gender equity & women’s health presenter tool – revised summer 2013
TRANSCRIPT

GENDER EQUITY & WOMEN’S HEALTH
P R E S E N T E R T O O L – R E V I S E D S U M M E R 2 0 1 3

GENDER EQUITY & WOMEN’S HEALTH (PREZI)
• Objectives• Ted Talk• Definitions• Global Context • Local Context• Role of Primary Care• Discussion / Activities

OBJECTIVES
• To describe and appreciate the effects of gender on health, at both the local and global level
• To be able to identify 2 major causes of maternal mortality
• To provide 3 examples of the role of the primary care team in improving women’s health
TED TALK:SHERYL WUDUNN: OUR CENTURY’S
GREATEST INJUSTICE
• Sheryl WuDunn's book "Half the Sky" investigates the oppression of women globally. Her stories shock. Only when women in developing countries have equal access to education and economic opportunity will we be using all our human resources.
• As a journalist reporting on China, Sheryl WuDunn saw the everyday oppression of women around the world. She and Nick Kristof wrote "Half the Sky," chronicling women's stories of horror and, especially, hope.
http://www.ted.com/talks/lang/en/sheryl_wudunn_our_century_s_greatest_injustice.html

WHAT TO PAY ATTENTION TO…
Examples of areas where gender inequity towards women is seen?
The role of education in making a change

TED TALK VIDEO CLIP

IN THE TED TALK:
• What are some examples of areas where gender inequity is seen?
• How does education for women effect change?

DEFINITIONS (1)
“NO ONE SHOULD BE SICK OR DIE BECAUSE OF GENDER INEQUALITY”
WHO

DEFINITIONS (2)
Gender refers to:• society-determined roles,• personality traits, • attitudes, • behaviors, • values, • relative power and influence
that society ascribes to the two sexes on a differential basis
• "Gendered" norms influence the health system's practices and priorities. Many health issues are a function of gender-based social status or roles.
http://hereisthecity.com/2011/03/31/sexism-in-the-city-the-gender-blender-poll-results/
http://www.phac-aspc.gc.ca/ph-sp/determinants/determinants-eng.php

DEFINITIONS (3) (EXTRA)
• Sociocultural factors that prevent women and girls from attaining quality health services and the best possible level of health include:
• unequal power relationships between men and women;• social norms that decrease education and paid
employment opportunities;• an exclusive focus on women’s reproductive roles; • potential or actual experience of physical, sexual and
emotional violence.
http://www.who.int/topics/womens_health/en/

DEFINITIONS (4) (PREZI)
• Examples of inequalities in health status & access to health care:
• A woman cannot receive needed health care because norms in her community prevent her from traveling alone to a clinic.
• A woman contracts HIV because societal standards prevent her from insisting on condom use.
• A country's lung cancer mortality rate is higher for men because smoking is considered an attractive marker of masculinity.
• A teenage boy dies in an accident because of trying to live up to his peers’ expectations that young men should be "bold" risk-takers.
http://www.who.int/gender/genderandhealth/en/index.html

DEFINITIONS (5)
Every minute, at least one woman dies from complications related to pregnancy or
childbirth
• Maternal health
• the health of women during pregnancy, childbirth and the postpartum period.
• Maternal death
• death of a woman while pregnant or within 42 days of termination of pregnancy
• irrespective of the duration and site of the pregnancy,
• from any cause related to or aggravated by the pregnancy or its management
• not from accidental or incidental causes.
• Maternal mortality ratio (per 100 000 live births) http://www.scientificamerican.com/article.cfm?id=maternal-health
Source: WHO

HOW DO OTHER SDOH EFFECT GENDER EQUALITY AND WOMEN'S HEALTH?

GLOBAL CONTEXT (1)

GLOBAL CONTEXT (2)
http://www.dhakacourier.com.bd/?p=4169
MDG 3: Provide Gender Equality and Empower Women

GLOBAL CONTEXT (3)
Eliminate gender disparity in primary and secondary education, preferably by 2005, and in all levels of education no later than 2015
• For girls in some regions, education remains elusive
• Poverty is a major barrier to education, especially among older girls
• In every developing region except the CIS, men outnumber women in paid employment
• Women are largely relegated to more vulnerable forms of employment
• Women are over-represented in informal employment, with its lack of benefits and security
• Top-level jobs still go to men — to an overwhelming degree
• Women are slowly rising to political power, but mainly when boosted by quotas and other special measures
http://www.un.org/millenniumgoals/gender.shtml
Source:WHO

GLOBAL CONTEXT (4)
http://www.countdown2015europe.org/why-family-planning/the-unmet-need-for-family-planning/http://www.healthandwelfare.idaho.gov/Health/VitalRecordsandHealthStatistics/HealthStatistics/PregnancyRiskAssessmentTrackingSystem/tabid/915/Default.aspxhttp://health.howstuffworks.com/pregnancy-and-parenting/pregnancy/labor-delivery/childbirth2.htm
MDG 5: Improve Maternal Health

GLOBAL CONTEXT (5)
SDOH – Global – MDG 5
Reduce by three quarters the maternal mortality ratio
• Most maternal deaths could be avoided• Giving birth is especially risky where most women deliver without
skilled care• The rural-urban gap in skilled care during childbirth has narrowed
Achieve universal access to reproductive health
• More women are receiving antenatal care• Inequalities in care during pregnancy are striking• Only one in three rural women in developing regions receive
the recommended care during pregnancy• Progress has stalled in reducing the number of teenage pregnancies,
putting more young mothers at risk• Poverty and lack of education perpetuate high adolescent birth
rates• Progress in expanding the use of contraceptives by women has
slowed• Use of contraception is lowest among the poorest women and
those with no education• Inadequate funding for family planning is a major failure in fulfilling
commitments to improving women’s reproductive healthSource: WHO

GLOBAL CONTEXT (6)
• Every day, approximately 1000 women die from preventable causes related to pregnancy and childbirth.
• 99% of all maternal deaths occur in developing countries.
• Maternal mortality is higher in rural areas and among poorer and less educated communities.
• Adolescents face a higher risk of complications and death as a result of pregnancy than older women.
• Skilled care before, during and after childbirth can save the lives of women and newborn babies.
• Between 1990 and 2008, maternal mortality worldwide dropped by one third.
Source: WHO

AUDIENCE QUESTIONS
• What are the major causes of maternal mortality worldwide?
• What factors influence this?
• How can these be easily prevented?
GLOBAL CONTEXT (7) (EXTRA)
• The major complications that account for 80% of all maternal deaths are:
• severe bleeding (mostly bleeding after childbirth)• infections (usually after childbirth)• high blood pressure during pregnancy (pre-eclampsia and eclampsia)• obstructed labour• unsafe abortion.
• The remainder are caused by diseases such as malaria, anemia and HIV/AIDS during pregnancy.
• Maternal health and newborn health are closely linked. More than three million newborn babies die every year, and an additional three million babies are stillborn
Source: WHO

GLOBAL CONTEXT (8)
• The high number of maternal deaths in some areas of the world reflects:
• Inequities in access to health services, and highlights the gap between rich and poor.
• The maternal mortality ratio in developing countries is 290 per 100 000 births versus 14 per 100 000 in developed countries
• Large disparities between countries, with some countries having extremely high maternal mortality ratios of 1000 or more per 100 000 live births
• Large disparities within countries, between people with high and low income and between people living in rural and urban areas.
• The risk of maternal mortality is highest for adolescent girls (under 15 years old)
• Complications in pregnancy and childbirth are the leading cause of death among adolescent girls in most developing countries.
• Women in developing countries have on average many more pregnancies:
• Their lifetime risk of death due to pregnancy is higher
• The probability that a 15-year-old woman will eventually die from a maternal cause – is 1 in 4300 in developed countries, versus 1 in 120 in developing countries.
Source: WHO
GLOBAL CONTEXT (9)
• Most maternal deaths are avoidable - the health-care solutions to prevent or manage complications are well known.
• All women need access to antenatal care in pregnancy, skilled care during childbirth, and care and support in the weeks after childbirth.
• Severe bleeding after birth can kill a healthy woman within two hours • Injecting oxytocin immediately after childbirth effectively reduces the risk of bleeding.
• Infection after childbirth can be eliminated if good hygiene is practiced • if early signs of infection are recognized and treated in a timely manner.
• Pre-eclampsia should be detected and appropriately managed before the onset of convulsions (eclampsia) and other life-threatening complications. • Administering drugs such as magnesium sulfate can lower a woman’s risk of developing
eclampsia.
• Obstructed labour • A simple tool for identifying these problems early in labour is the partograph
Source: WHO

GLOBAL CONTEXT (10)
• To avoid maternal deaths, it is also vital to prevent unwanted and too-early pregnancies. • All women, including adolescents, need access to family planning, safe abortion services to the
full extent of the law, and quality post-abortion care
• Only 66% of women in developing countries benefit from skilled care during childbirth
• In high-income countries, virtually all women have at least four antenatal care visits, are attended by a skilled health worker during childbirth and receive postpartum care.
VS• In low- and middle-income countries, less than half of all pregnant women have a
minimum of four antenatal care visits.
• Other factors that prevent women from receiving or seeking care during pregnancy and childbirth are:
• poverty• distance• lack of information• inadequate services• cultural practices.
• To improve maternal health, barriers that limit access to quality maternal health services must be identified and addressed at all levels of the health system.
Source: WHO

LOCAL CONTEXT (1) (PREZI)
http://www.christinelu.ca/2012/03/
The Heart Truth campaign
The face of heart disease is changing. Once considered “a man’s disease,” the number of deaths from heart disease and stroke are now virtually the same for men and women in Canada. The Heart Truth campaign aims to raise awareness among women of ways to reduce their risk of heart disease and stroke, and give them the tools they need to protect themselves.
The Heart Truth is a national public health education campaign to raise awareness that heart disease and stroke is the #1 killer of women in Canada.
The Heart Truth Fashion Show 2012
LOCAL CONTEXT (2)
• Nearly 3 million women live in rural, remote and northern areas
• 18% of RNs• 17% of GPs• 4% of specialists
• Poverty, limited health care and support services, geographic isolation, lack of confidentiality and anonymity, stress from multiple roles …
http://www.thecanadianencyclopedia.com/articles/health-of-native-people
http://www.womenshealthmatters.ca/health-resources/health-information/resources/feature-article/rural,-remote-and-northern-women-where-you-live-matters-to-your-health-%28womens-health-matters-article%29
LOCAL CONTEXT (3)
http://www.hc-sc.gc.ca/hl-vs/jfy-spv/women-femmes-eng.php

LOCAL CONTEXT (4)
http://www.womenshealthmatters.ca/art-not-violence/gallery.html
Send the images, spread the words: Art Not Violence postcards are on sale at Women’s College Hospital. All proceeds support the Art Not Violence Project.

LOCAL CONTEXT (5)
• Building Women's for Women
• VIDEO TO GO HERE (view 2:50 – 4:40)
http://www.youtube.com/watch?v=YJRuisx1hFk

RELATION TO PRIMARY CARE (1)
• WHY SHOULD FAMILY DOCTORS CARE?

WHY SHOULD FAMILY DOCTORS CARE?
• As family doctors we are in the business of preventative care and trying to create good health outcomes for patients
• It is therefore crucial for us to have a good understanding of the determinants of health
• Without understanding the factors influencing our patients’ health, it is difficult to have an impact upon their health
• Gender Equality & Maternal Health will greatly affect patients’ health and is therefore important for family doctors to address
WHY SHOULD FAMILY DOCTORS CARE? (EXTRA)
As a family physician in a health care system…
• You provide care to women & men & their families – of all ages, of various cultural backgrounds, etc.
• You provide appropriate preventative care
• You demonstrate sensitivity to cultural, gender and socioeconomic differences
• You explore the patient’s cultural and social context, including lived experiences and environmental factors to understand how these may influence:
• the presentation of their symptoms• their chronic condition• their illness experience.
• You integrate cultural sensitivity and awareness of the social context of the patient in a treatment plan
• You Identify the determinants of health within their communities, including barriers to accessing care and resource
• You Identify vulnerable or marginalized populations and respond as needed
In order to practice these and promote the health of individual patients, communities and populations, you must gain an appreciation and understand gender equity & women’s health in the setting of the social determinants of health


RELATION TO PRIMARY CARE (2) (PREZI)
Women & Smoking...
• Marketing aimed at women has led to rising tobacco use.
• Adolescent girls are increasingly using tobacco and alcohol• Evidence that tobacco advertising is increasingly targeting young girls and women.
• COPD rates are very high in women secondary to smoke from open fires/stoves (50% of 1.3 million annual COPD deaths) as they are traditionally in charge of cooking.
• Tobacco use and the burning of solid fuels for indoor heating and cooking are the primary risk factors for chronic obstructive pulmonary disease (COPD)
• Women prepare most of the family food, hence, the burden of COPD caused by exposure to indoor smoke is over 50% higher among women than among men.
Source: WHO

RELATION TO PRIMARY CARE (3)
Violence against Women...
• Some studies show that up to 1 in 5 women reports being sexually abused before the age of 15.
• Up to 71% of all women have suffered physical or sexual violence by an intimate male partner.
• Violence against women is widespread around the world.
• Women who have been physically or sexually abused have higher rates of:• mental ill-health, unintended pregnancies, abortions and miscarriages than
non-abused women.
• Increasingly in many conflicts sexual violence is also used as a tactic of war.
Source: WHO

RELATION TO PRIMARY CARE (4)
Early Marriage and Pregnancy...
• An estimated 100 million girls will marry before their 18th birthday over the next 10 years.
• About 14 million adolescent girls become mothers every year (>90% in developing countries).
• Young married girls often lack knowledge about sex and the risks of sexually transmitted infections and HIV/AIDS.
Source: WHO

RELATION TO PRIMARY CARE (5)
Maternal Deaths...
• Every day, 1600 women and more than 10 000 newborns die from preventable complications during pregnancy and childbirth.
Source: WHO

RELATION TO PRIMARY CARE (6) (EXTRA)
• Worldwide, in 2007, 55% of adults aged 60 years and over were women, a proportion that rises to 58% at age 70 and above.
• On average, women live 6-8 years longer than men globally
• Men are more likely to die prematurely than women largely as a result of heart disease, fatal unintentional injuries, cancer and suicide.
• In 2007, women's life expectancy at birth was more than 80 years in 35 countries, but only 54 years in the WHO African Region Source: WHO

RELATION TO PRIMARY CARE (7)
• Globally, cardiovascular disease, often thought to be a "male" problem, is the leading killer of women.
• Women often show different symptoms from men = under diagnosis
• Women tend to develop heart disease later in life than men.
• Tobacco is implicated in nearly 10% of cardiovascular disease in women.
• Chronic conditions – mainly cardiovascular disease and COPD – account for 45% of deaths in women over 60 years of age worldwide. Source: WHO

RELATION TO PRIMARY CARE (8)
• 15% of deaths are caused by cancers, mainly of the breast, lung and colon.
• While overall cancer death rates for men have declined, they have remained persistently stubborn among women:• Mainly due to increases in lung cancer mortality• Teenage girls more likely than boys to smoke
• Breast cancer is the leading cancer killer among women aged 20–59 years in high-income countries
• The incidence of breast cancer is much higher in high-income countries compared to low- and middle-income countries, but mortality is similar.
• This is due to the availability of better treatment in the high-income countries.
• For lung and colon cancer, both incidence and mortality are currently higher in high-income countries.
• Globally, 71% of lung cancer deaths are caused by tobacco use. Source: WHO

RELATION TO PRIMARY CARE (9)
• Cervical cancer is the second most common type of cancer among women
• Almost 80% of cases today and an even higher proportion of deaths from cervical cancer occur in low-income countries, where access to cervical cancer screening and treatment virtually does not exist.
Source: WHO

RELATION TO PRIMARY CARE (10)
• Injuries from road traffic accidents figure among the top 10 causes of death among adult women (20-59 years) globally.
• Women suffer significantly more fire-related injuries and deaths than men.
• Many related to cooking accidents and many a result of intimate partner and family violence.
Source: WHO

RELATION TO PRIMARY CARE (11)
• While women live longer than men, they are more likely to suffer:
• depression, • stress overload (often due to efforts to balance work and family life), • chronic conditions such as arthritis and allergies,• injuries and death resulting from family violence.
• An estimated 73 million adult women worldwide suffer a major depressive episode each year.
• Mental disorders following childbirth, including depression, are estimated to affect about 13% of women within a year of delivery.
• Suicide is the seventh top cause of death globally for women aged 20-59 years.
Source: WHO

RELATION TO PRIMARY CARE (12)
• Many of the health problems faced by women in older age are the result of risk factors that arise in their adolescence and adulthood, such as smoking, sedentary lifestyles and unhealthy diets.
• Other debilitating health problems faced by older women are poor vision (including cataracts), hearing loss, arthritis, depression and dementia.
Source: WHO

CASE DISCUSSION (1) (PREZI)
A case of maternal mortality in Haiti
• Mrs. X is a 29 y.o. G4P1A2 at home, in active labor. • She delivers a healthy baby boy at 38 weeks G.A.,
but unfortunately passes away minutes after the delivery due to postpartum hemorrhage.

CASE DISCUSSION (2)
What further details would you inquire about in order to assess how this could have been avoided?
• Regarding prenatal care?• Regarding labor and delivery care?• Regarding postpartum care?
• She has received no prenatal care, as the clinic where she lives has been closed for over 5 years.
• A traditional birth attendant with no formal training attended her birth, but was not equipped with the knowledge, skills or materials necessary to manage obstetrical emergencies
• No emergency transport was available. • The nearest medical care was 1 hour away, and nobody was available for
transport at night (no drivers were available, local international business declined providing emergency transport)
• Family members live in the village, and will care for the orphan child as the father is not involved.

GROUP ACTIVITY (1)
• Divide into groups• One group per category: World, Low, Middle, High• Provide a paper copy of the following slide and post the social
determinants of health slide on the big screen
• Together, strategize how as a group of family physicians working in collaboration with other potential partners (local, national and/or international) can effect change on the leading causes of mortality in women in your respective group (make sure to incorporate social determinants of health in your answers).
• World: HIV / Aids• Low Income Countries: Maternal Conditions• Middle Income Countries: COPD• High Income Countries: Ischemic Heart Disease
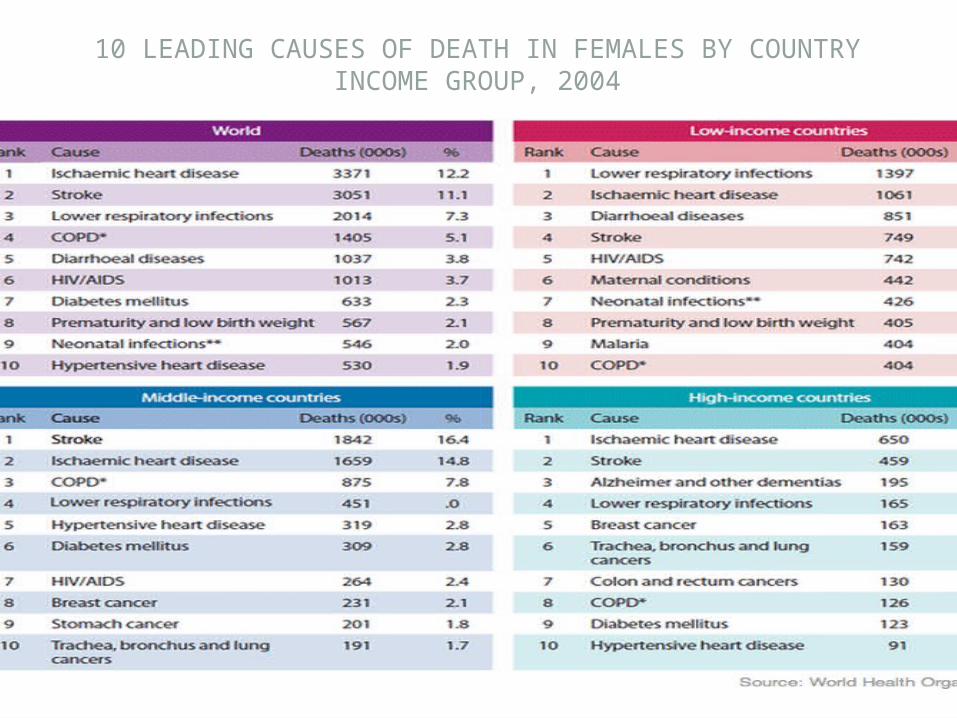
10 LEADING CAUSES OF DEATH IN FEMALES BY COUNTRY INCOME GROUP, 2004


ACTION PLAN
• Group Discussion – after today’s workshop, make a list of tangible action plans to implement in your respective practices.
• Examples: • Application of Women’s Health Specific Preventative Care
Checklist Items