glen t. steele, o.d. fcovd professor, southern college of ... steele.pdf · why do we do...
TRANSCRIPT
Glen T. Steele, O.D. FCOVDProfessor, Southern College of Optometry
Memphis TNMemphis, TN

Why do we do retinoscopy? “Refraction” limiting the potential Refraction - limiting the potential
information Determining how someone is attempting to Determining how someone is attempting to
obtain information and the amount of energy required and monitor these changes gy q gthrough time - longer observations are necessary
My preference is a spot retinoscope

What makes it so hard for ODs to let go of their deep seated beliefs about refractive findings?
Gerry Getman palsy◦ Gerry Getman – palsy Why have we allowed the rigid medical
model to overtake the observationalmodel to overtake the observational concepts developed by optometry?

The more the retinoscope is used to observe the visual performance of an individual, the more the observer will come to respect and appreciate the dynamics ofto respect and appreciate the dynamics of the total visual system, and all of the influences the total organism will bring intoinfluences the total organism will bring into the visual act. - Getman

All sights, sounds, thoughts, feelings, smells etc evoke responses in andsmells, etc. evoke responses in and throughout all processes
All of these processes are relatedp The responses may be stronger within any
one of us individually and each event may command stronger response than otherscommand stronger response than others.
There may be limitations in any or all of the processes that alter the influence of oneprocesses that alter the influence of one process on another.
The processes do not work in isolation

Refractive status is not static or stable – it is h iever-changing
Retinoscopy is an observation of the variations present in every patientvariations present in every patient
There is a presentation of the retinoscopic reflex that I perceive to be ideal
Patients/people may not consistently show this ideal reflex or may not show it at all
In the presence of a less than ideal reflex i I fi l k f lpresentation, I first look for a lens to move
them toward this ideal Start prescribing where you see the Start prescribing where you see the
baby/patient beginning to engage in the process. For some, simple activities may
ffi F th th f l bsuffice. For others, the use of lenses may be required to allow them to engage. Let near retinoscopy be your guide py y g

Retinoscopy should be our video of what goes into all those things that make upgoes into all those things that make up what we call “refractive state”
Observing the process of effective looking g p grequires patience on the part of the patient – and the optometrist
We often rush to the conclusion – with considerable impatience leading to fr stration if “refraction” is o r primar goalfrustration if “refraction” is our primary goal
AR is an example – slice through time rather than watching over timerather than watching over time

True looking during retinoscopy requires patience and practicepatience and practice
Much can be missed when one limits their brief looks only to a final “number”brief looks only to a final number
Dynamic retinoscopy can give us valuable information about the way the patient is y pselectively “looking” - IF we take the time to “look”

There are small variations shown by every infant and likel e er patient that ha einfant and likely every patient that have meaning during development.
There is evidence suggesting that when There is evidence suggesting that when these variations occur, the patient is exploring differently or under different
t i t th t ifi ll h h thconstraints that specifically change when the exploration changes. From Getman, Forrest, Norton and Smith over several , ,
decades, Should this be different as we develop into
adults – NO!adults – NO!

Social and emotional along with cognitive milestones are heavily based on the baby’s ability to develop the primary visual abilities we observe every daywe observe every day
Sh i i h Shy or anxious with strangers Cries when mother or father leaves Enjoys imitating people in his play j y g p p p y Shows specific preferences for certain people and
toys Tests parental responses to his actions during Tests parental responses to his actions during
feedings Tests parental responses to his behavior
M b f f l i i i May be fearful in some situations Prefers mother and/or regular caregiver over all
others Repeats sounds or gestures for attention Finger-feeds himself Extends arm or leg to help when being dressed Extends arm or leg to help when being dressed
12

13

Explores objects in many different ways ( h ki b i h i d i )(shaking, banging, throwing, dropping)
Finds hidden objects easily L k t t i t h th i i Looks at correct picture when the image is named
Imitates gestures Imitates gestures Begins to use objects correctly (drinking
from cup brushing hair dialing phonefrom cup, brushing hair, dialing phone, listening to receiver)
14
15
Babies who followed the gaze of parents toward an object and made a correspondingtoward an object and made a corresponding sound “understood significantly more words… than those who did not produce thi t” 337 37 194 50this act” 337.37 vs 194.50
Difference noted between open eyes and closed eyes by the parentclosed eyes by the parent The development of gaze following and its relation to language; Brooks
and Meltzoff; Developmental Science 2005 pp 535-543
What does that say about today’s parents at does t at say about today s pa e tswho are texting and twittering while feeding or at other times they should be visually engaging with the baby?engaging with the baby?

“These studies raise the possibility that infant refractive screening can identify not only visual problems, but also potential developmental and learning difficulties ”developmental and learning difficulties.
Infant Hyperopia: Detection, Distribution, Changes and Correlates-Outcomes From the Cambridge Infant Screening Programs.C g S g g
Optometry & Vision Science. 84(2):84-96, February 2007.ATKINSON, JANETTE PhD; BRADDICK, OLIVER PhD; NARDINI, MARKO PhD; ANKER, SHIRLEY BA

What is the human cost in patients who cannot meet the expected cultural demand?◦ ……. and their families?
and their teachers?◦ ……. and their teachers?◦ ……. and their employers?
What about those for whom we might have What about those for whom we might have over-prescribed?
Provide the patient with the best opportunity to complete tasks at nearpointopportunity to complete tasks at nearpoint◦ Engage in initial task Ability - reach
b l Sustainability - grasp Flexibility - manipulate Release Engage in next task◦ Repeatability
How can you find that information with only How can you find that information with only a snapshot or number?
What makes that process more effective? What makes that process more effective?

There are normal variations in development – do not mistake these normal variations for stable refractive measures after a single visit
There are many ways to observe/monitor these variations - Dynamic Retinoscopy, Stress Retinoscopy Bell Retinoscopy Book Retinoscopy MohindraRetinoscopy, Bell Retinoscopy, Book Retinoscopy, Mohindra Retinoscopy, Near Retinoscopy
But there is a need to use the retinoscope to Just Look!

Have the patient look at a near target MAKE IT AN INTERESTING TARGET! Compare right and left eyes before trying to
fdetermine a refractive amount Look at all parts of the retinoscopy reflex
M i i d d i b f Many variations and adaptations before settling into a stable pattern

Myopia, hyperopia and astigmatism can vary measurably throughout the first yearvary measurably throughout the first year.
Refraction may vary as much as6 00 - 8 00 diopters as you watch the baby6.00 8.00 diopters as you watch the baby – Just Look! Retinoscopy
Not from child to child but from an activity Not from child to child but from an activity or mood to other activities or moods
Stop! Look! Compare!P b ith i f l t d t i if Probe with pairs of lenses to determine if you can change a negative appearance to a more positive appearancemore positive appearance
The greater the change with lenses, the greater the likelihood of making a g gdifference in the patient’s life



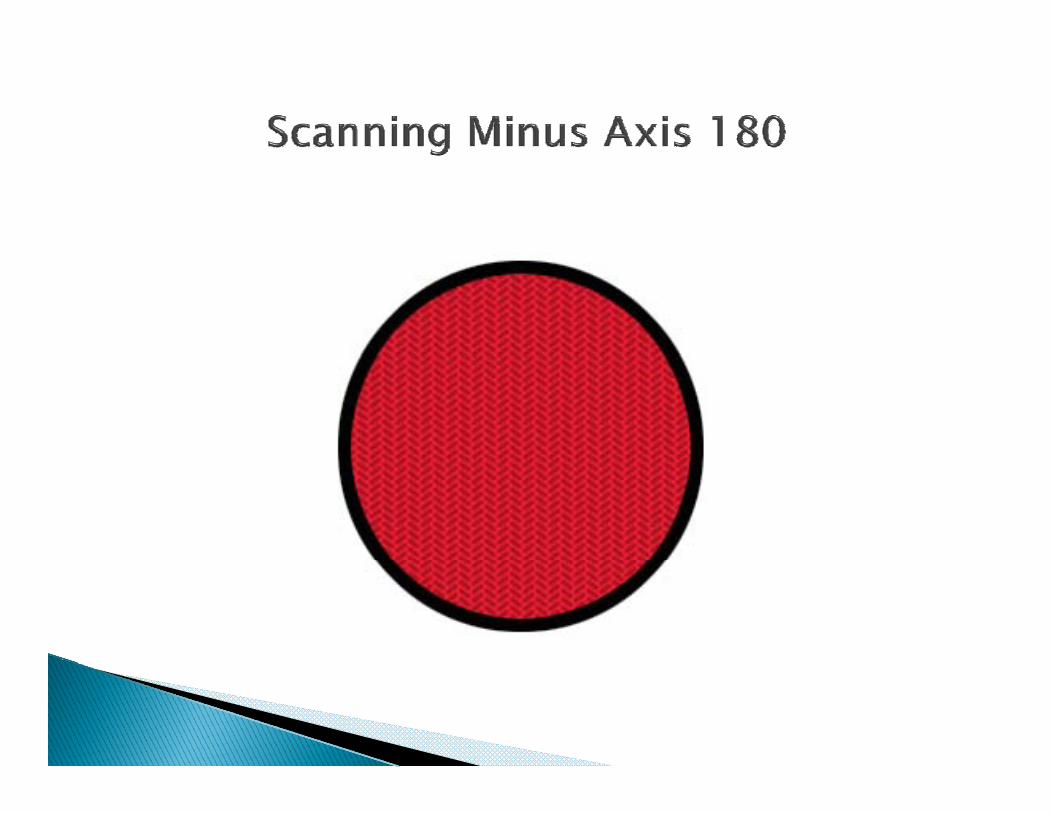


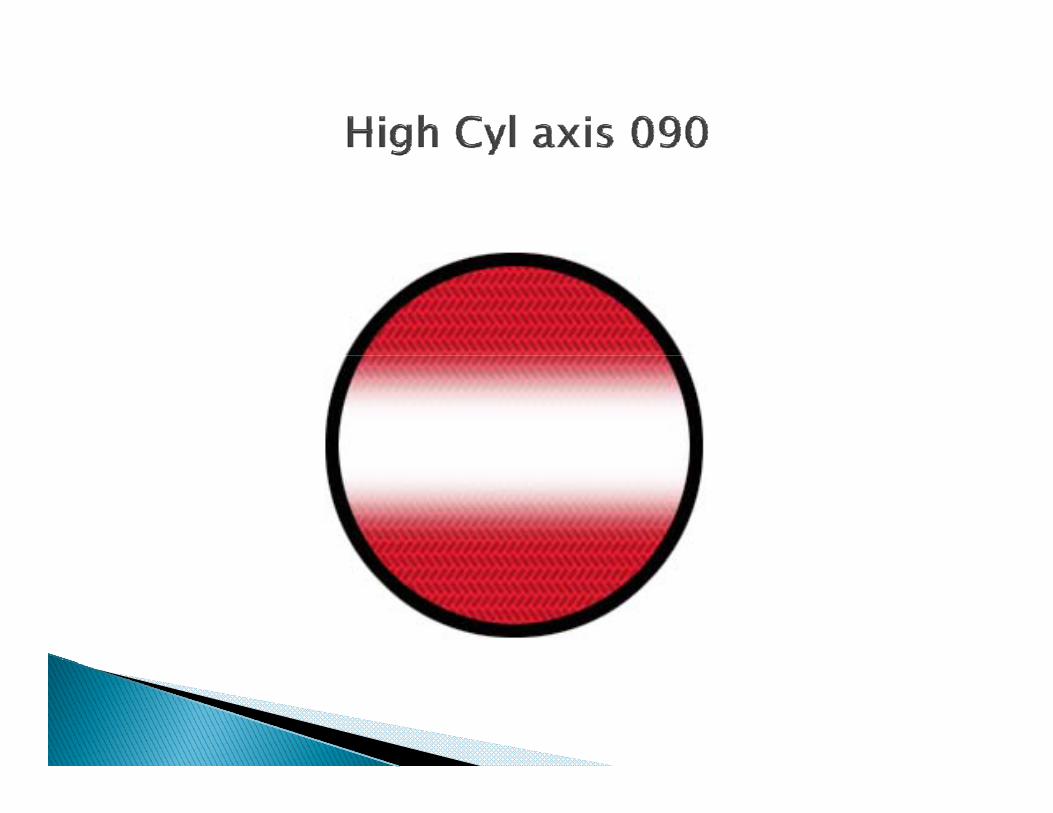

Initially shows –X90 Moves to –X180 Moves to spherical

Scissors motion at near - spherical at intermediate and far
(-) X 90 at near - sph at int and far◦ Playing with cars on a table or high chair
(-) X 180 at near - sph at int at far ( ) X 180 at near sph at int at far◦ Building towers
Spherical at near, int and farW h h h Went through the same process at intermediate and far distances
Pl –6.00 X 090 OU 20/20 Auto accident and in traction Auto accident and in traction C/O difficulty seeing with glasses Pl – 1.25 X 090 20/20/ Limitation of eye movement in the power
meridian is associated with higher bl ti timeasurable astigmatism
..\Emmetropization\Forrest Astigmatism docAstigmatism.doc

One-fourth ping pong ball on laboratory animal’s eye
The part of the retina receiving stimulation h d l hshowed normal growth
The part of the retina with no form stim lation de eloped significant m opiastimulation developed significant myopia

+5.00, -5.00, +10.00, -10.00 Eyes tend to grow toward the stimulus
except for the +10.00 which also grew toward myopia

Ten infant marmosets (8-13 weeks of age) wore soft CTL in one eye on a daily basis for 5-9 weeks
Eyes with hyperopic lenses were more Eyes with hyperopic lenses were more hyperopic (+2.39) and eye with the myopic lenses were more myopic (-2.48)lenses were more myopic ( 2.48)
Fellow eyes were unaffected Plano lenses did not affect eye growthy g

The result of the study makes it more yconvincing that the increasing tendency of children to stay indoors watching televisions, playing computer games or reading books too closely to their eyes can cause short sightednesscause short-sightedness
Ge Jian, director of Zhongshan Ophthalmic Centre under Guangzhou's Sun Yat sen UniversityYat-sen University

10 month oldP t h hi h ti ti◦ Parent has high astigmatism◦ In mother’s lap, child shows moderate to high
astigmatism >3.00 X 180 when casually lookingg y g◦ When looks at near target and hands become
involved, the response is spherical in both eyesWh l b k t ti◦ When relaxes – goes back to astig◦ Will you treat this one the same as one who shows
the cyl all the time?y
Four and ½ month old female – smiling Parents note no problems Parents note no problems Parents are myopic Near retinoscopy inside the baby’s arm’s py y
reach shows less than 1.00 of with motion Moving away from the baby, the motion
gradually decreases around the distance of arm’s reach and into an against motionl h l b d h b b ’ ’ h h Slightly beyond the baby’s arm’s reach, the
motion quickly returns to with and increases in with as the retinoscope isincreases in with as the retinoscope is moved further away
November 200912 h ld b b l il 12 month old baby – normal milestones according to parent
When looking at nearpoint target showed full When looking at nearpoint target, showed full reflex
When released to look at me, marked – X 090 When released to look at me, marked X 090 showed

O.D. O.S.
Born at 26 weeks Released by Retina Clinic Released by Retina Clinic Ocular health: normal Full EOM Full EOM Alignment - IXT dist and ortho at near Ret: OD: - 11.00 OS: - 11.00 Visual Acuity - FDD at 8” Mom’s comments
Hold on Rx LOTS of movement activities LOTS of movement activities Monitor frequently After six months the baby was now showing
-7.00 OU Parent was very aware of the child’s activities
and abilitiesand abilities Rx when the child begins to have difficulty
with ADL This was at age two – Rx - 5.00
Rx OD +7.00 + 0.50 X 090OS +8.50 + 1.00 X 090
Does not like to wear her glasses!!Cannot see airplanesDistance ret – runs up in plus to +7.00 to
+8 00+8.00 First change at distance +5.00 Near ret – stable at +3.50 Near ret stable at +3.50

Ocular motility normaly Four Dots Positive response on KBB without Rxp No apparent movement with 10 pd prism CT aligned w/o Rx on penlightg p g
Goes into ET when accommodative target is Goes into ET when accommodative target is used
Maintains alignment on accommodative Maintains alignment on accommodative target when current Rx is used
Maintains alignment on accommodative gtarget with +3.50
Dilated fundus examination - normal


Rx - +3 50 OU FTW Rx +3.50 OU FTW Binasal patches Three week follow-up Three week follow up

Does not bump into thingsD h ET l h k h Does not show ET unless she takes her glasses off
Positive response on KBB Positive response on KBB No suppression on R/G testing Continue Rx and follow in six weeks
Last seen at age 15 Wearing +0.75/+1.00 add Wanted contact lenses Went into CTL with Pl/+1.00 add Straight A student
l b k b ll d d Plays on basketball team and does not use CTL

These are the things we all have talked about and tried to communicate for well over 60 yearsW k th h h We now know the changes we have observed over the years can be demonstrated with video technologydemonstrated with video technology
Change in attention on video retinoscopy was dramaticwas dramatic

What can we show with newer video technology?gy
Changes in: Attention Manner of response to the task Spherical and meridional differences as the task changes
or attention to the task changes Ability to sustain attention over time Effort required to sustain attention AND get meaning from
the task Alignment when lenses are used In carrier versus on tummy Integration of primitive reflexes?Integration of primitive reflexes? ………. More