getting the most of antidepressants rvu 05-03-2014 larry o. sanders, md diplomate of the american...
TRANSCRIPT
Getting the Most of Antidepressants
RVU 05-03-2014
Larry O. Sanders, MDDiplomate of the American Board of Psychiatry and Neurology
Goals
Screening the Primary Care population for Mental Disease.
First Line and Second Line Treatment of MDD.
Evidence that more than Major Depression is Involved.
When to Refer to Mental Health.
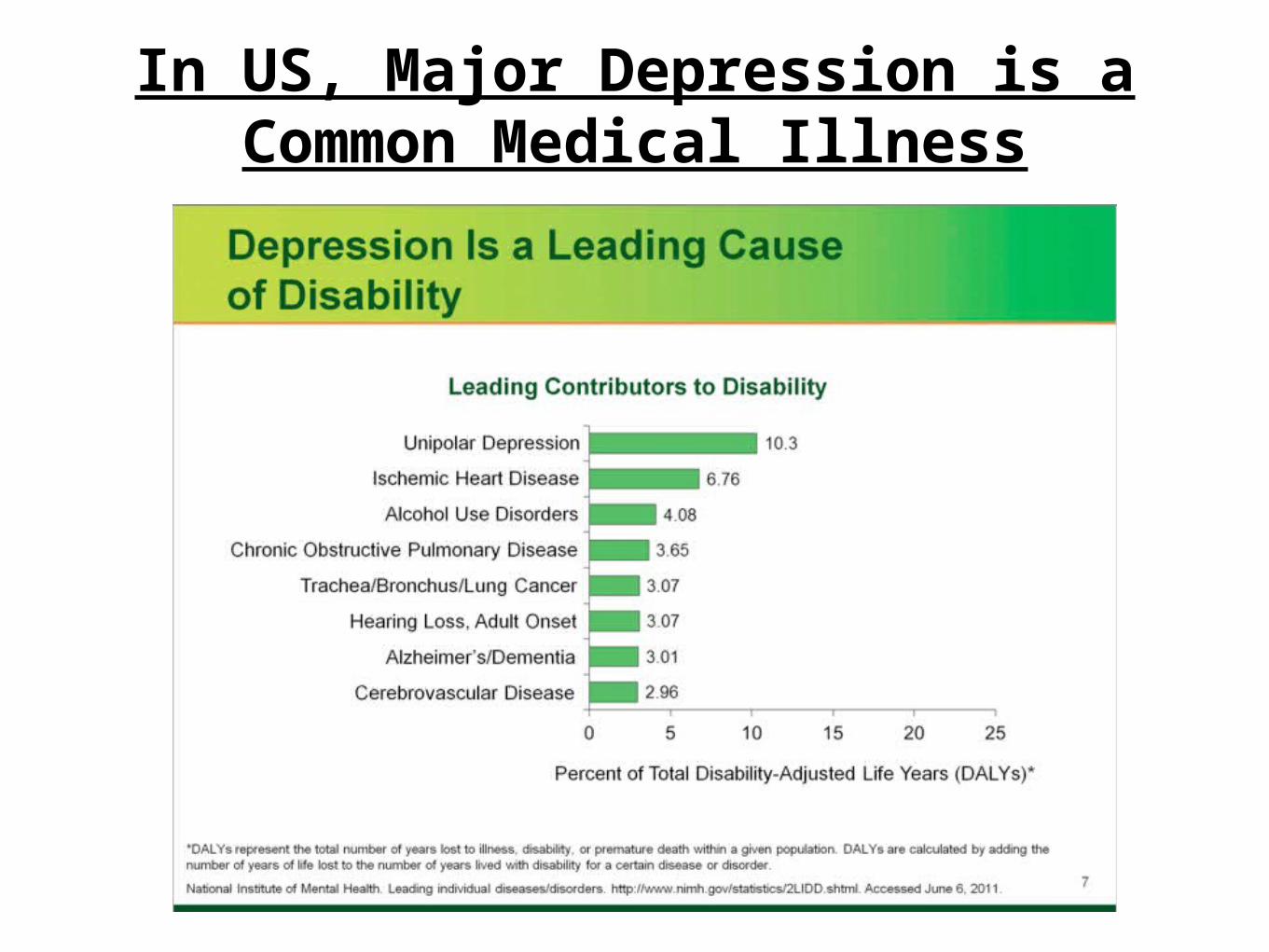
In US, Major Depression is aCommon Medical Illness
Why Treat Depression?
Disability
Morbidity- Depression makes existing somatic conditions worse. (Inflammatory Factors)
Mortality- Psychiatric patients die up to 20 years earlier than average. Most Common reason is Cardiovascular Disease!
Second is Suicide.
Inflammatory Factors, 1
Major Depression Increases
Inflammatory Factors, Worsening the Prognosis
ofSomatic Illness
Inflammatory Factors, 2
Somatic IllnessesIncrease
Inflammatory Factors,Worsening the Prognosis
ofMajor Depression
Depression and Atherosclerotic Disease.
• Major Depression carries 4X Risk of developing a Myocardial Infarction! Anda 1993, Barefot, et. Al. 1996, Pratt 1996
• MIs comorbid with MDD are 5X More likely to be Fatal. Anda 1993
• 16.5% Mortality Risk @ 6 months following Acute MI if also Depression vs 3% if not Depressed. Frasure-Smith 1993
• Major Depression carries same Risk Factor for developing an MI, as Cigarette Smoking!
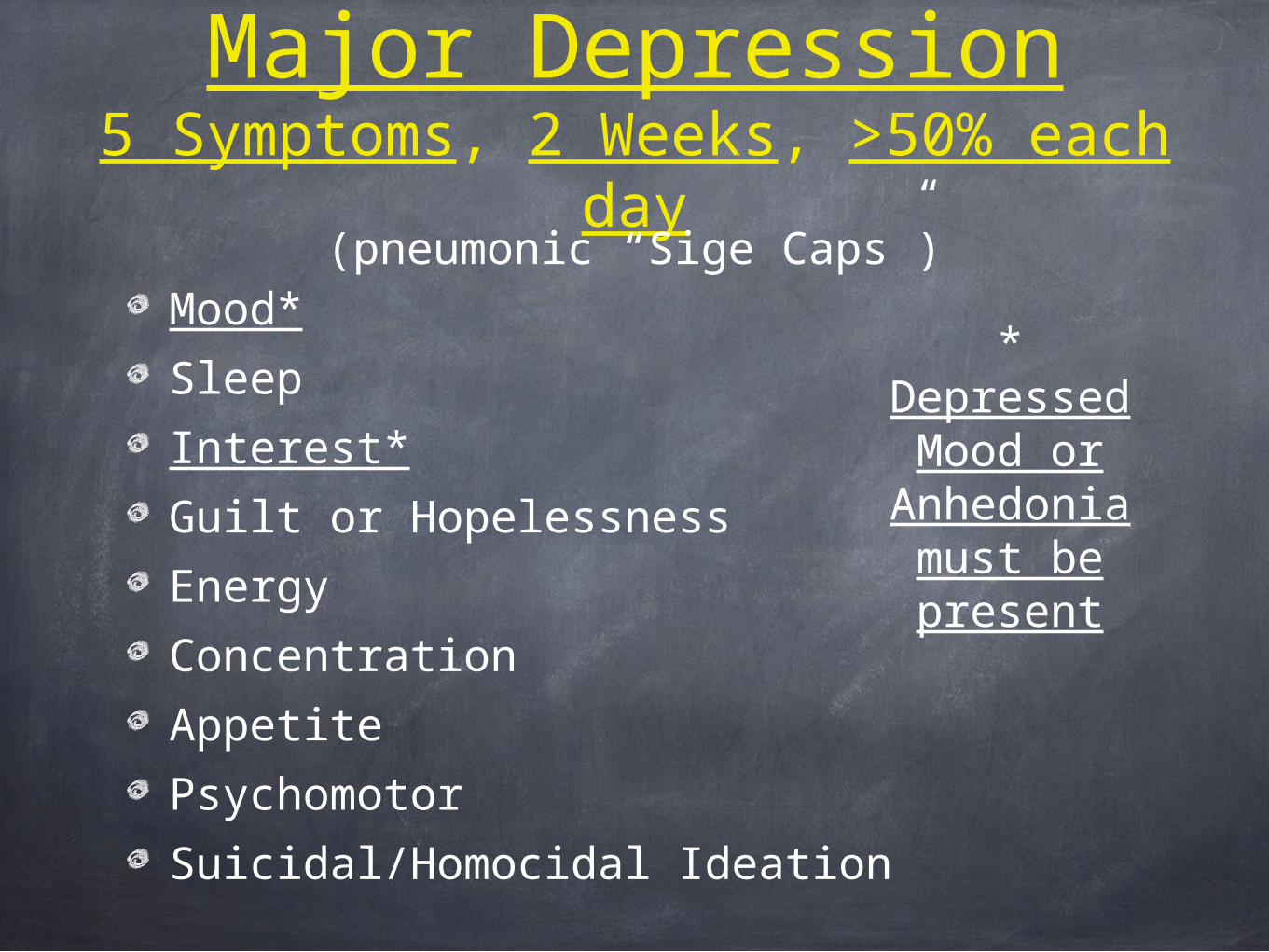
Major Depression5 Symptoms, 2 Weeks, >50% each
day
Mood*
Sleep
Interest*
Guilt or Hopelessness
Energy
Concentration
Appetite
Psychomotor
Suicidal/Homocidal Ideation
* Depressed
Mood or Anhedonia must be present
(pneumonic “Sige Caps”)
10
Nature vs Nurture
• MDD is strongly genetic, with well over 100 genes involved.
• However, the largest risk for developing MDD as an adult is losing a parent before age 12.
• Many Environmental, Psychological and Sociological factors can effect it.
10
11
Medical Disease can appear as Major Depressive Disorder
• Many Medical Diseases can appear as MDD. R/O:–Hypothyroidism–Anemia, both Microcytic and Macrocytic–Any inflammatory Disease–Hyperparathyroidism (even slightly elevated Ca++
may be important)–Various Vitamin deficiencies, including: D, B12,
B6, Folate, etc.• Vitamin D deficiency seems more common since the use of high SPF Sunscreens. 11
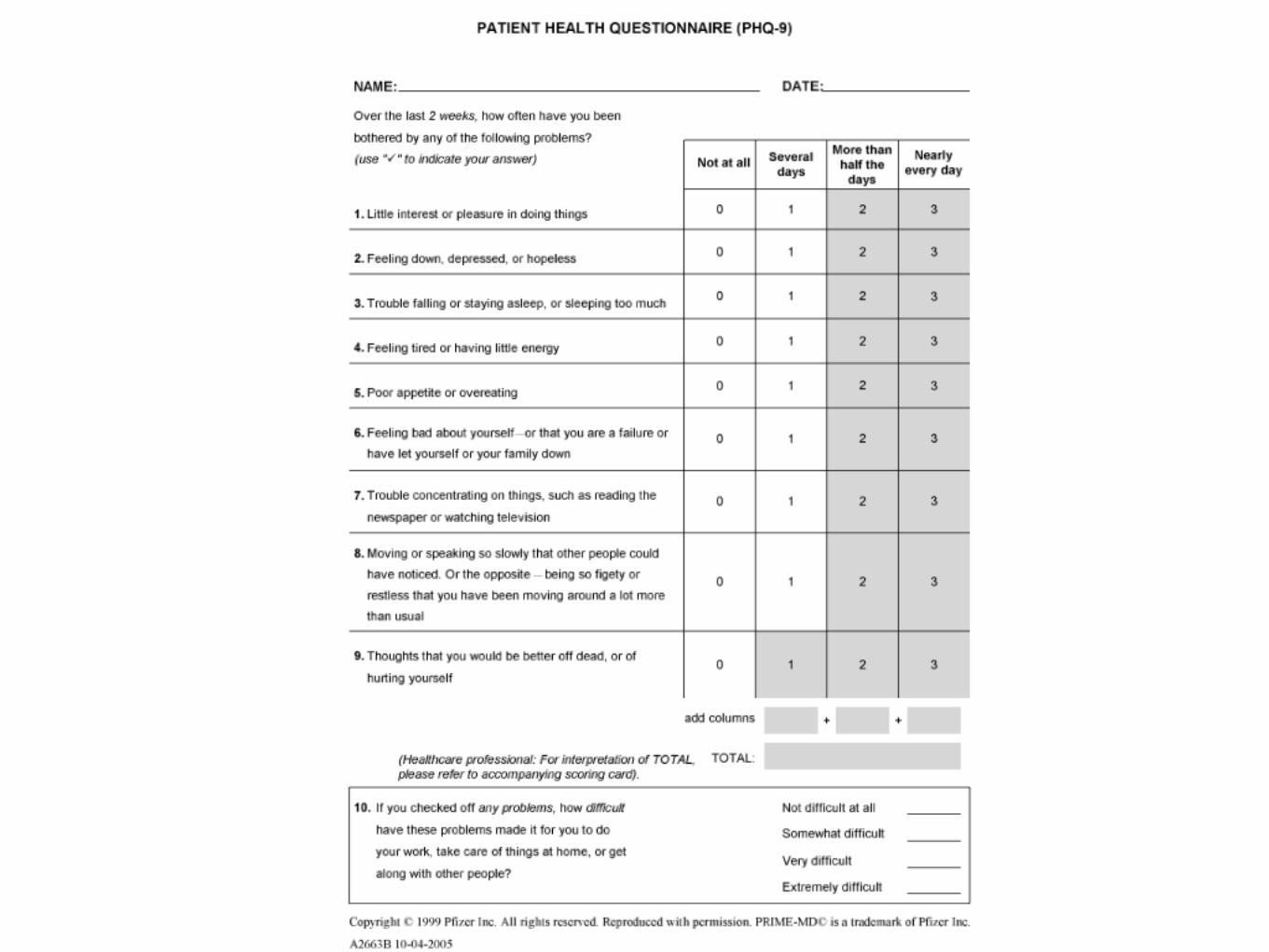
Other (Free) Scales•PHQ 2 Screener
• ( Very brief. I don’t encourage its’ use).
•Zung Depression Rating Scale
•QIDS-SR
• Quick Inventory Depressive Symptomatology (Self Report)
•CUDOS
• Clinically Useful Depression Outcome Scale
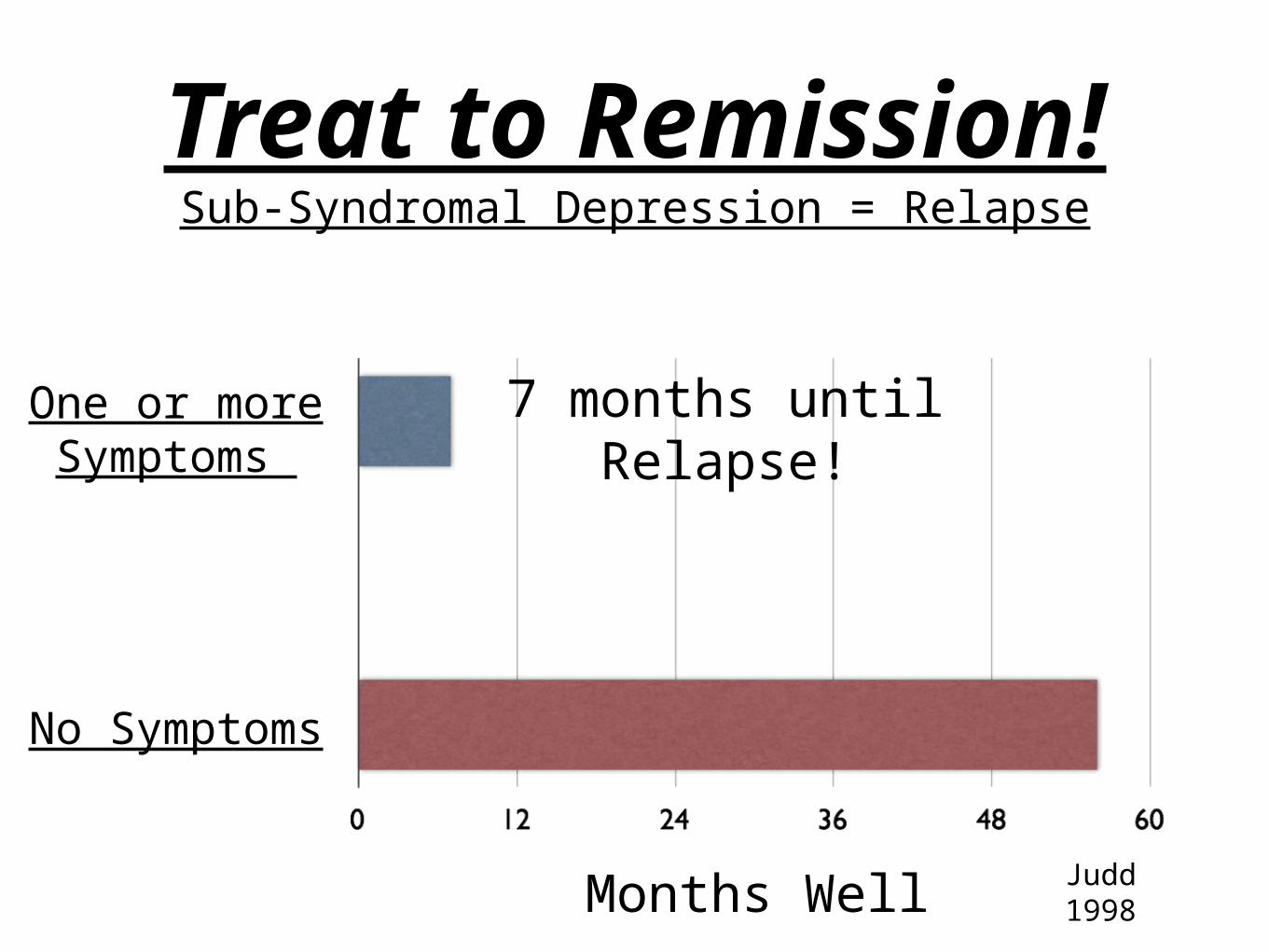
Treat to Remission!
Sub-Syndromal Depression = Relapse
Months Well Judd 1998
7 months until Relapse!
One or more Symptoms
No Symptoms
Symptoms and Circuits
Advocated byStephen M. Stahl, MD
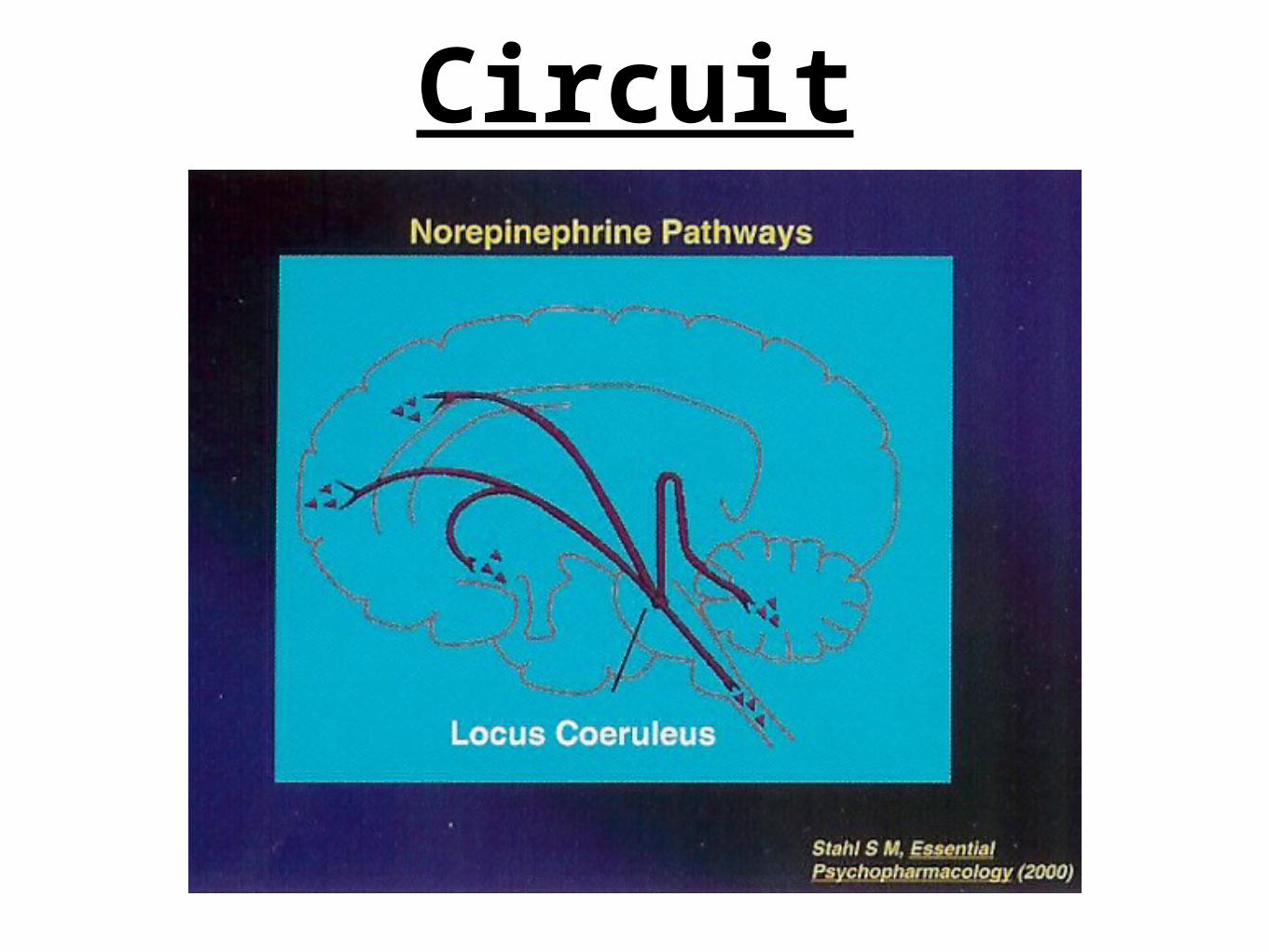
Circuit
When a Brain Circuit, when overstimulated or under-stimulated, it
will produce certain symptoms.
(adapted from Steven Stahl, MD)
Each Symptom, regardless of the disease,
comes from the Same Circuit Malfunction!
(adapted from Steven Stahl, MD)
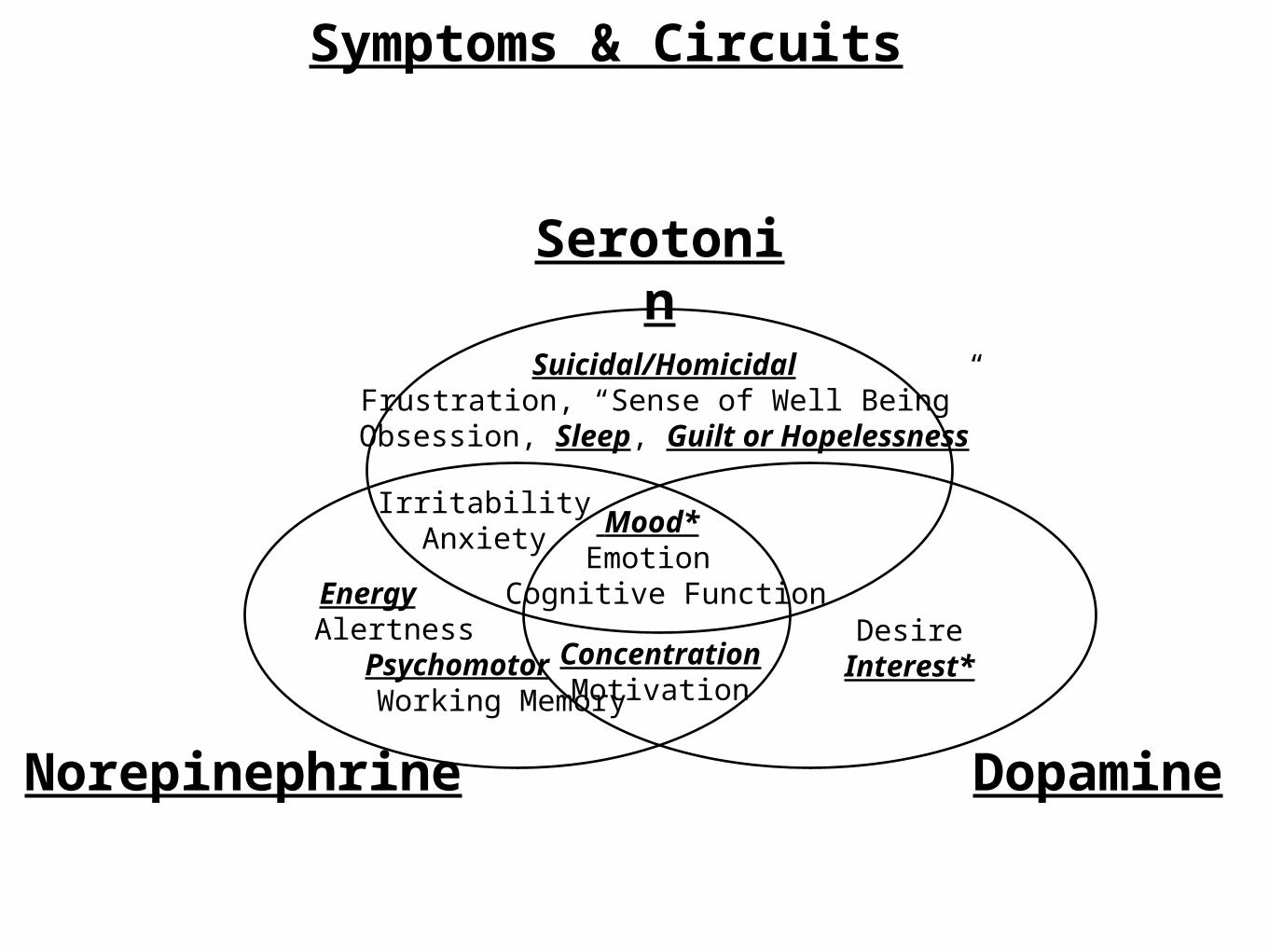
Symptoms & Circuits
By Knowing Which Symptom is related to which Circuit,
and by Knowing How Each Medication Effects Each Circuit
You can Logically Deduce Which Medication Will Best Treat Most Mental Conditions.
(adapted from Steven Stahl, MD)
3 Major Circuits Contributing toMental Illness
Serotonin
Circuits
Serotonin
Norepinephrine
Circuits
Serotonin
Norepinephrine Dopamine
Circuits
SymptomsAssociated with
theseCircuits
Symptoms associated with Serotonin
•Serotonin helps us “Cope”.
•If Serotonin is too Low: Irritable, Anxious, Easily Overwhelmed, Hopeless, Suicidal, “poor sense of Well-being”
•If Serotonin is too High: Serotonin Syndrome; Agitation, Fasciulations, Hyperthermia, Vital Sign Disturbance, leading to stupor, come then death. [Although pharmacists warn of this, neither I nor any Psychiatric Colleagues have ever seen this condition. So it appears to be very rare.]
Symptoms associated with Norepinephrine
•Norepinephrine is like “Adrenaline”.
•If Norepinephrine too Low: Anergy, Immediate Memory Impaired, Psychomotor Retardation.
•If Norepinephrine too High: Irritable, Agitation, Insomnia. (Similar Symptoms to Low Serotonin).
Symptoms associated with Dopamine
•Dopamine provides Interests/Desire, mentally. (Dopamine has other physical functions as well).
•If Dopamine too Low: Apathy, Dementia, Muscle
•If Dopamine too High: Hedonism, Psychosis, Mania
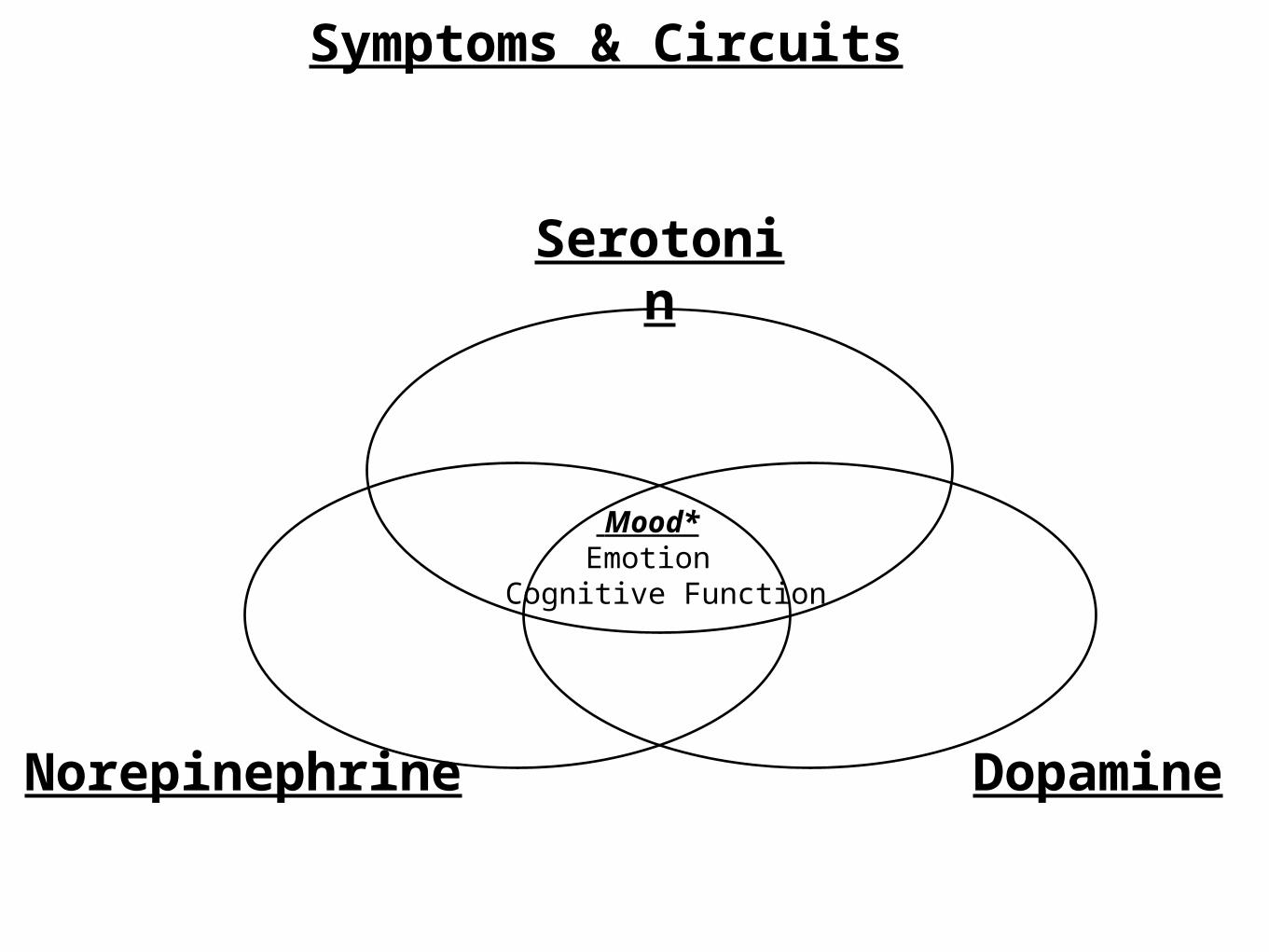
Mood*Emotion
Cognitive Function
Serotonin
Norepinephrine
Dopamine
Symptoms & Circuits
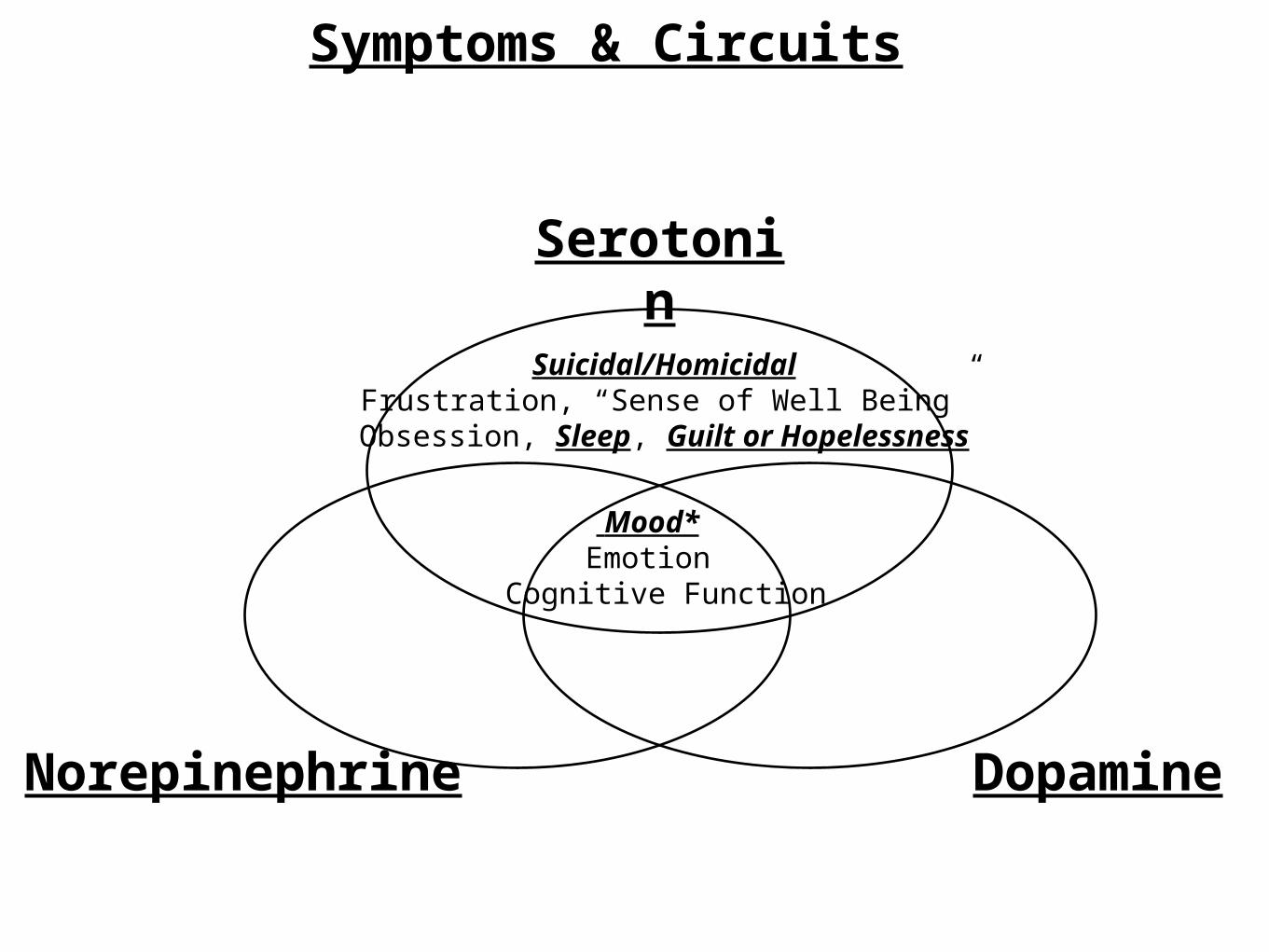
Mood*Emotion
Cognitive Function
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine
Dopamine
Symptoms & Circuits
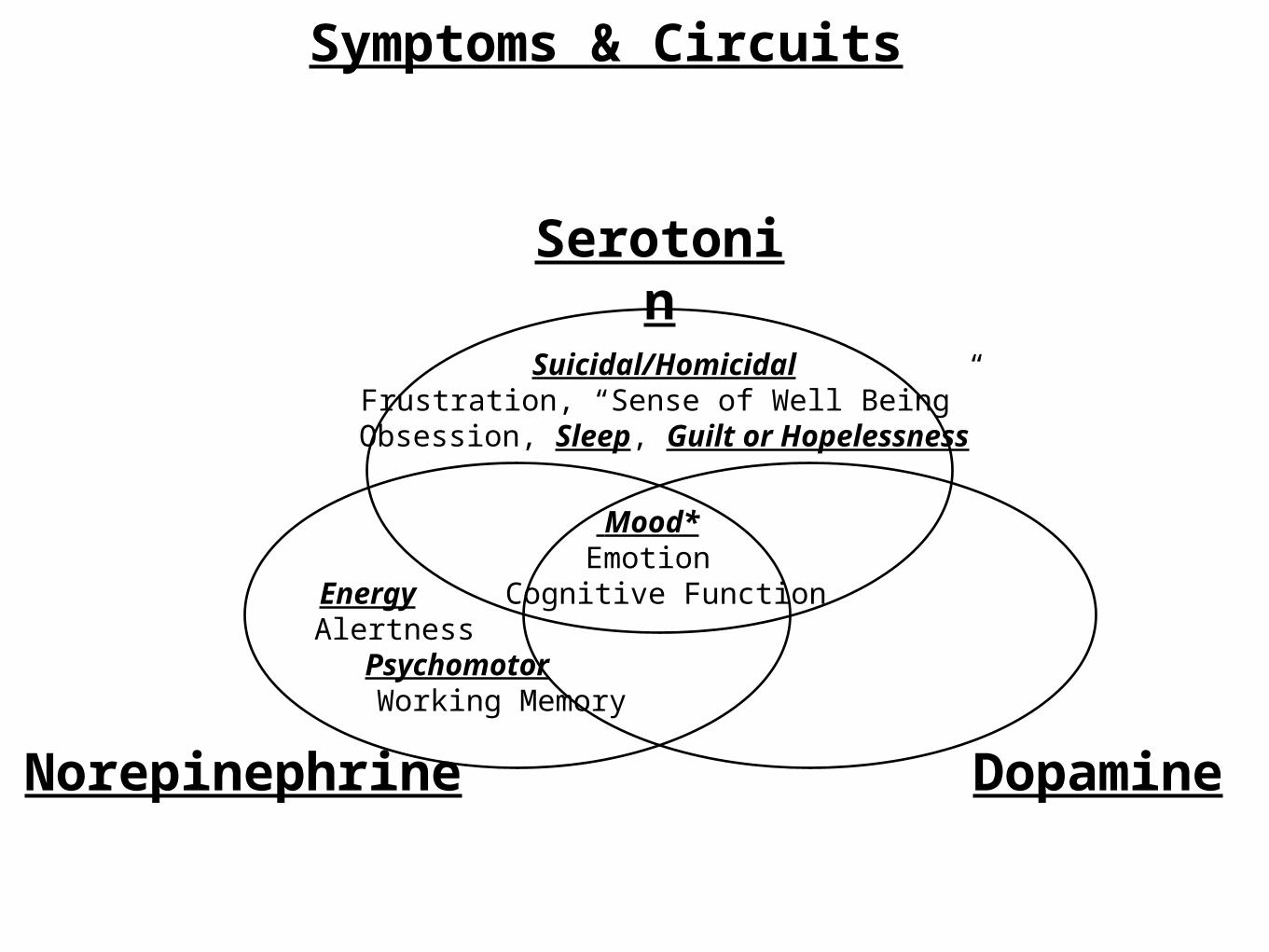
Mood*Emotion
Cognitive Function
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine
Dopamine
Energy Alertness
Psychomotor Working Memory
Symptoms & Circuits
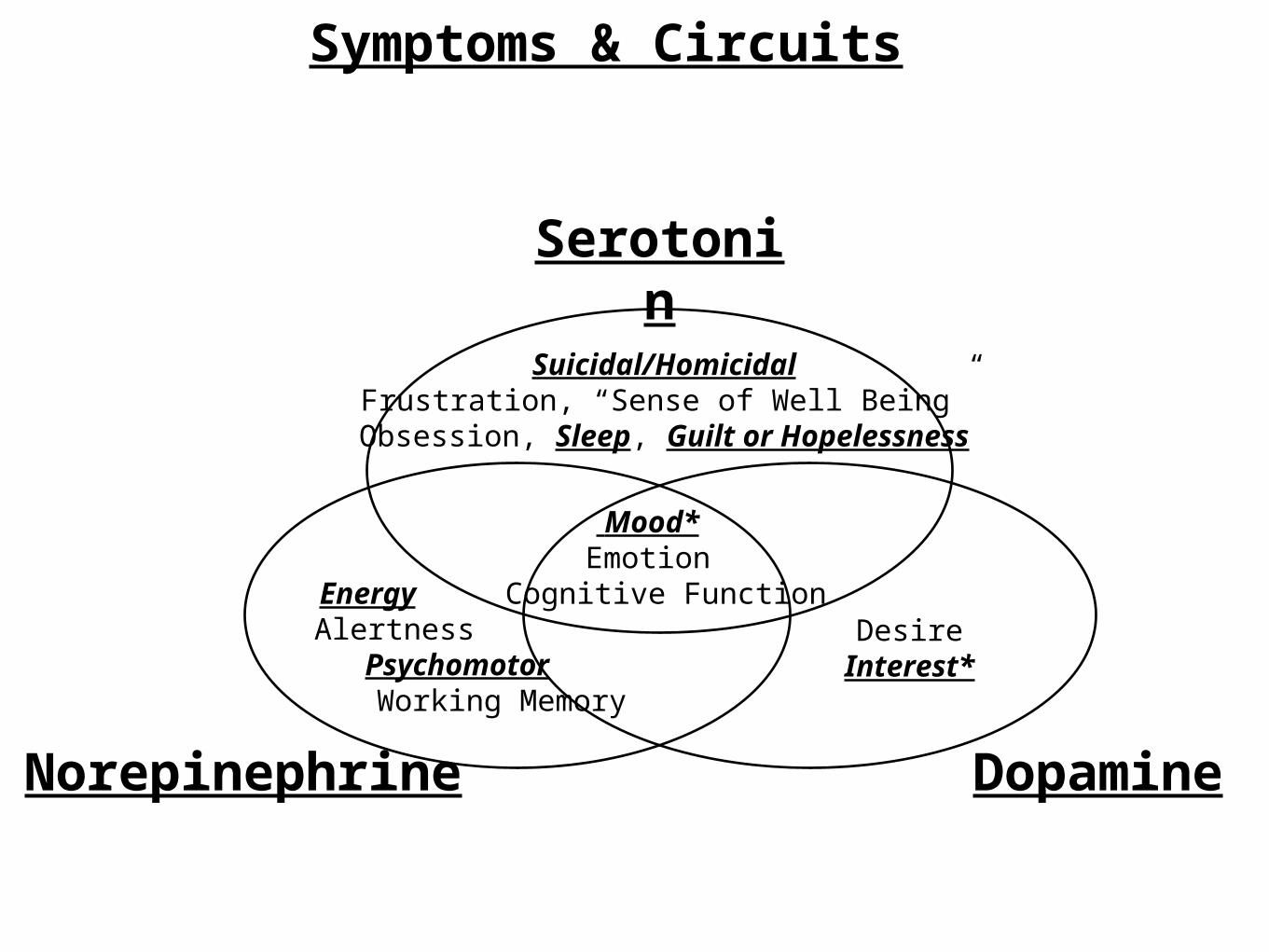
Mood*Emotion
Cognitive Function
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine
Dopamine
DesireInterest*
Energy Alertness
Psychomotor Working Memory
Symptoms & Circuits
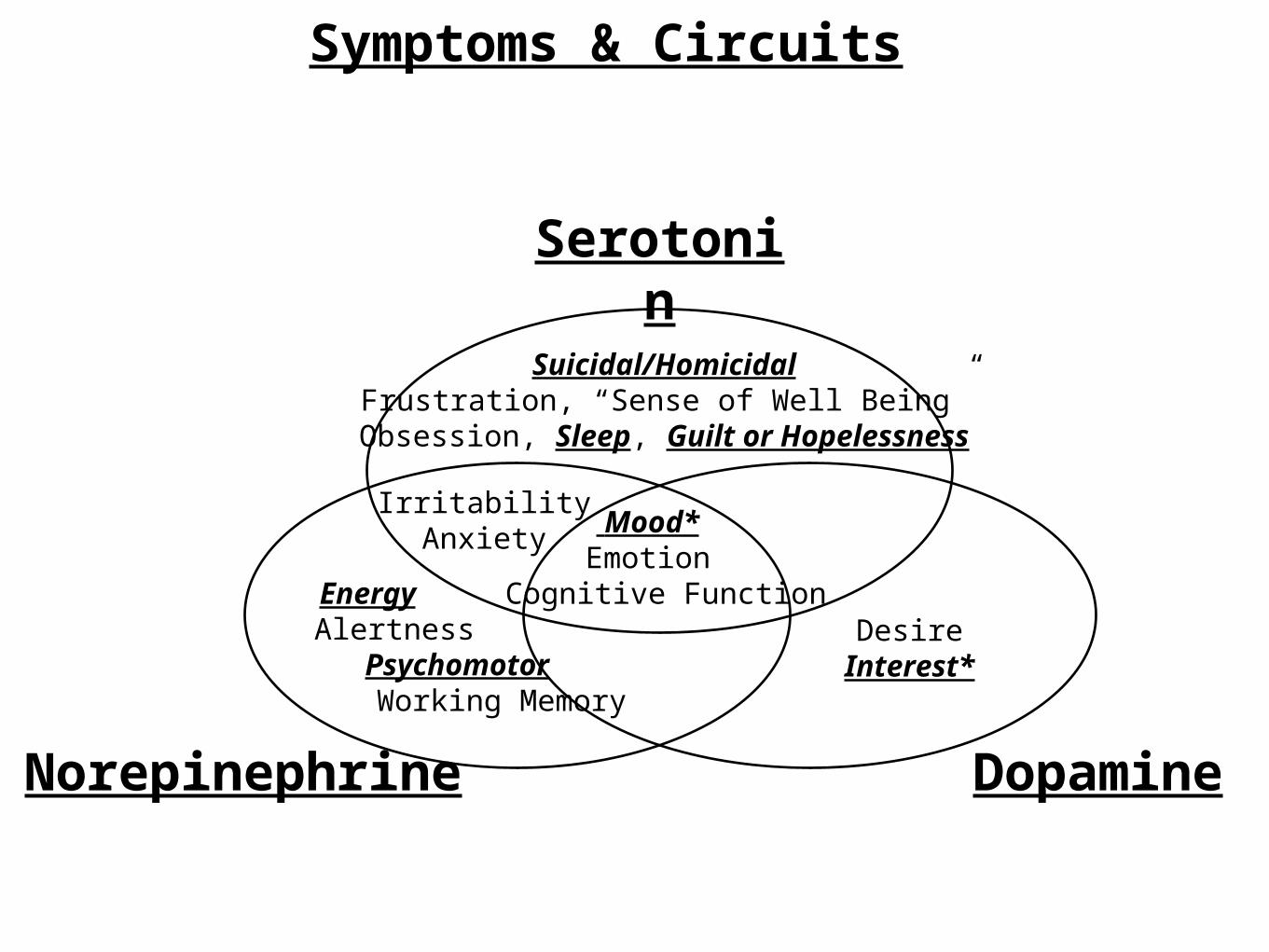
Mood*Emotion
Cognitive Function
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine
Dopamine
IrritabilityAnxiety
DesireInterest*
Energy Alertness
Psychomotor Working Memory
Symptoms & Circuits
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine
Dopamine
IrritabilityAnxiety
DesireInterest*
Energy Alertness
Psychomotor Working Memory
Symptoms & Circuits
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine
Dopamine
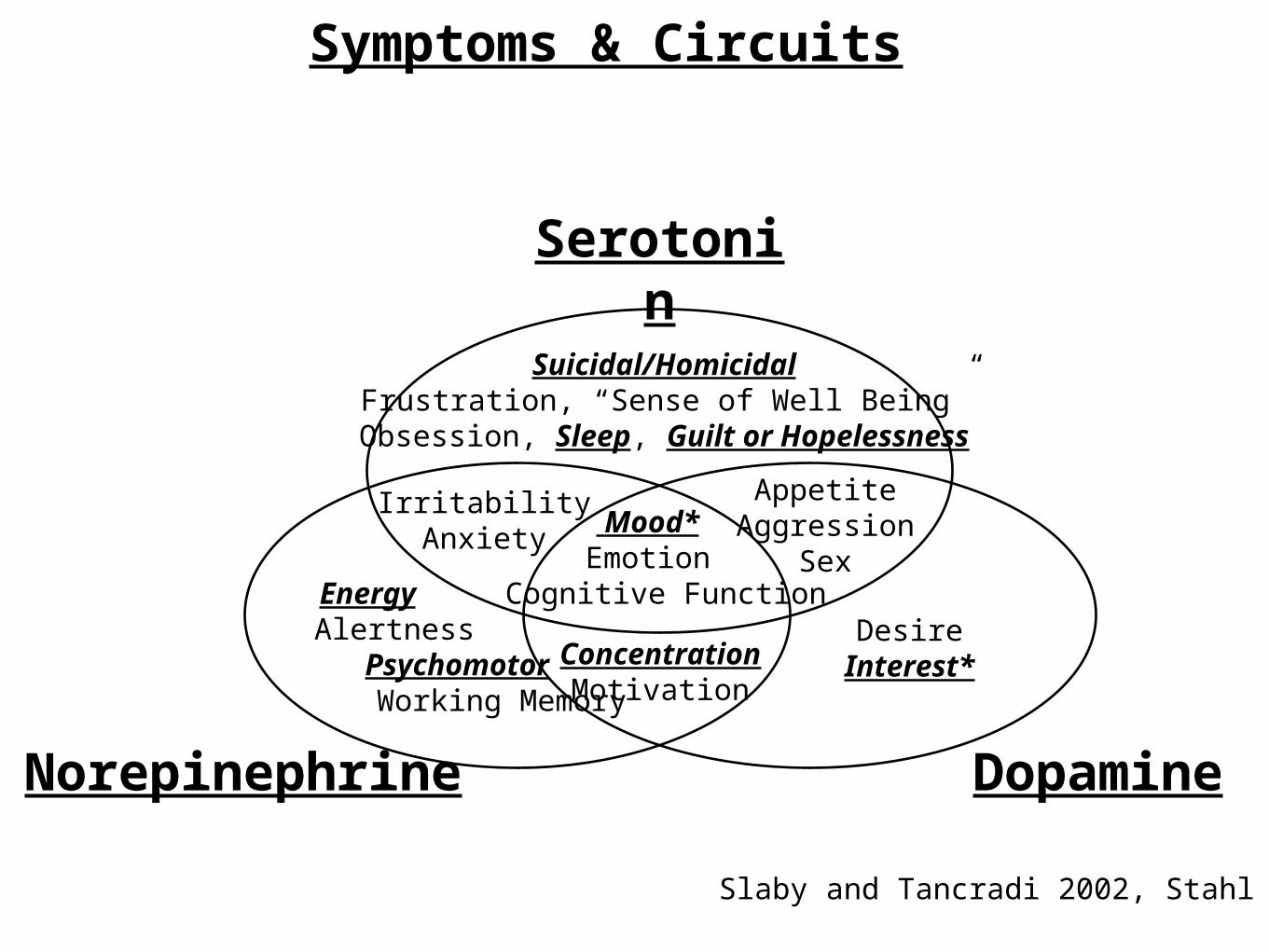
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
Symptoms & Circuits
Slaby and Tancradi 2002, Stahl 2004
Symptoms, Circuits & Medications
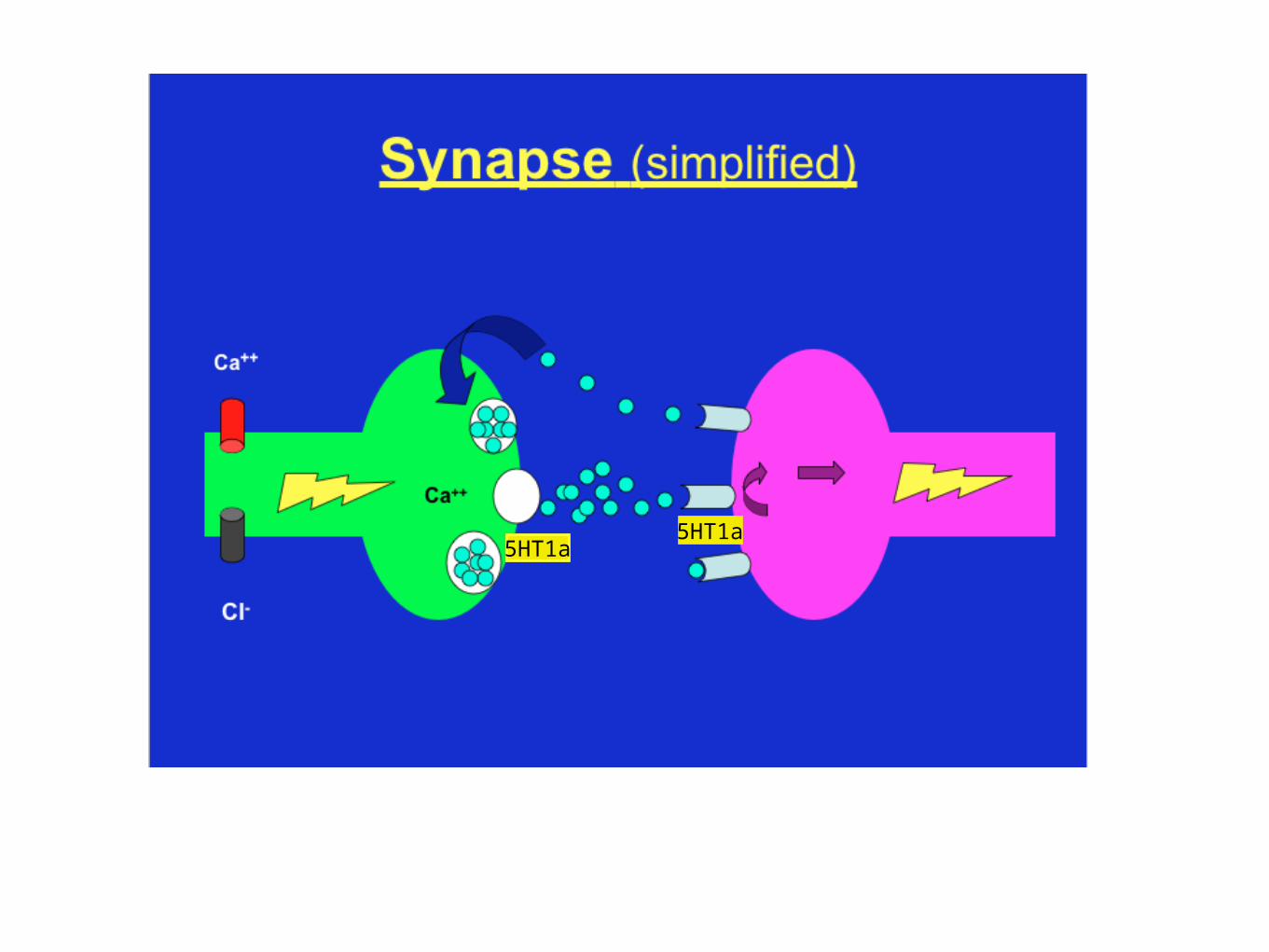
5HT1a5HT1a
Classes of Antidepressants
•SSRIs
•SNRIs, NaSSI
•SDRIs
•NDRIs (mechanism of Wellbutrin not fully understood)
•DRIs, DAgs
•NRIs – (not very effective).
• (MOAIs, not covered here, are powerful Antidepressants; but carry HTN risk with certain foods and/or meds and Serotonin Syndrome with SRIs.)
Suicidality vs Suicide
•An ironic fact about Antidepressant use is that Suicidality risk (thoughts, not death) increases transiently, BUT SUICIDE (DEATH) risk DECREASES in patients less than 24 y.o.! (expound)

Medications Effecting Primarily
Serotonin
SSRIs• “Multi Action” – ssri, 5HT1a, 1b, 3, & 7.
• Vortioxetine (Brintellix).
•“Dual Action” - SSRI & 5HT1a.
• Vilazadone (Viibryd).
• “Single Action” – SSRI.
• Escitalpram (Lexapro).
• Fluoxetine (Prozac). SSRI + bits of others.
• “Half Action” - Racemic mixture, half active.
• Cilatopram (Celexa).
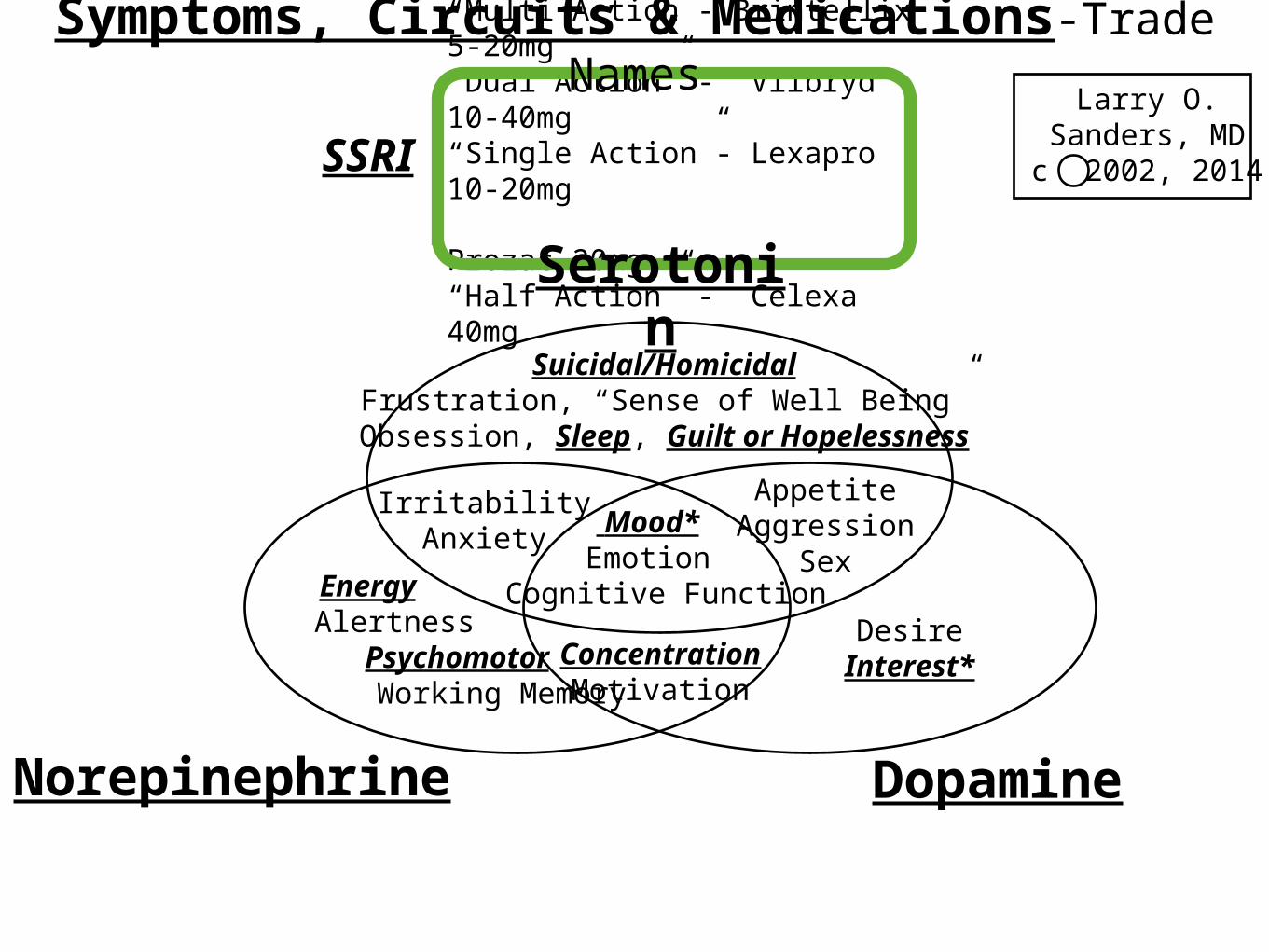
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
Larry O. Sanders, MDc 2002, 2014
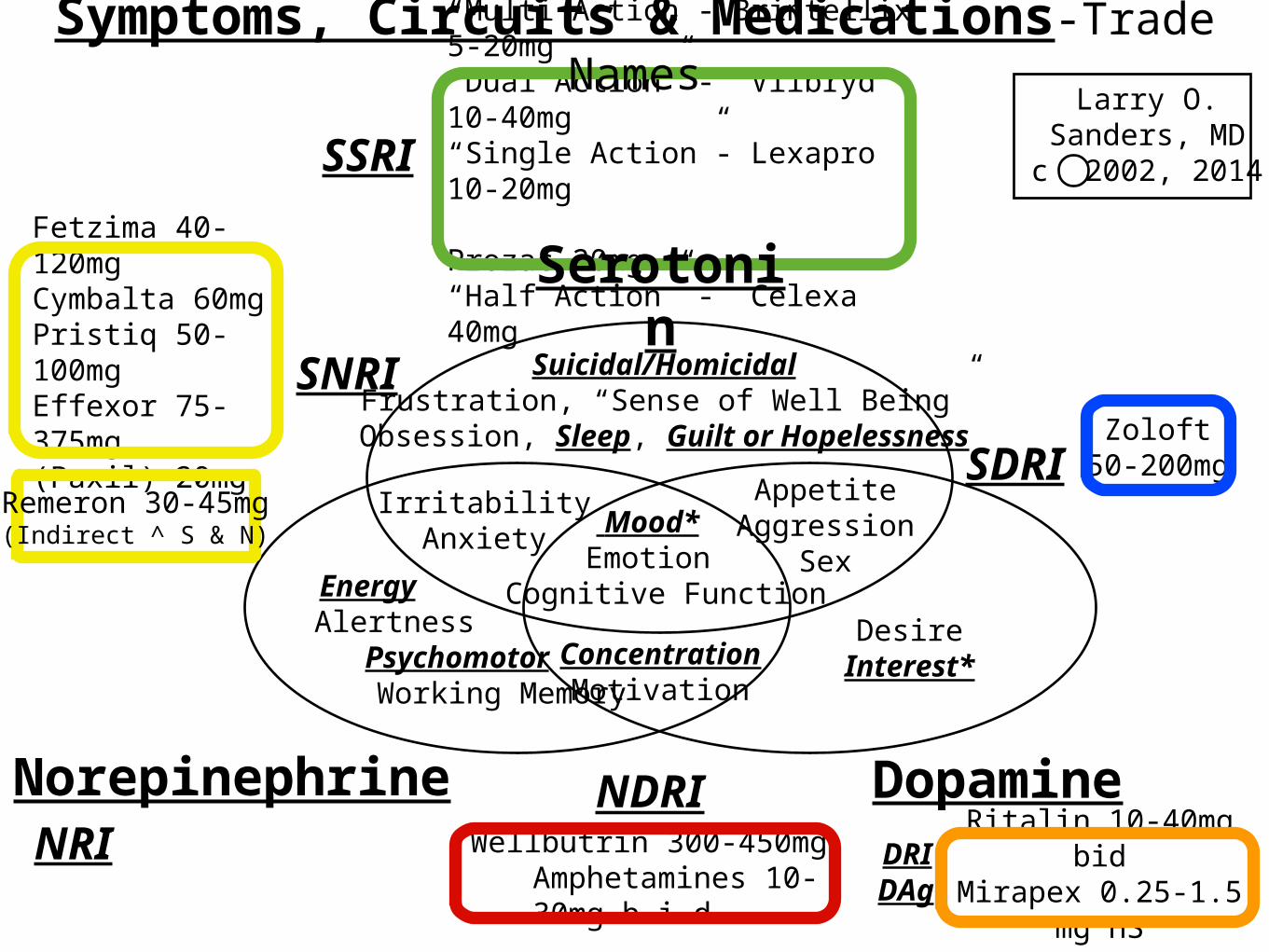
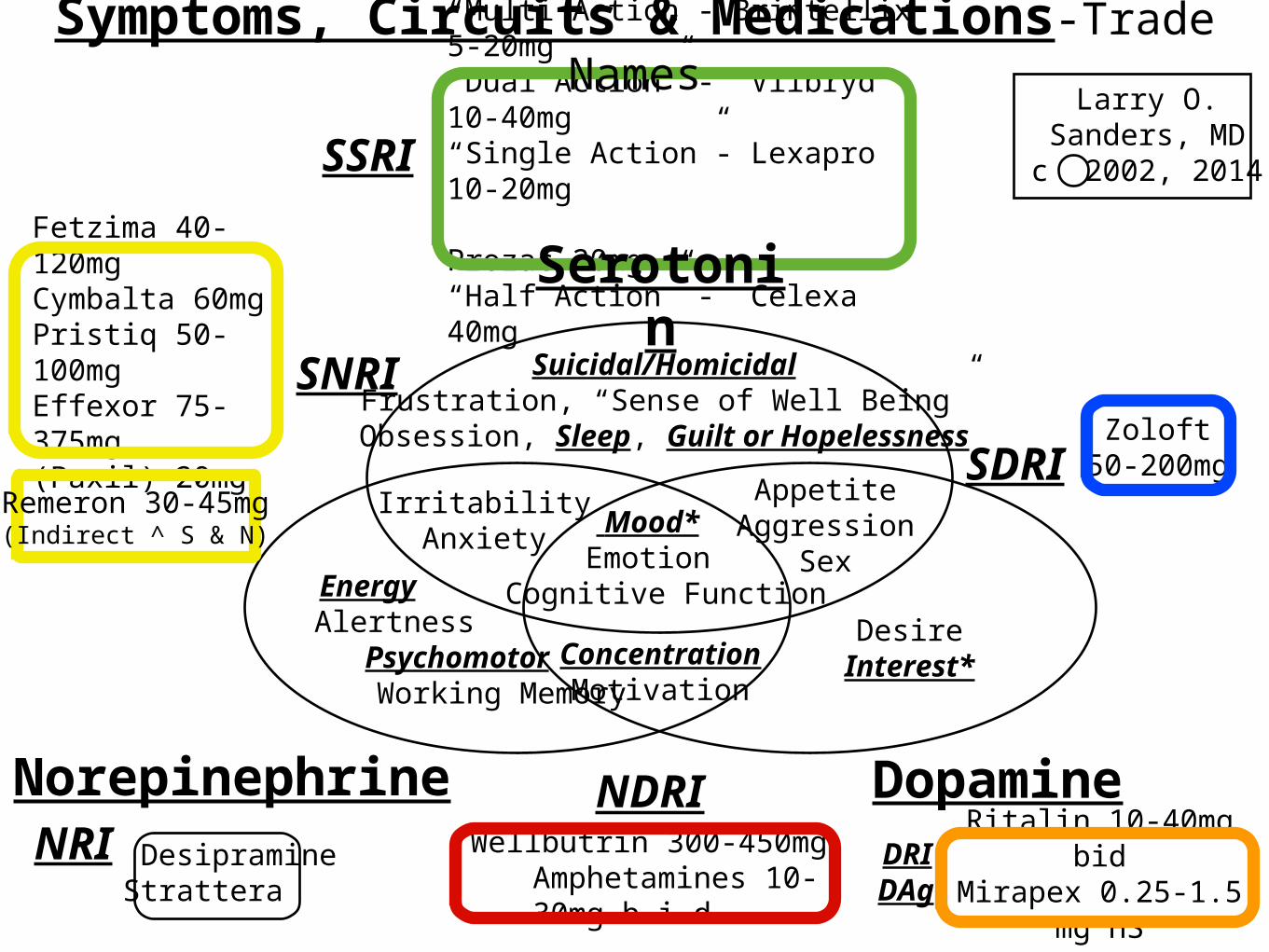
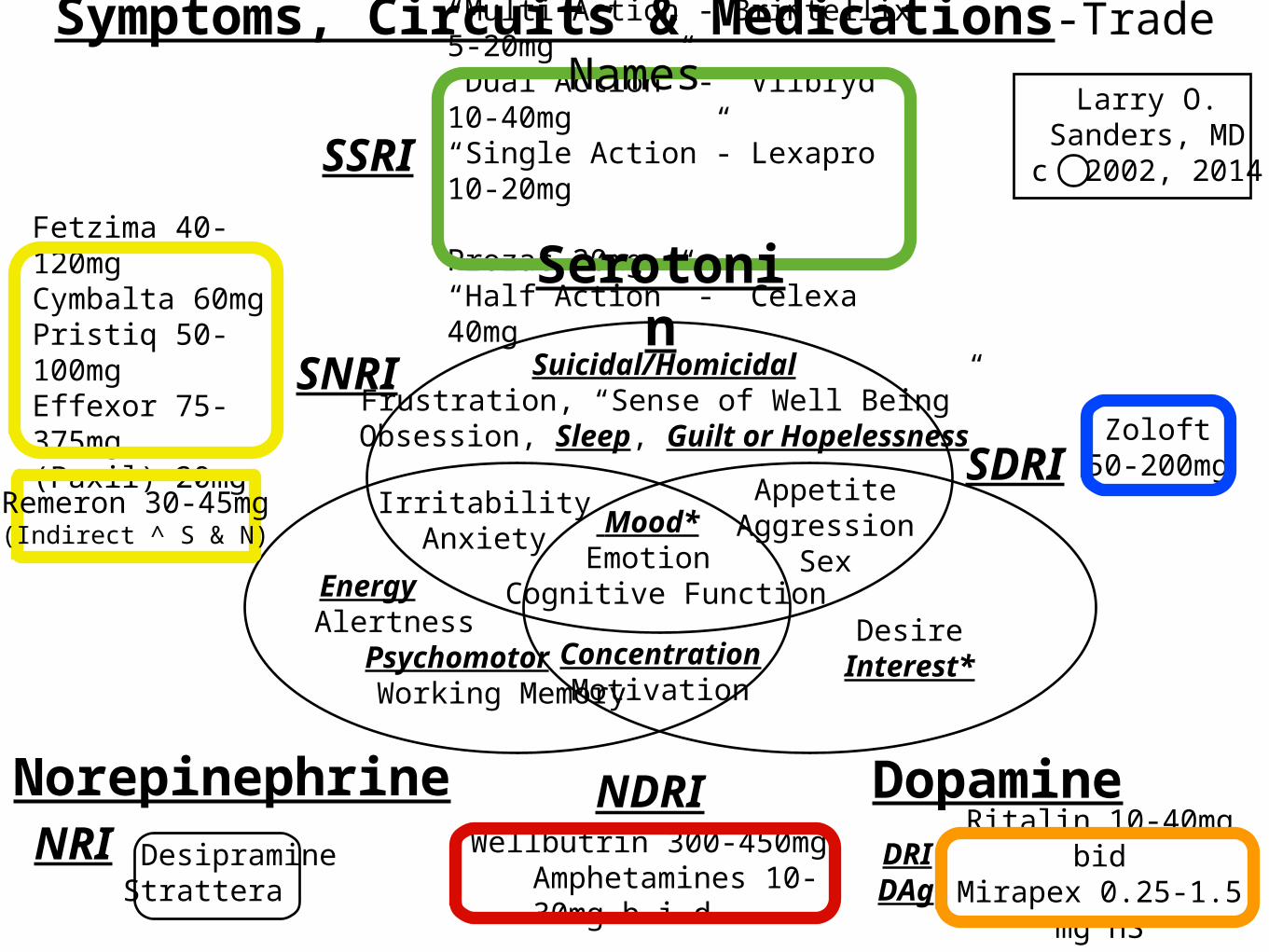
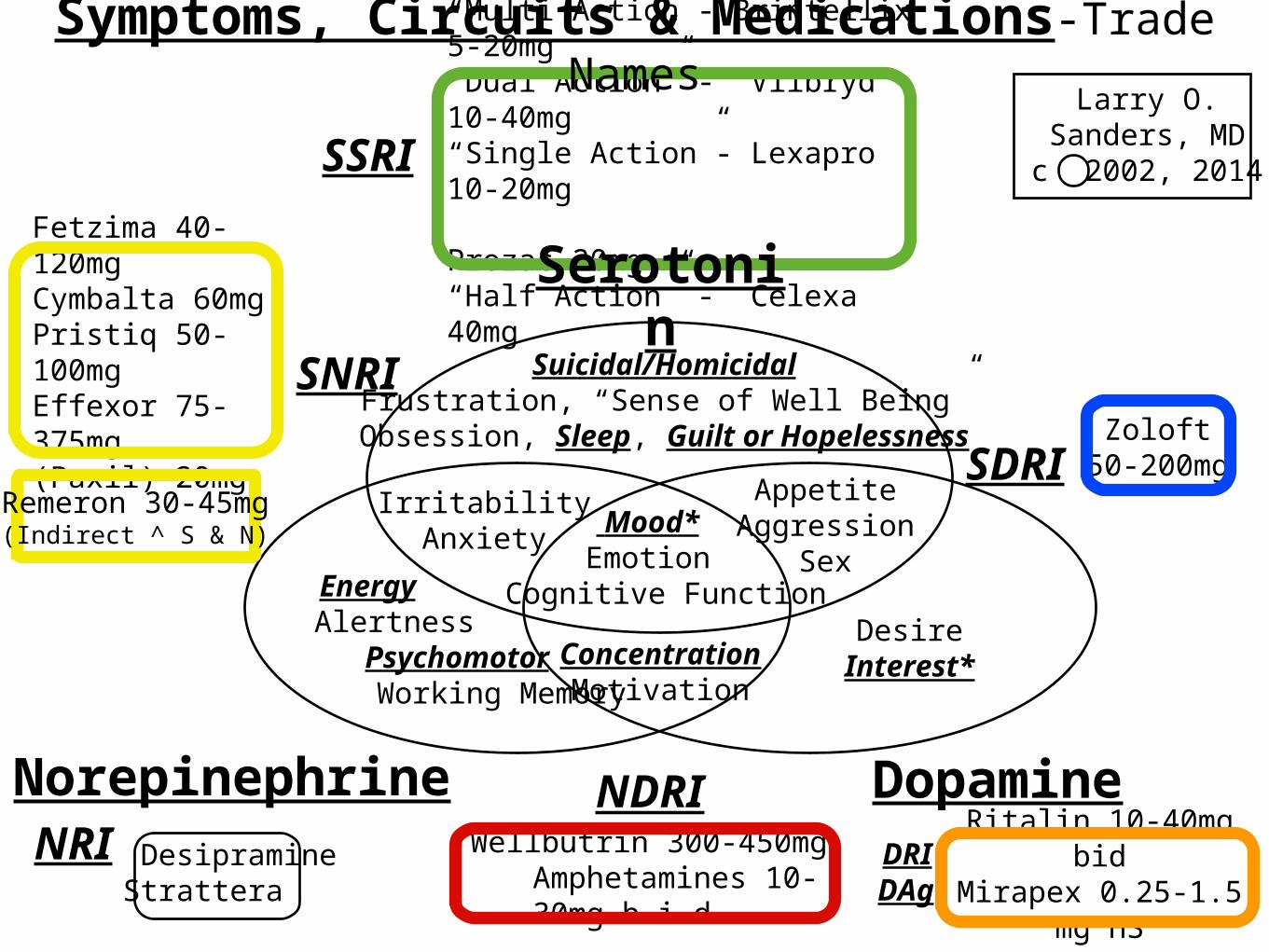
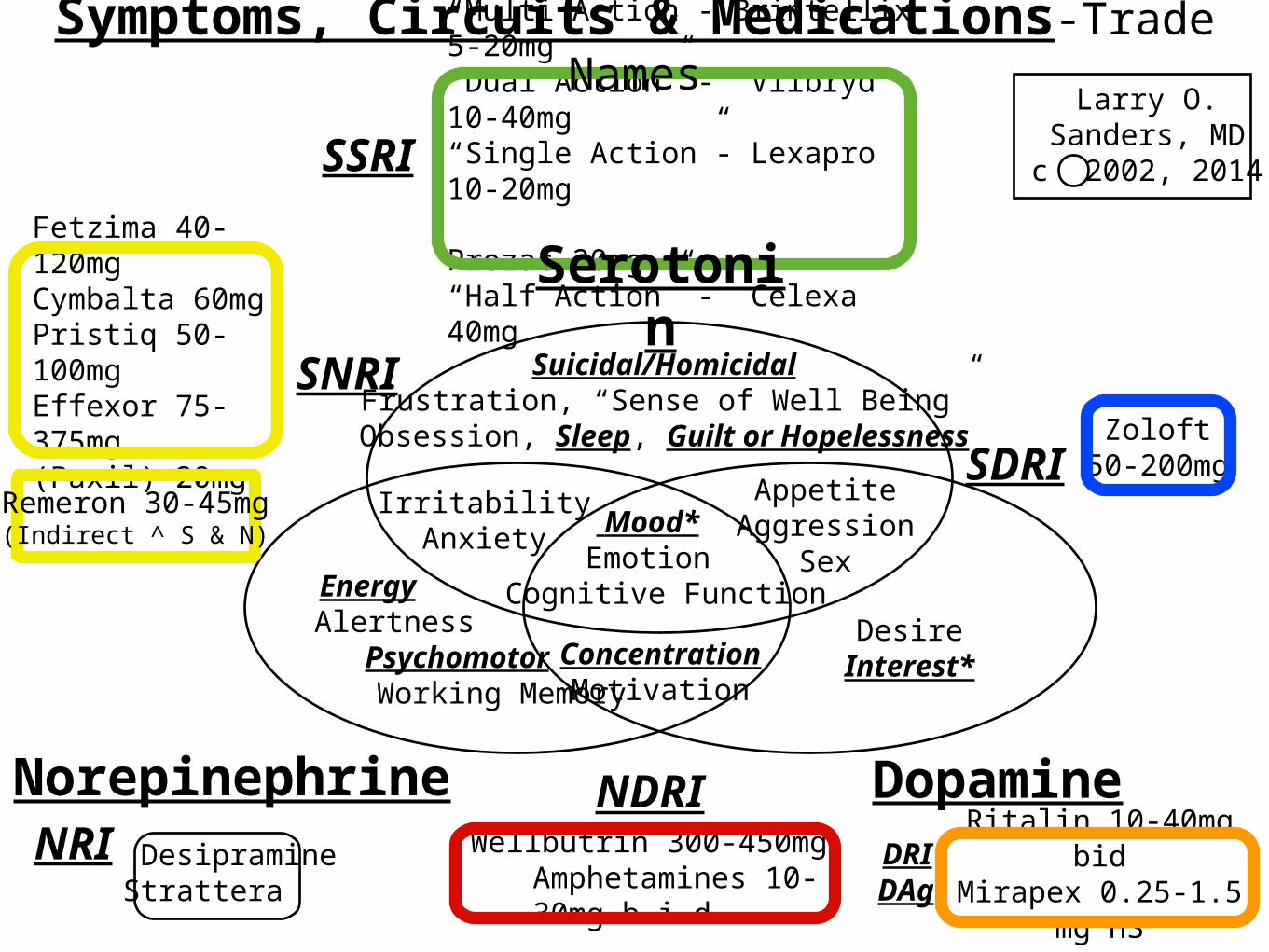
Symptoms, Circuits & Medications-Trade Names

Medications effecting Both Serotonin and
Norepinephrine
SNRIs• Levomilnacipram (Fetzima) 1:2 S:N
• Duloxetine (Cymbalta) 9:1 S:N
• Desvenlafaxine (Pristiq) 15:1 S:N
• Venlafaxine(Effexor) 30:1 S:N
• At low dose is SSRI. At high dose SNRI. Strong W/D issues!
• {Paroxetine (Paxil) 20-40mg}
• Weight gain, Fatigue, Strong W/D issues!
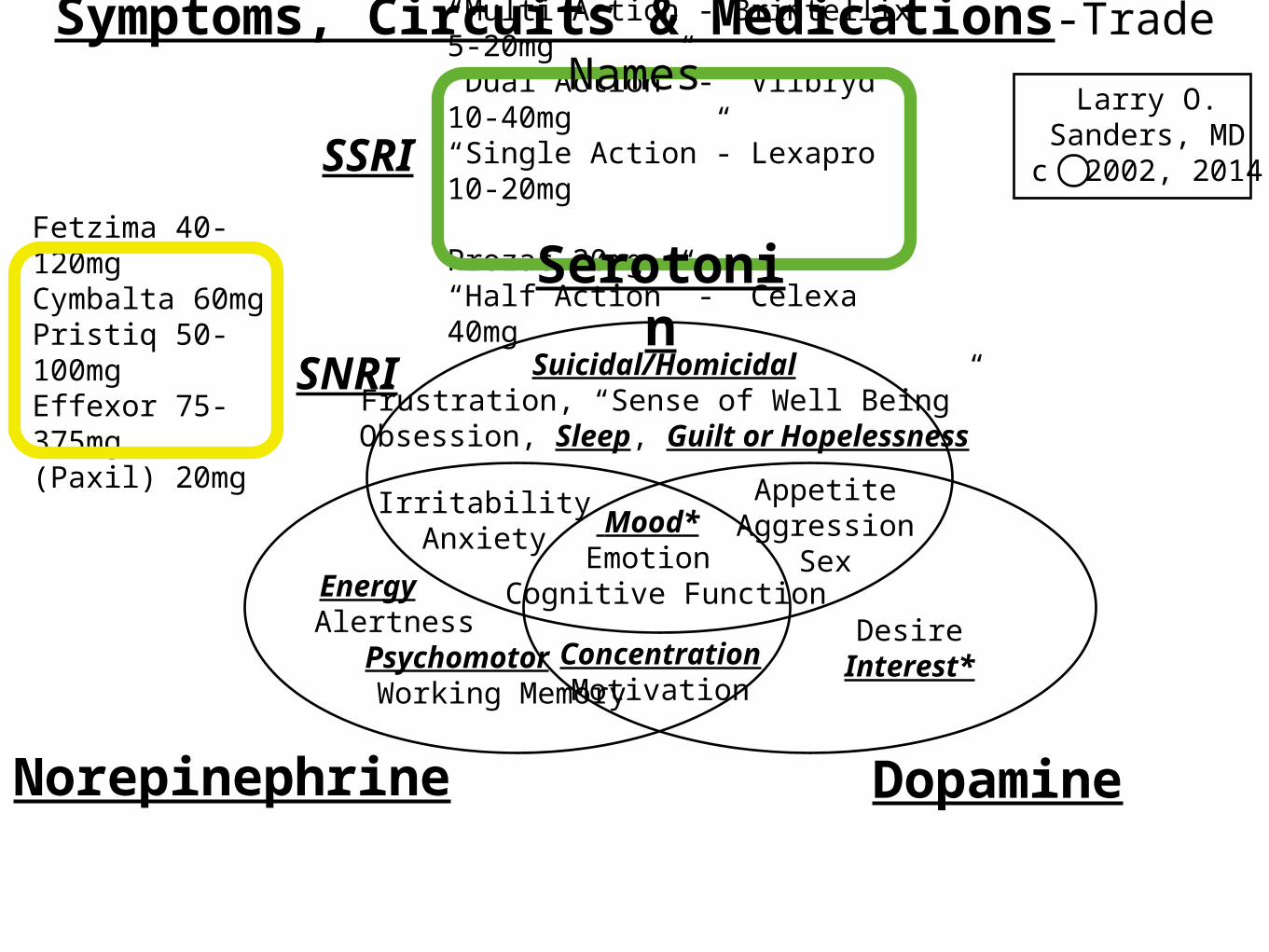
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
NaSSAIndirectly elevates
Norepinephrine (Noradrenaline) and Serotonin
•Mirtazapine (Remeron)
•Sedating, increases appetite and weight gain.
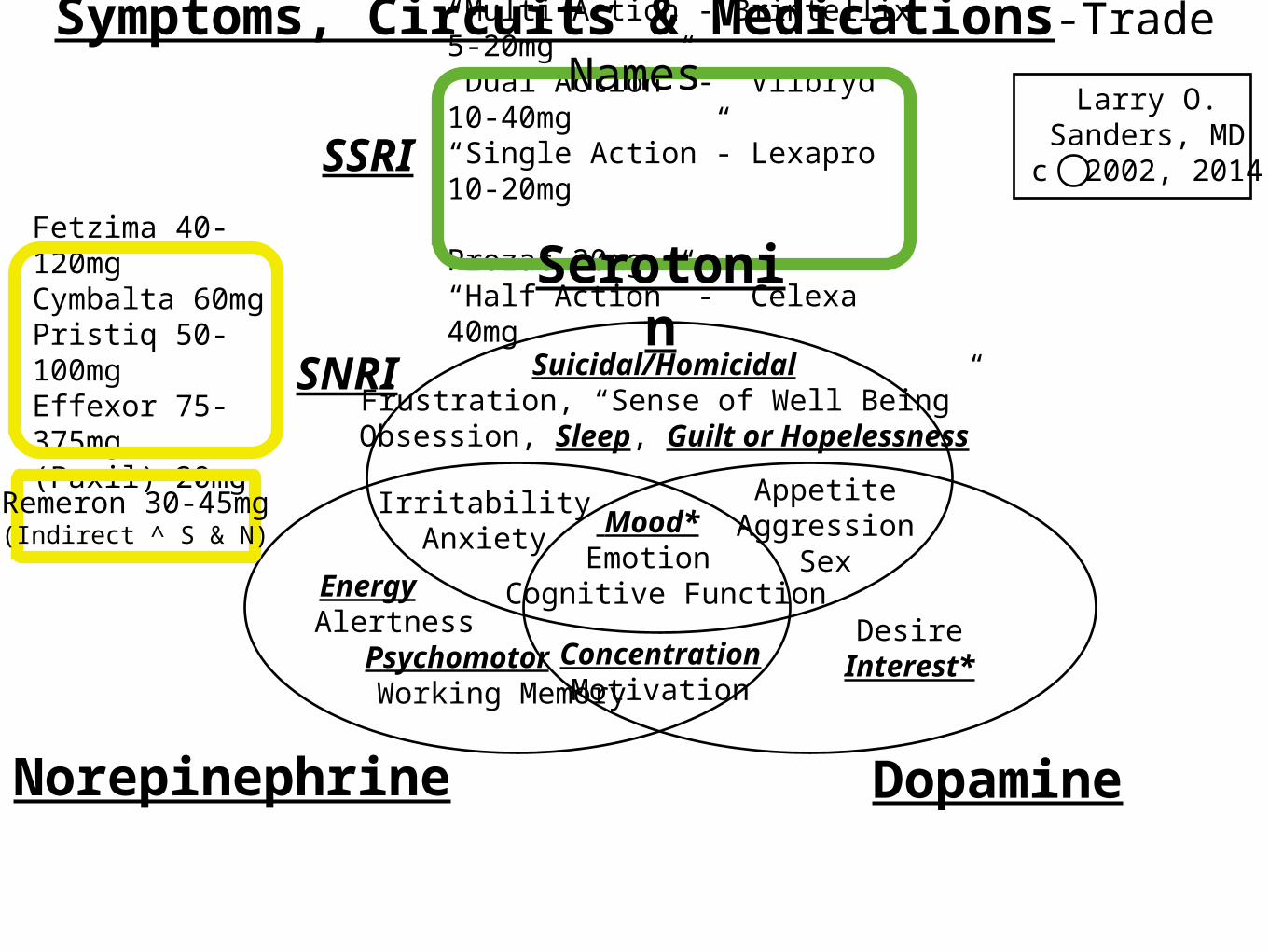
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
Remeron 30-45mg
(Indirect ^ S & N)
Medications Effecting
Norepinephrine and
Dopamine
NDRI
•Bupropion (Wellbutrin) 300-450mg
•IR. Not Well Tolerated.
•SR. Lasts 12 hours.
•XL. Lasts 24 hours.
Amphetamines
•Terminal Releasers
and
•Reuptake Inhibitors
of Norepinephrine and Dopamine
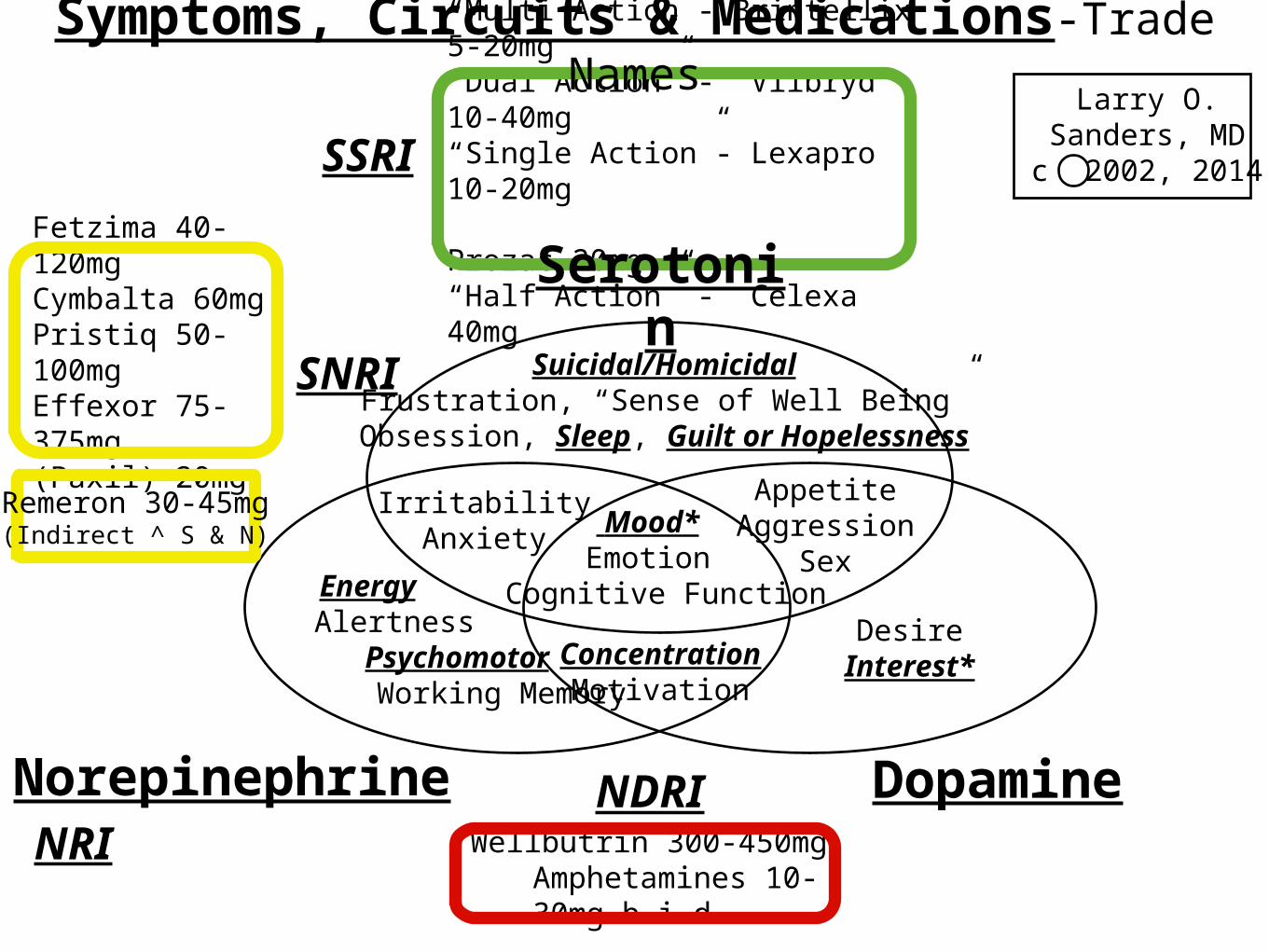
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRINDRI
Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
Remeron 30-45mg
(Indirect ^ S & N)

Medication Effecting
Serotonin and
Dopamine
SDRIs
•Sertraline (Zoloft)
•Usual Dose range 50-200 mg/d
•One of the best tolerated, most effective AD.
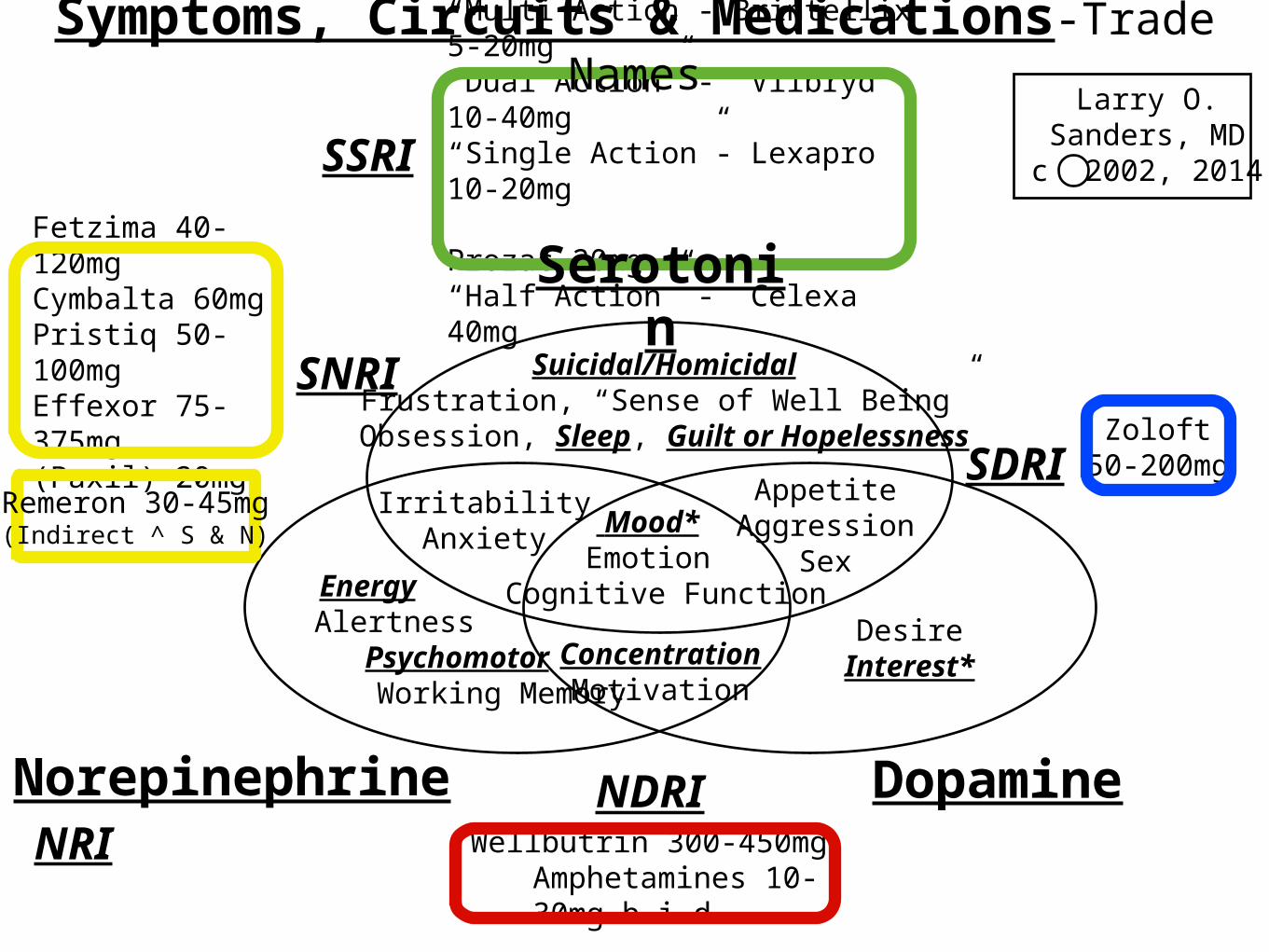
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRINDRI
Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
Remeron 30-45mg
(Indirect ^ S & N)
Medications Effecting Primarily
Dopamine

DRI & DAgs
•Methylphenidate (Ritalin)
•Dopamine Agonists:
•Pramipexole (Mirapex).
•Evidence based treatment. Avg dose 0.95 mg.
•Ropinirole (Requip).
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
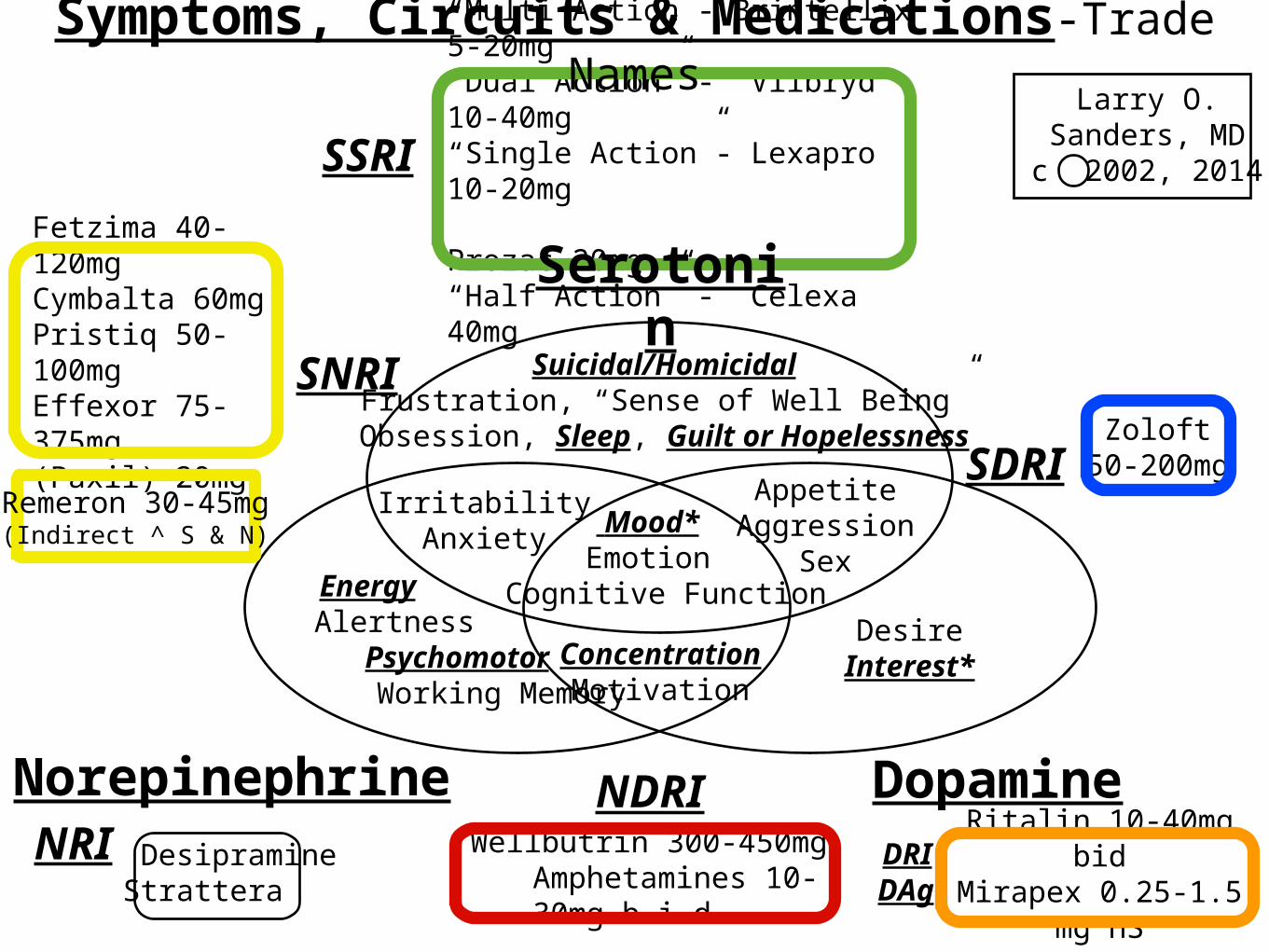
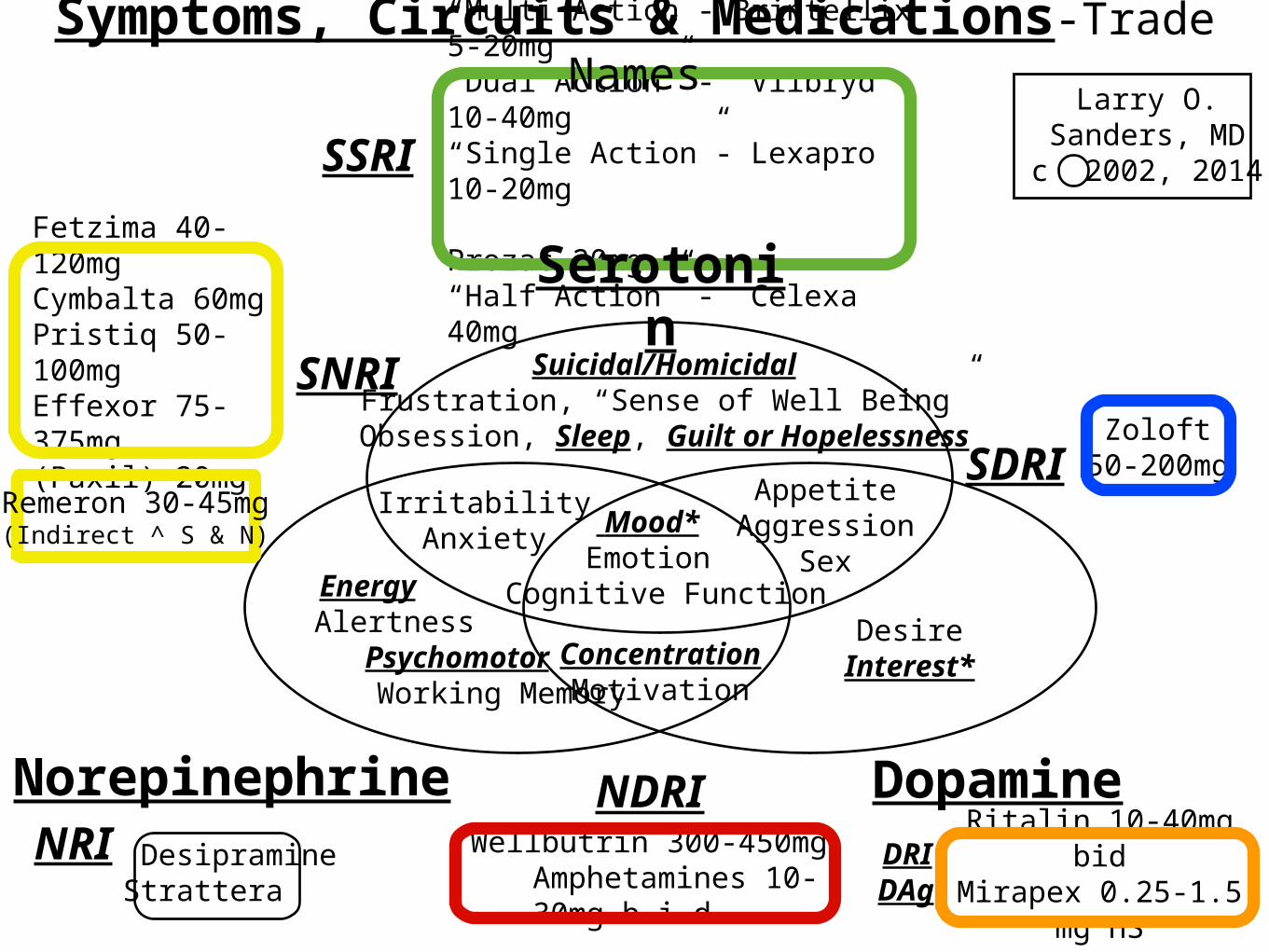
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)

Medications Effecting PrimarilyNorepinephrine
NRIs•Desiparamine
•Atomoxetine (Strattera)
•(Atomoxetine is a failed antidepressant approved for use in AD/HD. No NRI, other than the TCA Desipramine, has beat placebo).
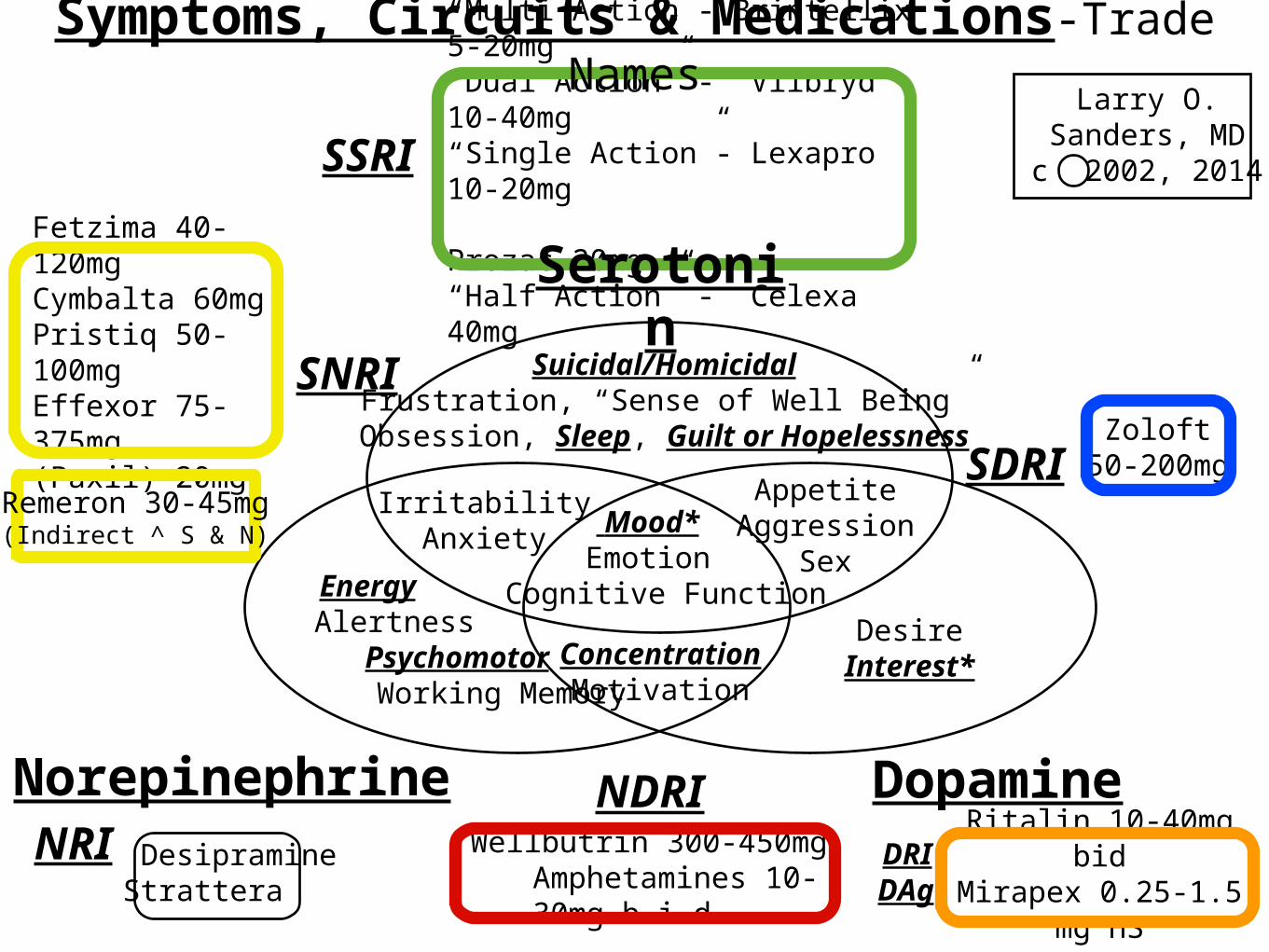
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
“Multi Action”- Brintellix 5-20mg“Dual Action” - Viibryd 10-40mg“Single Action”- Lexapro 10-20mg Prozac 20mg“Half Action” - Celexa 40mg
SSRI
Mood*Emotion
Cognitive Function
ConcentrationMotivation
Suicidal/HomicidalFrustration, “Sense of Well Being”
Obsession, Sleep, Guilt or Hopelessness
Serotonin
Norepinephrine Dopamine
NRI DesipramineStrattera
NDRI Wellbutrin 300-450mg Amphetamines 10-
30mg b.i.d.
DRI Ritalin 10-40mg bidMirapex 0.25-1.5
mg HS
IrritabilityAnxiety
AppetiteAggression
Sex
DesireInterest*
Energy Alertness
Psychomotor Working Memory
SDRI
SNRI
Fetzima 40-120mgCymbalta 60mgPristiq 50-100mgEffexor 75-375mg(Paxil) 20mg Zoloft
50-200mg
Larry O. Sanders, MDc 2002, 2014
Symptoms, Circuits & Medications-Trade Names
DAg
Remeron 30-45mg
(Indirect ^ S & N)
Compliance“No Involvement, No
Commitment”
•Month 1 40% of Patients are off meds.
•Month 2 60% of Patients are off meds.
•S/E-Weight Gain, Sexual Dysfunction, Emotional Blunting, Cognitive Dysfunction.
•Don’t Realize the Condition is Genetic.
•Confusion with Treatment vs Cure.
When 1st Line Fails in MDD
•Refer to Venn Diagram to
•Increase Dose,
•Change Meds or
•Augment.
•5HT1a - Abilify, Seroquel, Viibryd.
•Lithium.
Don’t Underdose!
If dose 50-200, PCP often give 50mg, maybe 75 mg.
“You haven’t reached maximum dose until you have reached effect or intolerable side effects.”
Just When I Learned All of Life’s Answers,
They Changed the Questions!
The Most Common Causes of Treatment Failure
•Non-Compliance.
•Comorbid Anxiety.
•Bipolar Depression.
•Most experts believe that 20-30% of all Depressed Patients have a Bipolar Disorder
•Comorid Substance Abuse
•Depression with Psychosis (47% risk of manifesting BP1 or BP11 with in 10 years).
When is more than MDD Involved?
•Anxiety
•Psychosis
•Mania
•Substance Abuse
Anxiety• Anxiety Disorders are present in 20% PC Pts.
• Depression and Anxiety are HIGHLY Co-Morbid.
• If Depression present, 60% Chance of having Significant Anxiety Disorder AND vice versa.
• Untreated Anxiety consumes
• 6x more of your time &
• 6x more resources.
• Most Antidepressants Treat Anxiety Disorders, but it is Really Important to Know How to Select Proper Medication.
Types of Anxiety Disorders•Generalized Anxiety Disorder (GAD) -
Chronic Worry.
•Social Phobia (aka Social Anxiety) - Fear Social Judgement.
•Panic Disorder - Sudden, Intense Fear with Physical Symptoms.
•Post-traumatic Stress Disorder (PTSD) - symptoms delayed by > 1 month after trauma. Can be years. For every 1 soldier killed in action in Afganistan, 25 will die by suicide.
•Acute Stress Disorder - within 1 month of trauma.
•Obsessive-Compulsive Disorder (OCD) - Germs, Order, Counting, that they have Harmed to Others.
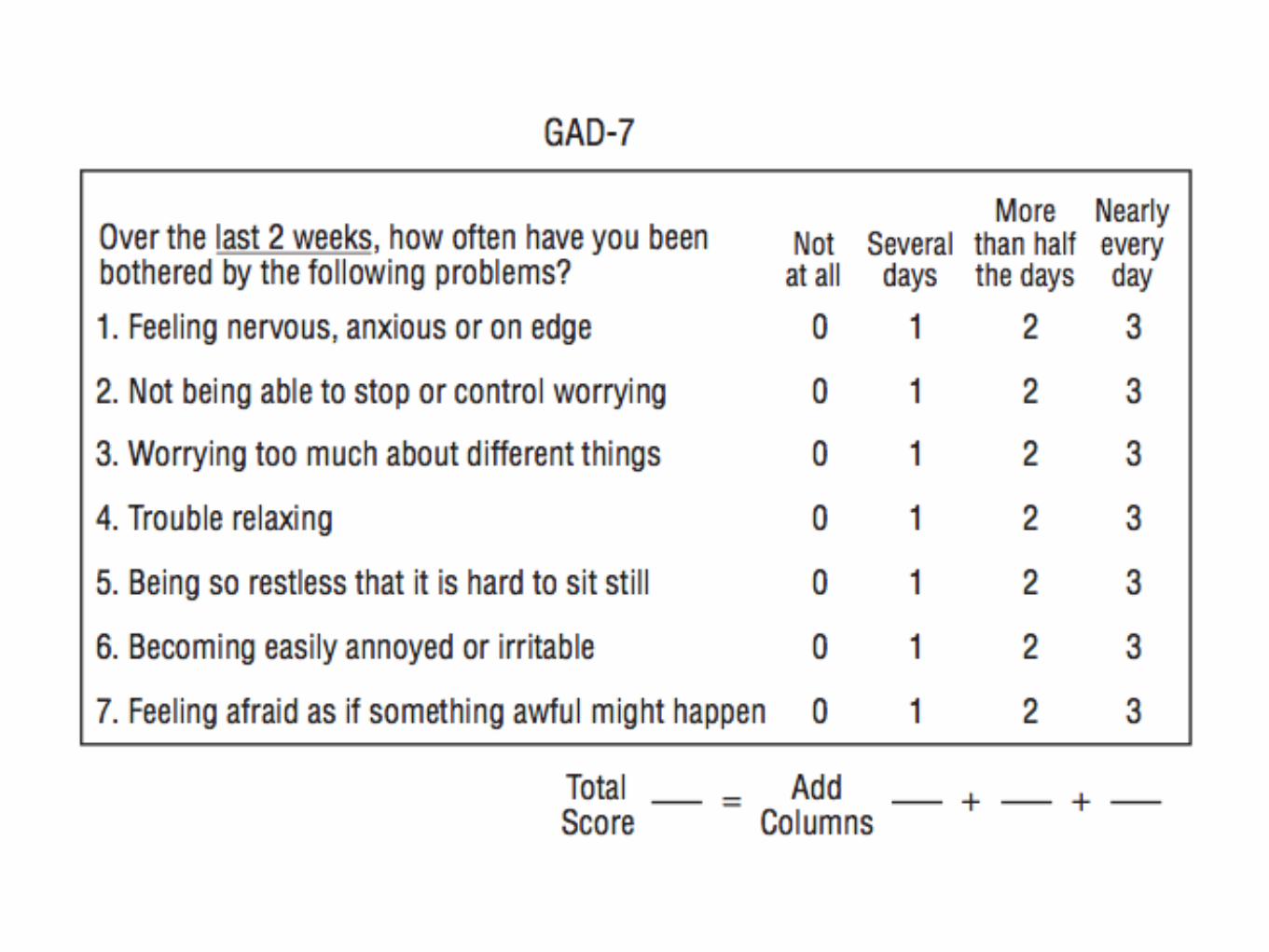
Anxiety Rating Scales
•GAD 7 - Rates GAD
•Zung Anxiety
•CUXOS
•YBOCS - for OCD
Treatment of Anxiety Disorders•Antidepressants
•Serotonin Agents treat all.
•NE helps GAD, but may make Panic Worse.
•BZs
•Gabapentin
Be Certain It’s NOT Bipolar
Depression!
Experts agree that 30-40% of ALL Depressive Disorders
have a component of Bipolar Disorder
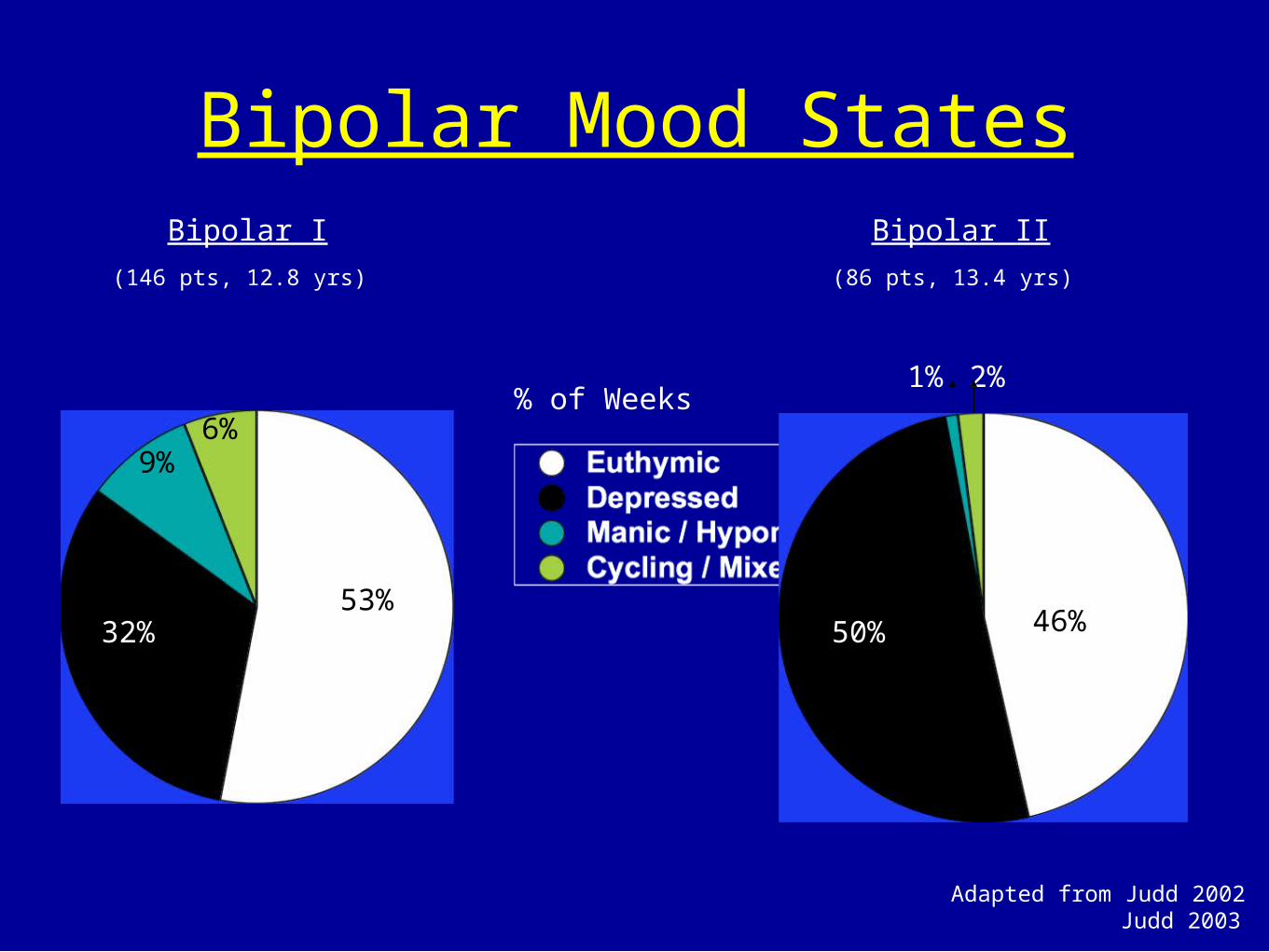
Bipolar Mood States
53%32%
9%6%
50% 46%
1% 2%
Bipolar I Bipolar II
Adapted from Judd 2002 Judd 2003
(146 pts, 12.8 yrs) (86 pts, 13.4 yrs)
% of Weeks
46%46%50% 46%
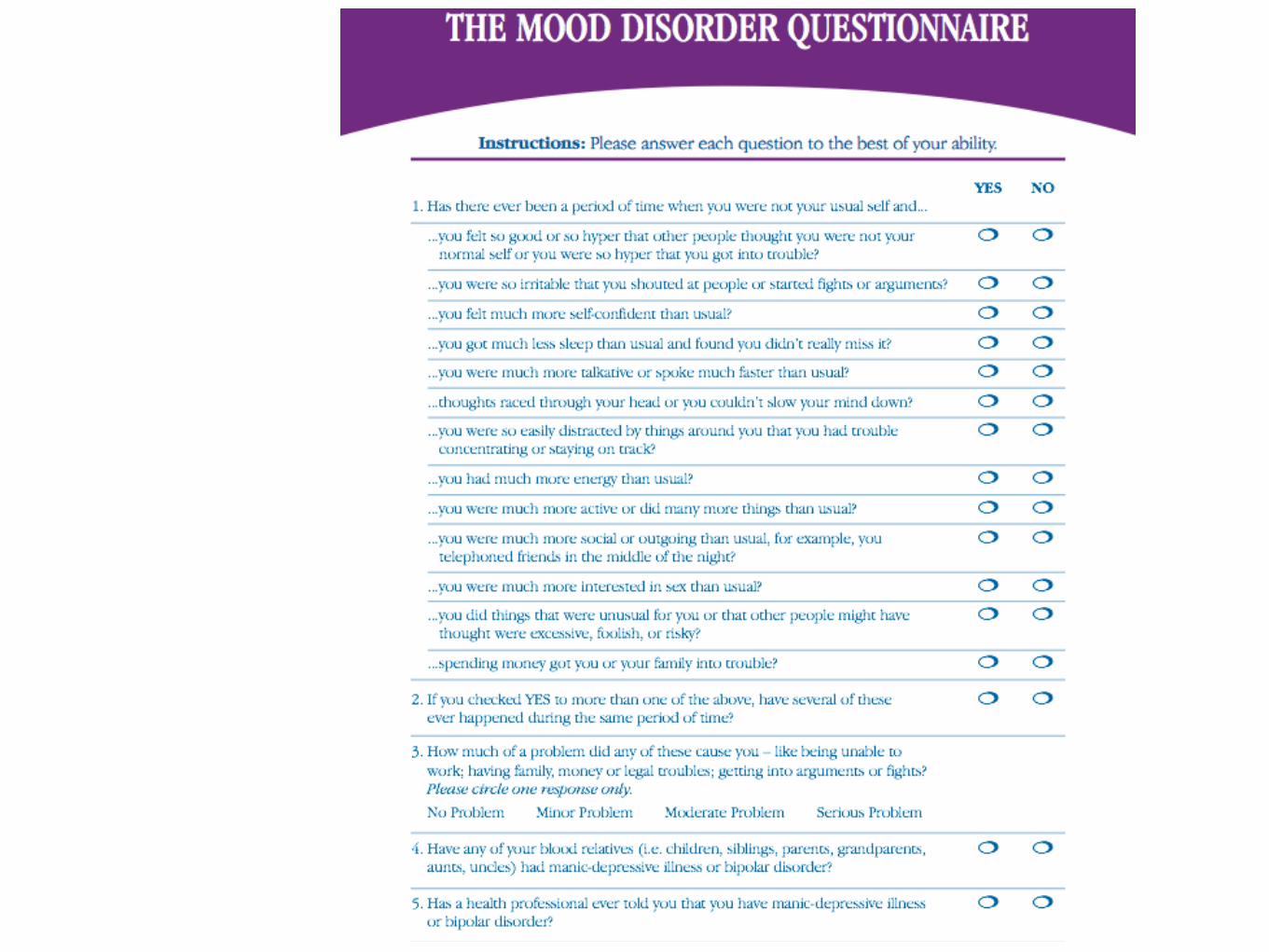
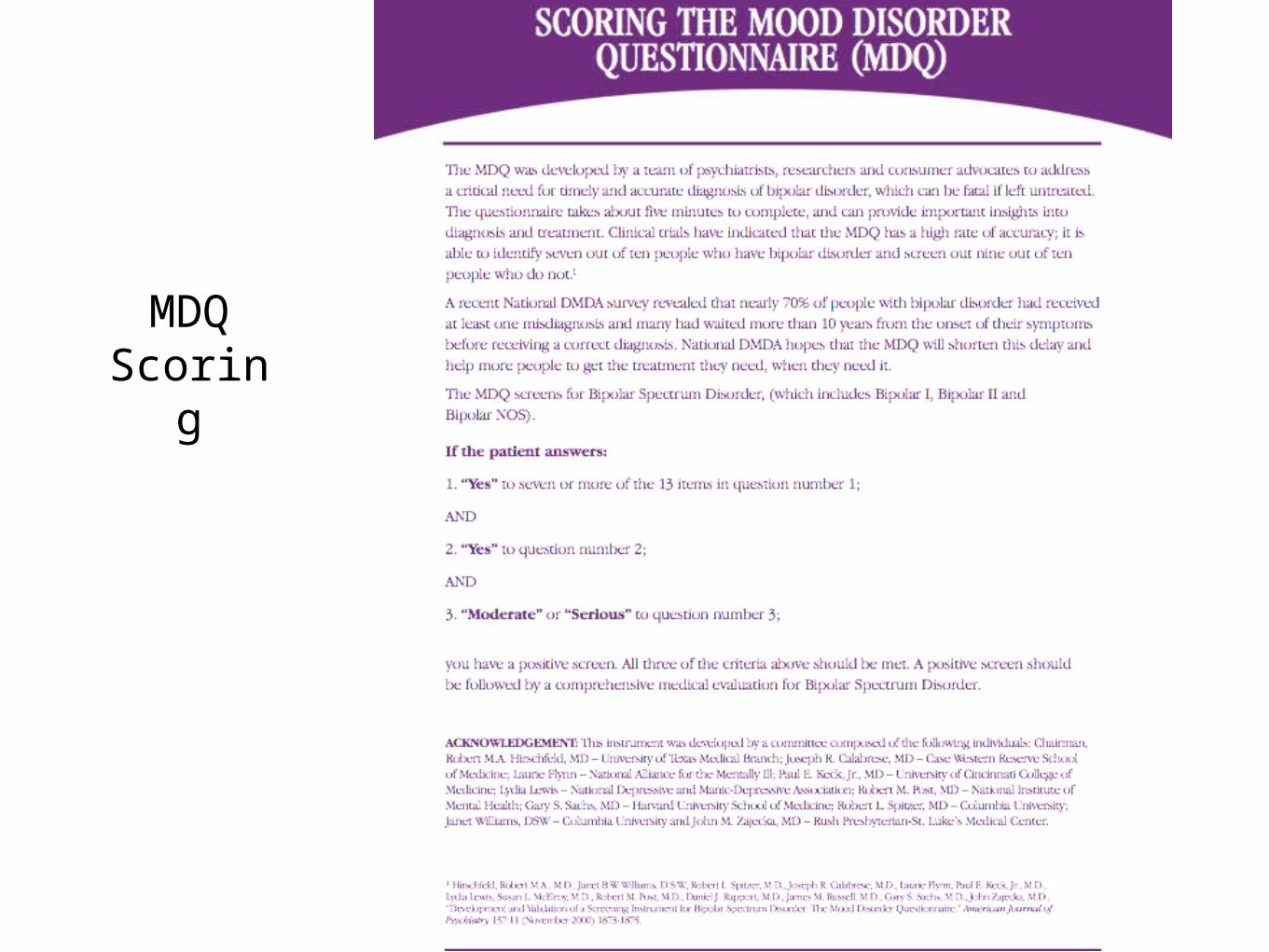
MDQScoring
False Positives and False Negatives
with MDQ
Treating Bipolar Disorder
•Treating Bipolar Disorder is often a Complex Challenge, much more difficult than treating Depression or Anxiety.
•“Every Bipolar is an “n of 1.”
•Must treat Current State and
•Prevent both Mania and Depression.
If Psychotic Depression
•Treat BOTH Psychosis and Mood.
•Psychotic Depression is a High Risk for having an underlying Bipolar Disorder

Non-Medical Treatments
•Individual Psychotherapies
•CBT, Supportive, Psychodynamic.
•Exercise
•Family Therapy
•Group Therapy
When to Refer•Anytime you are uncomfortable.
•When Gravely Disabled, Imminently Suicidal or Homocidal (SEND TO ER!!!)
•Mania is present
•Psychosis present
•Anxiety doesn’t respond rapidly (Suicide Risk)
•When Substance Abuse present
•Therapy Needed or Helpful.
Epitaph of the Hypochondriac(or the Psych Patient)