gaseous exchange
TRANSCRIPT

GASEOUS EXCHANGE

LEARNING OUTCOME (A)Student’s should be able to describe the structure of the human gas exchange system, including the microscopic structure of the walls of the trachea, bronchioles and alveoli with their associated blood vessels;Identify the structure of various tissue layers in the gaseous exchange systemConnect the role of various layers of tissue in the gaseous exchange system
Smooth muscle C-shaped cartilage
Identfiy and draw structure of chondrocytes Cilliated epithelial layer
Identify and draw cilliated cell Identify and draw goblet cells


TRACHEA
ciliated epithelium Goblet cells mucous glands C- shaped Cartilage rings





CILLIATED EPITHELIUM LAYER

LUNGSProtected by ribcageRib cage includes ribs and intercostal
muscles that help lungs expand and contract
Lungs connected to atmosphere by tracheaTrachea branches into 2 bronchiEach bronchi has many bronchiolesEach bronchiole has many air sacs (alveoli)


BRONCHUS

SECTION OF A TRACHEA


CARTILAGE TISSUE
Chondrocyte
Lacuna

BRONCHUS

BRONCHUS

BRONCHIOLE


RESPIRATORY BRONCHIOLE

TERMINAL BRONCHIOLE


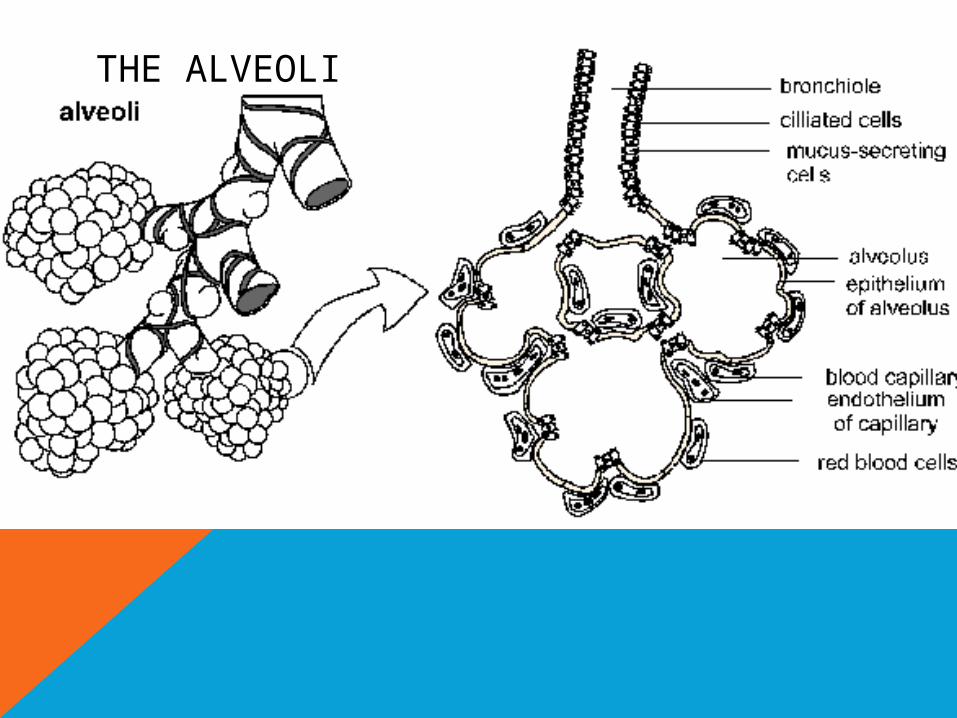
THE ALVEOLI

LEARNING OUTCOME (B) AND (C)Students should be able to describe the distribution of cartilage, ciliated epithelium, goblet cells and smooth muscle in the trachea, bronchi and bronchioles;Students should be able to describe the functions of cartilage, cilia, goblet cells, smooth muscle and elastic fibres in the gas exchange system;Connect the role of various layers of tissue in the gaseous exchange system
Smooth muscle C-shaped cartilage
Identfiy and draw structure of chondrocytes Cilliated epithelial layer
Identify and draw cilliated cell Identify and draw goblet cells

CARTILAGE
•Surrounds the trachea to provide structural support for the trachea and bronchus
•C-shaped/ horseshoe-shaped
•Rigid

GOBLET CELLSGlandular
columnar cellsSole purpose to
secrete mucusFound in
trachea, bronchus and (larger) bronchioles
Entraps particles and pathogens so that WBC can engulf them

CILLIATED EPITHELIUM CELLS•Thin layer of epithelial cells with hair-like organelles called cillia
•Responsible for moving (wave-like manner) entrapped dirt and pathogen particles up to the pharynx
•At the pharynx dirt laden mucus enters the esophagus and into the stomach
•In the stomach pathogens are destroyed due to acidic conditions
DO NOT CONFUSE IT
WITH VILLI OR
FLAGELLUM

SMOOTH MUSCLE
• Capable of contraction • Found in trachea, bronchi &
bronchioles • Its effect is in the bronchioles• Bronchioles are not supported by
cartilage • Contraction of the rings of
smooth muscles • around them causes the
bronchioles to constrict to control air flow

ELASTIC FIBERS
Allows alveoli to expand during inspiration and contract passively during expiration

ALVEOLUS

ALVEOLUS



no no

Airway No. Cartilage Goblet cells Smooth muscles
Cilia gas exchange
Trachea 1 Yes Yes Yes Yes No
Bronchus 2 Yes Yes Yes Yes No
Terminal bronchiole
48 000 No No Yes Yes No
Respiratory bronchiole
300000 No No No Yes Yes
Alveolar duct 9 x 106 No No No No Yes
Alveoli 3 x 109 No No No No Yes




LEARNING OUTCOME (D)Students should be able to describe the process of gas exchange between air in the alveoli and the blood;Describe the movement of oxygen from alveolar space into the blood vessels Describe movement of carbon dioxide out of blood out of into alveolar space
Able to understand the gradients involved Describe the manner in which the molecules move Features of the alveoli to increase efficiency of gas exchange
PROCESS OF GASEOUS EXCHANGE IN THE ALVEOLUSAir enters alveoli
Oxygen dissolves into film of liquid
Oxygen diffuses into blood or carbon dioxide diffuses out down concentration gradient
Gas passes through epithelium of alveolus and endothelium of capillary
Short distance between alveolus and capillary and thin wall of capillary allows efficient exchange of gas

ADAPTATIONS OF CAPILLARIES FOR GAS EXCHANGE
Thin cell wall (1 cell thick) approximately 0.5µm (squamous epithelium)
short diffusion distanceHigh amount of blood/capillaries quickly
takes away CO2 and supplies O2 (alveoli provide) large surface area (when
expanded) ;thinner layer of mucus/ moist surface ;

EMPHYSEMA
Healthy alveoli have elastin fibers around the alveoli
Alveoli will expand when filled with air
Elastin fibers will force the alveolus to return to their original shape

LEARNING OUTCOME (E)Students should be able to describe the effects of tar and carcinogens in tobacco smoke on the gas exchange systemDescribe the effect of TAR on the cilliated epithelial layer
Describe the sequence of events that lead to chronic bronchitis a form of COPD
Describe the sequence of events that lead to the formation of cancer cells in the gaseous exchange system

EFFECT OF TAR ON GASEOUS EXCHANGE
Settle on the lining of the airways in the lungsIt is an irritant that causes inflammation of
the mucus membranes lining the trachea, bronchi, bronchioles (Bronchitis)
As a response to tar deposition, goblet cells produce more mucus
Cillia would be paralysed as mucus and tar accumulates
So these cilia cannot remove the mucus secreted by the epithelial lining.
Also components of tar (benzpyrene) are carcinogenic and can cause lung cancer

LEARNING OUTCOME (F)Students should be able to describe the signs and symptoms of lung
cancer and chronic obstructive pulmonary disease Identify how the sequence of events in developing lung cancer and
COPD may result in symptoms Identify how symptoms may bot be absolute indications of the
disease Identify how the diseases influence lung capacities and volumes

There are four volume subdivisions which:
do not overlap.
can not be further divided.
when added together equal total lung capacity.

TIDAL VOLUME
INSPIRITORY RESERVE
VOLUME
EXPIRATORY EXPIRATORY RESERVE RESERVE
VOLUMEVOLUME
VITAL CAPACITY
RESERVE VOLUME
INSPIRATION CAPACITY
Lung capacities and volumes
EXPIRATION CAPACITY
FUNCTIONAL RESIDUAL CAPACITY TOTAL
CAPACITY



DEFINITIONS Tidal volume
Inspiratory reserve volumeExpiratory reserve volumeVital capacity
Residual volume
Total lung capacity
Volume of air breathed in and then breathed out during a single breath
After a normal inspiration and continue to inhale or the amount of air that can be taken into lungs after normal expiration
After a normal expiration and continue to exhale or the amount of air that can be exhaled after a normal inhalation
Maximum volume of air that can be exchanged during one breath in and out (forced inspiration and expiration)
The volume of air that is always left in the lungs.(Air remain in the lungs even after forced expiration)* Without the residual volume, the moist walls of the alveoli would stick together and it would be impossible to re-inflate the lungs
Total volume of air that the lungs can hold

Total Lung Capacity (TLC). The volume of air contained in the lungs at the end of a maximal inspiration. Called a capacity because it is the sum of the 4 basic lung volumes. TLC=RV+IRV+TV+ERV
Vital Capacity (VC). The maximum volume of air that can be forcefully expelled from the lungs following a maximal inspiration. Called a capacity because it is the sum of inspiratory reserve volume, tidal volume, and expiratory reserve volume. VC=IRV+TV+ERV=TLC-RV
Functional Residual Capacity (FRC). The volume of air remaining in the lung at the end of a normal expiration. Called a capacity because it equals residual volume plus expiratory reserve volume. FRC=RV+ERV
Inspiratory Capacity (IC). Maximum volume of air that can be inspired from end expiratory position. Called a capacity because it is the sum of tidal volume and inspiratory reserve volume. This capacity is of less clinical significance than the other three. IC=TV+IRV

EMPHYSEMA
Healthy alveoli have elastin fibers around the alveoli
Alveoli will expand when filled with air
Elastin fibers will force the alveolus to return to their original shape
EMPHYSEMAA result of heavy smokingWBC will produce a type of enzyme
(elastase) that breaks down elastinNormally a protein inhibitor will prevent
this from happeningIn smokers chemicals in the cigarette
smoke inactivate protein inhibitors. Increased Elastase activity and
breakdown of Elastin

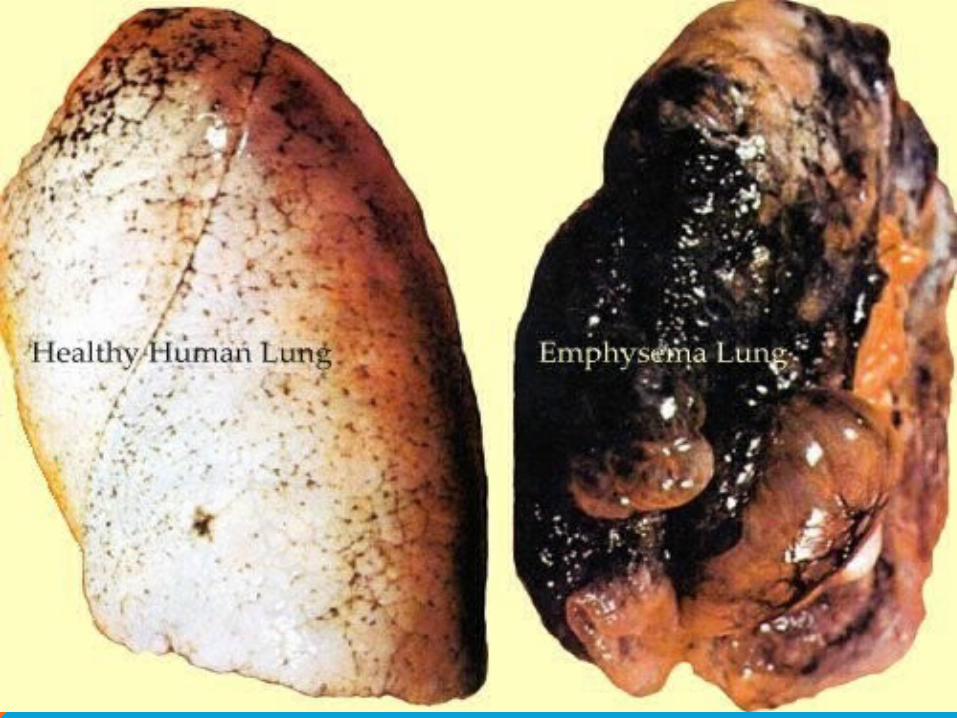
•Breakdown of elastin results in alveoli unable to return to original size
•Very little exchange of gas occurs as air remains in the lungs

CHRONIC BRONCHITISCaused by an accumulation of irritants
(such as tar, asbestos dust etc.) in trachea, bronchus and bronchioles
Goblet cells respond by over-producing mucus thick mucus makes it difficult to remove all the dirt and pathogens
Smooth muscle spasms Acumulation of dirt results in bacterial
infectionBronchiole lining gets inflamed and narrows
airways


•Results in coughing (a reflex to get rid of excess mucus)
•Breathlessness (restricted air movement in the bronchioles)


LEARNING OUTCOME (G)Students should be able to describe the effects of nicotine and carbon monoxide on the cardiovascular systemRecognize nicotine and carbon monoxide as components of cigarette smokeRecognize that nicotine and carbon monoxide will enter the blood circulatory system but not TAR

MAIN COMPONENTS OF CIGARETTE SMOKETarCarbon monoxideNicotine

EFFECT OF CARBON MONOXIDE ON GASEOUS EXCHANGECarbon monoxide readily diffuses through the walls
of alveoli in the lungHb has a higher affinity for carbon monoxide than it
has for oxygenBinds with haem groups in Hb to form
carboxyhaemglobinOxyhaemoglobin releases its oxygen BUT
carboxyhaemoglobin not released
Hb is not available to carry oxygen

EFFECT OF NICOTINE
Acts as a vasoconstrictorIncreases heart rate and blood pressureMakes blood platlets more ‘sticky’Reduces bloodflow to extremitiesDamages endothelium of arteriesLess glucose/ oxygen supplied to the heartLess waste removedCauses heart to contract less strongly

LEARNING OUTCOME (H)Students should be able to explain the link between smoking and atherosclerosis, coronary heart disease and Recognize that nicotine and carbon monoxide will enter the blood circulatory systemIdentify the effects of nicotine and carbon monoxide on tissues in the circulatory system and how it initiates the beginning of certain chronic diseases

ATHEROSCLEROSIS
Damage to artery inner lining/ endothelium due to CO or nicotine
Development of atheroma which consists of dead muscle, fibers and cholesterol.
high amounts of LDL molecules will deposit cholesterol in damage sites
deposition of fatty plaque and cholesterol will block the arteries.
Blood will no longer be able to flow properly and will clot and form a thrombus.

Cholesterol
Lipoprotein
Low density lipoproteinLDL
High density lipoproteinHDL
~ Transport cholesterol from the liver to the
tissues~ They tend to deposited
their cholesterol at any damage site
~ Remove cholesterol from tissuesand transport it to the liver
~ Helps to protect arteries against atherosclerosis


Normal arterythrombus

CORONARY HEART DISEASEWhen atherosclerosis occurs in the heart
arteries, it can starve the heart muscle of oxygen
Angina pectoris-blockage of heart arteries. Heart starved of oxygen. Accumulation of lactic acid causes acute pain.
Myocardial infarction- heart arteries blocked. Death of heart muscle.
Heart faliure-heart weakened due to blockage. Long term effect.

LEARNING OUTCOME (I)Students should be able to evaluate the epidemiological and
experimental evidence linking cigarette smoking to disease and early death;
Understand the differences between epidemiological and experimental evidence
Use knowledge in identifying trends in data to support or oppose the idea that smoking and diseases are linked.

EPIDEMIOLOGICAL EVIDENCE OF SMOKING AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE Epidemiological evidence of smoking and
disease50% smokers die due to smoking-related diseaseSmokers 3x more likely to die in middle ageCOPD incidences increase in smokers but is rare in non smokers
Emphysema -98% of emphysema patients are smokers; 20% of smokers are suffering from emphysema
Chronic bronchitisLung cancer
Risk of lung cancer increases when:Smokers inhaleStart youngNo. of cigarettes smoked per day increasedSmoke high tar cigarettes

HOWEVER….Epidemiological evidence provides no direct
link to disease. Only shows a casual associationMany other things can cause lung disease,
eg. Air pollution, occupation, climate.Epidemiological evidence is highly
dependant on data collection and interpretation. Eg. Were all the populations sampled, What other factors contribute to COPD?


PROVING THE LINKS BETWEEN SMOKING & CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
Experimental evidence shows a direct link between smoking and pulmonary diseases
Experiment 1:48 dogs were divided into 2 groups1 group exposed to filtered cigarette smoke & did not develop cancerThe other was exposed to unfiltered cigarette smoke & developed
abnormalities similar in humans lung cancer patientsThe group with filtered cigarettes had some dogs develop precancerous
lesions

Experiment 2:Lab mice painted with cigarette
tar develops cancerous growths
Proves the presence of carcinogenic chemicals in cigarette tar


•There is no positive correlation AW e.g. no link/no direct connection,between increased cigarette consumption and number of deaths;
•use of comparative figures to support this; both no of cigarettes and deaths must
•be quoted (2 sets of figs needed)
•people die before COPD develops (sufficiently);
•only 20 countries;
•cause of death may not be recorded accurately/maybe other cause(s) recorded on death certificate;
•COPD contributed to death but not main cause;
•maybe other factors contribute to developing COPD eg. air pollution/occupation/
•climate/population density;
•maybe other factors involved with smoking are more important e.g. number of years
•smoked/number of cigarettes smoked by smokers;

LEARNING OUTCOME (J)Students should be able to discuss the difficulties in achieving a
balance between preventions and cure with reference to coronary heart disease, coronary by-pass surgery and heart transplant surgery;
Understand the difference between coronary bypass and heart transplant
Understand the differences and difficulties in preventing a chronic disease and curing a chronic disease

CORONARY BYPASSBlockage in the coronary
artery may be difficult to remove especially if extensive
Ablood vessel from another part of the body is used to bypass the blocked section to allow blood to flow through
This allows the heart to continue to receive oxygen

HEART TRANSPLANTHeart transplant patients
require a donor heart to be provided and replace their own damaged heart
Requires a suitable donor. Lack of a donor results in high mortality rates in heart disease patients
High chance of complications even with a suitable donor ie. rejection