gene therapies for diseases other than cancers · 1 a gene therapy product has yet to be approved...
TRANSCRIPT

White Paper on Gene Therapies
Gene Therapies for Diseases Other Than Cancers Vying for Commercial Success

1
A gene therapy product has yet to be approved by the US FDA and despite an approval in the EU, Glybera has not yet launched.
Apart from clinical development and regulatory approval, several challenges need to be overcome for gene therapies to become commercially viable.
Over 2,000 gene therapy clinical studies have been
conducted across diverse therapeutic areas, with
80% of these studies conducted in various cancers.
Despite heroic efforts by basic researchers and clinical
investigators alike, no gene therapies have become
commercially available in the US or EU. The lack of
success of gene therapies to date highlights multiple
limitations still to be overcome, e.g. patient selection
TABLE 1: APPROVED GENE THERAPY PRODUCTS
Gene therapies for diseases other than cancers are
progressing through late stages of development,
indicating that some of these therapies are likely to
become available in the near future. Herein we have
discussed the characteristics of the diseases that
Gene Therapy
Gene/MoA Vector Disease/Indication Country of Approval
Year of Approval
Glybera Lipoprotein lipase (LPL)
Adeno Associated Virus
Familial LPLD (LPL deficiency) EU/EMA 2012
Oncorine Adenovirus V5 with E1B and E3B deleted
Adenovirus Head and neck squamous cell carcinoma, lung cancer, liver cancer, malignant pleural and peritoneal effusion, pancreatic cancer
China 2005
Rexin-G Cyclin G1 (cytocidal mutant)
Moloney murine leukemia virus Retrovirus
Solid tumors refractory to standard chemotherapy
Philippines 2007
Gendicine Wt p53 Adenovirus Head and neck squamous cell carcinoma
China 2003
for clinical trials, safer and more effective vectors, and
cost. The first gene therapy product approved in the
EU, Glybera, was for a rare genetic disease caused by a
mutation of the pancreatic enzyme lipoprotein lipase
that renders patients unable to break down fatty acids
effectively. The three other gene therapy products
now approved (Table 1) are for the treatment of
different cancers.
make them suitable for gene therapies, characteristics
of vectors for such modalities, changing industry
perceptions, and the possible future outlook for
these therapies.
Although 80% of global gene therapy clinical studies have been conducted for different cancers, the first and only approved gene therapy in the Western world – Glybera (alipogene tiparvovec) – was approved in the EU for a non-cancer monogenic condition (lipoprotein lipase (LPL) deficiency). Glybera, after several rounds of assessments by the Committee on Advanced Therapies (CAT) was authorized in 2012 under “exceptional circumstances.” Due to the small size of clinical trials supporting Glybera’s authorization, the EMA has required its maker to submit additional clinical data annually for 6 years and to establish a registry for long-term patient tracking. Despite approval, Glybera has yet to be marketed in EU countries due to pending pricing negotiations and other regulatory requirements - even though it made headlines in 2014 for a target €1.1M price tag in Germany.
Copyright©2015 SMARTANALYST®

2
Disease-specific characteristics make certain
monogenic disorders tractable for gene-replacement
strategies
The original goal of gene therapies was to treat
monogenic diseases by replacing a non-functional
or defective gene with a healthy copy. Monogenic
hematological disorders such as hemophilias are
particularly amenable to gene therapy because even a
limited increase in expression of the defective gene is
sufficient to offer a phenotypic cure. This notion has
been strengthened with results from recent trials for
hemophilia B. A single intravenous infusion of an adeno-
associated virus serotype 8 (AAV-8) vector expressing
Factor IX in 10 patients with severe hemophilia B
resulted in a dose-dependent increase in its circulating
levels to 1-6% of the normal value over a median period
of 3.2 years. In patients who received the high dose
(2×1012 vector genomes per kilogram of body weight),
there was a consistent increase in Factor IX level to over
5%. Despite such low levels of circulating factor, there
was over a 90% reduction in bleeding episodes and the
use of prophylactic Factor IX concentrate. Hemophilias
also tend to be suitable for gene therapy since minimal
logistic issues need to be addressed with respect to
intravenous administration of viral vectors encoding
clotting factors. Production of such vectors is now
routine, and there are very few manipulations of the
product prior to administration.
Other monogenic disorders such as childhood cerebral
adrenoleukodystrophy (CCALD), while certainly tractable
vis-à-vis gene replacement, present additional logistic
issues. This disease is caused by deficiency in ALD
protein – an adenosine triphosphate-binding cassette
transporter encoded by the ABCD1 gene – which can
be corrected by transducing autologous CD34+ cells ex
vivo with a lentiviral vector encoding wild-type gene and
then re-infusing transduced cells into the patients after
they have received myeloablative treatment. These
additional steps are likely to make it expensive and
restricted to the most advanced medical centers.
Polygenic disorders can be amenable to gene therapy
strategies if specific targets are identified
As many disorders such as diabetes, coronary artery
disease, and rheumatoid arthritis are polygenic,
replacement of a single gene is unlikely to cure the
disease. However, if a specific therapeutic target
(common disease pathway) can be identified, then
delivery of a gene product that expresses sufficient
levels of the protein, in theory, can sufficiently
ameliorate symptoms of a polygenic disease and be
a useful therapy. A case in point is Generx® a Phase
III adenoviral FGF-4 gene therapy for patients with
myocardial ischemia due to coronary artery disease,
developed by Cardium Therapeutics. FGF-4 has been
shown to stimulate the growth of microvascular
circulation in the heart, enhancing cardiac perfusion.
Generx®, is designed to be administered only once, by
an interventional cardiologist. The company recently
reported that the benefits from this gene therapy are
similar in magnitude to the large vessel revascularization
procedures such as bypass surgery or angioplasty.
Tissue tropism and viral integration are important
considerations determining the choice of vector
While there has been significant progress in vector
development in the past two decades, it is also clear
that no vectors can be universally utilized for all gene
therapy applications. There are a few important
considerations in this regard. First, the tropism of
vectors used will determine whether the gene product
will be expressed in the tissue of interest. For instance,
in the case of AAV vectors, as compared to other
serotypes, AAV1 is suitable for expression in skeletal
muscle and retina, AAV5 transduces neuronal and lung
cells efficiently and AAV8 demonstrates high levels
of expression in liver cells. A second consideration is
whether the viral vector employed stably integrates into
the host genome or remains episomally in the nucleus.
Lentivirus vectors have the ability to stably integrate
into target cells, thus providing genetic modification
of the cell and all of its progeny. However, insertional
mutagenesis is a potential issue for vectors that
integrate foreign DNA into the genome. On the other
hand, in case of vectors based on the Herpes Simplex
Virus (HSV), the latent HSV genome is maintained as an
episome, and the potential risks of viral integration into
host cell chromatin are avoided.
Copyright©2015 SMARTANALYST®
3
Immune responses need not be a barrier to their effective use in gene transfer While AAV and adenovirus-based vectors are popular gene therapy vectors, the human immune response to them might be considered problematic. AAV vectors often induce immune responses against the capsid or the transgene, especially when used in large doses required for clinical benefit, leading to a decrease in transgene expression. In addition to AAV, the efficacy of in vivo gene delivery with adenoviral vectors might be expected to be severely compromised owing to both innate and acquired immune responses as most immunocompetent people have been exposed to adenovirus. With up to 80% of the human population seropositive for AAV-2 (and vectors based on it), concerns over their immunogenicity are justified.
However, it is now recognized that although gene therapy vectors such as adenoviruses and AAV are highly immunogenic, this need not preclude successful gene expression, even long-term expression. The immune-privileged status of the eye makes AAV-mediated ocular gene transfer with low doses relatively efficient with low risk of immune-related events. This was seen in the trials that used AAV to deliver the RPE65 gene to retinal cells in patients of Leber Congenital Amaurosis (LCA), an inherited disorder that results in severe vision loss. As there are many gene therapies that do not target the eye, diverse strategies have been developed to overcome immunogenicity concerns when targeting other tissues. One broadly applicable strategy has been to transduce cells ex vivo and then transfer them into the body. Proof of principle for such a strategy has been obtained in preclinical models where myoblasts transduced with “gutless” adenoviral vectors expressing full-length dystrophin cDNA have been shown to fuse with mature myofibers ex vivo to successfully deliver the gene. Another strategy has been to use virus serotypes such as AAV-5 and AAV-8 which have low
sero-prevalence. Several other approaches to generate immunologically inert AAV vectors have been employed – including targeted mutagenesis, capsid shuffling, or directed evolution approaches – to alter the epitopes on the AAV capsid surface. Chemical modifications of immunogenic sites by strategies such as PEGylation or co-administration of immunosuppressive agents or plasmapharesis to reduce neutralizing antibodies have also been tried. All these approaches, while useful in obtaining a vector with immune-escape potential, are nevertheless fraught with potential problems. These include loss of infectivity, packaging ability, or tissue tropism. While not insurmountable, the obvious disadvantage of all these strategies is additional cost, as cell culture and lab-based engineering necessitates several additional manufacturing and quality control issues.
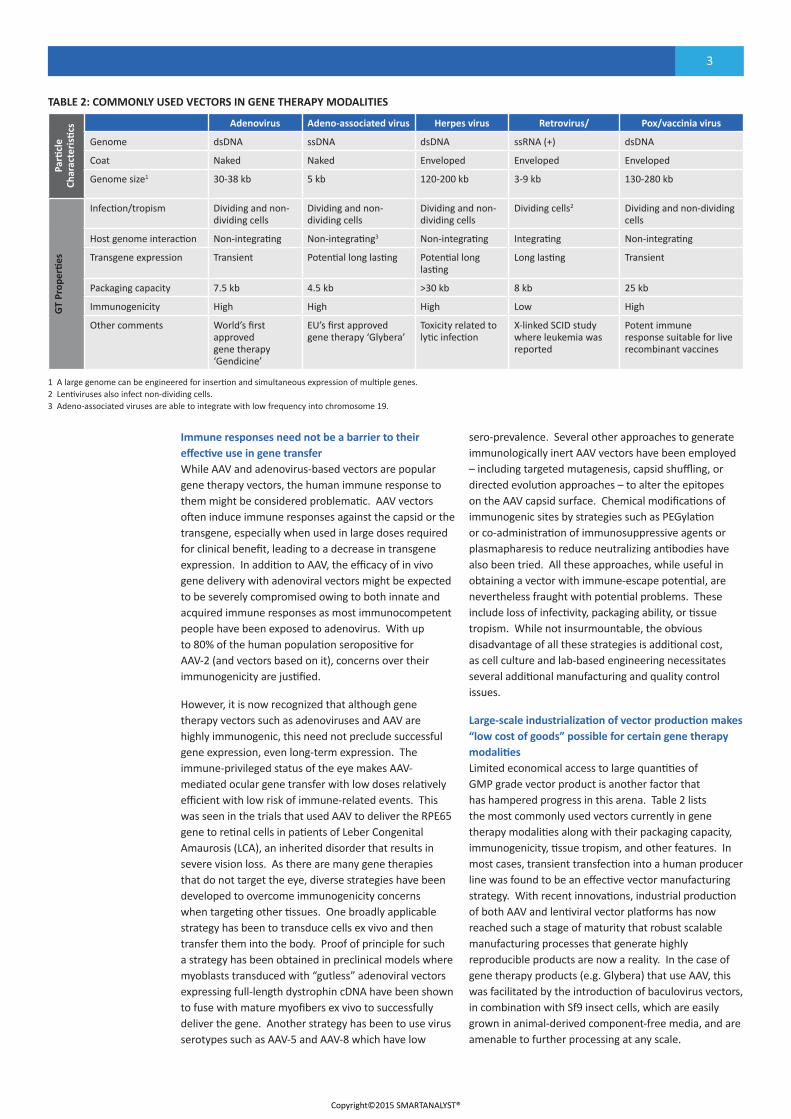
Large-scale industrialization of vector production makes “low cost of goods” possible for certain gene therapy modalitiesLimited economical access to large quantities of GMP grade vector product is another factor that has hampered progress in this arena. Table 2 lists the most commonly used vectors currently in gene therapy modalities along with their packaging capacity, immunogenicity, tissue tropism, and other features. In most cases, transient transfection into a human producer line was found to be an effective vector manufacturing strategy. With recent innovations, industrial production of both AAV and lentiviral vector platforms has now reached such a stage of maturity that robust scalable manufacturing processes that generate highly reproducible products are now a reality. In the case of gene therapy products (e.g. Glybera) that use AAV, this was facilitated by the introduction of baculovirus vectors, in combination with Sf9 insect cells, which are easily grown in animal-derived component-free media, and are amenable to further processing at any scale.
Parti
cle
Char
acte
risti
cs Adenovirus Adeno-associated virus Herpes virus Retrovirus/ Pox/vaccinia virus
Genome dsDNA ssDNA dsDNA ssRNA (+) dsDNA
Coat Naked Naked Enveloped Enveloped Enveloped
Genome size1 30-38 kb 5 kb 120-200 kb 3-9 kb 130-280 kb
GT
Prop
erti
es
Infection/tropism Dividing and non-dividing cells
Dividing and non-dividing cells
Dividing and non-dividing cells
Dividing cells2 Dividing and non-dividing cells
Host genome interaction Non-integrating Non-integrating3 Non-integrating Integrating Non-integrating
Transgene expression Transient Potential long lasting Potential long lasting
Long lasting Transient
Packaging capacity 7.5 kb 4.5 kb >30 kb 8 kb 25 kb
Immunogenicity High High High Low High
Other comments World’s first approved gene therapy ‘Gendicine’
EU’s first approved gene therapy ‘Glybera’
Toxicity related to lytic infection
X-linked SCID study where leukemia was reported
Potent immune response suitable for live recombinant vaccines
TABLE 2: COMMONLY USED VECTORS IN GENE THERAPY MODALITIES
1 A large genome can be engineered for insertion and simultaneous expression of multiple genes. 2 Lentiviruses also infect non-dividing cells. 3 Adeno-associated viruses are able to integrate with low frequency into chromosome 19.
Copyright©2015 SMARTANALYST®

4
Company Gene Therapy/ Disease Status
1 Uniqure hF-IX gene/ Hemophilia B Collaborator: Chiesi Farmaceutici (licensed from St. Jude Children’s Research Hospital ), Phase I/II
NaGlu gene/ San Fillipo B Syndrome Collaborator: Institute Pasteur, Phase I/II
2 Oxford Biomedica StarGen™ (Sanofi) / Stargardt Disease Phase I/IIa trial ongoing
UshStat® (Sanofi) / Usher Syndrome Type 1B Phase I/IIa
EncorStat® / Corneal Graft Rejection Phase I/II trial preparation
OXB-102 / ProSavin® / Parkinson’s Disease Phase I/II trial completed
Retinostat®/ Wet AMD Phase 1 trial ongoing
3 Bluebird Bio Lenti-D/ Childhood Cerebral ALD Phase II/III global study initiated
LentiGlobin/ Beta Thalassemia, SCD Beta thalassemia: Phase I/ II study initiated SCD: Phase I in US
4 Sangamo SB-728/ HIV/AIDS Phase II
CERE-110/ Alzheimer’s Disease Phase II
5 AGTC AATD / Alpha-1 Antitrypsin Deficiency Phase IIb
RS1 gene/ X-linked Juvenile Retinoschisis (XLRS) IND filed; Phase I/II expected to start 2Q2015
6 Spark Therapeutics
SPK-RPE65/ Inherited Retinal Dystrophies due to RPE65 Gene Mutations Phase III
SPK-CHM / Choroideremia Phase I/II
SPK-FIX / Hemophilia B Collaborator: PfizerPhase I/II expected 1H2015
7 AnGes MG Collategene™ Licensed from Vical (Also Known as Beperminogene Perplasmid, AMG0001)/ Critical Limb Ischemia
Phase III
AMG0001/Primary Lymphedema Phase I/II (Japan)
AMG0001/ Ischemic Heart Disease Phase I completed (US)
8 Taxus Cardium Generx® (Alferminogene Tadenovec) [Ad5FGF-4]/Cardiac Microvascular Insufficiency (CMI) in patients with Myocardial Ischemia and Symptomatic Chronic Stable Angina Pectoris
Phase III
9 Genethon WAS ( Wiskott–Aldrich Syndrome) Phase I/II
X-Linked CGD Patients Phase I/II
10 GSK GSK2696273/ ADA Gene Transfer into Hematopoietic Stem/Progenitor Cells for the Treatment of ADA-SCID
Phase II
11 Viromed Critical Limb Ischemia Phase II completed
Chronic Granulomatous Disease Phase I/II (Korea)
Painful Diabetic Neuropathy Phase II
Chronic Stable Angina Phase I/ II
12 Voyager Therapeutics
VY-AADC01/ Parkinson’s Disease Collaborators: UCSF and Genzyme Phase I
13 Avalanche Biotechnologies
AVA101/ Wet AMD Phase IIa
14 Celladon MYDICAR® (SERCA 2A) / Systolic HF Phase II/III
MYDICAR® ( (SERCA 2A) /Advanced HF with LVAD Phase I/II
TABLE 3: KEY PLAYERS WITH GENE THERAPIES IN CLINICAL DEVELOPMENT
Changing industry perception on risks and benefits of gene therapies The pharmaceutical industry is generally risk averse and understandably so. In 1999, the fatal systemic inflammatory response syndrome generated in an 18-year-old patient with partial ornithine transcarbamylase deficiency – following transfer of a vector based on human adenovirus type 5 – and the tough regulatory climate that ensued, were cause for concern. For many years, this led to a decline in interest in furthering such therapies, especially for non-lethal diseases where such risks were unacceptable. Despite these setbacks, consistent data from various trials showing sustained clinical benefits has now led to a re-evaluation by industry experts, and an improved investor climate. Major pharmaceutical companies
have demonstrated renewed interest and have struck numerous deals with academic groups and smaller biotech companies.
In December 2014, Pfizer inked a deal with a privately owned US biotech firm Spark Therapeutics to develop a gene therapy for hemophilia B. Among other major pharmaceutical companies, Bayer AG has struck a gene therapy deal with Dimension Therapeutics, while Novartis AG recently established a new cell and gene therapies unit, and Sanofi has a long-standing tie-up with Oxford BioMedica. Genzyme recently announced a major strategic collaboration with Voyager Therapeutics for gene therapies for CNS disorders. Perceptions are also changing about accepting the risks associated with gene delivery for the potential benefits, as evident from the large number of clinical studies in these indications.
Copyright©2015 SMARTANALYST®

5
Future Outlook Although the first gene therapy clinical trial began in 1990, progress has been slow. Recent developments, including the approval of Glybera and the increasing level of clinical trial activity, have indicated an upswing and a renewed interest in the role of gene therapy in diseases with high unmet need. For instance, in many hematological or metabolic monogenic disorders, where allogeneic hematopoeitic stem cell transplantation (HSCT) from donors has been successfully used to treat disease, gene therapy may correct the genetic defect and permit autologous HSCT. This approach will overcome the challenges associated with arranging a compatible donor and the consequences of an unmatched or unrelated transplantation as in case of graft-versus-host disease.
There is also an increased focus on the issues that would be relevant to maximizing commercial potential, including reimbursement, regulatory hurdles, manufacturing costs, and postmarketing surveillance. The approval of Glybera, while certainly encouraging, is a small step in an evolving field with enormous potential. Glybera’s approval in the EU was accompanied by requirements for a post-approval study, implementation of a disease registry, and a risk-management procedure. All of this can be costly and time-consuming, thereby hindering initial uptake.
Commercial success will depend on the ability of companies to develop gene therapy products with convincing clinical data to support the value proposition of potential long-term benefit or cure without any serious safety concern. They will also face reimbursement challenges as gene therapies may be a one-time or a short-term treatment, and the actual cost may be incurred upfront, unlike conventional therapies where the cost of treatment is incurred over a long period of time. This may be especially problematic in the US where commercial payers may balk at incurring the upfront cost with no certainty of the individual staying with the insurer to realize the long-term benefit. Further, specialist training, patient awareness, and dedicated infrastructure in the form of centers of excellence (to identify / diagnose patients early, to offer them gene therapy, and to manage them post treatment) may be required.
Overall, despite various challenges, gene therapies have the potential to change the future treatment paradigm or even become the standard-of-care (SoC) therapies for certain diseases. While the gene therapy market will largely depend on the regulatory environment, in view of the emerging encouraging data, there is a high likelihood that gene therapy will become a clinical reality in the near future.
Ophthalmic Diseases1. Lebers Congenital Amaurosis2. Stargardt Disease3. Age Related Macular Degenera�on4. Choroideremia5. Leber's Hereditary Op�c Atrophy
Neurological Disorders1. Parkinson’s Disease2. Spinal Muscle Atrophy3. Alzheimer’s disease4. Diabe�c Neuropathy
Cardiovascular Disorders1. Heart Failure2. Angina/Ischemic Heart Disease3. Cri�cal Limb Ischemia/ Intermi�ent Claudica�on
Musculoskeletal Disorders1. Limb Girdle Muscle Dystrophy 2C/2D2. Becker Muscle Dystrophy3. Duchenne Muscular Dystrophy
Other Diseases1. HIV2. Epidermolysis Bullosa3. Acute Intermi�ent Porphyria
Respiratory Diseases1. Cys�c Fibrosis2. Alpha-1 An�trypsin Deficiency
Metabolic Disorders1. Adrenoleukodystrophy2. Pompe3. Ba�en4. Metachtoma�c Leukodystrophy5. San Filippo A6. Hunter Syndrome
Blood Disorders1. Hemophilia2. ADA-SCID3. X Linked- SCID4. Chronic Granulomatous Disease 5. Wischo� Aldrich Syndrome6. Sickle Cell Anemia7. Beta Thalassemia8. Fanconi Anemia
FIGURE 1: CLINICAL APPLICATIONS OF GENE THERAPY
Copyright©2015 SMARTANALYST®

6
About SmartAnalyst
SmartAnalyst helps bio-pharma companies drive pipeline and portfolio value by providing strategic
consulting and analytical support for key decisions at the Disease, Asset, and Portfolio levels. Contact us
to discuss how we can assist you in your biologic portfolio decisions.
Copyright©2015 SMARTANALYST®