gestational diabetes: new concepts, new guidelines · gestational diabetes: new concepts, new...
TRANSCRIPT

Thank you for attending
Gestational Diabetes: New Concepts, New Guidelines A Live and Archived Webcast Sponsored by Community Health Association of Mountain/Plains States (CHAMPS) Presented by Dr. Linda Barbour on Wednesday, February 28, 2007 Supplementary Information Packet Contents:
o Learning Objectives o AAFP o Biography of Dr. Linda Barbour o Description of CHAMPS o Presentation Slides o GDM Guidelines – Long o GDM Guidelines – Short

Gestational Diabetes: New Concepts, New Guidelines Linda Barbour, MD, MSPH, February 28, 2007
Learning Objectives • Understand the existing controversies in the diagnosis and management of gestational
diabetes • Interpret the findings from the most recent landmark trials which shaped the
recommendations from the 5th International Workshop on Gestational Diabetes • Describe how to use a fetal-based strategy for the optimal treatment of GDM • Recognize the long term implications of GDM for both infant and mother and the
appropriate postpartum recommendations
AAFP This live webcast has been reviewed and is acceptable for up to 1.5 Prescribed credits by the American Academy of Family Physicians (AAFP). Application for 1.5 hours of Prescribed CME credit for the archived version of this webcast will be filed immediately after the live event. Linda Barbour has indicated that she has no relationships to disclose relating to the subject matter of his presentation. The AAFP invites comments on any activity that has been approved for AAFP CME credit. Please forward your comments on the quality of this activity to [email protected].
Biography of Linda Barbour, MD, MSPH Linda A. Barbour, MD, MSPH, is an Associate Professor of Medicine and Obstetrics and Gynecology in the divisions of Endocrinology, Metabolism, and Diabetes and Maternal-Fetal Medicine at the University of Colorado at Denver Health Sciences Center. She is Board Certified in Endocrinology and completed a second fellowship in Preventive Medicine and Biometrics. She is the Co-Director of the High Risk Obstetrics Clinic and Diabetes in Pregnancy Clinic. She chaired the Colorado Clinical Guidelines Collaborative on Gestational Diabetes and also co-authored the Endocrine Society Guidelines for Thyroid Disease in Pregnancy, soon to be published. Dr. Barbour is the past president of the North American Society of Obstetric Medicine, previous moderator and speaker for the Pregnancy and Reproductive Health Council for the American Diabetes Association, and the Director of Continuing Medical Education for the Department of Medicine. She is co-editor of the textbook, Medical Care of the Pregnant Patient, published in 2000, for which the 2nd edition is soon to be published. She is the principal investigator on a 5-year NIH grant which studies insulin signaling in gestational diabetes.
Description of CHAMPS CHAMPS, the Community Health Association of Mountain/Plains States, is a non-profit organization dedicated to providing a coordinating structure of service to non-profit primary health care programs whose primary purpose is to serve the medically indigent and medically underserved of Region VIII (CO, MT, ND, SD, UT, and WY). CHAMPS also serves the Region VIII State Primary Care Associations that assist those nonprofit primary health care programs (CCHN, MPCA, CHAD, AUCH, and WYPCA). Currently, CHAMPS programs and services focus on education and training, collaboration and networking, policy and funding communications, and the collection and dissemination of regional data for Region VIII Community Health Centers and Primary Care Associations. For more information, please visit www.champsonline.org or call (303) 861-5165.
Community Health Association of Mountain/Plains States

1
Gestational Diabetes: Gestational Diabetes: New Concepts, New Concepts, New GuidelinesNew GuidelinesLinda Barbour MD, MSPHLinda Barbour MD, MSPHAssociate Professor in Endocrinology Associate Professor in Endocrinology and Maternaland Maternal--Fetal Medicine, UCDHSCFetal Medicine, UCDHSCCoCo--Director Diabetes in Pregnancy ClinicDirector Diabetes in Pregnancy Clinic
Sponsored bySponsored byCommunity Health Association of Community Health Association of
Mountain/Plains States Mountain/Plains States (CHAMPS)(CHAMPS)
www.CHAMPSonline.orgwww.CHAMPSonline.org
This live webcast has been reviewed and is acceptable for up to 1.5 Prescribed credits by the American Academy of Family Physicians (AAFP). Application for 1.5 hours of Prescribed
CME credit for the archived version of this webcast is pending with AAFP. Linda Barbour has indicated that she has no relationships to disclose relating to
the subject matter of this presentation.
This presentation was supported by Grant Number 5 H68CS00150-20-00 from the Department of Health and Human Services (DHHS) Health Resources and Services
Administration (HRSA) Bureau of Primary Health Care (BPHC). Views of the presenter do not necessarily represent the official views of CHAMPS or HRSA/BPHC.
CCGC Guidelines CommitteeCCGC Guidelines CommitteeChair: Linda Barbour , MD, MSPHChair: Linda Barbour , MD, MSPHReviewers:Reviewers:–– Jill Davies MD, Mark Jill Davies MD, Mark DeutchmanDeutchman MD, Ronald Gibbs, MD, Oliver MD, Ronald Gibbs, MD, Oliver
Jones MD, Lisa Jones MD, Lisa LattsLatts, MD, Richard , MD, Richard PorrecoPorreco MD, Robert MD, Robert StettlerStettlerMD, Robert Wall MD, Marie HastingsMD, Robert Wall MD, Marie Hastings--TolsmaTolsma PhD, CNM, Nancy PhD, CNM, Nancy Nola NP, RN, Paula Stearns MSN, RN, Tanya Tanner CNM, MSNola NP, RN, Paula Stearns MSN, RN, Tanya Tanner CNM, MS
Committee:Committee:–– Deborah Davis RNC, MS, Deborah Davis RNC, MS, Julie Julie GormleyGormley MS, RDMS, RD, Teri , Teri
Hernandez RN, MS, Bonnie Hernandez RN, MS, Bonnie JortbergJortberg RD, MS, CDE, Linda RD, MS, CDE, Linda MatteiMatteiRN, MPH, CDE, Mandy McCulloch RD, Rhoda Rogers RN, BSN, RN, MPH, CDE, Mandy McCulloch RD, Rhoda Rogers RN, BSN, CDE, Pamela Spry PhD, CNM, Helen Stover RN, BSN, CDE CDE, Pamela Spry PhD, CNM, Helen Stover RN, BSN, CDE Gloria VellingaGloria Vellinga,, RD, CDE RD, CDE
CCGC Staff: CCGC Staff: MarjieMarjie HarbrechtHarbrecht MD, Cassidy Smith MPHMD, Cassidy Smith MPH
Linda Barbour, MD, MSPH
55thth International International Workshop on GDMWorkshop on GDMNovember 11November 11--15, 2005 Chicago15, 2005 Chicago
(Metzger BE, Women(Metzger BE, Women’’s Health 2006; 2(2):211s Health 2006; 2(2):211--16)16)
Linda Barbour, MD, MSPH
ObjectivesObjectivesAppreciate the rapidly rising prevalence of GDM due Appreciate the rapidly rising prevalence of GDM due to obesity epidemicto obesity epidemicUnderstand the importance of GDM on long term Understand the importance of GDM on long term maternal and childhood outcomesmaternal and childhood outcomesCite landmark studies that shaped the guidelines Cite landmark studies that shaped the guidelines and studies pending in 2007and studies pending in 2007Review the key elements of the guidelinesReview the key elements of the guidelinesUnderstand new management strategies including Understand new management strategies including fetalfetal--based approaches based approaches Underscore the importance of appropriate post Underscore the importance of appropriate post partum management for both mother and infant partum management for both mother and infant
Linda Barbour, MD, MSPH
What Is Gestational Diabetes What Is Gestational Diabetes (GDM)?(GDM)?
Glucose intolerance recognized for the first Glucose intolerance recognized for the first time during pregnancytime during pregnancy–– Does not exclude women with preDoes not exclude women with pre--existing existing
diabetes previously undiagnoseddiabetes previously undiagnosed–– Undiagnosed Type 2 with Undiagnosed Type 2 with ↑↑A1C have risk for A1C have risk for
major malformationsmajor malformations–– Most women diagnosed before 24 weeks have Most women diagnosed before 24 weeks have
IGT (preIGT (pre--diabetes) and are at very high risk for diabetes) and are at very high risk for developing Type 2 postpartum developing Type 2 postpartum
Linda Barbour, MD, MSPH
What Causes It?What Causes It?Vast majority of women who develop GDM are Vast majority of women who develop GDM are overweight and insulin resistantoverweight and insulin resistantPlacental hormones cause worsening insulin Placental hormones cause worsening insulin resistance in the late 2resistance in the late 2ndnd trimester intended to shunt trimester intended to shunt nutrients to the fetusnutrients to the fetusMoms are unable to produce enough insulin to Moms are unable to produce enough insulin to overcome the overwhelming resistance to maintain overcome the overwhelming resistance to maintain euglycemiaeuglycemiaFetuses are exposed to high levels of glucose, Fetuses are exposed to high levels of glucose, TGsTGsand and FFAsFFAs. Fetal . Fetal hyperglycemiahyperglycemia→→→→hyperinsulinemiahyperinsulinemia→→→→pancreatic hyperplasia. pancreatic hyperplasia. Insulin is a growth Insulin is a growth hormone causing excess fat deposition hormone causing excess fat deposition
Linda Barbour, MD, MSPH

2
How Big Is the Problem?How Big Is the Problem?~7.5% of mothers in Colorado have diabetic ~7.5% of mothers in Colorado have diabetic pregnancies (CO pregnancies (CO PRAMsPRAMs data) ~5000 data) ~5000 women women Incidence has Incidence has DoubledDoubled in the last 7in the last 7--8 years 8 years from 2from 2--5% of population to ~45% of population to ~4--12%12%A leading high risk complication of A leading high risk complication of pregnancy (after preterm birth and obesity) pregnancy (after preterm birth and obesity) Tremendous economic costs for mother and Tremendous economic costs for mother and infant infant Self perpetuating cycle feeding the Self perpetuating cycle feeding the obesity and diabetes epidemicobesity and diabetes epidemic
Linda Barbour, MD, MSPH
Percent of Women with Diabetes During Pregnancy, by Race/Ethnicity, 2002-2004
6.78.35.8
10.7
02468
101214161820
White/Non-Hispanic
White/Hispanic Black Other
Perc
ent (
%)
Data Source: Colorado PRAMS
Linda Barbour, MD, MSPH
Percent of Women with Diabetes During Pregnancy, by Age Group, 2002-2004
2.5 4.6
8.611.2
02468
10121416
15-19 20-24 25-34 35+ Age Group
Perc
ent (
%)
Data Source: Colorado PRAMS
Linda Barbour, MD, MSPH
Data Source: Colorado PRAMS
Percent of Women with Diabetes During Pregnancy, by Years of Education Received, 2002-2004
10.7
7.1 6.2
0
2
4
6
8
10
12
14
< 12 years 12 years >12 yearsYears of Education
Perc
ent (
%)
Linda Barbour, MD, MSPH
19961996→→20062006 GDM CostsGDM CostsKitzmillerKitzmiller DiabDiab Care 1998;21, Supp 2:B123Care 1998;21, Supp 2:B123
Diet treated GDM ~$11,000 per pt ($6,000)Diet treated GDM ~$11,000 per pt ($6,000)Insulin Treated GDM ~$20,000 ($11,000)Insulin Treated GDM ~$20,000 ($11,000)–– 1/3 patient require meds 1/3 patient require meds –– 8% require ~18% require ~1--2 days in NICU ~$4000 ($2300) 2 days in NICU ~$4000 ($2300)
70,000 births X 7.5% = 5,250 births70,000 births X 7.5% = 5,250 births–– 3,500 X $11,000 = $38.5 million3,500 X $11,000 = $38.5 million–– 1,750 X $20,000 = $35 million1,750 X $20,000 = $35 million
2006 costs state of CO = ~$80 million (6%)2006 costs state of CO = ~$80 million (6%)
Linda Barbour, MD, MSPH
Why Is It a ProblemWhy Is It a Problemto Mother?to Mother?
Intensive monitoring of blood Intensive monitoring of blood glucoses, diet restrictions, insulin glucoses, diet restrictions, insulin injections or meds, increased frequency of injections or meds, increased frequency of prenatal visits, financial burdenprenatal visits, financial burdenHigher risk of infectionsHigher risk of infectionsHigher risk of CHigher risk of C--sectionsection~50% Maternal risk of developing ~50% Maternal risk of developing Type 2 DM in 5Type 2 DM in 5--10 years!!!10 years!!!
Linda Barbour, MD, MSPH

3
What About the Baby???
Linda Barbour, MD, MSPH
Diabetic Effects on the FetusDiabetic Effects on the Fetus
↑ Birth trauma↑ C-sec
↑ Childhood Obesity/Diabetes
Measure of too much glucose getting to the
baby
↑ Glucose ↑Glucose ↑Insulin ↑Growth
Amniotic fluid insulin
FetalOvergrowth
Mother Fetus
Self BloodGlucoseMonitoring, Diet, Insulin
Linda Barbour, MD, MSPH
WhatWhat’’s So Bad About a s So Bad About a Big Baby???Big Baby???
Babies have central obesity and canBabies have central obesity and can’’t get through the t get through the birth canalbirth canal→→ →→ birth traumabirth traumaBabies at Babies at ↑↑ risk of stillbirth because they can outgrow risk of stillbirth because they can outgrow their oxygen supplytheir oxygen supplyBabies develop hypoglycemia at birth due to inability to Babies develop hypoglycemia at birth due to inability to ↓↓ their own insulin production immediately and may their own insulin production immediately and may require NICU. Also require NICU. Also polycythemiapolycythemia, , hyperbilirubinemiahyperbilirubinemiaBabies develop enlargement of their pancreas, heart, Babies develop enlargement of their pancreas, heart, and liverand liverBabies at Babies at ↑↑ risk for developing childhood obesity and risk for developing childhood obesity and Type 2 DM Type 2 DM
Linda Barbour, MD, MSPH
Fetal Programming:Fetal Programming:Long Term ImplicationsLong Term Implications
Metabolic factors in the intrauterine environment Metabolic factors in the intrauterine environment have a profound effect on prenatal development and have a profound effect on prenatal development and enhanced susceptibility to later chronic disease enhanced susceptibility to later chronic disease GDMGDM→→ ↑↑ fetal Insulin, neonatal fat, insulin resistance, and fetal Insulin, neonatal fat, insulin resistance, and enlargement of the pancreasenlargement of the pancreasBoth Large (LGA) and Average for Gestational Age (AGA) Both Large (LGA) and Average for Gestational Age (AGA) infants from GDM moms have infants from GDM moms have ↑↑ fat fat vsvs infants without GDM infants without GDM Catalano AJOG 2003Catalano AJOG 2003
High fetal Insulin levels influence hunger centers High fetal Insulin levels influence hunger centers (hypothalamus) involved in energy balance(hypothalamus) involved in energy balance→→ neonatal neonatal obesity and impaired glucose toleranceobesity and impaired glucose tolerance
Linda Barbour, MD, MSPH
Prevalence of IGT in Adolescent Offspring of Prevalence of IGT in Adolescent Offspring of Diabetic Mothers by Amniotic Fluid InsulinDiabetic Mothers by Amniotic Fluid Insulin
0
10
20
30
40
Normal Elevated
Prev
elen
ce (%
)
< 100 pmol/l ≥ 100 pmol/l
Silverman, Metzger et al., Diabetes Care 1995 18(5):611 Linda Barbour, MD, MSPH
Prevalence of Diabetes in Offspring from Prevalence of Diabetes in Offspring from Women with Diabetes Women with Diabetes --Pima IndiansPima Indians
0
10
20
30
40
50
60
70
5-9 10-14 15-19 20-24 25-29 30-34
NonDiabeticPreDiabeticGDM
Offspring of:Offspring of:
Prev
alen
ce (%
)
Age (yr)
Dabelea, Knowler, Pettitt J MFM 2000:9:83Linda Barbour, MD, MSPH
4
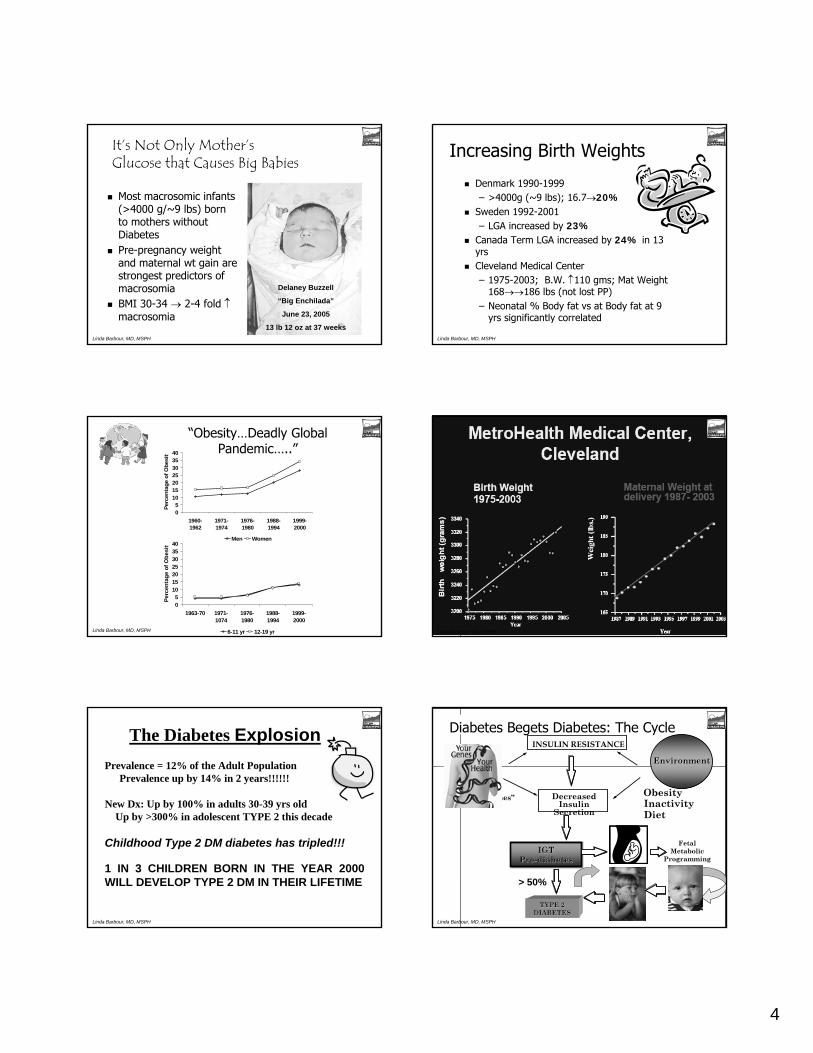
ItIt’’s Not Only Mothers Not Only Mother’’s s Glucose that Causes Big BabiesGlucose that Causes Big Babies
Most Most macrosomicmacrosomic infants infants (>4000 g/~9 lbs) born (>4000 g/~9 lbs) born to mothers without to mothers without DiabetesDiabetesPrePre--pregnancy weight pregnancy weight and maternal wt gain are and maternal wt gain are strongest predictors of strongest predictors of macrosomiamacrosomiaBMI 30BMI 30--34 34 →→ 22--4 fold 4 fold ↑↑macrosomiamacrosomia
Delaney Buzzell
“Big Enchilada”
June 23, 2005
13 lb 12 oz at 37 weeksLinda Barbour, MD, MSPH
Increasing Birth WeightsIncreasing Birth Weights
Denmark 1990Denmark 1990--19991999–– >4000g (~9 lbs); 16.7>4000g (~9 lbs); 16.7→→20%20%
Sweden 1992Sweden 1992--20012001–– LGA increased by LGA increased by 23%23%
Canada Term LGA increased by Canada Term LGA increased by 24%24% in 13 in 13 yrs yrs Cleveland Medical CenterCleveland Medical Center–– 19751975--2003; B.W. 2003; B.W. ↑↑110 110 gmsgms; ; Mat Weight Mat Weight
168168→→→→186 lbs (not lost PP)186 lbs (not lost PP)–– Neonatal % Body fat Neonatal % Body fat vsvs at Body fat at 9 at Body fat at 9
yrs significantly correlated yrs significantly correlated
Linda Barbour, MD, MSPH
05
10152025303540
1960-1962
1971-1974
1976-1980
1988-1994
1999-2000
Perc
enta
ge o
f Obe
sity
Men Women
05
10152025303540
1963-70 1971-1074
1976-1980
1988-1994
1999-2000
Perc
enta
ge o
f Obe
sity
6-11 yr 12-19 yr
““ObesityObesity……Deadly Global Deadly Global PandemicPandemic……....””
Linda Barbour, MD, MSPH Linda Barbour, MD, MSPH
Prevalence = 12% of the Adult Population Prevalence up by 14% in 2 years!!!!!!
New Dx: Up by 100% in adults 30-39 yrs oldUp by >300% in adolescent TYPE 2 this decade
Childhood Type 2 DM diabetes has tripled!!!
1 IN 3 CHILDREN BORN IN THE YEAR 2000 1 IN 3 CHILDREN BORN IN THE YEAR 2000 WILL DEVELOP TYPE 2 DM IN THEIR LIFETIME WILL DEVELOP TYPE 2 DM IN THEIR LIFETIME
The Diabetes Explosion
Linda Barbour, MD, MSPH
GenesGenes EnvironmentEnvironment
““DiabetogenesDiabetogenes”” ObesityObesityInactivityInactivityDietDiet
INSULIN RESISTANCEINSULIN RESISTANCE
DecreasedDecreasedInsulin Insulin
SecretionSecretion
IGTIGTPrePre--diabetesdiabetes
Fetal Fetal MetabolicMetabolic
ProgrammingProgramming
TYPE 2 TYPE 2 DIABETESDIABETES
> 50%> 50%
Diabetes Begets Diabetes: The Cycle
Linda Barbour, MD, MSPH
5
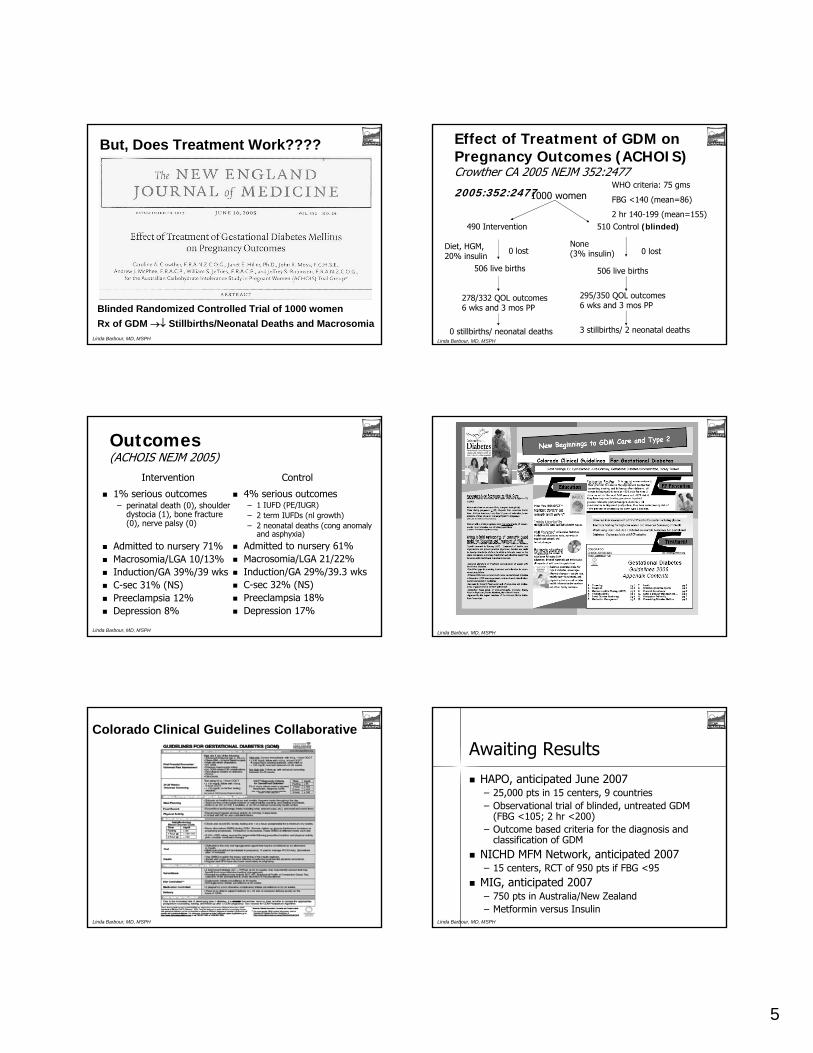
Blinded Randomized Controlled Trial of 1000 womenRx of GDM →↓ Stillbirths/Neonatal Deaths and Macrosomia
But, Does Treatment Work????
Linda Barbour, MD, MSPH
Effect of Treatment of GDM on Effect of Treatment of GDM on Pregnancy Outcomes (ACHOIS) Pregnancy Outcomes (ACHOIS) CrowtherCrowther CA 2005 NEJM 352:2477CA 2005 NEJM 352:2477
2005:352:24772005:352:24771000 womenWHO criteria: 75 gms
FBG <140 (mean=86)
2 hr 140-199 (mean=155)490 Intervention 510 Control (blinded)
0 lost
506 live births
278/332 QOL outcomes 6 wks and 3 mos PP
0 lost
506 live births
295/350 QOL outcomes 6 wks and 3 mos PP
Diet, HGM, 20% insulin
None (3% insulin)
0 stillbirths/ neonatal deaths 3 stillbirths/ 2 neonatal deathsLinda Barbour, MD, MSPH
OutcomesOutcomes(ACHOIS NEJM 2005)(ACHOIS NEJM 2005)
1% serious outcomes1% serious outcomes–– perinatalperinatal death (0), shoulder death (0), shoulder
dystociadystocia (1), bone fracture (1), bone fracture (0), nerve palsy (0)(0), nerve palsy (0)
Admitted to nursery 71%Admitted to nursery 71%MacrosomiaMacrosomia/LGA 10/13%/LGA 10/13%Induction/GA 39%/39 wksInduction/GA 39%/39 wksCC--sec 31% (NS)sec 31% (NS)PreeclampsiaPreeclampsia 12%12%Depression 8%Depression 8%
4% serious outcomes4% serious outcomes–– 1 IUFD (PE/IUGR)1 IUFD (PE/IUGR)–– 2 term 2 term IUFDsIUFDs ((nlnl growth)growth)–– 2 neonatal deaths (cong anomaly 2 neonatal deaths (cong anomaly
and asphyxia)and asphyxia)
Admitted to nursery 61%Admitted to nursery 61%MacrosomiaMacrosomia/LGA 21/22%/LGA 21/22%Induction/GA 29%/39.3 wksInduction/GA 29%/39.3 wksCC--sec 32% (NS)sec 32% (NS)PreeclampsiaPreeclampsia 18%18%Depression 17%Depression 17%
Intervention Control
Linda Barbour, MD, MSPH Linda Barbour, MD, MSPH
Colorado Clinical Guidelines Collaborative
Linda Barbour, MD, MSPH
Awaiting ResultsAwaiting Results
HAPO, anticipated June 2007HAPO, anticipated June 2007–– 25,000 pts in 15 centers, 9 countries25,000 pts in 15 centers, 9 countries–– Observational trial of blinded, untreated GDM Observational trial of blinded, untreated GDM
(FBG <105; 2 hr <200)(FBG <105; 2 hr <200)–– Outcome based criteria for the diagnosis and Outcome based criteria for the diagnosis and
classification of GDM classification of GDM
NICHD MFM Network, anticipated 2007NICHD MFM Network, anticipated 2007–– 15 centers, RCT of 950 pts if FBG <9515 centers, RCT of 950 pts if FBG <95
MIG, anticipated 2007MIG, anticipated 2007–– 750 pts in Australia/New Zealand750 pts in Australia/New Zealand–– MetforminMetformin versus Insulinversus Insulin
Linda Barbour, MD, MSPH

6
Update: 5Update: 5thth IntInt Workshop on Workshop on GDM, Nov 11GDM, Nov 11--13, 200513, 2005
Newer trials:Newer trials:–– CrowtherCrowther, NEJM, 2005, NEJM, 2005
Blinded RCT on Rx GDM Blinded RCT on Rx GDM
–– CGMS dataCGMS data–– RCTRCT’’ss of Fetal Based Strategy to guide Rxof Fetal Based Strategy to guide Rx–– GlyburideGlyburide trials 2004trials 2004--20062006
Jacobson, Jacobson, ChaitChait, Conway, Kremer, Kahn/Barbour , Conway, Kremer, Kahn/Barbour
–– Postpartum Diabetes PreventionPostpartum Diabetes PreventionDPT, PIPODDPT, PIPOD
Linda Barbour, MD, MSPH
Screening and DiagnosisScreening and Diagnosis
No significant change; universal No significant change; universal screening if high prevalencescreening if high prevalence–– If 130 mg/dl chosen; If 130 mg/dl chosen; senssens 90% but 90% but
specificity 80%specificity 80%–– If 140 mg/dl picked, If 140 mg/dl picked, senssens 80% but 80% but
specificity 90%specificity 90%Repeat 3 hr OGTT in 3Repeat 3 hr OGTT in 3--4 wks if 1 4 wks if 1 abnormal valueabnormal valueAwaiting for HAPO trial resultsAwaiting for HAPO trial results
Linda Barbour, MD, MSPH
ScreeningScreeningLow Risk:Low Risk: (must meet ALL criteria not to screen)(must meet ALL criteria not to screen)–– Age <25Age <25–– Normal weightNormal weight–– CaucasianCaucasian–– No DM in 1No DM in 1stst degree relativedegree relative–– No No hxhx of glucose intoleranceof glucose intolerance–– No No hxhx of poor obstetric outcomeof poor obstetric outcome
High Risk High Risk (must meet ANY criteria to screen (must meet ANY criteria to screen EARLYEARLY))–– ObesityObesity–– HxHx GDM (High prevalence of undiagnosed Type 2 DM)GDM (High prevalence of undiagnosed Type 2 DM)–– HxHx macrosomicmacrosomic infantinfant–– GlycosuriaGlycosuria–– FH DM FH DM –– PCOS (PCOS (40% 40% glucgluc intolintol) ) LegroLegro RS 2005 JCEM:90:3236RS 2005 JCEM:90:3236
Advanced maternal age (>35 yrs) and high risk ethnic pop Advanced maternal age (>35 yrs) and high risk ethnic pop ↑↑ risk)risk)
Linda Barbour, MD, MSPH
Diagnostic CriteriaDiagnostic Criteria--100 g OGTT100 g OGTT(Carpenter and (Carpenter and CoustanCoustan))
FBG FBG ≥≥ 95 mg/dl95 mg/dl1 hr 1 hr ≥≥ 180 mg/dl180 mg/dl2 hr 2 hr ≥≥ 155 mg/dl155 mg/dl3 hr 3 hr ≥≥ 140 mg/dl140 mg/dl
2 or more values diagnostic 2 or more values diagnostic
Linda Barbour, MD, MSPH
Screening/Screening/DiagnositcDiagnositcStrategiesStrategiesIf glucose on 50 gm If glucose on 50 gm glucolaglucola ≥≥200 mg/dl200 mg/dl–– Check FBG; If Check FBG; If ≥≥ 95 mg/dl, treat as GDM95 mg/dl, treat as GDMGlucolaGlucola abnlabnl early but 3 hr early but 3 hr nlnl→→ repeat 3 hr at repeat 3 hr at 2424--28 wks28 wksIf 1 If 1 abnlabnl value on 3 value on 3 hrhr→→repeatrepeat 3 hr in 33 hr in 3--4 wks; 4 wks; recommend MNT and physical activityrecommend MNT and physical activityIf GDM If GDM dxdx <24 wks; consider A1C to <24 wks; consider A1C to r/or/omalformation risk malformation risk BariaticBariatic surgery pts: self surgery pts: self glucgluc monitoring if monitoring if unable to drink 100 g OGTTunable to drink 100 g OGTT
Linda Barbour, MD, MSPH
Self Glucose MonitoringSelf Glucose MonitoringFBG and 1 or 2 hr postprandialFBG and 1 or 2 hr postprandialNo data to support testing < No data to support testing < q.i.dq.i.dCost issue: vary times of testing, usually FBG Cost issue: vary times of testing, usually FBG and after largest meal, attempt at least bid and after largest meal, attempt at least bid AlwaysAlways check glucose meter memories for check glucose meter memories for true values; do not rely on written valuestrue values; do not rely on written valuesBe suspicious of values ending in 0, 5, and less Be suspicious of values ending in 0, 5, and less than 15 points variation at given timethan 15 points variation at given timeCalibrate glucose meters oftenCalibrate glucose meters oftenMake sure fingertips are clean before sample Make sure fingertips are clean before sample
Linda Barbour, MD, MSPH

7
Medical Nutrition TherapyMedical Nutrition TherapyMacronutrient percentages dropped (min 175 g Macronutrient percentages dropped (min 175 g carbscarbs))Concerns about substituting high fatConcerns about substituting high fat
High fat intake may High fat intake may ↑↑ risk GDM risk GDM Saldana TM 2004Saldana TM 2004↑↑ Maternal Maternal TGsTGs associated with associated with macrosomiamacrosomiaIdeal macronutrient composition unknownIdeal macronutrient composition unknown
Avoid simple Avoid simple carbscarbs, saturated fats, saturated fatsCarbCarb counting may be useful to blunt PP glucosecounting may be useful to blunt PP glucoseAvoid excessive weight gain (1990 IOM guidelines)Avoid excessive weight gain (1990 IOM guidelines)–– BMI 20BMI 20--25: 2525: 25--35 lbs35 lbs–– BMI 26BMI 26--29: 1629: 16--25 lbs25 lbs–– BMI >29: 13 lbsBMI >29: 13 lbs--??–– 1600 1600 calscals: : ↓↓ glucgluc, , TGsTGs without without ketonuriaketonuria KnoppKnopp RH 1991RH 1991
Linda Barbour, MD, MSPH
Physical ActivityPhysical Activity
Adopt population recommendations Adopt population recommendations unless obstetric or medical unless obstetric or medical contraindicationcontraindication–– 30 30 minsmins 5 days a week5 days a week–– HR <140, Avoid overheating, dehydrationHR <140, Avoid overheating, dehydration–– May be split into shorter increments more May be split into shorter increments more
frequently frequently
Linda Barbour, MD, MSPH
Initiation of Medical TherapyInitiation of Medical Therapy
120 mg/dl120 mg/dl90 mg/dl90 mg/dlJovanovicJovanovic
120 120 mg/dlmg/dl
130130--140 140 mg/dlmg/dl
95 mg/dl95 mg/dl*ACOG, *ACOG, 2001; 4,52001; 4,5thth
WorkshopWorkshop
130 mg/dl130 mg/dl155 mg/dl155 mg/dl105 mg/dl105 mg/dlADA, 2004ADA, 2004(plasma)(plasma)
2 hr PP2 hr PP1 hr PP1 hr PPFBGFBG
Linda Barbour, MD, MSPH
Continuous Glucose Continuous Glucose Monitoring Sensor (CGMS)Monitoring Sensor (CGMS)
FBGFBG in normal pregnancy: in normal pregnancy: 7575 mg/dlmg/dlPeak postprandial: Peak postprandial: 110110 mg/dlmg/dlPeak ~70Peak ~70--90 90 minsmins but differs with fat but differs with fat intake intake YogevYogev Y AJOG 2004Y AJOG 2004
No changes in recommended targets No changes in recommended targets or timing until HAPO outor timing until HAPO out
Linda Barbour, MD, MSPH
Is Maternal Glucose Best Endpoint?Is Maternal Glucose Best Endpoint?Fetal Based Strategy Fetal Based Strategy
Maternal Glucoses Are Deceptive and Do Not Reflect Maternal Glucoses Are Deceptive and Do Not Reflect Accurately Excess Nutrition to FetusAccurately Excess Nutrition to Fetus–– FetalFetal--Placental Glucose Steal SyndromePlacental Glucose Steal Syndrome–– Progressive siphoning of Progressive siphoning of glucgluc by fetus with by fetus with hyperinsulinemiahyperinsulinemia
Fetal Criteria to Dictate Maternal Therapy Fetal Criteria to Dictate Maternal Therapy ↑↑ Abdominal circumference (AC) on US due to sq fat Abdominal circumference (AC) on US due to sq fat and visceral fat in liver (and visceral fat in liver (abdabd sq fat accounts for 63% sq fat accounts for 63% variance of fetal AC)variance of fetal AC)Correlates with Correlates with aminioticaminiotic fluid insulin levels (AFI)fluid insulin levels (AFI)
Linda Barbour, MD, MSPH
Rationale for Fetal Based StrategyRationale for Fetal Based Strategy
Measurement of fetal response to
excessive glucose transport
↑ Glucose ↑Glucose ↑Insulin ↑Growth
Amniotic fluid insulin
FetalOvergrowth
Mother Fetus
Self BloodGlucoseMonitoring
“Diabetic Fetopathy”
↑ AC on US at 30-32 wks
Linda Barbour, MD, MSPH

8
RCTRCT’’ss of Selected Insulin of Selected Insulin Therapy Based on Fetal USTherapy Based on Fetal US
Buchanan, Buchanan, KjosKjos 1994 1994 Diabetes Care 17:275Diabetes Care 17:275–– 59 A1GDM, good control; fetal AC>75% at 2959 A1GDM, good control; fetal AC>75% at 29--33 wks33 wks–– RCT HGM, Diet Vs HGM, Diet, Insulin (1.3 units/kg)RCT HGM, Diet Vs HGM, Diet, Insulin (1.3 units/kg)–– LGA 45% LGA 45% vsvs 13% (3878 13% (3878 vsvs 3647 3647 gmsgms) )
Rossi 2000 Rossi 2000 ActaActa ObstetObstet GynecolGynecol ScandScand 79:64979:649KjosKjos 2001 2001 Diabetes Care 24:1904Diabetes Care 24:1904SchaeferSchaefer--Graf, Graf, KjosKjos 2004 2004 Diabetes Care 2004;27:297Diabetes Care 2004;27:297BonomoBonomo 2004 2004 Diabetes & Diabetes & MetabMetab 2004;30:2372004;30:237
Linda Barbour, MD, MSPH
RCT of GDM Based on Fetal US RCT of GDM Based on Fetal US GrowthGrowth ((BonomoBonomo, , DiabDiab & & MetabMetab 2004;30:237)2004;30:237)
RCT of 229 GDM in ItalyRCT of 229 GDM in ItalyRx Goals:Rx Goals:–– Conventional 90/120 mg/dl Conventional 90/120 mg/dl –– Modified: AC<75% 100/140; AC>75% 80/100Modified: AC<75% 100/140; AC>75% 80/100
Insulin Used 17% Insulin Used 17% convconv vsvs 30% in modified30% in modifiedOutcomes:Outcomes:–– MacrosomiaMacrosomia: 11.5% in : 11.5% in convconv vsvs 3.3% in modified3.3% in modified–– LGA: 18% LGA: 18% vsvs 8%; SGA 9% 8%; SGA 9% vsvs 6%6%
Concentrate therapeutic efforts based on US Concentrate therapeutic efforts based on US evidence of Fetal evidence of Fetal HyperinsulinemiaHyperinsulinemia
Linda Barbour, MD, MSPH
Fetal Based TherapyFetal Based Therapy55thth IntInt WorkshopWorkshop
There are 5 There are 5 RCTsRCTs which which demonstrate that using a fetal demonstrate that using a fetal based strategy (AC>75based strategy (AC>75thth % at 28% at 28--32 wks) to guide therapy can be 32 wks) to guide therapy can be useful in identifying patients who useful in identifying patients who may benefit from more intensive may benefit from more intensive medical management medical management
Linda Barbour, MD, MSPH
Insulin TherapyInsulin TherapyShort acting insulin analogues have Short acting insulin analogues have advantage to blunt postprandial glucoseadvantage to blunt postprandial glucose–– LisproLispro (>500 pregnancies); (>500 pregnancies); Wyatt JW Wyatt JW
2005 Diabetic Med;22:8032005 Diabetic Med;22:803–– AspartAspart Pettit DJ 2003 Pettit DJ 2003 DiabDiab Care26:183Care26:183Not enough data with Not enough data with GlargineGlargine ((LantusLantus))–– Concern with affinity for IGFConcern with affinity for IGF--1 1
receptor, especially with receptor, especially with proliferativeproliferativeretinopathyretinopathy
Linda Barbour, MD, MSPH
Insulin pharmacokineticsInsulin pharmacokineticsLispro / AspartRegularNPHGlargine
2.5 hr 4 hr 12 hr 24 hrInsulin
Injection
Glyburide
Linda Barbour, MD, MSPH
Traditional insulin therapyTraditional insulin therapySplit mixed Regular/NPH BIDSplit mixed Regular/NPH BID
AMmeal
Noonmeal
PMmeal
HS
RegularNPH
3:00 a.m.
2/3 total dose in a.m. (2/3 N; 1/3 R)
1/3 in p.m. (1/2 N; 1/2 R)
Linda Barbour, MD, MSPH

9
Physiologic Glucose ProfilePhysiologic Glucose Profile
AMmeal
Noonmeal
PMmeal
HS
Glucose
∆30-40 mg/dL ∆30-40 mg/dL∆30-40 mg/dL
<100mg/dL
Linda Barbour, MD, MSPH
Physiologic insulin therapyPhysiologic insulin therapy
AMmeal
Noonmeal
PMmeal
HS
NPH/Glarginelispro / aspart
Basal amount ~50% Bolus amount ~50%Linda Barbour, MD, MSPH
Insulin dosing with Insulin dosing with Humalog/AspartHumalog/Aspart
Use weight based (0.5Use weight based (0.5--1U/kg) or present 1U/kg) or present dose (add % if poor control)dose (add % if poor control)Give Give ½½ total dose as NPHtotal dose as NPH–– Split equally in a.m. and p.m. (consider Split equally in a.m. and p.m. (consider qhsqhs
and more NPH in p.m. than a.m.) and more NPH in p.m. than a.m.)
Give Give ½½ as as HumalogHumalog or or NovalogNovalog–– Give 1/3 with each mealGive 1/3 with each meal–– Give according to % Give according to % carbscarbs at each mealat each meal–– Give according to preGive according to pre--meal correction factor meal correction factor
and and carbcarb ratioratioLinda Barbour, MD, MSPH
GlyburideGlyburideOctober 2000; LangerOctober 2000; Langer’’s landmark RCT of s landmark RCT of GlyburideGlyburide Vs Insulin in 404 women, NEJMVs Insulin in 404 women, NEJM–– NS difference in LGA, NS difference in LGA, macrosomiamacrosomia, neonatal , neonatal
outcomes; only 4% pts switched to insulinoutcomes; only 4% pts switched to insulinConway, 2004 (Conway, 2004 (UnivUniv Texas): 75 ptsTexas): 75 ptsKremer, 2004 (Kremer, 2004 (UnivUniv Florida): 73 pts Florida): 73 pts ChmaitChmait, 2004 (, 2004 (UnivUniv CA, San Diego): 69 ptsCA, San Diego): 69 ptsJacobson, 2005 (Kaiser, Northern Jacobson, 2005 (Kaiser, Northern CalifCalif): 236 pts): 236 ptsKahn, Barbour 2006 (Kahn, Barbour 2006 (UnivUniv CO) 95 pts CO) 95 pts
Linda Barbour, MD, MSPH
Predictors of Predictors of GlyburideGlyburideFailure in the Treatment of Failure in the Treatment of Gestational DiabetesGestational DiabetesObstetObstet GynecolGynecol 2006;107(6):13032006;107(6):1303
BronwenBronwen Kahn, Jill Davies, Anne Lynch, Kahn, Jill Davies, Anne Lynch, Regina Reynolds, Linda BarbourRegina Reynolds, Linda BarbourUniversity of Colorado Health Sciences CenterUniversity of Colorado Health Sciences CenterDepartments of OBDepartments of OB--GynGyn, Medicine, and Pediatrics , Medicine, and Pediatrics
Linda Barbour, MD, MSPH
Success Versus Failure Success Versus Failure
**Age = 29 yrsAge = 29 yrsGravidity =2.7Gravidity =2.7BMI = 30BMI = 30Mat Wt gain = 26 lbsMat Wt gain = 26 lbsHxHx GDM=17%GDM=17%FBG = 100 mg/dl FBG = 100 mg/dl GestGest Age at Age at DxDx=28 wks=28 wks
*Age = 35 yrs (p=0.0001)*Age = 35 yrs (p=0.0001)*Gravidity =4.4 (p=0.004)*Gravidity =4.4 (p=0.004)BMI = 32 BMI = 32 Mat Wt gain = 27 lbsMat Wt gain = 27 lbs**HxHx GDM=35% (p=0.08)GDM=35% (p=0.08)*FBG =111 mg/dl (p=0.03)*FBG =111 mg/dl (p=0.03)****GestGest Age at Age at DxDx =22 wks=22 wks(p=0.003)(p=0.003)
Successes (81) Failures (20)
*Multiple regression model; Gest age < 25 wks; OR=5.5
Linda Barbour, MD, MSPH

10
GlyburideGlyburide TroubleshootingTroubleshooting
Peaks at 3Peaks at 3--4 hours4 hoursGive 30 minsGive 30 mins--1 hr before breakfast/dinner1 hr before breakfast/dinnerEat portion of breakfast mid morning Eat portion of breakfast mid morning (instead of adding snack)(instead of adding snack)Hypoglycemia common mid morningHypoglycemia common mid morningMay need to add NPH May need to add NPH qhsqhs to treat to treat ↑↑ FBGFBG–– GlyburideGlyburide b.i.db.i.d. with meals; NPH . with meals; NPH qhsqhs
Linda Barbour, MD, MSPH
Oral Hypoglycemic RxOral Hypoglycemic Rx55thth IntInt WorkshopWorkshop
GlyburideGlyburide can be a useful adjunct to therapy can be a useful adjunct to therapy in women not controlled on MNTin women not controlled on MNT20% failure rate, especially women 20% failure rate, especially women diagnosed prior to 25 weeks of pregnancy, diagnosed prior to 25 weeks of pregnancy, marked hyperglycemia, and obesity marked hyperglycemia, and obesity Dose 30Dose 30--60 60 minsmins before meals due to 3before meals due to 3--4 4 hour peakhour peakInadequate data for continuing Inadequate data for continuing MetforminMetformin–– Readily crosses the placenta but no Readily crosses the placenta but no ↑↑ anomaliesanomalies
–– RCT RCT PalombaPalomba S JCEM 2005S JCEM 2005:: ↓↓ pregnancy loss in pregnancy loss in PCOS women but was not continued PCOS women but was not continued
Linda Barbour, MD, MSPH
Stay TunedStay Tuned…………………………
HAPO; new screening guidelines HAPO; new screening guidelines and thresholds for Rxand thresholds for RxMFMU; Rx recommendationsMFMU; Rx recommendationsMIG; MIG; MetforminMetformin
Linda Barbour, MD, MSPH
US and Fetal SurveillanceUS and Fetal SurveillanceNo significant changeNo significant changeFetal activity records in all GDM womenFetal activity records in all GDM womenConsider Consider NSTNST’’ss in women not controlled on in women not controlled on MNT aloneMNT aloneUS for growth at 28US for growth at 28--32 wks may be helpful 32 wks may be helpful to dictate aggressiveness of therapyto dictate aggressiveness of therapyEFW at term poor PPV but if >4200 EFW at term poor PPV but if >4200 gmsgmsand and ↑↑ AC, higher risk of shoulder AC, higher risk of shoulder dystociadystocia
Linda Barbour, MD, MSPH
Labor and DeliveryLabor and DeliveryDelivery at 38Delivery at 38--39 weeks in pts with good 39 weeks in pts with good dates and favorable cervix was shown in dates and favorable cervix was shown in one RCT to decrease one RCT to decrease macrosomiamacrosomia without without increasing Cesarean delivery rate increasing Cesarean delivery rate KjosKjos SLSL1993 AJOG;169:6111993 AJOG;169:611
Delivery prior to 38 wks requires Delivery prior to 38 wks requires amniocentesisamniocentesisTiming of delivery relatively openTiming of delivery relatively openCesarean delivery for obstetric indications Cesarean delivery for obstetric indications No new dataNo new data
Linda Barbour, MD, MSPH
What Happens to What Happens to Mother Postpartum?Mother Postpartum?
Pregnancy is a Pregnancy is a ““Stress TestStress Test”” for the development of for the development of Type 2 DMType 2 DM~50% Diabetes risk in 5~50% Diabetes risk in 5--10 yrs 10 yrs 75 gm Oral Glucose Tolerance Test at 675 gm Oral Glucose Tolerance Test at 6--12 wks PP12 wks PP–– If Impaired Glucose Tolerance/PreIf Impaired Glucose Tolerance/Pre--diabetes (~15%) diabetes (~15%)
→→ ~80% risk of Type 2 DM in 5~80% risk of Type 2 DM in 5--10 yrs10 yrsDiabetes Prevention Trial showed a Diabetes Prevention Trial showed a 17% progression 17% progression per year to Type 2 Diabetesper year to Type 2 Diabetes in moms with a in moms with a hxhx of of GDM and IGT GDM and IGT
Linda Barbour, MD, MSPH
11
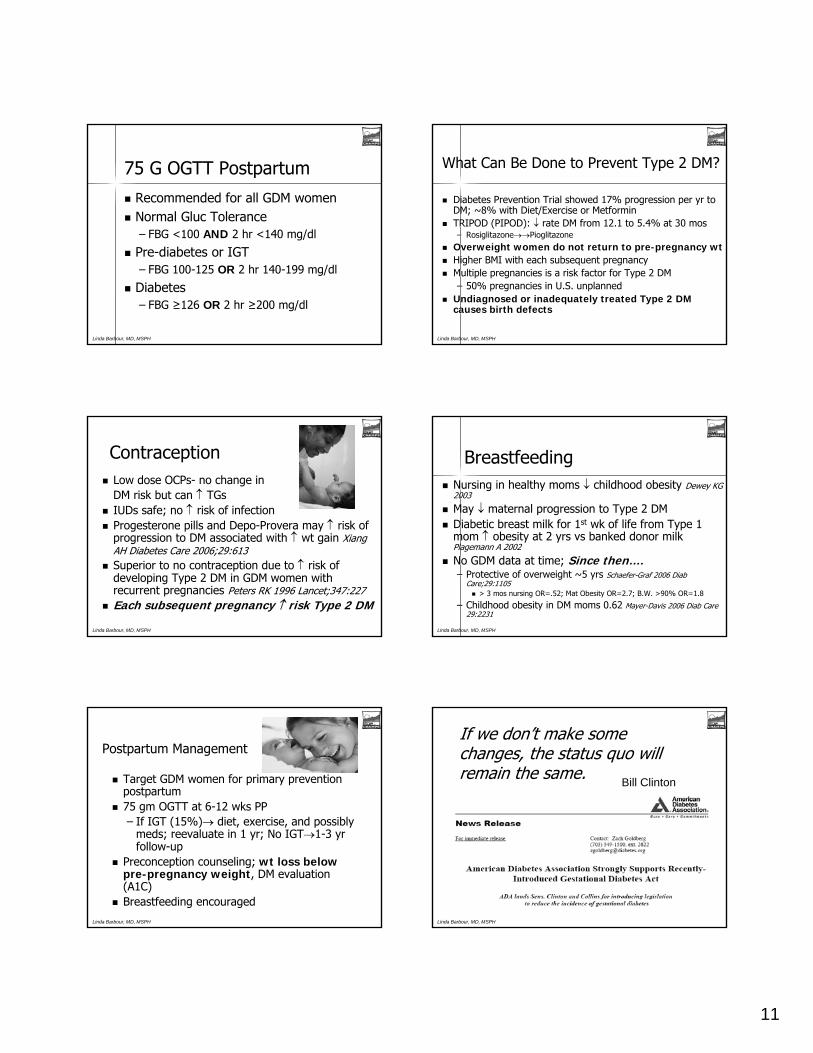
75 G OGTT Postpartum75 G OGTT Postpartum
Recommended for all GDM womenRecommended for all GDM womenNormal Normal GlucGluc ToleranceTolerance–– FBG <100 FBG <100 ANDAND 2 hr <140 mg/dl2 hr <140 mg/dl
PrePre--diabetes or IGTdiabetes or IGT–– FBG 100FBG 100--125 125 OROR 2 hr 1402 hr 140--199 mg/dl199 mg/dl
DiabetesDiabetes–– FBG FBG ≥≥126 126 OROR 2 hr 2 hr ≥≥200200 mg/dl mg/dl
Linda Barbour, MD, MSPH
What Can Be Done to Prevent Type 2 DM?What Can Be Done to Prevent Type 2 DM?
Diabetes Prevention Trial showed 17% progression per yr to Diabetes Prevention Trial showed 17% progression per yr to DM; ~8% with Diet/Exercise or DM; ~8% with Diet/Exercise or MetforminMetforminTRIPOD (PIPOD): TRIPOD (PIPOD): ↓↓ rate DM from 12.1 to 5.4% at 30 rate DM from 12.1 to 5.4% at 30 mosmos–– RosiglitazoneRosiglitazone→→→→PioglitazonePioglitazone
Overweight women do not return to preOverweight women do not return to pre--pregnancy wtpregnancy wtHigher BMI with each subsequent pregnancyHigher BMI with each subsequent pregnancyMultiple pregnancies is a risk factor for Type 2 DMMultiple pregnancies is a risk factor for Type 2 DM–– 50% pregnancies in U.S. unplanned 50% pregnancies in U.S. unplanned
Undiagnosed or inadequately treated Type 2 DM Undiagnosed or inadequately treated Type 2 DM causes birth defectscauses birth defects
Linda Barbour, MD, MSPH
ContraceptionContraceptionLow dose Low dose OCPsOCPs-- no change in no change in DM risk but can DM risk but can ↑↑ TGsTGsIUDs safe; no IUDs safe; no ↑↑ risk of infectionrisk of infectionProgesterone pills and DepoProgesterone pills and Depo--Provera may Provera may ↑↑ risk of risk of progression to DM associated with progression to DM associated with ↑↑ wt gain wt gain Xiang Xiang AH Diabetes Care 2006;29:613AH Diabetes Care 2006;29:613Superior to no contraception due to Superior to no contraception due to ↑↑ risk of risk of developing Type 2 DM in GDM women with developing Type 2 DM in GDM women with recurrent pregnancies recurrent pregnancies Peters RK 1996 Lancet;347:227Peters RK 1996 Lancet;347:227Each subsequent pregnancy Each subsequent pregnancy ↑↑ risk Type 2 DMrisk Type 2 DM
Linda Barbour, MD, MSPH
BreastfeedingBreastfeedingNursing in healthy moms Nursing in healthy moms ↓↓ childhood obesity childhood obesity Dewey KG Dewey KG 20032003
May May ↓↓ maternal progression to Type 2 DMmaternal progression to Type 2 DMDiabetic breast milk for 1Diabetic breast milk for 1stst wk of life from Type 1 wk of life from Type 1 mom mom ↑↑ obesity at 2 yrs obesity at 2 yrs vsvs banked donor milk banked donor milk PlagemannPlagemann A 2002A 2002
No GDM data at time; No GDM data at time; Since thenSince then……..–– Protective of overweight ~5 yrs Protective of overweight ~5 yrs SchaeferSchaefer--Graf 2006 Graf 2006 DiabDiab
Care;29:1105Care;29:1105> 3 > 3 mosmos nursing OR=.52; Mat Obesity OR=2.7; B.W. >90% OR=1.8nursing OR=.52; Mat Obesity OR=2.7; B.W. >90% OR=1.8
–– Childhood obesity in DM moms 0.62Childhood obesity in DM moms 0.62 MayerMayer--Davis 2006 Davis 2006 DiabDiab Care Care 29:2231 29:2231
Linda Barbour, MD, MSPH
Postpartum ManagementPostpartum Management
Target GDM women for primary prevention Target GDM women for primary prevention postpartum postpartum 75 gm OGTT at 675 gm OGTT at 6--12 wks PP12 wks PP–– If IGT (15%)If IGT (15%)→→ diet, exercise, and possibly diet, exercise, and possibly
meds; reevaluate in 1 yr; No IGTmeds; reevaluate in 1 yr; No IGT→→11--3 yr 3 yr followfollow--upup
Preconception counseling; Preconception counseling; wt loss below wt loss below prepre--pregnancy weightpregnancy weight, DM evaluation , DM evaluation (A1C) (A1C) Breastfeeding encouraged Breastfeeding encouraged
Linda Barbour, MD, MSPH
If we donIf we don’’t make some t make some changes, the status quo will changes, the status quo will remain the same.remain the same. Bill Clinton
Linda Barbour, MD, MSPH

12
Understanding and Monitoring GDMUnderstanding and Monitoring GDM–– Research Advisory Committee headed by CDCResearch Advisory Committee headed by CDC–– MultiMulti--site projects for identification and data collectionsite projects for identification and data collection–– Track mothers and prevent Type 2 DMTrack mothers and prevent Type 2 DM
Demonstration Grant Programs Demonstration Grant Programs –– Expand communityExpand community--based activitiesbased activities–– Support stateSupport state--based prevention programsbased prevention programs–– Train health providersTrain health providers
Research Expansion of GDM and Obesity Research Expansion of GDM and Obesity –– Expand basic, clinical and public health researchExpand basic, clinical and public health research
Investigative therapiesInvestigative therapiesFacilitate enrollment into clinical trials for high prevalence pFacilitate enrollment into clinical trials for high prevalence populationsopulationsDevelop better screening and diagnostic methodsDevelop better screening and diagnostic methodsElucidate causal factors Elucidate causal factors
Gestational Diabetes Actwww.diabetes.org/advocacy
Linda Barbour, MD, MSPH
In my beginning, is my end.T.S. Eliot, Four Quartlets, The Dry Salvages
Linda Barbour, MD, MSPH
Linda Barbour, MD, MSPH
Thank You for Joining CHAMPS and Thank You for Joining CHAMPS and Dr. Barbour for this Dr. Barbour for this
Distance Learning Event!Distance Learning Event!
Your opinions are very important to us. Your opinions are very important to us. Please take a few minutes to complete the Evaluation for this wePlease take a few minutes to complete the Evaluation for this webcast. If you are bcast. If you are
applying for Continuing Medical Education (CME) credit, you mustapplying for Continuing Medical Education (CME) credit, you must complete the complete the CME questions found at the end of the Evaluation. CME questions found at the end of the Evaluation.
Only one person per computer may use the Only one person per computer may use the online version of the Evaluation/CME form.online version of the Evaluation/CME form.
Click on the link to the side of your screen to download a printClick on the link to the side of your screen to download a printable form that can be able form that can be completed by additional participants and faxed to CHAMPS. completed by additional participants and faxed to CHAMPS.
The AAFP invites comments on any activity that has been approvedThe AAFP invites comments on any activity that has been approved for AAFP CME for AAFP CME credit. Please forward your comments on the quality of this actcredit. Please forward your comments on the quality of this activity to ivity to
[email protected]@aafp.org. .
We hope you will join us again!We hope you will join us again!
Community Health Association of Mountain/Plains States (CHAMPS)Community Health Association of Mountain/Plains States (CHAMPS)www.CHAMPSonline.orgwww.CHAMPSonline.org –– 303303--861861--51655165
SCREENING
Universal Risk Assessment at First Prenatal Encounter
• Complete risk assessment for gestational diabetes mellitus (GDM) accounting for patient history and clinicalrisk factors.
• Classify high-risk with one or more of the following risk factors:- Advanced maternal age (age ≥ 35 years).- Obesity (BMI > 29 kg/m2).- High-risk ethnic population (Asian/Pacific Islander, American Indian, Hispanic, Black).- Personal history of GDM.- Previous macrosomic infant.- History of GDM related obstetric complications.- First degree relative with diabetes.- Polycystic Ovary Syndrome (PCOS).- Glycosuria.
• If woman does not meet any of the above criteria, complete Universal Screening between 24–28 weeks.
• The option to preclude universal screening at any time during pregnancy, although not recommended due to theincreasing incidence of GDM in Colorado, may be considered only when ALL the following criteria are met:
- Age < 25 years.- BMI ≤ 26 kg/m2.- Caucasian.- No known diabetes in a 1st degree relative.- No history of abnormal glucose tolerance.- No history of poor obstetric outcome.
Early Screening for High-Risk Women
• Evaluate high-risk women for glucose tolerance as soon as prenatal care is established. Do not delay testing until24–28 weeks.
- Perform laboratory screening with a 50-g, 1-hour oral glucose challenge test (OGCT), administered withoutregard to time elapsed since the last meal.
- If OGCT is ≥ 135 mg/dl, follow with a diagnostic 100-g, 3-hour oral glucose tolerance test (OGTT).
1Approved 09/12/2006
1. Screening . . . . . . . . . . . . . . . . . . . . pg 12. Diagnosis . . . . . . . . . . . . . . . . . . . . pg 23. Medical Nutrition Therapy (MNT) . . pg 34. Physical Activity . . . . . . . . . . . . . . . pg 45. Blood Glucose Monitoring . . . . . . . pg 4
6. Medication Management . . . . . . . . pg 57. Prenatal Surveillance . . . . . . . . . . . pg 58. Labor & Delivery Management . . . . pg 69. Postpartum Follow-Up . . . . . . . . . . pg 6
10. Pre-existing Diabetes Mellitus . . . . pg 7
Gestational Diabetes Guidelines 2006
www.coloradoguidelines.org

- If OGTT reflects GDM diagnosis, and there is strong suspicion of pre-existing diabetes, obtain an HbA1c.- Possible signs of pre-existing diabetes include an early positive OGTT, very high fasting glucose ≥ 110mg/dl, or very high values on the 100-g, 3-hour OGTT > 250 mg/dl.
- HbA1c > 6.5% in any gestation indicates need for an anatomy scan and echocardiogram to rule outmajor malformations and possible further diagnostic testing.
- If all values on the 3-hour OGTT are normal, repeat OGTT between 24–28 weeks.
- If OGCT < 135 mg/dl, rescreen between 24–28 weeks.
Universal Screening between 24–28 weeks
• Perform laboratory screening with a 50-g, 1-hour OGCT administered without regard to time elapsed since thelast meal.
• If OGCT is ≥ 135 mg/dl, follow with a diagnostic 100-g, 3-hour oral glucose tolerance test (OGTT).
- If OGCT ≥ 200 mg/dl*, test serum fasting blood glucose (FBG) before 100-g, 3-hour OGTT is given.- If serum FBG < 95 mg/dl, proceed with OGTT.- If serum FBG ≥ 95 mg/dl, diagnose GDM. No OGTT necessary.- If FBG result is not immediately available, continue with OGTT.
* There are no accepted criteria or literature to support the 1-hour test alone.
- If suspect glucose intolerance due to macrosomia, polyhydramnios, or any other clinical indicators, rescreenanytime in the 3rd trimester.
• If OGCT < 135 mg/dl, no further testing required.
DIAGNOSIS
• The diagnostic test indicated for GDM is a 100-g, 3-hour OGTT in a fasting state after a 3-day unrestricted diet(150-g of carbohydrate or 10 carbohydrate servings per day).
- Most healthy women consume ≥ 150-g of carbohydrate per day.- If there is concern that carbohydrate intake is inadequate due to a low-carbohydrate diet, hyperemesisgravidarum, acute medical or lifestyle stress, chronic malnutrition, restricted diet due to philosophical/religious/health beliefs or eating disorders, instruct to consume at least 10 carbohydrate servings per day for 3 daysprior to test.
• Follow these guidelines for the OGTT:- No food or beverage 8–14 hours before test, except water.- No smoking during the test.- Remain at rest during the test.- Drink glucose solution in less than 5 minutes.
OGTT Diagnostic Criteria for Gestational Diabetes*
• If only one value meets or exceedsthresholds, repeat 100-g, 3-hour OGTT in3–4 weeks and recommend physical activityand nutrition counseling because 30% ofwomen subsequently develop GDM.
• If 2 or more values meet or exceedthresholds, diagnose GDM.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
2Approved 09/12/2006
Time mg/dl
Fasting ≥ 95
1-hour ≥ 180
2-hour ≥ 155
3-hour ≥ 140*American Diabetes Association, Carpenter and Coustan.
MEDICAL NUTRITION THERAPY (MNT)
Optimally, a registered dietitian (RD) and/or certified diabetes educator (CDE) should provide MNT, focusing onhealthy food choices and blood glucose control. If this resource is not available in your community, an RN or trainedcommunity health worker may provide nutrition counseling.
Assess
• Individualize the specific calorie level based on an assessment of pre-pregnancy weight (PPW), physical activitylevel, and pregnancy weight gain to date.
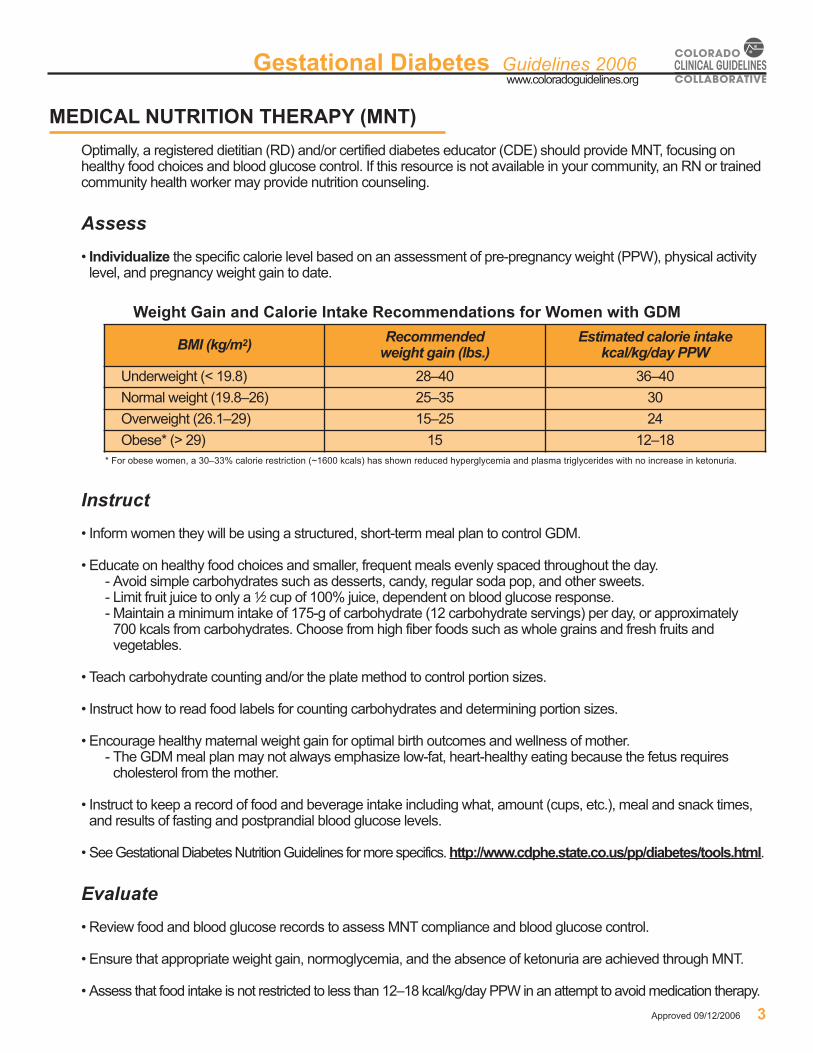
Weight Gain and Calorie Intake Recommendations for Women with GDM
* For obese women, a 30–33% calorie restriction (~1600 kcals) has shown reduced hyperglycemia and plasma triglycerides with no increase in ketonuria.
Instruct
• Inform women they will be using a structured, short-term meal plan to control GDM.
• Educate on healthy food choices and smaller, frequent meals evenly spaced throughout the day.- Avoid simple carbohydrates such as desserts, candy, regular soda pop, and other sweets.- Limit fruit juice to only a 1⁄2 cup of 100% juice, dependent on blood glucose response.- Maintain a minimum intake of 175-g of carbohydrate (12 carbohydrate servings) per day, or approximately700 kcals from carbohydrates. Choose from high fiber foods such as whole grains and fresh fruits andvegetables.
• Teach carbohydrate counting and/or the plate method to control portion sizes.
• Instruct how to read food labels for counting carbohydrates and determining portion sizes.
• Encourage healthy maternal weight gain for optimal birth outcomes and wellness of mother.- The GDM meal plan may not always emphasize low-fat, heart-healthy eating because the fetus requirescholesterol from the mother.
• Instruct to keep a record of food and beverage intake including what, amount (cups, etc.), meal and snack times,and results of fasting and postprandial blood glucose levels.
• See Gestational Diabetes Nutrition Guidelines for more specifics. http://www.cdphe.state.co.us/pp/diabetes/tools.html.
Evaluate
• Review food and blood glucose records to assess MNT compliance and blood glucose control.
• Ensure that appropriate weight gain, normoglycemia, and the absence of ketonuria are achieved through MNT.
• Assess that food intake is not restricted to less than 12–18 kcal/kg/day PPW in an attempt to avoid medication therapy.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
3Approved 09/12/2006
BMI (kg/m2) Recommended weight gain (lbs.)
Estimated calorie intake kcal/kg/day PPW
Underweight (< 19.8) 28–40 36–40
Normal weight (19.8–26) 25–35 30
Overweight (26.1–29) 15–25 24
Obese* (> 29) 15 12–18

PHYSICAL ACTIVITY
• Develop an individualized exercise plan based on a physical assessment by the provider.
• Regular physical activity (30 minutes/day, 5 days/week) has clear benefits, including reduced insulin resistance,reduced postprandial hyperglycemia, and prevention of excessive weight gain.
• Recommend moderate physical activity after meals to achieve postprandial blood glucose goals. This is especiallyeffective following the largest meal of the day.
• Actual heart rate should not exceed 140 beats/minute.
• Ensure adequate hydration and avoid overheating during all physical activity.
• Contraindications to physical activity include: preeclampsia, growth restriction, abruption, placenta previa, orvaginal bleeding.
BLOOD GLUCOSE MONITORING
• Train on self-monitoring of blood glucose (SMBG). Supply with a glucose meter and testing strips, as possible, toensure SMBG throughout pregnancy. A glucose meter with memory is ideal.
• Instruct to check blood glucose 4 times/day; fasting and 1 or 2-hours postprandial.
• Considerations of SMBG:- Postprandial glucose levels peak approximately 90 minutes from time of meal.- Postprandial glucose values are the most effective in determining the likelihood of macrosomia and otheradverse pregnancy outcomes. Daily SMBG may reduce adverse outcomes such as macrosomia.
- SMBG is an essential guide for evaluating MNT.- Continue testing 4 times/day or more throughout the pregnancy if possible.
Self-Monitoring Blood Glucose Goals
• Identify all abnormal values and determine if attributable to diet. If so, adjust or reinforce meal plan.
• When reliable blood glucose values have been collected for a minimum of 1–2 weeks, assess need formedication management. Consider medication therapy if patient is following the prescribed nutrition and physicalactivity plan and:
- 20% of blood glucose values exceed the target goals or;- Two or more elevated blood glucose values taken at the same time of day meet or exceed the target range(e.g. two abnormal fasting values, two abnormal postprandial dinner values).
• If frequency of SMBG is decreased, rotate SMBG with different meals each day.
• Never discontinue SMBG during GDM. Remain vigilant because glucose intolerance increases as pregnancyprogresses.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
4Approved 09/12/2006
Time mg/dl
Fasting < 95
1-hour postprandial < 130–140
2-hour postprandial < 120

MEDICATION MANAGEMENT
• Allow up to two weeks for blood glucose to optimize in response to MNT before prescribing medication.Initiate medication therapy if unsuccessful with MNT.
• For fasting blood glucose > 115 mg/dl begin medication therapy without prior MNT because MNT alone islikely to fail.
Insulin
• Prescribe human insulin.- Insulin Lispro (Humalog) and Aspart (Novolog) more effectively reduce postprandial glycemic excursions thanRegular insulin. However, NPH and Regular have also been used safely in pregnancy.
- Due to insufficient evidence, Glargine (Lantus) is not yet recommended for routine use during pregnancy andis especially discouraged when retinopathy is present. However, there is no evidence that Lantus crosses theplacenta and experience with its use is growing.
• SMBG should guide the doses and timing of the insulin regimen.
• Insulin therapy has shown benefits for pregnancies in which the fetal abdominal circumference (AC) is greaterthan the 75th percentile at 28–33 weeks gestation on ultrasound.
Oral Hypoglycemic Agents
• The FDA has not approved the use of any oral hypoglycemic agents in women with GDM.
• Glyburide has proved successful in recent controlled trials for treatment of hyperglycemia during pregnancy.Glyburide is the only oral hypoglycemic agent that should be considered as an alternative to insulin.
- Glyburide can be an option for individuals refusing insulin.- Glyburide peaks 2–3 hours after meals, therefore the dose should be given 30–60 minutes before breakfastand dinner, and should not be given before bedtime.
- Glyburide is more likely to fail in women who are diagnosed with GDM at < 24 weeks, have significantfasting hyperglycemia (especially >110 mg/dl), are morbidly obese, and have advanced maternal age(age ≥ 35 yrs old).
• Metformin should not be initiated during pregnancy. Unlike Glyburide, Metformin crosses the placenta and there isinadequate data at this time to determine its safety. If used to manage PCOS, discontinue use of Metformin after1st trimester.
• For pre-existing diabetes mellitus controlled by oral hypoglycemic agents, discontinue oral agents and initiateinsulin. The literature remains too weak at this point, especially with thiazolidinediones, to continue use duringpregnancy. Acarbose appears safe, but is usually poorly tolerated due to GI complaints.
PRENATAL SURVEILLANCE
• Initiate daily fetal movement determinations (“kick counts”) at 28 weeks.
• Prenatal surveillance includes a twice-weekly Non-stress Test (NST), weekly Amniotic Fluid Indices (AFI), weeklyBiophysical Profile or Contraction Stress Test.
- If woman is euglycemic with diet only, may delay surveillance until 40 weeks.- If medication therapy is not required, but euglycemia has not been documented, initiate surveillance at36 weeks.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
5Approved 09/12/2006

- If medication therapy is required, initiate surveillance in women with otherwise uncomplicated GDM at32–34 weeks.
- If woman has pre-existing diabetes, evidence of growth abnormalities, abnormal amniotic fluid levels,hypertension, or other adverse obstetric history, consider earlier surveillance.
• Using a fetal based strategy (AC > 75th %ile at 28–33 weeks) to guide therapy may help identify women that maybenefit from more intensive medical management.
• Selection of the prenatal test, whether NST, AFI, Biophysical Profile, or Contraction Stress Test, is at the discretionof the practitioner.
LABOR AND DELIVERY MANAGEMENT
• Do a clinical or ultrasound estimate of fetal weight (EFW) within 2 weeks of delivery.
• Timing of delivery remains relatively open. There is no data to support delivery prior to term or cesarean deliverypurely on the basis of GDM.
- Well-controlled GDM pregnancies on MNT have little indication for delivery prior to 38–39 weeks gestation.Delivery at ~39 weeks gestation has been shown to decrease macrosomia in women with good dating criteriaand a favorable cervix.
- Consider fetal lung maturity documentation by amniocentesis in women undergoing induction of labor orcesarean delivery prior to 38 weeks.
• Counsel all women regarding possible cesarean delivery.
• To determine mode of delivery when EFW is 4,000–4,500-g, consider past delivery history, clinical pelvimetry,evidence of body to head disproportion (fetal AC three weeks ahead of biparietal diameter measurement onultrasound), and progression of labor.
• Manage as a high-risk delivery if woman has poor glycemic control, hypertensive disorder, or previous stillbirth.
POSTPARTUM FOLLOW-UP
Immediately Postpartum
• It is crucial women return to their provider to receive the appropriate postpartum counseling, testing, and follow-upafter delivery. All women following GDM pregnancies have an approximate 50% risk for developing type 2diabetes within the next 5–10 years and ~80% if they have impaired fasting glucose (IFG) or impaired glucosetolerance (IGT) postpartum.
• Encourage breastfeeding, emphasizing the following benefits:- May decrease maternal progression to type 2 diabetes.- Reduces insulin resistance in mothers.- Promotes weight loss for the mother.
• Encourage women to aim for their pre-pregnancy weight 6 to 12 months after the baby is born. Then, ifoverweight, work to lose at least 5 to 7 percent (10 to 14 pounds for someone who weighs 200 pounds) of bodyweight slowly, over time, and keep it off.
• Educate on lifestyle modifications to lessen insulin resistance and prevent or delay the onset of type 2 diabetes.
• Schedule a follow-up 75-g, 2-hour oral glucose tolerance test (OGTT) in 6–12 weeks.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
6Approved 09/12/2006

6–12 Weeks Postpartum
• Perform a 75-g, 2-hour OGTT for reclassification of maternal glycemic status.
Reclassification Criteria for Postpartum Maternal Glycemic Status*
* American Diabetes Association criteria
- If glucose levels are normal following 2-hour OGTT, reassess glycemia at a minimum of 1–3 year intervals.- If fasting or 2-hour values reflect diagnosis of pre-diabetes (IFG or IGT), test for diabetes annually. Refer to aprimary care physician, advise to continue MNT, and follow an individualized exercise program. Women withpre-diabetes have ~17% risk per year of developing type 2 diabetes.
- If fasting or 2-hour values reflect diagnosis of type 2 diabetes, refer to providers for diabetes self-managementskills; PCP, CDE or nurse for SMBG education, RD, social worker, pharmacist, exercise physiologist, trainedcommunity health worker.
• Include contraceptive education to ensure optimal glycemic regulation from the start of any subsequentpregnancy. Given ~50% of pregnancies are unplanned in women with a history of gestational diabetes, womenshould be using adequate contraception starting 6–12 weeks postpartum.
- Combined estrogen and progesterone containing oral contraceptives do not appear to cause significanteffects on glucose metabolism, but should not be given to women with elevated triglycerides.
- Depo-Provera has been associated with an increased likelihood of weight gain and glucose intolerance;therefore postpartum weight loss and maintaining a healthy weight should be stressed.
- Intrauterine devices have not been shown to cause an increased risk of infection in women with a history ofGDM and may be a highly effective method for some women.
• It is critical that children born to women with GDM be followed closely for the development of obesity and/orabnormalities of glucose tolerance. Counsel on the importance of a healthy lifestyle for their newborn child andother family members as well.
PRE-EXISTING DIABETES MELLITUS
The management of pre-existing diabetes is beyond the scope of this document, however the following highlightssome of the important steps to take preconception and initially once a woman has entered into prenatal care.
Preconception
Diabetes and its coexisting medical complications may result in adverse maternal medical and obstetricaloutcomes. Therefore all women with diabetes should have preconception counseling, which addresses bothobstetrical and medical considerations.
• Counsel on the importance of near normal blood glucose control prior to conception (HbA1c < 6.5 %).Preconception euglycemia decreases the risk of both miscarriage and congenital anomalies to levels near equalto normal pregnancies. Document euglycemia by HbA1c and SMBG monitoring in the 3–6 months prior toconception.
• Discontinue statins, ace inhibitors and angiotensin receptor blockers prior to conception due to possibleadverse effects.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
7Approved 09/12/2006
Time Normoglycemia Pre-diabetes Type 2 Diabetes Mellitus
Fasting < 100 mg/dl ≥ 100 mg/dl and < 126 mg/dlImpaired Fasting Glucose (IFG) ≥ 126 mg/dl
2-hour < 140 mg/dl ≥ 140 mg/dl and < 200 mg/dlImpaired Glucose Tolerance (IGT) ≥ 200 mg/dl

• Ascertain that proliferative retinopathy is in remission or controlled before conception.
• Recommend that women actively trying to become pregnant discontinue oral agents and initiate insulin to achieveoptimal glycemic control before becoming pregnant.
• Recommend at least 1 mg folic acid supplements daily prior to conception to help prevent birth defects.
Prenatal
Due to the significant risk for adverse pregnancy outcomes without appropriate therapy and surveillance, includingintrauterine fetal death and severe maternal preeclampsia, women with pre-existing diabetes should see a high-riskobstetric specialist and endocrinologist for high-risk management throughout the pregnancy, whenever possible.The following recommendations are not extensive, and should not be considered the only source when managingpre-existing diabetes in pregnancy.
• Obtain an HbA1c test at first prenatal visit and every 12 weeks throughout pregnancy. Decreasing the HbA1c to< 7.0% is the goal (< 6.5% is optimal) and often requires intensive, flexible insulin regimens based on both pre-meal and post-meal glucose testing, and initiation of carbohydrate/insulin ratios and correction factors.
• Discontinue oral agents at first prenatal visit and initiate insulin, with the understanding that insulin requirementsoften decrease in the first trimester placing the mother at risk for nocturnal hypoglycemia and frequently increaseby 2–3 fold in the late 2nd and 3rd trimester.
• Continue SMBG 4–10 times/day especially in women on intensive, flexible insulin regimens and in women withtype 1 diabetes and hypoglycemic unawareness.
• Continue MNT and counsel on healthy maternal weight gain. Weight gain often does not need any restriction inwomen with type 1 diabetes who are at or below ideal body weight.
• Refer to an ophthalmologist in the first trimester, and then as needed.
• Obtain baseline preeclampsia labs and monitor for evidence of increasing proteinuria with 12 to 24-hour urines inwomen with proteinuric renal disease.
• Monitor mother for complications such as worsening renal disease, gastroparesis, progressive retinopathy, and forthe development of preeclampsia. Understand that DKA can occur in women with type 2 diabetes as well aswomen with type 1 diabetes with glucose values < 200 mg/dl.
• Monitor the fetus for evidence of growth restriction from placental insufficiency, large for gestational age due toinadequately treated diabetes and/or obesity, major malformations, fetal distress and consider earlier delivery,especially for fetuses at risk for intrauterine fetal demise. Initiate fetal activity records at 28 weeks and fetalsurveillance at 30–32 weeks in all women with pre-existing diabetes.
• Manage labor and delivery using an IV insulin drip to keep mother’s glucose 100–150 mg/dl to avoid neonatalhypoglycemia. Decrease mother’s insulin dose to pre-pregnancy levels (or lower) immediately after delivery.
These clinical guidelines (approved 9/12/2006) are adapted from the American Diabetes Association (ADA) Standards of Medical Carein Diabetes—2006. They are designed to assist clinicians in managing women with gestational diabetes and are not intended toreplace a clinician’s judgment or establish a protocol for all women with gestational diabetes. For references, important updates, oradditional copies of guidelines, go to http://www.coloradoguidelines.org or call 720-297-1681 or 1-866-401-2092.
Gestational Diabetes Guidelines 2006www.coloradoguidelines.org
8Approved 09/12/2006

* American Diabetes Association, Carpenter and Coustan criteria.
GUIDELINES FOR GESTATIONAL DIABETES (GDM)GUIDELINES FOR GESTATIONAL DIABETES (GDM)SCREENING AND DIAGNOSISSCREENING AND DIAGNOSIS
First Prenatal Encounter:Universal Risk Assessment
High-risk if any of the following:• Advanced maternal age (> 35 y.o.)• Obese (BMI > 29 kg/m2 based on ppw).• High-risk ethnic population.• h/o GDM.• Previous macrosomic infant. • h/o GDM related OB complications. • First degree relative w/ diabetes.• PCOS.• Glycosuria.
High-risk: Screen immediately with 50-g, 1-hour OGCT• ≥ 135 mg/dl, follow with 100-g, 3-hour OGTT. If suspect pre-existing diabetes, order HbA1c. • < 135 mg/dl, rescreen between 24–28 weeks.
Not high-risk: Follow-up with universal screening between 24–28 weeks.
24–28 Weeks:Universal Screening
Test using 50-g, 1-hour OGCT• ≥ 135 mg/dl, follow with 100-g, 3-hour OGTT.• < 135 mg/dl, no further testing required.See reverse for GDM Screening & Diagnosis Algorithm
• Educate on healthy food choices and smaller, frequent meals throughout the day.• Teach portion control (plate method or carbohydrate counting) and reading food labels.• Refer to an RD or CDE if available, or an RN or trained community health worker.
• Record food and beverage intake including what, amount (cups, etc.), and meal and snack times.
• Recommend regular physical activity 30 min/day, 5 days/week.• Consult with MD re: any contraindications.
• Glyburide is the only oral hypoglycemic agent that may be considered as an alternative to insulin.• Metformin should not be initiated in pregnancy. If used to manage PCOS risks, discontinue after 1st trimester.
• Use SMBG to guide the doses and timing of the insulin regimen.• Aspart and Lispro are the most effective at reducing postprandial glycemic excursions.• Regular and NPH have also been used safely in pregnancy.
• Euglycemic: initiate surveillance at 40 weeks.• Not euglycemic: initiate surveillance at 36 weeks.
• If pregnancy is not otherwise complicated, initiate surveillance at 32–34 weeks.
• There is no data to support delivery at < 38 wks or cesarean delivery purely on the basis of GDM.
POSTPARTUM FOLLOW-UPPOSTPARTUM FOLLOW-UP
Due to the increased risk of developing type 2 diabetes, it is crucialcrucial that women return to their provider to receive the appropriate postpartum counseling, testing, and follow-up after a GDM pregnancy. See reverse for GDM Postpartum Algorithm.
Self-MonitoringBlood Glucose Goals
Time mg/dlFasting ≥ 951-hour ≥ 1802-hour ≥ 1553-hour ≥ 140
www.coloradoguidelines.org
Time mg/dlFasting < 951-hour pp < 130–1402-hour pp < 120
(OGCT = Oral Glucose Challenge Test, 1-hour OGTT = Oral Glucose Tolerance Test, 3-hour)
OGTT Diagnostic Criteria for Gestational Diabetes*
If 2 or more values meet or exceed thresholds, diagnose GDM.
Note: If only 1 value meets or exceeds thresholds, re-test in 3-4 wks. using OGTT.
Meal Planning
Food Record
Physical Activity
Oral
Insulin
• A fetal based strategy (AC > 75th%ile at 28–33 weeks) may help identify women that may benefit from more intensive medical management.• Prenatal surveillance may include NST, AFI, Biophysical Profile or Contraction Stress Test. Selection of the prenatal test is at the discretion of the practitioner.
Surveillance
Diet Controlled**
Medication Controlled
Delivery
These clinical guidelines (approved 9/12/2006) are adapted from the American Diabetes Association (ADA) Standards of Medical Care in Diabetes—2006. They are designed to assist clinicians in managing women with gestational diabetes and are not intended to replace a clinician’s judgment or establish a protocol for all women with gestational diabetes. For references, important updates, additional copies of guidelines, go to http://www.coloradoguidelines.org or call 720-297-1681 or 1-866-401-2092.
MEDICAL NUTRITION THERAPY (MNT) AND PHYSICAL ACTIVITY**MEDICAL NUTRITION THERAPY (MNT) AND PHYSICAL ACTIVITY**
BLOOD GLUCOSE MONITORINGBLOOD GLUCOSE MONITORING
MEDICATION MANAGEMENTMEDICATION MANAGEMENT
PRENATAL SURVEILLANCE and DELIVERY MANAGEMENTPRENATAL SURVEILLANCE and DELIVERY MANAGEMENT
** For more specific GDM nutrition information, visit the Gestational Diabetes Nutrition Guidelines at http://www.cdphe.state.co.us/pp/diabetes/tools.html.
• Check and record BG 4x/day; fasting and 1 or 2-hours postprandial (pp) for a minimum of 2 weeks.
• Never discontinue SMBG during GDM. Remain vigilant as glucose intolerance increases as pregnancy progresses. If frequency is decreased, rotate SMBG at different meals each day.
• If 20% of BG values exceed the target while following prescribed nutrition and physical activity plan, consider medication therapy.

Tim
e
Fast
ing
< 1
00 m
g/dl
Nor
mog
lyce
mia
< 1
40 m
g/dl
2-ho
ur
Ges
tatio
nal D
iabe
tes
Post
part
um F
ollo
w-u
p
Wom
en w
ith G
DM
hav
e an
app
roxi
mat
e 50
% r
isk
for
deve
lopi
ng
type
2 d
iabe
tes
with
in th
e ne
xt 5
–10
year
s an
d 80
% r
isk
if th
ey
have
impa
ired
fast
ing
gluc
ose
or im
pair
ed g
luco
se to
lera
nce
post
part
um.
Ther
efor
e it
is c
ruci
al th
ey r
etur
n to
thei
r pr
ovid
er to
rec
eive
the
appr
opri
ate
post
part
um c
ouns
elin
g, te
stin
g, a
nd fo
llow
-up
afte
r a
GD
M p
regn
ancy
.
Nor
mog
lyce
mia
Nor
mog
lyce
mia
Pre
-dia
bete
sP
re-d
iab
ete
s(I
FG
ot
IGT
)(I
FG
ot
IGT
)Ty
pe 2
Dia
bete
s M
ellit
usTy
pe 2
Dia
bete
s M
ellit
us
Ref
er to
pro
vide
rs
for d
iabe
tes
self-
man
agem
ent
educ
atio
n an
d tre
atm
ent.
• Te
st b
lood
glu
cose
for
di
abet
es a
nnua
lly.
• R
efer
to p
rimar
y ca
re
phys
icia
n.•
Adv
ise
to c
ontin
ue M
NT.
• En
cour
age
phys
ical
ac
tivity
.
Rea
sses
s gl
ycem
ia a
t m
inim
um
of 1
–3 y
r. in
terv
als.
• En
cour
age
lifes
tyle
mod
ifica
tions
to im
prov
e in
sulin
resi
stan
ce, m
aint
ain
norm
al
bo
dy w
eigh
t, m
ake
heal
thy
food
cho
ices
, inc
reas
e ph
ysic
al a
ctiv
ity.
• R
ecom
men
d br
east
feed
ing
as it
may
dec
reas
e m
ater
nal p
rogr
essi
on to
type
2
di
abet
es fo
llow
ing
a G
DM
pre
gnan
cy.
• Ed
ucat
e on
effe
ctiv
e co
ntra
cept
ion
and
the
need
for p
reco
ncep
tion
coun
selin
g
and
eval
uatio
n be
fore
futu
re p
regn
anci
es.
• Em
phas
ize
impo
rtanc
e of
a h
ealth
y lif
esty
le in
chi
ldre
n bo
rn to
wom
en w
ith G
DM
.
- Mon
itor f
or d
evel
opm
ent o
f obe
sity
and
/or g
luco
se in
tole
ranc
e.
- Enc
oura
ge d
aily
phy
sica
l act
ivity
.
- Tea
ch a
nd m
odel
hea
lthy
eatin
g ha
bits
.
Po
stp
artu
m e
du
cati
on
for
all w
om
en w
ith
pri
or
GD
M:
Po
stp
artu
m e
du
cati
on
for
all w
om
en w
ith
pri
or
GD
M:
Rec
lass
ific
atio
n C
rite
ria
for
Po
stp
artu
m M
ater
nal
Gly
cem
ic S
tatu
sR
ecla
ssif
icat
ion
Cri
teri
a fo
r P
ost
par
tum
Mat
ern
al G
lyce
mic
Sta
tus
Ges
tatio
nal D
iabe
tes
Scre
enin
g an
d D
iagn
osis
Un
iver
sal S
cree
nin
gU
niv
ersa
l Scr
een
ing
24–2
8 w
ks. g
esta
tion
50-g
, 1-h
our O
GC
T
NO
NO
YE
SY
ES
If O
GC
T ≥
200
mg/
dl,
test
ser
um fa
stin
g bl
ood
gluc
ose
(FB
G)
befo
re 1
00-g
, 3-h
our O
GTT
.
If se
rum
FB
G <
95
mg/
dl,
proc
eed
with
OG
TT.
If se
rum
FB
G ≥
95
mg/
dl, w
oman
ha
s G
DM
. No
OG
TT n
eces
sary
.
No
abno
rmal
val
ues
No
abno
rmal
val
ues
1 ab
norm
al v
alue
1 ab
norm
al v
alue
2 or
mor
e ab
norm
al v
alue
s2
or m
ore
abno
rmal
val
ues
Rec
omm
end
phys
ical
act
ivity
and
nutri
tion
coun
selin
g.
1 Se
e Sc
reen
ing
sect
ion
in G
esta
tiona
l Dia
bete
s G
uide
lines
2 A
mer
ican
Dia
bete
s A
ssoc
iatio
n, C
arpe
nter
and
Cou
stan
Wom
an h
as G
DM
Wom
an h
as G
DM
≥ 12
6 m
g/dl
≥ 10
0 m
g/dl
and
< 1
26 m
g/dl
Im
paire
d Fa
stin
g G
luco
se (I
FG)
Type
2 D
iabe
tes
Mel
litus
Pre
-dia
bete
s
≥ 20
0 m
g/dl
≥ 14
0 m
g/dl
and
< 2
00 m
g/dl
Im
paire
d G
luco
se T
oler
ance
(IG
T)
If O
GTT
bet
wee
n24
–28
wks
,re
pea
t10
0-g
, 3-h
our
OG
TT in
3–4
wks
.
If te
stin
g do
ne p
rior t
o 24
wks
an
d su
spec
t pre
-exi
stin
g di
abet
es,
orde
r HbA
1c.
100-
g, 3
-hou
r OG
TTD
iagn
ostic
Crit
eria
FBG
≥ 9
5 m
g/dl
1-ho
ur ≥
180
mg/
dl2-
hour
≥ 1
55 m
g/dl
3-ho
ur ≥
140
mg/
dl
2
If O
GTT
prio
r to
24 w
ks,
resc
reen
bet
wee
n24
–28
wks
.
If O
GTT
bet
wee
n24
–28
wks
, no
furt
her t
estin
gre
qui
red
.
If O
GTT
prio
r to
24 w
ks,
resc
reen
bet
wee
n24
–28
wks
.
Un
iver
sal R
isk
Ass
essm
ent
Un
iver
sal R
isk
Ass
essm
ent
Firs
t Pre
nata
l Enc
ount
er
Hig
h-R
isk
50-g
, 1-h
our O
GC
T
OG
CT ≥
135
mg/
dl
Not
Hig
h-R
isk1
OG
CT ≥
135
mg/
dlN
ON
OS
TOP
STO
P
- Beg
in S
MB
G, M
NT,
and
p
hysi
cal a
ctiv
ity.
- Ref
er to
RD
or C
DE
if a
vaila
ble;
or R
N o
r tra
ined
c
omm
unity
hea
lth w
orke
r f
or e
duca
tion.
- Ref
er to
end
ocrin
olog
ist
(op
tiona
l).
6-12
Wee
ks P
ost
par
tum
6-12
Wee
ks P
ost
par
tum
75-g
, 2-h
our O
GTT
with
fast
ing
and
2-ho
ur re
sults