right shoulder. (a) Transverse sonogram shows a large mass (A) in the right lobe of the liver. Themass appears solid. (b) Axial CT scan shows the mass (A). Low-attenuation areas are seen, which reflect earlyliquefaction.
Figure 26. Recurrent pyogenic cholangiohepatitis ina 32-year-old Asian woman. Sagittal sonogram of theright lobe of the liver shows a linear band of shadowingstones (arrows) in the bile ducts of segment VI. Thebile ducts are close to the edge of the liver, an appear-ance that reflects marked atrophy of the involved seg-ment.
RG f Volume 24 ● Number 4 Hanbidge et al 1131
Radio
Gra
phic
s

bleed are hepatic adenoma and hepatocellularcarcinoma. Knowledge of the patient profile iscritical for distinguishing between these two pos-sibilities. Other masses that bleed include vascu-lar liver metastases, for example, from renal cellcarcinoma and neuroendocrine tumors.
Hepatic AdenomaHepatic adenomas are rare. They are most com-monly seen in women of reproductive age usingoral contraceptive pills. Men and women takingandrogen-containing steroids are also at increasedrisk, particularly if taking large doses for pro-longed periods. Another high-risk group is pa-tients with type 1 glycogen storage disease, inwhom lesions are more often multiple. Hepaticadenomas may occasionally undergo malignanttransformation (31).
Most patients with adenomas are asymptomatic.However, large and multiple adenomas are moreprone to complication, classically spontaneous rup-ture or hemorrhage. Life-threatening hemorrhage ismore likely if the adenoma is in a subcapsular loca-tion and ruptures into the peritoneal cavity. Thepresence of a heterogeneous liver mass with internalhemorrhage and/or hemoperitoneum is suggestiveof this diagnosis in the correct clinical setting (32)(Fig 27). If rupture is suspected with US, CT withthe inclusion of an unenhanced series is most help-ful for confirmation.
Hepatocellular CarcinomaHepatocellular carcinoma is a very common tu-mor worldwide, and its prevalence is increasing inNorth America. Risk factors include cirrhosis,often due to chronic hepatitis C virus or hepatitis
B virus infection or alcoholism. In persons in-fected with hepatitis B or hepatitis C virus inwhom hepatocellular carcinoma develops, there isa latency period of 1–3 decades. As the preva-lence of alcoholic liver disease is declining, it islikely that the increasing prevalence of hepatocel-lular carcinoma in North America is related tohigh hepatitis C and hepatitis B virus transmis-sion rates in the 1960s and 1970s (33).
It is estimated that spontaneous hemorrhageand/or rupture of hepatocellular carcinoma oc-curs in up to 10% of cases (34). Intraperitonealrupture of hepatocellular carcinoma has a dismalprognosis. US will frequently show a heteroge-neous, vascular liver mass with evidence of cirrho-sis, manifested by a nodular liver and lobar redis-tribution (atrophy of the right lobe and segmentIV with hypertrophy of segments I, II, and III).The presence of an echogenic “rind” around theliver at US is suggestive of acute hemoperitoneum(Fig 28). Triphasic CT may add additional infor-mation for preoperative planning if the patient isin stable condition. In addition, high-attenuationfree fluid in the peritoneal cavity, if present, willhelp confirm the hemoperitoneum.
Cavernous HemangiomaCavernous hemangiomas are the most commonbenign liver tumors, occurring in 7%–10% of thegeneral population. They are more common inwomen (male-to-female ratio, 1:5). The vast ma-jority are small and asymptomatic. There are onlysporadic case reports in the literature of hemor-rhage and rupture of cavernous hemangiomas.These invariably involve giant cavernous heman-giomas (�10 cm) and usually occur in associationwith minor trauma or pregnancy (35,36). Thereare very few reports of spontaneous rupture.
Figure 27. Ruptured hepatic adenoma in a 29-year-old woman using the oral contraceptive pill. She had ab-dominal pain and a falling hemoglobin level. (a) Axial contrast material–enhanced CT scan of the abdomenshows free fluid (arrows) around the liver and a large, heterogeneous mass (arrowheads), which is exophyticfrom the tip of the left lobe. (b) Photograph obtained during surgery shows the ruptured adenoma.
1132 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
US will show a large, heterogeneous mass in aliver of normal background morphology with evi-dence of free fluid or hemoperitoneum. The
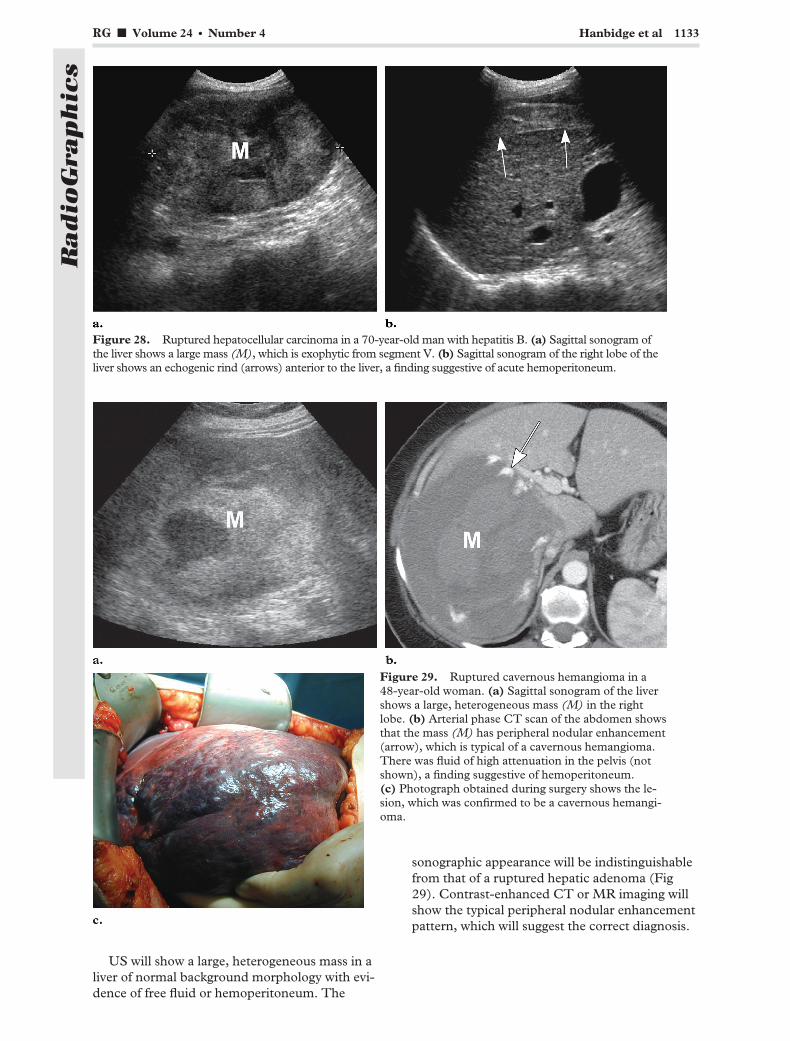
sonographic appearance will be indistinguishablefrom that of a ruptured hepatic adenoma (Fig29). Contrast-enhanced CT or MR imaging willshow the typical peripheral nodular enhancementpattern, which will suggest the correct diagnosis.
Figure 28. Ruptured hepatocellular carcinoma in a 70-year-old man with hepatitis B. (a) Sagittal sonogram ofthe liver shows a large mass (M), which is exophytic from segment V. (b) Sagittal sonogram of the right lobe of theliver shows an echogenic rind (arrows) anterior to the liver, a finding suggestive of acute hemoperitoneum.
Figure 29. Ruptured cavernous hemangioma in a48-year-old woman. (a) Sagittal sonogram of the livershows a large, heterogeneous mass (M) in the rightlobe. (b) Arterial phase CT scan of the abdomen showsthat the mass (M) has peripheral nodular enhancement(arrow), which is typical of a cavernous hemangioma.There was fluid of high attenuation in the pelvis (notshown), a finding suggestive of hemoperitoneum.(c) Photograph obtained during surgery shows the le-sion, which was confirmed to be a cavernous hemangi-oma.
RG f Volume 24 ● Number 4 Hanbidge et al 1133
Radio
Gra
phic
s

ConclusionsThe spectrum of conditions that may manifest asacute right upper quadrant pain was shown withemphasis on the most appropriate and effectiveimaging investigation. Noninvasive determinationof the explanation for the patient’s symptomatol-ogy is the expected standard (37) so that surgicalintervention can be promptly selected for thosepatients with early acute cholecystitis or withother surgical conditions such as ruptured livertumors and gallbladder torsion.
Acknowledgments: We thank Korosh Khalili, MD,FRCPC, for providing the images of gallbladder tor-sion and Murray Asch, MD, FRCPC, for providing theintraoperative photographs.
References1. Laing FC, Federle MP, Jeffrey RB, Brown TW.
Ultrasonic evaluation of patients with acute rightupper quadrant pain. Radiology 1981; 140:449–455.
2. Ralls PW, Colletti PM, Halls JM, Siemsen JK.Prospective evaluation of 99mTc-IDA cholescin-tigraphy and gray-scale ultrasound in the diagnosisof acute cholecystitis. Radiology 1982; 144:369–371.
3. Bree RL, Ralls PW, Balfe DM, et al. Evaluation ofpatients with acute right upper quadrant pain.American College of Radiology. ACR Appropri-ateness Criteria. Radiology 2000; 215(suppl):153–157.
4. Worthen NJ, Uszler JM, Funamura JL. Cholecys-titis: prospective evaluation of sonography and99mTc-HIDA cholescintigraphy. AJR Am JRoentgenol 1981; 137:973–978.
5. Shuman WP, Mack LA, Rudd TG, Rogers JV,Gibbs P. Evaluation of acute right upper quadrantpain: sonography and 99mTc-PIPIDA cholescin-tigraphy. AJR Am J Roentgenol 1982; 139:61–64.
6. Harvey RT, Miller WT Jr. Acute biliary disease:initial CT and follow-up US versus initial US andfollow-up CT. Radiology 1999; 213:831–836.
7. Laing FC: The gallbladder and bile ducts. In: Ru-mack CM, Wilson SR, Charboneau JW, eds. Di-agnostic ultrasound. 2nd ed. Vol 1. St Louis, Mo:Mosby–Year Book, 1998; 175–223.
8. Ralls PW, Colletti PM, Lapin SA, et al. Real-timesonography in suspected acute cholecystitis: pro-spective evaluation of primary and secondarysigns. Radiology 1985; 155:767–771.
9. Soyer P, Brouland JP, Boudiaf M, et al. Color ve-locity imaging and power Doppler sonography ofthe gallbladder wall: a new look at sonographicdiagnosis of acute cholecystitis. AJR Am J Roent-genol 1998; 171:183–188.
10. Jeffrey RB, Laing FC, Wong W, Callen PW. Gan-grenous cholecystitis: diagnosis by ultrasound.Radiology 1983; 148:219–221.
11. Simeone JF, Brink JA, Mueller PR, et al. Thesonographic diagnosis of acute gangrenous chole-cystitis: importance of the Murphy sign. AJR Am JRoentgenol 1989; 152:289–290.
12. Bennett GL, Rusinek H, Lisi V, et al. CT findingsin acute gangrenous cholecystitis. AJR Am JRoentgenol 2002; 178:275–281.
13. Mentzer RM Jr, Golden GT, Chandler JG, Hors-ley JS. A comparative appraisal of emphysematouscholecystitis. Am J Surg 1975; 129:10–15.
14. Bloom RA, Libson E, Lebensart PD, et al. Theultrasound spectrum of emphysematous cholecys-titis. J Clin Ultrasound 1989; 17:251–256.
15. Grayson DE, Abbott RM, Levy AD, ShermanPM. Emphysematous infections of the abdomenand pelvis: a pictorial review. RadioGraphics2002; 22:543–561.
16. Niemeier OW. Acute free perforation of the gall-bladder. Ann Surg 1934; 99:922–924.
1134 July-August 2004 RG f Volume 24 ● Number 4
Radio
Gra
phic
s
17. Sood BP, Kalra N, Gupta S, et al. Role of sonog-raphy in the diagnosis of gallbladder perforation.J Clin Ultrasound 2002; 30:270–274.
18. Oikarinen H, Paivansalo M, Tikkakoski T, SaarelaA. Radiological findings in biliary fistula and gall-stone ileus. Acta Radiol 1996; 37:917–922.
19. Aibe H, Honda H, Kuroiwa T, et al. Gallbladdertorsion: case report. Abdom Imaging 2002; 27:51–53.
20. Rosenthal SJ, Cox GG, Wetzel LH, Batnitzky S.Pitfalls and differential diagnosis in biliary sonog-raphy. RadioGraphics 1990; 10:285–311.
21. Laing FC, Jeffrey RB, Wing VW. Improved visual-ization of choledocholithiasis by sonography. AJRAm J Roentgenol 1984; 143:949–952.
22. Behan M, Kazam E. Sonography of the commonbile duct: value of the right anterior oblique view.AJR Am J Roentgenol 1978; 130:701–709.
23. Topal B, Van de Moortel M, Fieuws S, et al. Thevalue of magnetic resonance cholangiopancreatog-raphy in predicting common bile duct stones inpatients with gallstone disease. Br J Surg 2003;90:42–47.
24. Jimenez Cuenca I, del Olmo Martinez L, PerezHoms M. Helical CT without contrast in chole-docholithiasis diagnosis. Eur Radiol 2001; 11:197–201.
25. Green MH, Duell RM, Johnson CD, JamiesonNV. Haemobilia. Br J Surg 2001; 88:773–786.
26. Bramis J, Felekouras E, Kontos M, Leonardou P,Griniatsos J, Bastounis E. True giant commonhepatic artery aneurysm associated with obstruc-tive jaundice: a case report. Int Surg 2002; 87:142–146.
27. Hanau LH, Steigbigel NH. Acute (ascending)cholangitis. Infect Dis Clin North Am 2000; 14:521–546.
28. Mohsen AH, Green ST, Read RC, McKendrickMW. Liver abscess in adults: ten years experiencein a UK centre. QJM 2002; 95:797–802.
29. Lim JH. Radiologic findings of clonorchiasis. AJRAm J Roentgenol 1990; 155:1001–1008.
30. Park MS, Yu JS, Kim KW, et al. Recurrent pyo-genic cholangitis: comparison between MRcholangiography and direct cholangiography.Radiology 2001; 220:677–682.
31. Talente G, Coleman R, Alter C, et al. Glycogenstorage disease in adults. Ann Intern Med 1994;120:218–226.
32. Grazioli L, Federle MP, Brancatelli G, IchikawaT, Olivetti L, Blachar A. Hepatic adenomas: imag-ing and pathologic findings. RadioGraphics 2001;21:877–892; discussion 892–894.
33. El-Serag HB, Mason AC. Rising incidence ofhepatocellular carcinoma in the United States.N Engl J Med 1999; 340:745–750.
34. Primary liver cancer in Japan. Sixth report. TheLiver Cancer Study Group of Japan. Cancer 1987;60:1400–1411.
35. Hotokezaka M, Kojima M, Nakamura K, et al.Traumatic rupture of hepatic hemangioma. J ClinGastroenterol 1996; 23:69–71.
36. Graham E, Cohen AW, Soulen M, Faye R. Symp-tomatic liver hemangioma with intra-tumor hem-orrhage treated by angiography and embolizationduring pregnancy. Obstet Gynecol 1993; 81(5 pt2):813–816.
37. Trowbridge RL, Rutkowski NK, Shojania KG.Does this patient have acute cholecystitis? JAMA2003; 289:80–86.
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see the questionnaire on pp 1211–1217.
RG f Volume 24 ● Number 4 Hanbidge et al 1135
Radio
Gra
phic
s