functional outcomes in prosthetics. functional outcomes importance of functional outcome tools –...
TRANSCRIPT
FUNCTIONAL OUTCOMES IN PROSTHETICS
Functional Outcomes
• Importance of Functional Outcome tools– PT reimbursement: G-Codes required by
Medicare currently. Ability to document using a functional outcome measure most objective
– Prosthetic industry changes: ability to document patient improvement/potential helps justification with insurance
– Justifies treatment/services– Tool to document progression
Functional Outcomes
• 1995- Medicare adopted K-levels to describe “ability of a patient to reach a defined functional state within a reasonable period of time”
• Functional level of patient determines componentry- foot and knee
• Based on current medical status, comorbidities and desire to ambulate (subjective)
Functional OutcomesK-Levels
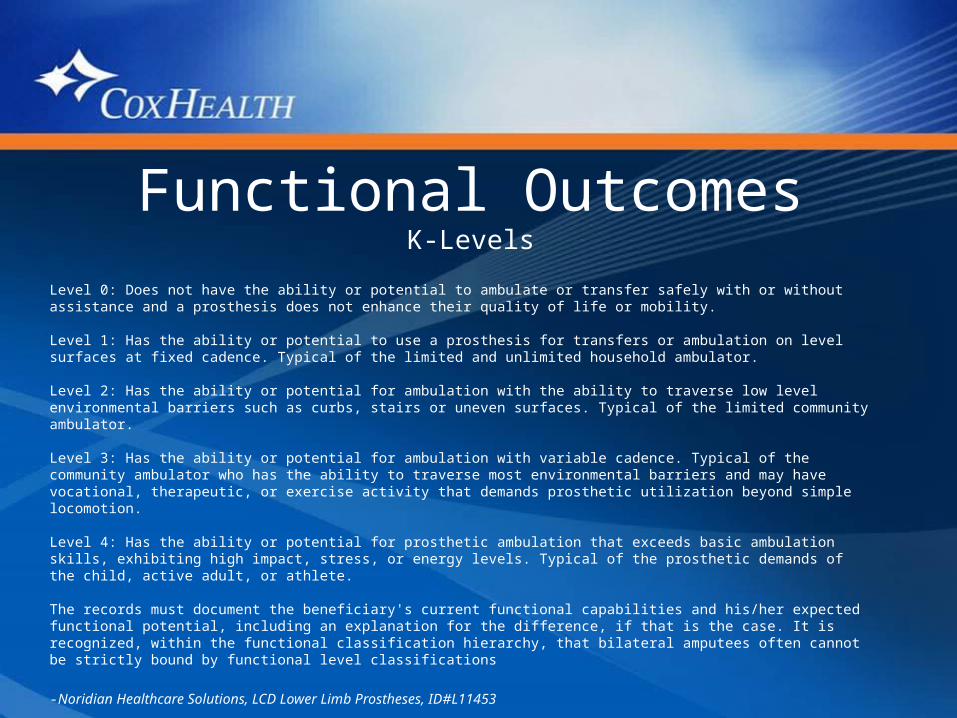
Level 0: Does not have the ability or potential to ambulate or transfer safely with or without assistance and a prosthesis does not enhance their quality of life or mobility.
Level 1: Has the ability or potential to use a prosthesis for transfers or ambulation on level surfaces at fixed cadence. Typical of the limited and unlimited household ambulator.
Level 2: Has the ability or potential for ambulation with the ability to traverse low level environmental barriers such as curbs, stairs or uneven surfaces. Typical of the limited community ambulator.
Level 3: Has the ability or potential for ambulation with variable cadence. Typical of the community ambulator who has the ability to traverse most environmental barriers and may have vocational, therapeutic, or exercise activity that demands prosthetic utilization beyond simple locomotion.
Level 4: Has the ability or potential for prosthetic ambulation that exceeds basic ambulation skills, exhibiting high impact, stress, or energy levels. Typical of the prosthetic demands of the child, active adult, or athlete.
The records must document the beneficiary's current functional capabilities and his/her expected functional potential, including an explanation for the difference, if that is the case. It is recognized, within the functional classification hierarchy, that bilateral amputees often cannot be strictly bound by functional level classifications
-Noridian Healthcare Solutions, LCD Lower Limb Prostheses, ID#L11453
Functional Outcomes
• Medicare dictates componentry based on K-Level• Higher K-Level = more advanced technology and
materials, increased cost• Example-feet
– K0: n/a– K1: SACH foot– K2: multiaxial foot– K3: flex foot– K4: all
Functional Outcomes• Types of measure– Self report– Physical performance– Professional report
MDC- minimum amount of change in score to ensure result isn’t due to measurement error
Functional Outcomes
Self Report• Pain/Socket Fit Comfort• Lower Extremity Functional Scale• Other mobility scales
Functional Outcomes
Physical Performance• Amputee Mobility Predictor(AMP-Pro,-noPro)• Timed Up and Go (TUG)• L Test• 6 Minute Walk test
Functional Outcomes
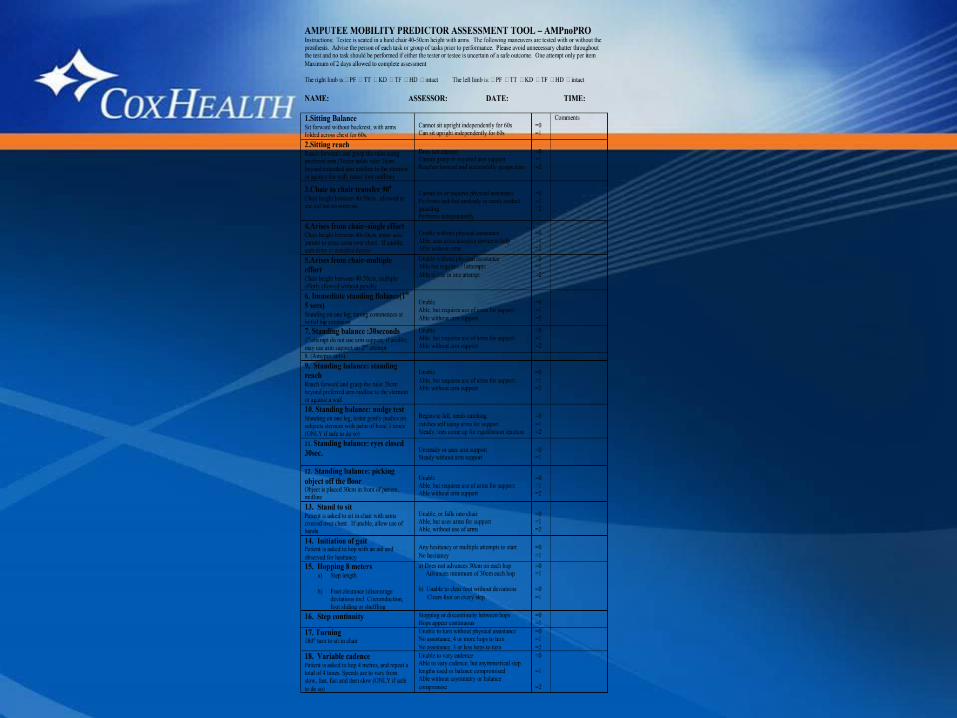
Amputee Mobility Predictor- AMP• Objective assessment of patient’s ability to
ambulate with prosthesis• Assist with K Level determination• AMP Pro…with prosthesis• AMP NoPro…without prosthesis• Same test• Arch Phys Med Rehabil Vol 83, May 2002
Robert S. Gailey, PhD, PT
Functional Outcomes
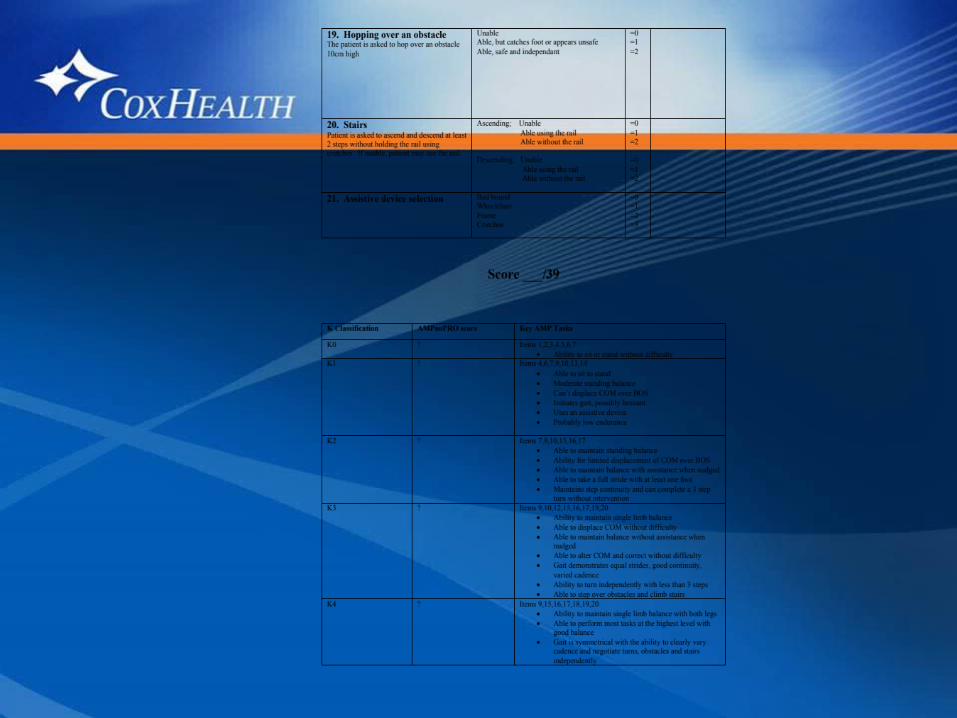
AMP- continued• 20 functional measurement items• Progress from least to most difficult• Approx 10-15 minutes• MDC established at 3.4• CPT 97750

AMP Scoring
K0 K1 K2 K3 K4AMP Pro n/a 15-26 27-36 37-42 43-47
AMP NoPro 0-8 9-20 21-28 29-36 37-43
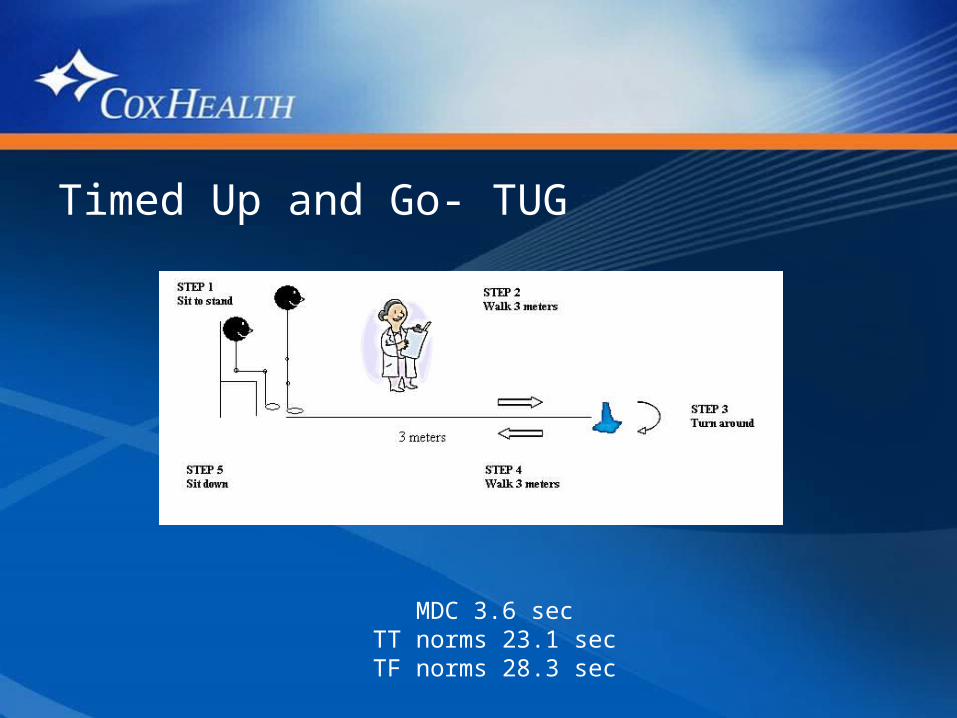
Timed Up and Go- TUG
MDC 3.6 secTT norms 23.1 secTF norms 28.3 sec
Minimal detectable change has been established at 3.0
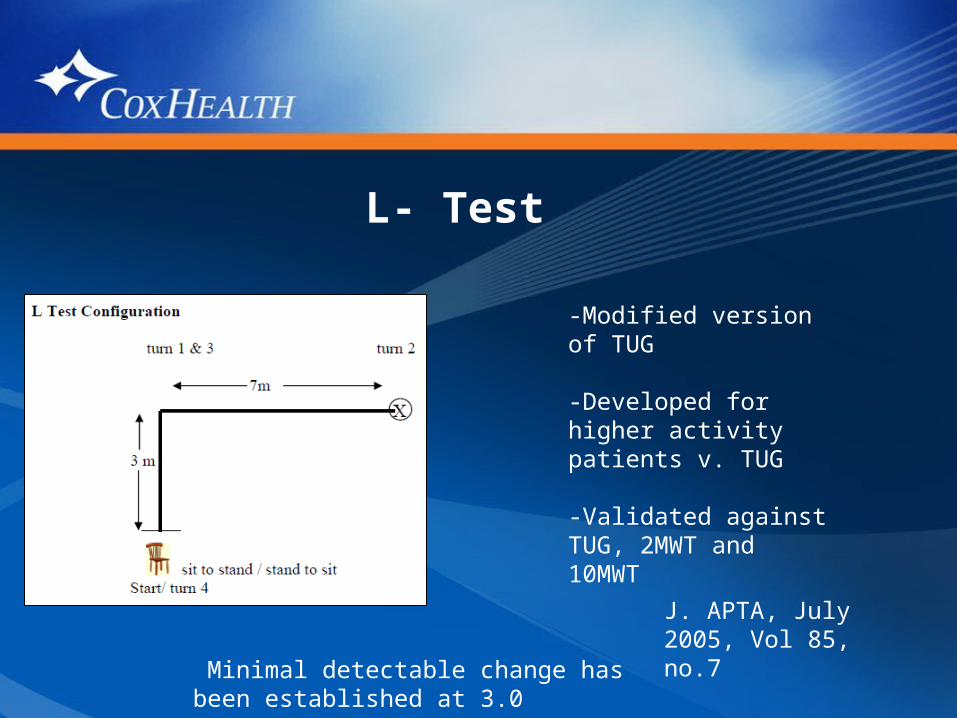
L- Test
-Modified version of TUG
-Developed for higher activity patients v. TUG
-Validated against TUG, 2MWT and 10MWT
J. APTA, July 2005, Vol 85, no.7
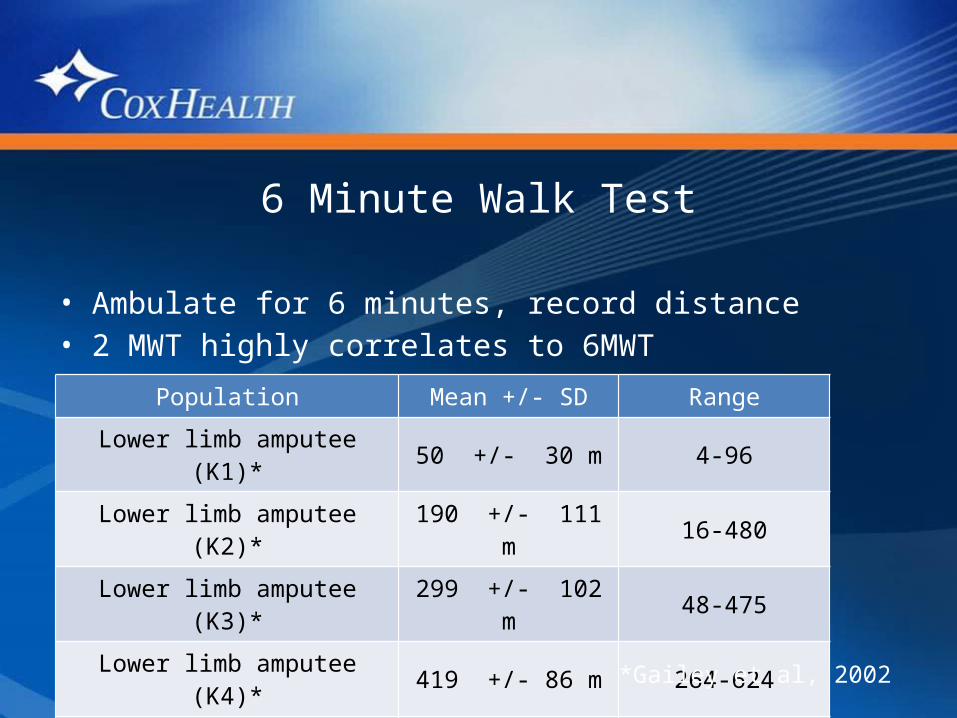
6 Minute Walk Test
• Ambulate for 6 minutes, record distance• 2 MWT highly correlates to 6MWT
Population Mean +/- SD Range
Lower limb amputee (K1)* 50 +/- 30 m 4-96
Lower limb amputee (K2)* 190 +/- 111 m 16-480
Lower limb amputee (K3)* 299 +/- 102 m 48-475
Lower limb amputee (K4)* 419 +/- 86 m 264-624
Health elderly adults^ 417 +/- 95 m n/a
*Gailey et al, 2002
Documentation• Document using language consistent with Medicare’s
language.– Mention the patient’s desire to ambulate.– State that the patient can vary their walking cadence (K3)– Document the patient’s ability to traverse low level
barriers (K2)• Document specific functional limitations• Document comorbidities thoroughly• Document prior level of function
Reasons for denial:• Documentation doesn't support the selected
functional level• Inadequate documentation that the patient will
reach or maintain a defined functional level within a reasonable time period
• No corroborating information in the physician's records
• No documentation that the patient is "motivated to ambulate"