gestational trophoblastic disease (gtd) department of obs. & gyn., first hospital of xi ’ an...
TRANSCRIPT
Gestational Trophoblastic Gestational Trophoblastic Disease (GTD)Disease (GTD)
Department of Obs.Department of Obs.&& Gyn., First Gyn., First Hospital of Xi’an Jiaotong UnivHospital of Xi’an Jiaotong Univ
ersity ersity
Gao Shang FengGao Shang Feng

IntroductionIntroduction What is GTD ?What is GTD ? It is a rare kind of disease in which abnorIt is a rare kind of disease in which abnor
mal trophoblastic proliferation occurs.mal trophoblastic proliferation occurs. It is too among the rare human malignaIt is too among the rare human maligna
ncies that can be cured even in the presencies that can be cured even in the presence of widespread metastases.nce of widespread metastases.

Which does it include?Which does it include? It includes a spectrum of interrelated tuIt includes a spectrum of interrelated tumors, includingmors, including hydatidiform mole (HM)hydatidiform mole (HM) invasive mole (IM)invasive mole (IM) Choriocarcinoma (CH)Choriocarcinoma (CH) Placental-site trophoblastic tumor (PSTT,Placental-site trophoblastic tumor (PSTT, borderline, very rare) borderline, very rare)

Relationship of HM. IM. CH Relationship of HM. IM. CH
hydatidiform therapeutic or hydatidiform therapeutic or molemole spontaneous abortionspontaneous abortion term pregnancyterm pregnancy ectopicectopic
invasion mole choriocarcinoma.invasion mole choriocarcinoma.
What is GTT (Gestational trophoblastic tuWhat is GTT (Gestational trophoblastic tumor)?mor)?
GTT is all GTD GTT is all GTD except hydatidiform mole.except hydatidiform mole.They has its unique pathologic characterisThey has its unique pathologic characteris
tics and biological behavior.tics and biological behavior.Even the most malignant case can be cureEven the most malignant case can be cure
d by chemotherapy.d by chemotherapy.

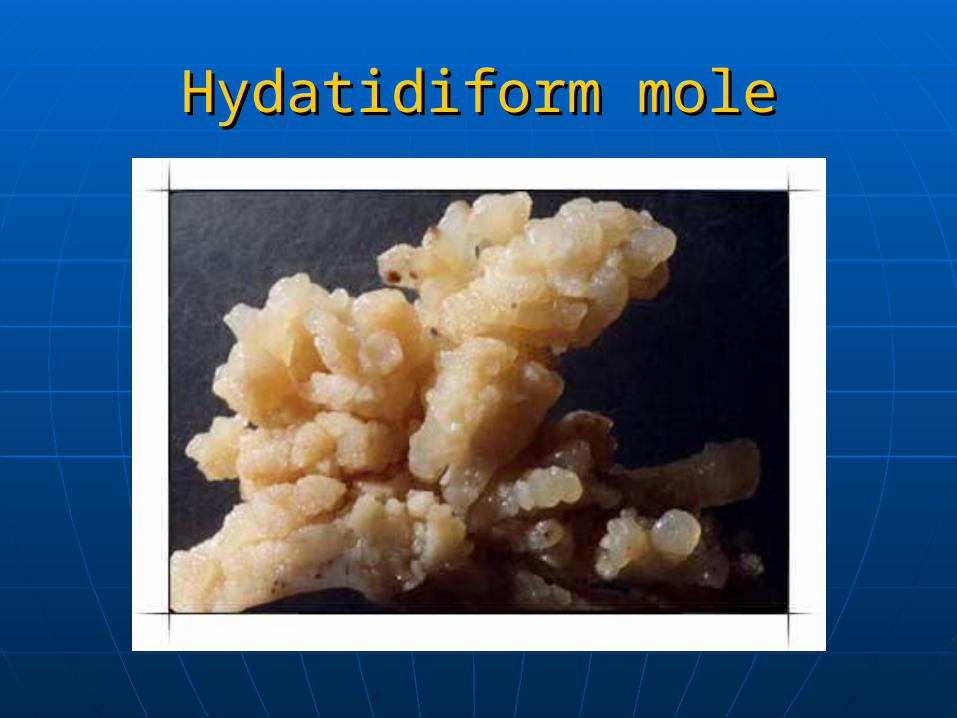
Hydatidiform moleHydatidiform mole
Hydatidiform moleHydatidiform mole

Hydatidiform moleHydatidiform mole
It is a neoplastic pIt is a neoplastic proliferation of throliferation of the trophoblast in e trophoblast in which the which the termiterminal villinal villi are trans are transformed into vesiformed into vesicles filled with clcles filled with clear viscid materiear viscid material.al.
It is usually benign but has malignant It is usually benign but has malignant potentiality.potentiality.
Incidence:Incidence: south east Asiasouth east Asia is 1/500-600 is 1/500-600 the US and Europe:1/500-2000 the US and Europe:1/500-2000 China:China:1/12381/1238
ClassificationClassification
It is divided into two classificationIt is divided into two classification
complete hydatidiform mole complete hydatidiform mole partial hydatidiform mole partial hydatidiform mole

complete hydatidiform mole(CHM):complete hydatidiform mole(CHM):
the entire the entire uterus uterus filled with filled with abnormal abnormal vesicles, no vesicles, no signs of signs of fetus.fetus.

partial hydatidiform molepartial hydatidiform mole
partial hydatipartial hydatidiform mole diform mole with evidence with evidence of a conceptuof a conceptus.s.

EtiologyEtiology
Though it is not known a number of Though it is not known a number of associated factors have been noted: associated factors have been noted:
the absence of fetal circulation;the absence of fetal circulation;
dietary protein deficiencydietary protein deficiency
viral infection;viral infection;
age:>45 years women are 10 times age:>45 years women are 10 times more likely to develop HM than more likely to develop HM than those youngerthose younger

abnormal fertilization process:abnormal fertilization process:
the fertilization of a normal ovum the fertilization of a normal ovum with a duplicated haploid with a duplicated haploid sperm:46XXsperm:46XX
the fertilization of an empty egg by the fertilization of an empty egg by two sperms(dispermy):46XYtwo sperms(dispermy):46XY
ChromosomesChromosomes
complete hydatidiform molescomplete hydatidiform moles Cytogenetic studies have demonstrated that cCytogenetic studies have demonstrated that c
omplete hydatidiform moles usually have a 46omplete hydatidiform moles usually have a 46xx karyotype, and the molar chromosomes are xx karyotype, and the molar chromosomes are entirely of paternal origin.entirely of paternal origin.
Complete moles appear to arise from an ovum Complete moles appear to arise from an ovum that has been fertilized by a haploid sperm, wthat has been fertilized by a haploid sperm, which then duplicates its own chromosomes, anhich then duplicates its own chromosomes, and the ovum nucleus may be either absent or ind the ovum nucleus may be either absent or inactivated activated

Although most complete moles have a 4Although most complete moles have a 46xx chromosomal pattern, approximatel6xx chromosomal pattern, approximately 10% have a 46xy karyotype. y 10% have a 46xy karyotype. Chromosomes in a 46xy complete mole Chromosomes in a 46xy complete mole also appear to be entirely of paternal orialso appear to be entirely of paternal origin, but in this circumstance, an apparegin, but in this circumstance, an apparently empty egg is fertilized by two sperm.ntly empty egg is fertilized by two sperm.

..
partial hydatidiform molepartial hydatidiform mole partial moles usually have a triploid karyotyppartial moles usually have a triploid karyotype (69 chromosomes ), with the extra haploid see (69 chromosomes ), with the extra haploid set of chromosomes derived from the father.t of chromosomes derived from the father. When a fetus is present in conjunction with a When a fetus is present in conjunction with a partial mole, it usually exhibits the stigmata of partial mole, it usually exhibits the stigmata of triploidy, including growth retardation and mutriploidy, including growth retardation and multiple congenital malformations.ltiple congenital malformations.

Pathologic findingsPathologic findings

complete hydatidiform molecomplete hydatidiform mole
pathology pathology Complete moles lack identifiable emComplete moles lack identifiable em
bryonic or fetal tissues, and the chorbryonic or fetal tissues, and the chorionic villi exhibit generalized hydatidionic villi exhibit generalized hydatidiform swelling and diffuse trophoblaiform swelling and diffuse trophoblastic hyperplasia.stic hyperplasia.

GrossGross
we see a mass of we see a mass of vesicles, vary in vesicles, vary in size, grape-like size, grape-like with stems, blood with stems, blood and clot filling the and clot filling the inter-vesicle spaceinter-vesicle space
partial hydatidiform molepartial hydatidiform mole
It are characterized by the following pathoIt are characterized by the following pathologic features :logic features : Chorionic villi if varying size with focal hChorionic villi if varying size with focal hydatidiform swelling and cavitation. ydatidiform swelling and cavitation. It contain identifiable embryonic or fetaIt contain identifiable embryonic or fetal tissues.l tissues.

GrossGross
we see a we see a mass of mass of vesicles, vesicles, vary in size, vary in size, grape-like grape-like and and identifiable identifiable embryonic embryonic or fetal or fetal tissues.tissues.

MicroscopicMicroscopic
trophoblastic proliferation. trophoblastic proliferation. hydropic degeneration of the sthydropic degeneration of the stroma.roma. absence of blood vessels or extabsence of blood vessels or extreme scantiness of blood vesselreme scantiness of blood vessels.s.
‘

Normaltrophoblastictrophoblastic
partial hydatidiform
partial hydatidiform
molemole
complete hydaticomplete hydatidiform mole
diform mole

trophoblastic proliferation is considered trophoblastic proliferation is considered the the most important single criteria.most important single criteria.
Ovaries respond to hCG stimulation ,30-Ovaries respond to hCG stimulation ,30-50% theca-lutein cysts develop, bilateral50% theca-lutein cysts develop, bilateral
Clinical courseClinical course
It has It has eight eight of of symptoms and symptoms and physical signs.physical signs.

amenorrhea amenorrhea
because it is a pregnancy.because it is a pregnancy. vaginal bleedingvaginal bleeding
after a period of amenorrhea after a period of amenorrhea (average 12 weeks) may continue (average 12 weeks) may continue intermittently for several weeks---intermittently for several weeks---profuse bleeding---anemia and profuse bleeding---anemia and infection. infection.
abdominal crampsabdominal cramps

abnormally abnormally enlarged and enlarged and soft uterussoft uterus
in about half the in about half the cases, the uterus cases, the uterus growth is rapid, growth is rapid, it is larger than it is larger than the dates the dates suggest.suggest.

ovarian cyst torsionovarian cyst torsion when we do pelvic exawhen we do pelvic exa
mination adnexal mamination adnexal masses may be found. it sses may be found. it is theca lutein cyst in is theca lutein cyst in about one third of thabout one third of the casese cases
severe and early –onset PIHsevere and early –onset PIH (Pregnancy Induced Hypertension (Pregnancy Induced Hypertension syndrome)syndrome)
hyperthyroidismhyperthyroidism plasma thyroxin concentration plasma thyroxin concentration
elevateselevates exaggerated early pregnancy exaggerated early pregnancy
symptomssymptoms nausea, vomit etcnausea, vomit etc

DiagnosisDiagnosis
suspicion:suspicion: abnormal bleeding after amenorrheaabnormal bleeding after amenorrhea inappropriately enlarged uterus; inappropriately enlarged uterus; absence of fetal heart sounds or could nabsence of fetal heart sounds or could not feel fetal parts by palpation between ot feel fetal parts by palpation between 16-2016-20thth week week hyperemesis gravidarumhyperemesis gravidarum bilateral ovarian cystsbilateral ovarian cysts
serum hCG monitorserum hCG monitor an unusually high titer of chorionic gonan unusually high titer of chorionic gon
adotropin, especially after the one-hundadotropin, especially after the one-hundredth day of pregnancy, help to confirm redth day of pregnancy, help to confirm the diagnosis of HM.the diagnosis of HM.
Ultrasonography:Ultrasonography: It is a reliable and sensitive technique for tIt is a reliable and sensitive technique for t
he diagnosis of complete molar pregnanche diagnosis of complete molar pregnancy. Because the chorionic villi exhibit diffuy. Because the chorionic villi exhibit diffuse hydatidiform swelling. Complete molese hydatidiform swelling. Complete moles produce a characteristic vesicular sonos produce a characteristic vesicular sonographic pattern, usually referred to as a graphic pattern, usually referred to as a ““snowstormsnowstorm” pattern.” pattern.

Ultrasonography may also contributUltrasonography may also contribute to the diagnosis of partial molar pe to the diagnosis of partial molar pregnancy by demonstrating focal cyregnancy by demonstrating focal cystic spaces in the placental tissues astic spaces in the placental tissues and an increase in the transverse diand an increase in the transverse diameter of the gestational sac.meter of the gestational sac.
Differential diagnosisDifferential diagnosis
abortion;abortion;
multiple pregnancy;multiple pregnancy;
polyhydramniospolyhydramnios

TreatmentTreatment
the uterus should be evacuated as soon the uterus should be evacuated as soon as possible after the diagnosis is made.as possible after the diagnosis is made.(by suction curettage)(by suction curettage) suction;suction; oxytocin administration:we can use blooxytocin administration:we can use blood transfusion or/and fluid infusion.it is od transfusion or/and fluid infusion.it is used to decrease the size of the uterus;used to decrease the size of the uterus;

tissue sent for histology: it tissue sent for histology: it should be routine practice should be routine practice with all cases of with all cases of incomplete miscarriage;incomplete miscarriage;
acute pulmonary acute pulmonary complicationscomplications

total abdominal total abdominal hysterectomyhysterectomyin older multiparas in older multiparas hysterectomy may hysterectomy may be indicated.be indicated.

management of theca-lutein cymanagement of theca-lutein cystssts
these tumors should not be excithese tumors should not be excised because they regress after sed because they regress after the trophoblastic tissue has bethe trophoblastic tissue has been removed.en removed.

chemotherapy chemotherapy
HM don’t need usually HM don’t need usually chemotherapy because chemotherapy because HM is benign disease.HM is benign disease.

㈧㈧ Follow-up examinationsFollow-up examinations
follow up mode in the 2 follow up mode in the 2
years after dischargeyears after discharge
on each follow-up on each follow-up
check, the following check, the following
should be addressedshould be addressed
symptomsymptom abnormal abnormal vaginal bleeding,vaginal bleeding, cough, hemoptysiscough, hemoptysis signs of metastasissigns of metastasis pelvic examinationpelvic examination hCG evaluation hCG evaluation B-ultrasound B-ultrasound chest X-ray filmchest X-ray film

contraceptive method contraceptive method
required for 1-2 yearsrequired for 1-2 years condom is recommended. condom is recommended. IUD (intrauterine device)and pills IUD (intrauterine device)and pills
are contraindicated for their are contraindicated for their potentiality of causing abnormal potentiality of causing abnormal vaginal bleeding.vaginal bleeding.
Ask questionAsk question
1.1. What is the etiology of GTD?What is the etiology of GTD?2.2. What is the classification of HM?What is the classification of HM?3.3. What is What is the main pathologic the main pathologic
changes of HM?changes of HM?4.4. What is the clinical course of What is the clinical course of
HM?HM?5.5. How Follow-up examinations is How Follow-up examinations is
we? we?

About 80% of the cases of HM have About 80% of the cases of HM have a benign course. one-half of patienta benign course. one-half of patients become pregnant subsequently. as become pregnant subsequently. about 16% of HM become invasion mbout 16% of HM become invasion moles and some 2.5% progress intooles and some 2.5% progress into cchoriocarcinomahoriocarcinoma

Invasion MoleInvasion Mole
IntroductionIntroduction
Invasion MoleInvasion Mole arises from HM arises from HM it has malignant potentialities, invait has malignant potentialities, inva
des the myometrium and penetratedes the myometrium and penetrates the uterine wall, extends into the bs the uterine wall, extends into the broad ligament or peritoneal cavity.road ligament or peritoneal cavity.
in half or more of all cases in half or more of all cases invasive mole metastasizes invasive mole metastasizes through the peripheral through the peripheral circulation to distant sites, circulation to distant sites, mostly to the lung.mostly to the lung.

Pathologic findingsPathologic findings
excessive trophoblastic prolifeexcessive trophoblastic proliferation and invasivenessration and invasiveness
the degree of anaplasia is varithe degree of anaplasia is variable: completely benign---highable: completely benign---highly malignantly malignant
differentiation between invasive modifferentiation between invasive mole and choriocarcinoma lies in whetle and choriocarcinoma lies in whether the villous pattern is preserved: her the villous pattern is preserved:
if we see villi, it must be invasion mif we see villi, it must be invasion mole; ole;
if we can’t see villi, it is choriocarciif we can’t see villi, it is choriocarcinoma.noma.
Clinical courseClinical course
Symptoms caused by primary lesionsSymptoms caused by primary lesionsvaginal bleedingvaginal bleeding
pelvic examination reveals delayed pelvic examination reveals delayed involution of the uterus, persisting involution of the uterus, persisting cyst .cyst .
abdominal painabdominal pain
intra-abdominal hemorrhage, intra-abdominal hemorrhage, penetration of the uterus .penetration of the uterus .

Metastatic symptomsMetastatic symptoms• cough, hemoptysis---positive X-ray sigcough, hemoptysis---positive X-ray sig
nsns• profuse vaginal bleeding---vaginal or cprofuse vaginal bleeding---vaginal or c
ervical metastasis, we can see ervical metastasis, we can see bluish nbluish noduleodule in vaginal in vaginal
• headache, nausea, vomit, paralysis or headache, nausea, vomit, paralysis or coma—it is caused by cerebral lesion.coma—it is caused by cerebral lesion.
DiagnosisDiagnosis
history and clinical manifestationhistory and clinical manifestation hCG assay:hCG assay:diagnosis suspected if hCG titers pediagnosis suspected if hCG titers persist to be high 12 weeks after evacursist to be high 12 weeks after evacuation of a HM, or once regress to noration of a HM, or once regress to normal range but rise rapidly.mal range but rise rapidly.

possible reasons : retained HMpossible reasons : retained HMpregnancypregnancyhuge theca-lutein cyst persisthuge theca-lutein cyst persistwhen we remove these reasons we cwhen we remove these reasons we can diagnosis invasive molean diagnosis invasive moleother measurementother measurementB-ultrasoundB-ultrasoundX-rayX-ray

ProphylaxisProphylaxis
respond well to chemotherapeutic respond well to chemotherapeutic agentsagents
main causes of death:main causes of death: hemorrhage, metastasis and hemorrhage, metastasis and infection infection
Treatment:Treatment:
Identical to that for chIdentical to that for choriocarcinomaoriocarcinoma
Choriocarcinoma Choriocarcinoma
It is highly malignant GTTIt is highly malignant GTT It may follow HM, invasion mIt may follow HM, invasion mole, abortion, normal pregnaole, abortion, normal pregnancy, ectopic pregnancy.ncy, ectopic pregnancy.

Pathologic findingsPathologic findings
Gross inspectionGross inspection irregular or circumscribed irregular or circumscribed hemorrhagic ghemorrhagic g
rowthrowth in the uterine wall in the uterine wallulcerating surface opens into the endomeulcerating surface opens into the endome
trial cavity (rarely embedded in myometritrial cavity (rarely embedded in myometrium)um)
penetration into broad ligament or the pepenetration into broad ligament or the peritoneal cavityritoneal cavity
dark red blood:.it is filled dark red blood:.it is filled metastatic nodmetastatic nodulesules

ulcerating surfulcerating surface opens into thace opens into the endometrial cae endometrial cavity (rarely embevity (rarely embedded in myometrdded in myometrium)ium)
Histologic findingsHistologic findings we see masses of anaplastic trophblastic we see masses of anaplastic trophblastic
cells in microscopy;cells in microscopy; invasion into the uterine wall, destroying invasion into the uterine wall, destroying
vessels, muscle tissuevessels, muscle tissue prominent necrosis and hemorrhageprominent necrosis and hemorrhage villi can not be recognizedvilli can not be recognized spread through circulationspread through circulation

Clinical ManifestationsClinical Manifestations
irregular bleeding after irregular bleeding after preceding gestation;preceding gestation;
malignant tumor cells enter the malignant tumor cells enter the circulation through the open circulation through the open blood vessels and are blood vessels and are transported to lungs, brain or to transported to lungs, brain or to other distant sites.other distant sites.

metastatic symptomsmetastatic symptoms pulmonary lesionspulmonary lesions cerebral lesionscerebral lesions metastatic nodule in the vagina, vulmetastatic nodule in the vagina, vul
va or cervix ,it is va or cervix ,it is bluish nodulebluish nodule filled filled dark red blood.dark red blood.
DiagnosisDiagnosis
Diagnosis must be suspected as a pDiagnosis must be suspected as a possible reason for continued (irregulossible reason for continued (irregular) bleeding after any form of pregnar) bleeding after any form of pregnancy.ancy.
we assay hCG , the time of hCG chanwe assay hCG , the time of hCG change into normal is different in various ge into normal is different in various diseases.diseases.

hCG changehCG change
HM:84-100 daysHM:84-100 daysArtificial abortion:30 daysArtificial abortion:30 daysSpontaneous abortion:19 daysSpontaneous abortion:19 daysNormal delivery:12 daysNormal delivery:12 daysEctopic pregnancy:8-9 daysEctopic pregnancy:8-9 days

StagingStaging
International staging of WHO may be sumInternational staging of WHO may be summarized as follows:marized as follows:
ⅠⅠ:: lesion localized in uterus, no metastasi lesion localized in uterus, no metastasis;s;
ⅡⅡ:: lesion extends beyond uterus, but still lesion extends beyond uterus, but still confined to internal genitalias;confined to internal genitalias;
ⅢⅢ:: pulmonary lesion pulmonary lesionⅣⅣ: : metastasis to other distant sites.metastasis to other distant sites.

TreatmentTreatment
highly sensitive to chemotherapy, whichighly sensitive to chemotherapy, which is invariably the treatment choice.h is invariably the treatment choice.surgery has little place (because of the hsurgery has little place (because of the high vascularity and the effectiveness of cigh vascularity and the effectiveness of chemotherapy). it is indicated for tumor rhemotherapy). it is indicated for tumor resistant to chemotherapy and single meesistant to chemotherapy and single metastases persisting despite chemotheraptastases persisting despite chemotherapy.y.

ChemotherapyChemotherapy
most often used drugsmost often used drugs methotrexate (MTX)methotrexate (MTX) actinomycin D (Act-D)actinomycin D (Act-D) 5-fluorouracil (5-Fu) 5-fluorouracil (5-Fu) vincristine (VCR)vincristine (VCR) cyclophosphamide (CTX)cyclophosphamide (CTX) chlo-ranbucil, etcchlo-ranbucil, etc
principlesprinciples low-risk patients are usually treated with a sinlow-risk patients are usually treated with a sin
gle agentgle agent medium-risk patients are usually treated with medium-risk patients are usually treated with
EMA-CO regimen with 80-90% survival rate. (EtEMA-CO regimen with 80-90% survival rate. (Etoposide, Methotrexate,Actinomycin,Cyclophooposide, Methotrexate,Actinomycin,Cyclophosphamide,Vincristin)sphamide,Vincristin)
toxic reaction: marrow depression ;toxic reaction: marrow depression ; gastrointestinal ulceration;gastrointestinal ulceration; change in liver and renal functionchange in liver and renal function
Standard for dischargeStandard for discharge
three consecutive weekly assays for hthree consecutive weekly assays for hCG are negativeCG are negative
two more courses for consolidationtwo more courses for consolidation all symptoms and signs disappearall symptoms and signs disappear

OperationOperation
unresponsive or drug fails to unresponsive or drug fails to reach the tumor;reach the tumor; if the tumor can be eradicated if the tumor can be eradicated by drug therapy, esp.in young by drug therapy, esp.in young women, there is no reason to women, there is no reason to remove the uterus;remove the uterus; the ovaries need not be the ovaries need not be removedremoved..

Follow-up examinationsFollow-up examinations
at 1-month interval for 1 year: at 3-at 1-month interval for 1 year: at 3-month interval for 2 yearsmonth interval for 2 years
at 1-year interval for 3 yearsat 1-year interval for 3 years at 2-year interval afterwards. at 2-year interval afterwards. pelvic pelvic
examinationexamination chest X-ray filmchest X-ray film hCGhCG

Ask question :Ask question :
What are the basic histologiWhat are the basic histologic and pathologic differences c and pathologic differences between invasive mole and between invasive mole and choriocarcinoma?choriocarcinoma?