future directions in hiv clinical research eric s. daar, m.d. chief, division of hiv medicine...
TRANSCRIPT

Future Directions in HIV Clinical Research
Eric S. Daar, M.D.Chief, Division of HIV MedicineHarbor-UCLA Medical Center
Professor of MedicineDavid Geffen School of Medicine at
UCLA

Overview
• Diagnosis
• Prevention
• Treatment
• Cure research

Diagnosis

Infected and UnawareIn
cid
ence
(%
)
Diagnosed Linked
to Care
Retained
In Care
Prescribed
ART
Viral
Suppression
85%
70%
36%
26%
41%
CDC and Prevention National HIV Surveillance System1
1. Hall HI, et al. 19th IAC. Washington, DC, 2012. Abstract FrLBX05.
2. Marks et al. AIDS 2006; 20:1447
n=1,148,200 HIV-infected persons, 18% of whom are unaware of their infection.
Females (n=279,200)
Males (n=869,000)81%
65%
35% 32%25%
~25% Unaware of Infxn
~75% Aware of Infxn ~46%
NewInfections
~54% New
Infections
New Sexual InfectionsPeople Living with HIV
Accounting for:
Transmission Risk2

Revised CDC Recommendations for HIV Testing in Healthcare Settings
• Routine testing all 13 to 64 years in healthcare settings– Not based on patient risk
• Opt-out testing • No separate consent for HIV• Pretest counseling not
required• Repeat HIV testing left to
discretion of provider– Based on patient risk
Branson BM, et al. MMWR Recomm Rep. 2006;55(RR-14):1-17.


Rapid Home HIV Testing(Approved July 2012)

Window Period and HIV Infection

Efficiency of HIV Transmission
Cohen MS, et al. JID 2005; 191:1391-3
Potential threshold for transmission
VL with intervention (e.g. ARVs)
VL in semen without ARVs

4th Generation Antigen/Antibody

Proposed Testing Algorithm
CDC. MMWR 2014


Future Directions for Diagnosis
• Expand testing
• Target high risk populations
• Identify early infection
• Making diagnosis is just the beginning

Prevention

Total: 35.0 million [33.2 million – 37.2 million]
Middle East & North Africa
230 000[160 000 – 330 000]Sub-Saharan Africa
24.7 million[23.5 million – 26.1 million]
Eastern Europe & Central Asia
1.1 million [980 000– 1.3 million]
Asia and the Pacific
4.8 million[4.1 million – 5.5 million]
North America and Western and Central Europe
2.3 million [2.0 million – 3.0 million]
Latin America
1.6 million[1.4 million – 2.1 million]
Caribbean
250 000[230 000 – 280 000]
Adults and children estimated to be living with HIV2013
Adults and Children Estimated to be Living with HIV- 2013

Estimated number of adults and children
newly infected with HIV2013
Middle East & North Africa
25 000[14 000 – 41 000]Sub-Saharan Africa
1.5 million[1.3 million – 1.6 million]
Eastern Europe & Central Asia
110 000 [86 000 – 130 000]
Latin America
94 000[71 000 – 170 000]
Caribbean
12 000[9400 – 14 000]
Total: 2.1 million [1.9 million – 2.4 million]
Asia and the Pacific
350 000[250 000 – 510 000]
North America and Western and Central Europe
88 000 [44 000 – 160 000]
Estimated Number of Adults and Children Newly Infected with HIV- 2013

Estimated New Infection in U.S. (2010)
Estimated total= 47,500

Preventing HIV Transmission

Scienceexpress, July 19th 2010.18th IAC 2010, Vienna, Austria, Abst. TUS505

Scienceexpress, July 19th 2010.
(N=444)
(N=445)
High adherers (>80%) effectiveness = 54%


Cu
mu
lati
ve P
rob
abili
ty o
f H
IV In
fect
ion
Weeks
N=64
N=36
Risk Reduction 44% (95% CI: 15, 63)
P=0.005
Grant R. et al. NEJM 2010, ePub ahead of press.
iPrEx Study (n=2499)

iPrEx Protection and Adherence
Overall >90% Adherence
Detectable Drug Levels
Grant R. et al. NEJM 2010, ePub ahead of press.

Efficacy (95% CI)
Conflicting Results with Oral PrEP Trials
0 10 20 30 40 50 60 70 80 90 100%
TDF for young heterosexuals
(TDF-2)63% (22; 83)
FTC/TDF for HIV discordant couples
(Partners PrEP)
75% (55; 87)
Modified from: Abdool Karim SS. Lancet 2013; 381(9883):2060-2.
TDF/FTC for MSM
and TW
(iPrEx)
44% (15; 63)
TDF/FTC for injecting drug users
(Bangkok TDF)49% (10; 72)
TDF for HIV discordant couples
(Partners PrEP)
67% (44; 81)
TDF/FTC for
women
(FEM-PrEP)
6% (-52; 41)
TDF for
women
(VOICE)
-49% (-129; 3)
TDF/FTC for
women
(VOICE)
-4% (-49; 27)
-70 -60 -50 40 -30 -20 -10

HPTN 052: Treatment as Prevention
Cohen MS, et al. IAS 2011. Abstract MOAX0102. Cohen MS, et al. N Engl J Med. 2011 Jul 18. [Epub ahead of print]
Immediate ART Initiate ART at CD4+ cell count 350-550 cells/mm3
(n = 886 couples)
Delayed ARTInitiate ART at CD4+ cell count ≤ 250 cells/mm3*
(n = 877 couples)
HIV-infected, sexually active serodiscordant
couples; CD4+ cell count of the infected partner:
350-550 cells/mm3
(N = 1763 couples)
*Based on 2 consecutive values ≤ 250 cells/mm3.
96% reduction in risk of transmission from those on treatment

Future Directions for Prevention
• Expand testing and early diagnosis
• Optimize treatment as prevention strategies– Linkage and retention into care– Adherence with therapy
• Refine PrEP strategies– Microbicide (e.g. dosing frequency, long acting forms)– Systemic (adherence interventions, dosing, long acting
therapy)
• Vaccine research

Treatment


Source: UNAIDS / Lohse et al / Hoog et al / May et al / Hogg et al
Projected Impact of ART on Survival of a 20-yo in a High Income Country

When to Start Treatment
Clinical CategoryCD4 Count (cells/mm3)
HIV RNA(copies/mL)
2014DHHS
Guidelines
2014IAS-USA
Guidelines
AIDS-defining illness or severe symptoms
Any value Any value Treat
Asymptomatic <500 Any value Treat
>500 Any value Treat
Pregnant women Any value Any value Treat
HIV-associated nephropathy
Any value Any value Treat
HIV/HBV coinfection when HBV treatment is indicated
Any value Any value Treat
DHHS. Available at: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Revision March 27, 2012; Thompson MA, et al. JAMA. 2012;308:387-402.
*Unless elite controller (HIV RNA <50 copies/mL) or has stable CD4 cell count and low-level viremia in absence of therapy.The IAS-USA guidelines also recommends initiating antiretroviral therapy in HIV-infected patients with active hepatitis C virus infection, active or high risk for cardiovascular disease, and symptomatic primary HIV infection.

HIV replication cycle and sites of drug activity
Capsidproteinsand viral
RNA
CD4Receptor
Viral RNA
New HIVparticles
Protease
Attachment Uncoating ReverseTranscription
Integration Transcription Translation
ReverseTranscriptase
Unintegrateddouble strandedViral DNA
Integratedviral DNA
ViralmRNA
Integrase
gag-polpolyprotein
1 2 3 4 56
Assembly andRelease
Protease InhibitorsIndinavir (Crixivan)Ritonavir (Norvir)
Saquinavir (Fortovase)Nelfinavir (Viracept)
Lopinavir/ritonavir (Kaletra)Atazanavir (Reyataz)
Fos Amprenavir (Lexiva)Tipranavir (Aptivus)Darunavir (Prezista)
NRTIsAZT (Zidovudine-Retrovir)
ddI (Didanosine-Videx)ddC (Zalcitabine-Hivid)d4T (Stavudine-Zerit)
3TC (Lamivudine-Epivir)ABC(Abacavir-Ziagen)
FTC (Emtricitabine, Emtriva)
NNRTIsEfavirenz (Sustiva)
Delavirdine (Rescriptor)Nevirapine (Viramune) (XR)
Etravirine (Intelense)Rilpivirine (Edurant)
Nucleus
Cellular DNA
HIV Virions
nRTITenofovir DF
(Viread)
Fusion InhibitorT-20
(Enfuvirtide, Fuzeon)
CCR5 AntagonistMaraviroc (Celsentri)
Integrase InhibitorRaltegravir (Isentress)
Elvitegravir /COBIDolutegravir (Trivicay)

Preferred Regimens
• EFV/TDF/FTC• ATV/r + TDF/FTC• DRV/r (once daily) + TDF/FTC• RAL + TDF/FTC•EVG/COBI/TDF/FTC•DTG + TDF/FTC•DTG + ABC/3TC[Pregnant Women Only: LPV/r (twice daily) + ZDV/3TC]
AlternativeRegimens
• EFV + ABC/3TC• RPV + (TDF or ABC)/(FTC or 3TC)• ATV/r or DRV/r + ABC/3TC• FPV/r or LPV/r (qd or bid) ABC/3TC or TDF/FTC• RAL + ABC/3TC
AcceptableRegimens
• EFV or RPV + ZDV/3TC• NVP + TDF/FTC or ZDV/3TC or ABC/3TC• ATV + (ABC or ZDV)/3TC• ATV/r, DRV/r, LPV/r, FPV/r , RAL + ZDV/3TC•MVC + ZDV or ABC/3TC•SQV/r + TDF/FTC or ABC/3TC or ZDV/3TC (with caution)
DHHS Guidelines May 2014: What to Start
DHHS Guidelines. Available at: http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf . Revision March 27, 2012.

HIV Cascade

Physical Manifestations of Fat Redistribution Syndromes

Increased age-related complications on ART
Frieberg et al., JAMA Internal Med 2013
Increased risk of AMI in HIV compared to HIV uninfected
HR = 1.48 (CI = 1.27 – 1.72)
Further increase HR if CD4<200 or HIV RNA>500
Mea
n A
MI e
vent
s pe
r
100
0 pe
rson
yea
rs
N=82,459; Veterans Ageing Cohort Study Virtual Cohort

36
Liver Kidney
Bone
Brain
Cardiovascular System
Genitourinary Tract

Lifestyle
Etiology of non-AIDS-related events• Non-AIDS-related events are more common in HIV disease, even after
adjustment for age, cART exposure and traditional risk factors
Deeks SG, Phillips AN. Br Med J 2009;338:a3172
cART
toxicity
Persistentinflammation(immune activation)
Non-AIDS
events
(e.g. smoking)

Inflammatory biomarkers remain elevated during long-term ART
Neuhaus JID 2010

Early ART is associated with less inflammation during ART
ART-naïve with CD4+ count > 500 cells/mm3
Early ART Group
Initiate ART immediately
N=2,300
Deferred ART Group
Defer ART until the CD4+ count declines to < 350 cells/mm3
N=2,300
START

Tenofovir alenofenamide (TAF): reduced toxicity
Zolopa CROI 2013, Atlanta, GA # 99LB
0
10
20
30
40
50
60
70
80
90
100
2 4 8 12 16 24
% H
IV-1
RN
A <
50
c/m
L
Time (Weeks)
TAF/FTC/EVG/c 88% (n=112)
TDF/FTC/EVG/c 90% (n=58)
TAF/FTC/EVG/COBI
Rx-naïve, VL >5000, CD4 >50 (N=170)


Studies of Neuropathogenesis
Central Nervous System• Timing of treatment
• Reducing inflammation
• Select or enhanced CNS active ART

Prevention of non AIDS events
• Lifestyle modifications– Reduce smoking, healthy diet, exercise
• Reduce modifiable risk factors– Assessment of blood pressure, glucose and lipids
• Counselling and screening for common cancers
• Enhance CD4 recovery and reduce inflammation
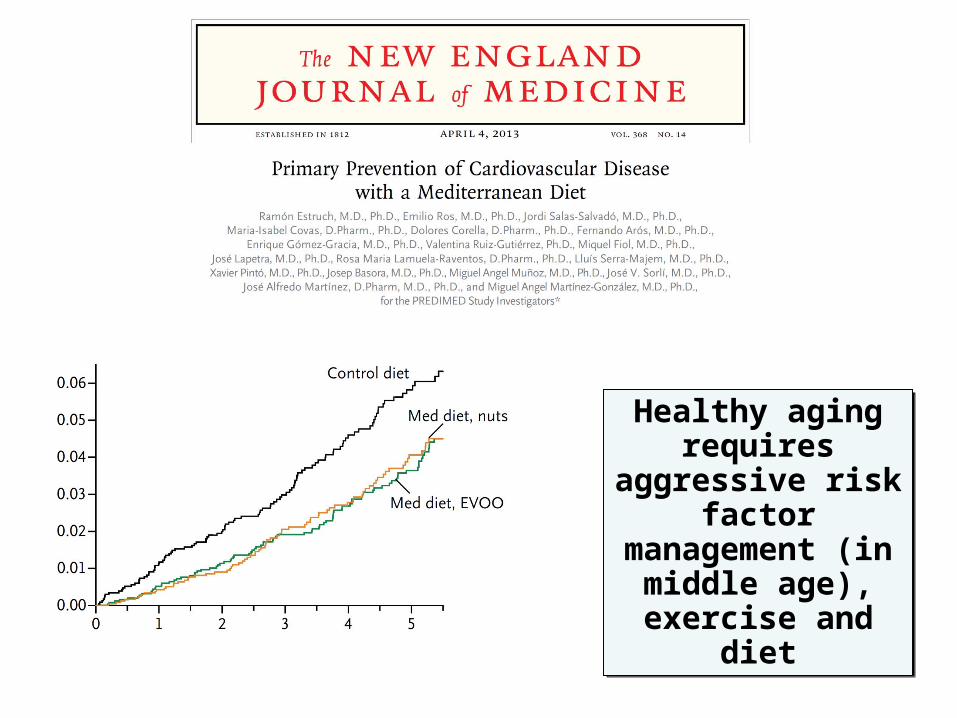
Healthy aging requires aggressive
risk factor management (in
middle age), exercise and diet
Healthy aging requires aggressive
risk factor management (in
middle age), exercise and diet

Future Directions for Treatment• Enhancing linkage and retention into care
– Outreach, patient navigators, incentives
• Defining benefits of early therapy– Prevent end-organ dz, delay non-AIDS events, transmission
• Optimizing treatment– New treatments/new formulations– Minimize toxicity– Target end-organs (e.g. CNS)
• Direct interventions to address chronic inflammation– Antiinflammatory– Target underlying pathogenesis

Cure Research


Siliciano JD, et al. Nature Med 2003;9:727-8
Obstacle to cure: At least one….
• Control• Purge• Minimize• Combination interventions

Procedure and Events• Ablative chemotherapy
• Total body XRT• Graft vs. host
• Transplant with CCR5∆32 homozygous donor
Hutter G, et al. N Engl J Med 2009; 360:692-8.

Saez-Cirion A, et al. PLOS Pathogen 2013; 9:e1003211
ANRS VISCONTI-14

Persaud D, et al. 21st CROI 2014, Abstract #75LB; Persaud D, et al. N Engl J Med 2013; 369: 1828-35
• Undetectable for ~2 years, including by provirus DNA, SCA, VOA and non-induced genome assay
Original report
• Sept 2014 announced confirmed viral rebound

1. Henrich TJ, et al. JID 2013; 207:1694-702.2. Henrich T, et al. 7th IAS Conference. Kuala Lumpur, 2013. Abstract WeLBA05.
• Treatment Interruption2
– Patient A: 7 weeks without detectable HIV RNA in plasma or DNA in PBMC– Patient B: 15 weeks without HIV RNA in plasma, DNA in PBMC and negative
single copy assay
• Extensive testing in setting of full donor chimerism failed to identify evidence of HIV infection of donor cells1
– Negative outgrowth assays and PCR with large number of PBMC and CD4 cells– No HIV DNA from rectal tissue– No HIV specific cellular immune responses

Boston Stem Cell Transplants Revisited
Henrich TJ, et al. 21st CROI 2014, Abstract #144LB
Days Post ATI

Zinc Finger Nuclease: Targeting CCR5

Conclusion
• HIV continues to be a global pandemic• Early diagnosis has potential to impact individuals and
the public• Multiple new interventions have shown promise in
reducing HIV transmission• Advances in HIV treatment are unprecedented in
medicine– Major benefits of treatment are limited by low rates of HIV
testing as well as poor linkage and retention in care– Persistent inflammation may have long-term consequences to
those on suppressive therapy• Cure research is heating up, energized by a high profile
anecdote and a few false hopes

Thank You!!