fulfilling the mdg an analysis of jamaica’s policy framework for improving maternal health
TRANSCRIPT

FULFILLING THE MDG: AN ANALYSIS OF JAMAICA’S POLICY
FRAMEWORK FOR IMPROVING MATERNAL HEALTH
A ThesisSubmitted in Partial Fulfilment of the Requirements of the Degree of
Masters of Science in Governance and Public Policy
ofThe University of the West Indies
Nicole Antoinette Hayles McGowan2009
Sir Arthur Lewis Institute of Social and Economic StudiesFaculty of Social SciencesMona Campus

2Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
TABLE OF CONTENTS
Abstract
Acknowledgements
Dedication
Chapter 1
Introduction
Maternal Mortality: A Global Perspective
Causes of Maternal Death
Chapter 2
Literature Review
Domestic Violence and Maternal Mortality
Maternal Mortality in Jamaica
Safe Motherhood in Jamaica
Chapter 3
Research Objectives and Methodology
Research Objectives
Methodology
Questionnaire
Sample
Limitations
Chapter 4
3Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Findings
Discussion
Chapter 5
Conclusion and Recommendations
References
Appendices
Questionnaire for Technical Experts
Questionnaire for Healthcare Providers
Questionnaire for Focus Group
Informed Consent Form
Informed Consent Form for Focus Group

4Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
ABSTRACT
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework
For Improving Maternal Health
Nicole Antoinette Hayles McGowan
The changing epidemiology of the causes of maternal deaths in Jamaica, that is adecrease in direct causes while there is an increase indirect causes, has sharpened thefocus for a more concerted effort in bringing the issue of maternal mortality to theforefront of national discourse. While efforts have been made over the past two decadesto reduce the direct causes of maternal deaths such as haemorrhage, sepsis, andhypertensive disorders, indirect causes such as HIV/AIDS, heart disease and diabetes areon the rise. In Jamaica, the classification of deaths have been limited in scope, eventhough international agencies have cited domestic violence as having an impact onmaternal mortality, and have described the social problem as an increasing public healthconcern.
In this thesis, an analysis of Jamaica’s policy framework for improving the country’smaternal health is assessed, with specific emphasis on domestic violence, which receiveslimited attention, if any at all, in the Ministry of Health’s policy document for safemotherhood. The research examines the possible impact of its exclusion on Jamaica’sprospects of reducing its Maternal Mortality Rates by 75% by 2015.
The analysis is based on the findings of elite interviews and focus group discussions withexperts in the field of maternal health, and pregnant women who are the ultimateassessors of the care they receive, and whose outlook evaluates the efforts of the policy inachieving its prescribed mandate.
The research found that domestic violence was excluded from the national policyframework as the issue is not seen as a priority for maternal health; domestic violencefalls outside the purview of the Ministry of Health. Despite this, pregnant women whoparticipated in the research believe that this social issue should be included in any policyframework aimed at improving maternal health, as safe motherhood should encompass awholistic approach to maternal health.
Keywords: maternal mortality; domestic violence; safe motherhood; policy; Jamaica

5Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
ACKNOWLEDGEMENTS
The researcher would like to thank a myriad of persons for helping to make this paper a
reality. Special thanks to Rowena Palmer, Dr. Karen Lewis-Bell and Dr. Yvonne Munroe
of the Ministry of Health; Prof. Affette McCaw-Binns of the University of the West
Indies; Georgette Campbell and Dr. Heather Reid-Jones of the South East Regional
Health Authority; Maria Rankine of Woman Inc.; the team of the Spanish Town Hospital
and the Bureau of Women’s Affairs. Heartfelt gratitude is also accorded to my
supervisor, Dr. Aldrie Henry-Lee, whose guidance, assistance, and constant words of
encouragement were invaluable in making this research paper a reality.
Gratitude is also extended my husband, Fabian McGowan, my most valuable supporter
and critic, whose constant insight keeps me intact and keeps the demon of procrastination
away. Many thanks are also in order to the many well-wishers for their words of
encouragement. Eternal thanks to the Lord for giving me the strength to persevere.

6Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
DEDICATION
To my children: brilliantly shining brightly.
7Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
CHAPTER 1
Introduction
Why have 1091017 (women) died in 2008? Women died for the lack of family planning,skilled birth attendance, or emergency obstetric care. Another 1,440 will die today unlesswe act.
United Nations Population Fund (2009a)1.
The drive towards improving maternal health has become a global priority as it is placed
at the forefront as one of the eight Millennium Development Goals (MDGs) that world
leaders have committed to address by 2015. Over the past two decades a lot of work has
been done to reduce annual maternal mortality statistics, particularly with the
introduction of the Safe Motherhood Initiative which was launched in 1987 in Nairobi,
Kenya. The aim of the initiative was to address the issue of women dying during
pregnancy and child birth, by reducing maternal mortality by 50% by the start of the
millennium. While this target was not achieved, the Safe Motherhood Initiative is seen as
the first global effort in addressing the world’s high maternal mortality and morbidity
rates (McCaw-Binns 2005; Smith and Sulzbach 2008; Women Deliver 2009).
Safe motherhood is the ability of a woman to undertake pregnancy and childbirth, if and
when desired, without injury to her self and her child (Ransom and Yinger 2002). Safe
motherhood programmes are designed to reduce the high numbers of maternal deaths and
illnesses which result from complications of pregnancy and childbirth. In many countries,
1 http://www.unfpa.org/safemotherhood/, retrieved June 25, 2009.

8Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
the leading cause of maternal deaths is haemorrhage, complications of unsafe abortion,
pregnancy-induced hypertension, sepsis and obstructed labour (UNFPA 2009a). A
country’s safe motherhood programmes is therefore targeted at addressing these medical
complications as well as implement and undertake the appropriate measures to ensure
that women have access to health services.
The global thrust towards improve maternal health, also went further by quantifying
global targets through the creation of the MDGs which were adopted in 2001 by the 192
United Nations (UN) member states. The objective is that by 2015 the targets outlined in
the Millennium Development declaration would have been met. The MDGs include:
1. Eradicate extreme poverty and hunger
Halve, between 1990 and 2015, the proportion of people whose income is less than
one dollar a day.
Achieve full and productive employment and decent work all, including women and
young people.
Halve, between 1990 and 2015, the proportion of people who suffer from hunger.
2. Achieve universal primary education
Ensure that, by 2015, children everywhere, boys and girls alike, will be able to
complete a full course of primary schooling.

9Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
3. Promote gender equality and empower women
Eliminate gender disparity in primary and secondary education preferably by
2005, and at all levels by 2015.
4. Reduce child mortality
Reduce by two-thirds, between 1990 and 2015, the under-five mortality rate.
5. Improve maternal health
Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio.
Achieve, by 2015, universal access to reproductive health.
6. Combat HIV/AIDS, malaria, and other diseases
Have halted by 2015 and begun to reverse the spread of HIV/AIDS.
Achieve, by 2010, universal access to treatment for HIV/AIDS for all those who
need it.
Have halted by 2015 and begun to reverse the incidence of malaria and other
major diseases.
7. Ensure environmental sustainability
Integrate the principles of sustainable development into country policies and
programmes; reverse loss of environmental resources.
Reduce biodiversity loss, achieving, by 2010, a significant reduction in the rate of

10Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
loss.
Halve, by 2015, the proportion of people without sustainable access to safe
drinking water and basic sanitation.
By 2020, to have achieved a significant improvement in the lives of at least 100
million slum-dwellers.
8. Develop a global partnership for development
Develop further an open trading and financial system that is rule-based,
predictable and non-discriminatory. Includes a commitment to good governance,
development and poverty reduction—nationally and internationally.
Address the special needs of the least developed countries. This includes tariff
and quota free access for their exports; enhanced programme of debt relief for
heavily indebted poor countries; and cancellation of official bilateral debt; and
more generous official development assistance for countries committed to poverty
reduction.
Address the special needs of landlocked and Small Island Developing States.
Deal comprehensively with the debt problems of developing countries through
national and international measures in order to make debt sustainable in the long
term.
In cooperation with pharmaceutical companies, provide access to affordable in
developing countries.
In cooperation with the private sector, make available the benefits of new

11Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
technologies, especially information and communications. (UN 2009)2.
2 http://www.un.org/millenniumgoals/, retrieved June 25, 2009.

12Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Maternal Mortality: A Global Perspective
Progress towards the MDGs has been uneven as each country is said to have different
degrees of achievement towards each target (ECLAC 2005, 254). In the case of maternal
mortality, it remains “unacceptably high across much of the developing world”; reducing
global statistics by three-quarters remains a challenging task (UNFPA 2009b). According
to the World Health Organization maternal mortality is defined as “the death of a woman
while pregnant or within forty-two days of termination of pregnancy, irrespective of the
duration and site of the pregnancy, from any cause related to or aggravated by the
pregnancy or its management, but not from accidental or incidental causes”. Maternal
mortality is also seen as “the number of deaths due to complications of pregnancy,
labour, puerperium and abortion per 100,000 total live births” (Ashley 1973). Such
definitions therefore highlights that death can be direct or indirect. Direct cause of death
encompasses factors relating to the complications of pregnancy, delivery, or their
management, while indirect death relates to “death in a patient with a pre-existing or
newly developed health problem” (WHO 2009). Any other causes of death that a woman
might experience that are unrelated to the pregnancy are classified as accidental,
incidental or non-obstetrical maternal deaths (Ibid). The definitions posited are however
limited in their scope, as maternal deaths may occur after forty-two days after a
termination of pregnancy or delivery (Koonin et al 1988). Maternal mortality may also be
influenced by factors outside the realms of physical pregnancy. Violence against women;
war and civil unrest; the quality of maternity services; socio-economic circumstances

13Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
such as poverty, large families, over crowding, illiteracy, poor sanitation; as well as
culture and customs can also have an impact on maternal mortality rates (Thomas 1993).
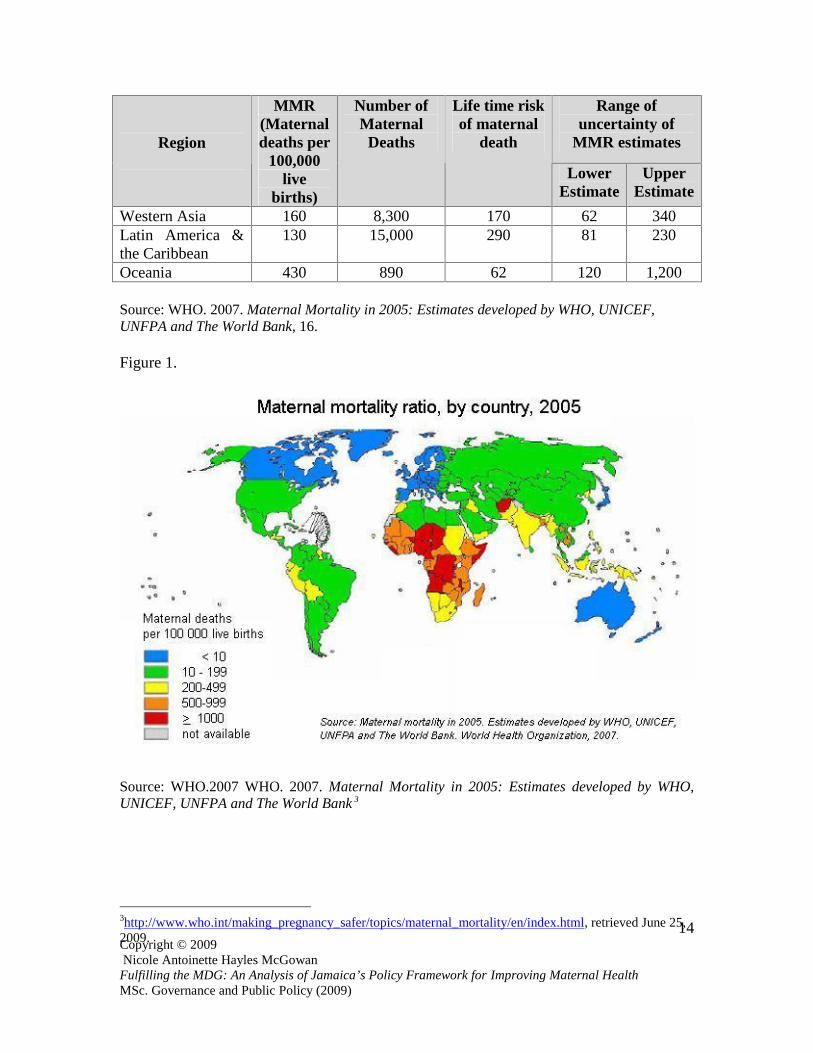
According to the World Health Organization et al (2007) in its Maternal Mortality 2005
report, up to 15% of pregnant women worldwide experienced potentially fatal
complications during birth, which equated to approximately twenty million women each
year. The report also noted that 80% of the global statistics on maternal deaths are due to
five direct causes: haemorrhage, sepsis, unsafe abortion, obstructed labour and
hypertensive diseases of pregnancy. The report also revealed that of the 536,000 maternal
deaths, approximately 21% was due to haemorrhaging (see Table 1 and Figure 1).
Table 1. Estimates of Maternal Mortality Rates (MMR), number of maternal deaths,lifetime risk, and range of uncertainty by United Nations MDG regions, 2005
Range ofuncertainty of
MMR estimatesRegion
MMR(Maternaldeaths per
100,000live
births)
Number ofMaternal
Deaths
Life time riskof maternal
death
LowerEstimate
UpperEstimate
World Total 400 536,000 92 220 650
DevelopedCountries
9 960 7,300 8 17
Countries of thecommonwealth ofindependent states
51 1,800 1,200 28 140
DevelopingCountries
450 533,000 75 240 730
Africa 820 276,000 26 410 1,400Northern Africa 160 5,700 210 85 290Sub-SaharanAfrica
900 270,000 22 450 1,500
Asia 330 241,000 120 190 520Eastern Asia 50 9,200 1,200 31 80South-Eastern Asia 300 35,000 130 160 550
14Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Range ofuncertainty of
MMR estimatesRegion
MMR(Maternaldeaths per
100,000live
births)
Number ofMaternal
Deaths
Life time riskof maternal
death
LowerEstimate
UpperEstimate
Western Asia 160 8,300 170 62 340Latin America &the Caribbean
130 15,000 290 81 230
Oceania 430 890 62 120 1,200
Source: WHO. 2007. Maternal Mortality in 2005: Estimates developed by WHO, UNICEF,UNFPA and The World Bank, 16.
Figure 1.
Source: WHO.2007 WHO. 2007. Maternal Mortality in 2005: Estimates developed by WHO,UNICEF, UNFPA and The World Bank 3
3http://www.who.int/making_pregnancy_safer/topics/maternal_mortality/en/index.html, retrieved June 25,2009.
15Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Of the 536,000 maternal deaths, developing countries accounted for 99% of the deaths,
which translated to 533,000. More than half of the world’s 2005 MMR occurred in sub-
Saharan Africa which totaled 270,000. Sub-Saharan Africa also has the highest MMR,
accounting for 900 deaths per 100,000 live births, compared to South Asia 490, Oceania
430, South-Eastern Asia 300, West Asia 160, Northern Africa 160, Latin America and
the Caribbean 130, and Eastern Asia 50. India was ranked as the country with the highest
number of maternal deaths which totaled 117,000, followed by Nigeria 59,000, the
Democratic Republic of Congo 32,000, Afghanistan 26,000, Ethiopia 22,000, Bangladesh
21,000, Indonesia 19,000, Pakistan 15,000, Niger 14,000, Tanzania 13,000, and Angola
11,000. All these countries accounted for 65% of the maternal deaths recorded in 2005
(WHO 2007, 15).
Despite the figures for 2005 figures, maternal mortality is said to be on the decline
globally in all regions, however the decline is marginal (UNFPA 2009b). MMR was
down by just 1% when data from 1990 to 2005 are compared. The WHO et al. (2005)
note that the decline is too low to meet MDG target of a 75% reduction in MMR from
1990 to 2015, as achieving this will require rates of up to 5.5% annually (See Table 2).

16Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Table 2. Comparison of 1990 and 2005 maternal mortality by United Nations MDGregions
1990 2005
RegionMMR Maternal
DeathsMMR Maternal
Deaths%change inMMRbetween1990 and2005
Annual%change inMMRbetween1990 and2005
World Total 430 576,000 400 536,000 -5.4 -0.4DevelopedCountries
11 1,300 9 960 -23.6 -1.8
Countries of theCommonwealthStates
58 2,800 51 1,800 -12.5 -0.9
DevelopingCountries
480 572,000 450 533,000 -6.6 -0.5
Africa 830 221,000 820 276,000 -0.6 0.0North Africa 250 8,900 160 5,700 -36.3 -3.0Sub-SaharanAfrica
920 212,000 900 270,000 -1.8 -0.1
Asia 410 329,000 330 241,000 -19.7 -1.5Eastern Asia 95 24,000 50 9,200 -47.1 -4.2South-EasternAsia
450 56,000 300 35,000 -32.8 -2.6
Western Asia 190 8,500 160 8,300 -16.2 -1.2Latin America &the Caribbean
180 21,000 130 15,000 -26.3 -2.0
Oceania 550 1,000 430 890 -22.2 -1.7
Source: WHO. 2007. Maternal Mortality in 2005: Estimates developed by WHO, UNICEF,UNFPA and The World Bank, 17.
17Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
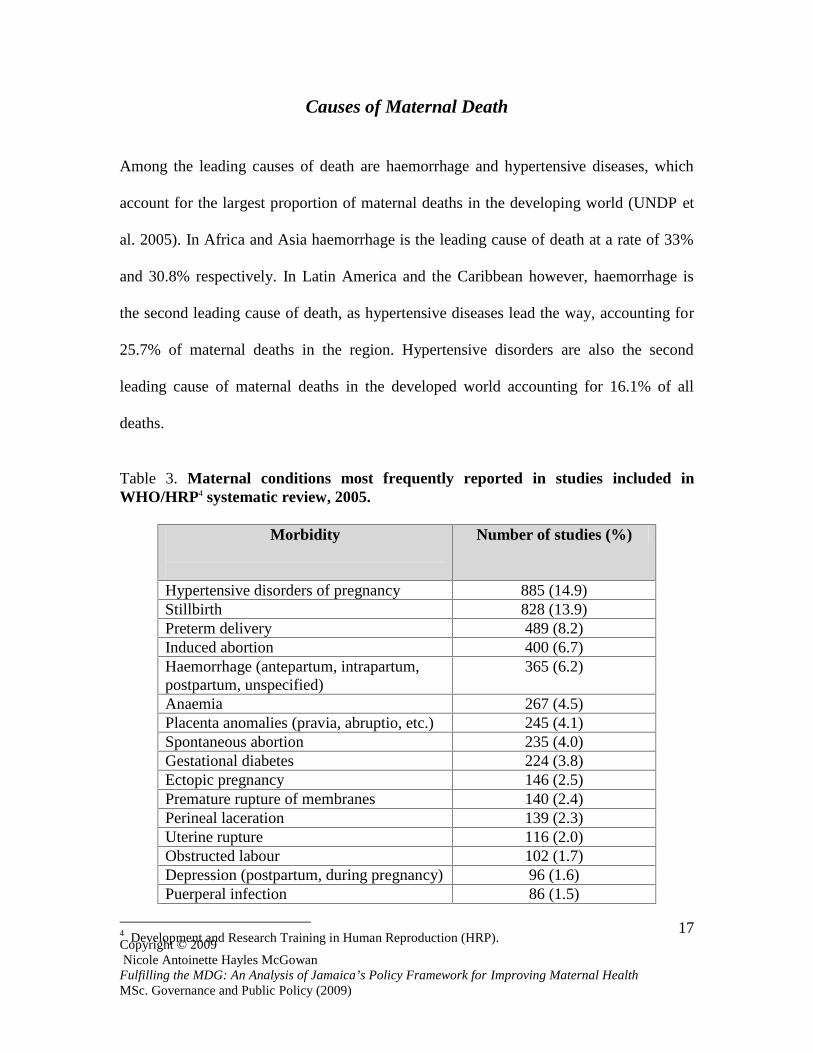
Causes of Maternal Death
Among the leading causes of death are haemorrhage and hypertensive diseases, which
account for the largest proportion of maternal deaths in the developing world (UNDP et
al. 2005). In Africa and Asia haemorrhage is the leading cause of death at a rate of 33%
and 30.8% respectively. In Latin America and the Caribbean however, haemorrhage is
the second leading cause of death, as hypertensive diseases lead the way, accounting for
25.7% of maternal deaths in the region. Hypertensive disorders are also the second
leading cause of maternal deaths in the developed world accounting for 16.1% of all
deaths.
Table 3. Maternal conditions most frequently reported in studies included inWHO/HRP4 systematic review, 2005.
Morbidity Number of studies (%)
Hypertensive disorders of pregnancy 885 (14.9)Stillbirth 828 (13.9)Preterm delivery 489 (8.2)Induced abortion 400 (6.7)Haemorrhage (antepartum, intrapartum,postpartum, unspecified)
365 (6.2)
Anaemia 267 (4.5)Placenta anomalies (pravia, abruptio, etc.) 245 (4.1)Spontaneous abortion 235 (4.0)Gestational diabetes 224 (3.8)Ectopic pregnancy 146 (2.5)Premature rupture of membranes 140 (2.4)Perineal laceration 139 (2.3)Uterine rupture 116 (2.0)Obstructed labour 102 (1.7)Depression (postpartum, during pregnancy) 96 (1.6)Puerperal infection 86 (1.5)
4 Development and Research Training in Human Reproduction (HRP).

18Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Morbidity Number of studies (%)
Violence during pregnancy 77 (1.3)Urinary tract infection 66 (1.1)Malaria 54 (0.9)Other conditions 973 (16.4)Total 5933
Source: UNDP, UNFPA,WHO, World Bank Special Programme of Research, Development andResearch Training in Human Reproduction. 2005. Progress in Reproductive Health Research, 4.
According to the Beijing Platform for Action adopted at the Fourth World Conference on
Women in 1995, complications related to pregnancy and childbirth are the leading cause
of death and morbidity among women of reproductive age in the developing world (UN
2006). Despite this though, reliable statistics on maternal deaths over the years is still
difficult to obtain which further compounds the problem in fully understanding the causes
of death worldwide. The United Nations (2006) reports that there is significant
underreporting and misclassification of maternal deaths, as there are often problems at
the point of civil registration, as deaths are sometimes not correctly identified, therefore
compromising the reliability of data. The UN also notes that maternal deaths are also
hard to identify because information regarding the age of women, pregnancy status, as
well as the medical cause of death is sometimes hard to ascertain. The UN states that:
(The) experience in developing international estimates ofmaternal mortality illustrates the many difficulties thatcountries face in measuring maternal mortality. Theaccuracy of data on maternal deaths depends largely onthe existence and reliability of national civil registrationsystems, which are the primary source of data on

19Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
deaths….Policy makers and planners increasinglydemand that data be annually reported and that these dataare current. However that is not the situation observed inmost countries…Limited reporting is therefore affectingthe continuous availability of up-to-date annualinformation for a number of countries (which) is largelydue to delays in data compilation and dissemination. (UN2006, 26)
This underreporting also makes it difficult to gather information on the cause of maternal
deaths which are a result of violence against women. Discourse on domestic violence and
maternal mortality has been receiving prominence as the two are said to be “linked”
(PAHO 2005; Espinoza and Camacho 2005; Mitchell 2000; Bacchus et al 2004; Edin and
Högberg 2002), as some women die from domestic violence while pregnant or during the
forty-two days after pregnancy. It is however still not known what proportion of maternal
deaths is due to domestic violence, the estimates among countries, as well as the factors
that could explain the disparities (PAHO 2005).
20Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
CHAPTER 2
(Literature Review)
Domestic Violence and Maternal Mortality
Violence against women both violates and impairs or nullifies the enjoyment by women totheir human rights and fundamental freedoms…the human rights of women and of thegirl child are an inalienable, integral and indivisible part of universal human rights.
Beijing Platform for Action (1995)5.
The Beijing Platform for Action reaffirms the principles of human rights outlined in the
Vienna Declaration and Programme of Action adopted by the World Conference on
Human Rights. As an agenda for action, the Platform is aimed at promoting and
protecting the full enjoyment of all human rights and the fundamental freedoms of all
women throughout their life cycle. Likewise, the Convention on the Elimination of All
Forms of Discrimination against Women (1979) calls on governments to:
incorporate the principle of equality of men and women in their legal system,
abolish all discriminatory laws and adopt appropriate ones prohibiting
discrimination against women;
establish tribunals and other public institutions to ensure the effective
protection of women against discrimination; and
ensure elimination of all acts of discrimination against women by persons,
organizations or enterprises.
5 United Nations, World’s Women 2005: Progress in Statistics (New York: United Nations, 2006), 69.

21Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
The Declaration also espouses that:
Any act of gender-based violence that results in, or islikely to result in, physical, sexual or psychological harmor suffering to women, including threats of such acts,coercion or arbitrary deprivation of liberty, whetheroccurring in public or private life. It encompasses, but isnot limited to, physical, sexual and psychologicalviolence occurring in the family, including battering,sexual abuse of female children in the household, dowryrelated violence, marital rape, female genital mutilationand other traditional practices harmful to women; non-spousal violence and violence related to exploitation;physical, sexual and psychological violence occurringwithin the general community, including rape, sexualabuse, sexual harassment and intimidation at work, ineducational institutions and elsewhere; trafficking inwomen and forced prostitution; and physical, sexual andpsychological violence perpetrated or condoned by thestate, wherever it occurs.6
Violence against women is a multi-faceted and multi-dimensional phenomenon as its
definition varies depending on whose perception through which the act is interpreted.
According to Gelles and Straus (1979) (cited in Crowell and Burgess1996, 9) violence is
“any act carried out with the intention of or perceived intention of causing physical pain
or injury to another person.” Violence can also be seen as “physical, visual, verbal, or
sexual acts that are experienced by a woman or a girl as a threat, invasion, or assault and
that have the effect to hurting her or degrading her and or taking away her ability to
control contact, intimate of otherwise with another individual” (Koss et al 1994 cited in
Crowell and Burgess 1996, 10). Violence against women is also characterised as
“coercive control that is maintained by tactics such as physical violence, psychological
6http://www.un.org/womenwatch/daw/cedaw/text/econvention.htm, retrieved June 25, 2009.

22Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
abuse, sexual violence and denial of resources” (Crowell and Burgess 1996, 10). An
important element in comprehending violence against women and finding ways to solve
it, is understanding what the causes of this social problem. Researchers have pointed to
two main elements: an examination of the characteristics that influences the perpetrator’s
behaviour and deciphering whether some women are more vulnerable to being victimised
(Crowell and Burgess 1996).
Crowell and Burgess (1996) argue that violence against women is not caused by a single
factor; it is therefore difficult to isolate a sole determinant that could be fingered as the
cause of this social problem. From an evolutionary perspective the goal of violence that is
perpetuated against women by men is for the sole purpose of passing on their genes. In
other words, the goal of the perpetrator is to have offspring with his victim, which will
stand the chance of survival and possibly promulgate the same set of genes The
physiological or neurophysiological perspective argues that violence and aggression are
the function of hormones such as testosterone or the by product of abnormalities or brain
dysfunctions that interfere with cognition. Crowell and Burgess (1996) also cite
personality disorders, cultural myths about violence and gender based roles, as well as a
motivated means by men to dominate women as causes that perpetuate gender based
violence. Crowell and Burgess (1996) also posit that violence against women is also done
in a dyadic context in that “a man often refrains from physical (verbal, psychological)
violence until a woman has made an emotional commitment to him such as moving in
together, getting engaged or married, or becoming pregnant.”
23Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Not only is violence against women a substantial public health concern, but violence
against a pregnant woman not only harms her but also increases the risk of injury to the
unborn child. The consequences are also broader as it affects families and loved ones not
only of the victim but the perpetrators themselves. Children who lose their mother are
more likely to die before reaching the age of five (UNICEF 2009; UNFPA 2009a).
Violence can harm the foetus through direct injury causing “placental damage, premature
contractions, membrane rupture, or foetal death” (Koenig et al. 2006). According to
Koenig et al (2006), between 4% to 8% of women experience violence during their
pregnancies. The authors say women who are engaged in HIV risk behaviour have an
elevated chance of being abused while pregnant; women who engage in sex work or use
narcotics are more likely to be abused than women who do not lead such lifestyles.
Becoming pregnant at a young age, low education, income levels as well as being
unmarried, are also seen as factors that increases a woman’s chances of being abused
(Matthews 2002)
A 2006 study (Koenig et al. 2006) in the United States revealed that of the 628 women
between the ages of 13 to 45 interviewed in a nationwide study, 8.9% of them reported
physical and sexual abuse during their pregnancy. The report also revealed that 4.9% of
the women also reported being abused at least 6 months after their deliveries. The report
noted however, that very little is still known about the differences in violence risk during
pregnancy and after delivery, as the opportunities to detect abuse are being missed.
Protecting women from violence during and after pregnancy will depend on how best the

24Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
health care system and other social services are able to identify women who are already
being abused and enact the appropriate actions needed to end the violence against them
(Koenig et al 2006).
Domestic violence and maternal mortality are increasingly become a major global public
health concern (PAHO 2005). Both domestic violence and maternal mortality are
interconnected, even though the proportion of maternal deaths due to domestic violence
still poses a challenge in maternal mortality data (PAHO 2005). According to Espinoza
and Camacho (2005) the definition of maternal mortality should take into account
“several components, including violent death, violence against women, and the current
international definition of maternal death, (as) maternal death due to domestic violence
(warrants questions such as): which maternal deaths are caused by domestic violence?
Would it only be deaths caused by direct lethal trauma, or should deaths due to obstetric
complications that are initially caused by physical injuries also be included (for example,
a placental abruption secondary to an abdominal trauma)? Can psychological violence be
included as a cause of maternal death? Would these deaths refer only to domestic
violence by the intimate partner? And, should the motives of violence be considered as
part of the definition as well?” However based on the traditional medical definition of
what maternal deaths are, deaths caused by domestic violence are simply classified as
external causes.
The Pan-American Health Organization (2005) notes that the murder of pregnant women
by their partners and suicide among women while pregnant or following the end of

25Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
pregnancy, are often attributable to unwanted pregnancy. A study in Matlab, Bangladesh
between 1976 to 1993, revealed that pregnant teenagers were at a greater risk of
committing suicide compared to non-pregnant teens. In 2001 it was revealed that in
Morelos, Mexico approximately 15% of violent deaths of women were attributable to
unwanted pregnancies (Ronsmans and Khlat 1999 cited in PAHO 2005; Walker et al.
2005).
The problem that lies herein is that the international definition of maternal death does not
consider “incidental or accidental causes of death, (thereby) exclud(ing) deaths from
domestic violence from the numerator of the maternal mortality ratio” (Espinoza and
Camacho 2005, 126). In most developed countries maternal mortality is low as it
accounts for only 1% of 2005 statistics, yet the deaths that are attributable to domestic
violence is not known. According to Gazmararian et al (1995), pregnant women die of
external injuries more often than medical complications. However reasons for the
external cause of death are hard to source. It was also noted that women abused during
pregnancy were three times more likely to be murdered by their spouses, compared to
non abused pregnant women. However, Mitchell (2000) argues that the influence of
violence on maternal mortality is not always linear as “violence does not have to be
proximal to be causal” In other word, the influence of violence on maternal mortality is
not necessarily linear or clear cut, as there can be a myriad of factors that contribute to
the problem.
In researching domestic violence and maternal mortality in the Otavalo and Cotacahi

26Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
provinces of Ecuador, Mitchell (2000), found that domestic violence was pervasive even
during the periods when a woman was with child, as public hospital records revealed that
13.6% of women treated had a reported lifetime history of physical abuse during
pregnancy. The study also uncovered that both married and unmarried women agreed that
husbands had the right to corporally punish wives who were “lazy, adulterous, refused to
do household chores or sleep until the sun rise(s)”. In Otavalo and Cotacahi, gossip and
suspicion surrounding a woman’s pregnancy were also causal factors that perpetuate
domestic violence against pregnant women. A pregnant woman’s capacity to escape the
violence would therefore “depend on her ability to marshal social capital in her defense”.
Social capital, that is the level of trust a woman has with her relatives and neighbours, is
seen as the most salient asset in Otavalo and Cotacahi, as the geographical isolation of
women who live far away from immediate family members, sometimes due to marriage,
makes them more at risk to violence (Mitchell 2000).
Domestic violence against pregnant women is further compounded at the healthcare level
as those offering care, although knowledgeable of the sensitive needs of pregnant women,
will not do the necessary research to ascertain if the women are being physically abused.
A 1999 study of 51 midwives in 36 antenatal clinics in the Swedish county of
Västerbotten, revealed that these healthcare professionals, though cognisant of the
frequency of physical and sexual abuse before and during the current pregnancy of some
of their patients, did not report the matter. The report further revealed that midwives also
did not make adequate enquiries even if they were suspicious that the pregnant women

27Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
were being abused. The situation in Västerbotten was further compounded as “the local
programme for antenatal care provided no guidelines regarding response to violence, no
instruments for disclosure and no directions about support when confronted with an
abused pregnant woman. (M)idwives were (also) disclosing only a fraction of the cases of
abuse against women” (Edin and Högberg 2002, 268). The study further noted that
domestic violence against pregnant women will remain hidden as long as the issue of
violence is not addressed and included in the national or local programmes for antenatal
care (Ibid).
The failure of health professionals to identify domestic violence and offer appropriate
support is a significant problem. Bacchus et al (2004) argue that most women who are in
an abusive relationship at some point requested medical assistance, therefore pregnancy
should provide an opportunity for doctors and midwives to identify and help women
experiencing domestic violence because of their frequent visits to healthcare centres.
Studies have shown that repeated enquiry using structured questions in pregnancy
significantly increases the rate of detection of domestic violence, as rates of violence
during pregnancy perpetrated by a partner are said to range from 3.4% to 33.7%. Higher
rates can however be elicited through direct questioning by trained health professionals
and repeated questioning (Bacchus et al 2004).
While domestic violence against pregnant women occurs in all countries, the lack of
greater discussion of the topic, appropriate questioning by those offering health care to
pregnant women, as well as reliable data to support and broaden discussions on the

28Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
implications of domestic violence on maternal mortality is lacking. Generating data on
the interconnectedness between domestic violence and maternal mortality is important in
developing a strategic framework on Safe Motherhood (PAHO 2005). Preventing
violence during pregnancy can also assist in the achievement of MDG 5 which calls for
the reduction of maternal mortality by 75% by 2015. In doing this it will have a ripple
effect in the attainment of components of the other MDGs, which call for the totality of
human development.

29Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Maternal Mortality in Jamaica
Jamaica is small developing state located in the Caribbean Sea at latitude 18° 15' and
longitude 77° 30'. It has a population of approximately 2.7 million and is a heavily
indebted country, as it has the fourth largest debt-to-GDP ratio in the world (PIOJ 2009,
5). The country has a total land area of 234 kilometres, and is located within the Greater
Antilles group of islands in the Caribbean Sea. Jamaica is located approximately,
145 kilometres south of Cuba and 190 kilometres west of Hispaniola.
Jamaica was once inhabited by Taino Indians who called the island Xaymaca, meaning
the land of “wood and water”. The Taino population is said to have been between 6,000
to 9,000 persons. Their existence was however disrupted when Spanish explorer
Christopher Columbus landed, in what is now known as St. Ann’s Bay, on May 4, 1494.
The Tainos were defeated by Columbus and his men, and by 1509, Jamaica was declared
a colony of Spain and renamed Santiago. However Spain’s rule was not long lived, as the
British defeated them and seized control of what is now known as Jamaica in 1655.
Jamaica remained under British rule from 1655 until it gained independence in 1962
(Satchell 1999).
While under British rule slavery was a prominent economic activity, as “the wealth
created in Jamaica by the labour of black slaves has been estimated at £18,000,000, more
than half of the estimated total of £30,000,000 for the entire British West Indies”
(Satchell 1999). But despite the high economic yield Jamaica derived from the labour of

30Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
slaves, the health of the slaves was not seen as a priority as there was always
“replacement stock” that could be bought from Africa (McCaw-Binns 2005, 255).
Pregnant slaves received little attention, as they were deemed inefficient and seen as an
economic cost because of the amount of time they would need to recovery from
deliveries and care for their babies. In the same vein, slave reproduction in Jamaica was
seen as inefficient as 20% of births were still births and less than 50% of infants survived
after the first year. Things however changed in 1807 when the trading of slaves was
abolished (Patterson 1967 cited in McCaw-Binns 2005).
The abolition of the slave trade saw more focus being placed on the health of ex-slaves,
as estate doctors were employed to attend to the need of the remaining ones. The fertility
needs of female ex-slaves were also given attention, as plantation owners could no longer
“replenish” their stock from Africa; pregnant ex-slaves were therefore seen as a prized
investment. However those privileges soon came to an end, as the granting of full
emancipation in Jamaica in 1838 saw “the withdrawal of indulgences enjoyed by female
ex-slaves” (McCaw-Binns 2005, 255). By 1838 plantation owners no longer saw the
health of the freed slaves as their responsibility, as by then, the estates were being toiled
by indentured workers from China and India. However the collapse of the estate-based
health system is said to have prompted the authorities in England to enact legislative
provisions in 1875 that resulted in the poor and destitute indentured workers, as well as
members of the police force receiving medical care. By 1903, 45 district doctors were
dispatched across all the health districts in the island (Ford and Cundall 1910 cited in

31Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
McCaw-Binns 2005).
While the British government tried to fill the gap left by the collapse of the estate-based
health care system following emancipation with legislation in 1875, the island’s maternal
mortality rate was high as the Registrar General reported an MMR of 660.9/100,000
compared to 230/100,000 in the United Kingdom (Registrar General 1878 cited in
McCaw-Binns 2005). This revelation is said to have promoted the British authorities to
establish the Victoria Jubilee Hospital (VJH) which opened its doors, nine years later in
1887 to commemorate the fiftieth anniversary of Queen Victoria. By 1929 Jamaica’s
MMR fell to 488/100,000 (McCaw-Binns 2005) (See Table 4).
Table 4. Maternal Mortality by cause: Jamaica 1929
Cause of Death Number Ratio per 100,000 livebirths
Eclampsia/ pre-eclampsia 34 91.0
Puerperal sepsis 27+ 72.3
Post partum haemorrhage 21 56.2
Accidents of pregnancy 19 50.9
Other accidents of
pregnancy
58 155.3
Embolism/ sudden death 3 8.0
Puerperal insanity 3 8.0
Total 165 488

32Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Source: Medical Superintendent’s Report, Jamaica 1930 cited in McCaw-Binns (2005), 256.
By 1960, Jamaica’s MMR stood at approximately 200/100,000, which was attributed to
declines in sepsis deaths. There was also an improvement in maternal care, as the VJH
had improved its antenatal screenings and hospital delivery bookings. By the time
Jamaica gained independence in 1962, the role of community midwives had expanded
beyond deliveries to include family planning services, antenatal, post natal, and child
services. In 1980, over 80% of the population lived within at least ten miles of a primary
health facility, thereby improving women’s access to basic health care (McCaw-Binns
2005).
Improvements in Jamaica’s MMR were also attributed to an increase in the literacy levels
of women of reproductive age. Secondary or higher education among women increased
from 16.5% in 1970 to 70% by 2001. This increase in the education levels of women was
coupled by an increase in their exposure and general expectations, as they were starting
to “move away from having babies at home and became more selective where they gave
birth” (McCaw-Binns 2005, 258). Between 1981 to 2001, births at hospitals increased
from 70% to 91% respectively. Women’s exposure to the family planning programme,
which was launched by the government in 1967 and integrated into the Ministry of
Health’s maternal and child health programmes in 1979 also contributed to women’s
increased awareness about their reproductive health, as Jamaica’s total fertility rate
declined from 4.5 to 2.5 between 1975 to 2001 (McCaw-Binns 2005).

33Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
While there have been improvements in maternal healthcare in Jamaica, the lack of vital
registration of maternal deaths continues to offer erroneous data due to misclassification
of the cause of death (McCaw-Binns et al 2007). This promoted the government to
implement a Reproductive Age Mortality Surveillance (RAMOS) with the first study
being done between 1981 to 1983, and the other two between 1986 to 1987 and 1993 to
1995. Based on the findings of the studies a comprehensive strategy to manage
pregnancy-induced disorders such as hypertension was developed, as well as
improvements in the quality of care at health facilities. The studies also prompted health
officials to reduce the delays associated with the distance between health facilities, the
referral of high risk patients, as well as improving the skills of health care professionals.
The study also revealed a decrease in Jamaica’s MMR to 106/100,000 in 1993 to 1995
(McCaw-Binns 2005; McCaw-Binns et al 2007) (See Figure 2). In a bid for continuous
surveillance the Ministry of Health instituted a policy in 1998 that all maternal deaths
must be notified. All maternal deaths now had to be reported to the Ministry by all the
four Regional Health Authorities which are expected to investigate all deaths (McCaw-
Binns et al 2007). But despite the policy directive there are still gaps and fluctuations in
the Ministry’s data sets, as there are reporting periods during which no data is available
(See Tables 5 and 6).

34Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Figure 2.
Source: 1931–64: Annual Reports: Registrar General, Spanish Town, Jamaica; West IndianMedical Journal 2001, cited in McCaw-Binns et al (2007), 257.
Table 5. Maternal Mortality by cause: Jamaica 2002-2005 (Source: Ministry of Health (2009))
Year Cause of Death Total Maternal Deaths forYear
2002 Pregnancy, childbirth,
puerperium
12
2003 Pregnancy, childbirth,
puerperium
14
2004 Pregnancy, childbirth,
puerperium
4
2005 Pregnancy, childbirth,
puerperium
19

35Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Table 6. Maternal Morbidity: Jamaica 2003-2006
Year ObstetricDischarges
Total LiveBirths
Obstetriccomplications
Percentage ofcomplications
2003 51,316 43,705 2110 4.10%
2004 49,146 42,960 2581 5.30%
2005 48,675 45,114 2059 4.20%
2006 36,562 N/A 1859 5.10%
Source: Ministry of Health (2009).
While efforts have been made to reduce maternal mortality in Jamaica, the improvements
are still seen as unsatisfactory, as key indicators reveal that there has been a failure to
meet even the 2005 national MMR target of 80/100,000 (PIOJ 2009). The problem that
lies herein, is that only a small portion of women initiate care in the first trimester of
pregnancy. There are still unresolved data management problems even though the
regional health authorities are to make mandatory reports; there are however underlying
problems such as inadequate staffing and facilities to conduct proper post mortems.
While maternal deaths from direct causes are said to have halved over the past 10 years,
there has been an increase in indirect causes such as HIV/AIDS and non-communicable

36Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
lifestyle diseases such as diabetes and obesity. There is also a 47% shortage in the
midwife cadre due to migration (PIOJ 2009). While figures of violence against women
have fluctuated over the years, even though in the homes continue to feature prominently
as the place women are more likely to be victims of violence, data is still lacking with
regards to disaggregating figures for those which cause maternal deaths, or acts of
violence committed against pregnant women (See Tables 7, 8, 9, 10, 11). While there’s
no evidence regarding the impact of violence on Jamaica’s MMR (MOH 2009), Jamaica
is however far behind in achieving MDG5 by 2015, as for the country to achieve the goal,
Jamaica’s MMR would have to be reduced to 25/100,000 (PIOJ 2009; UNICEF 2009).
Table 7. Violence related injuries by gender, 2003-2006.
Gender 2003 2004 2005 2006
Males 8996 8787 8367 7481
Females 6567 6198 5792 5366
Total 15,563 14,985 14,159 12,847
Source: Ministry of Health, cited in National Progress Report 2004-2006 (2008), 266.
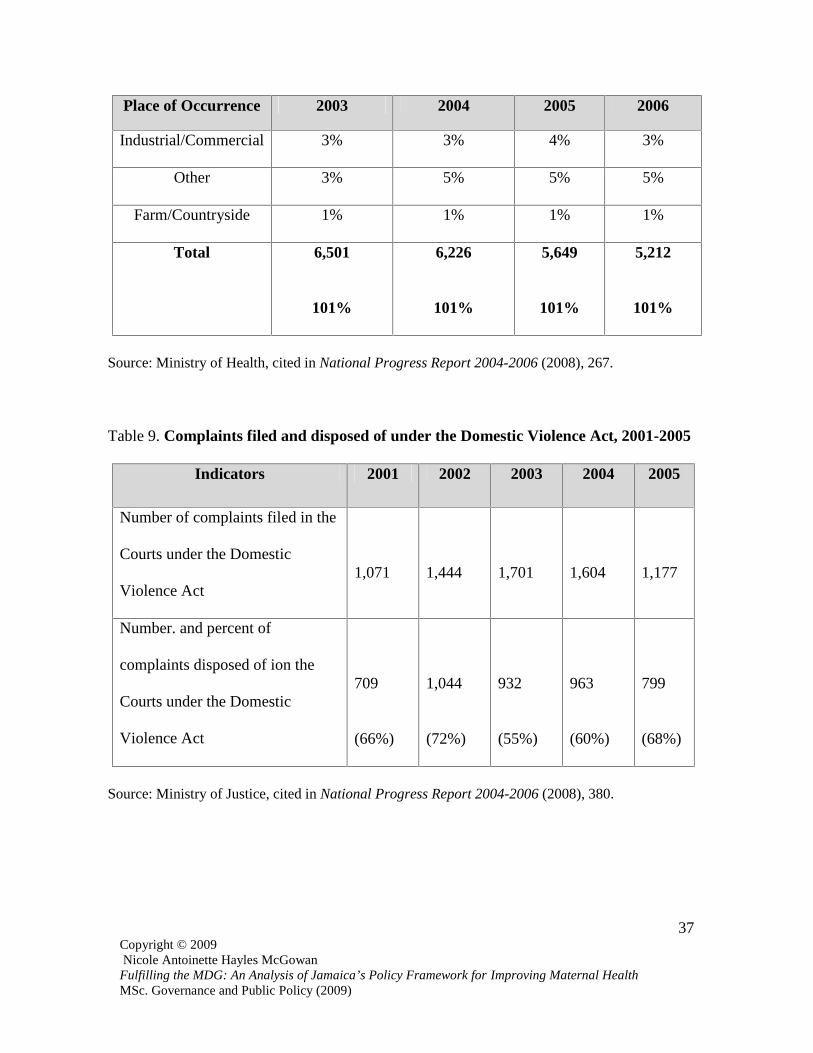
Table 8. Places of occurrences of injuries for females, 2003-2006
Place of Occurrence 2003 2004 2005 2006
Street/Public Area 34% 32% 33% 34%
Home 57% 57% 55% 54%
Institution/School 3% 3% 3% 4%
37Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Place of Occurrence 2003 2004 2005 2006
Industrial/Commercial 3% 3% 4% 3%
Other 3% 5% 5% 5%
Farm/Countryside 1% 1% 1% 1%
Total 6,501
101%
6,226
101%
5,649
101%
5,212
101%
Source: Ministry of Health, cited in National Progress Report 2004-2006 (2008), 267.
Table 9. Complaints filed and disposed of under the Domestic Violence Act, 2001-2005
Indicators 2001 2002 2003 2004 2005
Number of complaints filed in the
Courts under the Domestic
Violence Act1,071 1,444 1,701 1,604 1,177
Number. and percent of
complaints disposed of ion the
Courts under the Domestic
Violence Act
709
(66%)
1,044
(72%)
932
(55%)
963
(60%)
799
(68%)
Source: Ministry of Justice, cited in National Progress Report 2004-2006 (2008), 380.

38Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Table 10. Woman Inc. data, May-June 2009
Activities May June July
Calls to centre 14 15 10
Calls to centre forrape
4 0 0
Calls to centre forincest
0 0 0
Calls to centre onother issues7
8 11 10
Total 26 26 20
Visits to centre forabuse
5 5 1
Visits to centre forrape
0 0 4
Visits to centre forincest
0 0 0
Visits to centre forother issues
8 2 1
Total 13 7 6
Calls to hotline forabuse
2 3 6
Calls to hotline forrape
0 2 0
Calls to hotline forincest
0 0 0
Calls to hotline forother issues
15 19 13
Total 17 24 19
Source: Woman Inc. (2009).
7 Other issues relate to domestic violence, infidelity, marital conflicts, child molestation

39Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Table 11. Woman Inc. data, 2007-2009
Source: Woman Inc. (2009).
January 2007- December 2008
Domestic Abuse 423
Rape 64
January 2009- July 2009
Domestic Abuse 146
Rape 20

40Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Safe Motherhood in Jamaica
According to the Ministry of Health (2007), between 1996 and 2004, the proportion of
hospital birth increased from 86% to 95% respectively. Skilled attendance at birth was
also reported to be at 91%. Jamaica’s total fertility rate also declined to 2.5%, as teenage
fertility decreased from 112 per 1,000 live births to 79 per 1,000 live births. Jamaican
women, despite the disparity in urban and rural access and resource constraints, have
access to family planning and child care. In other words, Jamaica’s rating for maternal
and neonatal services is ranked 69 in the Maternal and Neonatal Program Effort Index
(MNPI) compared to the average of 56 for the 49 countries which are ranked on the
index; this rating thus placed Jamaica second in service delivery among all the 49
countries (Bulatao and Ross 2000). The MNPI is used to assess a country’s health care
services as well as track its progress over time (See Figure 3). Jamaica also has a
relatively low MMR, when compared to other Caribbean countries (See Table 12).
Figure 3. Comparison of global and Jamaica MNPI scores for selected items, 1999(Source: POLICY Brief. 2002. Maternal and Neonatal Program Effort Index: Jamaica)

41Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Table 12. Reported Maternal Mortality Rates in the Caribbean, 2000-2006
Country MMR (Maternal deaths per 100,000 livebirths)
Haiti 630
Dominican Republic 92
Antigua and Barbuda 0
Belize 130
Barbados 16
Bahamas 16
St. Kitts and Nevis 0
Guyana 120
Jamaica 95
Trinidad and Tobago 45
Dominica 0
Cuba 37
St. Lucia 35
Grenada 0
Source: UNICEF. 2008. Progress for Children: A Report Card on Maternal Mortality, 43.
Based on the figures presented in Table 7, it is clear that Jamaica is making strides in its
efforts to reduce its MMR, when compared to other Caribbean countries in terms of the
total number of births, particularly as Jamaica’s MMR remained static over a 20 year
period at 106/100,000; since 2005, local figures have indicated a decline to 95/100,000
42Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
(MOH 2007). However the WHO in its Maternal Mortality 2005 report cited Jamaica as
having a MMR of 170/100,000. The WHO was quick to caution however that their figure
was computed to ensure comparability amongst countries in a particular region, however
the figures presented may not necessarily be the official statistics of the country “which
may use rigorous methods” of assessment (WHO 2007, 24) .
While the major causes of maternal death in Jamaica continue to be hypertensive disease,
haemorrhage and sepsis, these direct causes have been declining over the past 4 years.
However indirect causes such as HIV/AIDS, violence8, and other chronic conditions such
as obesity and cardiac disease have been on the rise. Additionally, life stresses and their
impact on mental health have also increased, as suicide has accounted for some cases of
indirect maternal deaths in recent times (MOH 2009). Jamaica’s Safe Motherhood
Programme has been influenced by global initiatives to improve maternal and infant
health in the context of equity, poverty reduction and human rights, and is in keeping
with the MDG of reducing maternal mortality by 75% by 2015 (MOH 2007).
The public education component of Jamaica’s Safe Motherhood Progamme was officially
launched on July 1, 2009 at the Maxfield Park Comprehensive Health Centre; there were
however pre-implementation stages over the past two years in health centres and
hospitals with support from PAHO, UNFPA and WHO. Assistance from the international
8 Although cited here as an indirect cause of death, the Ministry of Health has no reporting system thatclassifies deaths due to violence.

43Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
organizations was in the region of $55 million9, however with contribution from the
Government of Jamaica pushed the amount to approximately $86 million. The
expectation of the programme is that by 2015 Jamaica’s MMR would be reduced by
75%, resulting in a decrease from 95/100,000 to 25/100,000.
Jamaica’s safe motherhood policy framework addresses four main areas:
1. Creating an enabling policy environment
2. Quality of care
3. Surveillance
4. Health Promotion.
Through the creation of an enabling policy environment, the government has committed
to: developing policy guidelines and standards for service delivery and the investigation
of maternal deaths; the revision of policies that guide the operations of midwifery
schools; address the issue of training, employment and retention of midwives and public
health nurses; as well as establish a national maternal mortality committee. By increasing
the quality of care the government has made a commitment to: drafting of guidelines for
the management of common obstetric emergencies; provision of equipment and supplies
for comprehensive care; the establishment of regional maternal mortality committees to
monitor quality of care in clinics and hospitals; the upgrading of hospitals to improve
care; as well as continuous education of doctors and nurses on various aspects of Safe
Motherhood. As it relates to surveillance the aim is for: a revision of the existing
surveillance guidelines, as well as the timely reporting and investigation of maternal; the
9 Figure quoted in Jamaican dollars

44Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
creation of a database for summary reports on maternal deaths, as well as continuous
monitoring an analysis of the causes of maternal mortality. Additionally, health
promotion, an integral component, is aimed at dissemination information about maternal
health through the use of various media as well as at the institutional level.
While the policy speaks to addressing issues critical to improving and addressing the
shortages in the delivery of care necessary for the overall physical well being of pregnant
women, the policy document however fails to address social issues that may affect a
woman while with child. The Ministry of Health’s Strategic Framework for Safe
Motherhood within the Family Health Programme 2007-2011 policy document, fails to
address issues such as “culture and customs which (places) limits (on a pregnant woman)
by withholding certain foods during pregnancy or encouraging unhygienic practices
(which might) increase the risk to mother and child. (The policy also does not speak to
issues such as) war, civil unrest and poverty (which) are other well known risk factors”
(Thomas 1993, 30).

45Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
CHAPTER 3
Research Objectives and Methodology
RESEARCH OBJECTIVES
Domestic violence against pregnant women is seen as a significant public health concern
and if not addressed there is the likelihood that it could affect the gains of countries in
achievement its target of reducing maternal mortality by 75% by 2015 (PAHO 2005, 1-
2). The aim of this research is to assess the social problem of domestic violence within
the context of the Ministry of Health’s Strategic Framework for Safe Motherhood within
the Family Health Programme 2007-2011 policy document. More specifically the
research paper aims to:
1. Assess the issue of domestic violence within the national policy framework for
safe motherhood.
2. Assess whether healthcare providers ask direct questions regarding domestic
violence within the context of healthcare delivery for pregnant women.
3. Increase awareness about the issue of domestic violence and its impact on
maternal health.
4. Identify recommendations that can be used to inform the policy framework about
domestic violence and its impact on maternal mortality.
46Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
The paper also aims to answer the following research questions:
1. What is the placement of domestic violence in the national health policy
framework?
2. Do healthcare workers routinely ask pregnant women direct questions about
domestic violence?
3. What is the impact of domestic violence on maternal health?
4. What policy adjustments are necessary to increase the awareness of the
importance of domestic violence?
5. Will the issue of domestic violence derail Jamaica’s efforts in achieving MDG5?
METHODOLOGY
This research paper is explanatory in nature. The research method employed is qualitative
in the form of elite interviews and focus group sessions. Interviews were conducted with
senior officials in Jamaica’s health care system including: Director of Family Services,
and Programme Officer at Ministry of Health; Professor, Reproductive Health
Epidemiology, University of the West Indies; Counselor, Woman Inc; Healthcare
providers at the Spanish Town. Focus group discussion was conducted with pregnant
women receiving antenatal care at the Spanish Town Hospital.
Elite interviews and focus group discussion proved the best research methods of choice to
collect specialized information about the issue of domestic violence and its impact on
47Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
maternal health, and the current policy focus. These research methods were also chosen
as there is currently no reporting mechanism that captures the issue of domestic violence
and its impact on maternal mortality in Jamaica.
QUESTIONNAIRE
The researcher’s choice of content for the questions asked in the elite interviews and
focus group sessions were informed by the myriad of literature reviewed (see appendix
for a copy of the questionnaires used during the elite interviews and focus group
discussions). The impact of domestic violence on the health of pregnant women and its
impact on maternal mortality were repeatedly explored therefore the researcher
incorporated the issues raised in the questions posed to the interviewees.
SAMPLE
The sample chosen for this research paper is the South-East Regional Health Authority
(SERHA) which accounts for one-third of the births in Jamaica. SERHA is one of the
four statutory bodies of the Ministry of Health. SERHA was established as a part of the
health sector reform through the National Health Services Act of 1997. SERHA is
responsible for the delivery of healthcare services to the residents of St. Catherine, St.
Thomas, and Kingston and St. Andrew, which represents 47% of the population of
Jamaica10.
10 http://www.serha.gov.jm/, retrieved July 28, 2009.

48Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
LIMITATIONS
Time- based on the magnitude of the issue of domestic violence and its possible impact
on Jamaica’s prospects towards achieving MDG 5, the three month period given to the
researcher to explore such a multi-faceted and multi-dimensional social problem that
possibly affects the lives of many Jamaican women was a major drawback.
Financial- this handicap prevented the researcher from visiting more healthcare facilities
and interviewing more health care professionals which fall under the jurisdiction of
SERHA.
Bureaucracy (access delay and denial)- the researcher experienced delays in accessing
the healthcare facilities which fell under the jurisdiction of SERHA to conduct the elite
interviews and focus group session. The delay was attributed to the series of criteria that
were outlined and had to be met by the researcher, before SERHA approved and granted
access. Access delays were also experienced at the Spanish Town Hospital, as the
researcher had to undergo another screening process, even though permission was
granted by SERHA which has overall responsibility for the facility.
Access was denied to the Victoria Jubilee Hospital and Comprehensive Health Centre on
Slipe Pen Road by the senior officers in charge of the facilities, even though SERHA,
which has overall responsibilities for these healthcare facilities, had granted the
researcher permission to conduct elite interviews and focus group sessions. The senior
officers in charge of the facilities were not willing to make the necessary arrangements to

49Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
accommodate the researcher.
The denial of access to the Victoria Jubliee Hospital and the Comprehensive Health
Centre, therefore limited the researcher’s efforts in obtaining feedback on the research
topic by more healthcare providers and women who visit the facilities for antenatal
services.
Gaps in data- there was difficulty securing maternal mortality statistics for Jamaica for
consecutive years. Data requested from the Registrar General’s Department was not
forthcoming; the Ministry of Health also did not have data sets for all the years requested.

50Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
CHAPTER 4
Findings and Discussion
FINDINGS
The results of the elite interviews and focus group discussion for this research paper are
presented separately in order for the responses of each group to be deciphered easily, and
each issue that will impact the objective outcomes and answer the research questions of
this paper are presented in italic headings. Three main groups were incorporated in the
study: technical experts, healthcare providers, and respondents of focus group discussion.
Technical experts refer to the group of persons involved in research and policy planning
for maternal health, and issues relating to violence against women. These individuals
have been working in their respective fields for an average of 14 years; range 3 to 25
years. Technical experts do not offer direct care to pregnant women, however they are
critical in informing and helping to set policy for women and the delivery of services in
the local healthcare system, as well as addressing the issue of violence against women.
Healthcare providers are those individuals who interface with pregnant women at a
localized level. They have been offering antenatal care for an average of 13.5 years;
range 1.6 to 27 years.
Healthcare providers each oversee the delivery of care to approximately 3,000 women
annually. The focus group involves women between the ages of 18 to 37 years old in
their first to fourth pregnancy who receive care at the Spanish Town Hospital. The

51Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
women were not asked direct questions about whether they were being abused due to the
sensitivity of the subject. They were however asked to give their general views on the
issue of domestic violence against pregnant women within the context of the MOH’s safe
motherhood programme.
TECHNICAL EXPERTS
Based on the responses of technical experts, it was apparent that they understood why the
issue of domestic violence was being raised by the researcher within the context of its
exclusion from the Ministry of Health’s Strategic Framework for Safe Motherhood within
the Family Health Programme 2007-2011 policy document. While not all respondents
agreed with the objectives of the research, it was apparent that they acknowledged that
the debate on the issue needs to be opened.
Domestic violence in the national safe motherhood policy framework
The general physical health of a pregnant woman is the primary focus at every antenatal
visit. This ensures accurate information about delivery date, blood pressure, weight and
urine analysis. Information is also gathered on whether the current pregnancy is the
woman’s first or if she has had past pregnancies and the relevant outcomes of those
pregnancies. Such inquires are important to assess the woman’s obstetric history, as the
most common complication in Jamaica relates to eclampsia and pre-eclampsia. Social
issues such as the woman’s living situation, and whether the baby’s father is present in
her life to offer support, are also discussed during antenatal visits.

52Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
The policy established for the delivery of antenatal care requires that each pregnant
woman has a maternal record booklet. This “maternal passport” records the history of all
the women’s pregnancy related medical history. The booklet has a section where the
primary care officer (midwives, public health nurse) records information relating to
obstetric problems. When such problems are detected the women are usually referred to
the nearest Type A or B hospital11 to be seen by an obstetrician. For mental related issues,
the women are referred to a mental health officer. The referred institutions or officer
would then write a report12.
The healthcare providers who initially gave the referral, would then give these women an
appointment to return to the community health centre one week later. If the women fail to
show up, the primary care officer or a community health aide conducts a home visit to
check for compliance with the referral, and if necessary, escort the women to the hospital.
In the event that the women need transportation, arrangements are made; this can
however sometimes be a problem as vehicles within the public health system are often
centralised.
As it relates to girls under 18 years old who become pregnant, the Child Care and
Protection Act (2004) dictates that prescribed persons, in this instance healthcare
providers, having an inclination of a person under 18 years of age being pregnant, must
11 Type A and B hospitals provide inpatient and outpatient services in: general surgery, general medicine,obstetrics and gynaecology, paediatrics, and anaesthetics.
12 Reports submitted to the MOH by the Regional Health Authorities, might not indicate that a referral wasmade, however based on the reporting format the MOH would decipher that a health problem was referred.

53Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
submit a report to the relevant authorities13. While the legal age of consent is 16 years old,
the healthcare provider is still duty bound to make a report as the girl is under 18 years
old.
In the event that a maternal death occurs, the death is to be reported to the parish health
department on suspicion and investigation initiated which includes: a home visit by a
midwife or public health nurse; a clinical report by the obstetrician or other health
provider handling the case; and a post mortem investigation. When these reports are in
place, a case review is to be held on conclusion of which a final report is to be submitted
to the MOH.
The technical experts have admitted that the policy established to guide safe motherhood
in Jamaica is lacking as it relates to addressing social problems that might affect pregnant
women in the realization of “true” safe motherhood. At present Jamaica relies on the
classifications from the WHO regarding what constitutes a maternal death. The country’s
policy framework therefore only focuses on four main areas:
1. Family planning- expanded contraceptive mix; prevention of unwanted pregnancies
2. Quality of care- staffing ratio; clinical guidelines; complications of pregnancy
3. Surveillance- monitoring maternal deaths; guidelines for timely reporting
4. Health promotion- educating women and the public about safe pregnancy.
The policy mostly focuses on the health needs of the women related to pregnancy and
childbirth. The technical experts noted that given the resource constraints of the MOH, it
13 These include the police, child services, MOH, etc

54Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
is difficult to expect the policy to address all the needs of the pregnant women which go
beyond addressing their immediate healthcare concerns. The policy’s main strength the
experts assert, is that it attempts to comprehensively address the health problems by
developing guidelines and ensuring that the staff is adequately trained to deal with the
leading complications of pregnancy.
One technical expert noted that for the policy to address social issues it will depend on
what the issues are. There are the usual referrals for support from the National Health
Fund, if there is a co-existing chronic disease to provide help with financing prescription
drugs. Initiatives such as the Programme for the Advancement through Health and
Education (PATH) is also in place to assist pregnant and lactating women maintain
adequate nutrition. Some NGOs also provide additional help to families in need, however
this varies based on location. The technical expert therefore noted that it might be unfair
to expect the MOH to address the social issues affecting pregnant women, as that is not
the purview of the MOH. It was noted that other social sector ministries and agencies
need to take on such responsibilities with appropriate strategies for referring at risk
persons to the appropriate agency that is able to address the women’s specific social
needs.
Another technical expert noted that if domestic violence were to be included in the
policy, the country’s RAMOS would have to be modified to capture the impact of
domestic violence on safe motherhood, as often times, the issue of violence may

55Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
sometimes be seen as anecdotal. There was also the point that even if domestic violence
were to be included in the reporting system, it might be ranked very low on the list of
causes of maternal death based on financial constraints, as there will be the tendency to
focus on more immediate causes of death.
While domestic violence may be a cause of psychological distress to some pregnant
women and may be a source of physical pain and discomfort, there is currently no data to
support this, as the impact of domestic violence on pregnant women is not a priority area
within the safe motherhood agenda14. One technical expert noted that in the case of death
due to accidents and violence, there are more deaths related to motor vehicle accidents,
which the technical expert believes, more emphasis should be placed in developing a
strategy for educating pregnant women about the safe use of the roads during pregnancy,
as this is currently is not addressed in the policy. There is also the recommendation of a
strategy to deal comprehensively with the issue of suicide among pregnant women which
is also not addressed within Jamaica’s Safe Motherhood Programme.
Antenatal care and domestic violence
A protocol does not exist to address domestic violence during pregnancy. The discussions
in the Ministry of Health’s Strategic Framework for Safe Motherhood within the Family
Health Programme 2007-2011 policy document focuses on maternal self care related to
pregnancy, identifying the complications of pregnancy, and the appropriate responses
regarding health seeking behaviour. While healthcare providers might try to ascertain if
14 National data ascertained for this research paper also did not disaggregate the data to indicate the impactof violence against pregnant women

56Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
the women are experiencing problems at home, direct questions about domestic violence
are not asked, as there are no policy guidelines to conduct such enquires.
Guidelines by the WHO about what constitutes a direct or indirect maternal death, is the
criteria used by Jamaica to monitor issues of safe motherhood. The current parameters
do not include domestic violence in the classification of deaths. While the MOH
documents all maternal deaths, those that are a result of domestic violence are not
classified as such, as there are no criteria. For example, a woman had a fight with her
spouse and her blood pressure went up and later died on arrival at hospital, while another
had a fight with her partner and was kicked in the abdomen and also died. Based on
national figures these deaths would not be classified as being attributed to domestic
violence. The former case would be classified as death by eclampsia, even though it was
the fight that caused her blood pressure to rise. The latter case would be classified as
placenta abruptio, even though it was the act of a physical blow to the abdomen that
caused the death.
One of the technical experts interviewed noted that the main ethical challenge with
screening for any health condition is whether the capacity exists to diagnose and then
treat. While the MOH might be able to address the acute consequences of domestic
violence such as treating injuries, managing the social consequences of domestic violence
are outside the purview of the MOH. It was also noted that domestic violence alone
cannot be taken into isolation as homicide and suicide amongst pregnant women must
57Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
also be included in the discourse.
The maternal mortality surveillance of 2001-2003 highlighted two to three deaths of
pregnant women who were the partners of ‘dons’ from the inner-city; the reasons why
these women were targeted was however not explored. As for suicide among pregnant
women, the MOH has not created any mechanism to capture evidence for the reasons
why women commit this act. For example, a 16 year old girl got pregnant and committed
suicide by drinking the pesticide gramoxone. While there was no concrete evidence,
investigations suggested that the girl drank the pesticide because her boyfriend had
rejected her. The technical expert argued that until there are services and programmes in
place to assist victims of violence and abuse in a serious and comprehensive manner, then
the issue cannot be addressed wholesomely, otherwise it is unethical to screen.
It was further articulated that the MOH also has to develop a clear definition of what is
domestic violence. One of the challenges is that domestic abuse has both physical and
mental health components, the latter of which is more difficult to measure. Issues such as
verbal abuse and neglect need clear indicators and criteria for measurement, even though
the measurement and reporting of physical abuse is not necessarily straight forward.
Clear guidelines would therefore have to be developed.
There is also the issue that pregnant women who will not speak, ignore or lie about being
abused. Such silence or disregard on the part of the pregnant women, might create
difficulties for healthcare providers to identify that there is a problem. One technical

58Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
expert pointed to the three delay model which speaks to: the woman not recognizing that
there is a problem; recognizing that there is a problem but delay getting care; and
recognizing that there is a problem, go to get care, but there is a delay in accessing care at
the healthcare facility. These delays, it was noted, have to be resolved before even
scratching the surface in trying to address the problem.
There is also the concern about the lack of shelters or existing social programmes to send
these pregnant women if there are screened during antenatal visits. The shelters that are
operated by voluntary organizations are often times inadequate, and in some instances
might depreciate the quality of life to which the women might be accustomed. It is also
believed that asking pregnant women direct questions about whether they are being
abused by their partners might cause anguish, as there is currently nothing to offer these
women.
One technical expert noted that one particular non-governmental organization which
offers outreach services for abused women, would be hesitant in accepting a pregnant
woman at its shelter. Housing at the shelter is temporary and lasts for two weeks; an
extension may be granted, however each case is evaluated based on its own merit. In the
case of a pregnant woman, she would be accepted at the shelter if she is employed. The
technical expert noted that the woman’s having employment is critical, because if she is
not, the organization may deem the woman to be an inappropriate candidate as she will
more likely expect to stay for more than the two week period. Also based on her physical
state, it might be difficult for her to attain employment, thereby causing her to be a

59Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
“burden” to the facility.
Based on the current reality, one technical expert noted that they would never include the
issue of domestic violence in a strategic plan as it is not a priority; resources are limited
therefore there has to be focus on the most critical and immediate needs for pregnant
women. The other experts argue however, that such an inclusion would have to be
considered based on the evidence gathered from a comprehensive research.
Domestic violence and its impact on maternal health
The changing epidemiology of maternal deaths in Jamaica, that is a decrease in direct
while there is an increase indirect causes, requires constant modification of the strategies
aimed at reducing maternal deaths. Reducing indirect deaths caused by heart disease,
HIV/AIDS, and diabetes, will require lifestyle modifications aimed at reducing
overweight, obesity and unsafe sexual practices. The technical experts note that reducing
exposure to the risk of dying from these conditions is however difficult to bring about in
the short term. The inability to control these lifestyle related disorders, will therefore
make achieving MDG 5 a difficult goal to attain.
It was also noted that the MDGs were set on a global scale. The technical experts believe
that the target of MDG 5 of reducing maternal mortality by 75% is more geared towards
Sub-Saharan Africa where MMR is high (See Tables 1 and 2; Figure 1); a 75% reduction
would therefore be more critical for them. The ‘one-size fits all’ approach is therefore

60Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
seen as inappropriate. The technical experts say that for a middle income country like
Jamaica to reduce its MMR by 75% by 2015 is unattainable, as the country would have to
attain an MMR like that of the developed world (See Tables 1 and 2; Figure 1).
It was also noted that based the economic situation in Jamaica and the availability of
limited resources also makes the target an impossible one. More effort and resources need
to be directed toward training healthcare providers to improve the outcomes from the
leading direct complications (hypertension, haemorrhage, abortion, embolism), as well as
including improving access to tertiary intensive care for women with acute complications
which require ventilatory support. It was noted that each health region should have access
to high dependency unit beds in order to manage these women without the need for long
distance transfer to Kingston or Montego Bay.
The need to address the shortage of staffing for maternity wards due to migration was
also an issue that needs to be addressed. One technical expert noted that the removal of
user fees was not a good decision, as this policy directive has limited the resources
available to the sector. Persons with health insurance which could be used to reimburse
the health sector for services provided to insured persons are not being billed, thereby
denying the public health sector of well needed facilities and economic resources.
Despite the challenges, Jamaica’s MMR is said to be below the average of the Caribbean
and Latin America (See Table 13), as Jamaica is not doing badly when compared to
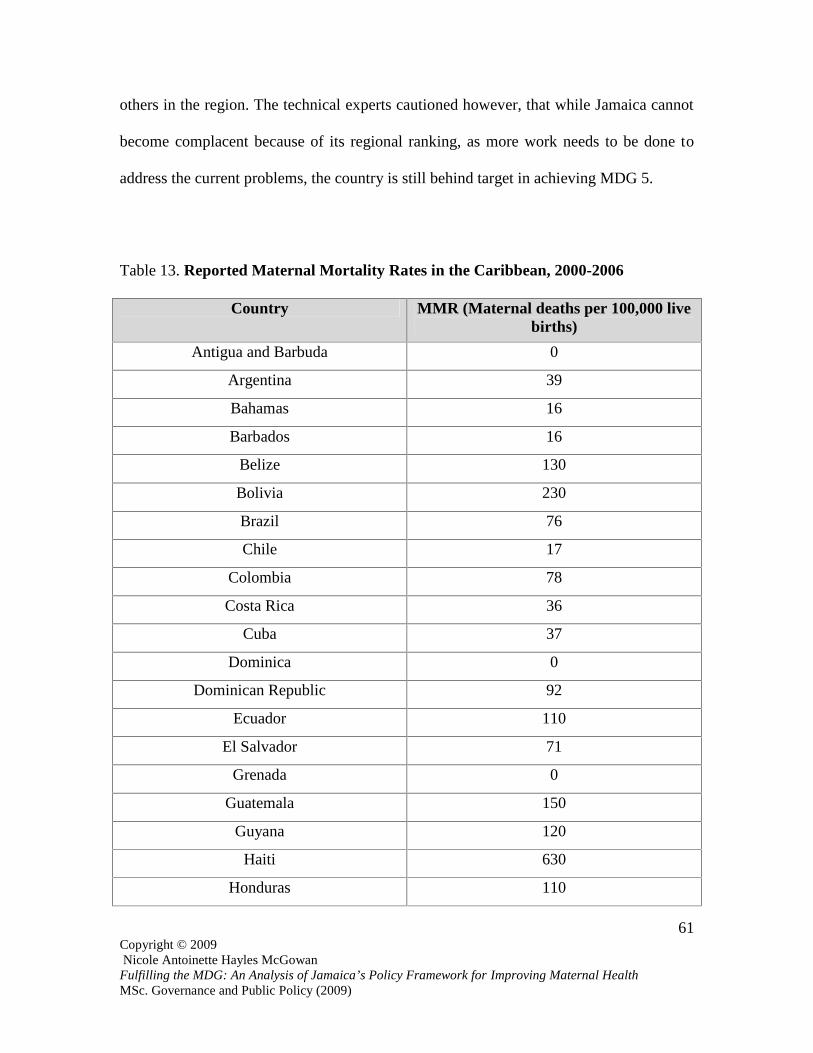
61Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
others in the region. The technical experts cautioned however, that while Jamaica cannot
become complacent because of its regional ranking, as more work needs to be done to
address the current problems, the country is still behind target in achieving MDG 5.
Table 13. Reported Maternal Mortality Rates in the Caribbean, 2000-2006
Country MMR (Maternal deaths per 100,000 livebirths)
Antigua and Barbuda 0
Argentina 39
Bahamas 16
Barbados 16
Belize 130
Bolivia 230
Brazil 76
Chile 17
Colombia 78
Costa Rica 36
Cuba 37
Dominica 0
Dominican Republic 92
Ecuador 110
El Salvador 71
Grenada 0
Guatemala 150
Guyana 120
Haiti 630
Honduras 110

62Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Country MMR (Maternal deaths per 100,000 livebirths)
Jamaica 95
Mexico 62
Nicaragua 87
Panama 40
Paraguay 170
Peru 190
St. Kits and Nevis 0
St. Lucia 35
St. Vincent and the Grenadines 0
Suriname 150
Trinidad and Tobago 45
Uruguay 26
Venezuela 60
Source: UNICEF. 2008. Progress for Children: A Report Card on Maternal Mortality, 43.
Despite Jamaica’s progress in reducing its MMR, social issues such as poverty, crime and
violence were cited as subjects that need urgent attention, as pregnant women are
sometimes unable to leave their communities to access care because of these social ills.
The majority of technical experts noted that there is a possibility that domestic violence
might derail Jamaica’s prospects in achieving MDG 5. They noted however that despite
there being no data to give credence to the impact of domestic violence on maternal
mortality, the issue must not be disregarded. Crime and violence are major public health
issues, which the technical experts believe not only affects safe motherhood, but also the

63Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
delivery of healthcare. It was noted however that data is needed to inform the decisions
that may be necessary to address the problem if it exists.
One technical expert was however strident in noting that Jamaica’s failure to address
domestic violence will in no way derail the country’s prospects of achieving a reduction
in maternal mortality, as the direct contribution of domestic violence to maternal deaths is
negligible. The technical expert noted that domestic violence is more of an issue of
maternal morbidity than maternal mortality, therefore it will not in any way affect
Jamaica in reducing its MMR by 75% by 2015. It was also noted that there needs to be
more investment in improving the quality of the current obstetric services, before the
MOH moves into an area which is outside its direct control to efficiently and effectively
improve outcome. The technical expert notes that the issue at hand is how much domestic
abuse, verbal abuse and neglect contributes to unwanted pregnancy, maternal morbidity,
and poor maternal interest in seeking antenatal care, as well as complying with the
directives of the healthcare providers.
HEALTHCARE PROVIDERS
Based on the responses of healthcare providers, it was apparent that they understood why
the issue of domestic violence was being raised by the researcher within the context of its
exclusion from the Ministry of Health’s Strategic Framework for Safe Motherhood within
the Family Health Programme 2007-2011 policy document. It was apparent however that
some healthcare providers did not know what the term “safe motherhood” meant, as they

64Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
were accustomed to word “antenatal care”, which is a component of safe motherhood.
While not all respondents agreed with the objectives of the research it was apparent that
they acknowledged that the debate on the issue needs to be opened.
Domestic violence in the national safe motherhood policy framework
The general issues discussed by healthcare providers with pregnant women to whom they
offer care are: personal hygiene, nutrition and diet, layette, signs and symptoms of
pregnancy, and attire during pregnancy. Issues relating to delivery date, blood pressure,
weight and urine analysis is also discussed. Healthcare providers also speak with women
about their obstetric history of they have had previous pregnancies.
Healthcare providers adhere to the policy protocol as outlined in the responses given by
the technical experts above. In SERHA all high risk patients are referred to the Victoria
Jubilee or Spanish Town Hospitals.
The healthcare providers with whom the researcher spoke, said they did not know of the
Ministry of Health’s Strategic Framework for Safe Motherhood within the Family Health
Programme 2007-2011 policy document. They also noted that the term “safe
motherhood” was foreign to them, as they have never heard the term until the researcher
used it. The healthcare providers added that they have not received any training or
sensitization from their regional health authorities or the MOH regarding the term “safe
motherhood”. The healthcare providers noted however that they are familiar with the
term “antenatal care”, which is what they are accustomed to, and which is what they use

65Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
when they speak of issue relating to maternal health. The healthcare providers have
suggested that they be sensitized and made aware of the issue of safe motherhood, as it
was the researcher who explained that the provision of antenatal care is only a component
of safe motherhood.
Despite the confusion of terminology, the healthcare providers were ambivalent as it
related to the exclusion of domestic violence in the MOH’s strategic framework for safe
motherhood. Some healthcare providers noted that it would be unethical to diagnose a
problem if there is no capacity to treat, as often times there are no relevant agencies to
which patients would be referred. They cited for example the inadequacy of healthcare
facilities to adequately report incidences of girls under 18 years of age who are pregnant
and attend healthcare facilities to get care. While the Child Care and Protection Act
(2004) stipulates that a report be submitted and the relevant authorities notified, some
healthcare providers noted that the issue is not being addressed wholesomely, as reports
are sometimes not submitted on time, which can cause delays in the relevant authorities
being made aware of the situation.
Some healthcare providers believe however that the issue of domestic violence should be
addressed by the safe motherhood policy. They noted that the MOH should implement
systems, so that when the diagnosis is made the healthcare provider refers the pregnant
women to the appropriate agencies which deal with social issues. The healthcare
providers were quick to caution that dealing with social issues should not be the purview
of the MOH. They explain that issues relating to self respect, self esteem and many of the

66Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
social ills such as crime and violence that are affecting Jamaica are “too big” for the
MOH to undertake and fall outside the purview of the Ministry. They noted however that
the Ministry, though it is not its responsibility, should play a role in helping to address the
problem.
The healthcare providers note that much of the problem of domestic violence in Jamaica
has to do with the issue of some women not being motivated and have little self respect.
They argue that is evident in the values that these women have as they continue to see too
many underage pregnancies and the mothers of these young girls failing to report the men
who have impregnated their daughters. The healthcare providers note that such behaviour
perpetuates abuse against womenand this they add will not stop even when the women
become pregnant.
Some healthcare providers also note that for the issue of domestic violence against
pregnant women to be adequately addressed, the MOH has to revises its HIV policy. The
healthcare providers say that when a person is diagnosed with HIV the MOH should
contact the person’s partner, as the issue of ‘patient confidentiality’ can foster abuse. One
healthcare worker noted that in treating a woman is HIV positive and recently gave birth
(the woman had not informed her partner about her status), the healthcare provider said
the woman was told to tell the woman to tell her partner that she is unable to breast feed
the baby because she is hypertensive. The healthcare provider says that with the woman
withholding her status from her partner, it might cause the man to abuse the woman. The
healthcare provider noted that if the MOH’s HIV policy were revised, then the healthcare

67Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
provider could have informed the man and get counselling for both parties.
Antenatal care and domestic violence
The healthcare providers note that they do not discuss the issue of domestic violence with
pregnant women when they visit them for antenatal care. They explain that there is no
policy protocol that exists, therefore they do not go outside the realms of what they are
mandated to do. The healthcare workers also say that they have not received any training
on how to detect when and if a woman is being abused, whether or not she is pregnant.
They note however, that while they have knowledge to detect when woman are being
abused, they say no training is given to them, therefore they do not venture into an area
outside what they are required to do, which is to offer care towards the physical health of
pregnancy as stipulated by the MOH.
Some of the healthcare providers explain however, that if the pregnant women confide in
them and tell them that they are being abused they refer them to get counseling; this is
however voluntary as the women are not compelled to get such assistance as they do so
on their own volition. Other healthcare providers noted that at times they do observe
signs of physical abuse on pregnant women to whom they offer care, and are often times
compelled to ask these women if they are in fact being abused. The healthcare providers
said however that they do not ask, out of fear that the abused pregnant women might
inform their partners about the healthcare providers’ enquires, and these partners would
then possibly physically harm the healthcare providers when they see them on the road.
68Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
The healthcare providers note that while they have observed, on occasions, pregnant
women showing signs of physical abuse, they are caught in a quandary which makes
them turn a blind eye to what they observe, even though they know that the matter needs
to be addressed, but this they say is done out of fear for their own safety. The healthcare
providers also note that it is also difficult to ascertain if a pregnant woman is being
verbally abused; this is only know if the woman speaks about it, and if she does she is
referred to get counseling which is solely her decision to accept or reject.
Domestic violence and its impact on maternal health
The healthcare providers noted that more effort needs to be done in encouraging women
to seek early antenatal care. They note that despite the elimination of user fees at health
facilities the numbers that give birth at hospitals come pared to those who receive
antenatal care is not comparable. They note that pregnant women receiving early
antenatal care will assist in detecting complications early, so that healthcare providers can
make the necessary referrals. It was also noted that more facilities such as bed spaces,
wards and resources are needed, as well as more healthcare workers which are critical to
the delivery of care for pregnant women.
The healthcare workers also note that they have seen instances where financial resources
have been pumped into the sector targeted towards family planning and reducing
HIV/AIDS, yet they say pregnancies are still increasing as well as the number of HIV
cases. The added that, while not exorbitant, some amount of money is being spent on

69Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
helping to reduce Jamaica’s MMR, yet they are not seeing the results. The healthcare
providers questioned whether the correct target audience was being reached, whether the
efforts were not being fruitful because of social stigma, or if it had to do with the lack of
alacrity politicians display regarding issues affecting women, why Jamaica’s efforts were
not reaping the desired results.
The healthcare providers noted that while the issue of domestic violence against pregnant
women is an issue that must be addressed at the policy level, they say however that they
do not believe that this social problem will derail Jamaica’s efforts in achieving MDG5
by 2015. The say that while there are no statistics to evaluate the extent of the problem,
they say based on their observation, the incidence of domestic violence against pregnant
women are isolated.
The healthcare workers further espoused that the issue of domestic violence needs to be
addressed at the community level, because until women realise that something is wrong
with men battering them, whether or not they are pregnant, there is hardly anything the
government can do to stop the problem. They explain that while it is the responsibility of
the government to enact legislation to protect women, women themselves have to speak
up and acknowledge that the issue of abuse is a problem.

70Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
FOCUS GROUP RESPONDENTS
Based on the responses of the women who participated in the focus group discussion, it
was apparent that some of them believe that the existing Ministry of Health’s Strategic
Framework for Safe Motherhood within the Family Health Programme 2007-2011 policy
document does not address issues they deem important to their overall pregnancy
experience. While the women were not asked direct questions by the researcher whether
or not they were being abused by their partners, due to the sensitivity of the topic and the
researcher having no written protocol that would guide such enquires, the discussion
however brought to the fore the importance, as viewed by the women, for the inclusion of
addressing the issue of violence against women within the safe motherhood agenda.
Domestic violence in the national safe motherhood policy framework
The women note that when they visit healthcare facilities for antenatal care they are
asked general questions regarding their health. The respondents say they are asked
whether they have diabetes, hypertension, or have physical disabilities. They are also
asked questions about their family health history, when they had their last period, diet, if
they are taking their vitamins or prescribed medication (if necessary), they are asked if
the baby has moved, information regarding their next of kin, information regarding blood
donor. One woman noted that she has also been asked if she lives with her partner.
The women note that when the healthcare provider detects a problem, they are informed
of the treatment they will receive. They say in some instances, they are told of the
treatment and they get to choose whether or not they want the treatment. However in

71Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
instances where the treatment is necessary to save both the mother’s and baby’s life, the
woman is told of the treatment she will receive, however she cannot choose whether or
not she wants the treatment that the healthcare provider will administer. One respondent
who said she had a low blood count, noted however that she was told of her situation,
however no treatment was administered as she said she was told that there is no treatment
for her condition.
The focus group respondents noted that while they were not aware, and had never heard
about the MOH’s strategic framework for safe motherhood until the researcher explained
the policy, they believe however that the issue of domestic violence and other social
problems pregnant women might face should be addressed.
The women note that they have seen instances in which women have been abused by
their partners while pregnant. One respondent noted that she witnessed one of her aunts
being abused by her child’s father while pregnant. The woman noted that the abuse of not
an isolated incident as it happened repeatedly. The woman’s aunt, while she gave birth to
the child safely, failed to report the matter to the police or seeking help. The woman
noted that while family members have witnessed the psychological impact the abuse has
had on her aunt, she has however failed to seek assistance. In such an instance they
women note that systems should be in place to address the issue.
They note that while the MOH might not have the resources to address the issue of
domestic violence, they argue however that something has to be done to address the

72Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
social problems might affect the well-being of pregnant women, as not enough is being
done. The respondents also cited a recent court case published in a popular newspaper,
where a woman was badly beaten by her partner, yet when he appeared before a
magistrate he was fined a mere $10,000.00.
The focus group respondents also note that issues such as crime and violence in
communities, and poverty which can prohibit them from attending their antenatal visits,
also needs to be addressed. They note that while the social issues they have raised might
fall outside the purview of the MOH, the women note however that the Ministry has to
lead the way and liaise with the appropriate agencies as safe motherhood has to be
addressed wholesomely, and pregnant women need all the support they can get to make
motherhood safe.
Antenatal care and domestic violence
The women say they have never been asked about the issue of domestic violence while
receiving antenatal care. While the women noted that this was an important issue to
address during antenatal visits, they had varying views on the matter.
One woman was quick to point out that she does not believe that healthcare providers
should make such enquires, as doing so could risk the healthcare providers’ safety. She
noted that there have been instances in her community where she has witnessed a woman
being abused by her partner and neighbours intervene by calling the authorities, yet the
abused woman in turn lashes out against the neighbours for “fassin’ inna har bizniz”. The

73Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
respondent noted that while the healthcare workers might have the abused pregnant
woman’s interest at heart, the abused woman might not view the situation as such, and
could possibly push her partner or associates to attack the healthcare provider. The other
respondents in the focus group noted that while they understood the safety concerns of
healthcare providers, they say those offering them care, particularly while they are in the
process of fostering a new life, have an ethical responsibility for the overall well being of
their patients.
The respondents note that while some healthcare workers do not want to get involved in
the social welfare of expectant mothers, they believe however that enquires about
domestic violence should be made. This the women say is important particularly as the
women are bringing forth a new life; the health of the woman is important for the health
of the baby. They also note that healthcare providers must move beyond the realms of
physicality and focus must also be placed on the mental health of pregnant women. The
respondents note that making such enquires might also help healthcare providers finding
out the cause of some of the ailments that pregnant women might have such as high blood
pressure, as they note that it could be the woman’s situation at home which has caused
her blood pressure to elevate.
The women admitted that while there might be instances in which the healthcare
providers ask such direct questions and the women lie, the respondents noted however
that the healthcare providers, being the professionals they are, can detect signs of abuse.
They say where necessary the healthcare providers should make the appropriate referrals

74Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
for treatment or counseling. They also added that in instances where there needs to be
intervention by the police, that should be done with or without the abused woman’s
consent.
Domestic violence and its impact on maternal health
The respondents of the focus group discussion noted that they had never heard of the
term “maternal mortality” until the researcher used the term and explained what it meant.
The women also note that they had never been told of the possible health complications
that can lead to maternal death by their healthcare providers. It was therefore difficult for
the researcher to ascertain the pregnant women’s feedback regarding Jamaica’s efforts in
achieving MDG 5, and if they thought the issue of domestic violence would derail the
country’s efforts in meeting the 2015 target. The women noted however that would like
to see more discussion about the issue of domestic violence being done by their
healthcare providers, as they note that the effects of domestic violence might have
devastating effects for a pregnant woman and the unborn child.

75Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
DISCUSSION
It is apparent, based on the findings of the researcher, that the views regarding the issue
of domestic violence and its impact on maternal mortality varies depending on the target
group.
The technocrats who have crafted the MOH’s policy framework on safe motherhood, and
those involved in directly administering care to pregnant women, while they recognize,
for the most part, that domestic violence against pregnant women might be a possible
threat to the well-being of these women, there is however some degree of ambivalence in
addressing the matter. The researcher concedes that the spectrum within which to tackle
the issue of domestic violence falls outside the purview of the MOH, the safe motherhood
agenda must however encompass a wholisitc approach in dealing with all the issues that
makes motherhood safe.
It is also apparent, based on the tone of the responses, particularly of the crafters of the
policy document, that a bottom-up approach was not adopted in the formulation of the
policy. In today’s modern society it is important to incorporate the views of the target
audience which the policy being crafted is expected to enhance their quality of life. While
not all recommendations posited by this group might be incorporated in the policy
document, if any at all, it is important to garner insight from those which the policy will
ultimately affect.
While the issue of domestic violence is not addressed in the Ministry of Health’s

76Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Strategic Framework for Safe Motherhood within the Family Health Programme 2007-
2011 policy document, as the technocrats have cited its exclusion as “not a priority”, and
outside the classification of the WHO, the women whose healthcare depends on the
stipulations articulated within the document have noted that such a social issue should be
addressed. Jamaica cannot afford to take a one-sided approach to safe motherhood by
only focusing on the medical aspects of pregnancy, as in doing so, other critical
components, which could possibly derail Jamaica’s efforts in achieving the MDG 5 target
might be overlooked. While the responses gathered in this study do not indicate that the
issue of domestic violence will derail Jamaica’s efforts in reducing its MMR by 75% by
2015, the lack of data and the classification of deaths attributable to domestic violence
makes the impact of the social problem on the country’s MMR inconclusive to determine.
As the De Brouwere (1998) model states, which is seen as the hallmark in highlighting
strategies for reducing maternal mortality by expounding the best practices of the
developed world (McCaw-Binns 2005), “developing countries (must not be) hindered by
the limited awareness of the magnitude and manageability (of addressing maternal
mortality, as) ill-informed strategies focusing on antenatal care…have by and large been
ineffective”. Those responsible for the crafting of policy guidelines and the delivery of
care must therefore move beyond the realms of their limited scope and adopt a more
comprehensive approach in addressing safe motherhood.
Likewise, there must be political will to address the issue of domestic violence, as this
has to be done with clear and concrete political and social strategies that are imperative to

77Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
an adequate knowledge base of the social problem (Richmond and Kotelchuck 1985;
Atwood et al 1997, cited in De Brouwere et al 1998). Increased awareness of the
population about the problem is also important as putting the maternal mortality agenda
at the forefront of public discourse is important for more persons to be aware of the
problem. This can be further augmented through strong political will, and through
parliamentarians addressing the issue in Gordon House with alacrity like so many of
Jamaica’s other problems.
The magnitude of the effects of domestic violence on maternal mortality needs greater
discussion, as this study was carried out at only one healthcare facility within the South-
East Regional Health Authority. It is therefore possible that the findings from other health
regions might be different. Research is also needed to assess how domestic abuse, verbal
abuse and neglect contribute to unwanted pregnancy. There also needs to be research on
how domestic violence affects maternal morbidity (the grave impacts on maternal health),
as well as how domestic violence contributes to poor maternal interest in seeking
antenatal care and complying with the directives of healthcare providers. It would also be
interesting to ascertain how other social problems such as crime and violence and even
poverty will impact Jamaica’s prospects in achieving MDG 5. The issue of culture,
customs and religious beliefs must also be explored to ascertain whether these might also
affect a women’s health seeking behaviour for maternal care.
78Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
CHAPTER 4
Conclusion and Recommendations
The issue of domestic violence and its impact on maternal mortality in Jamaica needs
greater discourse, as the issue must not be seen as a sideline item simply because the
WHO does not recognise it in its classification of what constitutes maternal deaths or it is
“not a priority” by policy planners. Despite Jamaica being a small developing state, it is
often times seen as a pioneer in the Caribbean region for making headway in the areas of
discourse and policy planning (World Bank 2009). More research and statistics regarding
the impact of violence against pregnant women need to be developed and disaggregated
in the presentation of national figures. Likewise, the following recommendations should
be considered, and possibly incorporated in strategies aimed at addressing the issue of
domestic violence against pregnant women in future policy developments.
1. A national committee should be developed which would hold discourse and make
recommendations targeted towards a wholisitc approach towards safe motherhood.
This committee would comprise of representatives from the Ministry of Health, the
Bureau of Women’s Affairs, the Ministry of Labour and Social Security, other
government agencies armed with the responsibility of providing social services,
non-governmental organizations which focus on women’s issues and civil society.
A wide representative panel on the committee will foster a wider debate on the
issues that affect women during pregnancy, as well as allow varying views to be
brought to the fore in policy planning for maternal health.
79Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
2. In formulating a strategy to address the issue of domestic violence against pregnant
women, strict guidelines regarding privacy and confidentiality must be maintained
by those offering care. Social capital is therefore an important ingredient in crafting
such a policy, as it is likely that the pregnant women will not buy-in to the
programme if their identities and their accompanying problems are revealed.
3. Social programmes needed to address the issue of domestic violence must to be
strengthened if screening is to take place. Diagnosis cannot take place if there is no
proper medium to treat, however if left unattended the problem might be
exacerbated.
4. Violence against pregnant women remains unrecognized, therefore it is important
that during the delivery of care healthcare providers develop a “sensitive ear” (Edin
and Högberg 2002). A policy framework which would guide the creation of
standardized questions that healthcare providers would ask, needs to be developed.
The issue of domestic violence can only be tackled if there is knowledge that the
problem exists by policy planners, healthcare providers and the pregnant women
that are being abused.

80Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
5. Training and educating healthcare workers about domestic violence is critical, as
these professional interface with pregnant women frequently. Those who provide
care to pregnant women need to learn more about the problem as well as assess
their own attitudes towards domestic violence. Education related to violence can
help change negative attitudes that can assist in making a difference in healthcare
providers’ behaviour toward the issue (Moore et al 1998, Ellsberg et al 2001, cited
in Edin and Högberg 2002). The education should also be expanded to technocrats,
as those involved in setting the policy agenda for the treatment and delivery of care
to pregnant women must also be educated about the issue.
6. Greater sensitization is needed about the issue of safe motherhood, not only for
healthcare workers but for pregnant women as well. There needs to be wider
discourse on MDG 5 by all stakeholders, and not just those who set the policy
framework.
7. Political will is also an important ingredient in tackling the problem (De Brouwere
et al 1998). In Jamaica it is evident that polices and programmes that have the
strong and visible support of politicians often times receives the blessings of the
masses. A strong buy-in by politicians is therefore seen as important in driving the
issue.

81Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
8. RAMOS should be revised to incorporate the classification of maternal deaths
which are a result of domestic violence. Guidelines for the amendment of the
surveillance system would have to be developed and best practices adopted from
countries which have informed research on the impact of violence against pregnant
women.
9. The impact of domestic violence on maternal morbidity also needs analysis, as there
might be instances where violence against pregnant women may not lead to death,
but may have grave impacts maternal and fetal health.
Maternal mortality is not the only outcome with which progress towards MDG 5 will be
judged as all the eight goals are intertwined. The discourse on maternal mortality must
therefore incorporate a continuum of all the social systems needed to enhance the quality
of life women lead (Ronsmans et al 2006, 1189). While the unavailability and quality of
data and information needed to inform decisions, evidence about the issue and its
possible impact must be guided by informed awareness. To disregard an issue that could
possibly derail social progress in any country cannot be held as an ideal in today’s
modern society, even if it is not seen as a priority for those who hold the power to craft
the decisions which will dictate the quality of life people lead. The constraints that exists,
particularly as Jamaica faces tumultuous economic times, the country cannot be forced to
dwell on the false impression that a problem that affects only a few today cannot be
exacerbate and a future implications for many.

82Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Capturing the causes of maternal deaths is not straight forward, as even in countries
where there are highly developed statistical and data gathering instruments, there are still
constraints (Ronsmans et al 2006, 1197). Women however need to know that there are
systems in place to protect them at all levels of their life, as often times it is the most
vulnerable in society that is left to suffer. While we do not have all the answers, a
concerted effort must be made to address problems that may exists as can assist persons
in possibly attaining the fulfillment of true development.
The proposals and recommendations put forth in this paper do not have all the answers,
neither does it purports to be the magic bullet, the research however feels that “no woman
should die giving life” (UNFPA 2009c).
83Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
CHAPTER 6
References
Ashley, Deanne. “Factors related to the delivery of healthcare services in Jamaica with
reference to problems related to maternal and child health.” Ph. D. diss.,
University of the West Indies, 1973.
Bacchus, Loraine, Gill Mezey, Susan Bewley, Alison Haworth. 2004. “Prevalence of
domestic violence when midwives routinely enquire in pregnancy”. BJOG: an
international journal of obstetrics and gynaecology 111: 441-445.
Bulatao, Rodolfo and John A. Ross. 2000. Rating maternal and neonatal health
programs in developing countries. Chapel Hill: University of North Carolina
Crowell, Nancy and Ann Burgess (eds). 1996. Understanding violence against women.
Washington D.C: National Academy Press.
De Brouwere, Vincent, Rene Tonglet, Wim Van Lerberghe. 1998. “Strategies for
reducing maternal mortality in developing countries: what can we learn from the
history of the industrialized west?” Tropical medicine and international health 3

84Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
(10): 771-782
Economic Commission for Latin America and the Caribbean. 2005. “Achieving the
millennium development goals in Latin America and the Caribbean”. The
millennium development Goals: A Latin America and Caribbean perspective.
Santiago: United Nations.
Edin, Kerstin, and Ulf Högberg. 2002. “Violence against pregnant women will remain
hidden as long as no direct questions are asked”. Midwifery 18: 268-278.
Espinoza, Henry, and Alma Virginia Camacho. 2005. “Maternal death due to domestic
violence: An unrecognized critical component of maternal mortality.” Pan
American Journal of Public Health 17 (2):123-129.
Gazamararian, JA, MM Adams. L.E Saltzman, C.H Johnson, F.C Bruce, JS Marks, SC
Zahniser. 1995. “The relationship between pregnancy intendedness and physical
violence in mothers of newborns”. Obstetrics & Gynecology 85 (6): 1031-1038.
http://www.serha.gov.jm/

85Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Jamaica Social Policy Evaluation. 2008. National progress report 2004-2006 on
Jamaica’s social policy goals. Kingston: Office of the Cabinet.
Koblinsky, M.A, O. Campbell, J. Heichelheim. 1999. “Organizing delivery care: what
works for safe motherhood?” Bulletin of the World Health Organization 77(5):
399-406.
Koenig, Lisa, Daniel Whitaker, Robert Royce, Tracey Wilson, Kathleen Ethier, Isabel
Fernandez. 2006. “Physical and sexual violence during pregnancy and after
delivery: A prospective multistate study of women with or at risk for HIV
infection”. American Journal of Public Health 96 (6):1-9.
Koonin, Lisa, H. Atrash, R. Rochat, J. Smith. 1988.Maternal mortality surveillance:
United States, 1980–1985.
http://www.cdc.gov/mmwR/preview/mmwrhtml/00001754.htm.
Matthews, Zoe. 2002. Maternal mortality and poverty. United Kingdom: DFID Resource
Centre for Sexual and Reproductive Health.

86Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
McCaw-Binns, Affette, S.F Alexander, J.L.M Lindo, C Escofery, K Spence, K Lewis-
Bell, G Lewis G. 2007. “Epidemiologic transition in maternal mortality and
morbidity: New challenges for Jamaica”. International journal of gynecology and
obstetrics 96: 226-232.
McCaw-Binns, Affette. 2005. “Safe motherhood in Jamaica: from slavery to self-
determination”. Paediatric and Perinatal Epidemiology 19:254-261.
Ministry of Health data, several years.
Ministry of Health. 2007. Strategic framework for safe motherhood within the family
health programme 2007-2011. Kingston: Ministry of Health.
Ministry of Health. 2009. Address by Acting Director of Family Services Dr. Yvonne
Munroe at the launch of Healthy mother. Healthy baby. Healthy family, Safe motherhood
programme launch, July 1, 2009. Kingston: Ministry of Health.
Mitchell, Ellen. 2000. Why Should I Lie? Maternal mortality and domestic violence in
Otavalo and Cotacachi Ecuador. New Orleans: Tulane University.
87Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Pan American Health Organization. 2005. “Maternal death due to domestic violence”.
Fact sheet: Gender, ethnicity and health, July 2005. Washington: Pan American
Health Organization.
POLICY Brief. 2002. Maternal and Neonatal Program Effort Index: Jamaica.
Glastonbury: Futures Group.
Planning Institute of Jamaica, Ministry of Foreign Affairs and Foreign Trade. 2009.
National report of Jamaica on millennium development goals for the UN
Economic and Social Council annual ministerial review. Kingston: Planning
Institute of Jamaica.
Ransom, Elizabeth, and Nancy Yinger. 2002. “Making motherhood safer: Overcoming
obstacles in the pathway to care”. MEASURE Communication Policy Brief.
Washington D.C: Population Reference Bureau.
Ronsmans, Carine and Wendy Graham. 2006. “Maternal mortality: who, when, where
and why”. Lancet 368: 1189-1200.
Satchell, Vernon. 1999. Jamaica. http://www.hartford-hwp.com/archives/43/130.htmlSmith, Kimberly, and Sara Sulzbach. 2008. “Community-based health insurance and
88Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
access to maternal health service: Evidence from three West African countries”.
Social Science and Medicine 66: 2460-2473.
Thomas, Shirley. “An assessment of maternity service in Portland and St. Mary.” MSc.
thesis, University of the West Indies, Mona, 1993.
UNDP, UNFPA,WHO, World Bank Special Programme of Research, Development and
Research Training in Human Reproduction. 2005. “Promoting evidence-based
sexual and reproductive health care”. Progress in Reproductive Health Research
71 .
United Nations. 1979. Declaration on the elimination of violence against women.
http://www.un.org/womenwatch/daw/cedaw/text/econvention.htm
United Nations. 2009. End poverty 2015: Millennium development goals.
http://www.un.org/millenniumgoals/
United Nations. 2006. The world’s women 2005: progress in statistics. New York:
United Nations.

89Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
United Nations Children’s Fund. 2009. Address by UNICEF Representative to Jamaica
Robert Fuderich at the launch of Healthy mother. Healthy baby. Healthy family,
Safe motherhood programme launch, July 1, 2009. Kingston: Ministry of Health.
United Nations Children’s Fund. 2008. Progress for children: a report card on maternal
mortality. Number 7, September 2008. New York: UNICEF.
United Nations Population Fund. 2009a. No woman should die giving life: Facts and
figures. http://www.unfpa.org/safemotherhood/
United Nations Population Fund. 2009b. Maternal Mortality Statistics: Making
Motherhood Safer. http://www.unfpa.org/mothers/statistics.htm
United Nations Population Fund. 2009c. Stepping up efforts to save mothers’ lives.
http://www.unfpa.org/mothers/
Women Deliver. 2009. The safe motherhood initiative.
http://www.womendeliver.org/overview/Background.htm
Woman Inc. data, several years.

90Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
World Bank. 2009. Address by World Bank Special Representative Badrul Haque at
the presentation of the Jamaica/World Bank Country Strategy for Jamaica 2010-
2013 in Gordon House, July 14, 2009. Kingston: Television Jamaica Limited.
World Health Organization. 2007. Maternal mortality in 2005: Estimates developed by
WHO, UNICEF, UNFPA and the World Bank. Geneva: World Health
Organization.

91Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
APPENDIX
QUESTIONNAIRE(TECHNICAL EXPERTS)
I am a student of the University of the West Indies, reading for a Masters of Sciencedegree in Governance and Public Policy. I am researching the issue of domestic violenceand its impact on Jamaica’s efforts in reducing maternal mortality. The aim of thisquestionnaire is to seek responses about why the issue of domestic violence againstpregnant women is not addressed or included as an integral component in the Ministry ofHealth’s Strategic Framework for Safe Motherhood within the Family HealthProgramme 2007-2011 policy document. The questionnaire also aims to get feedback onhow the issue of domestic violence against pregnant women can be addressed at thenational policy level, as well as views regarding maternal mortality and the country’sprospects of achieving MDG 5.
1. How long have you been offering care to pregnant women or researching theissue of maternal health?
__________________________________________________________________
__________________________________________________________________
2. How many pregnant women do you offer care annually?
__________________________________________________________________
__________________________________________________________________
3. What issues are addressed by you (midwife, public health nurse, obstetrician)when pregnant women visit health centres for antenatal care?
__________________________________________________________________
__________________________________________________________________
4. When problems are detected how are they addressed or dealt with by you whooffer care to pregnant women?
__________________________________________________________________
__________________________________________________________________

92Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
5. What are the reporting systems employed to track the problems that are detected?
__________________________________________________________________
__________________________________________________________________
6. When pregnant women visit health centres for antenatal care is the issue ofdomestic violence discussed?
__________________________________________________________________
__________________________________________________________________
6a. If yes, how is the matter addressed?
__________________________________________________________________
__________________________________________________________________
6b. If no, why is the matter not addressed?
__________________________________________________________________
__________________________________________________________________
7. Do you routinely ask pregnant women the direct question about whether they areabused by their partners?
__________________________________________________________________
__________________________________________________________________
7a. If yes, what are some of the responses obtained from the pregnant women?
93Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
__________________________________________________________________
7b. If no, why are such enquires not made?
__________________________________________________________________
__________________________________________________________________
8. What systems are in place to track women who visit healthcare facilities fortreatment following episodes of domestic violence?
__________________________________________________________________
__________________________________________________________________
9. What systems are in place to track these abused women when they becomepregnant?
__________________________________________________________________
__________________________________________________________________
10. What are the indicators do you use to detect whether or not a woman is beingabused while pregnant?
__________________________________________________________________
__________________________________________________________________
11. What type of training do you or did you receive to detect if pregnant women arevictims of domestic violence?
__________________________________________________________________
94Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
12. How often are you or were you trained?
__________________________________________________________________
__________________________________________________________________
13. Do you think the MOH’s Strategic Framework for Safe Motherhood policyadequately addresses the issue of domestic violence against pregnant women, aswell as other social issues that may affect this group?
__________________________________________________________________
__________________________________________________________________
13a. If yes, what are the strengths of the policy in addressing the issue of domestic violence against pregnant women and other social issues that may affect this group?
__________________________________________________________________
__________________________________________________________________
13b. If no, what are the shortcomings of the policy regarding the issue of domesticviolence against pregnant women and other social issues that may affect thisgroup?
__________________________________________________________________
__________________________________________________________________
14. How adequate is the MOH’s Strategic Framework for Safe Motherhood policy inlight of the current social realities affecting Jamaica?
__________________________________________________________________

95Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
15. What improvements do you think are needed for a more wholistic approachtowards Safe Motherhood in Jamaica?
__________________________________________________________________
__________________________________________________________________
16. What are your general views regarding the issue of domestic violence againstpregnant women?
__________________________________________________________________
__________________________________________________________________
17. What are your views regarding Jamaica’s efforts in achieving MDG5 by 2015?
__________________________________________________________________
__________________________________________________________________
18. What are your views regarding the current strategies being employed to helpJamaica achieve its goal of reducing maternal mortality by 75% by 2015?
__________________________________________________________________
__________________________________________________________________
19. How confident are you that enough emphasis is being placed on the issue ofmaternal mortality in Jamaica?
__________________________________________________________________
__________________________________________________________________

96Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
20. What more would you like to see done to address the issue of maternal mortalityin Jamaica?
__________________________________________________________________
__________________________________________________________________
21. How adequate has the budget for the MOH over the past five years been inaddressing the issue of maternal mortality in Jamaica?
__________________________________________________________________
__________________________________________________________________
22. In what ways might the issue of domestic violence derail Jamaica’s prospects ofachieving a reduction in maternal mortality rates by 75% by 2015?
__________________________________________________________________
__________________________________________________________________

97Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
QUESTIONNAIRE(HEALTHCARE PROVIDERS)
I am a student of the University of the West Indies, reading for a Masters of Sciencedegree in Governance and Public Policy. I am researching the issue of domestic violenceand its impact on Jamaica’s efforts in reducing maternal mortality. The aim of thisquestionnaire is to seek responses about why the issue of domestic violence againstpregnant women is not addressed or included as an integral component in the Ministry ofHealth’s Strategic Framework for Safe Motherhood within the Family HealthProgramme 2007-2011 policy document. The questionnaire also aims to get feedback onhow the issue of domestic violence against pregnant women can be addressed at thenational policy level, as well as views regarding maternal mortality and the country’sprospects of achieving MDG 5.
1. How long have you been offering care to pregnant women?
__________________________________________________________________
__________________________________________________________________
2. How many pregnant women do you offer care annually?
__________________________________________________________________
__________________________________________________________________
3. What issues are addressed by you (midwife, public health nurse, obstetrician)when pregnant women visit health centres for antenatal care?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
4. When problems are detected how are they addressed or dealt with by you whooffer care to pregnant women?
__________________________________________________________________
__________________________________________________________________

98Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
5. What are the reporting systems employed to track the problems that are detected?__________________________________________________________________
__________________________________________________________________
6. When pregnant women visit health centres for antenatal care is the issue ofdomestic violence discussed?
__________________________________________________________________
__________________________________________________________________
6a. If yes, how is the matter addressed?
__________________________________________________________________
__________________________________________________________________
6b. If no, why is the matter not addressed?
__________________________________________________________________
__________________________________________________________________
7. Do you routinely ask pregnant women the direct question about whether they areabused by their partners?
__________________________________________________________________
__________________________________________________________________
99Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
7a. If yes, what are some of the responses obtained from the pregnant women?
__________________________________________________________________
__________________________________________________________________
7b. If no, why are such enquires not made?
__________________________________________________________________
__________________________________________________________________
8. What systems are in place to track women who visit healthcare facilities fortreatment following episodes of domestic violence?
__________________________________________________________________
__________________________________________________________________
9. What systems are in place to track these abused women when they becomepregnant?
__________________________________________________________________
__________________________________________________________________
10. What are the indicators do you use to detect whether or not a woman is beingabused while pregnant?
__________________________________________________________________
__________________________________________________________________

100Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
11. What type of training do you or did you receive to detect if pregnant women arevictims of domestic violence?
__________________________________________________________________
__________________________________________________________________
12. How often are you or were you trained?
__________________________________________________________________
__________________________________________________________________
13. Do you think the MOH’s Strategic Framework for Safe Motherhood policyadequately addresses the issue of domestic violence against pregnant women, aswell as other social issues that may affect this group?
__________________________________________________________________
__________________________________________________________________
13a. If yes, what are the strengths of the policy in addressing the issue of domesticviolence against pregnant women and other social issues that may affect thisgroup?
__________________________________________________________________
__________________________________________________________________
13b. If no, what are the shortcomings of the policy regarding the issue of domesticviolence against pregnant women and other social issues that may affect thisgroup?
__________________________________________________________________
__________________________________________________________________
14. How adequate is the MOH’s Strategic Framework for Safe Motherhood policy inlight of the current social realities affecting Jamaica?

101Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
__________________________________________________________________
15. What improvements do you think are needed for a more wholistic approachtowards Safe Motherhood in Jamaica?
__________________________________________________________________
__________________________________________________________________
16. What are your general views regarding the issue of domestic violence againstpregnant women?
__________________________________________________________________
__________________________________________________________________
17. What are your views regarding Jamaica’s efforts in achieving MDG5 by 2015?
__________________________________________________________________
__________________________________________________________________
18. What are your views regarding the current strategies being employed to helpJamaica achieve its goal of reducing maternal mortality by 75% by 2015?
__________________________________________________________________
__________________________________________________________________
19. How confident are you that enough emphasis is being placed on the issue ofmaternal mortality in Jamaica?
__________________________________________________________________

102Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
20. What more would you like to see done to address the issue of maternal mortalityin Jamaica?
__________________________________________________________________
__________________________________________________________________
21. How adequate has the budget for the MOH over the past five years been inaddressing the issue of maternal mortality in Jamaica?
__________________________________________________________________
__________________________________________________________________
22. In what ways might the issue of domestic violence derail Jamaica’s prospects ofachieving a reduction in maternal mortality rates by 75% by 2015?
__________________________________________________________________
__________________________________________________________________

103Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
QUESTIONNAIRE(FOCUS GROUP)
I am a student of the University of the West Indies, reading for a Masters of Sciencedegree in Governance and Public Policy. I am researching the issue of domestic violenceand its impact on Jamaica’s efforts in reducing maternal mortality. The aim of thisquestionnaire is to seek responses about why the issue of domestic violence againstpregnant women is not addressed or included as an integral component in the Ministry ofHealth’s Strategic Framework for Safe Motherhood within the Family HealthProgramme 2007-2011 policy document. The questionnaire also aims to get feedback onhow the issue of domestic violence against pregnant women can be addressed at thenational policy level, as well as views regarding maternal mortality and the country’sprospects of achieving MDG 5.
1. How old are you?a. 18-22 ( ) b. 23-27 ( ) c. 28-32 ( ) d. 33-37 ( ) e. 38-over ( )
2. Is this your first pregnancy?
__________________________________________________________________
__________________________________________________________________
2a. If no, how many children do you have?a. 1 ( ) b. 2 ( ) c. 3 ( ) d. 4 ( ) e. 5 and over ( )
3. What questions are you asked by the healthcare professional (midwife, publichealth nurse, obstetrician) who offer you care when you attend antenatal caresessions?
__________________________________________________________________
__________________________________________________________________
4. When problems arise how does the health professional offering you care handlethe matter?

104Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
__________________________________________________________________
5. Is the issue of domestic violence discussed with you by the health professionaloffering you care?
__________________________________________________________________
__________________________________________________________________
5a. If yes, how is the issue of domestic violence dealt with by the healthcare professional offering you care?
__________________________________________________________________
__________________________________________________________________
5b. If no, do you think that the issue of domestic violence should be raised by the healthcare professional offering you care?
__________________________________________________________________
__________________________________________________________________
6. Have you ever been asked any direct questions about domestic violence by thehealth care professional offering you care?
__________________________________________________________________
__________________________________________________________________
7. What are your general views regarding violence against pregnant women?
__________________________________________________________________
__________________________________________________________________

105Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
8. Do you think enough is being done to address the issue of violence againstpregnant women?
__________________________________________________________________
__________________________________________________________________
8a. If yes, what is being done to address the issue of domestic violence against pregnant women that you applaud?
__________________________________________________________________
__________________________________________________________________
8b. If no, what would you like to see done to address the issue of violence against pregnant women?
__________________________________________________________________
__________________________________________________________________
9. Do you know what maternal mortality is?
__________________________________________________________________
__________________________________________________________________
9a. If yes, what is maternal mortality?
__________________________________________________________________
__________________________________________________________________
9b. If no, is the issue of maternal mortality discussed with you by the healthcareprofessional offering you care?
__________________________________________________________________

106Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
__________________________________________________________________
10. What do you know of the Ministry of Health’s Safe Motherhood Programme?
__________________________________________________________________
__________________________________________________________________
11. What are your views regarding the inclusion of strategies to address domesticviolence when women visit healthcare facilities for antenatal care?
__________________________________________________________________
__________________________________________________________________

107Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
INFORMED CONSENT FORM
Title of study
The fight for MDG 5: An analysis of Jamaica’s policy framework for improving maternal
health
Description and Procedure
This study is being done to assess why the issue of domestic violence is not addressed or
included as an integral component in the Ministry of Health’s Strategic Framework for
Safe Motherhood within the Family Health Programme 2007-2011 policy document. The
study also aims to assess how the issue of domestic violence against pregnant women can
be addressed at the national policy level, as well as views regarding maternal mortality
and Jamaica’s prospects of achieving MDG 5 by 2015.
You will be asked a number of questions via a questionnaire during the elite interview
session. These questions will not require you to provide the details of names and
addresses or any other information that distinctly identifies you publicly. The entire
process is anonymous. All information received will be strictly confidential.
Your participation in this elite interview is entirely voluntary. You can choose not to
answer or respond to any of the questions.
There is no prolonged period or follow-up to this study. This is a one-time interview
lasting approximately 15-20 minutes.
Risks
There are no perceived risks, physical or psychological associated with taking part in this
research.

108Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
Benefits
No financial compensation or expenses are involved. You may not benefit personally or
immediately from the study. The overall benefit is to society at large.
Consent
I have read or had this statement read to me, understand its contents and have had
sufficient time to consider my voluntary participation in this study.
____________________________ ____________________Healthcare Provider’s Signature Date
_____________________________ ______________________Witness’s Signature Date
I testify that I have fully and appropriately informed the subject about the study and
offered to answer any questions she/he may have.
_________________________________ ________________________Researcher’s Signature Date

109Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
INFORMED CONSENT FORM FORFOCUS GROUP DISCUSSION
I agree to participate in this focus group discussion being conducted by a Masters of
Science Student at the Sir Arthur Lewis Institute for Social and Economic Studies,
University of the West Indies (Mona). The discussion will focus on the issue of domestic
violence and why it is not addressed or included as an integral component in the Ministry
of Health’s Strategic Framework for Safe Motherhood within the Family Health
Programme 2007-2011 policy document. The discussion will also focus on how the issue
of domestic violence against pregnant women can be addressed at the national policy
level, as well as views regarding maternal mortality and Jamaica’s prospects of achieving
MDG 5 by 2015.
I understand that:
* The session will be recorded and notes taken
*Confidentiality will be maintained and when analyzed, names will not be associated
with responses.
* My participation is voluntary and I am free to withdraw at any time.
Names Signature
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________

110Copyright © 2009Nicole Antoinette Hayles McGowan
Fulfilling the MDG: An Analysis of Jamaica’s Policy Framework for Improving Maternal HealthMSc. Governance and Public Policy (2009)
________________________________________________________________________
________________________________________________________________________
_________________________________ ________________________
Witness’s Signature Date
I testify that I have fully and appropriately informed the subject about the study and
offered to answer any questions she may have.
_________________________________ ________________________Researcher’s Signature Date
c/o Sir Arthur Lewis Institute of Economic and Social Studies
University of the West Indies
Mona
Kingston 7
Telephone: (876) 927-1020