gastric cancer final
TRANSCRIPT

Gastric cancer
Hamzeh Halawani M.D.
American University of Beirut

EPIDEMIOLOGY
• The most common cancer among men in Japan.• Highest incidence in China
• Generally-- Disease of the elderly• Lower socioeconomic status• Blacks 2 times > whites
Younger patients-- more of the diffuse variety• Large• Aggressive, • Poorly differentiated,• Sometimes infiltrating the entire stomach (linitis plastic)

Primary
Common Primary
• Adenocarcinoma (95%),
• Lymphoma (4%),
• Malignant GIST (1%)
Rare Primary
• Carcinoid, Angiosarcoma, Carcinosarcoma, and Squamous cell carcinoma

Secondary
From :
Melanoma , Breast(Blood born)
Colon or Pancreas (Direct ext.)
Ovary (By peritoneal seeding )

ETIOLOGY
More common in
- Pernicious anemia
- Blood group A
-A family history of gastric cancer
- Environmental factors appear more related to the intestinal form

Factors Increasing or Decreasing the Risk of Gastric Cancer
Increase risk• Family history• Diet (high in nitrates, salt, fat)• Familial polyposis• Gastric adenomas• Hereditary nonpolyposis
colorectal cancer• Helicobacter pylori infection • Atrophic gastritis, intestinal
metaplasia, dysplasia• Previous gastrectomy or
gastrojejunostomy (>10 y ago)• Tobacco use• Ménétrier's disease
Decrease risk• Aspirin • Diet (high fresh fruit and
vegetable intake)• Vitamin C

Premalignant Conditions

PATHOLOGY
Dysplasia
- Universal precursor
Mild dysplasia - endoscopic biopsy/surveillance, and Helicobacter eradication

Early Gastric Cancer
Mucosa and submucosa, regardless of lymph node status
• 10% have lymph node metastases
70% well differentiated
30% poorly differentiated
Cure rate with adequate gastric resection and lymphadenectomy - 95%

Types/SubTypes(Early Gastric Cancer)
• Type I Exophytic lesion extending into the gastric lumen• Type II Superficial variant
IIA Elevated lesions with a height no more than the thickness of the adjacent mucosaIIB Flat lesionsIIC Depressed lesions with an eroded but not deeply
ulcerated appearance• Type III Excavated lesions that may extend into the
muscularis propria without invasion of this layer by actual cancer cells

Pathologic types of early gastric cancer

Japanese classification of early gastric cancer

Advanced gastric cancer
Involves the muscularis
Macroscopically classified by Bormann into four types
Types III and IV are commonly incurable

Gross Morphology and HistologicSubtypes
Four Gross forms :
• Polypoid
• Fungating
• Ulcerative
• Scirrhous

Borrmann classification of advanced gastric cancer

• Polypoid tumors are not ulcerated
• Fungating tumors are elevated intraluminally, but also ulcerated
• Ulcerative tumors (self-descriptive)
• Scirrhous infiltrate the entire thickness of the stomach (linitis plastica) poor prognosis, involve entire stomach

Important Prognostic Indicators
• Lymph node involvement
• Depth of tumor invasion
• Tumor grade (degree of differentiation: well, moderately, poorly)

Histologic Classifications

Lauren classification
• Intestinal type (53%), • Diffuse type (33%),• Unclassified (14%).
The Intestinal type associated withchronic atrophic gastritis, severe intestinal metaplasia, and dysplasia, less aggressive than the diffuse type
The Diffuse type of gastric cancer associated withyounger patients and proximal tumors, poorly differentiated

Ming classification
• Expanding (67%)
• Infiltrative (33%)

World Health Organization HistologicTyping
• Adenocarcinoma• Papillary adenocarcinoma• Tubular adenocarcinoma• Mucinous adenocarcinoma• ---------------------------------------• Signet-ring cell carcinoma• Adenosquamous carcinoma• Squamous cell carcinoma• Small cell carcinoma• ---------------------------------------• Undifferentiated carcinoma• Others
The Japanese classification(more detailed)

Transperitoneal spread
Indicates Incurability
- Ascites
- Advanced palpated either abdominally or rectally as a tumour ‘shelf ’
- Ovaries (Krukenberg’s tumours)
- Umbilicus (Sister Joseph’s nodule)
Laparoscopy and cytology

Staging
• Japanese classification
–Based on Anatomic involvement
• AJCC American Joint committee on cancer7th edition
• 15 Lymph node the minimum recommended
– SEER study , number of LN correlates with OS
CLINICAL MANIFESTATIONS
- Weight loss
- Anorexia / early satiety
- Abdominal pain
- Nausea, vomiting, bloating
- Acute GI bleeding (5%)
- Chronic occult blood loss is common ( iron deficiency anemia and heme-positive stool)
- Dysphagia (cardia)

Paraneoplastic syndromes
Rare
Trousseau's syndrome (thrombophlebitis)
Acanthosis nigricans (hyperpigmentation of the axilla and groin)
Peripheral neuropathy

Physical examination
Focused examination :
Neck
Chest
Abdomen
Rectum and pelvis

• Cervical
• supraclavicular (on the left referred to as Virchow's node)
• axillary lymph nodes may be enlarged
FNAC

- Metastatic pleural effusion
- Aspiration pneumonitis
- An abdominal mass indicate a large primary tumor
- Liver metastases
- Carcinomatosis - Krukenberg's tumor
- Palpable umbilical nodule (Sister Joseph's nodule) malignant ascites

Rectal exam
• Heme-positive stool
• Hard nodularity extraluminally and anteriorly
Drop metastases, or rectal shelf of Blumer in the pouch of Douglas

DIAGNOSTIC EVALUATION
Peptic ulcer / Gastric cancer clinical grounds impossible
• age 45 years Endoscopy and biopsy
• new onset dyspepsia
• alarm symptoms Double-contrast barium
• family history

Preoperative staging
• Abdominal/Pelvic CT scanning ( contrast)
• MRI
• Locally EUS - enlarged (>5 mm) perigastric and celiac lymph nodes
• EUS- early gastric cancer (T1) from more advanced tumors
• Positron Emission Tomography Scanning(+CT)
• Staging Laparoscopy and Peritoneal Cytology

TREATMENT
• Surgical resection Curative treatment
Exceptions:
• cannot tolerate operation
• overwhelming metastatic disease
Goal
• R0 resection / adequate lymphadenectomy
(only 50%)
• Negative margin of at least 5 cm required
(4cm is adequate NCCN)
• In diffuse variety, beyond 5 cm desirable
• Routine splenectomy is not indicated

Gastrectomy
Curative - Primary tumor resected en bloc with adjacent involved organs (distal pancreas, transverse colon, or spleen)
Palliative - indicated in incurable disease

Subtotal gastric resection
- ligation of the left and right gastric and gastroepiploic arteries at origin
- en bloc removal of the distal 75% of the stomach, 2 cm of duodenum- the greater and lesser omentum, associated lymphatic tissue
• Reconstruction - Billroth II gastrojejunostomy• the spleen and pancreatic tail not removed In
absence of involvement• operative mortality - 2 to 5%

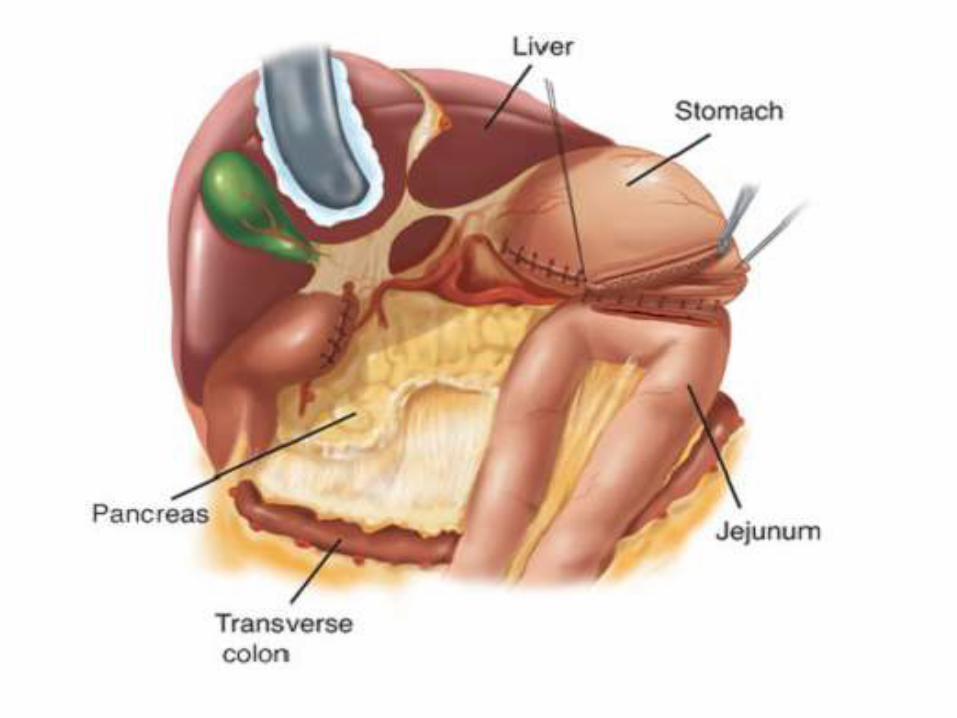

Total gastrectomy
• with Roux-en-Y esophagojejunostomy in
proximal gastric adenocarcinoma
• Total gastrectomy - superior functional, not oncologic, results for proximal gastric cancer


EMR, ESD
• Tis or T1a
• First in Japan
• En-block resection for ESD
• Endoscopic Robotic ?
– https://www.youtube.com/watch?v=0hQKl7HYOIo
– https://www.youtube.com/watch?v=L9d4PncxRlE
Extent of Lymphadenectomy
• The Japanese Research Society for Gastric Cancer numbered the lymph node stations that potentially drain the stomach
Generally these are grouped into• level D1 • level D2 • level D3 • N1- Perigastric LN lesser curvature (1,3,5) greater
curvature (2,4,6)• N2- Left gastric artery 7, common hepatic artery 8, celiac
artery 9, splenic artery 10,11• N3 Paraaortic

The standard operation for gastric cancer is
D2 Is standard of care in Asia,
D1 is recommended in West