fundamental questions
DESCRIPTION
Fundamental questions. How does the brain damage occur? Can we select at risk patients? What therapies do we have? How do they work? What is the side effect? What is the risk –benefit picture?. CBF & CPP. CBF - 50ml/100g/min -750ml/min – 15-20% CO 20-25 ml/100g/min – cerebral impairment - PowerPoint PPT PresentationTRANSCRIPT

Fundamental questions
How does the brain damage occur? Can we select at risk patients? What therapies do we have? How do they work? What is the side effect? What is the risk –benefit picture?
CBF & CPP
CBF-50ml/100g/min -750ml/min – 15-20% CO
20-25 ml/100g/min – cerebral impairment
15-20 ml/100g/min - isoelectric EEG
<10 ml/100g/min - irreversible damage
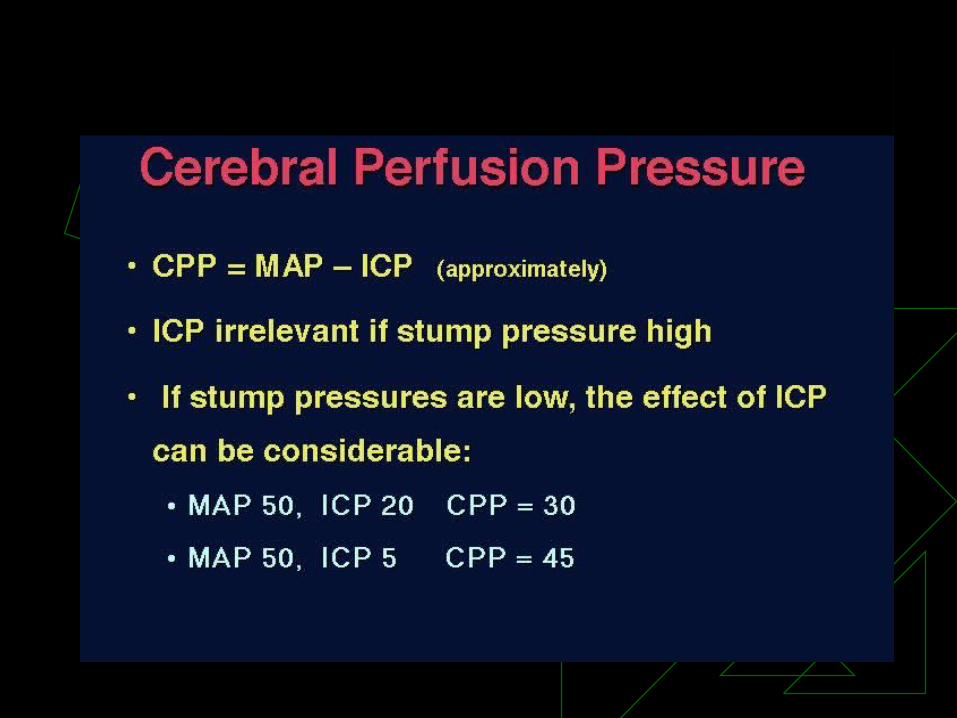
CPP = MAP – ICP : 80-100 –normal
<50 – slowing EEG ,cerebral impairment
25 - 40 – Flat EEG
<25 - irreversible damage

CBF- Auto regulation
CBF
MAP60 mmHg 160 mmHg
50

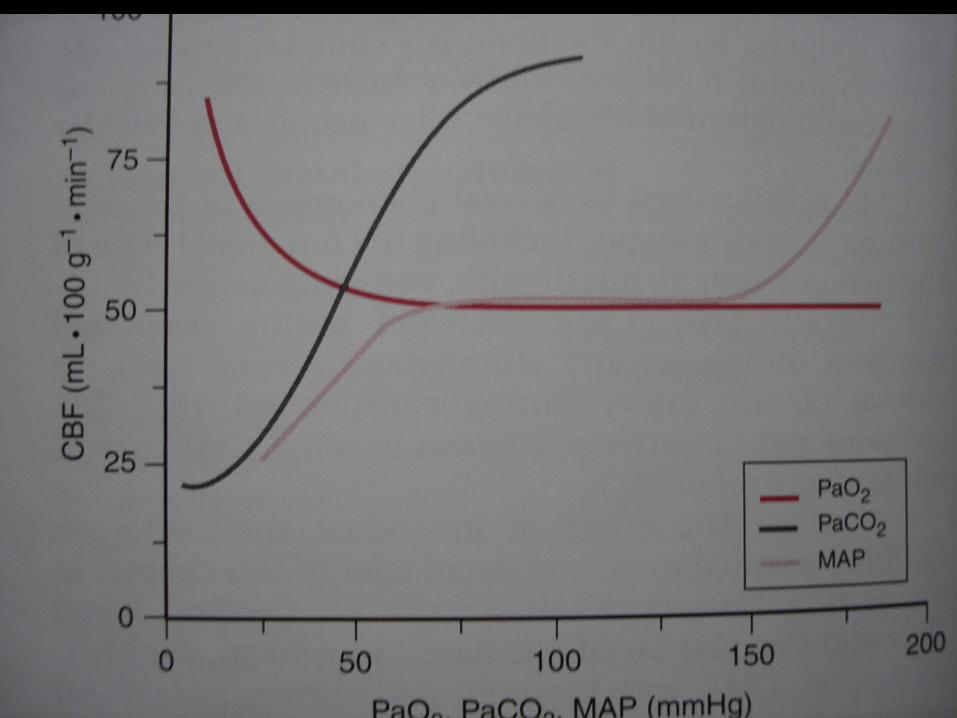
CBF &Variables
CBF depends on, PaCO2 (20-80mmHg)-1-2 ml/100g/min
/mmHg
T- 5-7%change/ 1 change
PaO2 <50 mmHg CBF
0


Cerebral protection

Cerebral protection -Strategies
Optimize CPP Decrease CMR Block the mediators of cell injury
- at ischemic cascade
- at reperfusion cascade

Protective techniques
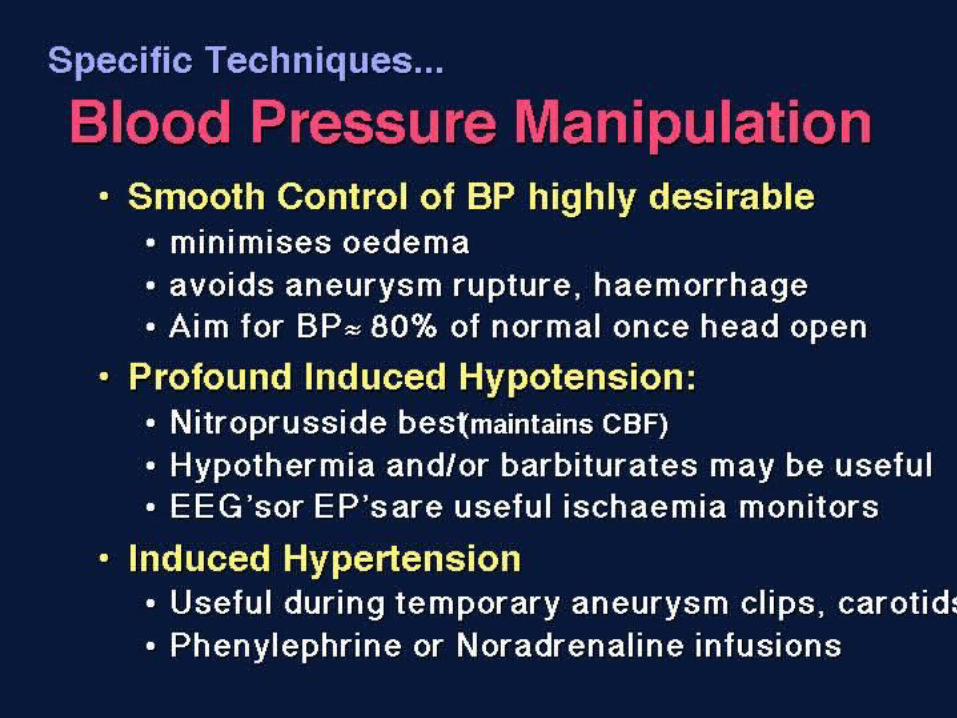
Brain Shrinkage Hyperventilation Optimize CPP Appropriate BP
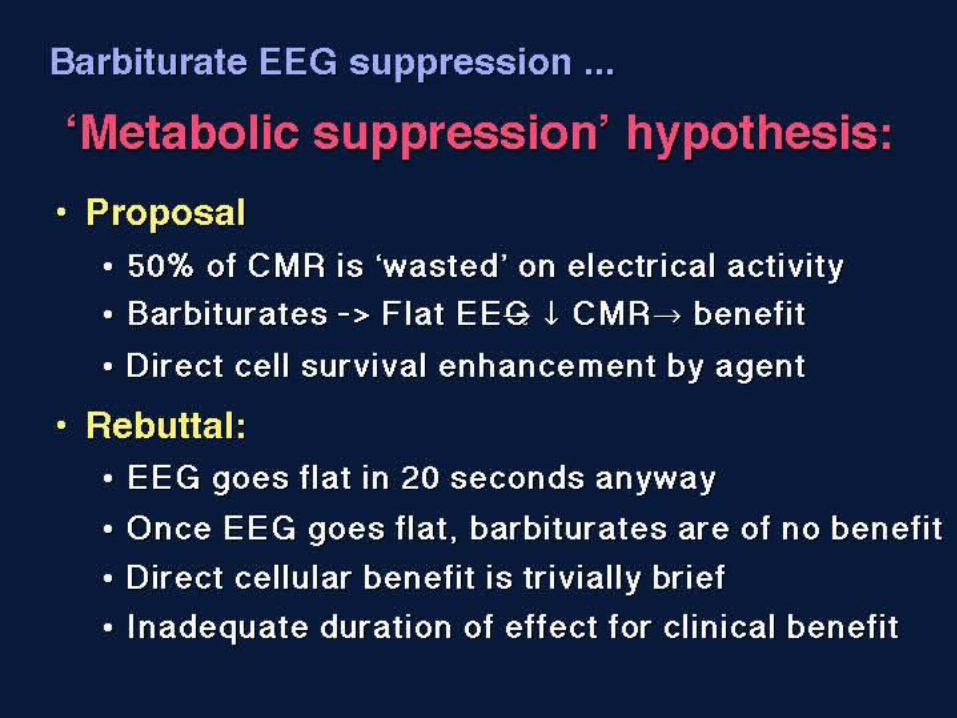
Hypothermia Decrease CMR Burst suppression
Pharmacological protectors -Block the mediators of cell injury

Brain shrinkage

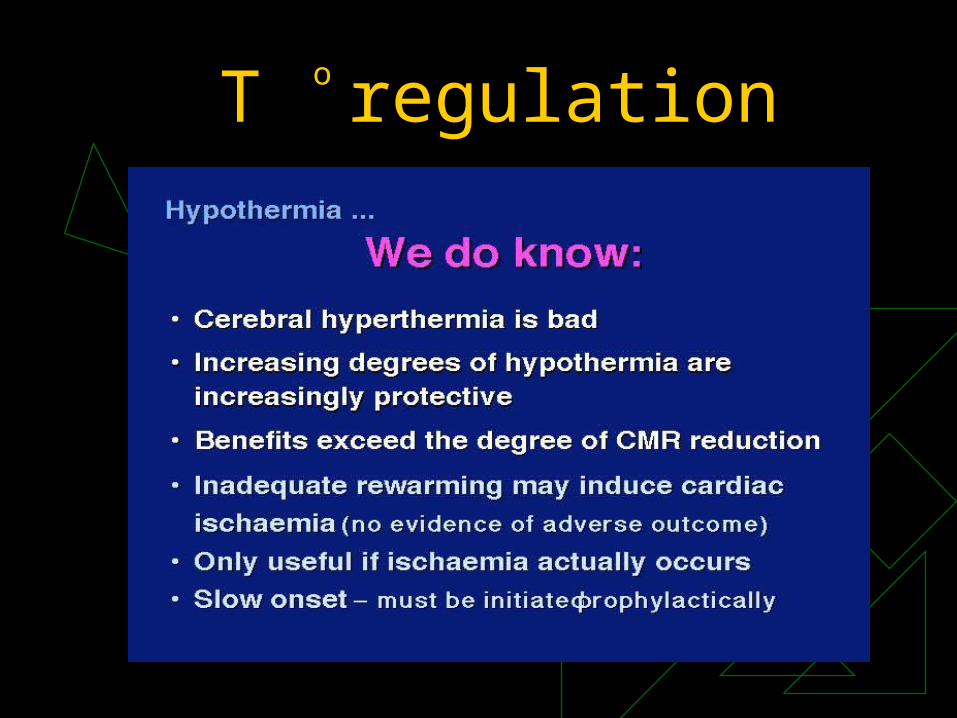
T regulationo
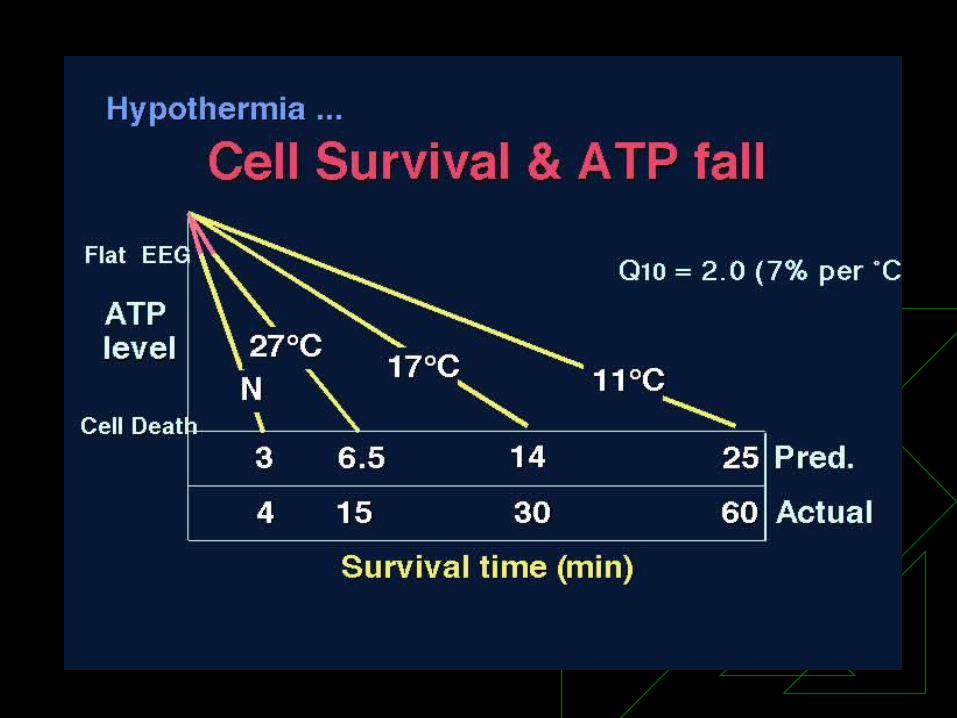

Mild hypothermia
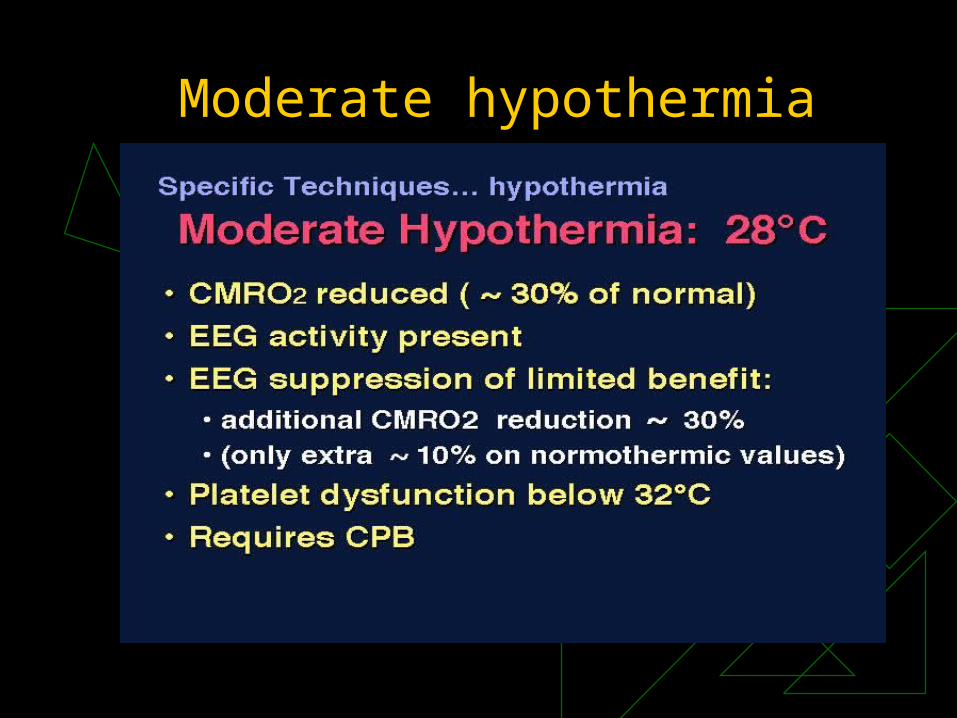
Moderate hypothermia

Profound hypothermia

Na-K pump failure
Na+
Ca+
Glutamate
Phosholipases
FFA
PL
ISCHEMIC CASCADE
TAXLTPG
OFR
Arachidonic acid
FFA
PL
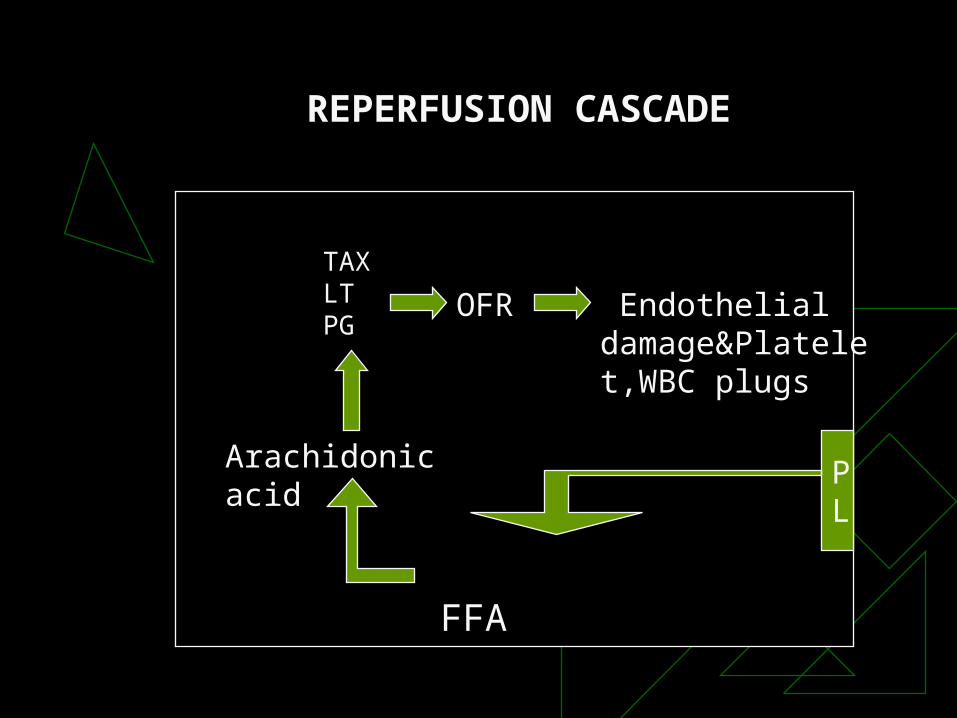
REPERFUSION CASCADE
Endothelial damage&Platelet,WBC plugs

Pharmacological intervention
CMR Reduction Barbiturates: Decreases CMR
Decreases Ca+
Decreases OFR
Na+ channel blockade
Decreases Glucose entry
Decreases refractory ICP
Inverse steal blood flow

Pharmacological intervention
CMR Reduction Propofol, Etomidate Morphine, Fentanil, Sufentanil,
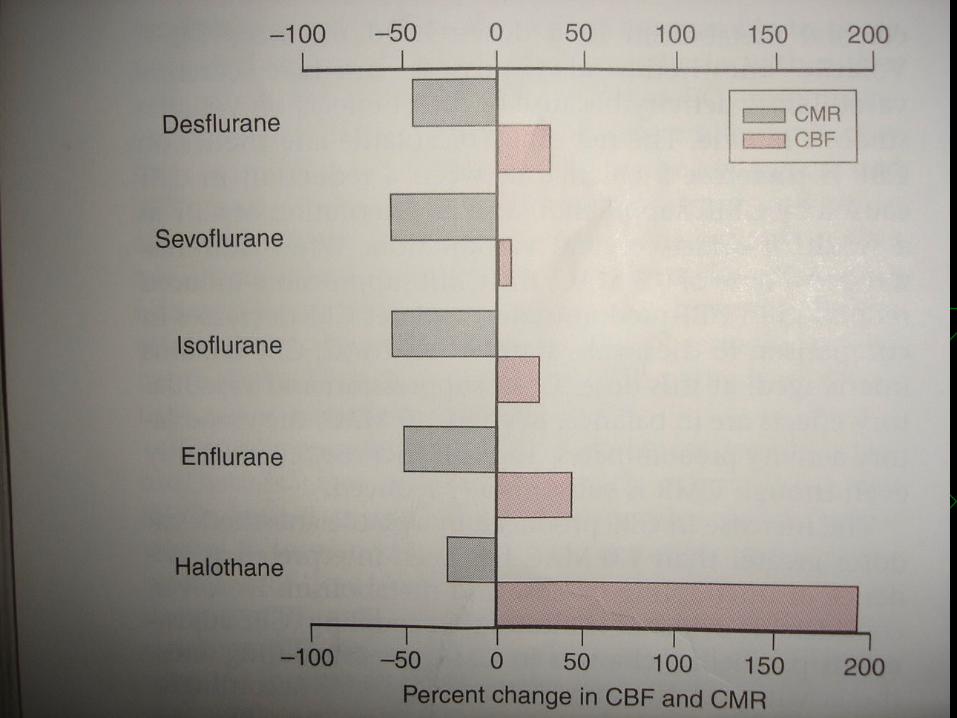
Remifentanil Diazepam, Midazolam Ketamine, Dexmedetomidine Halothane, Enflurane, Isoflurane,
Sevoflurane, Desflurane



Pharmacological intervention
Neuronal injury protectorsA} pre synaptic level- SNX III –Ca+ blocker
B} post synaptic level1.Na+ blocker- All volatile anaesthetic agents -Barbiturates -Lamotrigine - Riluzole -Lubeluzole2. Ca+ blocker -Nimodipine -Nicardipine
3.NMDA antagonists: Competitive blocker-Selfotel Non Competitive blocker-Dizoclypine -Dexromethorphan -ketamine

Pharmacological intervention
4.Glycine site analogues-felbamate, Licostinel
5.NO synthase inhibitors –lifarizine, 7nitroindazole
6.Mg+-Ca+ blockade, NMDA antagonist
7.steroids-anti inflammatory action, ?neuronal protection
-MPS, Tirilazad
8.OFR scavengers- Vit-E, PBN{phenyl derbuyl nitrone},
Tirilazad,Mannitol
9.Cytokinin inhibition-TNF Receptor I, TNF alfa mab
10. Anti adhesion molecule Ab


