g. elzinga who, geneva 14 - 02 - 2005. who cares?
TRANSCRIPT
G. ElzingaWHO, Geneva14 - 02 - 2005
Who cares?

Life Expectancy: Advancing and Slipping
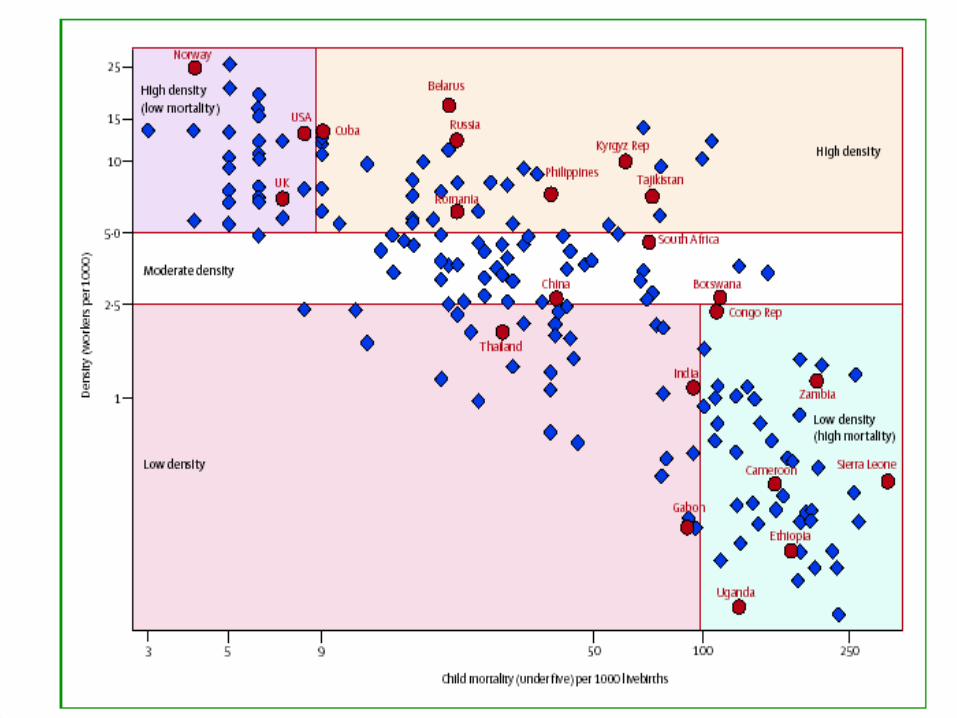
Differences in health
increase within countries
and between countries.
W
HY CAN’T
WE C
OPE?
HEALTH WORKFORCE PROBLEM
Joint Learning Initiative
Diagnosis (The Lancet, 27-11-2004)
Global Health Workforce cannot
cope with global health crisis;
SSA hit hardest
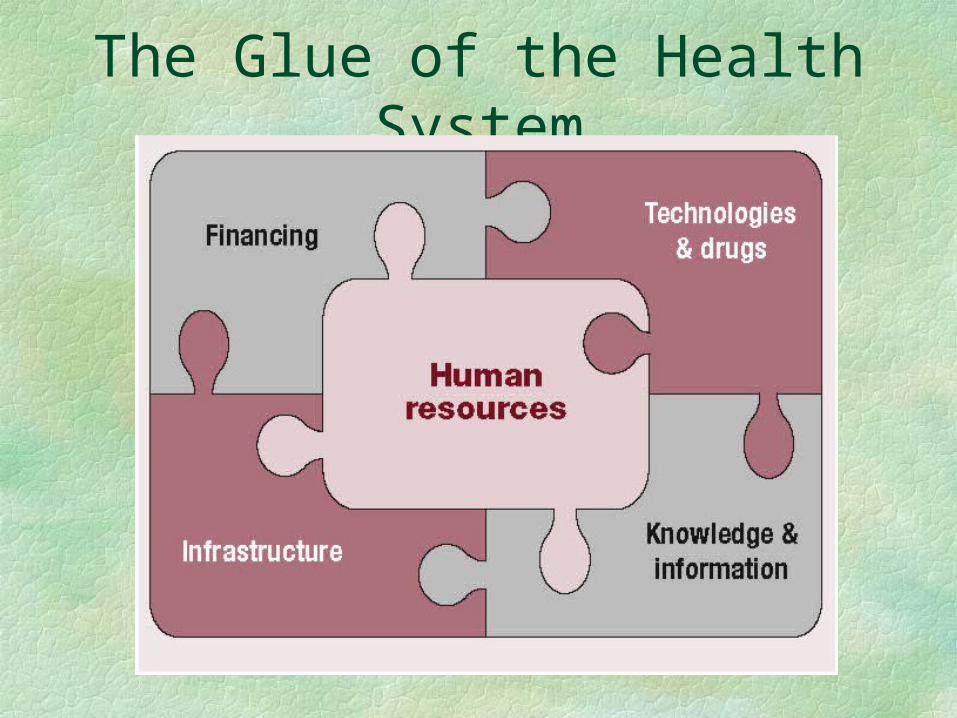
The Glue of the Health System
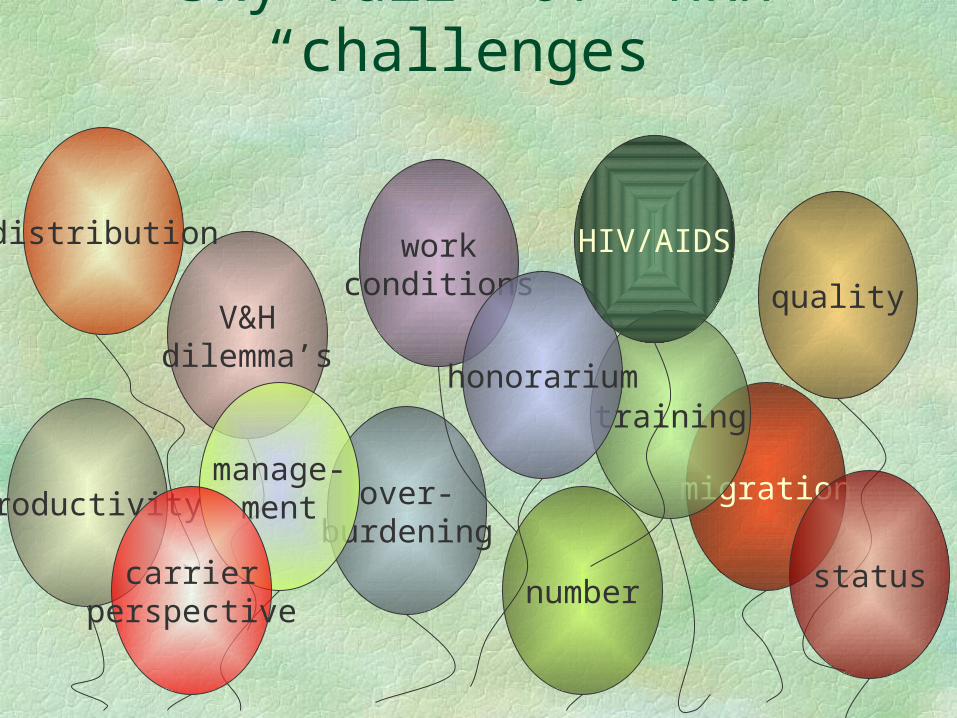
migration
training
Sky full of HRH “challenges”
V&Hdilemma’s
productivity over-burdening
workconditions quality
distribution
number
honorarium
manage-ment
HIV/AIDS
statuscarrierperspective
PROVIDING HEALTH IN POVERTY
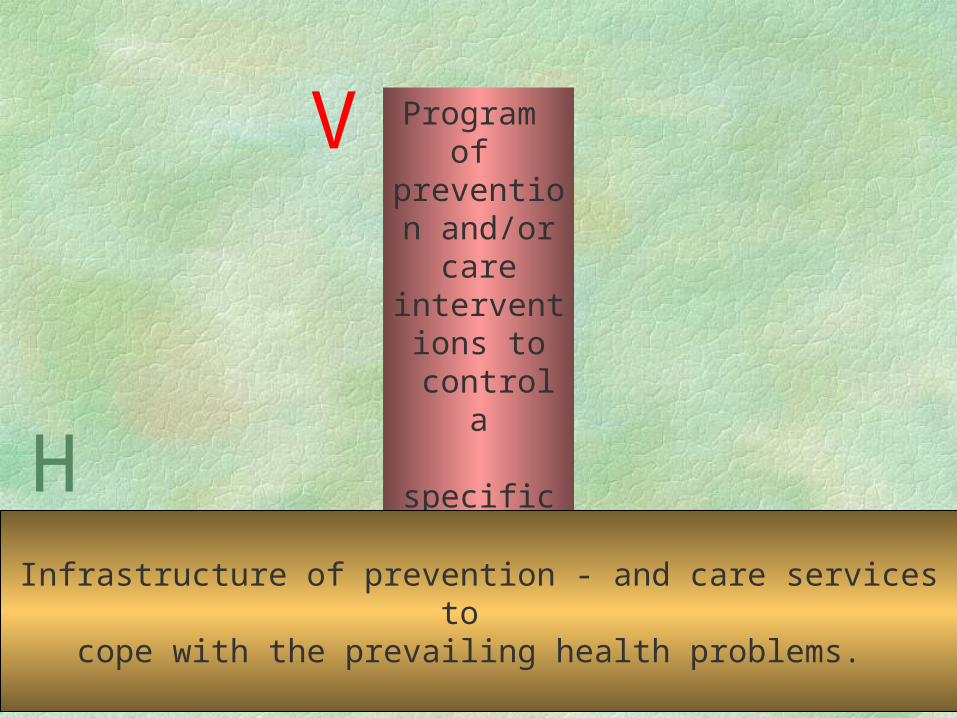
Program of
prevention and/or care
interventions to
controla
specific health-
problem.
V
Infrastructure of prevention - and care services to cope with the prevailing health problems.
H

VH
V
H
Vertical-horizontal indeveloping countries
Vertical-horizontal indeveloped countries
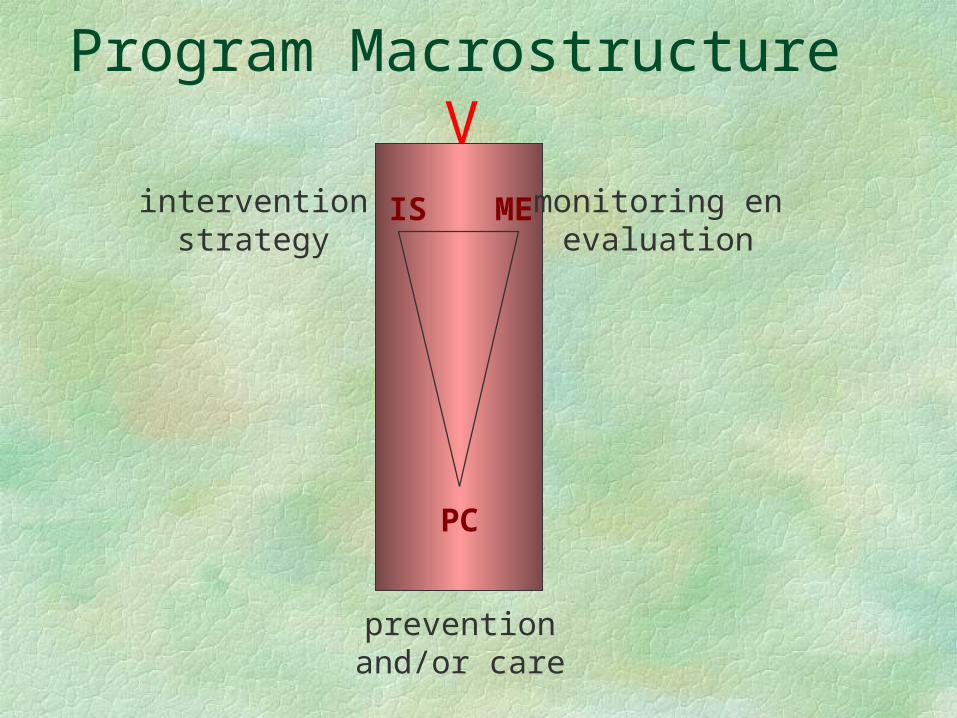
Program Macrostructure
MEIS
PC
Vintervention
strategymonitoring en
evaluation
preventionand/or care
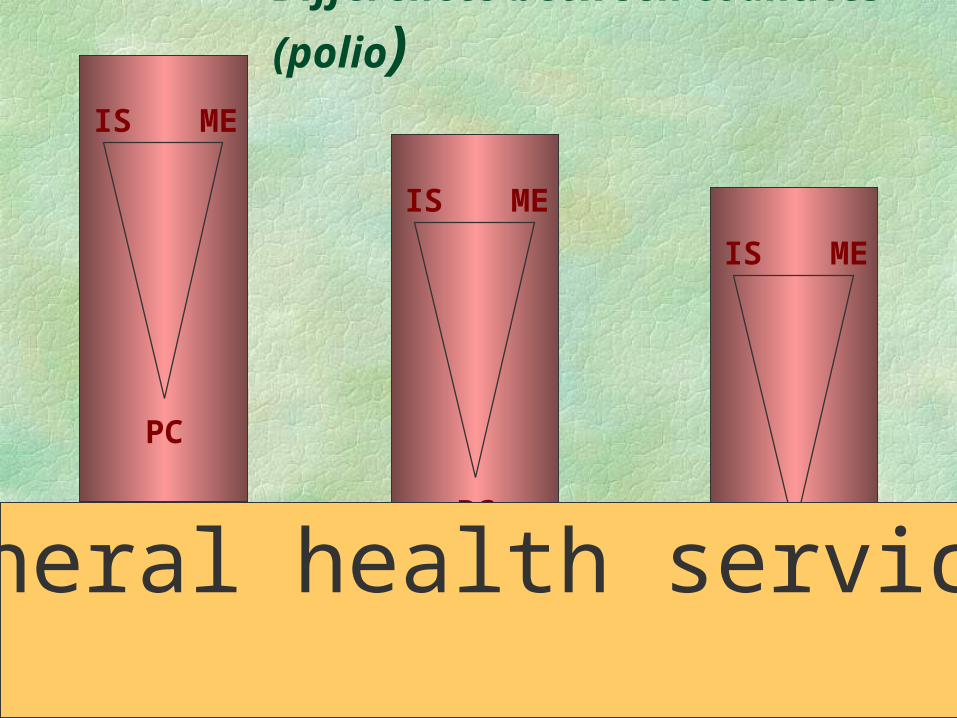
Differences between countries (polio)
MEIS
PC
MEIS
PC
MEIS
PC
General health services
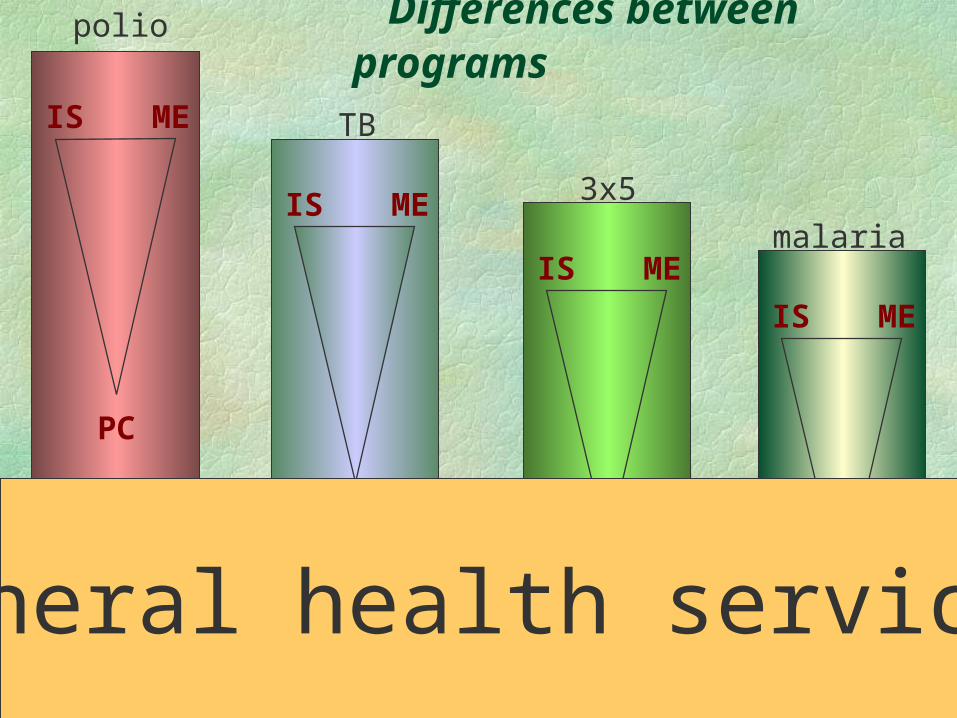
Differences between programspolio
MEIS
PC
TB
MEIS
PC
3x5
MEIS
PC
malaria
MEIS
PCGeneral health services
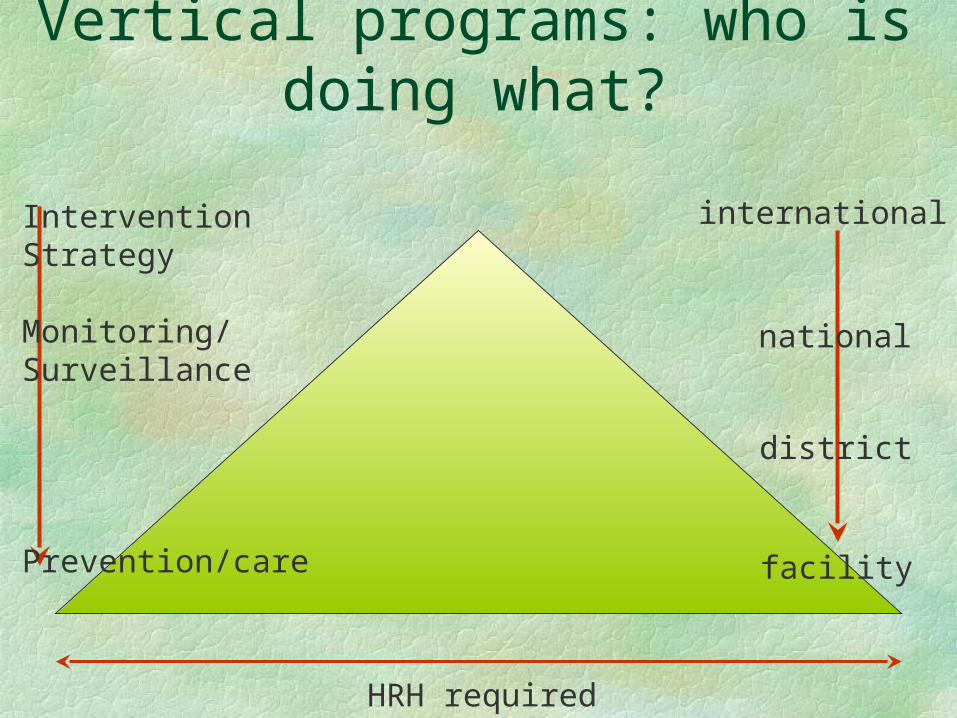
Vertical programs: who is doing what?
Intervention Strategy
Monitoring/ Surveillance
Prevention/care
international
national
HRH required
district
facility
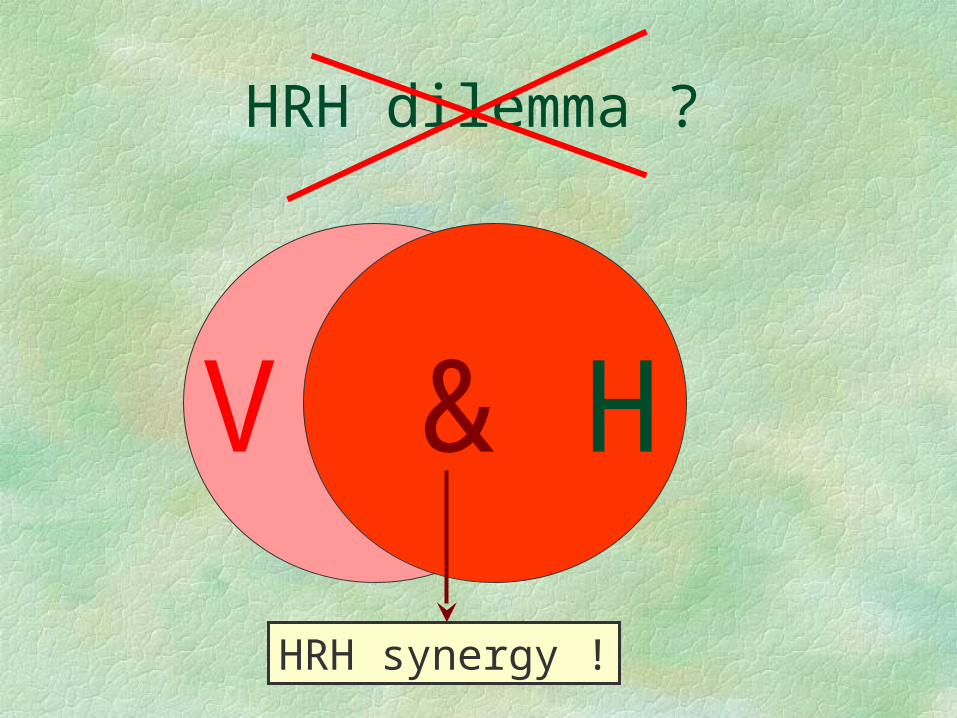
HRH dilemma ?
V H
HRH synergy !
&
RESEARCH CONTRIBUTIONS TO HEALTH WORKFORCE STRENGTHENING
Health systems and workforces are ‘man-made’
Research outcomes depend more on time and place than those of biomedical research.
However, research is not second rate: Relevance: crucial to reach health outcomes and
cost contaiment Intellectually: methodology often quite
demanding because of complexities
SPECIFIC
GENERIC
2 VALUABLE ‘RESEARCH’ LAYERS
SPECIFIC
POLICYCYCLE
analysis
M&E planning
implementation
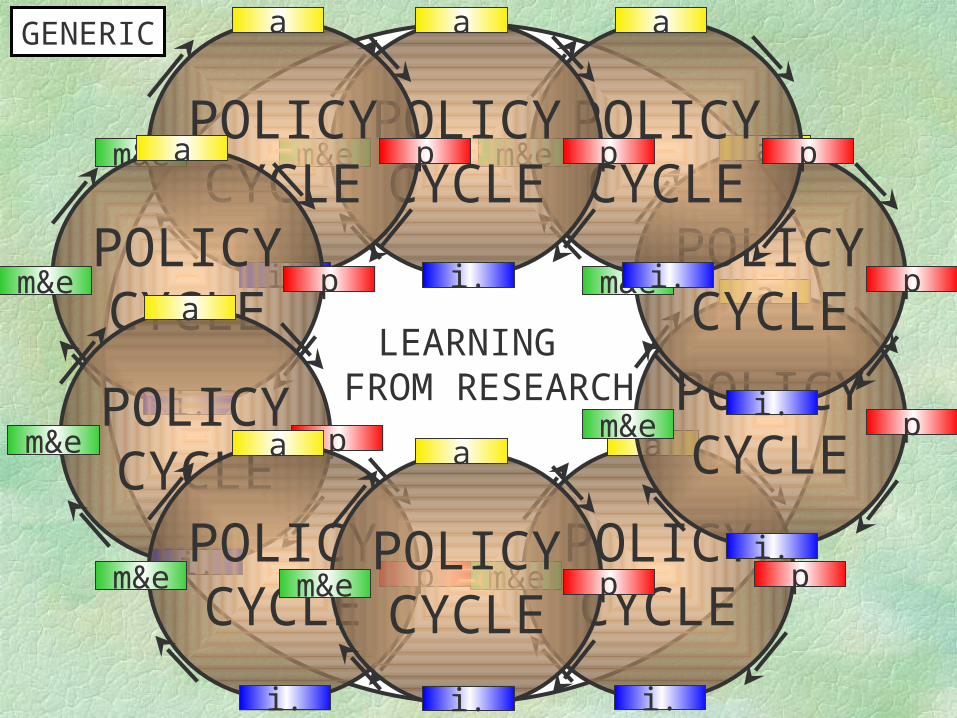
LEARNING FROM RESEARCH
GENERIC
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&ePOLICYCYCLE
a
p
i.
m&ePOLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&ePOLICYCYCLE
a
p
i.
m&e
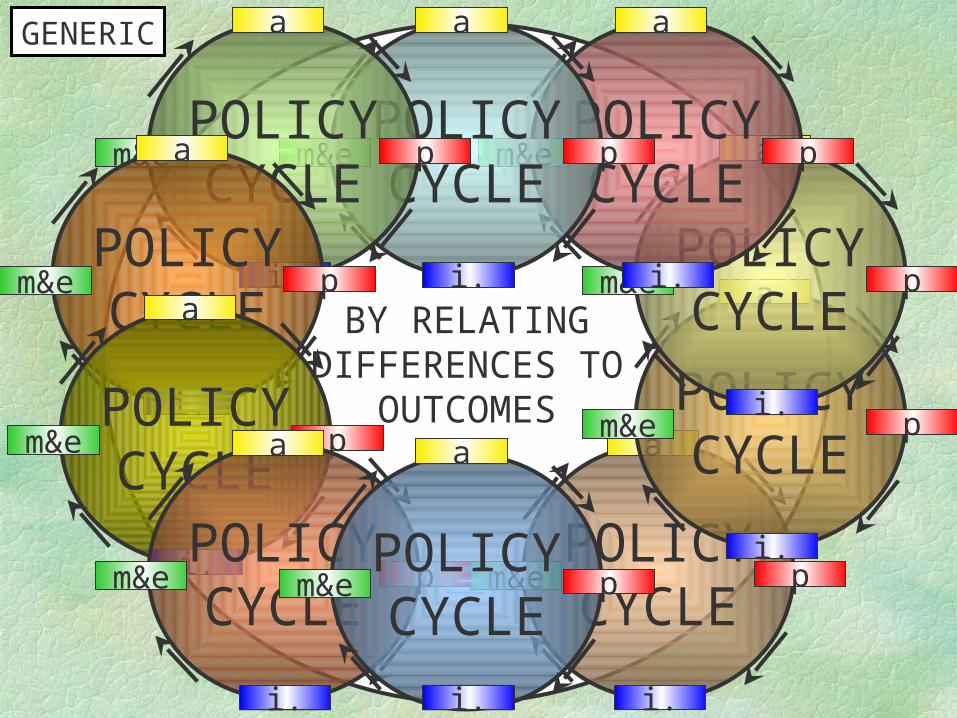
BY RELATINGDIFFERENCES TO
OUTCOMES
GENERIC
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&ePOLICYCYCLE
a
p
i.
m&ePOLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e
POLICYCYCLE
a
p
i.
m&e POLICYCYCLE
a
p
i.
m&e
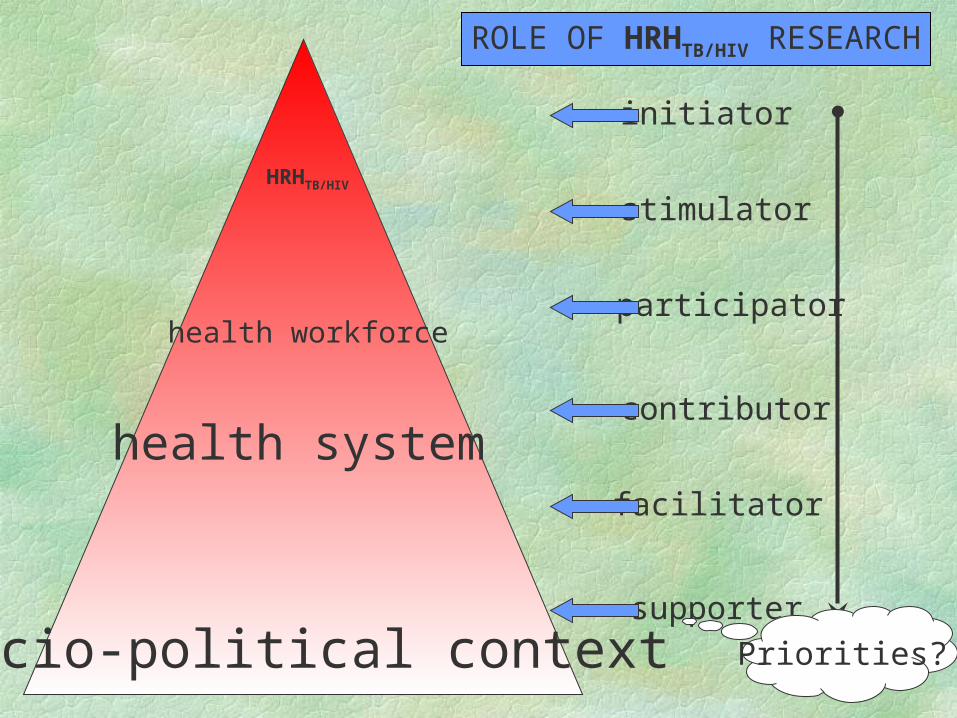
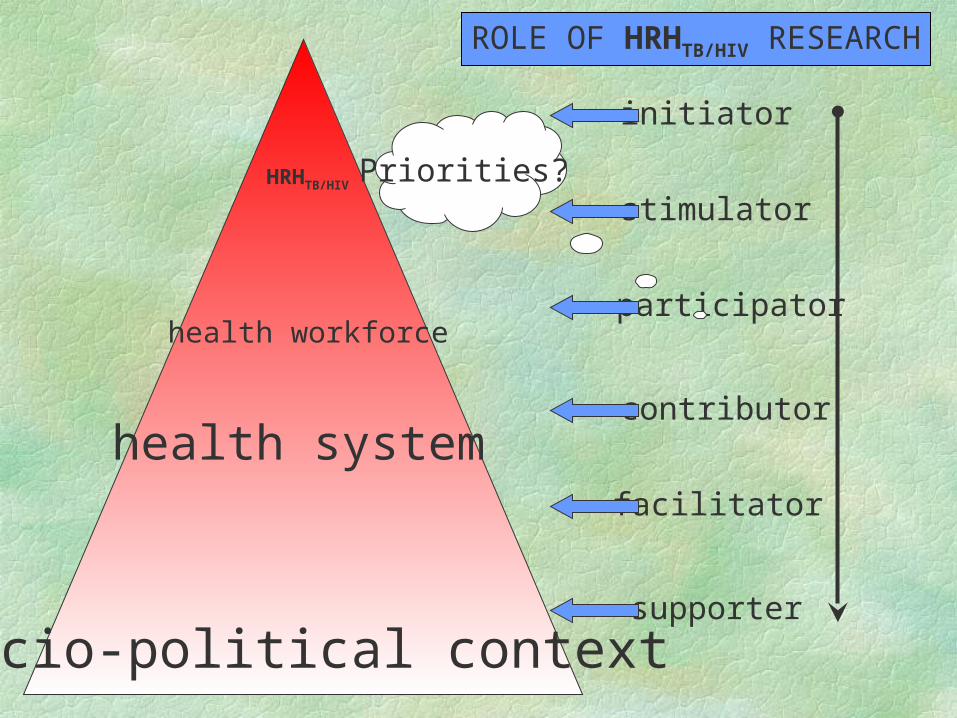
socio-political contexthealth systemhealth workforceHRHTB/HIV
socio-political context
health system
health workforce
HRHTB/HIV
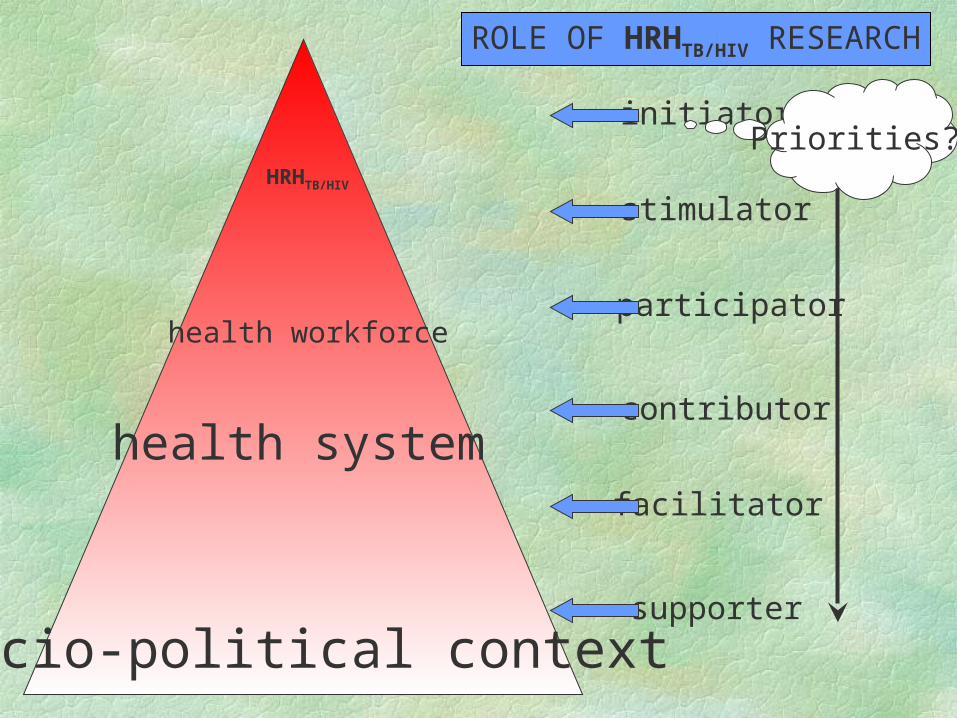
ROLE OF HRHTB/HIV RESEARCH
supporter
facilitator
contributor
participator
stimulator
initiatorPriorities?
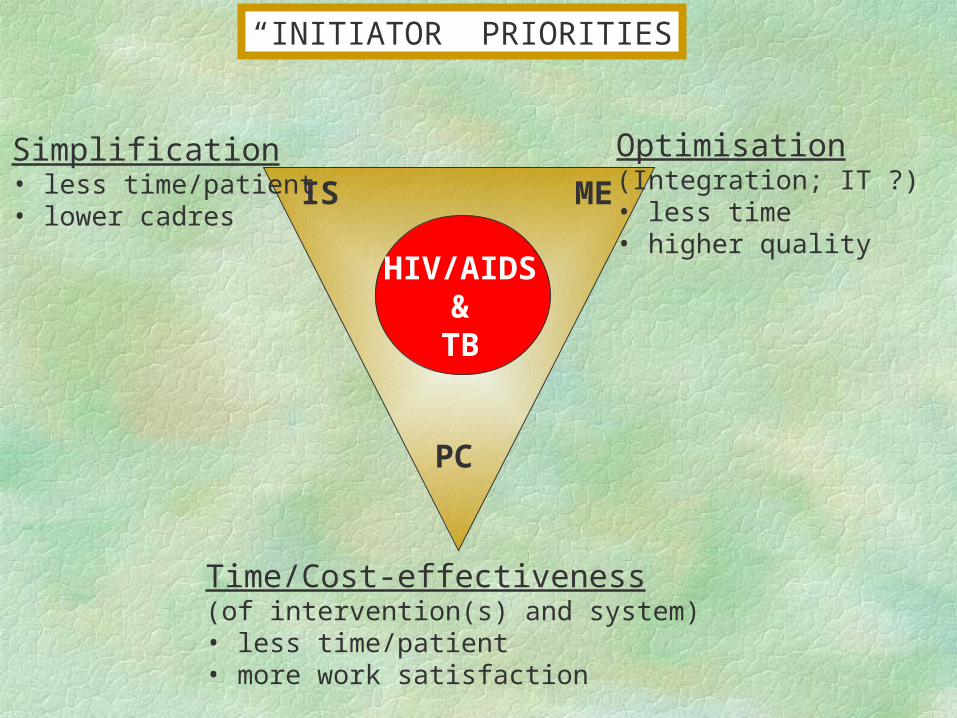
PC
IS MESimplification• less time/patient• lower cadres
Time/Cost-effectiveness(of intervention(s) and system)• less time/patient• more work satisfaction
HIV/AIDS&TB
Optimisation(Integration; IT ?)• less time• higher quality
“INITIATOR” PRIORITIES
socio-political context
health system
health workforce
HRHTB/HIV
ROLE OF HRHTB/HIV RESEARCH
initiator
participator
stimulator
contributor
facilitator
supporter
Priorities?

Policy truths
Economic
growth cures
poverty
Health Care is a cost not a profit
Thus, keep health expenditure low!
Social realitiesPoor populations havehigh disease burdens
They therefore needmore health services
while they can infact afford less.
Health belowa critical state tends
to deteriorate
HIV/AIDS & TB/HIVcan push health below that
critical state, causinglife expectancy to fall, the labor force to falter, and
social costs to sore!
EXAMPLES OF “SUPPORTER” PRIORITIES
WHAT REALISTIC INTERVENTIONS CAN COUNTER
MIGRATION OF HEALTH WORKERS?
WHEN DOES HEALTH CARE CHANGE FROM COST TO INVESTMENT?
Thank you
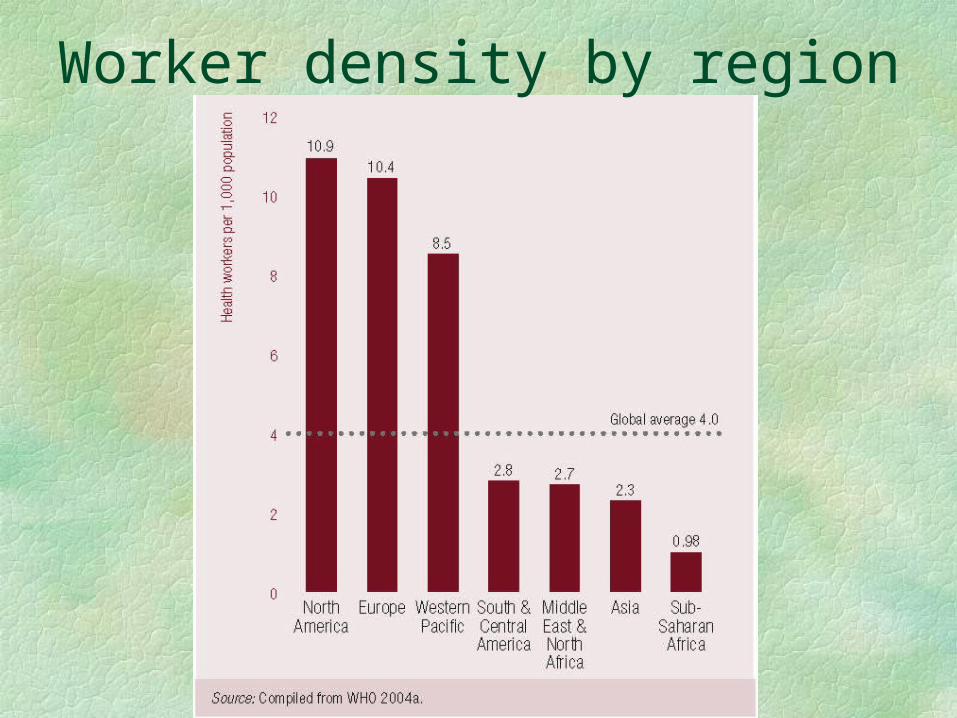
Worker density by region
socio-political context
health system
health workforce
HRHTB/HIV
ROLE OF HRHTB/HIV RESEARCH
initiator
participator
stimulator
contributor
facilitator
supporter
Priorities?
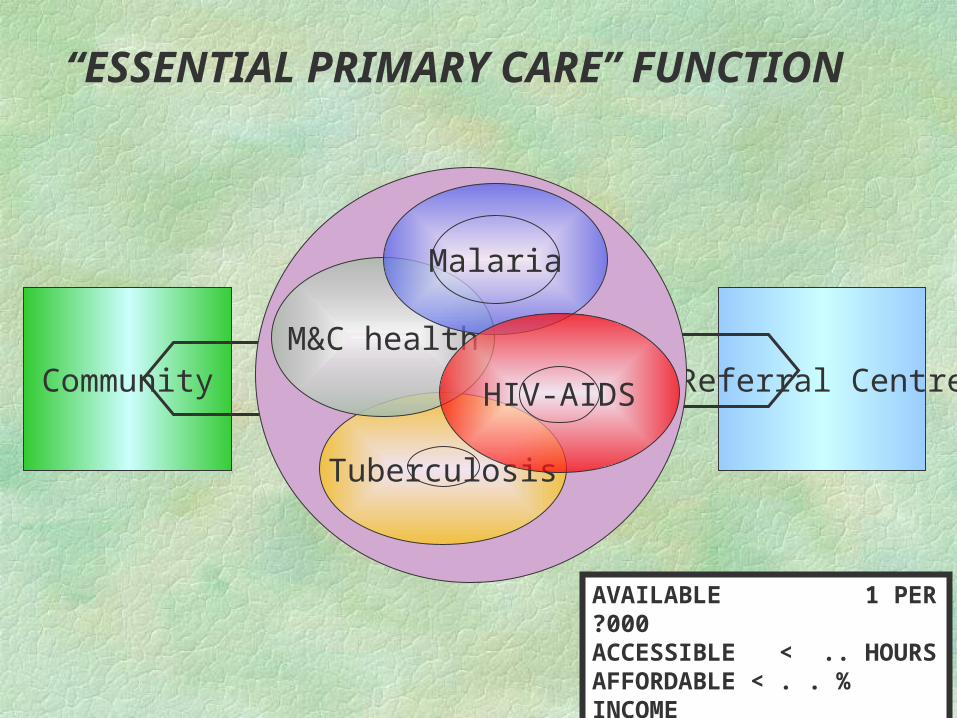
Community Referral Centre
“ESSENTIAL PRIMARY CARE” FUNCTION
AVAILABLE 1 PER ?000ACCESSIBLE < .. HOURSAFFORDABLE < . . % INCOME
Tuberculosis
M&C health
Malaria
HIV-AIDS
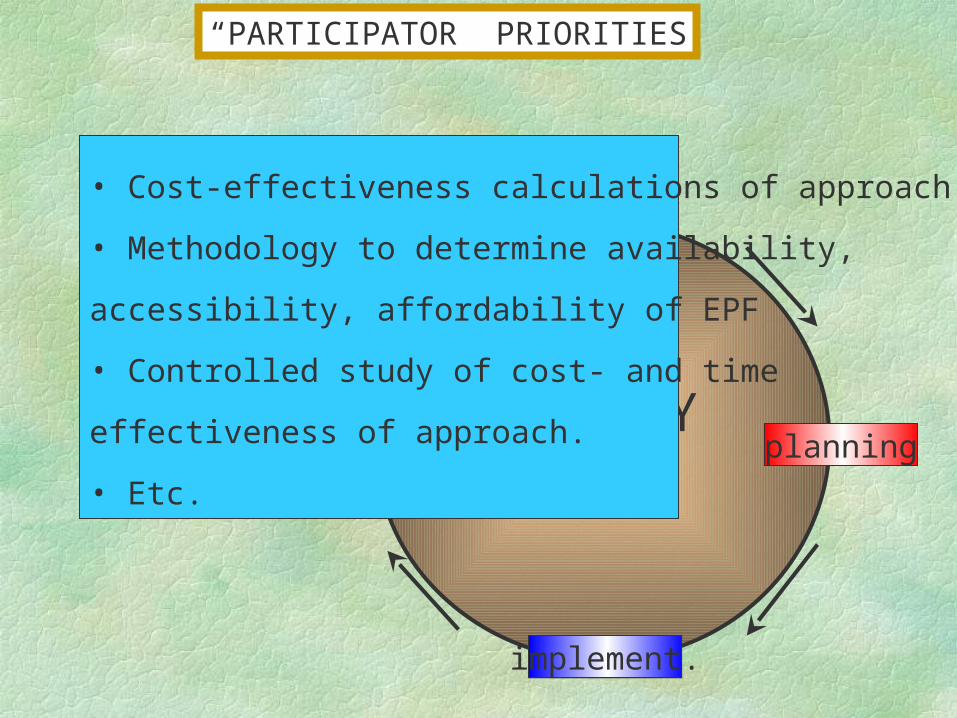
POLICYCYCLE
analysis
M&E planning
implement.
• Cost-effectiveness calculations of approach.
• Methodology to determine availability,
accessibility, affordability of EPF
• Controlled study of cost- and time
effectiveness of approach.
• Etc.
“PARTICIPATOR” PRIORITIES
MDG’s countries
donors High level forum WHO
Worldbank NGO’s
UNDP Post JLI ILO
Technical agencies Foundations
ILOPost JLI
Foundations
MDG’s countries
donors High level forum WHO
Worldbank NGO’s
UNDP
Technical agencies
THANK YOU
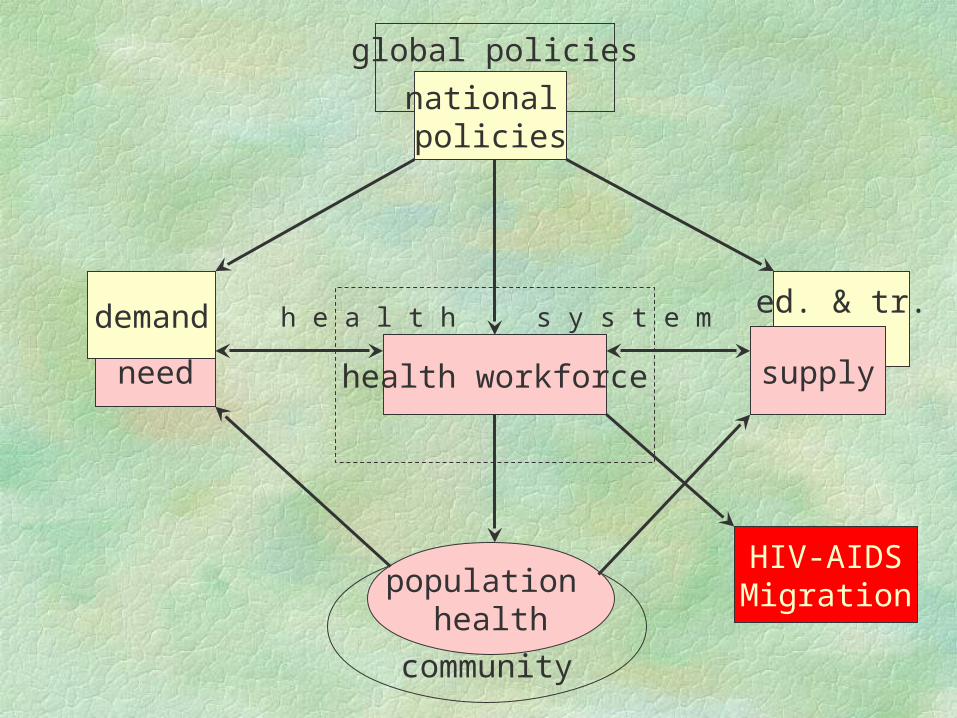
ed. & tr.
community
global policies
population health
need supplyhealth workforce
h e a l t h s y s t e m
national policies
demand
HIV-AIDSMigration
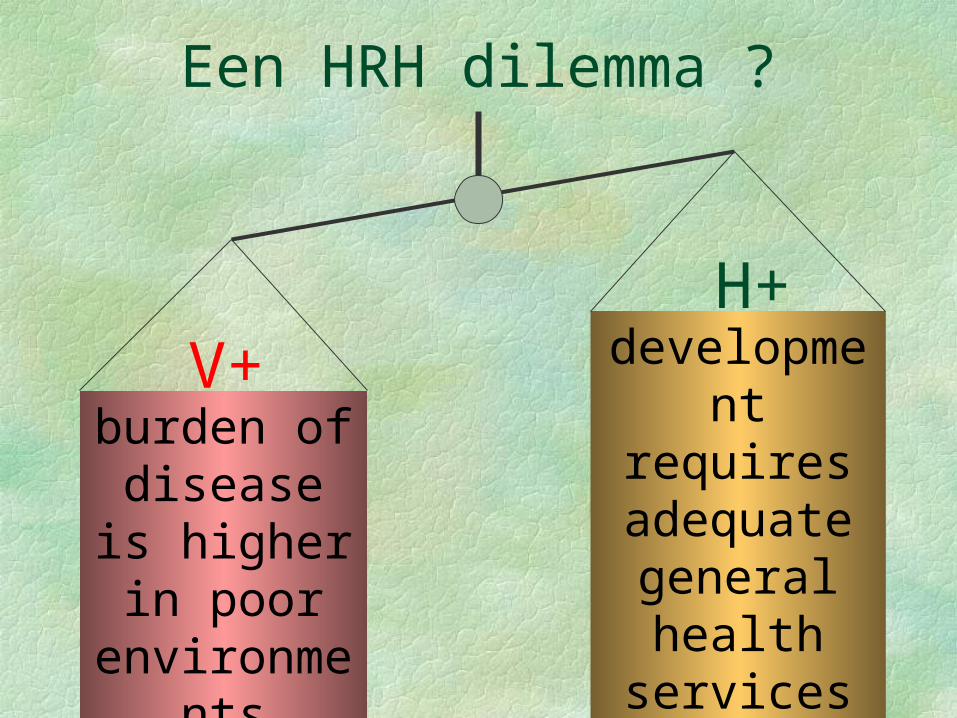
Een HRH dilemma ?
burden of disease is higher in
poor environments
V+ development requires adequate
general health services
H+