full-mouth restoration of a severely decayed dentition options and the pros and cons of each option....
TRANSCRIPT
68
DENTALCETODAY.COM • DECEMBER 2013
INTRODUCTIONPatients present to the dental office with avariety of needs both pressing and unique;some require a hygiene appointment androutine clinical examination, while otherspresent with much greater challenges. Inall cases, patients present with hope: thattheir teeth are cavity free, the nagging painin one of their molars is a simple fix, a cos-metic concern can be corrected, or perhapsyears of poor oral hygiene and the resultingdecay can be repaired, allowing a fresh startwith a healthy smile.
Such was the case with the full-mouthrestorative case detailed below. The patienthad presented to the author’s office with exten-sive dental decay on both arches, the end resultof years of neglect and poor oral hygiene, andwas eager to save his teeth through extensivesurgical and restorative therapies. Porcelainveneers were selected as the main restorativetherapy, coupled with anterior periodontalcrown lengthening on both arches, endodon-tics, and man dibular and maxillary posteriorcrowns, to bring his teeth back to good health,form, and function.1-4
CASE REPORTDiagnosis and Treatment Planning
A 24-year-old male in good health, accom-panied by his parents, arrived at our officefor a new patient interview and compre-hensive examination. During a review ofhis medical history, the patient reportedthat he had been living on his own for thepast 4 years and had severely neglected histeeth and oral health. Poor dental hygieneincluded a lack of regular tooth brushingand flossing as well as the regular daily con-sumption of soft drinks and candy. Thepatient was now practicing an improved,healthy lifestyle, and wished to restore histeeth before returning to college.
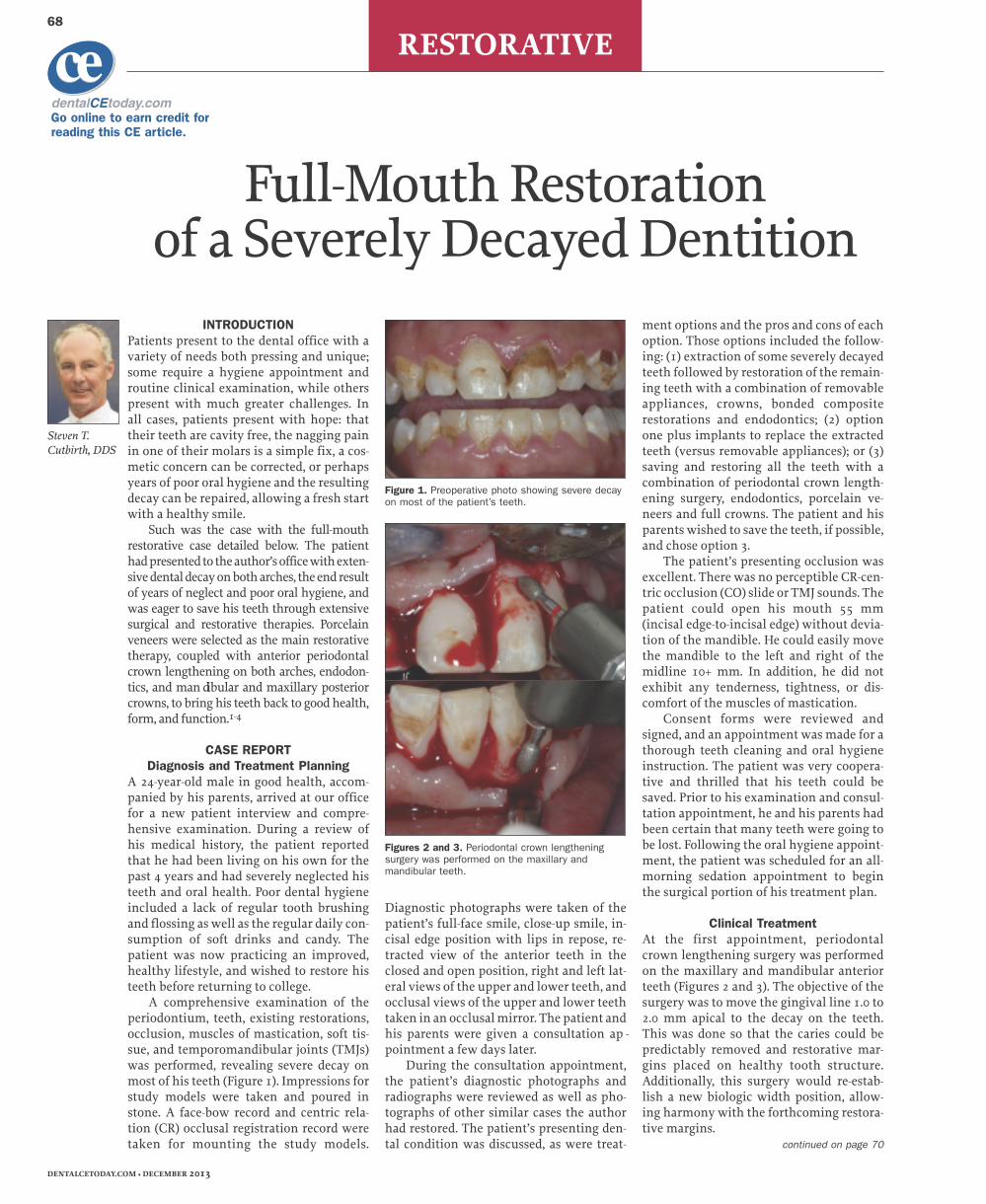
A comprehensive examination of theperiodontium, teeth, existing restorations,occlusion, muscles of mastication, soft tis-sue, and temporomandibular joints (TMJs)was performed, revealing severe decay onmost of his teeth (Figure 1). Impressions forstudy models were taken and poured instone. A face-bow record and centric rela-tion (CR) occlusal registration record weretaken for mounting the study models.
Diagnostic photographs were taken of thepatient’s full-face smile, close-up smile, in -cisal edge position with lips in repose, re -tracted view of the anterior teeth in theclosed and open position, right and left lat-eral views of the upper and lower teeth, andocclusal views of the upper and lower teethtaken in an occlusal mirror. The patient andhis parents were given a consultation ap -pointment a few days later.
During the consultation appointment,the patient’s diagnostic photographs andradiographs were reviewed as well as pho-tographs of other similar cases the authorhad restored. The patient’s presenting den-tal condition was discussed, as were treat-
ment options and the pros and cons of eachoption. Those options included the follow-ing: (1) extraction of some severely decayedteeth followed by restoration of the remain-ing teeth with a combination of removableappliances, crowns, bonded compositerestorations and endodontics; (2) optionone plus implants to replace the extractedteeth (versus removable appliances); or (3)saving and restoring all the teeth with acombination of periodontal crown length-ening surgery, endodontics, porcelain ve -neers and full crowns. The patient and hisparents wished to save the teeth, if possible,and chose option 3.
The patient’s presenting occlusion wasexcellent. There was no perceptible CR-cen-tric occlusion (CO) slide or TMJ sounds. Thepatient could open his mouth 55 mm(incisal edge-to-incisal edge) without devia-tion of the mandible. He could easily movethe mandible to the left and right of themidline 10+ mm. In addition, he did notexhibit any tenderness, tightness, or dis-comfort of the muscles of mastication.
Consent forms were reviewed andsigned, and an appointment was made for athorough teeth cleaning and oral hygieneinstruction. The patient was very coopera-tive and thrilled that his teeth could besaved. Prior to his examination and consul-tation appointment, he and his parents hadbeen certain that many teeth were going tobe lost. Following the oral hygiene appoint-ment, the patient was scheduled for an all-morning sedation appointment to beginthe surgical portion of his treatment plan.
Clinical TreatmentAt the first appointment, periodontalcrown lengthening surgery was performedon the maxillary and mandibular anteriorteeth (Figures 2 and 3). The objective of thesurgery was to move the gingival line 1.0 to2.0 mm apical to the decay on the teeth.This was done so that the caries could bepredictably removed and restorative mar-gins placed on healthy tooth structure.Additionally, this surgery would re-estab-lish a new biologic width position, allow-ing harmony with the forthcoming restora-tive margins.
Steven T.Cutbirth, DDS
Full-Mouth Restoration of a Severely Decayed Dentition
continued on page 70
Figure 1. Preoperative photo showing severe decayon most of the patient’s teeth.
Figures 2 and 3. Periodontal crown lengthening surgery was performed on the maxillary andmandibular teeth.
RESTORATIVE
dentalCEtoday.comGo online to earn credit for reading this CE article.
cece

RESTORATIVE70
It is important in periodontalcrown lengthening surgery that bothalveolar bone and gingival tissue areproportionally removed. If only gingi -vectomy is performed, the gingivaltis sue will regrow approximately 2 to3 mm coronal to the alveolar crest andre-establish the original biologicwidth and gingival line position. If 2.0mm of gingival height is to be re -moved (gingivectomy), a gingival flapmust be reflected following gingivec-tomy and the alveolar crest must thenbe reduced apically (ostectomy) thesame 2.0 mm so there are 3.0 mm be -tween the newly recontoured alveolarcrest line and the newly establishedgingival line. This measurement al -lows a healthy biologic width to be re-established apical to the de sired gingi-val line, which is now also apical tothe decay on the teeth. Also note thatonly the facial half of each papillae isreflected, leaving the pa latal/lingualhalf of each papillae in place, to pre-vent potential formation of an inter-proximal “black triangle.” (Techniqueby Dr. Pat Allen, Dallas Tex.)
At the comprehensive examina-tion appointment, a previously undi-agnosed globulomaxillary cyst wasdiscovered between the roots of themaxillary right cuspid and lateralincisor. This is just one example ofthe importance of a comprehensiveexamination on all new patients. Thecyst was surgically removed and sentfor pathologic evaluation (Figures 4aand 4b). As expected, the pathologicevaluation confirmed the diagnosisof a globulomaxillary cyst.
A 5-O Prolene interrupted suture(Ethicon, a Johnson & Johnson Com -pany) was placed to secure the gingi-val flap following crown-lengtheningsurgery (Figure 5), and was removed 2weeks later. The tissue was healingwell and was allowed to continuehealing for 3 months prior to dentalrestoration (Figure 6). During thattime, the patient was advised to rinse
for one minute at bedtime with Crest3D White Multi-Care Whiten ingRinse (Procter & Gamble). This so -lution contains hydrogen peroxideand may be diluted if too strong.Rinsing was to be followed by floss-ing and brushing (especially at thegumline) with a Sonicare ultrasonictoothbrush (Philips Oral Healthcare);and then a one-minute rinse withchlorhexidine gluconate (PerioGard[Colgate Palmolive]). Each morningthe patient rinsed with mouthwashfor one minute, brushed with theSoni care toothbrush, and then rinsedfor one minute with PerioGard.
Following 3 months of periodon-tal healing, impressions of the teethwere taken along with a face-bowrecord. Occlusal registration recordswere not necessary for mounting,since there was no perceptible CR-COslide and the patient contacted simul-taneously in centric relation occlu-sion (CRO) on the right and left cus-pids through first molars. The studymodels were poured in stone, whichwere then mounted on a semi-ad -justable articulator (Hanau articula-tor) with the arbitrary face-bow andwaxed up to ideal tooth dimensions.The waxed-up models would be usedto fabricate the matrix for provisionalrestorations (Figure 7). The patientwas scheduled for an all-morningappointment (with sedation planned)to begin the restorative process.
The mandibular anterior teethwere prepared for porcelain veneers,and the first and second mandibularbicuspids were prepared for all-porce-
lain crowns (Figures 8a and 8b). Fol -lowing retraction cord placement inthe gingival sulci of the bicuspid teeth(the gingival tissue surrounding themandibular anterior teeth was toofragile and the gingival sulci too tinyfor retraction cord placement), a poly-ether impression (3M Impregum Pen -ta Soft Custom Tray and Im pregumGarant Soft Im pression [3M ESPE])with custom tray (Figures 9a and 9b)was taken of the mandibular teeth;followed by a second reversible hy -drocolloid im pression (Van R Den talProducts). The author utilizes this sec-ond impression as a backup, just incase there was some unseen inaccura-cy with the polyether impression. Themodel from the reversible hydrocol-loid impression can also be used as asolid model for perfecting the inter-proximal contacts of the restorations.In that utilization, the gingival quar-ter of the stone teeth are first cut backwith an acrylic bur.
Provisional restorations were fab-ricated with bis-acrylic provisionalmaterial (Luxatemp [DMG America])using a vinyl polysiloxane (VPS) (or a
vacuum-formed) matrix fabricatedfrom the wax-up model. Note that if avacuum-formed matrix is utilized, asin this case, the wax-up model mustfirst be impressed and poured in stoneprior to fabrication of the matrix; oth-erwise, heat will melt the wax. Themandibular anterior and bicuspidprovisional restorations were adjust-ed to fit the prepared teeth, but theywere not cemented at this time.
Since the patient lived in anotherstate, it was determined that themandibular and maxillary anteriorand bicuspid teeth would be pre-pared, impressed, and provisionalizedat the same appointment. Nor mally,only the mandibular anterior andbicuspid teeth would have been pre-pared and impressed at the first res -torative appointment; the maxillaryanterior and bicuspid teeth wouldhave been prepared and restored atthe next appointment, when the man -dibular anterior and bicuspid finalrestorations were returned from thelaboratory team and seated.
The maxillary anterior teeth andbicuspids were prepared for porce-
DENTALCETODAY.COM • DECEMBER 2013
Figures 4a and 4b. During the clinical examination, a globulomaxillary cyst was discovered between the roots of themaxillary right cuspid and lateral incisor. It was surgicallyremoved and sent for evaluation.
Figure 5. Following crown lengthening surgery, sutures were placed to secure thegingival flap; they were removed 2 weekslater.
Figure 6. Gingival tissues were allowed toheal for 3 months before beginning therestorative phase of treatment. Healing progressed without incident.
Figure 7. Study models were poured instone, mounted on a semi-adjustable articulator, and waxed-up to ideal toothdimensions.
Figures 8a and 8b. Mandibular anterior teeth were prepared for porcelain veneers, and bicuspids were prepared for all-ceramic crowns.
a b
Figures 9a and 9b. A polyether impression of the lower arch was taken with a custom tray.
a b
Full-Mouth Restoration of a Severely...continued from page 68
Patients present tothe dental officewith a variety ofneeds both pressingand unique; somerequire a hygieneappointment....
a b

RESTORATIVE
lain veneers (Figures 10a and 10b).Impres sions were taken and provi-sional restorations fabricated exactlylike those of the mandibular anteriorteeth and bicuspids, with the excep-tion that the retraction cord (1n [VanR Dental Products]) wasplaced in the facial sulci ofthe maxillary anterior teethas well as the bicuspids priorto impression taking.
An arbitrary face-bow re -cord was taken as well as aVPS occlusal registration re -cord (JET BLUE BITE Fast Set[Col tène]) of the preparedteeth. The provisional restor -ations were trimmed and pol-ished, and then tried on theteeth; care was taken to en -sure correct incisal planes,occlusion, and well-adaptedgingival margins.
Quality full-face photo-graphs were taken of the pre-pared maxillary and mandibu-lar teeth with the teeth slight-ly parted and lip retractors inplace (Figures 10c and 10d).These photos allow the dentallaboratory technician to ob -serve the maxillary and man -dibular incisal planes of theprepared teeth compared tothe pupillary line (represent-ing a horizontal plane). Thisalso allows the technician toconfirm that the face-bowmounting is correct.
The bis-acrylic provision-al res torations were luted tothe teeth as follows:
A dot of 38% phosphoricacid gel (3M ESPE) was placedfor 15 seconds on each toothprepared for a veneer, thenrinsed. Unfilled resin (Scotch -bond Universal Adhesive [3MESPE]) was then copiouslyapplied to the teeth preparedfor veneers and also to theinside (tooth-side) of the pro-visional veneer restorations.Next, temporary crown andbridge cement (Fynal [DENT -SPLY Caulk]) was placed inthe mandibular bicuspidcrown provisional restora-tions. The 10 maxillary and 10mandibular connected provi-sional restorations were thenplaced firmly on the preparedteeth. As the anterior provi-sional restorations were heldfirmly in place with thethumb and pointer finger ofone hand, the excess unfilledresin was blown from the
teeth onto a 2 x 2 gauze using an airsyringe. Two curing lights were usedto cure each anterior veneer provi-sional restoration for 20 seconds si -multaneously on both the facial andlingual surfaces. Following initial set,
the excess temporary cement was re -moved from the mandibular bicuspidprovisional crown restorations.
Full-face photos of the maxillaryand mandibular provisional restora-tions were taken with the lips retract-
ed and the incisal edges slightly part-ed, as well as with the patient smilingand with “lips in repose,” showingthe incisal edge position in relation tothe slightly parted lips (Figures 11a to11c). These views allow the laborato-
71

RESTORATIVE72
ry team to observe the seated provi-sional restorations in relation to thepupillary line, gingival line, and lips.
Quality alginate impressions (Iden -tic Alginate [DUX Dental]) were takenof the provisional restorations andpoured in stone, and a face-bow recordwas taken of the provisionals. The lab-oratory team can use the mountedmodels of the provisionals for a cus-tom incisal guide table or VPS matrixguide for the final restorations.
The final restorations (feldspath-ic porcelain veneers and all-ceramiccrowns [Tanaka Dental Laboratory])were fabricated by our lab team andreturned to our office. The maxillaryand mandibular provisional restora-tions were removed, and the preparedteeth were polished with plainpumice and water. The remaining“dot” of retained unfilled resin,where the original “dot” of acid etchwas placed on the facial surface ofeach veneer-prepared tooth, was re -moved with a 5379-023 football-shaped diamond (Brasseler USA). Thefinal restorations were tried-in, andany necessary (very minor) interprox-imal adjustments were made. Notethat these adjustments generallyshould not be necessary if accurateimpressions and provisional restora-tions have been made. If significantinterproximal adjustments are re -quired, and excellent prepared teethimpressions and provisional restora-tions were made, then inaccurate lab-
oratory die/model systems are usual-ly the problem.
The mandibular anterior veneerprepared teeth were first etched with38% phosphoric acid for 15 seconds(dentin) to 30 seconds (enamel), thenrinsed thoroughly with water for 15seconds. The porcelain veneers werepreviously etched with 8% hydrofluo-ric acid in the laboratory, then placed inan ultrasonic cleaner for several min-utes to remove any caked powder thatwas created from the etching process.Following try-in, the 6 mandibularanterior veneers were wiped with iso-propyl alcohol on a small cotton ball,then dried with aspirator air. The roomlights in the operatory were turned offso that only the operatory light, turneddownward toward the patient’s feetand set on low intensity, was on forminimum illumination.
Unfilled resin primer/adhesive(3M Adper Scotchbond Multi-Pur -pose Adhesive [3M ESPE]) was placedin each mandibular veneer as well ason the facial surface of each veneerprepared tooth. The excess liquid wasblown off with an air syringe toremove the acetone carrier. Filledveneer luting resin (RelyX shade B0.5[3M ESPE]) was next placed in the
veneer restorations, which were thenplaced on the prepared teeth. All 6veneers were placed at once, withoutcuring. Placement of all 6 veneers atonce is not a problem and is done sothat the interproximal contacts of theveneers are ideal and do not “swim”microscopically, as often happenswhen adjacent veneers are placed andcured individually.
Once the veneers were in place onthe teeth, a curing light was activatedand moved fluidly from the lingualsurface of the mandibular left cuspidto the lingual of the lower right cus-pid. This initial cure was only forabout 3 seconds total for the 6 ve -neers. Next, the same curing lightwas placed on the facial surface of themandibular left cuspid veneer, acti-vated, and then moved fluidly acrossthe facial surfaces of all the mandibu-lar anterior veneers, ending at theright cuspid. This initial cure wasalso done for no more than 3 seconds.This minimum cure creates an initial“set” of the veneer luting composite.
The excess luting composite wasnow easily “chipped” away from theveneers with the backside of a sharp-tipped scaler, followed by interproxi-mal flossing with waxed dental floss.It is critical not to remove any excessluting composite before it is initiallyset. If excess luting composite is re -moved in the flowable stage, “suck-back” will occur under the veneermargin, leading to microvoids in thetooth-veneer microgap. These micro -voids can lead to marginal decay, sen-sitivity, and staining.
Once the excess veneer lutingmaterial was removed, the bicuspidall-porcelain crowns were tried onthe teeth, interproximal adjustmentswere made if necessary, the crownsand teeth were cleaned, and thecrowns were cemented in place withRelyX Unicem (3M ESPE) resin ce -ment. Vaseline was placed on the in -terproximal contacts prior to cemen-tation to facilitate easy interproximalcement removal. Again, except forinterproximal contacts, excess ce -ment should not be removed untilinitial set takes place; the excess ce -ment is then easily chipped away.Waxed floss should be poppedthrough the interproximal contactsas soon as the crowns are seated to besure the contact does not becomeblocked with set cement.
DENTALCETODAY.COM • DECEMBER 2013
Figures 10c and 10d. Full-face photos of the prepared teeth allowed the laboratory team toobserve the patient’s incisal planes.
Figures 10a and 10b. The patient’s maxillary anteriors and bicuspids were prepared toreceive porcelain veneers.
a b
c dFigures 11a to 11c. Full-face photos of theprovisionalized teeth allowed the laboratorytechnicians to observe the seated restorations in relation to the pupillary line,gingival line, and lips.
a
b
c
Figure 12. A hard acrylic centric relation occlusion flat plane maxillary nightguard wasfabricated to protect the patient’s restorations.
The importance of following oral hygiene instructions and keeping all scheduled appointments should also be emphasized.

RESTORATIVE
The maxillary anterior veneerswere seated in the same sequence.Following maxillary and mandibularanterior veneer seating, initial cur-ing, and excess luting compositeremoval, each veneer was cured 60seconds with a curing light (Deme -tron [Kerr]) on both the facial and lin-gual surfaces. Two lights were usedsimultaneously so the total curing
time for 16 veneers (10 upper, 6lower) was 16 minutes.
Final luting cement removal wasaccomplished with dental floss andscalers. If required, the margins maybe further polished with ultra finediamond burs then 33-fluted carbideburs (Brasseler USA Fluted CarbideBur No. H246LUF.31.012) with a lighttouch and high water volume, fol-lowed by rubber wheels and diamondpolishing paste in a prophy cup.
The occlusion was adjusted sothat there were no premature con-tacts on the anterior teeth, and con-tacts were bilateral and simultaneouson the cuspid and bicuspid teethwhen the condyles were seated in CRposition (CRO). The incisal edges ofthe veneers were perfected with afine, flame-shaped diamond (Bras -seler USA Diamond Bur No.8862.31.012). The patient sat upstraight in the operatory chair forthis process so that the pupillary linewas parallel to the floor (the “alertfeeding position”). Final polish wasdone with rubber polishing wheels(Shofu) and diamond paste (MirageDiamond Paste) in a prophy cup.
The maxillary and mandibularmolar teeth were next prepared forfull crowns at the same appointment,impressed, and provisionalized. Oncereceived from the lab, the final molarcrowns were cemented, similar to thecementation procedure for the lowerbicuspid all-porcelain crowns.
Final occlusal equilibration toCRO was performed. The anteriorocclusion was again checked with thepatient sitting upright in the alertfeeding position to ensure there wereno premature contacts on the anteri-or teeth. A flat plane, hard acrylicCRO maxillary nightguard was fabri-cated and delivered to the patient(Figure 12).5 Maxillary and mandibu-lar night guards may be fabricatedand worn simultaneously for maxi-mum restor ation protection.
The patient was given the follow-ing postoperative instructions: (1) Atbedtime, rinse vigorously withmouthwash (may be diluted) for oneminute followed by dental flossingand brushing with a Sonicare tooth-brush; (2) Each morning, rinse withmouthwash followed by brushing;(3) Wear the nightguard each night;(4) Limit sticky sweets, soft drinks,mints, and cough drops; (5) Do notbite or chew hard foods (especiallywith the anterior teeth) and do notbite anything harder than a sandwichwith the anterior teeth; (6) Cut pizza,corn on the cob, apples, etc, into bitesand chew these only with the posteri-
or teeth. While studies show thatwell-constructed porcelain veneersare as strong as natural teeth and canbe a good long-term restorative solu-tion,1-4 shear forces on maxillary an -terior teeth, as well as on the porce-lain veneers, can cause fracture due tothe facial (outward) direction of bit-ing forces.
The patient’s final photos afterrestorative care are shown in Figures13a to 13e.
DISCUSSIONWhen a treatment plan is complexand calls for multiple procedures, it isespecially important that patients befully informed from the outset re -garding treatment options, durationof treatment, cost of therapy, mainte-nance of restorations, principles ofover all dental health, and their re -sponsibility for maintaining the res -torations. The importance of follow-ing oral hygiene instructions andkeeping all scheduled appointmentsshould also be emphasized. The pa -tient must understand some ap -pointments will often be severalhours long. Missed appointments canbe costly for the dental practice. Se -dation is another important consider-ation with longer appointments, es -pecially when surgery is involved.
The dental and medical healthhistories should be carefully re -viewed for potential contradictionsto therapy and the patient advisedaccordingly. Examples of potentialcontradictions to full-mouth recon-struction might be extreme bruxismor periodontal disease. If these condi-tions exist preoperatively, it is imper-ative serious conversations take placewith the patient regarding possiblerestoration breakage and tooth loss.
With any restorative treatment,and especially extensive treatment,con sideration must be given to lon -gevity of the restorations and re spon -sibility of repair should it be neces-sary. The possibility always existsthat the patient will relapse into thedetrimental habits that resulted inone’s initial presentation for therapy.The younger the patient is at presen-tation, the greater the possibility thatsome or all of the restorations willeven tually need to be repaired or re -done. Even if the restoration is per-formed well, there is tremendousstress on dental restorations in themouth. Just like automobile upkeep,periodic restorative repairs should beexpected.
IN SUMMARYAn outline of the sequence of treat-
ment for this full-mouth reconstruc-tion was as follows:
l A patient presented to the au -thor’s office in need of a full-mouthrestoration, and brought with himthe hope that his teeth, and his smile,could be saved.
l Endodontic procedures, peri-odontal surgery, occlusal equilibra-tion into CRO;
l Study models mounted on asemi-adjustable articulator with anarbitrary face-bow for wax-up to idealteeth anatomy and position;
l Restoration of the lower anteri-or teeth, then the upper anteriorteeth, establishing appropriate ante-rior guidance;
l Restoration of the mandibularand maxillary posterior teeth;
l Placement of a hard acrylic,CRO nightguard.5
With careful treatment planninginvolving periodontal crown length-ening surgery, endodontics, porcelainve neers, and crowns, the patient’steeth were systematically and suc-cessfully restored.�
ACKNOWLEDGMENTThe author would like to thank the den-tal laboratory team at Asami Tan akaLaboratory (Chicago, Ill) for their excel-lent technical work seen in this case.
References1. Beier S, Kapferer I, Burtscher D, et al. Clinicalperformance of porcelain laminate veneers forup to 20 years. Int J Prosthodont. 2012;25:79-85.
2. D’Arcangelo C, De Angelis F, Vadini M, et al.Clinical evaluation on porcelain laminateveneers bonded with light-cured composite:results up to 7 years. Clin Oral Investig.2012;16:1071-1079.
3. Aykor A, Ozel E. Five-year clinical evaluation of300 teeth restored with porcelain laminateveneers using total-etch and a modified self-etchadhesive system. Oper Dent. 2009;34:516-523.
4. Layton DM, Clarke M, Walton TR. A systematicreview and meta-analysis of the survival of felds-pathic porcelain veneers over 5 and 10 years.Int J Prosthodont. 2012;25:590-603.
5. Pankey LD. The PMS technique: an historicalperspective. Continuum (N Y). 1981:5-11.
Dr. Cutbirth practices restorative dentistry inWaco, Tex (wacosedationdentist.com), and isdirector of the Center for Aesthetic RestorativeDentistry (CARD) (centerforard.com), located inDallas, Tex, a hands-on, complex restorativeteaching center for practicing dentists. Hegraduated from Baylor Dental College in 1979,then completed a 2-year Fellow ship at Baylor,then was a member of the teaching faculty atthe Pankey Institute in Florida for 20 years. Dr.Cutbirth has lectured and published extensive-ly on the topics of systematic restoration of theseverely worn dentition with vertical dimensionincrease, diagnosis and treatment of occlusalproblems and facial pain, complex aestheticrestorative dentistry, ridge modification andbone grafting for small-diameter implant uti-lization, and the most effective/productive den-tal practice system. He can be reached at(254) 772-5420 or at [email protected].
Disclosure: Dr. Cutbirth is an occasional lec-turer for 3M ESPE but has received no com-pensation for writing this article.
73
DECEMBER 2013 • DENTALCETODAY.COM
a
b
c
d
e
Figures 13a to 13e. Final photos of thepatient with the completed restorative care.