glutamate for metabolic intervention in coronary surgery446486/... · 2011. 10. 21. · outcome in...
TRANSCRIPT

Glutamate for Metabolic Intervention in Coronary Surgery

To Elisabet and Per
”You don’t have to go fast, you just have to keep moving” M Lemmel, Race Director Ö till Ö
Örebro Studies in Medicine 58
MÅRTEN VIDLUND
Glutamate for Metabolic Intervention in Coronary Surgery
with special reference to the GLUTAMICS-trial
To Elisabet and Per
”You don’t have to go fast, you just have to keep moving” M Lemmel, Race Director Ö till Ö
Örebro Studies in Medicine 58
MÅRTEN VIDLUND
Glutamate for Metabolic Intervention in Coronary Surgery
with special reference to the GLUTAMICS-trial

© Mårten Vidlund, 2011
Title: Glutamate for Metabolic Intervention in Coronary Surgery.
Publisher: Örebro University 2011
www.publications.oru.se [email protected]
Print: Ineko, Kållered 10/2011
ISSN 1652-4063 ISBN 978-91-7668-824-3
Abstract Mårten Vidlund (2011): Glutamate for Metabolic Intervention in Coronary Surgery with special reference to the GLUTAMICS-trial Örebro Studies in Medicine 58, 87 pp. Myocardial ischemia is a major cause of postoperative heart failure and adverse outcome in coronary artery bypass graft surgery (CABG). Conventional treatment of postoperative heart failure with inotropic drugs may aggravate underlying ischemic injury. Glutamate has been claimed to increase myocardial tolerance to ischemia and promote metabolic and hemodynamic recovery after ischemia. The aim of this work was to investigate if intravenous glutamate infusion given in asso-ciation with CABG for acute coronary syndrome can reduce mortality and prevent or mitigate myocardial injury and postoperative heart failure. We also wanted to assess neurological safety issues, as a concern with the use of glutamate is that it may act as an excitotoxin under certain conditions.
A metabolic strategy for perioperative care was assessed in an observational study on 104 consecutive patients with severe left ventricular dysfunction undergo-ing CABG. Based on encouraging clinical results, unsurpassed in the literature, the GLUTAMICS-trial was initiated. 861 patients undergoing CABG for acute coro-nary syndrome were randomly allocated to blinded intravenous infusion of L-glutamic acid solution or saline. The primary endpoint was a composite of postop-erative mortality (≤30 days), perioperative myocardial infarction and left ventric u-lar heart failure in association with weaning from cardiopulmonary bypass. Secon-dary endpoints included neurological safety issues, degree of myocardial injury, postoperative hemodynamic state, use of circulatory support and cardiac mortality. The event rate was lower than anticipated and the primary endpoint did not differ significantly between the groups. Regarding secondary endpoints there were signifi-cant differences compatible with a beneficial effect of glutamate on post-ischemic myocardial recovery. The putative effect of glutamate infusion was seen in more ischemic patients (CCS class IV) and in patients with evident or anticipated LV-failure on weaning from CPB. No evidence for increased incidence of clinical or subclinical neurological injury was found. In conclusion, intravenous glutamate infusion is safe in the dosages employed and could provide a novel and important way of promoting myocardial recovery after ischemic injury.
Keywords: myocardial ischemia, coronary artery bypass, cardiac surgery, acute coronary syndrome, glutamate, metabolic intervention, postoperative heart failure, myocardial recovery.
Mårten Vidlund, School of Health and Medical Sciences, Örebro University, SE-701 82 Örebro, Sweden, [email protected]

© Mårten Vidlund, 2011
Title: Glutamate for Metabolic Intervention in Coronary Surgery.
Publisher: Örebro University 2011
www.publications.oru.se [email protected]
Print: Ineko, Kållered 10/2011
ISSN 1652-4063 ISBN 978-91-7668-824-3
Abstract Mårten Vidlund (2011): Glutamate for Metabolic Intervention in Coronary Surgery with special reference to the GLUTAMICS-trial Örebro Studies in Medicine 58, 87 pp. Myocardial ischemia is a major cause of postoperative heart failure and adverse outcome in coronary artery bypass graft surgery (CABG). Conventional treatment of postoperative heart failure with inotropic drugs may aggravate underlying ischemic injury. Glutamate has been claimed to increase myocardial tolerance to ischemia and promote metabolic and hemodynamic recovery after ischemia. The aim of this work was to investigate if intravenous glutamate infusion given in asso-ciation with CABG for acute coronary syndrome can reduce mortality and prevent or mitigate myocardial injury and postoperative heart failure. We also wanted to assess neurological safety issues, as a concern with the use of glutamate is that it may act as an excitotoxin under certain conditions.
A metabolic strategy for perioperative care was assessed in an observational study on 104 consecutive patients with severe left ventricular dysfunction undergo-ing CABG. Based on encouraging clinical results, unsurpassed in the literature, the GLUTAMICS-trial was initiated. 861 patients undergoing CABG for acute coro-nary syndrome were randomly allocated to blinded intravenous infusion of L-glutamic acid solution or saline. The primary endpoint was a composite of postop-erative mortality (≤30 days), perioperative myocardial infarction and left ventric u-lar heart failure in association with weaning from cardiopulmonary bypass. Secon-dary endpoints included neurological safety issues, degree of myocardial injury, postoperative hemodynamic state, use of circulatory support and cardiac mortality. The event rate was lower than anticipated and the primary endpoint did not differ significantly between the groups. Regarding secondary endpoints there were signifi-cant differences compatible with a beneficial effect of glutamate on post-ischemic myocardial recovery. The putative effect of glutamate infusion was seen in more ischemic patients (CCS class IV) and in patients with evident or anticipated LV-failure on weaning from CPB. No evidence for increased incidence of clinical or subclinical neurological injury was found. In conclusion, intravenous glutamate infusion is safe in the dosages employed and could provide a novel and important way of promoting myocardial recovery after ischemic injury.
Keywords: myocardial ischemia, coronary artery bypass, cardiac surgery, acute coronary syndrome, glutamate, metabolic intervention, postoperative heart failure, myocardial recovery.
Mårten Vidlund, School of Health and Medical Sciences, Örebro University, SE-701 82 Örebro, Sweden, [email protected]

Swedish summary
Syrebrist i hjärtat är en viktig orsak till hjärtsvikt och negativt utfall efter kranskärlsoperationer. Konventionell behandling av postoperativ hjärtsvikt med inotropa läkemedel kan förvärra den bakomliggande hjärtmuskelska-dan. Glutamat, som är en icke-essentiell aminosyra, har hävdats att öka hjärtats tolerans mot syrebrist och främja den metabola och hemodyna-miska återhämtningen efter syrebrist. Syftet med detta avhandlingsarbete var att undersöka om intravenös glutamatinfusion i samband med krans-kärlsoperation pga akut koronart syndrom kan minska dödligheten och förhindra eller mildra hjärtmuskelskada och postoperativ hjärtsvikt. Vi ville också utvärdera neurologiska säkerhetsaspekter, då glutamat under vissa betingelser anses fungera som ett excitotoxin.
Denna avhandling bygger på en observationell studie och på en prospek-tiv klinisk prövning (GLUTAMICS-studien). I den observationella studien på 104 konsekutiva patienter med svår vänsterkammardysfunktion som genomgick kranskärlsoperation, utvärderades en metabol strategi för peri-operativ vård. Den metabola strategin gick ut på att minska hjärtats syr-gasförbrukning samt att ge metabolt stöd med högdos glukos-insulin-kalium infusion samt glutamatinfusion. Baserat på uppmuntrande kliniska erfarenheter i denna studie planerades GLUTAMICS-studien. I GLUTA-MICS-studien randomiserades 861 patienter som genomgick kranskärls-operation pga. akut koronart syndrom till intravenös infusion av glutamat eller placebo med koksaltlösning. Primär endpoint var kombinationen av postoperativ mortalitet (≤ 30 dagar), perioperativ hjärtinfarkt och vänste r-kammarsvikt i samband med avveckling av hjärt-lungmaskin. Sekundära endpoints omfattade neurologiska säkerhetsaspekter, grad av hjärtmu-skelskadaskada, postoperativ hemodynamik, användning av cirkulatoriskt stöd och kardiell mortalitet. Resultaten visade ingen signifikant skillnad på primär endpoint mellan grupperna. Beträffande sekundära endpoints fanns signifikanta skillnader som talade för en gynnsam effekt av glutamat på hjärtats återhämtning efter syrebrist. Den förmodade effekten av glutamat-infusionen sågs hos de patienterna med svårast kärlkramp (CCS klass IV) innan operationen samt hos patienter med uppenbar eller förväntad väns-terkammarsvikt i samband med avveckling av hjärt-lungmaskin. Vi fann ingen ökad incidens av kliniska eller subkliniska neurologiska skador eller andra biverkningar hos patienter som erhöll glutamatinfusion.
Sammanfattningsvis kan intravenös glutamatinfusion visa sig bli ett vik-tigt och skonsamt sätt att befrämja hjärtats återhämtning efter skada orsa-kad av syrebrist.

Swedish summary
Syrebrist i hjärtat är en viktig orsak till hjärtsvikt och negativt utfall efter kranskärlsoperationer. Konventionell behandling av postoperativ hjärtsvikt med inotropa läkemedel kan förvärra den bakomliggande hjärtmuskelska-dan. Glutamat, som är en icke-essentiell aminosyra, har hävdats att öka hjärtats tolerans mot syrebrist och främja den metabola och hemodyna-miska återhämtningen efter syrebrist. Syftet med detta avhandlingsarbete var att undersöka om intravenös glutamatinfusion i samband med krans-kärlsoperation pga akut koronart syndrom kan minska dödligheten och förhindra eller mildra hjärtmuskelskada och postoperativ hjärtsvikt. Vi ville också utvärdera neurologiska säkerhetsaspekter, då glutamat under vissa betingelser anses fungera som ett excitotoxin.
Denna avhandling bygger på en observationell studie och på en prospek-tiv klinisk prövning (GLUTAMICS-studien). I den observationella studien på 104 konsekutiva patienter med svår vänsterkammardysfunktion som genomgick kranskärlsoperation, utvärderades en metabol strategi för peri-operativ vård. Den metabola strategin gick ut på att minska hjärtats syr-gasförbrukning samt att ge metabolt stöd med högdos glukos-insulin-kalium infusion samt glutamatinfusion. Baserat på uppmuntrande kliniska erfarenheter i denna studie planerades GLUTAMICS-studien. I GLUTA-MICS-studien randomiserades 861 patienter som genomgick kranskärls-operation pga akut koronart syndrom till blindad intravenös infusion av glutamat eller placebo (koksaltlösning). Primär endpoint var kombinatio-nen av postoperativ mortalitet (≤ 30 dagar), perioperativ hjärtinfarkt och vänsterkammarsvikt i samband med avveckling av hjärt-lungmaskin. Se-kundära endpoints omfattade neurologiska säkerhetsaspekter, grad av hjärtmuskelskadaskada, postoperativ hemodynamik, användning av cirku-latoriskt stöd och kardiell mortalitet. Resultaten visade ingen signifikant skillnad avseende primär endpoint mellan grupperna. Beträffande sekundä-ra endpoints fanns signifikanta skillnader som talade för en gynnsam effekt av glutamat på hjärtats återhämtning efter syrebrist. Den förmodade effek-ten av glutamatinfusion sågs hos patienterna med svårast kärlkramp (CCS klass IV) innan operationen samt hos patienterna med uppenbar eller för-väntad vänsterkammarsvikt vid avveckling av hjärt-lungmaskin. Vi fann ingen ökad incidens av kliniska eller subkliniska neurologiska skador eller andra biverkningar hos patienter som fick glutamatinfusion.
Sammanfattningsvis kan intravenös glutamatinfusion visa sig bli ett vik-tigt och skonsamt sätt att befrämja hjärtats återhämtning efter skada orsa-kad av syrebrist.

Table of contents
LIST OF ORIGINAL PAPERS ................................................................. 11
ABBREVIATIONS ................................................................................... 12
1 BACKGROUND ................................................................................... 13 1.1 Introduction ....................................................................................... 13 1.2 Myocardial ischemia and cardiac surgery .......................................... 13 1.3 Metabolic strategy in cardiac surgery ................................................. 14 1.4 Glutamate .......................................................................................... 15 1.5 Glutamate for metabolic intervention in coronary surgery ................. 17
2 AIMS OF THE THESIS ........................................................................ 19
3 PATIENTS AND METHODS ............................................................... 21 3.1 Patients .............................................................................................. 21 3.2 GLUTAMICS-trial ............................................................................. 24 3.3 Post-hoc analysis ................................................................................ 26 3.4 Clinical management .......................................................................... 26 3.5 Metabolic intervention ....................................................................... 28 3.6 Data collection ................................................................................... 29 3.7 Biochemical analyses .......................................................................... 30 3.8 Hemodynamic measurements ............................................................. 31 3.9 Definitions ......................................................................................... 31 3.10 Statistics ........................................................................................... 32 3.11 Ethics ............................................................................................... 33
4 RESULTS .............................................................................................. 35 4.1 Observational study on a metabolic strategy (Paper I) ....................... 35 4.2 S-100B substudy of the GLUTAMICS-trial (Paper II) ........................ 39 4.3 Results of the GLUTAMICS-trial (Paper III) ...................................... 42 4.4 The influence of inotropes in the GLUTAMICS-trial (Paper IV) ........ 51
5 GENERAL DISCUSSION ..................................................................... 57 5.1 Metabolic strategy in CABG patients with LV-dysfunction................ 58 5.2 The GLUTAMICS-trial ...................................................................... 60 5.3 The influence of inotropic drugs in the GLUTAMICS-trial ................ 62 5.4 Defining postoperative heart failure ................................................... 64 5.5 Biochemical mechanisms of glutamate ............................................... 65 5.6 Adverse events .................................................................................... 67 5.7 Limitations ......................................................................................... 68 5.8 Clinical perspectives ........................................................................... 68
Table of contents
LIST OF ORIGINAL PAPERS ................................................................. 11
ABBREVIATIONS ................................................................................... 12
1 BACKGROUND ................................................................................... 13 1.1 Introduction ....................................................................................... 13 1.2 Myocardial ischemia and cardiac surgery .......................................... 13 1.3 Metabolic strategy in cardiac surgery ................................................. 14 1.4 Glutamate .......................................................................................... 15 1.5 Glutamate for metabolic intervention in coronary surgery ................. 17
2 AIMS OF THE THESIS ........................................................................ 19
3 PATIENTS AND METHODS ............................................................... 21 3.1 Patients .............................................................................................. 21 3.2 GLUTAMICS-trial ............................................................................. 24 3.3 Post-hoc analysis ................................................................................ 26 3.4 Clinical management .......................................................................... 26 3.5 Metabolic intervention ....................................................................... 28 3.6 Data collection ................................................................................... 29 3.7 Biochemical analyses .......................................................................... 30 3.8 Hemodynamic measurements ............................................................. 31 3.9 Definitions ......................................................................................... 31 3.10 Statistics ........................................................................................... 32 3.11 Ethics ............................................................................................... 33
4 RESULTS .............................................................................................. 35 4.1 Observational study on a metabolic strategy (Paper I) ....................... 35 4.2 S-100B substudy of the GLUTAMICS-trial (Paper II) ........................ 39 4.3 Results of the GLUTAMICS-trial (Paper III) ...................................... 42 4.4 The influence of inotropes in the GLUTAMICS-trial (Paper IV) ........ 51
5 GENERAL DISCUSSION ..................................................................... 57 5.1 Metabolic strategy in CABG patients with LV-dysfunction................ 58 5.2 The GLUTAMICS-trial ...................................................................... 60 5.3 The influence of inotropic drugs in the GLUTAMICS-trial ................ 62 5.4 Defining postoperative heart failure ................................................... 64 5.5 Biochemical mechanisms of glutamate ............................................... 65 5.6 Adverse events .................................................................................... 67 5.7 Limitations ......................................................................................... 68 5.8 Clinical perspectives ........................................................................... 68

SUMMARY ............................................................................................. 71
CONCLUSIONS ...................................................................................... 73
ACKNOWLEDGEMENTS ...................................................................... 75
REFERENCES ......................................................................................... 77
PAPER I–IV.............................................................................................. 89
APPENDIX .............................................................................................. 00
11
List of original papers
I. Svedjeholm R, Vidlund M, Vanhanen I, Håkanson E. A meta-bolic protective strategy could improve long-term survival in patients with LV-dysfunction undergoing CABG. Scand Car-diovasc J 2010;44:45-58.
II. Vidlund M, Holm J, Håkanson E, Friberg Ö, Sunnermalm L,
Vanky F, Svedjeholm R. The S-100B substudy of the GLU-TAMICS-trial: Glutamate infusion not associated with sus-tained elevation of plasma S-100B after coronary surgery. Clin Nutr 2009;21:358-64.
III. Vidlund M, Håkanson E, Friberg Ö, Juhl-Andersen S, Holm J,
Vanky F, Sunnermalm L, Borg J, Sharma R, Svedjeholm R. GLUTAMICS-A randomized clinical trial on glutamate infu-sion in patients operated for acute coronary syndrome. Submitted.
IV. Vidlund M, Håkanson E, Friberg Ö, Holm J, Sunnermalm L,
Vanky F, Svedjeholm R. The influence of inotropic drugs on the outcome of the GLUTAMICS-trial. Manuscript.
167

SUMMARY ............................................................................................. 71
CONCLUSIONS ...................................................................................... 73
ACKNOWLEDGEMENTS ...................................................................... 75
REFERENCES ......................................................................................... 77
PAPER I–IV.............................................................................................. 89
APPENDIX .............................................................................................. 00
11
List of original papers
I. Svedjeholm R, Vidlund M, Vanhanen I, Håkanson E. A meta-bolic protective strategy could improve long-term survival in patients with LV-dysfunction undergoing CABG. Scand Car-diovasc J 2010;44:45-58.
II. Vidlund M, Holm J, Håkanson E, Friberg Ö, Sunnermalm L,
Vanky F, Svedjeholm R. The S-100B substudy of the GLU-TAMICS-trial: Glutamate infusion not associated with sus-tained elevation of plasma S-100B after coronary surgery. Clin Nutr 2009;21:358-64.
III. Vidlund M, Håkanson E, Friberg Ö, Juhl-Andersen S, Holm J,
Vanky F, Sunnermalm L, Borg J, Sharma R, Svedjeholm R. GLUTAMICS-A randomized clinical trial on glutamate infu-sion in patients operated for acute coronary syndrome. Submitted.
IV. Vidlund M, Håkanson E, Friberg Ö, Holm J, Sunnermalm L,
Vanky F, Svedjeholm R. The influence of inotropic drugs on the outcome of the GLUTAMICS-trial. Manuscript.

12
Abbreviations ATP adenosine triphosphate BMI body mass index CABG coronary artery bypass graft CCS Canadian Cardiovascular Society CI confidence interval CK-MB creatine kinase-muscular band CO cardiac output COPD chronic obstructive pulmonary disease CPB cardiopulmonary bypass CT computed tomography ECG electrocardiogram FFA free fatty acid GIK glucose-insulin-potassium IABP intra-aortic balloon pump ICU intensive care unit LV left ventricular LVEF left ventricular ejection fraction LVSWI left ventricular stroke work index NT-proBNP N-terminal pro-brain natriuretic peptide OPCAB off pump coronary artery bypass OR odds ratio SD standard deviation STS Society of Thoracic Surgeons
13
1 Background
1.1 Introduction Ischemia of some degree is unavoidable in association with cardiac surgery. It is conceivable that ischemic myocardial injury and heart failure was common in the early days of cardiac surgery before modern techniques of myocardial protection were developed. However, there is surprisingly little documentation about postoperative heart failure or low cardiac output syndrome. In 1967 J Kirklin noted that when death occurs early after car-diac surgery it is often related to low cardiac output1. In spite of the pro-gress in cardiac surgery and perioperative management postoperative heart failure remains a leading cause of death. O’Connor found postoperative heart failure to account for almost two thirds of all in-hospital deaths in a survey of 8641 patients undergoing CABG2.
Although acknowledged as a major problem in cardiac surgery there are no generally accepted criteria for the diagnosis of postoperative heart fail-ure. This in turn could explain why treatment for postoperative heart fail-ure is poorly documented with regard to clinical outcome3-5.
The causes and mechanisms for postoperative heart failure have also re-ceived limited attention. From a therapeutic aspect, it appears as if postop-erative heart failure is regarded mainly as an issue of myocardial stunning that can be alleviated by inotropic drugs. Given that inotropic drugs in-crease oxygen expenditure excessively in relation to the increase in cardiac output such an approach may not be ideal for all patients. It has been demonstrated that ischemia and evolving myocardial infarction account for a large proportion of patients with postoperative heart failure after CABG3,
6, 7. In animal models inotropic agents not only aggravate ischemia and increase the size of evolving myocardial infarction, but also stimulate apop-totic processes8, 9.
1.2 Myocardial ischemia and cardiac surgery As late as 1965 myocardial necrosis was not recognized as a cause of post-operative complications in cardiac surgery10, 11. In 1967 Morales and Taber suggested that patchy areas of myocardial necrosis was the cause of post-operative heart failure in patients dying early after cardiac surgery12. In 1985 Slogoff and Keats demonstrated that perioperative ischemia prior to cardiopulmonary bypass (CPB) was the main cause of myocardial infarc-tion after CABG13. It was also shown that the incidence of postoperative myocardial infarction was closely related to the perioperative management

12
Abbreviations ATP adenosine triphosphate BMI body mass index CABG coronary artery bypass graft CCS Canadian Cardiovascular Society CI confidence interval CK-MB creatine kinase-muscular band CO cardiac output COPD chronic obstructive pulmonary disease CPB cardiopulmonary bypass CT computed tomography ECG electrocardiogram FFA free fatty acid GIK glucose-insulin-potassium IABP intra-aortic balloon pump ICU intensive care unit LV left ventricular LVEF left ventricular ejection fraction LVSWI left ventricular stroke work index NT-proBNP N-terminal pro-brain natriuretic peptide OPCAB off pump coronary artery bypass OR odds ratio SD standard deviation STS Society of Thoracic Surgeons
13
1 Background
1.1 Introduction Ischemia of some degree is unavoidable in association with cardiac surgery. It is conceivable that ischemic myocardial injury and heart failure was common in the early days of cardiac surgery before modern techniques of myocardial protection were developed. However, there is surprisingly little documentation about postoperative heart failure or low cardiac output syndrome. In 1967 J Kirklin noted that when death occurs early after car-diac surgery it is often related to low cardiac output1. In spite of the pro-gress in cardiac surgery and perioperative management postoperative heart failure remains a leading cause of death. O’Connor found postoperative heart failure to account for almost two thirds of all in-hospital deaths in a survey of 8641 patients undergoing CABG2.
Although acknowledged as a major problem in cardiac surgery there are no generally accepted criteria for the diagnosis of postoperative heart fail-ure. This in turn could explain why treatment for postoperative heart fail-ure is poorly documented with regard to clinical outcome3-5.
The causes and mechanisms for postoperative heart failure have also re-ceived limited attention. From a therapeutic aspect, it appears as if postop-erative heart failure is regarded mainly as an issue of myocardial stunning that can be alleviated by inotropic drugs. Given that inotropic drugs in-crease oxygen expenditure excessively in relation to the increase in cardiac output such an approach may not be ideal for all patients. It has been demonstrated that ischemia and evolving myocardial infarction account for a large proportion of patients with postoperative heart failure after CABG3,
6, 7. In animal models inotropic agents not only aggravate ischemia and increase the size of evolving myocardial infarction, but also stimulate apop-totic processes8, 9.
1.2 Myocardial ischemia and cardiac surgery As late as 1965 myocardial necrosis was not recognized as a cause of post-operative complications in cardiac surgery10, 11. In 1967 Morales and Taber suggested that patchy areas of myocardial necrosis was the cause of post-operative heart failure in patients dying early after cardiac surgery12. In 1985 Slogoff and Keats demonstrated that perioperative ischemia prior to cardiopulmonary bypass (CPB) was the main cause of myocardial infarc-tion after CABG13. It was also shown that the incidence of postoperative myocardial infarction was closely related to the perioperative management

14
of ischemia13. The role of myocardial ischemia for precipitating postopera-tive myocardial infarction and postoperative heart failure after CABG has been confirmed by other investigators6, 7, 14. Whereas perioperative myocar-dial ischemia plays a key role for outcome after CABG the role of ischemia for eliciting postoperative heart failure after valve surgery appears to be of secondary importance6, 7. Occurrence of perioperative myocardial infarc-tion is less frequent and other factors than ischemia account for the major proportion of cases with postoperative heart failure after valve surgery6, 7,
14. In patients undergoing CABG those with unstable angina are particu-
larly prone to perioperative ischemia and the risk for development of per-manent myocardial injury14-16. Patients that arrive to surgery with limited cardiac reserve i.e. preoperatively compromised left ventricular function are particularly likely to require treatment for postoperative heart failure17,
18.
1.3 Metabolic strategy in cardiac surgery Besides using conventional pharmacological treatment, an alternative ap-proach to prevent and treat postoperative heart failure could involve ad-herence to physiological principles to minimize myocardial and systemic oxygen expenditure, and specific measures such as metabolic interventions with glutamate and high-dose GIK to increase myocardial tolerance to ischemia and facilitate myocardial recovery after ischemia. Glucose-Insulin-Potassium (GIK) Over the last few years the debate regarding the salutary effects of insulin in association with cardiac surgery has focused on blood glucose control19-
23. However, none of these studies have been designed to identify the mechanisms behind the success of blood glucose control or to discriminate between the effects of insulin per se or the effects of blood glucose control. Beyond blood glucose control insulin has several potentially beneficial effects in the post-traumatic state including direct and indirect influence on systemic and myocardial metabolism, hemodynamic state, inflammatory response, endothelia function, coagulation and apoptosis.
Basic research suggests that glucose is important for the preservation of mechanical function, structure, histology and ionic balance during ische-mia24, 25. It appears that moderate doses of insulin can suffice to achieve blood glucose control and suppression of plasma FFAs after cardiac sur-gery. Although it is probable that moderate doses of insulin have a benefi-
15
cial effect on myocardial metabolism, direct effects on myocardial metabo-lism have so far only been documented with high-dose GIK (1 IU/kg bodyweight and hour). Assessed with coronary sinus catheter technique a shift in myocardial uptake of substrates from FFA to glucose has been demonstrated not only in elective CABG patients, but also in patients treated with catecholamines after CABG and in diabetic patients undergo-ing CABG26-28.
In experimental models insulin has been shown to have both inotropic29-
31 and vasodilatory properties32-35. Intraoperative assessment has confirmed beneficial effects on hemodynamic state with improved cardiac output28, 36-
44, improved LVSWI37, 38, less reduction in left ventricular ejection fraction measured by nuclear angiography45, improved central venous oxygen satu-ration46, fewer episodes of low cardiac output47, and less need for ino-tropes39, 40, 47-49.
In contrast to inotropic agents, this improvement has been achieved without excessive increase of myocardial oxygen demand38 or myocardial oxygen consumption measured by coronary sinus catheters50. The after-load reducing vasodilatory effect has been pronounced in studies using high-dose GIK43, 51, 52 and it appears that this vasodilation is not explained by luxury perfusion of skeletal muscle41. The inotropic effect has been more difficult to discriminate in the clinical setting after cardiac surgery but interestingly echocardiographic studies have shown improvement of regional myocardial function in patients with acute myocardial infarction53,
54.
1.4 Glutamate Glutamate, C5H9NO4, is a genetically coded non-essential acidic amino acid. Glutamate is the salt of glutamic acid of which there are two forms, L-glutamic acid and D-glutamic acid. The only form of glutamic acid found in higher organisms and in proteins is L-glutamic acid, whereas D-glutamic acid only is found in the cell walls of certain bacteria.
In humans glutamate is a key molecule in cellular metabolism where it contributes to intermediates in the citric acid cycle55-57. Glutamate also plays an important role in disposal of excess nitrogen and lactate50, 58, 59.
In the central nervous system of vertebrae, glutamate acts as an excita-tory neurotransmitter and is involved in cognitive functions like learning and memory60. Under certain conditions it may act as an excitotoxin and participate in events leading to neurological damage61. Glutamate admini-stration has been shown to cause neurological injury in rodents but not in primates due to the blood-brain barrier that prevents passage of exogenous

14
of ischemia13. The role of myocardial ischemia for precipitating postopera-tive myocardial infarction and postoperative heart failure after CABG has been confirmed by other investigators6, 7, 14. Whereas perioperative myocar-dial ischemia plays a key role for outcome after CABG the role of ischemia for eliciting postoperative heart failure after valve surgery appears to be of secondary importance6, 7. Occurrence of perioperative myocardial infarc-tion is less frequent and other factors than ischemia account for the major proportion of cases with postoperative heart failure after valve surgery6, 7,
14. In patients undergoing CABG those with unstable angina are particu-
larly prone to perioperative ischemia and the risk for development of per-manent myocardial injury14-16. Patients that arrive to surgery with limited cardiac reserve i.e. preoperatively compromised left ventricular function are particularly likely to require treatment for postoperative heart failure17,
18.
1.3 Metabolic strategy in cardiac surgery Besides using conventional pharmacological treatment, an alternative ap-proach to prevent and treat postoperative heart failure could involve ad-herence to physiological principles to minimize myocardial and systemic oxygen expenditure, and specific measures such as metabolic interventions with glutamate and high-dose GIK to increase myocardial tolerance to ischemia and facilitate myocardial recovery after ischemia. Glucose-Insulin-Potassium (GIK) Over the last few years the debate regarding the salutary effects of insulin in association with cardiac surgery has focused on blood glucose control19-
23. However, none of these studies have been designed to identify the mechanisms behind the success of blood glucose control or to discriminate between the effects of insulin per se or the effects of blood glucose control. Beyond blood glucose control insulin has several potentially beneficial effects in the post-traumatic state including direct and indirect influence on systemic and myocardial metabolism, hemodynamic state, inflammatory response, endothelia function, coagulation and apoptosis.
Basic research suggests that glucose is important for the preservation of mechanical function, structure, histology and ionic balance during ische-mia24, 25. It appears that moderate doses of insulin can suffice to achieve blood glucose control and suppression of plasma FFAs after cardiac sur-gery. Although it is probable that moderate doses of insulin have a benefi-
15
cial effect on myocardial metabolism, direct effects on myocardial metabo-lism have so far only been documented with high-dose GIK (1 IU/kg bodyweight and hour). Assessed with coronary sinus catheter technique a shift in myocardial uptake of substrates from FFA to glucose has been demonstrated not only in elective CABG patients, but also in patients treated with catecholamines after CABG and in diabetic patients undergo-ing CABG26-28.
In experimental models insulin has been shown to have both inotropic29-
31 and vasodilatory properties32-35. Intraoperative assessment has confirmed beneficial effects on hemodynamic state with improved cardiac output28, 36-
44, improved LVSWI37, 38, less reduction in left ventricular ejection fraction measured by nuclear angiography45, improved central venous oxygen satu-ration46, fewer episodes of low cardiac output47, and less need for ino-tropes39, 40, 47-49.
In contrast to inotropic agents, this improvement has been achieved without excessive increase of myocardial oxygen demand38 or myocardial oxygen consumption measured by coronary sinus catheters50. The after-load reducing vasodilatory effect has been pronounced in studies using high-dose GIK43, 51, 52 and it appears that this vasodilation is not explained by luxury perfusion of skeletal muscle41. The inotropic effect has been more difficult to discriminate in the clinical setting after cardiac surgery but interestingly echocardiographic studies have shown improvement of regional myocardial function in patients with acute myocardial infarction53,
54.
1.4 Glutamate Glutamate, C5H9NO4, is a genetically coded non-essential acidic amino acid. Glutamate is the salt of glutamic acid of which there are two forms, L-glutamic acid and D-glutamic acid. The only form of glutamic acid found in higher organisms and in proteins is L-glutamic acid, whereas D-glutamic acid only is found in the cell walls of certain bacteria.
In humans glutamate is a key molecule in cellular metabolism where it contributes to intermediates in the citric acid cycle55-57. Glutamate also plays an important role in disposal of excess nitrogen and lactate50, 58, 59.
In the central nervous system of vertebrae, glutamate acts as an excita-tory neurotransmitter and is involved in cognitive functions like learning and memory60. Under certain conditions it may act as an excitotoxin and participate in events leading to neurological damage61. Glutamate admini-stration has been shown to cause neurological injury in rodents but not in primates due to the blood-brain barrier that prevents passage of exogenous

16
glutamate to the brain62-64. Furthermore, concentration of glutamate in the brain is fifty-fold higher than in human plasma65.
Glutamate accounts for 20% of body protein, which equals around 2 kilograms in a person weighing 70 kilograms. Only 10 grams of this is free and less than 0.1 grams is free in the circulation66-69.
Free glutamic acid is present in a wide variety of foods. The substance was identified in 1866 by the German chemist K Ritthausen. Glutamic acid is responsible for the fifth taste, Umami, termed by the Japanese researcher K Ikeda in 190770. It has been used as a flavor enhancer since the ancient roman kitchen and professor Ikeda patented a method of mass-production in 190871. The commercially produced glutamic acid is monosodium glu-tamate, MSG. The global demand of MSG is roughly 1.7 million tons per year72. Extensive use of MSG as a food additive has been claimed to cause the “chinese restaurant syndrome” supposed to be a hypersensitive allergic reaction to MSG, however, several blinded studies could not link MSG to symptoms associated with the “chinese restaurant syndrome”73-75.
17
1.5 Glutamate for metabolic intervention in coronary surgery In 1979 Rau observed that certain amino acids protected isolated rabbit myocardium from hypoxia55. The amino acids were glutamate, aspartate, ornithine and arginine. They are all active in the malate-asparate shuttle which links metabolism in the cytosol with mitochondria55, 56, 58. Of these amino acids, aspartate and in particular glutamate have been subject to further investigation regarding their metabolic role in association with ischemia. In animal in vitro and in vivo models numerous studies have shown that they protect the myocardium from ischemia and promote re-covery of oxidative metabolism after ischemia55, 58, 76-85.
In 1976 Mudge demonstrated that specific alterations of myocardial amino acid metabolism characterized patients with coronary artery dis-ease86. These patients exhibited an increased myocardial uptake of gluta-mate and an increased release of alanine. Thomassen and Pisarenko later confirmed these observations87-91. Thomassen subsequently demonstrated that glutamate administration was associated with delayed onset of angina and ECG-changes in patients subject to exercise testing and pacing92.
In 1985 Pisarenko reported beneficial hemodynamic and metabolic ef-fects of intravenous glutamate infusion to patients treated with dopamine because of heart failure after cardiac surgery93. Later it was demonstrated that myocardial uptake of amino acids and in particular glutamate pre-ceded normalization of myocardial substrate utilization after CABG27, 50. Infusion of intravenous glutamate after CABG was associated with in-creased myocardial uptake of glutamate, improved lactate utilization and improved hemodynamic state94.
Other investigators reported improved cardiac output due to peripheral vasodilatation after intravenous glutamate infusion in routine CABG but failed to demonstrate any metabolic changes as the metabolic state was normal at baseline95-97.
Furthermore a positive effect on ATP preservation in human myocar-dium during cardioplegic arrest has been shown with glutamate enhance-ment of cardioplegic solutions98.
Intravenous infusion provides the opportunity to supply the heart with substrate during the preoperative and postoperative phase. With this ap-proach encouraging results have been achieved in CABG on high-risk pa-tients, both in study populations and in clinical practice94, 99, 100. Based on this experience we wanted to pursue the role of intravenous glutamate as metabolic intervention in coronary surgery in a randomized clinical trial and thus the GLUTAMICS-trial was initiated.

16
glutamate to the brain62-64. Furthermore, concentration of glutamate in the brain is fifty-fold higher than in human plasma65.
Glutamate accounts for 20% of body protein, which equals around 2 kilograms in a person weighing 70 kilograms. Only 10 grams of this is free and less than 0.1 grams is free in the circulation66-69.
Free glutamic acid is present in a wide variety of foods. The substance was identified in 1866 by the German chemist K Ritthausen. Glutamic acid is responsible for the fifth taste, Umami, termed by the Japanese researcher K Ikeda in 190770. It has been used as a flavor enhancer since the ancient roman kitchen and professor Ikeda patented a method of mass-production in 190871. The commercially produced glutamic acid is monosodium glu-tamate, MSG. The global demand of MSG is roughly 1.7 million tons per year72. Extensive use of MSG as a food additive has been claimed to cause the “chinese restaurant syndrome” supposed to be a hypersensitive allergic reaction to MSG, however, several blinded studies could not link MSG to symptoms associated with the “chinese restaurant syndrome”73-75.
17
1.5 Glutamate for metabolic intervention in coronary surgery In 1979 Rau observed that certain amino acids protected isolated rabbit myocardium from hypoxia55. The amino acids were glutamate, aspartate, ornithine and arginine. They are all active in the malate-asparate shuttle which links metabolism in the cytosol with mitochondria55, 56, 58. Of these amino acids, aspartate and in particular glutamate have been subject to further investigation regarding their metabolic role in association with ischemia. In animal in vitro and in vivo models numerous studies have shown that they protect the myocardium from ischemia and promote re-covery of oxidative metabolism after ischemia55, 58, 76-85.
In 1976 Mudge demonstrated that specific alterations of myocardial amino acid metabolism characterized patients with coronary artery dis-ease86. These patients exhibited an increased myocardial uptake of gluta-mate and an increased release of alanine. Thomassen and Pisarenko later confirmed these observations87-91. Thomassen subsequently demonstrated that glutamate administration was associated with delayed onset of angina and ECG-changes in patients subject to exercise testing and pacing92.
In 1985 Pisarenko reported beneficial hemodynamic and metabolic ef-fects of intravenous glutamate infusion to patients treated with dopamine because of heart failure after cardiac surgery93. Later it was demonstrated that myocardial uptake of amino acids and in particular glutamate pre-ceded normalization of myocardial substrate utilization after CABG27, 50. Infusion of intravenous glutamate after CABG was associated with in-creased myocardial uptake of glutamate, improved lactate utilization and improved hemodynamic state94.
Other investigators reported improved cardiac output due to peripheral vasodilatation after intravenous glutamate infusion in routine CABG but failed to demonstrate any metabolic changes as the metabolic state was normal at baseline95-97.
Furthermore a positive effect on ATP preservation in human myocar-dium during cardioplegic arrest has been shown with glutamate enhance-ment of cardioplegic solutions98.
Intravenous infusion provides the opportunity to supply the heart with substrate during the preoperative and postoperative phase. With this ap-proach encouraging results have been achieved in CABG on high-risk pa-tients, both in study populations and in clinical practice94, 99, 100. Based on this experience we wanted to pursue the role of intravenous glutamate as metabolic intervention in coronary surgery in a randomized clinical trial and thus the GLUTAMICS-trial was initiated.

19
2 Aims of the thesis
- to report the short term and long term clinical experience of a metabolic strategy in patients with left ventricular dysfunction un-dergoing CABG
- to review the literature on clinical outcome in patients with left ven-
tricular dysfunction undergoing CABG
- to investigate safety aspects of intravenous glutamate infusion with particular reference to neurological injury in patients undergoing CABG
- to investigate if intravenous glutamate infusion prevents periopera-
tive myocardial infarction in patients undergoing CABG for acute coronary syndrome
- to investigate if intravenous glutamate infusion prevents postopera-
tive heart failure in patients undergoing CABG for acute coronary syndrome
- to investigate if intravenous glutamate infusion prevents postopera-
tive mortality in patients undergoing CABG for acute coronary syn-drome
- to investigate if intravenous glutamate infusion promotes postopera-
tive hemodynamic recovery in patients undergoing CABG for acute coronary syndrome
- to investigate if intravenous glutamate infusion reduces need for
hemodynamic support and intensive care in patients undergoing CABG for acute coronary syndrome
- to investigate if preemptive use of inotropic drugs influenced the
primary endpoint of the GLUTAMICS-trial
- to investigate the influence of intravenous glutamate infusion on the outcome in patients receiving inotropic drugs intraoperatively

19
2 Aims of the thesis
- to report the short term and long term clinical experience of a metabolic strategy in patients with left ventricular dysfunction un-dergoing CABG
- to review the literature on clinical outcome in patients with left ven-
tricular dysfunction undergoing CABG
- to investigate safety aspects of intravenous glutamate infusion with particular reference to neurological injury in patients undergoing CABG
- to investigate if intravenous glutamate infusion prevents periopera-
tive myocardial infarction in patients undergoing CABG for acute coronary syndrome
- to investigate if intravenous glutamate infusion prevents postopera-
tive heart failure in patients undergoing CABG for acute coronary syndrome
- to investigate if intravenous glutamate infusion prevents postopera-
tive mortality in patients undergoing CABG for acute coronary syn-drome
- to investigate if intravenous glutamate infusion promotes postopera-
tive hemodynamic recovery in patients undergoing CABG for acute coronary syndrome
- to investigate if intravenous glutamate infusion reduces need for
hemodynamic support and intensive care in patients undergoing CABG for acute coronary syndrome
- to investigate if preemptive use of inotropic drugs influenced the
primary endpoint of the GLUTAMICS-trial
- to investigate the influence of intravenous glutamate infusion on the outcome in patients receiving inotropic drugs intraoperatively

21
3 Patients and methods
3.1 Patients This thesis is based on patients from an observational study leading to a prospective randomized clinical trial, the GLUTAMICS-trial.
Patients in Paper I consist of 104 consecutive patients with severe left ventricular dysfunction (LVEF <0.40) undergoing CABG at the University Hospital of Linköping between 1991-1995.
Patients in Paper II-IV are all from the GLUTAMICS-trial. The 861 pa-tients in the GLUTAMICS-trial were operated with CABG for acute coro-nary syndrome between October 4, 2005 and November 12, 2009 at three Swedish Cardiac Surgery Centers (Örebro University Hospital, University Hospital of Linköping and Blekinge County Hospital, Karlskrona). During the study period 2087 patients underwent coronary surgery for acute coro-nary syndrome, 1064 patients were assessed for eligibility, 865 underwent randomization, 4 patients were excluded due to intraoperative exclusion criteria and 861 completed the study (Figure 1).
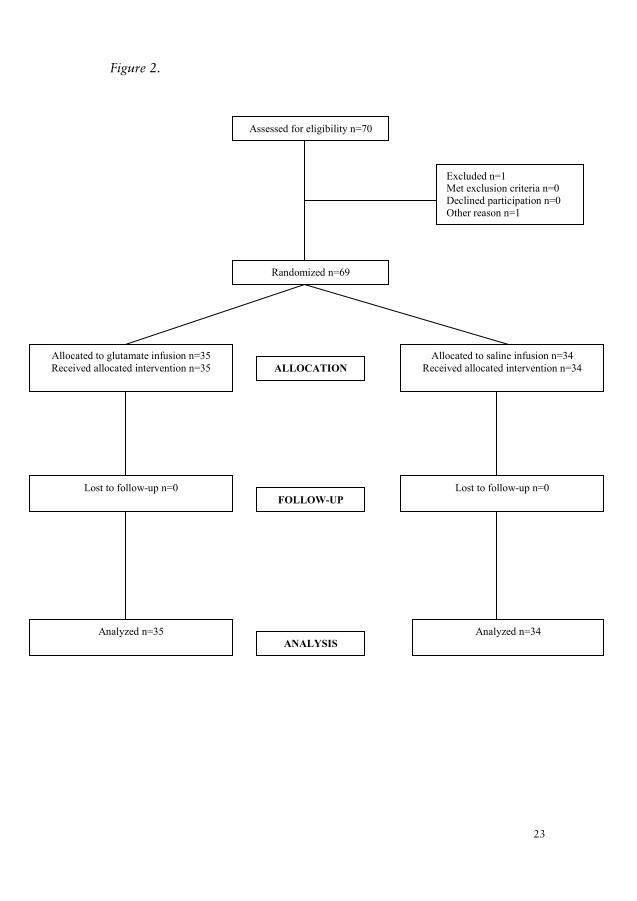
Paper II is based on a prespecified subgroup (n=69) in the GLUTAM-ICS-trial (Figure 2).
Paper III is based on the whole study population in the GLUTAMICS-trial (n=861).
Paper IV is a post hoc analysis of patients from two of the participating centers in the GLUTAMICS-trial (n=788) and of all patients in the GLU-TAMICS-trial receiving inotropic drugs intraoperatively (n=166).

21
3 Patients and methods
3.1 Patients This thesis is based on patients from an observational study leading to a prospective randomized clinical trial, the GLUTAMICS-trial.
Patients in Paper I consist of 104 consecutive patients with severe left ventricular dysfunction (LVEF <0.40) undergoing CABG at the University Hospital of Linköping between 1991-1995.
Patients in Paper II-IV are all from the GLUTAMICS-trial. The 861 pa-tients in the GLUTAMICS-trial were operated with CABG for acute coro-nary syndrome between October 4, 2005 and November 12, 2009 at three Swedish Cardiac Surgery Centers (Örebro University Hospital, University Hospital of Linköping and Blekinge County Hospital, Karlskrona). During the study period 2087 patients underwent coronary surgery for acute coro-nary syndrome, 1064 patients were assessed for eligibility, 865 underwent randomization, 4 patients were excluded due to intraoperative exclusion criteria and 861 completed the study (Figure 1).
Paper II is based on a prespecified subgroup (n=69) in the GLUTAM-ICS-trial (Figure 2).
Paper III is based on the whole study population in the GLUTAMICS-trial (n=861).
Paper IV is a post hoc analysis of patients from two of the participating centers in the GLUTAMICS-trial (n=788) and of all patients in the GLU-TAMICS-trial receiving inotropic drugs intraoperatively (n=166).

22
Figure 1. 2087 patients underwent coronary surgery for acute coronary syndrome between October 4, 2005 and
november 12, 2009
1064 patients were assessed for eligibility
865 underwent randomization
58 met exclusion criteria 98declined participation 30 participated in other trial 13 other reason
Allocated to glutamate infusion n=430 Allocated to saline infusion n=435
Excluded due to intraoperative exclusioncriteria n=2
Excluded due to intraoperative exclusioncriteria n=2
Received allocated intervention n=428 Received allocated intervention n=433
Follow-up n=428 Follow-up n=433
Analyzed n=433 Analyzed n=433
ALLOCATION
FOLLOW-UP
ANALYSIS
23
Figure 2. Assessed for eligibility n=70
Excluded n=1 Met exclusion criteria n=0 Declined participation n=0 Other reason n=1
Randomized n=69
Allocated to glutamate infusion n=35 Received allocated intervention n=35
Lost to follow-up n=0
Analyzed n=35
Allocated to saline infusion n=34 Received allocated intervention n=34
Lost to follow-up n=0
Analyzed n=34
ALLOCATION
FOLLOW-UP
ANALYSIS
2087 patients underwent coronary surgery for acute coronary syndrome between October 4 , 2005 and November 12, 2009
1064 patients were assessed for eligibility
865 underwent randomization
Allocated to Glutamate infusion n=430 Allocated to Saline infusion n=435
Follow-up n=428
Lost to follow-up n=0
Analyzed n=428
Excluded from analysis n=0
Analyzed n=433
Excluded from analysis n=0
ALLOCATION
FOLLOW-UP
ANALYSIS
ENROLLMENT58 met exclusion criteria98 declined participation30 participated in other trial13 other reason
Excluded due to intraoperative exclusioncriteria n=2
Excluded due to intraoperative exclusioncriteria n=2
Follow-up n=433
Lost to follow-up n=0
Received allocated intervention n=428 Received allocated intervention n=433
Assessed for eligibility n=70
Excluded n=1Met exclusion criteria n=0Declined participation n=0Other reason n=1
Randomized n=69
Allocated to glutamate infusion n=35Received allocated intervention n=35
Lost to follow-up n=0
Analyzed n=35
Allocated to saline infusion n=34Received allocated intervention n=34
Lost to follow-up n=0
Analyzed n=34
ALLOCATION
FOLLOW-UP
ANALYSIS
22
Figure 1. 2087 patients underwent coronary surgery for acute coronary syndrome between October 4, 2005 and
november 12, 2009
1064 patients were assessed for eligibility
865 underwent randomization
58 met exclusion criteria 98declined participation 30 participated in other trial 13 other reason
Allocated to glutamate infusion n=430 Allocated to saline infusion n=435
Excluded due to intraoperative exclusioncriteria n=2
Excluded due to intraoperative exclusioncriteria n=2
Received allocated intervention n=428 Received allocated intervention n=433
Follow-up n=428 Follow-up n=433
Analyzed n=433 Analyzed n=433
ALLOCATION
FOLLOW-UP
ANALYSIS
23
Figure 2. Assessed for eligibility n=70
Excluded n=1 Met exclusion criteria n=0 Declined participation n=0 Other reason n=1
Randomized n=69
Allocated to glutamate infusion n=35 Received allocated intervention n=35
Lost to follow-up n=0
Analyzed n=35
Allocated to saline infusion n=34 Received allocated intervention n=34
Lost to follow-up n=0
Analyzed n=34
ALLOCATION
FOLLOW-UP
ANALYSIS
23
Figure 2. Assessed for eligibility n=70
Excluded n=1 Met exclusion criteria n=0 Declined participation n=0 Other reason n=1
Randomized n=69
Allocated to glutamate infusion n=35 Received allocated intervention n=35
Lost to follow-up n=0
Analyzed n=35
Allocated to saline infusion n=34 Received allocated intervention n=34
Lost to follow-up n=0
Analyzed n=34
ALLOCATION
FOLLOW-UP
ANALYSIS
Assessed for eligibility n=70
Excluded n=1Met exclusion criteria n=0Declined participation n=0Other reason n=1
Randomized n=69
Allocated to glutamate infusion n=35Received allocated intervention n=35
Lost to follow-up n=0
Analyzed n=35
Allocated to saline infusion n=34Received allocated intervention n=34
Lost to follow-up n=0
Analyzed n=34
ALLOCATION
FOLLOW-UP
ANALYSIS
22
Figure 1. 2087 patients underwent coronary surgery for acute coronary syndrome between October 4, 2005 and
november 12, 2009
1064 patients were assessed for eligibility
865 underwent randomization
58 met exclusion criteria 98declined participation 30 participated in other trial 13 other reason
Allocated to glutamate infusion n=430 Allocated to saline infusion n=435
Excluded due to intraoperative exclusioncriteria n=2
Excluded due to intraoperative exclusioncriteria n=2
Received allocated intervention n=428 Received allocated intervention n=433
Follow-up n=428 Follow-up n=433
Analyzed n=433 Analyzed n=433
ALLOCATION
FOLLOW-UP
ANALYSIS
23
Figure 2. Assessed for eligibility n=70
Excluded n=1 Met exclusion criteria n=0 Declined participation n=0 Other reason n=1
Randomized n=69
Allocated to glutamate infusion n=35 Received allocated intervention n=35
Lost to follow-up n=0
Analyzed n=35
Allocated to saline infusion n=34 Received allocated intervention n=34
Lost to follow-up n=0
Analyzed n=34
ALLOCATION
FOLLOW-UP
ANALYSIS

24
3.2 GLUTAMICS-trial GLUTAMICS: GLUTAmate for Metabolic Interventionin Coronary Surgery ClinicalTrials.gov Identifier: NCT00489827 The GLUTAMICS-trial was an investigator initiated clinical phase III trial with parallel assignment to intravenous infusion of glutamate or placebo (saline) on patients undergoing CABG for acute coronary syndrome. The trial was first registered at the Swedish medical Product Agency 151/2003/70403 in December 2003. Later as the role of Clinical Trials Gov became increasingly acknowledged a secondary registration was made there: NCT00489827. External monitoring and reporting of adverse events was done according to Good Clinical Practice standard. Power analysis (80% power; p<0.05) suggested that 2214 patients would be required with regard to primary endpoint assuming 30% reduction of events occurring in 12% of untreated patients. Interim analysis was planned to occur after inclusion of 800 patients. The trial was terminated after interim analysis as prespecified stopping criteria per protocol were fulfilled.
Intervention Intravenous infusion of 0.125M glutamate solution or saline at a rate of 1.65ml/kg body weight and hour commencing at the induction of anesthe-sia and discontinued 2.5 hours after declamping the aorta or when a total of 500 ml had been infused. Glutamate solution 500 ml 0.125M solution of L-glutamic acid with pH 6.0 and 280 mos-mol/kg containing L-glutamic acid 9.2 g, NaCl 0.8g, H2O ad 500 ml and NaOH quantum satis. Production of glutamate solution and quality control was done by Apote-ket AB, Produktion & Laboratorier (APL), Box 6124, SE 90604 Umeå, Sweden.
Inclusion criteria Inclusion criteria were coronary artery bypass surgery for acute coronary syndrome. Patients were eligible for inclusion regardless if the procedure was done on-pump or off-pump or if the patient had a simultaneous valve procedure.
25
Exclusion criteria Exclusion criteria were, informed consent not possible because of critical condition or other reason, preoperative use of inotropic drugs or mechani-cal circulatory assist, preoperative dialysis, redo-procedure, unexpected intraoperative finding or event that increased the dignity of the procedure to overshadow the originally planned operation, age > 85 years, body weight > 125 kg and food allergy known to have caused flush, rash or asthma.
Study design Prospective, randomized, placebo controlled, double-blind clinical trial. Primary endpoint The primary endpoint was a composite of postoperative mortality (≤30 - days), perioperative myocardial infarction and left ventricular heart failure in association with weaning from CPB.
Secondary endpoints The secondary endpoints included neurological safety issues, degree of myocardial injury, postoperative hemodynamic state, use of inotropic drugs and mechanical circulatory support, severe circulatory failure, atrial fibrillation, renal function, ICU-treatment, cardiac mortality and late mor-tality.
Subgroup analysis Patients with CCS class IV angina were planned for a subgroup analysis. S-100B substudy As an early safety measure in the GLUTAMICS-trial a prespecified sub-group of patients (n=69) were analyzed with regard to postoperative S-100B levels to detect potential subclinical neurological injury related to glutamate infusion. Furthermore, we wanted to assess the relationship between S-100B and clinical signs of neurological injury and established risk factors for stroke (Paper II).
24
3.2 GLUTAMICS-trial GLUTAMICS: GLUTAmate for Metabolic Interventionin Coronary Surgery ClinicalTrials.gov Identifier: NCT00489827 The GLUTAMICS-trial was an investigator initiated clinical phase III trial with parallel assignment to intravenous infusion of glutamate or placebo (saline) on patients undergoing CABG for acute coronary syndrome. The trial was first registered at the Swedish medical Product Agency 151/2003/70403 in December 2003. Later as the role of Clinical Trials Gov became increasingly acknowledged a secondary registration was made there: NCT00489827. External monitoring and reporting of adverse events was done according to Good Clinical Practice standard. Power analysis (80% power; p<0.05) suggested that 2214 patients would be required with regard to primary endpoint assuming 30% reduction of events occurring in 12% of untreated patients. Interim analysis was planned to occur after inclusion of 800 patients. The trial was terminated after interim analysis as prespecified stopping criteria per protocol were fulfilled.
Intervention Intravenous infusion of 0.125M glutamate solution or saline at a rate of 1.65ml/kg body weight and hour commencing at the induction of anesthe-sia and discontinued 2.5 hours after declamping the aorta or when a total of 500 ml had been infused. Glutamate solution 500 ml 0.125M solution of L-glutamic acid with pH 6.0 and 280 mos-mol/kg containing L-glutamic acid 9.2 g, NaCl 0.8g, H2O ad 500 ml and NaOH quantum satis. Production of glutamate solution and quality control was done by Apote-ket AB, Produktion & Laboratorier (APL), Box 6124, SE 90604 Umeå, Sweden.
Inclusion criteria Inclusion criteria were coronary artery bypass surgery for acute coronary syndrome. Patients were eligible for inclusion regardless if the procedure was done on-pump or off-pump or if the patient had a simultaneous valve procedure.
25
Exclusion criteria Exclusion criteria were, informed consent not possible because of critical condition or other reason, preoperative use of inotropic drugs or mechani-cal circulatory assist, preoperative dialysis, redo-procedure, unexpected intraoperative finding or event that increased the dignity of the procedure to overshadow the originally planned operation, age > 85 years, body weight > 125 kg and food allergy known to have caused flush, rash or asthma.
Study design Prospective, randomized, placebo controlled, double-blind clinical trial. Primary endpoint The primary endpoint was a composite of postoperative mortality (≤ 30- days), perioperative myocardial infarction and left ventricular heart failure in association with weaning from CPB.
Secondary endpoints The secondary endpoints included neurological safety issues, degree of myocardial injury, postoperative hemodynamic state, use of inotropic drugs and mechanical circulatory support, severe circulatory failure, atrial fibrillation, renal function, ICU-treatment, cardiac mortality and late mor-tality.
Subgroup analysis Patients with CCS class IV angina were planned for a subgroup analysis. S-100B substudy As an early safety measure in the GLUTAMICS-trial a prespecified sub-group of patients (n=69) were analyzed with regard to postoperative S-100B levels to detect potential subclinical neurological injury related to glutamate infusion. Furthermore, we wanted to assess the relationship between S-100B and clinical signs of neurological injury and established risk factors for stroke (Paper II).

26
3.3 Post-hoc analysis In the GLUTAMICS-trial two of the participating centers (A and B) exhib-ited markedly different policies regarding preemptive use of inotropic drugs to facilitate weaning from CPB. Paper IV consists of a post-hoc analysis regarding the influence of inotropic drugs on the GLUTAMICS-trial. This analysis compares the two centers with different policies regarding preemp-tive use of inotropic drugs and also analyzes the influence of intravenous glutamate infusion on primary and secondary outcome variables in all patients receiving inotropic drugs intraoperatively.
3.4 Clinical management Paper I A metabolic strategy was implied which included adherence to physiologi-cal principles to minimize myocardial and systemic oxygen expenditure and specific measures such as extended CPB and metabolic support to fa-cilitate myocardial recovery in patients with inadequate hemodynamic state. Volume work by the heart rather than pressure work was promoted by after-load reduction when feasible. The adequacy of hemodynamic state was primarily assessed by measurement of SvO2 and urinary output. Ino-tropic drugs were used only if SvO2 or urinary output suggested that car-diac output was inadequate despite correction of volume and treatment of other causes. A mechanical assist device was preferred in favor of increas-ing the dose of inotropic drugs such as dobutamine above 5 μ/kg/min.
On the day of surgery all patients were given their individual doses of beta-blockers and calcium-antagonists. After premedication with morphine hydrochloride and scopolamine, anesthesia was induced with thiopentone and fentanyl, and maintained with fentanyl and isoflurane. Pancuronium bromide was used for neuromuscular blockade. CPB was conducted with a membrane oxygenator and a roller pump generating non-pulsatile flow. Ringer’s acetate and mannitol were used for priming the extracorporeal circuit. Moderate hemodilution (hematocrit 20–25%) and mild to moder-ate hypothermia (32–35°C) were employed. Antegrade or combined ante-grade and retrograde delivery of St.Thomas’ cold crystalloid cardioplegic solution was used for myocardial protection. CPB was prolonged until recovery of left ventricular function was evident. Heparin was neutralized with protamine chloride. In the postoperative period rewarming was facili-tated by radiant heat provided by thermal ceiling. Shed mediastinal blood was routinely retransfused after surgery. Ringer’s acetate was used for volume substitution.
27
Paper II-IV Clinical management was standardized and similar at the three participat-ing centers with minor differences concerning choice of anesthetic drugs. After an overnight fast, patients received beta-blockers and calcium-antagonists orally, whereas antihypertensive and antidiabetic agents were withheld. Standard premedication consisted of orally administered fluni-trazepam (0,5-1,0 mg) or diazepam (5-10 mg) and ketobemidone (0,1-0,2 mg/kg body weight) or morphine (0.1-0.2 mg/kg body weight). Anesthesia was induced with thiopentone (2-3 mg/kg body weight) or propofol (2 mg/kg body weight) supplemented by a bolus dose of fentanyl (3-5 μg/kg body weight). Muscle relaxation was achieved with pancuronium (0.1 mg/kg body weight) or rocuronium (0.6 mg/kg body weight). Anesthesia was maintained with isoflurane, sevoflurane or propofol supplemented with intermittent doses of fentanyl.
Standard monitoring was used consisting of 5-lead echocardiogram, pulse oximetry, continuous arterial blood pressure monitoring using a can-nula in the radial artery, central venous pressure and transesophageal echocardiography. A surgical pulmonary artery catheter was introduced in all patients.
Standard surgical techniques were employed. A median sternotomy was performed in all patients. CPB was achieved with an extracorporeal circuit consisting of a heart-lung machine (Stöckert SIII, Sorin Group, Munich, Germany or HL 30, MAQUET Cardiopulmonary AG, Hirrlingen, Ger-many), an open venous reservoir primed with 2,000 mL Ringer´s acetate, a roller pump with non-pulsatile flow, a hollow-fibre oxygenator with inte-grated heat exchanger, and a polyvinyl tubingsystem (Sorin Group, Miran-dola, Italy). Systemic heparinization was used to keep the activated clotting time >480 seconds. Myocardial protection was achieved with either cold blood cardioplegia or cold crystalloid cardioplegia.
Propofol was used for postoperative sedation. Postoperative analgesia regimen consisted of ketobemidone 7-15 µg/kg body weight administered intermittent intravenously and acetaminophen 1 g every 6th hour.
Extubation was performed when body temperature reached a level above 37°C, hemodynamic values were stable including a mixed venous saturation exceeding 55 %, pO2 was above 10 kPa with FiO2 0,4 and pCO2 was below 6,5 kPa with a respiratory rate less than 30 and drainage loss was less than 100 ml per hour and declining.
26
3.3 Post-hoc analysis In the GLUTAMICS-trial two of the participating centers (A and B) exhib-ited markedly different policies regarding preemptive use of inotropic drugs to facilitate weaning from CPB. Paper IV consists of a post-hoc analysis regarding the influence of inotropic drugs on the GLUTAMICS-trial. This analysis compares the two centers with different policies regarding preemp-tive use of inotropic drugs and also analyzes the influence of intravenous glutamate infusion on primary and secondary outcome variables in all patients receiving inotropic drugs intraoperatively.
3.4 Clinical management Paper I A metabolic strategy was implied which included adherence to physiologi-cal principles to minimize myocardial and systemic oxygen expenditure and specific measures such as extended CPB and metabolic support to fa-cilitate myocardial recovery in patients with inadequate hemodynamic state. Volume work by the heart rather than pressure work was promoted by after-load reduction when feasible. The adequacy of hemodynamic state was primarily assessed by measurement of SvO2 and urinary output. Ino-tropic drugs were used only if SvO2 or urinary output suggested that car-diac output was inadequate despite correction of volume and treatment of other causes. A mechanical assist device was preferred in favor of increas-ing the dose of inotropic drugs such as dobutamine above 5 μ/kg/min.
On the day of surgery all patients were given their individual doses of beta-blockers and calcium-antagonists. After premedication with morphine hydrochloride and scopolamine, anesthesia was induced with thiopentone and fentanyl, and maintained with fentanyl and isoflurane. Pancuronium bromide was used for neuromuscular blockade. CPB was conducted with a membrane oxygenator and a roller pump generating non-pulsatile flow. Ringer’s acetate and mannitol were used for priming the extracorporeal circuit. Moderate hemodilution (hematocrit 20–25%) and mild to moder-ate hypothermia (32–35°C) were employed. Antegrade or combined ante-grade and retrograde delivery of St.Thomas’ cold crystalloid cardioplegic solution was used for myocardial protection. CPB was prolonged until recovery of left ventricular function was evident. Heparin was neutralized with protamine chloride. In the postoperative period rewarming was facili-tated by radiant heat provided by thermal ceiling. Shed mediastinal blood was routinely retransfused after surgery. Ringer’s acetate was used for volume substitution.
27
Paper II-IV Clinical management was standardized and similar at the three participat-ing centers with minor differences concerning choice of anesthetic drugs. After an overnight fast, patients received beta-blockers and calcium-antagonists orally, whereas antihypertensive and antidiabetic agents were withheld. Standard premedication consisted of orally administered fluni-trazepam (0,5-1,0 mg) or diazepam (5-10 mg) and ketobemidone (0,1-0,2 mg/kg body weight) or morphine (0.1-0.2 mg/kg body weight). Anesthesia was induced with thiopentone (2-3 mg/kg body weight) or propofol (2 mg/kg body weight) supplemented by a bolus dose of fentanyl (3-5 μg/kg body weight). Muscle relaxation was achieved with pancuronium (0.1 mg/kg body weight) or rocuronium (0.6 mg/kg body weight). Anesthesia was maintained with isoflurane, sevoflurane or propofol supplemented with intermittent doses of fentanyl.
Standard monitoring was used consisting of 5-lead echocardiogram, pulse oximetry, continuous arterial blood pressure monitoring using a can-nula in the radial artery, central venous pressure and transesophageal echocardiography. A surgical pulmonary artery catheter was introduced in all patients.
Standard surgical techniques were employed. A median sternotomy was performed in all patients. CPB was achieved with an extracorporeal circuit consisting of a heart-lung machine (Stöckert SIII, Sorin Group, Munich, Germany or HL 30, MAQUET Cardiopulmonary AG, Hirrlingen, Ger-many), an open venous reservoir primed with 2,000 mL Ringer´s acetate, a roller pump with non-pulsatile flow, a hollow-fibre oxygenator with inte-grated heat exchanger, and a polyvinyl tubingsystem (Sorin Group, Miran-dola, Italy). Systemic heparinization was used to keep the activated clotting time >480 seconds. Myocardial protection was achieved with either cold blood cardioplegia or cold crystalloid cardioplegia.
Propofol was used for postoperative sedation. Postoperative analgesia regimen consisted of ketobemidone 7-15 µg/kg body weight administered intermittent intravenously and acetaminophen 1 g every 6th hour.
Extubation was performed when body temperature reached a level above 37°C, hemodynamic values were stable including a mixed venous saturation exceeding 55 %, pO2 was above 10 kPa with FiO2 0,4 and pCO2 was below 6,5 kPa with a respiratory rate less than 30 and drainage loss was less than 100 ml per hour and declining.

28
3.5 Metabolic intervention Paper I
In study I a metabolic strategy was implied which included adherence to physiological principles to minimize myocardial and systemic oxygen ex-penditure and specific measures such as extended CPB and metabolic sup-port with glutamate and/or high-dose GIK to facilitate myocardial recovery in patients with inadequate hemodynamic state.
During the time frame of the study availability of glutamate solutions was restricted due to limited capacity of the local pharmacy to produce solutions. Hence, prophylactic glutamate infusion was reserved for patients with signs of severe myocardial ischemia or heart failure in the operating room before surgery. In these patients glutamate was infused intrave-nously preoperatively and after release of cross clamp to prevent heart failure at weaning from CPB. Intravenous glutamate was also instituted as treatment in patients with failure to wean from CPB at the first attempt.
High dose glucose-insulin-potassium (GIK) was added to intravenous glutamate infusion in patients with failure to wean from CPB at the first attempt. Details of treatment with intravenous glutamate and high-dose GIK have been reported previously99.
Paper II-IV In Paper II-IV patients were randomly allocated to blinded intravenous infusion of 0.125M L-glutamic acid solution or saline at a rate of 1.65 ml/kg body weight and hour commencing at the induction of anesthesia. As the by cardioplegia arrested heart is reported to leak glutamate rather than extract exogenous glutamate, the infusions were temporarily stopped during aortic cross-clamping101. Infusions were resumed after declamping of the aorta and continued for a further 2 hours at this rate after which the infusion rate was halved and an additional 50 ml infused. The maximum volume infused to any patient was 500 ml of study solution. The dosage of glutamate was based on studies demonstrating that an infusion rate of 30-40 mg glutamate/kg body weight and hour increased arterial whole blood levels by two-three fold, which was sufficient to meet the myocardial de-mands or to saturate myocardial capacity to extract glutamate from the circulation102.
29
3.6 Data collection Paper I During a five-year period (1991-1995) when the metabolic strategy was introduced 775 consecutive patients operated for ischemic heart disease by two surgeons were registered in a database. Left ventricular function was assessed by angiography or echocardiography. 104 patients presented with compromised left ventricular function (LVEF<0.40) before surgery. The records of the patients were investigated in detail according to a protocol and data retrieved and stored in a database. Data on late mortality were retrieved from the Swedish Civil Registry. Paper II-IV Basic demographic, intraoperative and postoperative data were recorded prospectively in an institutional database, Carath, used at all participating centers.
Key study data were prospectively recorded in a CRF. Preoperatively the patients were classified with regard to CCS class and Braunwald class. Occurrence of angina at rest within 48 hours prior to surgery and occur-rence of ST-segment depression ≥ 1 mm or ST -segment elevation ≥ 2 mm from admission to the operating room to the onset of CPB were recorded. Use of inotropic drugs or mechanical circulatory assist was recorded. CT-scan was performed in cases with suspected permanent neurological injury.
In the S-100B substudy, epiaortic scanning of the ascending aorta with ultrasound (Vivid 7 Dimension GE ultrasound scanner and a GE Ultra-sound transducer 5.5–9.0 MHz, GE Parallel Design, Tempe, AZ, USA), was done intraoperatively before cannulation for CPB in all patients. Re-sults were recorded according to a protocol. Aortic calcification was classi-fied by the operating surgeon as none, mild, moderate, severe or com-pletely calcified.

28
3.5 Metabolic intervention Paper I
In study I a metabolic strategy was implied which included adherence to physiological principles to minimize myocardial and systemic oxygen ex-penditure and specific measures such as extended CPB and metabolic sup-port with glutamate and/or high-dose GIK to facilitate myocardial recovery in patients with inadequate hemodynamic state.
During the time frame of the study availability of glutamate solutions was restricted due to limited capacity of the local pharmacy to produce solutions. Hence, prophylactic glutamate infusion was reserved for patients with signs of severe myocardial ischemia or heart failure in the operating room before surgery. In these patients glutamate was infused intrave-nously preoperatively and after release of cross clamp to prevent heart failure at weaning from CPB. Intravenous glutamate was also instituted as treatment in patients with failure to wean from CPB at the first attempt.
High dose glucose-insulin-potassium (GIK) was added to intravenous glutamate infusion in patients with failure to wean from CPB at the first attempt. Details of treatment with intravenous glutamate and high-dose GIK have been reported previously99.
Paper II-IV In Paper II-IV patients were randomly allocated to blinded intravenous infusion of 0.125M L-glutamic acid solution or saline at a rate of 1.65 ml/kg body weight and hour commencing at the induction of anesthesia. As the by cardioplegia arrested heart is reported to leak glutamate rather than extract exogenous glutamate, the infusions were temporarily stopped during aortic cross-clamping101. Infusions were resumed after declamping of the aorta and continued for a further 2 hours at this rate after which the infusion rate was halved and an additional 50 ml infused. The maximum volume infused to any patient was 500 ml of study solution. The dosage of glutamate was based on studies demonstrating that an infusion rate of 30-40 mg glutamate/kg body weight and hour increased arterial whole blood levels by two-three fold, which was sufficient to meet the myocardial de-mands or to saturate myocardial capacity to extract glutamate from the circulation102.
29
3.6 Data collection Paper I During a five-year period (1991-1995) when the metabolic strategy was introduced 775 consecutive patients operated for ischemic heart disease by two surgeons were registered in a database. Left ventricular function was assessed by angiography or echocardiography. 104 patients presented with compromised left ventricular function (LVEF<0.40) before surgery. The records of the patients were investigated in detail according to a protocol and data retrieved and stored in a database. Data on late mortality were retrieved from the Swedish Civil Registry. Paper II-IV Basic demographic, intraoperative and postoperative data were recorded prospectively in an institutional database, Carath, used at all participating centers.
Key study data were prospectively recorded in a CRF. Preoperatively the patients were classified with regard to CCS class and Braunwald class. Occurrence of angina at rest within 48 hours prior to surgery and occur-rence of ST-segment depression ≥ 1 mm or ST -segment elevation ≥ 2 mm from admission to the operating room to the onset of CPB were recorded. Use of inotropic drugs or mechanical circulatory assist was recorded. CT-scan was performed in cases with suspected permanent neurological injury.
In the S-100B substudy, epiaortic scanning of the ascending aorta with ultrasound (Vivid 7 Dimension GE ultrasound scanner and a GE Ultra-sound transducer 5.5–9.0 MHz, GE Parallel Design, Tempe, AZ, USA), was done intraoperatively before cannulation for CPB in all patients. Re-sults were recorded according to a protocol. Aortic calcification was classi-fied by the operating surgeon as none, mild, moderate, severe or com-pletely calcified.

30
3.7 Biochemical analyses Creatine kinase (CK-MB) Creatine kinase (CK-MB) in plasma was sampled on the first postoperative day and analyzed using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland). Troponin-T Troponin-T in plasma was sampled immediately before surgery and on the third postoperative day. Analyses were performed using an electro-chemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland).
NT proBNP NT-proBNP in plasma was sampled in the operating room immediately before induction of anesthesia, postoperatively 24 hours after declamping the aorta and on the third postoperative day. Analyses were performed using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland). The between-run coef-ficient variation at 150 ng/L was 5.0% and at 1400 ng/L it was 6.2%. S-100B S-100B in plasma was sampled on the third postoperative day. Analyses were performed using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland). Cystatin-C Cystatin-C in plasma was sampled on the third postoperative day. Analyses were performed with the Gentian Cystatin-C Immunoassay on a Vitros 5.1 instrument (Ortho Clinical Diagnostics Johnson & Johnson, Raritan, NJ, USA) Creatinine Creatinine in plasma was sampled on the third postoperative day. The highest postoperative plasma Creatinine was also registered. Analyses were performed using enzymatic dry chemistry methods on a Vitros 5.1 instu-ment (Ortho Clinical Diagnostics Johnson & Johnson, Raritan, NJ, USA).
31
Lactate Arterial plasma lactate was measured five minutes after administration of protamine sulphate. Lactate was analyzed by a calorimetric method on on an ABL 500 (Radiometer Medical ApS, Brønshøj, Denmark) or a Vitros 5.1 instument (Ortho Clinical Diagnostics Johnson & Johnson, Raritan, NJ, USA).
3.8 Hemodynamic measurements Left ventricular function was assessed with transesophageal echocardi-ography prior to surgical incision and in association with weaning from CPB (Agilent Sonos 4500, Philips Electronics, Amsterdam, The Nether-lands and Acuson 128XP/10C, Siemens AG, Erlangen, Germany)
Hemodynamic variables (mixed venous oxygen saturation, arterial satu-ration, heart rate, systolic and diastolic arterial pressure, diastolic pulmo-nary artery pressure, central venous pressure) were recorded on weaning from CPB or after termination of the last graft in off-pump surgery, five minutes after administration of protamine sulphate and on admission to ICU.
Arterial pressure was measured in the radial artery. Pulmonary artery pressure and intermittent blood sampling for analysis of mixed venous oxygen saturation, SvO2, was retrieved by either a Swan-Ganz catheter or an epidural catheter introduced during surgery through the right ventricu-lar outflow tract into the pulmonary artery. Analyses were performed on an ABL 500 (Radiometer Medical ApS, Brønshøj, Denmark).
3.9 Definitions Paper I Use of inotropes was defined as a continuous infusion of beta-receptor stimulants or a bolus or continuous infusion of phosphodiesterase inhibi-tors regardless of dose. Complications presented refer to in-hospital events. Intraoperative myocardial infarction was diagnosed by biochemical mark-ers or by findings at autopsy as reported previously6, 103. Postoperative re-nal failure is presented according to STS data base definition104 and fur-thermore the proportion of patients having an increase of s-creatinine of 50% or more compared to preoperative value is given. Neurological injury included the following cerebral complications: 1) stroke 2) depression of consciousness or confusion if associated with signs of cerebral injury on CT-scan or focal neurological deficit 3) transient ischemic attacks with focal neurological deficit. The majority of patients with suspected neuro-

30
3.7 Biochemical analyses Creatine kinase (CK-MB) Creatine kinase (CK-MB) in plasma was sampled on the first postoperative day and analyzed using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland). Troponin-T Troponin-T in plasma was sampled immediately before surgery and on the third postoperative day. Analyses were performed using an electro-chemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland).
NT proBNP NT-proBNP in plasma was sampled in the operating room immediately before induction of anesthesia, postoperatively 24 hours after declamping the aorta and on the third postoperative day. Analyses were performed using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland). The between-run coef-ficient variation at 150 ng/L was 5.0% and at 1400 ng/L it was 6.2%. S-100B S-100B in plasma was sampled on the third postoperative day. Analyses were performed using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 instrument (Roche Diagnostics, Basel, Switzerland). Cystatin-C Cystatin-C in plasma was sampled on the third postoperative day. Analyses were performed with the Gentian Cystatin-C Immunoassay on a Vitros 5.1 instrument (Ortho Clinical Diagnostics Johnson & Johnson, Raritan, NJ, USA) Creatinine Creatinine in plasma was sampled on the third postoperative day. The highest postoperative plasma Creatinine was also registered. Analyses were performed using enzymatic dry chemistry methods on a Vitros 5.1 instu-ment (Ortho Clinical Diagnostics Johnson & Johnson, Raritan, NJ, USA).
31
Lactate Arterial plasma lactate was measured five minutes after administration of protamine sulphate. Lactate was analyzed by a calorimetric method on on an ABL 500 (Radiometer Medical ApS, Brønshøj, Denmark) or a Vitros 5.1 instument (Ortho Clinical Diagnostics Johnson & Johnson, Raritan, NJ, USA).
3.8 Hemodynamic measurements Left ventricular function was assessed with transesophageal echocardi-ography prior to surgical incision and in association with weaning from CPB (Agilent Sonos 4500, Philips Electronics, Amsterdam, The Nether-lands and Acuson 128XP/10C, Siemens AG, Erlangen, Germany)
Hemodynamic variables (mixed venous oxygen saturation, arterial satu-ration, heart rate, systolic and diastolic arterial pressure, diastolic pulmo-nary artery pressure, central venous pressure) were recorded on weaning from CPB or after termination of the last graft in off-pump surgery, five minutes after administration of protamine sulphate and on admission to ICU.
Arterial pressure was measured in the radial artery. Pulmonary artery pressure and intermittent blood sampling for analysis of mixed venous oxygen saturation, SvO2, was retrieved by either a Swan-Ganz catheter or an epidural catheter introduced during surgery through the right ventricu-lar outflow tract into the pulmonary artery. Analyses were performed on an ABL 500 (Radiometer Medical ApS, Brønshøj, Denmark).
3.9 Definitions Paper I Use of inotropes was defined as a continuous infusion of beta-receptor stimulants or a bolus or continuous infusion of phosphodiesterase inhibi-tors regardless of dose. Complications presented refer to in-hospital events. Intraoperative myocardial infarction was diagnosed by biochemical mark-ers or by findings at autopsy as reported previously6, 103. Postoperative re-nal failure is presented according to STS data base definition104 and fur-thermore the proportion of patients having an increase of s-creatinine of 50% or more compared to preoperative value is given. Neurological injury included the following cerebral complications: 1) stroke 2) depression of consciousness or confusion if associated with signs of cerebral injury on CT-scan or focal neurological deficit 3) transient ischemic attacks with focal neurological deficit. The majority of patients with suspected neuro-

32
logical injury were examined by a neurologist and by CT-scan. Cognitive dysfunction was not assessed.
Paper II-III Primary and secondary endpoints in the GLUTAMICS-trial were based on a number of prespecified definitions. The most central were 30-day mortal-ity, perioperative myocardial infarction, LV-failure at weaning from CPB, hemodynamic instability at completion of surgery, severe circulatory fail-ure and cardiac mortality. Details of all definitions are presented in the Appendix.
Due to the lack of generally accepted criteria for postoperative heart failure in association with cardiac surgery a clinical endpoints committee was considered necessary. The clinical endpoints committee consisted of consultants in cardiothoracic surgery and cardiothoracic anesthesiology from each of the participating centers. The members of the committee were blinded to the treatment assignment and prespecified criteria were used to reach a consensus decision.
Stroke was defined as appearance of a focal neurological deficit persist-ing for more than 24 h or depression of consciousness or confusion if asso-ciated with signs of cerebral injury on CT scan. Postoperative confusion was registered in the clinical database when there was a state of confusion verified by both nurse and physician that prevented normal mobilization of the patient. Patients with clinical suspicion of neurological injury under-went CT scan of the brain.
Paper IV Intraoperative use of inotropic drugs was defined as infusion of inotropic drugs for at least 30 minutes or a bolus dose of milrinone.
Preemptive use of inotropic drugs to facilitate weaning from CPB was defined as use of inotropic drugs in patients that according to prespecified criteria were deemed, by the clinical endpoints committee, not to have had heart failure at weaning.
3.10 Statistics The data are presented as percentages, means ± standard deviation or me-dians with range or inter-quartile range. Two-sided Fisher’s exact test was used for comparison of categorical data. Student’s t-test or Mann-Whitney U-test was used as appropriate for comparison of continuous variables. Long-term survival is given as crude 5-year survival and cumulative 10-year survival according to Kaplan-Meier analysis. Forward stepwise multi-variable logistic regression analysis was used for identification of inde-
33
pendent risk factors for severe circulatory failure. Hosmer-Lemeshow goodness-of-fit statistics was calculated for the final model. For all tests statistical significance was defined as p<0.05. Adjustment for multiple test-ing was not performed.
In Paper II statistical analysis was performed by an external professional statistician and blinded to the investigators, as this was a substudy in the still ongoing GLUTAMICS-trial.
All statistical analyses were performed with computerized statistical packages (Statistica 9.1, StatSoft Inc.,Tulsa, OK, USA, and SPSS Statistics 18, SPSS Inc., Chicago, IL, USA).
3.11 Ethics All studies were performed according to the Helsinki Declaration of Hu-man Rights and the Regional Ethical Review Board in Linköping (Paper I: Dnr 03-597; 2003-12-16 Papers II-IV: M76-05; 2005-05-09). The GLU-TAMICS-trial (Paper II-IV) was approved by the Swedish Medical Prod-ucts Agency (151:2003/70403) and registered on ClinicalTrials.gov (Identi-fier: NCT00489827). After written informed consent the patients were enrolled in the study.
The Swedish Medical Products Agency requested surveillance and un-blinding in cases of CT-verified stroke within 24 hours of surgery, mortal-ity and suspected unexpected serious adverse reactions (SUSAR). An independent professional monitoring team did external monitoring of all key data and unblinding procedures.
32
logical injury were examined by a neurologist and by CT-scan. Cognitive dysfunction was not assessed.
Paper II-III Primary and secondary endpoints in the GLUTAMICS-trial were based on a number of prespecified definitions. The most central were 30-day mortal-ity, perioperative myocardial infarction, LV-failure at weaning from CPB, hemodynamic instability at completion of surgery, severe circulatory fail-ure and cardiac mortality. Details of all definitions are presented in the Appendix.
Due to the lack of generally accepted criteria for postoperative heart failure in association with cardiac surgery a clinical endpoints committee was considered necessary. The clinical endpoints committee consisted of consultants in cardiothoracic surgery and cardiothoracic anesthesiology from each of the participating centers. The members of the committee were blinded to the treatment assignment and prespecified criteria were used to reach a consensus decision.
Stroke was defined as appearance of a focal neurological deficit persist-ing for more than 24 h or depression of consciousness or confusion if asso-ciated with signs of cerebral injury on CT scan. Postoperative confusion was registered in the clinical database when there was a state of confusion verified by both nurse and physician that prevented normal mobilization of the patient. Patients with clinical suspicion of neurological injury under-went CT scan of the brain.
Paper IV Intraoperative use of inotropic drugs was defined as infusion of inotropic drugs for at least 30 minutes or a bolus dose of milrinone.
Preemptive use of inotropic drugs to facilitate weaning from CPB was defined as use of inotropic drugs in patients that according to prespecified criteria were deemed, by the clinical endpoints committee, not to have had heart failure at weaning.
3.10 Statistics The data are presented as percentages, means ± standard deviation or me-dians with range or inter-quartile range. Two-sided Fisher’s exact test was used for comparison of categorical data. Student’s t-test or Mann-Whitney U-test was used as appropriate for comparison of continuous variables. Long-term survival is given as crude 5-year survival and cumulative 10-year survival according to Kaplan-Meier analysis. Forward stepwise multi-variable logistic regression analysis was used for identification of inde-
33
pendent risk factors for severe circulatory failure. Hosmer-Lemeshow goodness-of-fit statistics was calculated for the final model. For all tests statistical significance was defined as p<0.05. Adjustment for multiple test-ing was not performed.
In Paper II statistical analysis was performed by an external professional statistician and blinded to the investigators, as this was a substudy in the still ongoing GLUTAMICS-trial.
All statistical analyses were performed with computerized statistical packages (Statistica 9.1, StatSoft Inc.,Tulsa, OK, USA, and SPSS Statistics 18, SPSS Inc., Chicago, IL, USA).
3.11 Ethics All studies were performed according to the Helsinki Declaration of Hu-man Rights and the Regional Ethical Review Board in Linköping (Paper I: Dnr 03-597; 2003-12-16 Papers II-IV: M76-05; 2005-05-09). The GLU-TAMICS-trial (Paper II-IV) was approved by the Swedish Medical Prod-ucts Agency (151:2003/70403) and registered on ClinicalTrials.gov (Identi-fier: NCT00489827). After written informed consent the patients were enrolled in the study.
The Swedish Medical Products Agency requested surveillance and un-blinding in cases of CT-verified stroke within 24 hours of surgery, mortal-ity and suspected unexpected serious adverse reactions (SUSAR). An independent professional monitoring team did external monitoring of all key data and unblinding procedures.

35
4 Results
4.1 Observational study on a metabolic strategy (Paper I) Major demographic and intraoperative data for the study cohort of 104 patients are given in Table 1. The mean age was 65±9 years, 29.8% had unstable angina and the logistic EuroSCORE was 8.3 (95% CI 5.8–10.8). The mean left ventricular ejection fraction was 0.30±0.05 (range 0.20–0.37).
Table 1. Demographic and intraoperative data (mean±SD or count n %).
n=104 Age (years) 65±9 Female gender 19.2% (20/104) Diabetes mellitus 20.2% (21/104) Logistic EuroSCORE 8.3 (95% CI 5.8–10.8) LVEF 0.30±0.05 s-Creatinine (μmol/L) 106±21 Unstable angina 29.8% (31/104) Urgent/Emergent procedure 27.9% (29/104) Number of bypassed vessels 3.5±1.3 Cross clamp time (minutes) 41±22 CPB time (minutes) 95±46
Outcome The overall thirty-day mortality was 1.0% compared to expected mortality of 8.3% according to logistic EuroSCORE. Crude five-year survival overall was 89.4%. Ten-year survival according to Kaplan-Meier is shown in Fig-ure 3.
SvO2 on arrival to ICU averaged 65.8±7.4%. Mean stay in the ICU was 1.9±2.3 days. Postoperatively 10.6% of the patients had signs of myocar-dial infarction. Postoperative increase of s-Creatinine by ≥50% of the pre-operative level was found in 2.9% of the patients and the incidence of postoperative renal failure according to the STS definition was 1.0%.

35
4 Results
4.1 Observational study on a metabolic strategy (Paper I) Major demographic and intraoperative data for the study cohort of 104 patients are given in Table 1. The mean age was 65±9 years, 29.8% had unstable angina and the logistic EuroSCORE was 8.3 (95% CI 5.8–10.8). The mean left ventricular ejection fraction was 0.30±0.05 (range 0.20–0.37).
Table 1. Demographic and intraoperative data (mean±SD or count n %).
n=104 Age (years) 65±9 Female gender 19.2% (20/104) Diabetes mellitus 20.2% (21/104) Logistic EuroSCORE 8.3 (95% CI 5.8–10.8) LVEF 0.30±0.05 s-Creatinine (μmol/L) 106±21 Unstable angina 29.8% (31/104) Urgent/Emergent procedure 27.9% (29/104) Number of bypassed vessels 3.5±1.3 Cross clamp time (minutes) 41±22 CPB time (minutes) 95±46
Outcome The overall thirty-day mortality was 1.0% compared to expected mortality of 8.3% according to logistic EuroSCORE. Crude five-year survival overall was 89.4%. Ten-year survival according to Kaplan-Meier is shown in Fig-ure 3.
SvO2 on arrival to ICU averaged 65.8±7.4%. Mean stay in the ICU was 1.9±2.3 days. Postoperatively 10.6% of the patients had signs of myocar-dial infarction. Postoperative increase of s-Creatinine by ≥50% of the pre-operative level was found in 2.9% of the patients and the incidence of postoperative renal failure according to the STS definition was 1.0%.
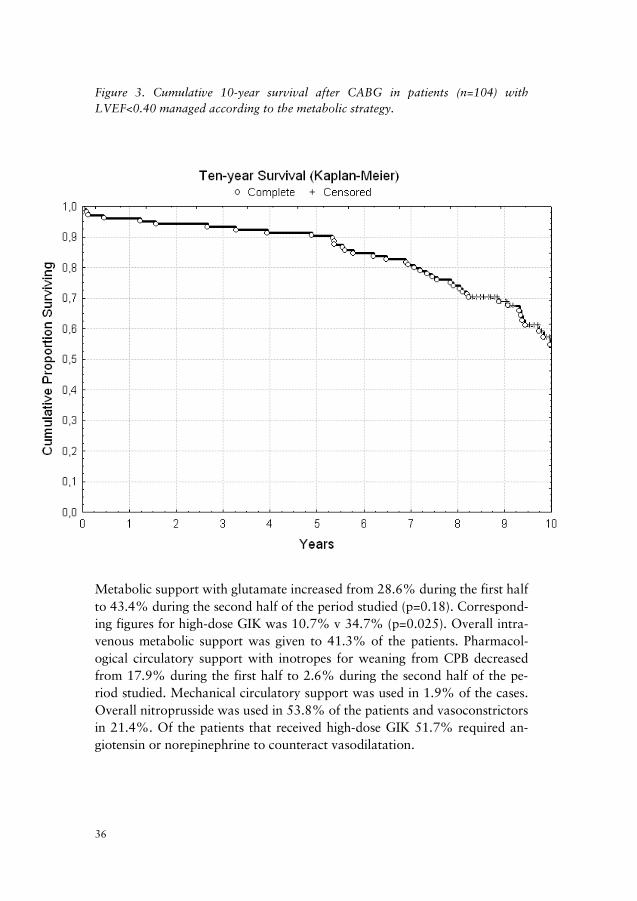
36
Figure 3. Cumulative 10-year survival after CABG in patients (n=104) with LVEF<0.40 managed according to the metabolic strategy.
‘
Metabolic support with glutamate increased from 28.6% during the first half to 43.4% during the second half of the period studied (p=0.18). Correspond-ing figures for high-dose GIK was 10.7% v 34.7% (p=0.025). Overall intra-venous metabolic support was given to 41.3% of the patients. Pharmacol-ogical circulatory support with inotropes for weaning from CPB decreased from 17.9% during the first half to 2.6% during the second half of the pe-riod studied. Mechanical circulatory support was used in 1.9% of the cases. Overall nitroprusside was used in 53.8% of the patients and vasoconstrictors in 21.4%. Of the patients that received high-dose GIK 51.7% required an-giotensin or norepinephrine to counteract vasodilatation.
37
In the ICU low dose inotropes or phosphodiesterase inhibitors were used to enhance urinary output in a total of 37.3% of the patients. The average doses when used were for dobutamine 2.2±1.1 µg/kg and min (n=30), dopamine 1.6±1.1 µg/kg and min (n=6) and for epinephrine 28±27 ng/kg and min (n=5).
Thirty-day mortality and five-year survival in relationship to type of metabolic treatment is shown in Table 2-3.
Table 2. Patients treated with intravenous glutamate (mean±SD or count n %).
Intravenous glutamate overall 39.4% (41/104) Intravenous glutamate to prevent heart failure at weaning from CPB
24.0% (25/104)
Intravenous glutamate as treatment of heart failure at weaning from CPB
15.4% (16/104)
Addition of high-dose GIK 67% (27/41) Inotropes for weaning from CPB 14.6% (6/41) LVEF 0.27±0.05 Logistic EuroSCORE 15.1% 30-day mortality 2.4% 5-year survival 82.9%
Table 3. Patients treated with high-dose GIK (mean±SD or count n %).
High-dose GIK as treatment of heart failure at weaning from CPB
27.9%(29/104)
Addition of intravenous glutamate 93%(27/29) Inotropes for weaning from CPB 17%(5/29) LVEF 0.26±0.05 Logistic EuroSCORE 17.4% 30-day mortality 3.4% 5-year survival 82.8%

36
Figure 3. Cumulative 10-year survival after CABG in patients (n=104) with LVEF<0.40 managed according to the metabolic strategy.
‘
Metabolic support with glutamate increased from 28.6% during the first half to 43.4% during the second half of the period studied (p=0.18). Correspond-ing figures for high-dose GIK was 10.7% v 34.7% (p=0.025). Overall intra-venous metabolic support was given to 41.3% of the patients. Pharmacol-ogical circulatory support with inotropes for weaning from CPB decreased from 17.9% during the first half to 2.6% during the second half of the pe-riod studied. Mechanical circulatory support was used in 1.9% of the cases. Overall nitroprusside was used in 53.8% of the patients and vasoconstrictors in 21.4%. Of the patients that received high-dose GIK 51.7% required an-giotensin or norepinephrine to counteract vasodilatation.
37
In the ICU low dose inotropes or phosphodiesterase inhibitors were used to enhance urinary output in a total of 37.3% of the patients. The average doses when used were for dobutamine 2.2±1.1 µg/kg and min (n=30), dopamine 1.6±1.1 µg/kg and min (n=6) and for epinephrine 28±27 ng/kg and min (n=5).
Thirty-day mortality and five-year survival in relationship to type of metabolic treatment is shown in Table 2-3.
Table 2. Patients treated with intravenous glutamate (mean±SD or count n %).
Intravenous glutamate overall 39.4% (41/104) Intravenous glutamate to prevent heart failure at weaning from CPB
24.0% (25/104)
Intravenous glutamate as treatment of heart failure at weaning from CPB
15.4% (16/104)
Addition of high-dose GIK 67% (27/41) Inotropes for weaning from CPB 14.6% (6/41) LVEF 0.27±0.05 Logistic EuroSCORE 15.1% 30-day mortality 2.4% 5-year survival 82.9%
Table 3. Patients treated with high-dose GIK (mean±SD or count n %).
High-dose GIK as treatment of heart failure at weaning from CPB
27.9%(29/104)
Addition of intravenous glutamate 93%(27/29) Inotropes for weaning from CPB 17%(5/29) LVEF 0.26±0.05 Logistic EuroSCORE 17.4% 30-day mortality 3.4% 5-year survival 82.8%

38
A key issue in the metabolic strategy was extended reperfusion time on CPB, to allow the heart to recover from ischemia. In patients that could be weaned at the first attempt, CPB time and aortic cross clamp time were 81±27 minutes and 40±19 minutes respectively. In patients with difficulty to wean at the first attempt (n=32) CPB time averaged 127±62 minutes while cross clamp time was 45±28 minutes. Of the patients with initial weaning difficulties 94% were treated with metabolic support and 78% could be weaned from CPB without inotropes. Mechanical circulatory support was used in 1.9% of the cases.
Outcome related to mixed venous oxygen saturation showed that of pa-tients who arrived to the ICU with SvO2>55% and without history of weaning problems no one developed renal failure, 30-day mortality was zero and five-year survival was 95.6%.
Comment This observational study on a metabolic strategy showed lower 30-day mortality (1.0%) than previously reported in patients with severe LV-dysfunction undergoing CABG. 30-day mortality was also substantially lower than the expected risk adjusted mortality of 8.3% according to logis-tic EuroSCORE. Long-term survival was encouraging with a crude 5-year survival of 89.4%.
39
4.2 S-100B substudy of the GLUTAMICS-trial (Paper II) Of the 69 patients included in this prespecified substudy, 35 patients re-ceived intravenous glutamate infusion and 34 patients received placebo (intravenous saline infusion). No patients were lost to follow-up (Figure 2). Major pre-, intra-, and postoperative data are given in Table 4.
Table 4. Pre-, intra-, and postoperative data for the S-100B substudy (mean±SD or count n %.)
There was no statistically significant difference in S-100B levels between the glutamate group and the control group (0.07±0.034 µg/L v 0.090±0.042 µg/L; p=0.25). No patient suffered from stroke and there was no mortality.
Overall 21 patients had S-100B above reference level (0.10 µg/L). Major pre-, intra-, and postoperative data for this group versus the group with normal level of S-100B are given in Table 5.
Placebo n=34
Glutamate n=35
p value
Age (years) 66±11 68±9 0.40 Female gender 9.0%(3) 20.0%(7) 0.31 Diabetes mellitus 29.4%(10) 40.0%(14) 0.45 Cerebrovascular disease 2.9%(1) 11.4%(4) 0.36 Moderate-severe LV-dysfunction 26.5%(9) 20.0%(7) 0.58 CCS class IV angina 84.0%(29) 80.6%(28) 1.00 Additive EuroSCORE 4.8±3.1 5.6±3.5 0.30 Calcification of ascending aorta 34.2%(12) 29.4%(10) 1.00 Emergency procedure 0 8.6%(3) 0.24 Number of bypassed vessels 4.1±1.4 3.8±1.3 0.46 Other operation than isolated CABG 5.9%(2) 8.6%(3) 1.00 Cross clamp time (minutes) 59±22 64±23 0.34 CPB time (minutes) 84±29 91±30 0.37 Stroke 0 0 1.00 Confusion 8.8%(3) 5.7%(2) 0.67

38
A key issue in the metabolic strategy was extended reperfusion time on CPB, to allow the heart to recover from ischemia. In patients that could be weaned at the first attempt, CPB time and aortic cross clamp time were 81±27 minutes and 40±19 minutes respectively. In patients with difficulty to wean at the first attempt (n=32) CPB time averaged 127±62 minutes while cross clamp time was 45±28 minutes. Of the patients with initial weaning difficulties 94% were treated with metabolic support and 78% could be weaned from CPB without inotropes. Mechanical circulatory support was used in 1.9% of the cases.
Outcome related to mixed venous oxygen saturation showed that of pa-tients who arrived to the ICU with SvO2>55% and without history of weaning problems no one developed renal failure, 30-day mortality was zero and five-year survival was 95.6%.
Comment This observational study on a metabolic strategy showed lower 30-day mortality (1.0%) than previously reported in patients with severe LV-dysfunction undergoing CABG. 30-day mortality was also substantially lower than the expected risk adjusted mortality of 8.3% according to logis-tic EuroSCORE. Long-term survival was encouraging with a crude 5-year survival of 89.4%.
39
4.2 S-100B substudy of the GLUTAMICS-trial (Paper II) Of the 69 patients included in this prespecified substudy, 35 patients re-ceived intravenous glutamate infusion and 34 patients received placebo (intravenous saline infusion). No patients were lost to follow-up (Figure 2). Major pre-, intra-, and postoperative data are given in Table 4.
Table 4. Pre-, intra-, and postoperative data for the S-100B substudy (mean±SD or count n %.)
There was no statistically significant difference in S-100B levels between the glutamate group and the control group (0.07±0.034 µg/L v 0.090±0.042 µg/L; p=0.25). No patient suffered from stroke and there was no mortality.
Overall 21 patients had S-100B above reference level (0.10 µg/L). Major pre-, intra-, and postoperative data for this group versus the group with normal level of S-100B are given in Table 5.
Placebo n=34
Glutamate n=35
p value
Age (years) 66±11 68±9 0.40 Female gender 9.0%(3) 20.0%(7) 0.31 Diabetes mellitus 29.4%(10) 40.0%(14) 0.45 Cerebrovascular disease 2.9%(1) 11.4%(4) 0.36 Moderate-severe LV-dysfunction 26.5%(9) 20.0%(7) 0.58 CCS class IV angina 84.0%(29) 80.6%(28) 1.00 Additive EuroSCORE 4.8±3.1 5.6±3.5 0.30 Calcification of ascending aorta 34.2%(12) 29.4%(10) 1.00 Emergency procedure 0 8.6%(3) 0.24 Number of bypassed vessels 4.1±1.4 3.8±1.3 0.46 Other operation than isolated CABG 5.9%(2) 8.6%(3) 1.00 Cross clamp time (minutes) 59±22 64±23 0.34 CPB time (minutes) 84±29 91±30 0.37 Stroke 0 0 1.00 Confusion 8.8%(3) 5.7%(2) 0.67

40
Table 5. Normal versus elevated S-100B (mean±SD or count n %).
In the group with elevated S-100B there was significantly higher Euro-SCORE, significantly more calcification of the ascending aorta and signifi-cantly higher occurrence of postoperative confusion.
The patients with postoperative confusion also showed significantly ele-vated S-100B compared with those without confusion (0.132±0.047 µg/L v 0.081±0.036 µg/L; p=0.003).
The levels of S-100B on the third postoperative day depending on study group, occurrence of postoperative confusion and prevalence of aortic calcification on intraoperative epiaortic scanning are shown in Figure 4.
Normal S-100B n=48
Elevated S-100B n=21
p value
Age (years) 65±9 70±10 0.10 Female gender 8.3%(4) 28.6%(6) 0.06 Diabetes mellitus 31.3%(15) 42.9%(9) 0.42 Cerebrovascular disease 6.3%(3) 9.5%(2) 0.64 Moderate-severe LV-dysfunction 25.0%(12) 19.0%(4) 0.76 CCS class IV angina 80.0%(38) 87.5%(18) 0.71 Additive EuroSCORE 4.5±3.1 7.0±3.1 0.003 Calcification of ascending aorta 21.3%(10) 52.4%(11) 0.02 Emergency procedure 4.2%(2) 4.8%(1) 1.00 Number of bypassed vessels 4.0±1.3 3.8±1.3 0.58 Other operation than isolated CABG 4.2%(2) 14.3%(3) 0.16 Cross clamp time (minutes) 59±21 67±26 0.21 CPB time (minutes) 85±29 93±30 0.35 Stroke 0 0 1.00 Confusion 2.1%(1) 19.0%(4) 0.03
41
Figure 4. S-100B levels on the third postoperative day depending on study group, occurrence of postoperative confusion and prevalence of aortic calcification.
Comment This substudy of the GLUTAMICS-trial regarding neurological safety is-sues showed that intravenous glutamate infusion during surgery for acute coronary syndrome did not initiate a sustained elevation of plasma S-100B postoperatively. Thus, no evidence for subclinical neurological injury re-lated to glutamate infusion was found. In contrast, postoperative elevation of plasma S-100B was linked to calcification of the ascending aorta and postoperative confusion.
* p<0.05

40
Table 5. Normal versus elevated S-100B (mean±SD or count n %).
In the group with elevated S-100B there was significantly higher Euro-SCORE, significantly more calcification of the ascending aorta and signifi-cantly higher occurrence of postoperative confusion.
The patients with postoperative confusion also showed significantly ele-vated S-100B compared with those without confusion (0.132±0.047 µg/L v 0.081±0.036 µg/L; p=0.003).
The levels of S-100B on the third postoperative day depending on study group, occurrence of postoperative confusion and prevalence of aortic calcification on intraoperative epiaortic scanning are shown in Figure 4.
Normal S-100B n=48
Elevated S-100B n=21
p value
Age (years) 65±9 70±10 0.10 Female gender 8.3%(4) 28.6%(6) 0.06 Diabetes mellitus 31.3%(15) 42.9%(9) 0.42 Cerebrovascular disease 6.3%(3) 9.5%(2) 0.64 Moderate-severe LV-dysfunction 25.0%(12) 19.0%(4) 0.76 CCS class IV angina 80.0%(38) 87.5%(18) 0.71 Additive EuroSCORE 4.5±3.1 7.0±3.1 0.003 Calcification of ascending aorta 21.3%(10) 52.4%(11) 0.02 Emergency procedure 4.2%(2) 4.8%(1) 1.00 Number of bypassed vessels 4.0±1.3 3.8±1.3 0.58 Other operation than isolated CABG 4.2%(2) 14.3%(3) 0.16 Cross clamp time (minutes) 59±21 67±26 0.21 CPB time (minutes) 85±29 93±30 0.35 Stroke 0 0 1.00 Confusion 2.1%(1) 19.0%(4) 0.03
41
Figure 4. S-100B levels on the third postoperative day depending on study group, occurrence of postoperative confusion and prevalence of aortic calcification.
Comment This substudy of the GLUTAMICS-trial regarding neurological safety is-sues showed that intravenous glutamate infusion during surgery for acute coronary syndrome did not initiate a sustained elevation of plasma S-100B postoperatively. Thus, no evidence for subclinical neurological injury re-lated to glutamate infusion was found. In contrast, postoperative elevation of plasma S-100B was linked to calcification of the ascending aorta and postoperative confusion.
* p<0.05

42
4.3 Results of the GLUTAMICS-trial (Paper III) The GLUTAMICS-trial was conducted between October 4, 2005 and No-vember 12, 2009. A total of 865 patients were randomized and 4 patients, 2 in the glutamate group and 2 in the placebo group were excluded due to intraoperative exclusion criteria. The total study cohort consists of 861 patients. No patients were lost to follow-up (Figure 1). Patients included in the study were analyzed according to intention to treat.
A summary of the patient characteristics is given in Table 6. The groups were evenly distributed with the exception of significantly more patients with extra-cardiac arterial disease (p=0.04) and left main stenosis (p=0.03) in the glutamate group. There was a trend towards higher EuroSCORE in the glutamate group (p=0.13).
Table 6. Demographic and intraoperative data for the GLUTAMICS-trial (mean±SD or count n %).
Placebo n=433
Glutamate n=428
Age (years) 68±9 68±9 Female gender 18.9% 17.5% Diabetes mellitus 25.4% 23.9% Cerebrovascular disease 8.1% 8.5% Extra-cardiac arterial disease 9.3% 13.9% COPD 5.4% 7.6% Moderate-severe LV-dysfunction 19.2% 18.5% CCS class IV angina 55.9% 54.4% Angina at rest <48h preop 23.6% 19.2% Intravenous nitroglycerine preop 8.5% 8.9% Left main stem stenosis 35.2% 42.6% Additive EuroSCORE 5.0±2.8 5.3±2.8 Emergency procedure 5.5% 4.2% Number of bypassed vessels 3.8±1.2 3.8±1.2 Other operation than isolated CABG 4.6% 3.7% Cross clamp time (minutes) 54±22 53±21 CPB time (minutes) 83±30 84±31
43
Outcome for the whole study population in the GLUTAMICS-trial There was no significant difference in the incidence of the primary compos-ite endpoint between the groups. Secondary endpoints showed a trend towards fewer patients in the glutamate group who were hemodynamically unstable at completion of surgery (0.3% v 1.8%; p=0.07) and fewer pa-tients in the glutamate group requiring IABP on admission to ICU (0% v 1.2%; p=0.06).
Primary and major secondary endpoints for the GLUTAMICS-trial are shown in Table 7.
Table 7. Outcome GLUTAMICS-trial (mean±SD or count n %).
Placebo n=433
Glutamate n=428
p-value
Primary endpoint 5.8% 7.3% 0.41 LV-failure at weaning from CPB 4.2% 4.7% 0.74 Perioperative myocardial infarction 1.4% 2.6% 0.23 30-day mortality 1.2% 0.9% 1.0 Secondary endpoints Inotropes at weaning from CPB 12.3% 13.8% 0.54 SvO2 at weaning from CPB 72.2±7.3 72.0±7.6 0.69 a-Lactate mmol/L 5 minutes after protamine 1.7±0.6 1.6±0.6 0.07 Hemodynamic state at completion of surgery -Stable without inotropes 77.4% 78.5% 0.73 -Stable with inotropes 19.8% 22.3% 0.38 -Unstable with inotropes / IABP 1.8% 0.3% 0.07 IABP on admission to ICU 1.2% 0% 0.06 Severe circulatory failure 4.2% 2.3% 0.18 Stroke within 24h post op 1.4% 0.9% 0.75 Dialysis post op 1.4% 0.5% 0.29 Cardiac mortality (in hospital or 30-day) 0.9% 0.2% 0.37

42
4.3 Results of the GLUTAMICS-trial (Paper III) The GLUTAMICS-trial was conducted between October 4, 2005 and No-vember 12, 2009. A total of 865 patients were randomized and 4 patients, 2 in the glutamate group and 2 in the placebo group were excluded due to intraoperative exclusion criteria. The total study cohort consists of 861 patients. No patients were lost to follow-up (Figure 1). Patients included in the study were analyzed according to intention to treat.
A summary of the patient characteristics is given in Table 6. The groups were evenly distributed with the exception of significantly more patients with extra-cardiac arterial disease (p=0.04) and left main stenosis (p=0.03) in the glutamate group. There was a trend towards higher EuroSCORE in the glutamate group (p=0.13).
Table 6. Demographic and intraoperative data for the GLUTAMICS-trial (mean±SD or count n %).
Placebo n=433
Glutamate n=428
Age (years) 68±9 68±9 Female gender 18.9% 17.5% Diabetes mellitus 25.4% 23.9% Cerebrovascular disease 8.1% 8.5% Extra-cardiac arterial disease 9.3% 13.9% COPD 5.4% 7.6% Moderate-severe LV-dysfunction 19.2% 18.5% CCS class IV angina 55.9% 54.4% Angina at rest <48h preop 23.6% 19.2% Intravenous nitroglycerine preop 8.5% 8.9% Left main stem stenosis 35.2% 42.6% Additive EuroSCORE 5.0±2.8 5.3±2.8 Emergency procedure 5.5% 4.2% Number of bypassed vessels 3.8±1.2 3.8±1.2 Other operation than isolated CABG 4.6% 3.7% Cross clamp time (minutes) 54±22 53±21 CPB time (minutes) 83±30 84±31
43
Outcome for the whole study population in the GLUTAMICS-trial There was no significant difference in the incidence of the primary compos-ite endpoint between the groups. Secondary endpoints showed a trend towards fewer patients in the glutamate group who were hemodynamically unstable at completion of surgery (0.3% v 1.8%; p=0.07) and fewer pa-tients in the glutamate group requiring IABP on admission to ICU (0% v 1.2%; p=0.06).
Primary and major secondary endpoints for the GLUTAMICS-trial are shown in Table 7.
Table 7. Outcome GLUTAMICS-trial (mean±SD or count n %).
Placebo n=433
Glutamate n=428
p-value
Primary endpoint 5.8% 7.3% 0.41 LV-failure at weaning from CPB 4.2% 4.7% 0.74 Perioperative myocardial infarction 1.4% 2.6% 0.23 30-day mortality 1.2% 0.9% 1.0 Secondary endpoints Inotropes at weaning from CPB 12.3% 13.8% 0.54 SvO2 at weaning from CPB 72.2±7.3 72.0±7.6 0.69 a-Lactate mmol/L 5 minutes after protamine 1.7±0.6 1.6±0.6 0.07 Hemodynamic state at completion of surgery -Stable without inotropes 77.4% 78.5% 0.73 -Stable with inotropes 19.8% 22.3% 0.38 -Unstable with inotropes / IABP 1.8% 0.3% 0.07 IABP on admission to ICU 1.2% 0% 0.06 Severe circulatory failure 4.2% 2.3% 0.18 Stroke within 24h post op 1.4% 0.9% 0.75 Dialysis post op 1.4% 0.5% 0.29 Cardiac mortality (in hospital or 30-day) 0.9% 0.2% 0.37

44
ICU-stay or time on ventilator did not differ between the groups overall. However, patients with LV-failure at weaning from CPB had significantly shorter median ICU stay (25 [18-57] hours v 92 [41-139] hours; p=0.02) and ventilator treatment (5.0 [3.3-8.0] hours v 7.4 [5.8-49] hours; p=0.02) if they received glutamate infusion (Figure 5).
Cardiac mortality (in-hospital or 30-day) was 0.2% in the glutamate group and 0.9% the control group (p=0.37). There were no significant differences regarding the incidence of postoperative stroke.
Figure 5. Duration of ICU stay and ventilator treatment in patients with LV-failure at weaning from CPB (median+ interquartile range).
45
Adverse events There were no significant differences in the incidence of serious or non-serious adverse events between the glutamate group and the placebo group in the GLUTAMICS-trial. A table with all adverse events is presented in the Appendix.

44
ICU-stay or time on ventilator did not differ between the groups overall. However, patients with LV-failure at weaning from CPB had significantly shorter median ICU stay (25 [18-57] hours v 92 [41-139] hours; p=0.02) and ventilator treatment (5.0 [3.3-8.0] hours v 7.4 [5.8-49] hours; p=0.02) if they received glutamate infusion (Figure 5).
Cardiac mortality (in-hospital or 30-day) was 0.2% in the glutamate group and 0.9% the control group (p=0.37). There were no significant differences regarding the incidence of postoperative stroke.
Figure 5. Duration of ICU stay and ventilator treatment in patients with LV-failure at weaning from CPB (median+ interquartile range).
45
Adverse events There were no significant differences in the incidence of serious or non-serious adverse events between the glutamate group and the placebo group in the GLUTAMICS-trial. A table with all adverse events is presented in the Appendix.

46
Patients with CCS class IV angina In the GLUTAMICS-trial patients with CCS class IV angina undergoing isolated CABG were analyzed separately to address the population with unstable angina. A summary of the patient characteristics for this study cohort (n=458) is given in Table 8. The groups were evenly distributed with the exception of significantly more patients with left main stenosis (p=0.03) in the gluta-mate group.
Table 8. Demographic and intraoperative data for patients with CCS class IV an-gina undergoing isolated CABG (mean±SD or count n %).
Placebo n=233
Glutamate n=225
Age (years) 68±9 68±9 Female gender 19.7% 17.3% Diabetes mellitus 27.0% 23.6% Cerebrovascular disease 8.6% 8.9% Extra-cardiac arterial disease 10.7% 14.5% COPD 5.6% 9.0% Moderate-severe LV-dysfunction 21.0% 18.2% Angina at rest <48h preop 38.2% 31.2% Intravenous nitroglycerine preop 13.7% 13.3% Left main stem stenosis 34.3% 44.4% Additive EuroSCORE 5.2±3.0 5.4±2.9 Emergency procedure 9.0% 5.3% Number of bypassed vessels 3.8±1.2 3.8±1.2 Cross clamp time (minutes) 53±17 53±17 CPB time (minutes) 81±25 83±30
47
Outcome for patients with CCS class IV angina undergoing isolated CABG The primary composite endpoint did not differ significantly between the groups. Regarding secondary endpoints significantly fewer patients in the glutamate group developed severe circulatory failure (1.3% v 6.9%; p=0.004). Primary and major secondary endpoints for this subgroup analy-sis of the GLUTAMICS-trial are shown in Table 9.
Table 9. Outcome for patients with CCS class IV angina undergoing isolated CABG (mean±SD or count n %).
Placebo
n=233 Glutamate
n=225 p-value
Primary endpoint 7.8%(18) 7.6%(17) 1.0 LV-failure at weaning from CPB 5.2%(12) 5.3%(12) 1.0 Perioperative myocardial infarction 2.2%(5) 2.7%(6) 0.77 30-day mortality 1.3%(3) 0.9%(2) 1.0 Secondary endpoints Inotropes at weaning from CPB 12.0%(28) 11.2%(25) 0.88 SvO2 at weaning from CPB 71.7±7.1 71.6±7.6 0.82 a-Lactate mmol/L 5 minutes after protamine 1.8±0.6 1.6±0.5 0.006 Hemodynamic state at completion of surgery -Stable without inotropes 80.9%(188) 79.8%(180) 0.81 -Stable with inotropes 17.0%(40) 19.7%(44) 0.47 -Unstable with inotropes / IABP 2.2%(5) 0.5%(1) 0.22 IABP on admission to ICU 2.1%(5) 0 0.06 Severe circulatory failure 6.9%(16) 1.3%(3) 0.004 Stroke within 24h post op 0.8%(2) 0.9%(2) 1.0 Dialysis post op 2.6%(6) 0.4%(1) 0.12 Cardiac mortality (in hospital or 30-day) 0.9%(2) 0.4%(1) 1.0

46
Patients with CCS class IV angina In the GLUTAMICS-trial patients with CCS class IV angina undergoing isolated CABG were analyzed separately to address the population with unstable angina. A summary of the patient characteristics for this study cohort (n=458) is given in Table 8. The groups were evenly distributed with the exception of significantly more patients with left main stenosis (p=0.03) in the gluta-mate group.
Table 8. Demographic and intraoperative data for patients with CCS class IV an-gina undergoing isolated CABG (mean±SD or count n %).
Placebo n=233
Glutamate n=225
Age (years) 68±9 68±9 Female gender 19.7% 17.3% Diabetes mellitus 27.0% 23.6% Cerebrovascular disease 8.6% 8.9% Extra-cardiac arterial disease 10.7% 14.5% COPD 5.6% 9.0% Moderate-severe LV-dysfunction 21.0% 18.2% Angina at rest <48h preop 38.2% 31.2% Intravenous nitroglycerine preop 13.7% 13.3% Left main stem stenosis 34.3% 44.4% Additive EuroSCORE 5.2±3.0 5.4±2.9 Emergency procedure 9.0% 5.3% Number of bypassed vessels 3.8±1.2 3.8±1.2 Cross clamp time (minutes) 53±17 53±17 CPB time (minutes) 81±25 83±30
47
Outcome for patients with CCS class IV angina undergoing isolated CABG The primary composite endpoint did not differ significantly between the groups. Regarding secondary endpoints significantly fewer patients in the glutamate group developed severe circulatory failure (1.3% v 6.9%; p=0.004). Primary and major secondary endpoints for this subgroup analy-sis of the GLUTAMICS-trial are shown in Table 9.
Table 9. Outcome for patients with CCS class IV angina undergoing isolated CABG (mean±SD or count n %).
Placebo
n=233 Glutamate
n=225 p-value
Primary endpoint 7.8%(18) 7.6%(17) 1.0 LV-failure at weaning from CPB 5.2%(12) 5.3%(12) 1.0 Perioperative myocardial infarction 2.2%(5) 2.7%(6) 0.77 30-day mortality 1.3%(3) 0.9%(2) 1.0 Secondary endpoints Inotropes at weaning from CPB 12.0%(28) 11.2%(25) 0.88 SvO2 at weaning from CPB 71.7±7.1 71.6±7.6 0.82 a-Lactate mmol/L 5 minutes after protamine 1.8±0.6 1.6±0.5 0.006 Hemodynamic state at completion of surgery -Stable without inotropes 80.9%(188) 79.8%(180) 0.81 -Stable with inotropes 17.0%(40) 19.7%(44) 0.47 -Unstable with inotropes / IABP 2.2%(5) 0.5%(1) 0.22 IABP on admission to ICU 2.1%(5) 0 0.06 Severe circulatory failure 6.9%(16) 1.3%(3) 0.004 Stroke within 24h post op 0.8%(2) 0.9%(2) 1.0 Dialysis post op 2.6%(6) 0.4%(1) 0.12 Cardiac mortality (in hospital or 30-day) 0.9%(2) 0.4%(1) 1.0

48
Multivariable analysis was added to exclude that significant results ob-tained in the subgroup analysis were due to a skewed distribution of risk factors. This analysis showed that glutamate infusion was independently associated with a reduced risk of developing severe circulatory failure (OR 0.2; 95% confidence interval 0.04-0.72; p=0.02) (Table 10).
Table 10. Multivariable analysis of risk factors for severe circulatory failure in patients with CCS class IV angina undergoing isolated CABG.
Variables
Adjusted OR CI(95%) p-value
Preoperative troponin-T level* 2.2 1.3-3.7 0.004
Extra-cardiac vascular disease 6.5 1.8-23.6 0.005
Severe systolic LV-dysfunction 7.3 1.6-34.6 0.01
Emergency procedure 5.1 1.4-18.9 0.01
ST-depression ≥ 1 mV 3.8 1.0-14.4 0.05
Intravenous glutamate infusion 0.2 0.04-0.72 0.02
Hosmer-Lemeshow goodness-of-fit test-X2 (df 5) = 3.51, p = 0.62.
CI = confidence interval; LV = left ventricular; OR = odds ratio; * per unit change.
Results for the non-study cohort during the GLUTAMICS-trial period During the study period of the GLUTAMICS-trial a total of 2087 patients underwent surgery for acute coronary syndrome at the three participating centers. Of these 2087 patients 1064 were assessed for eligibility. An over-view of patient characteristics and outcome for the patients that never were assessed is presented in Table 11.
49
Table 11. Preoperative, intraoperative and outcome data for patients operated for acute coronary syndrome during the study period but not included in the GLU-TAMICS-trial (mean±SD or count n %).
* complete data available from two of the participating centers (n=780) ** data from all three participating centers (n=1222)
Patients operated for acute coronary syndrome during the study period but not included
in the GLUTAMICS-trial (n=780*)
Age (years) 68±9 Female gender 26.3% Diabetes 28.1% Cerebrovascular disease 8.6% Extra-cardiac arterial disease 11.4% COPD 7.1% Moderate-severe LV-dysfunction 25.9% Intravenous nitroglycerine preop 11.5% Left main stem stenosis 44.1% Additive EuroSCORE 6.1±3.9 Emergency procedure 11.5% Number of bypassed vessels 3.5±1.2 Cross clamp time (minutes) 58±29 CPB time (minutes) 95±47 Outcome 30-day mortality** 4.0% Hemodynamic state at completion of surgery -Stable without inotropes 65.4% -Stable with inotropes 29.7% -Unstable with inotropes / IABP 4.3% Dialysis post op 2.2% Stroke during hospital stay 2.3%
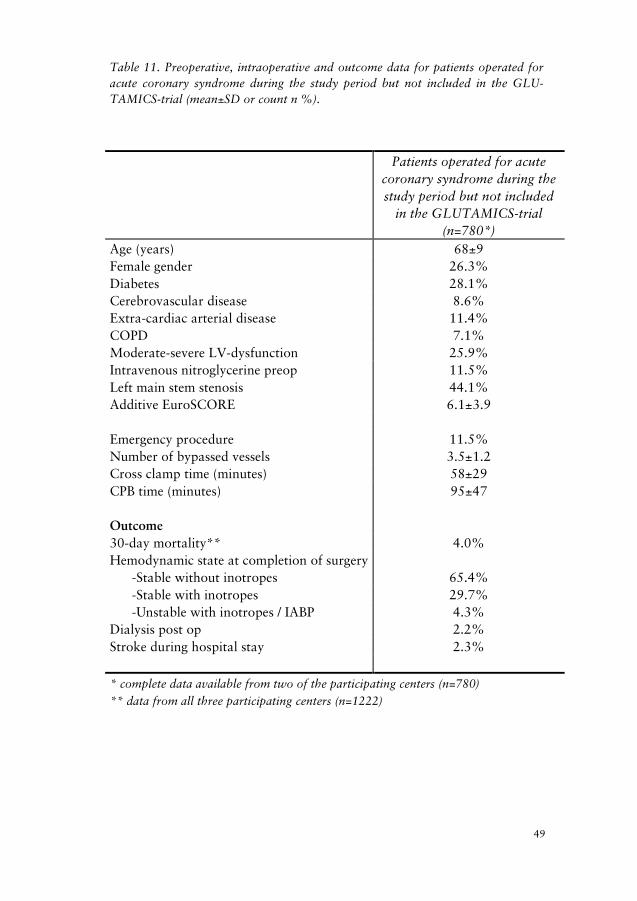
48
Multivariable analysis was added to exclude that significant results ob-tained in the subgroup analysis were due to a skewed distribution of risk factors. This analysis showed that glutamate infusion was independently associated with a reduced risk of developing severe circulatory failure (OR 0.2; 95% confidence interval 0.04-0.72; p=0.02) (Table 10).
Table 10. Multivariable analysis of risk factors for severe circulatory failure in patients with CCS class IV angina undergoing isolated CABG.
Variables
Adjusted OR CI(95%) p-value
Preoperative troponin-T level* 2.2 1.3-3.7 0.004
Extra-cardiac vascular disease 6.5 1.8-23.6 0.005
Severe systolic LV-dysfunction 7.3 1.6-34.6 0.01
Emergency procedure 5.1 1.4-18.9 0.01
ST-depression ≥ 1 mV 3.8 1.0-14.4 0.05
Intravenous glutamate infusion 0.2 0.04-0.72 0.02
Hosmer-Lemeshow goodness-of-fit test-X2 (df 5) = 3.51, p = 0.62.
CI = confidence interval; LV = left ventricular; OR = odds ratio; * per unit change.
Results for the non-study cohort during the GLUTAMICS-trial period During the study period of the GLUTAMICS-trial a total of 2087 patients underwent surgery for acute coronary syndrome at the three participating centers. Of these 2087 patients 1064 were assessed for eligibility. An over-view of patient characteristics and outcome for the patients that never were assessed is presented in Table 11.
49
Table 11. Preoperative, intraoperative and outcome data for patients operated for acute coronary syndrome during the study period but not included in the GLU-TAMICS-trial (mean±SD or count n %).
* complete data available from two of the participating centers (n=780) ** data from all three participating centers (n=1222)
Patients operated for acute coronary syndrome during the study period but not included
in the GLUTAMICS-trial (n=780*)
Age (years) 68±9 Female gender 26.3% Diabetes 28.1% Cerebrovascular disease 8.6% Extra-cardiac arterial disease 11.4% COPD 7.1% Moderate-severe LV-dysfunction 25.9% Intravenous nitroglycerine preop 11.5% Left main stem stenosis 44.1% Additive EuroSCORE 6.1±3.9 Emergency procedure 11.5% Number of bypassed vessels 3.5±1.2 Cross clamp time (minutes) 58±29 CPB time (minutes) 95±47 Outcome 30-day mortality** 4.0% Hemodynamic state at completion of surgery -Stable without inotropes 65.4% -Stable with inotropes 29.7% -Unstable with inotropes / IABP 4.3% Dialysis post op 2.2% Stroke during hospital stay 2.3%

50
Comment The GLUTAMICS-trial was terminated after interim analysis, as prespeci-fied stopping criteria (Appendix) were fulfilled with no absolute between group differences regarding the composite primary endpoint or significant difference regarding markers for myocardial injury or postoperative renal function in favor of glutamate. However, subsequent analysis revealed significant between group differences in favor of the glutamate group re-garding secondary endpoints related to hemodynamic recovery.
Patients with weaning problems from CPB had substantially shorter ICU-stay and ventilator treatment if they received intravenous glutamate infusion. In more ischemic patients (CCS class IV angina) significantly fewer patients developed severe circulatory failure in the glutamate group. Arterial lactate after weaning from CPB was lower in the glutamate group. No increase in serious or non-serious adverse events in patients receiving intravenous glutamate was detected.
51
4.4 The influence of inotropes in the GLUTAMICS-trial (Paper IV) Two of the three participating centers in the GLUTAMICS-trial accounted for 91% of the recruited patients. These centers exhibited markedly differ-ent policies regarding preemptive use of inotropic drugs to facilitate wean-ing from CPB. Inotropic drugs were used preemptively in 23.4% of the patients at Center A compared to 4.5% of the patients at Center B (p<0.0001)
Of all the patients in the GLUTAMICS-trial (n=861), 166 patients re-ceived inotropic drugs intraoperatively. These patients were analyzed with regard to the influence of intravenous glutamate infusion on primary and secondary outcome variables.
Comparison of Center A and Center B A total of 788 patients were included in the GLUTAMICS-trial at center A (n=252) and center B (n=536). Patient characteristics and intraoperative data for centers A and B are given in Table 12.

50
Comment The GLUTAMICS-trial was terminated after interim analysis, as prespeci-fied stopping criteria (Appendix) were fulfilled with no absolute between group differences regarding the composite primary endpoint or significant difference regarding markers for myocardial injury or postoperative renal function in favor of glutamate. However, subsequent analysis revealed significant between group differences in favor of the glutamate group re-garding secondary endpoints related to hemodynamic recovery.
Patients with weaning problems from CPB had substantially shorter ICU-stay and ventilator treatment if they received intravenous glutamate infusion. In more ischemic patients (CCS class IV angina) significantly fewer patients developed severe circulatory failure in the glutamate group. Arterial lactate after weaning from CPB was lower in the glutamate group. No increase in serious or non-serious adverse events in patients receiving intravenous glutamate was detected.
51
4.4 The influence of inotropes in the GLUTAMICS-trial (Paper IV) Two of the three participating centers in the GLUTAMICS-trial accounted for 91% of the recruited patients. These centers exhibited markedly differ-ent policies regarding preemptive use of inotropic drugs to facilitate wean-ing from CPB. Inotropic drugs were used preemptively in 23.4% of the patients at Center A compared to 4.5% of the patients at Center B (p<0.0001)
Of all the patients in the GLUTAMICS-trial (n=861), 166 patients re-ceived inotropic drugs intraoperatively. These patients were analyzed with regard to the influence of intravenous glutamate infusion on primary and secondary outcome variables.
Comparison of Center A and Center B A total of 788 patients were included in the GLUTAMICS-trial at center A (n=252) and center B (n=536). Patient characteristics and intraoperative data for centers A and B are given in Table 12.

52
Table 12. Demographic and intraoperative data for patients at center A and B (mean±SD or count n %).
Outcome Center A versus Center B The incidence of the composite primary endpoint was significantly lower at Center A (4.0% v 8.1%;p=0.03) mainly explained by a lower rate of LV-failure at weaning from CPB. However, the incidence of the secondary endpoint severe circulatory failure did not differ (3.6% v 2.6%). Thirty-day mortality was 1.2% v 1.1%. Primary and major secondary endpoints for Centers A and B are given in Table 13.
Center A n=252
Center B n=536
p-value
Age (years) 69±9 68±9 0.63 Female gender 20.6% 16.6% 0.17 Weight (kg) 83±15 82±14 0.46 Length (cm) 174±9 173±8 0.22 Diabetes mellitus 27.1% 24.8% 0.51 p-creatinine (µmol/L) 92±34 102±25 <0.001 Cerebrovascular disease 6.8% 9.4% 0.22 Extra-cardiac arterial disease 8.8% 13.4% 0.06 Active smokers 10.4% 20.5% 0.004 COPD 6.6% 6.9% 0.94 LV-dysfunction: moderate 11.2% 16.4% 0.05 LV-dysfunction: severe 6.4% 3.5% 0.09 CCS class IV angina 40.9% 68.1% <0.001 Angina at rest <48h preop 22.5% 21.8% 0.80 Intravenous nitroglycerine preop 6.0% 9.7% 0.10 Left main stem stenosis 49.0% 36.4% <0.001 Additive EuroSCORE 5.0±2.8 5.3±2.8 0.19 Emergency procedure 8.7% 3.5% 0.002 Number of bypassed vessels 3.6±1.0 3.9±1.3 <0.001 Other operation than isolated CABG 6.4% 3.4% 0.05 Cross clamp time (minutes) 52±23 55±20 <0.001 CPB time (minutes) 86±32 83±30 0.20
53
Table 13. Outcome for patients at Center A and B (mean±SD or count n %)
Center A n=252
Center B n=536
p-value
Primary endpoint 4.0% 8.1% 0.03 LV-failure at weaning from CPB 2.8% 5.4% 0.14 Perioperative myocardial infarction 1.6% 2.3% 0.79 30-day mortality 1.6% 1.5% 1.0 Secondary endpoints Inotropes at weaning from CPB 25.9% 7.6% <0.001 SvO2 at weaning from CPB 74.0±8.2 70.9±6.9 <0.001 a-Lactate mmol/L 5 minutes after protamine 1.68±0.7 1.72±0.5 0.04 Hemodynamic state at completion of surgery -Stable without inotropes 57.9% 86.9% <0.001 -Stable with inotropes 41.3% 11.4% <0.001 -Unstable with inotropes / IABP 0.8% 1.1% 1.0 IABP on admission to ICU 0.4% 0.7% 1.0 Severe circulatory failure 3.6% 2.6% 0.5 Stroke within 24h post op 1.2% 1.1% 1.0 Dialysis post op 1.6% 0.8% 0.28 Postop increase of p-Creatinine (∆ µmol/L) 12±43 6±33 0.04 Cardiac mortality (in hospital or 30-day) 0.8% 0.6% 0.66
Influence of glutamate in patients receiving inotropes intraoperatively Inotropic drugs were instituted intraoperatively in 166 patients. The most commonly used inotropic drugs where milrinone (58.8%) and epinephrine (46.4%). Levosimendan (7.3%), dopamine (4.2%) and dopexamine (1.8%) were also used. Of the 166 patients 78 where in the control group and 88 in the glutamate group. Patient characteristics and intraoperative data are given in Table 14.

52
Table 12. Demographic and intraoperative data for patients at center A and B (mean±SD or count n %).
Outcome Center A versus Center B The incidence of the composite primary endpoint was significantly lower at Center A (4.0% v 8.1%;p=0.03) mainly explained by a lower rate of LV-failure at weaning from CPB. However, the incidence of the secondary endpoint severe circulatory failure did not differ (3.6% v 2.6%). Thirty-day mortality was 1.2% v 1.1%. Primary and major secondary endpoints for Centers A and B are given in Table 13.
Center A n=252
Center B n=536
p-value
Age (years) 69±9 68±9 0.63 Female gender 20.6% 16.6% 0.17 Weight (kg) 83±15 82±14 0.46 Length (cm) 174±9 173±8 0.22 Diabetes mellitus 27.1% 24.8% 0.51 p-creatinine (µmol/L) 92±34 102±25 <0.001 Cerebrovascular disease 6.8% 9.4% 0.22 Extra-cardiac arterial disease 8.8% 13.4% 0.06 Active smokers 10.4% 20.5% 0.004 COPD 6.6% 6.9% 0.94 LV-dysfunction: moderate 11.2% 16.4% 0.05 LV-dysfunction: severe 6.4% 3.5% 0.09 CCS class IV angina 40.9% 68.1% <0.001 Angina at rest <48h preop 22.5% 21.8% 0.80 Intravenous nitroglycerine preop 6.0% 9.7% 0.10 Left main stem stenosis 49.0% 36.4% <0.001 Additive EuroSCORE 5.0±2.8 5.3±2.8 0.19 Emergency procedure 8.7% 3.5% 0.002 Number of bypassed vessels 3.6±1.0 3.9±1.3 <0.001 Other operation than isolated CABG 6.4% 3.4% 0.05 Cross clamp time (minutes) 52±23 55±20 <0.001 CPB time (minutes) 86±32 83±30 0.20
53
Table 13. Outcome for patients at Center A and B (mean±SD or count n %)
Center A n=252
Center B n=536
p-value
Primary endpoint 4.0% 8.1% 0.03 LV-failure at weaning from CPB 2.8% 5.4% 0.14 Perioperative myocardial infarction 1.6% 2.3% 0.79 30-day mortality 1.6% 1.5% 1.0 Secondary endpoints Inotropes at weaning from CPB 25.9% 7.6% <0.001 SvO2 at weaning from CPB 74.0±8.2 70.9±6.9 <0.001 a-Lactate mmol/L 5 minutes after protamine 1.68±0.7 1.72±0.5 0.04 Hemodynamic state at completion of surgery -Stable without inotropes 57.9% 86.9% <0.001 -Stable with inotropes 41.3% 11.4% <0.001 -Unstable with inotropes / IABP 0.8% 1.1% 1.0 IABP on admission to ICU 0.4% 0.7% 1.0 Severe circulatory failure 3.6% 2.6% 0.5 Stroke within 24h post op 1.2% 1.1% 1.0 Dialysis post op 1.6% 0.8% 0.28 Postop increase of p-Creatinine (∆ µmol/L) 12±43 6±33 0.04 Cardiac mortality (in hospital or 30-day) 0.8% 0.6% 0.66
Influence of glutamate in patients receiving inotropes intraoperatively Inotropic drugs were instituted intraoperatively in 166 patients. The most commonly used inotropic drugs where milrinone (58.8%) and epinephrine (46.4%). Levosimendan (7.3%), dopamine (4.2%) and dopexamine (1.8%) were also used. Of the 166 patients 78 where in the control group and 88 in the glutamate group. Patient characteristics and intraoperative data are given in Table 14.
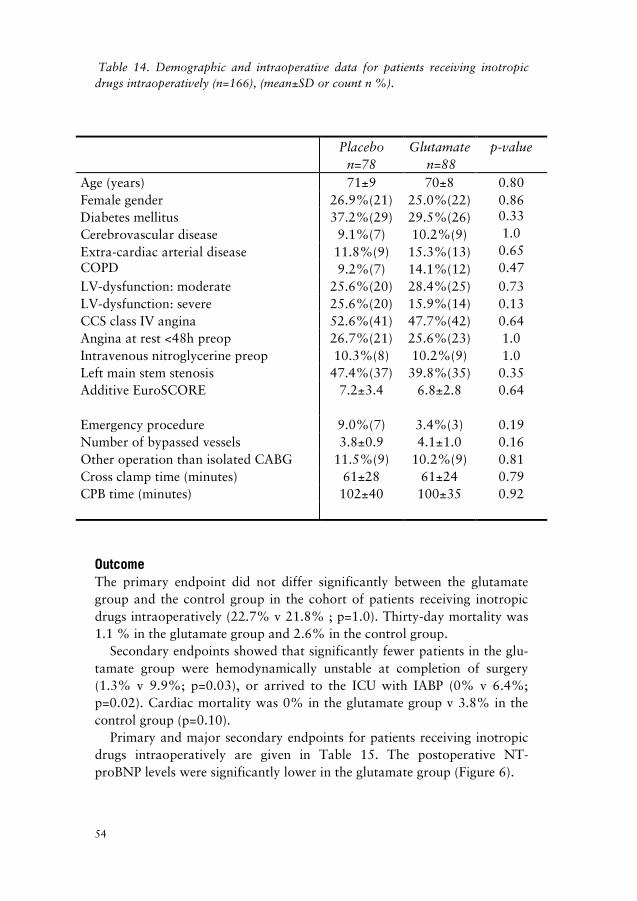
54
Table 14. Demographic and intraoperative data for patients receiving inotropic drugs intraoperatively (n=166), (mean±SD or count n %).
Outcome The primary endpoint did not differ significantly between the glutamate group and the control group in the cohort of patients receiving inotropic drugs intraoperatively (22.7% v 21.8% ; p=1.0). Thirty-day mortality was 1.1 % in the glutamate group and 2.6% in the control group.
Secondary endpoints showed that significantly fewer patients in the glu-tamate group were hemodynamically unstable at completion of surgery (1.3% v 9.9%; p=0.03), or arrived to the ICU with IABP (0% v 6.4%; p=0.02). Cardiac mortality was 0% in the glutamate group v 3.8% in the control group (p=0.10).
Primary and major secondary endpoints for patients receiving inotropic drugs intraoperatively are given in Table 15. The postoperative NT-proBNP levels were significantly lower in the glutamate group (Figure 6).
Placebo n=78
Glutamate n=88
p-value
Age (years) 71±9 70±8 0.80 Female gender 26.9%(21) 25.0%(22) 0.86 Diabetes mellitus 37.2%(29) 29.5%(26) 0.33 Cerebrovascular disease 9.1%(7) 10.2%(9) 1.0 Extra-cardiac arterial disease 11.8%(9) 15.3%(13) 0.65 COPD 9.2%(7) 14.1%(12) 0.47 LV-dysfunction: moderate 25.6%(20) 28.4%(25) 0.73 LV-dysfunction: severe 25.6%(20) 15.9%(14) 0.13 CCS class IV angina 52.6%(41) 47.7%(42) 0.64 Angina at rest <48h preop 26.7%(21) 25.6%(23) 1.0 Intravenous nitroglycerine preop 10.3%(8) 10.2%(9) 1.0 Left main stem stenosis 47.4%(37) 39.8%(35) 0.35 Additive EuroSCORE 7.2±3.4 6.8±2.8 0.64 Emergency procedure 9.0%(7) 3.4%(3) 0.19 Number of bypassed vessels 3.8±0.9 4.1±1.0 0.16 Other operation than isolated CABG 11.5%(9) 10.2%(9) 0.81 Cross clamp time (minutes) 61±28 61±24 0.79 CPB time (minutes) 102±40 100±35 0.92
55
Table 15. Outcome for patients receiving inotropic drugs intraoperatively (n=166), (mean±SD or count n %)* n=71 ** n=78.
Placebo n=78
Glutamate n=88
p-value
Primary endpoint 21.8%(17) 22.7%(20) 1.0 LV-failure at weaning from CPB 20.5%(16) 18.2%(16) 0.84 Perioperative myocardial infarction 3.8%(3) 6.8%(6) 0.50 30-day mortality 2.6%(2) 1.1%(1) 0.49 Secondary endpoints Inotropes at weaning from CPB 64.9%(50) 65.9%(58) 0.87 SvO2 at weaning from CPB 70.1±8.5 71.2±10.3 0.37 a-Lactate mmol/L 5 minutes after protamine 2.05±0.8 1.78±0.6 0.09 Hemodynamic state at completion of surgery -Stable without inotropes 14.1%(10)* 19.2%(15)** 0.52 -Stable with inotropes 76.1%(54)* 79.5%(62)** 0.87 -Unstable with inotropes / IABP 9.9%(7)* 1.3%(1)** 0.03 IABP on admission to ICU 6.4%(5) 0 0.02 Severe circulatory failure 16.7%(13) 8.0%(7) 0.10 Stroke within 24h post op 2.6%(2) 1.1%(1) 0.49 Dialysis post op 3.8%(3) 1.1%(1) 0.34 Cardiac mortality (in hospital or 30-day) 3.8%(3) 0 0.10

54
Table 14. Demographic and intraoperative data for patients receiving inotropic drugs intraoperatively (n=166), (mean±SD or count n %).
Outcome The primary endpoint did not differ significantly between the glutamate group and the control group in the cohort of patients receiving inotropic drugs intraoperatively (22.7% v 21.8% ; p=1.0). Thirty-day mortality was 1.1 % in the glutamate group and 2.6% in the control group.
Secondary endpoints showed that significantly fewer patients in the glu-tamate group were hemodynamically unstable at completion of surgery (1.3% v 9.9%; p=0.03), or arrived to the ICU with IABP (0% v 6.4%; p=0.02). Cardiac mortality was 0% in the glutamate group v 3.8% in the control group (p=0.10).
Primary and major secondary endpoints for patients receiving inotropic drugs intraoperatively are given in Table 15. The postoperative NT-proBNP levels were significantly lower in the glutamate group (Figure 6).
Placebo n=78
Glutamate n=88
p-value
Age (years) 71±9 70±8 0.80 Female gender 26.9%(21) 25.0%(22) 0.86 Diabetes mellitus 37.2%(29) 29.5%(26) 0.33 Cerebrovascular disease 9.1%(7) 10.2%(9) 1.0 Extra-cardiac arterial disease 11.8%(9) 15.3%(13) 0.65 COPD 9.2%(7) 14.1%(12) 0.47 LV-dysfunction: moderate 25.6%(20) 28.4%(25) 0.73 LV-dysfunction: severe 25.6%(20) 15.9%(14) 0.13 CCS class IV angina 52.6%(41) 47.7%(42) 0.64 Angina at rest <48h preop 26.7%(21) 25.6%(23) 1.0 Intravenous nitroglycerine preop 10.3%(8) 10.2%(9) 1.0 Left main stem stenosis 47.4%(37) 39.8%(35) 0.35 Additive EuroSCORE 7.2±3.4 6.8±2.8 0.64 Emergency procedure 9.0%(7) 3.4%(3) 0.19 Number of bypassed vessels 3.8±0.9 4.1±1.0 0.16 Other operation than isolated CABG 11.5%(9) 10.2%(9) 0.81 Cross clamp time (minutes) 61±28 61±24 0.79 CPB time (minutes) 102±40 100±35 0.92
55
Table 15. Outcome for patients receiving inotropic drugs intraoperatively (n=166), (mean±SD or count n %)* n=71 ** n=78.
Placebo n=78
Glutamate n=88
p-value
Primary endpoint 21.8%(17) 22.7%(20) 1.0 LV-failure at weaning from CPB 20.5%(16) 18.2%(16) 0.84 Perioperative myocardial infarction 3.8%(3) 6.8%(6) 0.50 30-day mortality 2.6%(2) 1.1%(1) 0.49 Secondary endpoints Inotropes at weaning from CPB 64.9%(50) 65.9%(58) 0.87 SvO2 at weaning from CPB 70.1±8.5 71.2±10.3 0.37 a-Lactate mmol/L 5 minutes after protamine 2.05±0.8 1.78±0.6 0.09 Hemodynamic state at completion of surgery -Stable without inotropes 14.1%(10)* 19.2%(15)** 0.52 -Stable with inotropes 76.1%(54)* 79.5%(62)** 0.87 -Unstable with inotropes / IABP 9.9%(7)* 1.3%(1)** 0.03 IABP on admission to ICU 6.4%(5) 0 0.02 Severe circulatory failure 16.7%(13) 8.0%(7) 0.10 Stroke within 24h post op 2.6%(2) 1.1%(1) 0.49 Dialysis post op 3.8%(3) 1.1%(1) 0.34 Cardiac mortality (in hospital or 30-day) 3.8%(3) 0 0.10

56
Figure 6. Pre- and postoperative NT-proBNP levels in patients receiving inotropic drugs intraoperatively.
Comment This post-hoc analysis suggests that a liberal policy regarding preemptive use of inotropic drugs to facilitate weaning from CPB had a significant influence on the primary endpoint of the GLUTAMICS-trial since LV-failure at weaning from CPB constituted the major component of the com-posite primary endpoint in the trial. Preemptive use of inotropic drugs did not, however, lower the incidence of severe circulatory failure.
Glutamate infusion was associated with significantly lower postopera-tive NT-proBNP levels, fewer patients hemodynamically unstable at com-pletion of surgery or in need of IABP on arrival to the ICU.
NT-proBNP ng/L
0
2000
4000
6000
8000
10000
12000
Preop Postop day 1 Postop day 3
placebo n=29glutamate n=31
p=0.017
57
5 General discussion Postoperative heart failure precipitated by myocardial ischemia remains a major cause of postoperative morbidity and mortality after CABG2, 6, 13. Conventional treatment with inotropic drugs is poorly documented with regard to outcome and carries potential hazards due to increased myocar-dial oxygen demand3-5, 9, 26. In this thesis an alternative approach with the aim to prevent ischemic injury and promote post-ischemic myocardial re-covery was studied.
A metabolic strategy to prevent and treat postoperative heart failure in-volving adherence to physiological principles to minimize myocardial and systemic oxygen expenditure, and metabolic interventions with glutamate and high-dose GIK to increase myocardial tolerance to ischemia and facili-tate myocardial recovery after ischemia was evolved during a five-year period100. Based on encouraging clinical results in patients with LV-dysfunction the GLUTAMICS-trial was initiated. In this trial 861 patients undergoing surgery for acute coronary syndrome were randomly allocated to blinded intravenous infusion of L-glutamic acid or saline. The trial was conducted at three cardiac surgery centers in Sweden according to the prin-ciples of Good Clinical Practice including professional external monitoring.
The event rate in the GLUTAMICS-trial was lower than anticipated re-ducing the power of the trial and no difference regarding the primary end-point – a composite of postoperative mortality, perioperative myocardial infarction or LV-failure on weaning from CPB – was detected. However, regarding secondary endpoints significant differences compatible with a beneficial effect of glutamate on post-ischemic myocardial recovery was found.

56
Figure 6. Pre- and postoperative NT-proBNP levels in patients receiving inotropic drugs intraoperatively.
Comment This post-hoc analysis suggests that a liberal policy regarding preemptive use of inotropic drugs to facilitate weaning from CPB had a significant influence on the primary endpoint of the GLUTAMICS-trial since LV-failure at weaning from CPB constituted the major component of the com-posite primary endpoint in the trial. Preemptive use of inotropic drugs did not, however, lower the incidence of severe circulatory failure.
Glutamate infusion was associated with significantly lower postopera-tive NT-proBNP levels, fewer patients hemodynamically unstable at com-pletion of surgery or in need of IABP on arrival to the ICU.
NT-proBNP ng/L
0
2000
4000
6000
8000
10000
12000
Preop Postop day 1 Postop day 3
placebo n=29glutamate n=31
p=0.017
57
5 General discussion Postoperative heart failure precipitated by myocardial ischemia remains a major cause of postoperative morbidity and mortality after CABG2, 6, 13. Conventional treatment with inotropic drugs is poorly documented with regard to outcome and carries potential hazards due to increased myocar-dial oxygen demand3-5, 9, 26. In this thesis an alternative approach with the aim to prevent ischemic injury and promote post-ischemic myocardial re-covery was studied.
A metabolic strategy to prevent and treat postoperative heart failure in-volving adherence to physiological principles to minimize myocardial and systemic oxygen expenditure, and metabolic interventions with glutamate and high-dose GIK to increase myocardial tolerance to ischemia and facili-tate myocardial recovery after ischemia was evolved during a five-year period100. Based on encouraging clinical results in patients with LV-dysfunction the GLUTAMICS-trial was initiated. In this trial 861 patients undergoing surgery for acute coronary syndrome were randomly allocated to blinded intravenous infusion of L-glutamic acid or saline. The trial was conducted at three cardiac surgery centers in Sweden according to the prin-ciples of Good Clinical Practice including professional external monitoring.
The event rate in the GLUTAMICS-trial was lower than anticipated re-ducing the power of the trial and no difference regarding the primary end-point – a composite of postoperative mortality, perioperative myocardial infarction or LV-failure on weaning from CPB – was detected. However, regarding secondary endpoints significant differences compatible with a beneficial effect of glutamate on post-ischemic myocardial recovery was found.

58
5.1 Metabolic strategy in CABG patients with LV-dysfunction This is one of few studies to address this category of patients from a pers-pective of perioperative management and it raises important questions that deserve to be addressed in future studies. The metabolic strategy evolved during a five-year period and the study cohort of patients with LV-dysfunction comprises 104 patients from a cohort of 775 patients operated for ischemic heart disease by two surgeons.
Figure 7. Demonstrating the shift in preferred therapy from 1991-1995 in 775 patients when the metabolic strategy was introduced.
The metabolic strategy was associated with lower 30-day mortality (1.0%) than previously reported in patients with severe LV-dysfunction undergo-ing CABG. It was also substantially lower than the expected risk adjusted mortality of 8.3% according to logistic EuroSCORE. Long-term survival was an even more encouraging with a crude 5-year survival of 89.4%.
91 92 93 94 95
0
5
10
15
20
25
30
35
Inotropes for weaningMechanical assistGIKGlutamate
59
Alternative measures that can enhance myocardial recovery and function without putting further strain on the heart are particularly desirable in patients with limited myocardial reserve. Our experience demonstrates that traditional pharmacological inotropic support for weaning from CPB can be replaced by alternative measures even in patients with severely com-promised LV-function without jeopardizing renal function. As the confi-dence in the metabolic strategy grew the use of inotropes for weaning from CPB during the latter half of the studied period was reduced to 2.6%. The average doses of inotropes when used were low (Paper I), usually in the dose interval known to enhance renal perfusion.
Some degree of extended CPB was employed in virtually all patients and CPB was substantially extended in patients with weaning difficulty with an average reperfusion time of approximately 80 minutes to permit myocar-dial recovery during metabolic support. The potential adverse effects of CPB are well known and many surgeons advocate short perfusion times and even avoidance of CPB. However, our results suggest that under cer-tain circumstances the benefits of unloading the heart may outweigh the drawbacks of CPB. These results are in agreement with Royster et al who found that long pump times were associated with lower need for inotropes after coronary surgery on patients with LVEF ≤ 0.4518. In animals prema-ture use of inotropic drugs for weaning from CPB has been shown to im-pede metabolic and functional recovery of the heart105.
It can be argued that a strategy that accepts low cardiac outputs could jeopardize perfusion of vital organs. Renal function is a sensitive marker of the adequacy of hemodynamic treatment. This report and previous ex-perience show that patients with compromised ventricular function and even overt postoperative heart failure can be treated with a low incidence of renal complications. In this study an increase of s-creatinine by 50% or more compared to preoperative values was found in 2.9 % of the cases, which is substantially lower than the 16% overall incidence after CABG surgery reported from a comparable Scandinavian Center106.
The metabolic strategy comprises a multimodal approach and although it is difficult to discern the relative importance of each issue from the present study, all major aspects have been addressed separately by our group and others107. To elucidate the clinical role of glutamate or high-dose GIK adequately powered randomized trials are necessary. From other areas of surgical research it has been argued that it may be difficult to improve clinical outcome with single measures and that a multimodal approach might be necessary to achieve such aims107.

58
5.1 Metabolic strategy in CABG patients with LV-dysfunction This is one of few studies to address this category of patients from a pers-pective of perioperative management and it raises important questions that deserve to be addressed in future studies. The metabolic strategy evolved during a five-year period and the study cohort of patients with LV-dysfunction comprises 104 patients from a cohort of 775 patients operated for ischemic heart disease by two surgeons.
Figure 7. Demonstrating the shift in preferred therapy from 1991-1995 in 775 patients when the metabolic strategy was introduced.
The metabolic strategy was associated with lower 30-day mortality (1.0%) than previously reported in patients with severe LV-dysfunction undergo-ing CABG. It was also substantially lower than the expected risk adjusted mortality of 8.3% according to logistic EuroSCORE. Long-term survival was an even more encouraging with a crude 5-year survival of 89.4%.
91 92 93 94 95
0
5
10
15
20
25
30
35
Inotropes for weaningMechanical assistGIKGlutamate
59
Alternative measures that can enhance myocardial recovery and function without putting further strain on the heart are particularly desirable in patients with limited myocardial reserve. Our experience demonstrates that traditional pharmacological inotropic support for weaning from CPB can be replaced by alternative measures even in patients with severely com-promised LV-function without jeopardizing renal function. As the confi-dence in the metabolic strategy grew the use of inotropes for weaning from CPB during the latter half of the studied period was reduced to 2.6%. The average doses of inotropes when used were low (Paper I), usually in the dose interval known to enhance renal perfusion.
Some degree of extended CPB was employed in virtually all patients and CPB was substantially extended in patients with weaning difficulty with an average reperfusion time of approximately 80 minutes to permit myocar-dial recovery during metabolic support. The potential adverse effects of CPB are well known and many surgeons advocate short perfusion times and even avoidance of CPB. However, our results suggest that under cer-tain circumstances the benefits of unloading the heart may outweigh the drawbacks of CPB. These results are in agreement with Royster et al who found that long pump times were associated with lower need for inotropes after coronary surgery on patients with LVEF ≤ 0.4518. In animals prema-ture use of inotropic drugs for weaning from CPB has been shown to im-pede metabolic and functional recovery of the heart105.
It can be argued that a strategy that accepts low cardiac outputs could jeopardize perfusion of vital organs. Renal function is a sensitive marker of the adequacy of hemodynamic treatment. This report and previous ex-perience show that patients with compromised ventricular function and even overt postoperative heart failure can be treated with a low incidence of renal complications. In this study an increase of s-creatinine by 50% or more compared to preoperative values was found in 2.9 % of the cases, which is substantially lower than the 16% overall incidence after CABG surgery reported from a comparable Scandinavian Center106.
The metabolic strategy comprises a multimodal approach and although it is difficult to discern the relative importance of each issue from the present study, all major aspects have been addressed separately by our group and others107. To elucidate the clinical role of glutamate or high-dose GIK adequately powered randomized trials are necessary. From other areas of surgical research it has been argued that it may be difficult to improve clinical outcome with single measures and that a multimodal approach might be necessary to achieve such aims107.

60
5.2 The GLUTAMICS-trial Several hundred experimental interventions have been reported to protect the ischemic myocardium in animals; however, with the exception of early reperfusion, none has been translated into clinical practice according to Bolli et al108. Lack of commercial interest in substances not protected by patents may have limited the conductance of adequately powered random-ized controlled trials. Glutamate is one of these substrates that has been claimed to protect the heart from ischemia and facilitate metabolic and hemodynamic recovery after ischemic insults58, 59, 76-83, 85, 87, 92-94, 98, 109, 110.
Based on the encouraging clinical experience with the metabolic strategy the GLUTAMICS-trial was initiated (Paper III). In this trial we decided to focus on the clinical effects of intravenous glutamate infusion rather than high-dose GIK because of several reasons. Intravenous glutamate is easy to administer, it does not require specific monitoring and it can be studied in a blinded fashion111. Furthermore, it would have been difficult to interpret the results if both interventions had been investigated simultaneously and the sample size required to investigate both interventions separately was beyond our resources. Also, in our clinical practice based on the Leuven experience, high-dose GIK had been replaced by a modified blood glucose protocol similar to the STS guidelines22, 112.
Patients with acute coronary syndrome were chosen for the GLUTAM-ICS-trial as they represented the largest risk group in our practice. Since the planning of the trial the proportion of patients with unstable angina un-dergoing CABG decreased in favor of patients accepted for urgent surgery due to non-STEMI. Patients requiring emergency surgery were not eligible because of ethical reasons further contributing to lower than anticipated event rates. Thus, it is questionable if the cohort studied can be regarded a high-risk group. The incidence of the primary endpoint was also influenced by clinical management, as will be discussed below.
No significant between group differences were found regarding the composite primary endpoint or markers for myocardial injury or postop-erative renal function. The latter finding implied that prespecified stopping criteria were fulfilled at interim analysis and, hence, the study was termi-nated. Subsequent analysis revealed significant between group differences in favor of the glutamate group regarding secondary endpoints related to hemodynamic recovery.
The results are compatible with the hypothesis that glutamate mitigates postoperative heart failure by enhancing myocardial recovery. Although the incidence of LV-failure at weaning from CPB did not differ between the groups, post-hoc analysis revealed that patients with weaning problems treated with glutamate had substantially shorter ICU stay and ventilator
61
treatment (Figure 5). Patients with heart failure at weaning from CPB were those in whom the first encouraging clinical experience with intravenous glutamate was obtained in our practice99. Unpublished clinical results for this category of patients in the GLUTAMICS-trial, further support the above suggested mechanism (Table 16).
Table 16. Outcome data for patients with LV-failure at weaning from CPB (median+ interquartile range, mean±SD or count n %).
Placebo n=18
Glutamate n=20
p-value
a-Lactate mmol/L 5 minutes after protamine 2.5±1.0 1.7±0.5 0.004 Hemodynamic state at completion of surgery -Unstable with inotropes / IABP 31% (5/16) 0 0.01 Severe circulatory failure 56%(10/18) 15%(3/20) 0.02 Postop increase of p-Creatinine (∆ µmol/L) 58±87 19±34 0.08 Ventilator treatment (hours) 7.4 [5.8-49] 5.0 [3.3-8.0] 0.02 ICU stay (hours) 92 [41-139] 25 [18-57] 0.02 Patients with CCS class IV angina undergoing isolated CABG were ana-lyzed separately to address the issue of unstable angina. In this cohort sig-nificantly fewer patients developed severe circulatory failure in the gluta-mate group. Multivariable analysis identified intravenous glutamate infu-sion as the only independent variable associated with a reduced incidence of severe circulatory failure.
To conclude, in this investigator initiated trial on 861 patients with acute coronary syndrome undergoing CABG glutamate did not prevent perioperative myocardial infarction or postoperative heart failure but the results are compatible with a beneficial effect of glutamate on post-ischemic myocardial recovery.
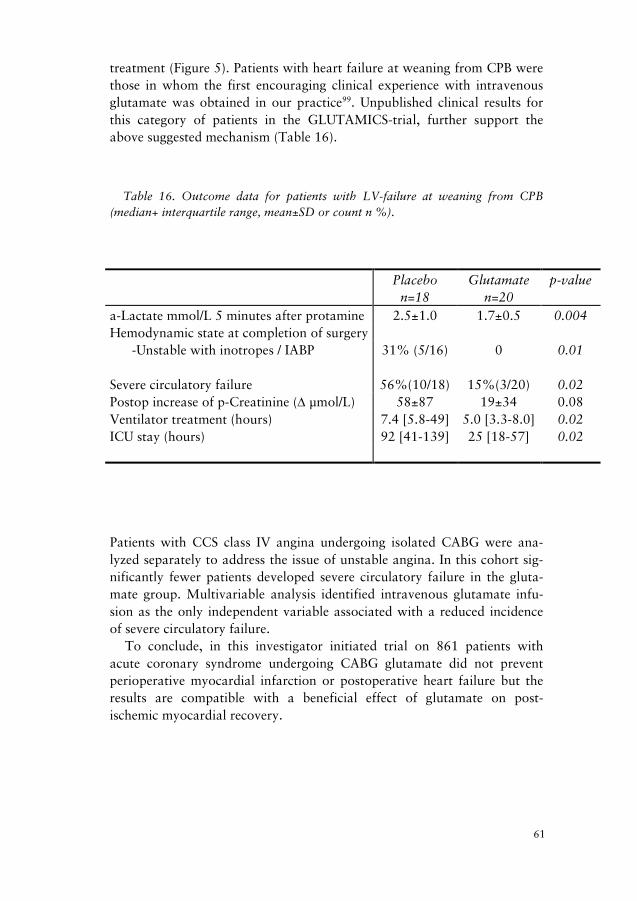
60
5.2 The GLUTAMICS-trial Several hundred experimental interventions have been reported to protect the ischemic myocardium in animals; however, with the exception of early reperfusion, none has been translated into clinical practice according to Bolli et al108. Lack of commercial interest in substances not protected by patents may have limited the conductance of adequately powered random-ized controlled trials. Glutamate is one of these substrates that has been claimed to protect the heart from ischemia and facilitate metabolic and hemodynamic recovery after ischemic insults58, 59, 76-83, 85, 87, 92-94, 98, 109, 110.
Based on the encouraging clinical experience with the metabolic strategy the GLUTAMICS-trial was initiated (Paper III). In this trial we decided to focus on the clinical effects of intravenous glutamate infusion rather than high-dose GIK because of several reasons. Intravenous glutamate is easy to administer, it does not require specific monitoring and it can be studied in a blinded fashion111. Furthermore, it would have been difficult to interpret the results if both interventions had been investigated simultaneously and the sample size required to investigate both interventions separately was beyond our resources. Also, in our clinical practice based on the Leuven experience, high-dose GIK had been replaced by a modified blood glucose protocol similar to the STS guidelines22, 112.
Patients with acute coronary syndrome were chosen for the GLUTAM-ICS-trial as they represented the largest risk group in our practice. Since the planning of the trial the proportion of patients with unstable angina un-dergoing CABG decreased in favor of patients accepted for urgent surgery due to non-STEMI. Patients requiring emergency surgery were not eligible because of ethical reasons further contributing to lower than anticipated event rates. Thus, it is questionable if the cohort studied can be regarded a high-risk group. The incidence of the primary endpoint was also influenced by clinical management, as will be discussed below.
No significant between group differences were found regarding the composite primary endpoint or markers for myocardial injury or postop-erative renal function. The latter finding implied that prespecified stopping criteria were fulfilled at interim analysis and, hence, the study was termi-nated. Subsequent analysis revealed significant between group differences in favor of the glutamate group regarding secondary endpoints related to hemodynamic recovery.
The results are compatible with the hypothesis that glutamate mitigates postoperative heart failure by enhancing myocardial recovery. Although the incidence of LV-failure at weaning from CPB did not differ between the groups, post-hoc analysis revealed that patients with weaning problems treated with glutamate had substantially shorter ICU stay and ventilator
61
treatment (Figure 5). Patients with heart failure at weaning from CPB were those in whom the first encouraging clinical experience with intravenous glutamate was obtained in our practice99. Unpublished clinical results for this category of patients in the GLUTAMICS-trial, further support the above suggested mechanism (Table 16).
Table 16. Outcome data for patients with LV-failure at weaning from CPB (median+ interquartile range, mean±SD or count n %).
Placebo n=18
Glutamate n=20
p-value
a-Lactate mmol/L 5 minutes after protamine 2.5±1.0 1.7±0.5 0.004 Hemodynamic state at completion of surgery -Unstable with inotropes / IABP 31% (5/16) 0 0.01 Severe circulatory failure 56%(10/18) 15%(3/20) 0.02 Postop increase of p-Creatinine (∆ µmol/L) 58±87 19±34 0.08 Ventilator treatment (hours) 7.4 [5.8-49] 5.0 [3.3-8.0] 0.02 ICU stay (hours) 92 [41-139] 25 [18-57] 0.02 Patients with CCS class IV angina undergoing isolated CABG were ana-lyzed separately to address the issue of unstable angina. In this cohort sig-nificantly fewer patients developed severe circulatory failure in the gluta-mate group. Multivariable analysis identified intravenous glutamate infu-sion as the only independent variable associated with a reduced incidence of severe circulatory failure.
To conclude, in this investigator initiated trial on 861 patients with acute coronary syndrome undergoing CABG glutamate did not prevent perioperative myocardial infarction or postoperative heart failure but the results are compatible with a beneficial effect of glutamate on post-ischemic myocardial recovery.

62
5.3 The influence of inotropic drugs in the GLUTAMICS-trial The aim of this study (Paper IV) was to investigate if preemptive use of inotropic drugs influenced the primary endpoint of the GLUTAMICS trial and if glutamate influenced outcome in patients receiving inotropes intra-operatively.
At an early stage of the GLUTAMICS-trial the clinical endpoints com-mittee identified that preemptive use of inotropic drugs in patients with anticipated circulatory problems often prohibited the diagnosis of heart failure on weaning from CPB even in patients that later developed severe circulatory failure.
The fact that the two major centers participating in the trial exhibited markedly different policies regarding preemptive use of inotropic drugs permitted us to assess its implications on the primary endpoint. The results of our post-hoc analysis agree with the clinical impression of the clinical endpoints committee.
A liberal policy for preemptive use of inotropic drugs to facilitate wean-ing from CPB was associated with more patients developing severe circula-tory failure than fulfilled criteria for LV-failure at weaning from CPB. A restrictive policy was associated with the opposite finding. Given that LV-failure at weaning from CPB constituted the major component of the com-posite primary endpoint we conclude that preemptive use of inotropic drugs had substantial implications on the primary endpoint of the GLU-TAMICS-trial.
The choice of primary endpoint was based on clinical experience with metabolic interventions employing restrictive use of inotropic drugs100, 113. However, participating centers and individual clinicians were free to insti-tute inotropic drugs according to their choice and usual practice. In retro-spect, the discrepancy in the use of inotropic drugs between center A and B is not unexpected given the lack of generally accepted guidelines for ino-tropic therapy3-5.
The secondary endpoint late circulatory failure was added to the proto-col as an amendment to identify these cases. In conjunction with the sec-ondary endpoint severe circulatory failure it allowed discrimination of mild short-lasting heart failure at weaning from CPB from clinically significant heart failure requiring substantial circulatory support and leading to pro-longed ICU stay or death.
The patients that received inotropic drugs intraoperatively were those in whom circulatory failure was anticipated or manifest. Patients at higher risk are obviously better suited to evaluate metabolic intervention assumed to enhance myocardial recovery (Figure 8). In patients that received ino-
63
tropic drugs intraoperatively, intravenous glutamate infusion was associ-ated with significantly fewer patients hemodynamically unstable at comple-tion of surgery or in need of IABP on admisson to ICU.
Postoperative NT-proBNP levels were also significantly lower in the glu-tamate group (Figure 6).
Figure 8. Proportion of patients hemodynamically unstable at completion of sur-gery despite inotropes or in need of IABP.
To conclude, a liberal policy regarding preemptive use of inotropic drugs to facilitate weaning from CPB had a significant influence on the primary endpoint of the GLUTAMICS-trial but did not lower the incidence of se-vere circulatory failure. Intravenous glutamate infusion was associated with a beneficial effect on hemodynamic outcome in patients receiving inotropic drugs intraoperatively.

62
5.3 The influence of inotropic drugs in the GLUTAMICS-trial The aim of this study (Paper IV) was to investigate if preemptive use of inotropic drugs influenced the primary endpoint of the GLUTAMICS trial and if glutamate influenced outcome in patients receiving inotropes intra-operatively.
At an early stage of the GLUTAMICS-trial the clinical endpoints com-mittee identified that preemptive use of inotropic drugs in patients with anticipated circulatory problems often prohibited the diagnosis of heart failure on weaning from CPB even in patients that later developed severe circulatory failure.
The fact that the two major centers participating in the trial exhibited markedly different policies regarding preemptive use of inotropic drugs permitted us to assess its implications on the primary endpoint. The results of our post-hoc analysis agree with the clinical impression of the clinical endpoints committee.
A liberal policy for preemptive use of inotropic drugs to facilitate wean-ing from CPB was associated with more patients developing severe circula-tory failure than fulfilled criteria for LV-failure at weaning from CPB. A restrictive policy was associated with the opposite finding. Given that LV-failure at weaning from CPB constituted the major component of the com-posite primary endpoint we conclude that preemptive use of inotropic drugs had substantial implications on the primary endpoint of the GLU-TAMICS-trial.
The choice of primary endpoint was based on clinical experience with metabolic interventions employing restrictive use of inotropic drugs100, 113. However, participating centers and individual clinicians were free to insti-tute inotropic drugs according to their choice and usual practice. In retro-spect, the discrepancy in the use of inotropic drugs between center A and B is not unexpected given the lack of generally accepted guidelines for ino-tropic therapy3-5.
The secondary endpoint late circulatory failure was added to the proto-col as an amendment to identify these cases. In conjunction with the sec-ondary endpoint severe circulatory failure it allowed discrimination of mild short-lasting heart failure at weaning from CPB from clinically significant heart failure requiring substantial circulatory support and leading to pro-longed ICU stay or death.
The patients that received inotropic drugs intraoperatively were those in whom circulatory failure was anticipated or manifest. Patients at higher risk are obviously better suited to evaluate metabolic intervention assumed to enhance myocardial recovery (Figure 8). In patients that received ino-
63
tropic drugs intraoperatively, intravenous glutamate infusion was associ-ated with significantly fewer patients hemodynamically unstable at comple-tion of surgery or in need of IABP on admisson to ICU.
Postoperative NT-proBNP levels were also significantly lower in the glu-tamate group (Figure 6).
Figure 8. Proportion of patients hemodynamically unstable at completion of sur-gery despite inotropes or in need of IABP.
To conclude, a liberal policy regarding preemptive use of inotropic drugs to facilitate weaning from CPB had a significant influence on the primary endpoint of the GLUTAMICS-trial but did not lower the incidence of se-vere circulatory failure. Intravenous glutamate infusion was associated with a beneficial effect on hemodynamic outcome in patients receiving inotropic drugs intraoperatively.

64
5.4 Defining postoperative heart failure Although postoperative heart failure is a major cause for postoperative mortality there are no generally accepted criteria for this diagnosis, and the criteria used are inevitably debatable.
In the GLUTAMICS-trial we addressed this issue by using criteria based on variables documented with regard to outcome and we provided the blinded clinical endpoints committee with strict prespecified criteria to minimize bias from individual clinical judgement100, 113-115.
The clinical endpoints committee consisted of consultants in cardiotho-racic surgery and cardiothoracic anesthesiology from each of the partici-pating centers. The members of the committee were blinded to the treat-ment assignment and prespecified criteria reported in the Appendix were used to reach a consensus decision.
All cases with suspected postoperative heart failure based on SvO2 and other hemodynamic data, use of inotropic drugs or mechanical circulatory support, extended ICU stay, circulatory problems reported by anesthesi-ologists or surgeons in the clinical database were reviewed. Based on pre-specified criteria (Appendix) the committee decided whether circulatory problems had occurred, if these circulatory problems were severe and if they were cardiac in origin, if they were evident at weaning from CPB or presented later in the postoperative course. The committee also decided if events leading to death were cardiac in origin.
LV-failure at weaning from CPB constituted a major component of the composite primary endpoint in the GLUTAMICS-trial. The complexity of defining heart failure at weaning from CPB and postoperative heart failure in general emphasizes the need for robust endpoints and definitions in both clinical management and when evaluating novel circulatory treatment. To discriminate mild short-lasting heart failure at weaning from CPB from clinically significant heart failure requiring substantial circulatory support and leading to prolonged ICU stay or death we introduced the secondary endpoint severe circulatory failure as an amendment to the study protocol.
With increasing acknowledgement of NT-proBNP as a reliable marker of the severity of heart failure116-123, an amendment was filed to the Swedish MPA to add this marker to the study protocol. The results of NT-proBNP analyses were blinded to the clinical endpoints committee and, hence, per-mitted evaluation of the clinical endpoint committee decisions with an unbiased marker (Figure 9).
65
Figure 9. Clinical endpoints committee decisions regarding hemodynamic state compared to NT-proBNP levels.*Indicates statistically significant difference (p<0.05) compared to patients without PHF.
5.5 Biochemical mechanisms of glutamate Intravenous glutamate infusion according to the protocol in the GLUTA-MICS-trial could influence postoperative outcome by two different bio-chemical mechanisms. First, glutamate could improve myocardial tolerance to ischemia by facilitated anaerobic metabolism during ischemia55, 58, 81, 92,
109, 124. In the present study, no clinical evidence for this mechanism was detected by markers of myocardial injury or the incidence perioperative myocardial infarction.
The second mechanism by which glutamate could improve postoperative outcome after coronary surgery is related to the anaplerotic role of gluta-mate. Glutamate contributes to replenishment of Krebs cycle intermediates lost during ischemia, which enhances recovery of myocardial metabolism

64
5.4 Defining postoperative heart failure Although postoperative heart failure is a major cause for postoperative mortality there are no generally accepted criteria for this diagnosis, and the criteria used are inevitably debatable.
In the GLUTAMICS-trial we addressed this issue by using criteria based on variables documented with regard to outcome and we provided the blinded clinical endpoints committee with strict prespecified criteria to minimize bias from individual clinical judgement100, 113-115.
The clinical endpoints committee consisted of consultants in cardiotho-racic surgery and cardiothoracic anesthesiology from each of the partici-pating centers. The members of the committee were blinded to the treat-ment assignment and prespecified criteria reported in the Appendix were used to reach a consensus decision.
All cases with suspected postoperative heart failure based on SvO2 and other hemodynamic data, use of inotropic drugs or mechanical circulatory support, extended ICU stay, circulatory problems reported by anesthesi-ologists or surgeons in the clinical database were reviewed. Based on pre-specified criteria (Appendix) the committee decided whether circulatory problems had occurred, if these circulatory problems were severe and if they were cardiac in origin, if they were evident at weaning from CPB or presented later in the postoperative course. The committee also decided if events leading to death were cardiac in origin.
LV-failure at weaning from CPB constituted a major component of the composite primary endpoint in the GLUTAMICS-trial. The complexity of defining heart failure at weaning from CPB and postoperative heart failure in general emphasizes the need for robust endpoints and definitions in both clinical management and when evaluating novel circulatory treatment. To discriminate mild short-lasting heart failure at weaning from CPB from clinically significant heart failure requiring substantial circulatory support and leading to prolonged ICU stay or death we introduced the secondary endpoint severe circulatory failure as an amendment to the study protocol.
With increasing acknowledgement of NT-proBNP as a reliable marker of the severity of heart failure116-123, an amendment was filed to the Swedish MPA to add this marker to the study protocol. The results of NT-proBNP analyses were blinded to the clinical endpoints committee and, hence, per-mitted evaluation of the clinical endpoint committee decisions with an unbiased marker (Figure 9).
65
Figure 9. Clinical endpoints committee decisions regarding hemodynamic state compared to NT-proBNP levels.*Indicates statistically significant difference (p<0.05) compared to patients without PHF.
5.5 Biochemical mechanisms of glutamate Intravenous glutamate infusion according to the protocol in the GLUTA-MICS-trial could influence postoperative outcome by two different bio-chemical mechanisms. First, glutamate could improve myocardial tolerance to ischemia by facilitated anaerobic metabolism during ischemia55, 58, 81, 92,
109, 124. In the present study, no clinical evidence for this mechanism was detected by markers of myocardial injury or the incidence perioperative myocardial infarction.
The second mechanism by which glutamate could improve postoperative outcome after coronary surgery is related to the anaplerotic role of gluta-mate. Glutamate contributes to replenishment of Krebs cycle intermediates lost during ischemia, which enhances recovery of myocardial metabolism

66
and function55, 58, 81, 124-126. The results of this trial are compatible with en-hanced post-ischemic myocardial recovery.
Promoting recovery represents a different and more appealing concept than the use of inotropic drugs, which increase oxygen expenditure regard-less of the state of myocardial recovery. This may have contributed to the low cardiac mortality in the glutamate group and could explain the en-couraging clinical outcomes previously reported with metabolic interven-tions43, 82, 93, 100.
67
5.6 Adverse events There have been concerns regarding the safety of intravenous administra-tion of glutamate66. In the central nervous system glutamate acts as an excitatory neurotransmitter. Under certain conditions it may act as an exci-totoxin and participate in events leading to neurological damage. Gluta-mate administration has been shown to cause neurological injury in ro-dents but not in primates due to the blood-brain barrier that prevents pas-sage of exogenous glutamate to the brain62-64. Furthermore, the concentra-tion of glutamate in the brain is fifty-fold higher than in human plasma65.
The pathophysiological role of exogenously administered glutamate in patients undergoing cardiac surgery with CPB and potential blood brain barrier dysfunction remains to be clarified. Assessment of this issue is ob-scured by the fact that cardiac surgery per se is associated with a substan-tial risk of neurological injury127. Available data have not demonstrated any increase in clinically evident neurological injury when glutamate en-hanced cardioplegic solutions or intravenous infusions have been used in clinical practice127, 128.
In our clinical practice neurological complications have been monitored continuously. As an early safety measure in the GLUTAMICS trial a pre-specified subgroup of patients were analyzed with regard to postoperative S-100B levels to detect potential subclinical neurological injury related to intravenous glutamate infusion (Paper II).
The Swedish Medical Products Agency requested surveillance and un-blinding in cases of CT-verified stroke within 24 hours of surgery, mortal-ity and suspected unexpected serious adverse reactions (SUSAR). Before unblinding was done the case was reviewed by the Clinical endpoints committee if suspected circulatory problems had occurred.
The S-100B substudy of the GLUTAMICS-trial and the outcome data from the whole GLUTAMICS-trial show no differences in neurological outcome and there was no evidence of subclinical neurological injury asso-ciated with intravenous glutamate infusion.
Regarding other serious and non-serious adverse events no statistically significant differences were found between the glutamate group and con-trol group (Appendix).
To conclude we found that intravenous glutamate infusions in the dos-ages employed can be safely administered to patients undergoing cardiac surgery.

66
and function55, 58, 81, 124-126. The results of this trial are compatible with en-hanced post-ischemic myocardial recovery.
Promoting recovery represents a different and more appealing concept than the use of inotropic drugs, which increase oxygen expenditure regard-less of the state of myocardial recovery. This may have contributed to the low cardiac mortality in the glutamate group and could explain the en-couraging clinical outcomes previously reported with metabolic interven-tions43, 82, 93, 100.
67
5.6 Adverse events There have been concerns regarding the safety of intravenous administra-tion of glutamate66. In the central nervous system glutamate acts as an excitatory neurotransmitter. Under certain conditions it may act as an exci-totoxin and participate in events leading to neurological damage. Gluta-mate administration has been shown to cause neurological injury in ro-dents but not in primates due to the blood-brain barrier that prevents pas-sage of exogenous glutamate to the brain62-64. Furthermore, the concentra-tion of glutamate in the brain is fifty-fold higher than in human plasma65.
The pathophysiological role of exogenously administered glutamate in patients undergoing cardiac surgery with CPB and potential blood brain barrier dysfunction remains to be clarified. Assessment of this issue is ob-scured by the fact that cardiac surgery per se is associated with a substan-tial risk of neurological injury127. Available data have not demonstrated any increase in clinically evident neurological injury when glutamate en-hanced cardioplegic solutions or intravenous infusions have been used in clinical practice127, 128.
In our clinical practice neurological complications have been monitored continuously. As an early safety measure in the GLUTAMICS trial a pre-specified subgroup of patients were analyzed with regard to postoperative S-100B levels to detect potential subclinical neurological injury related to intravenous glutamate infusion (Paper II).
The Swedish Medical Products Agency requested surveillance and un-blinding in cases of CT-verified stroke within 24 hours of surgery, mortal-ity and suspected unexpected serious adverse reactions (SUSAR). Before unblinding was done the case was reviewed by the Clinical endpoints committee if suspected circulatory problems had occurred.
The S-100B substudy of the GLUTAMICS-trial and the outcome data from the whole GLUTAMICS-trial show no differences in neurological outcome and there was no evidence of subclinical neurological injury asso-ciated with intravenous glutamate infusion.
Regarding other serious and non-serious adverse events no statistically significant differences were found between the glutamate group and con-trol group (Appendix).
To conclude we found that intravenous glutamate infusions in the dos-ages employed can be safely administered to patients undergoing cardiac surgery.

68
5.7 Limitations This thesis consists of data from an observational study and from a ran-domized clinical trial. A major limitation regarding Paper I is of course that it, like most studies on patients with severe LV-dysfunction undergoing CABG, is retrospective and observational.
The major limitation of Paper IV is that although the same inclusion cri-teria were employed demographics of patients included at center A and center B differed. Demographics for patients randomized to glutamate infusion or placebo receiving inotropes intraoperatively were more compa-rable but the results have to be interpreted cautiously as they are based on a post-hoc analysis.
Regarding the GLUTAMICS-trial there are certain study limitations that deserve comment. The issues concerning patient selection and the defini-tion of postoperative heart failure have been discussed above.
The major findings in the GLUTAMICS-trial are related to secondary outcomes and subgroup analyses, which are somewhat provisional even when prespecified. However, the results should be regarded in the context of current evidence. Treatment for postoperative heart failure is based on expert opinion and the need for large studies to assess the optimal way to manage postoperative heart failure has been emphasized.
5.8 Clinical perspectives The importance of clinical trials is receiving increased attention in cardiac surgery but there is still a chasm to bridge before our practice is permeated by evidence-based medicine.
Without a generally accepted definition of myocardial infarction the rapid evolution in the cardiological management of myocardial infarction would never have occurred. To some extent the situation in cardiac surgery resembles the situation in cardiology fifty years ago when cardiologist GE Burch stated that it was interesting that nobody wanted to define myocar-dial infarction but that everybody talked about it and all seemed to know what they were talking about129. In cardiac surgery several of the most important complications such as postoperative renal failure, postoperative myocardial infarction and postoperative heart failure lack generally ac-cepted definitions 6, 7, 103, 104, 130 . A recent paper demonstrated that by choosing different definitions of renal failure the incidence, patient identifi-cation and risk-factors were influenced104. Before the issue of definitions is addressed evaluation of treatment of these conditions will be impeded and dissemination of progress may be delayed.
69
In 1979 E. Rau proposed that use of glutamate could provide an impor-tant step in efforts to protect cardiac tissue during stress induced at cardiac surgery or by ischemia55. Despite this and other animal experimental data suggesting a beneficial effect of glutamate in association with myocardial ischemia further exploration of clinical benefits in humans has been sparse. Lack of commercial interest and fears of potential neurological adverse effects could explain this.
Our long-standing clinical experience and a prospective randomized double-blind clinical trial in 861 patients suggest that intravenous gluta-mate infusion could provide a novel and clinically important way of pro-moting myocardial recovery after ischemic injury.
Further studies are warranted to confirm these results and to elucidate the role of metabolic intervention with glutamate for other high-risk groups in cardiac surgery. Eventually glutamate could find a role in the management of acute post-ischemic heart failure in cardiology practice.
Intravenous glutamate infusion in the dosages employed in our experi-ence provides a safe and inexpensive treatment. Paradoxically, the latter may be an issue due to the lack of commercial interest and obstruct clinical exploration in the future.

68
5.7 Limitations This thesis consists of data from an observational study and from a ran-domized clinical trial. A major limitation regarding Paper I is of course that it, like most studies on patients with severe LV-dysfunction undergoing CABG, is retrospective and observational.
The major limitation of Paper IV is that although the same inclusion cri-teria were employed demographics of patients included at center A and center B differed. Demographics for patients randomized to glutamate infusion or placebo receiving inotropes intraoperatively were more compa-rable but the results have to be interpreted cautiously as they are based on a post-hoc analysis.
Regarding the GLUTAMICS-trial there are certain study limitations that deserve comment. The issues concerning patient selection and the defini-tion of postoperative heart failure have been discussed above.
The major findings in the GLUTAMICS-trial are related to secondary outcomes and subgroup analyses, which are somewhat provisional even when prespecified. However, the results should be regarded in the context of current evidence. Treatment for postoperative heart failure is based on expert opinion and the need for large studies to assess the optimal way to manage postoperative heart failure has been emphasized.
5.8 Clinical perspectives The importance of clinical trials is receiving increased attention in cardiac surgery but there is still a chasm to bridge before our practice is permeated by evidence-based medicine.
Without a generally accepted definition of myocardial infarction the rapid evolution in the cardiological management of myocardial infarction would never have occurred. To some extent the situation in cardiac surgery resembles the situation in cardiology fifty years ago when cardiologist GE Burch stated that it was interesting that nobody wanted to define myocar-dial infarction but that everybody talked about it and all seemed to know what they were talking about129. In cardiac surgery several of the most important complications such as postoperative renal failure, postoperative myocardial infarction and postoperative heart failure lack generally ac-cepted definitions6, 7, 103, 104, 130, 131. A recent paper demonstrated that by choosing different definitions of renal failure the incidence, patient identifi-cation and risk-factors were influenced104. Before the issue of definitions is addressed evaluation of treatment of these conditions will be impeded and dissemination of progress may be delayed.
69
In 1979 E. Rau proposed that use of glutamate could provide an impor-tant step in efforts to protect cardiac tissue during stress induced at cardiac surgery or by ischemia55. Despite this and other animal experimental data suggesting a beneficial effect of glutamate in association with myocardial ischemia further exploration of clinical benefits in humans has been sparse. Lack of commercial interest and fears of potential neurological adverse effects could explain this.
Our long-standing clinical experience and a prospective randomized double-blind clinical trial in 861 patients suggest that intravenous gluta-mate infusion could provide a novel and clinically important way of pro-moting myocardial recovery after ischemic injury.
Further studies are warranted to confirm these results and to elucidate the role of metabolic intervention with glutamate for other high-risk groups in cardiac surgery. Eventually glutamate could find a role in the management of acute post-ischemic heart failure in cardiology practice.
Intravenous glutamate infusion in the dosages employed in our experi-ence provides a safe and inexpensive treatment. Paradoxically, the latter may be an issue due to the lack of commercial interest and obstruct clinical exploration in the future.

71
Summary
- A metabolic strategy to prevent and treat postoperative heart failure involving adherence to physiological principles to minimize myo-cardial and systemic oxygen expenditure, and metabolic interven-tions with glutamate and high-dose GIK to increase myocardial tol-erance to ischemia and facilitate myocardial recovery after ischemia was evolved during a five-year period
- The metabolic strategy allowed restrictive use of inotropes and was
associated with short-term and long-term survival that compares fa-vorably with the literature in patients with LV-dysfunction under-going CABG
- The metabolic strategy was associated with particularly encouraging
results regarding preservation of renal function
- The GLUTAMICS-trial was an investigator-initiated randomized clinical trial investigating if intravenous glutamate infusion given in association with surgery for acute coronary syndrome can reduce mortality and prevent or mitigate myocardial injury and postopera-tive heart failure
- The trial was conducted according to the principles of Good Clini-
cal Practice including professional external monitoring.
- The composite primary endpoint did not differ between the gluta-mate group and the control group
- The event rates in the GLUTAMICS-trial were substantially lower
than calculated reducing the power of the trial
- A liberal policy regarding preemptive use of inotropic drugs to faci-litate weaning from CPB influenced the primary endpoint of the GLUTAMICS-trial further reducing the power of the trial
- Patients with LV-failure on weaning from CPB had significantly
shorter ventilator treatment and ICU-stay if they received intrave-nous glutamate infusion

71
Summary
- A metabolic strategy to prevent and treat postoperative heart failure involving adherence to physiological principles to minimize myo-cardial and systemic oxygen expenditure, and metabolic interven-tions with glutamate and high-dose GIK to increase myocardial tol-erance to ischemia and facilitate myocardial recovery after ischemia was evolved during a five-year period
- The metabolic strategy allowed restrictive use of inotropes and was
associated with short-term and long-term survival that compares fa-vorably with the literature in patients with LV-dysfunction under-going CABG
- The metabolic strategy was associated with particularly encouraging
results regarding preservation of renal function
- The GLUTAMICS-trial was an investigator-initiated randomized clinical trial investigating if intravenous glutamate infusion given in association with surgery for acute coronary syndrome can reduce mortality and prevent or mitigate myocardial injury and postopera-tive heart failure
- The trial was conducted according to the principles of Good Clini-
cal Practice including professional external monitoring.
- The composite primary endpoint did not differ between the gluta-mate group and the control group
- The event rates in the GLUTAMICS-trial were substantially lower
than calculated reducing the power of the trial
- A liberal policy regarding preemptive use of inotropic drugs to faci-litate weaning from CPB influenced the primary endpoint of the GLUTAMICS-trial further reducing the power of the trial
- Patients with LV-failure on weaning from CPB had significantly
shorter ventilator treatment and ICU-stay if they received intrave-nous glutamate infusion

72
- In patients with unstable angina (CCS class IV) undergoing isolated CABG intravenous glutamate infusion was associated with signifi-cantly lower arterial lactate early after weaning from CPB
- In patients with unstable angina (CCS class IV) undergoing isolated
CABG intravenous glutamate infusion was associated with signifi-cantly lower incidence of severe circulatory failure
- In patients with unstable angina (CCS class IV) undergoing isolated
CABG multivariable analysis identified intravenous glutamate infu-sion as the only independent variable associated with a reduced in-cidence of severe circulatory failure
- In patients receiving inotropic drugs intraoperatively intravenous
glutamate infusion was associated with significantly fewer patients hemodynamically unstable or in need of IABP
- In patients receiving inotropic drugs intraoperatively intravenous
glutamate infusion was associated with significantly lower postop-erative NT-proBNP
- Intravenous glutamate infusion during surgery for acute coronary
syndrome did not initiate a sustained elevation of plasma S-100B postoperatively
- Intravenous glutamate infusion during surgery for acute coronary
syndrome was not associated with an increased incidence of neuro-logical injury or other adverse events
73
Conclusions
- The metabolic strategy was associated with encouraging clinical re-sults, unsurpassed in the literature, in patients with LV-dysfunction undergoing CABG
- Intravenous glutamate infusion did not improve the composite pri-
mary endpoint but was associated with secondary outcomes com-patible with a beneficial effect of on post-ischemic myocardial re-covery
- The putative effect on post-ischemic myocardial recovery was seen
in more ischemic patients (CCS class IV) and in patients with evi-dent or anticipated LV-failure on weaning from CPB
- Intravenous glutamate infusion in association with surgery for acute
coronary syndrome was safe in the dosages employed - Intravenous glutamate infusion could provide a novel and important
way of promoting myocardial recovery after ischemic injury

72
- In patients with unstable angina (CCS class IV) undergoing isolated CABG intravenous glutamate infusion was associated with signifi-cantly lower arterial lactate early after weaning from CPB
- In patients with unstable angina (CCS class IV) undergoing isolated
CABG intravenous glutamate infusion was associated with signifi-cantly lower incidence of severe circulatory failure
- In patients with unstable angina (CCS class IV) undergoing isolated
CABG multivariable analysis identified intravenous glutamate infu-sion as the only independent variable associated with a reduced in-cidence of severe circulatory failure
- In patients receiving inotropic drugs intraoperatively intravenous
glutamate infusion was associated with significantly fewer patients hemodynamically unstable or in need of IABP
- In patients receiving inotropic drugs intraoperatively intravenous
glutamate infusion was associated with significantly lower postop-erative NT-proBNP
- Intravenous glutamate infusion during surgery for acute coronary
syndrome did not initiate a sustained elevation of plasma S-100B postoperatively
- Intravenous glutamate infusion during surgery for acute coronary
syndrome was not associated with an increased incidence of neuro-logical injury or other adverse events
73
Conclusions
- The metabolic strategy was associated with encouraging clinical re-sults, unsurpassed in the literature, in patients with LV-dysfunction undergoing CABG
- Intravenous glutamate infusion did not improve the composite pri-
mary endpoint but was associated with secondary outcomes com-patible with a beneficial effect of on post-ischemic myocardial re-covery
- The putative effect on post-ischemic myocardial recovery was seen
in more ischemic patients (CCS class IV) and in patients with evi-dent or anticipated LV-failure on weaning from CPB
- Intravenous glutamate infusion in association with surgery for acute
coronary syndrome was safe in the dosages employed - Intravenous glutamate infusion could provide a novel and important
way of promoting myocardial recovery after ischemic injury

75
Acknowledgements The work in this thesis was carried out at the Departements of Cardiotho-racic Surgery and Anesthesiology at Örebro University Hospital, the Uni-versity Hospital of Linköping and at Blekinge County Hospital, Karlskrona.
Financial support was received from The Swedish Heart-Lung Foundation (20030595), Capio Research Foundation (2005-1021; 2006-1203), the Research Committee of the Örebro County Council, Örebro University and Östergötlands County Council.
I would like to express my gratitude to all who have helped and supported me to complete the studies that have resulted in this thesis. I especially want to thank: My principal supervisor, Professor Rolf Svedjeholm, for your endless sup-port and guidance in my scientific work. With your unsurpassed attention to detail you really inspire me to do my very best. During these years you have always taken your time for my questions and showed me tremendous patience. I am grateful for all you have taught me. My second supervisor, Örjan Friberg, for leading me over the first thresh-olds in scientific work. Your great support has helped me a lot, and your knowledge regarding the Carath database has been invaluable. My co-authors Erik Håkanson, Jonas Holm, Farkas Vanky, Lena Sunner-malm, Rajiv Sharma, Jan-Olov Borg and Sören Juhl-Andersen for your important contributions to this work. The study nurses Inger Huljebrant, Sara Thybell, Anna Krantz and Anki Olsson for all your work with patient records and the Clinical Report Forms. This work would not have been possible without your help. Eva Norgren-Holst and all the staff at Clinical Research Support, for your professional monitoring of the GLUTAMICS-trial. Olle Eriksson, statistical expert, for your professional help. Olof Lundblad and Mathias Sandin, heads of the Departement of Cardio-thoracic Surgery and Anesthesiology, Örebro University Hospital, for your

75
Acknowledgements The work in this thesis was carried out at the Departements of Cardiotho-racic Surgery and Anesthesiology at Örebro University Hospital, the Uni-versity Hospital of Linköping and at Blekinge County Hospital, Karlskrona.
Financial support was received from The Swedish Heart-Lung Foundation (20030595), Capio Research Foundation (2005-1021; 2006-1203), the Research Committee of the Örebro County Council, Örebro University and Östergötlands County Council.
I would like to express my gratitude to all who have helped and supported me to complete the studies that have resulted in this thesis. I especially want to thank: My principal supervisor, Professor Rolf Svedjeholm, for your endless sup-port and guidance in my scientific work. With your unsurpassed attention to detail you really inspire me to do my very best. During these years you have always taken your time for my questions and showed me tremendous patience. I am grateful for all you have taught me. My second supervisor, Örjan Friberg, for leading me over the first thresh-olds in scientific work. Your great support has helped me a lot, and your knowledge regarding the Carath database has been invaluable. My co-authors Erik Håkanson, Jonas Holm, Farkas Vanky, Lena Sunner-malm, Rajiv Sharma, Jan-Olov Borg and Sören Juhl-Andersen for your important contributions to this work. The study nurses Inger Huljebrant, Sara Thybell, Anna Krantz and Anki Olsson for all your work with patient records and the Clinical Report Forms. This work would not have been possible without your help. Eva Norgren-Holst and all the staff at Clinical Research Support, for your professional monitoring of the GLUTAMICS-trial. Olle Eriksson, statistical expert, for your professional help. Olof Lundblad and Mathias Sandin, heads of the Departement of Cardio-thoracic Surgery and Anesthesiology, Örebro University Hospital, for your

76
support and encouragement in both my clinical work and in my research work. I also want to thank Olle “Slim Fin” for struggling side by side with me between and across the islands of the Stockholm archipelago, respect! Anders Ahlsson, for your excellent mentorship during my training in car-diothoracic surgery and for your wonderful sense of humour. Oswaldo Fernandes and Stig-Olov Almgren, for your enthusiasm and pa-tience in teaching me thoracic surgery. All my colleagues and all the staff at the Departement of Cardiothoracic Surgery and Anesthesiology, Örebro University Hospital for your encour-agement and for being my friends. My sister-in-law Helena and family for your generous hospitality during my stays in Linköping. My sister Malin and Jonas for all your support and encouragement. Finally, I want to express my gratitude to my wife Åsa and our children Erik, Jacob and Elsa for all your fantastic efforts, for your love and sup-port and for being the wonderful persons you all are.
77
References
1. Kirklin JW, Rastelli GC. Low cardiac output after open intracar-diac operations. Prog Cardiovasc Dis 1967;10(2):117-22.
2. O'Connor GT, Birkmeyer JD, Dacey LJ, Quinton HB, Marrin CA, Birkmeyer NJ, et al. Results of a regional study of modes of death associated with coronary artery bypass grafting. Northern New England Cardiovascular Disease Study Group. Ann Thorac Surg 1998;66(4):1323-8.
3. Fellahi JL, Parienti JJ, Hanouz JL, Plaud B, Riou B, Ouattara A. Perioperative use of dobutamine in cardiac surgery and adverse cardiac outcome: propensity-adjusted analyses. Anesthesiology 2008;108(6):979-87.
4. Gillies M, Bellomo R, Doolan L, Buxton B. Bench-to-bedside re-view: Inotropic drug therapy after adult cardiac surgery - a syste-matic literature review. Crit Care 2005;9(3):266-79.
5. Mebazaa A, Pitsis AA, Rudiger A, Toller W, Longrois D, Ricksten SE, et al. Clinical review: practical recommendations on the man-agement of perioperative heart failure in cardiac surgery. Crit Care 2010;14(2):201. Epub 2010 Apr 28.
6. Vanky F, Hakanson E, Maros T, Svedjeholm R. Different charac-teristics of postoperative heart failure after surgery for aortic ste-nosis and coronary disease. Scand Cardiovasc J 2004;38(3):152-8.
7. Vanky FB, Hakanson E, Svedjeholm R. Long-term consequences of postoperative heart failure after surgery for aortic stenosis com-pared with coronary surgery. Ann Thorac Surg 2007;83(6):2036-43.
8. Khoynezhad A, Jalali Z, Tortolani AJ. Apoptosis: pathophysiology and therapeutic implications for the cardiac surgeon. Ann Thorac Surg 2004;78(3):1109-18.
9. Maroko PR, Kjekshus JK, Sobel BE, Watanabe T, Covell JW, Ross Jr J, et al. Factors influencing infarct size following experimental coronary artery occlusions. Circulation 1971;43:67-82.
10. Rosky LP, Rodman T. Medical aspects of open-heart surgery. N Engl J Med 1966;274(16):886-93.
11. Williams JF, Jr., Morrow AG, Braunwald E. The incidence and management of "medical" complications following cardiac opera-tions. Circulation 1965;32(4):608-19.
12. Morales AR, Fine G, Taber RE. Cardiac surgery and myocardial necrosis. Arch Pathol 1967;83(1):71-9.
13. Slogoff S, Keats AS. Does perioperative myocardial ischemia lead to postoperative myocardial infarction? Anesthesiology 1985;62:107-14.

76
support and encouragement in both my clinical work and in my research work. I also want to thank Olle “Slim Fin” for struggling side by side with me between and across the islands of the Stockholm archipelago, respect! Anders Ahlsson, for your excellent mentorship during my training in car-diothoracic surgery and for your wonderful sense of humour. Oswaldo Fernandes and Stig-Olov Almgren, for your enthusiasm and pa-tience in teaching me thoracic surgery. All my colleagues and all the staff at the Departement of Cardiothoracic Surgery and Anesthesiology, Örebro University Hospital for your encour-agement and for being my friends. My sister-in-law Helena and family for your generous hospitality during my stays in Linköping. My sister Malin and Jonas for all your support and encouragement. Finally, I want to express my gratitude to my wife Åsa and our children Erik, Jacob and Elsa for all your fantastic efforts, for your love and sup-port and for being the wonderful persons you all are.
77
References
1. Kirklin JW, Rastelli GC. Low cardiac output after open intracar-diac operations. Prog Cardiovasc Dis 1967;10(2):117-22.
2. O'Connor GT, Birkmeyer JD, Dacey LJ, Quinton HB, Marrin CA, Birkmeyer NJ, et al. Results of a regional study of modes of death associated with coronary artery bypass grafting. Northern New England Cardiovascular Disease Study Group. Ann Thorac Surg 1998;66(4):1323-8.
3. Fellahi JL, Parienti JJ, Hanouz JL, Plaud B, Riou B, Ouattara A. Perioperative use of dobutamine in cardiac surgery and adverse cardiac outcome: propensity-adjusted analyses. Anesthesiology 2008;108(6):979-87.
4. Gillies M, Bellomo R, Doolan L, Buxton B. Bench-to-bedside re-view: Inotropic drug therapy after adult cardiac surgery - a syste-matic literature review. Crit Care 2005;9(3):266-79.
5. Mebazaa A, Pitsis AA, Rudiger A, Toller W, Longrois D, Ricksten SE, et al. Clinical review: practical recommendations on the man-agement of perioperative heart failure in cardiac surgery. Crit Care 2010;14(2):201. Epub 2010 Apr 28.
6. Vanky F, Hakanson E, Maros T, Svedjeholm R. Different charac-teristics of postoperative heart failure after surgery for aortic ste-nosis and coronary disease. Scand Cardiovasc J 2004;38(3):152-8.
7. Vanky FB, Hakanson E, Svedjeholm R. Long-term consequences of postoperative heart failure after surgery for aortic stenosis com-pared with coronary surgery. Ann Thorac Surg 2007;83(6):2036-43.
8. Khoynezhad A, Jalali Z, Tortolani AJ. Apoptosis: pathophysiology and therapeutic implications for the cardiac surgeon. Ann Thorac Surg 2004;78(3):1109-18.
9. Maroko PR, Kjekshus JK, Sobel BE, Watanabe T, Covell JW, Ross Jr J, et al. Factors influencing infarct size following experimental coronary artery occlusions. Circulation 1971;43:67-82.
10. Rosky LP, Rodman T. Medical aspects of open-heart surgery. N Engl J Med 1966;274(16):886-93.
11. Williams JF, Jr., Morrow AG, Braunwald E. The incidence and management of "medical" complications following cardiac opera-tions. Circulation 1965;32(4):608-19.
12. Morales AR, Fine G, Taber RE. Cardiac surgery and myocardial necrosis. Arch Pathol 1967;83(1):71-9.
13. Slogoff S, Keats AS. Does perioperative myocardial ischemia lead to postoperative myocardial infarction? Anesthesiology 1985;62:107-14.

78
14. Dahlin LG, Olin C, Svedjeholm R. Perioperative myocardial in-farction in cardiac surgery--risk factors and consequences. A case control study. Scand Cardiovasc J 2000;34(5):522-7.
15. Bjessmo S, Ivert T. Troponin-T in patients with unstable and sta-ble angina pectoris undergoing coronary bypass surgery. Thorac Cardiovasc Surg 2000;48(3):140-4.
16. Bjessmo S, Ivert T, Flink H, Hammar N. Early and late mortality after surgery for unstable angina in relation to Braunwald class. Am Heart J 2001;141(1):9-14.
17. McKinlay KH, Schinderle DB, Swaminathan M, Podgoreanu MV, Milano CA, Messier RH, et al. Predictors of inotrope use during separation from cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2004;18(4):404-8.
18. Royster RL, Butterworth JFt, Prough DS, Johnston WE, Thomas JL, Hogan PE, et al. Preoperative and intraoperative predictors of inotropic support and long-term outcome in patients having coro-nary artery bypass grafting. Anesth Analg 1991;72(6):729-36.
19. Furnary AP, Wu Y. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland Diabetic Project. Endocr Pract 2006;12 Suppl 3:22-6.
20. Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and con-tinuous intravenous insulin infusions on outcomes of cardiac sur-gical procedures: the Portland Diabetic Project. Endocr Pract 2004;10 Suppl 2:21-33.
21. Furnary AP, Zerr KJ, Grunkemeier GL, Starr A. Continuous intra-venous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical proce-dures. Ann Thorac Surg 1999;67(2):352-60.
22. van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in the critically ill pa-tients. N Engl J Med 2001;345(19):1359-67.
23. Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V, Starr A. Glucose control lowers the risk of wound infection in di-abetics after open heart operations. Ann Thorac Surg 1997;63(2):356-61.
24. Rackley CE, Russell RO, Jr., Rogers WJ, Mantle JA, McDaniel HG, Papapietro SE. Clinical experience with glucose-insulin-potassium therapy in acute myocardial infarction. Am Heart J 1981;102(6 Pt 1):1038-49.
25. Rackley CE, Russell RO, Jr., Rogers WJ, Mantle JA, McDaniel HG, Papapietro SE. Glucose-insulin-potassium administration in acute myocardial infarction. Annu Rev Med 1982;33:375-83.
26. Svedjeholm R, Hallhagen S, Ekroth R, Joachimsson PO, Ronquist G. Dopamine and high-dose insulin infusion (glucose-insulin-
79
potassium) after a cardiac operation: effects on myocardial meta-bolism. Ann Thorac Surg 1991;51(2):262-70.
27. Svensson S, Svedjeholm R, Ekroth R, Milocco I, Nilsson F, Sabel KG, et al. Trauma metabolism and the heart. Uptake of substrates and effects of insulin early after cardiac operations. J Thorac Car-diovasc Surg 1990;99(6):1063-73.
28. Szabo Z, Arnqvist H, Hakanson E, Jorfeldt L, Svedjeholm R. Ef-fects of high-dose glucose-insulin-potassium on myocardial meta-bolism after coronary surgery in patients with Type II diabetes. Clin Sci (Lond) 2001;101(1):37-43.
29. Holger JS, Engebretsen KM, Fritzlar SJ, Patten LC, Harris CR, Flottemesch TJ. Insulin versus vasopressin and epinephrine to treat beta-blocker toxicity. Clin Toxicol (Phila) 2007;45(4):396-401.
30. Lucchesi BR, Medina M, Kniffen FJ. The positive inotropic action of insulin in the canine heart. Eur J Pharmacol 1972;18(1):107-15.
31. Hsu CH, Wei J, Chen YC, Yang SP, Tsai CS, Lin CI. Cellular me-chanisms responsible for the inotropic action of insulin on failing human myocardium. J Heart Lung Transplant 2006;25(9):1126-34.
32. Steinberg HO, Brechtel G, Johnson A, Fineberg N, Baron AD. Insulin-mediated skeletal muscle vasodilation is nitric oxide de-pendent. A novel action of insulin to increase nitric oxide release. J Clin Invest 1994;94(3):1172-9.
33. Sundell J, Nuutila P, Laine H, Luotolahti M, Kalliokoski K, Raita-kari O, et al. Dose-dependent vasodilating effects of insulin on adenosine-stimulated myocardial blood flow. Diabetes 2002;51(4):1125-30.
34. Ueda S, Petrie JR, Cleland SJ, Elliott HL, Connell JM. The vasodi-lating effect of insulin is dependent on local glucose uptake: a double blind, placebo-controlled study. J Clin Endocrinol Metab 1998;83(6):2126-31.
35. Ueda S, Petrie JR, Cleland SJ, Elliott HL, Connell JM. Insulin va-sodilatation and the "arginine paradox". Lancet 1998;351(9107):959-60.
36. Gradinac S, Coleman GM, Taegtmeyer H, Sweeney MS, Frazier OH. Improved cardiac function with glucose-insulin-potassium af-ter aortocoronary bypass grafting. Ann Thorac Surg 1989;48(4):484-9.
37. Girard C, Quentin P, Bouvier H, Blanc P, Bastien O, Lehot JJ, et al. Glucose and insulin supply before cardiopulmonary bypass in cardiac surgery: a double-blind study. Ann Thorac Surg 1992;54(2):259-63.
38. Hiesmayr M, Haider WJ, Grubhofer G, Heilinger D, Keznickl FP, Mares P, et al. Effects of dobutamine versus insulin on cardiac per-formance, myocardial oxygen demand, and total body metabolism

78
14. Dahlin LG, Olin C, Svedjeholm R. Perioperative myocardial in-farction in cardiac surgery--risk factors and consequences. A case control study. Scand Cardiovasc J 2000;34(5):522-7.
15. Bjessmo S, Ivert T. Troponin-T in patients with unstable and sta-ble angina pectoris undergoing coronary bypass surgery. Thorac Cardiovasc Surg 2000;48(3):140-4.
16. Bjessmo S, Ivert T, Flink H, Hammar N. Early and late mortality after surgery for unstable angina in relation to Braunwald class. Am Heart J 2001;141(1):9-14.
17. McKinlay KH, Schinderle DB, Swaminathan M, Podgoreanu MV, Milano CA, Messier RH, et al. Predictors of inotrope use during separation from cardiopulmonary bypass. J Cardiothorac Vasc Anesth 2004;18(4):404-8.
18. Royster RL, Butterworth JFt, Prough DS, Johnston WE, Thomas JL, Hogan PE, et al. Preoperative and intraoperative predictors of inotropic support and long-term outcome in patients having coro-nary artery bypass grafting. Anesth Analg 1991;72(6):729-36.
19. Furnary AP, Wu Y. Clinical effects of hyperglycemia in the cardiac surgery population: the Portland Diabetic Project. Endocr Pract 2006;12 Suppl 3:22-6.
20. Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and con-tinuous intravenous insulin infusions on outcomes of cardiac sur-gical procedures: the Portland Diabetic Project. Endocr Pract 2004;10 Suppl 2:21-33.
21. Furnary AP, Zerr KJ, Grunkemeier GL, Starr A. Continuous intra-venous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical proce-dures. Ann Thorac Surg 1999;67(2):352-60.
22. van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, et al. Intensive insulin therapy in the critically ill pa-tients. N Engl J Med 2001;345(19):1359-67.
23. Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V, Starr A. Glucose control lowers the risk of wound infection in di-abetics after open heart operations. Ann Thorac Surg 1997;63(2):356-61.
24. Rackley CE, Russell RO, Jr., Rogers WJ, Mantle JA, McDaniel HG, Papapietro SE. Clinical experience with glucose-insulin-potassium therapy in acute myocardial infarction. Am Heart J 1981;102(6 Pt 1):1038-49.
25. Rackley CE, Russell RO, Jr., Rogers WJ, Mantle JA, McDaniel HG, Papapietro SE. Glucose-insulin-potassium administration in acute myocardial infarction. Annu Rev Med 1982;33:375-83.
26. Svedjeholm R, Hallhagen S, Ekroth R, Joachimsson PO, Ronquist G. Dopamine and high-dose insulin infusion (glucose-insulin-
79
potassium) after a cardiac operation: effects on myocardial meta-bolism. Ann Thorac Surg 1991;51(2):262-70.
27. Svensson S, Svedjeholm R, Ekroth R, Milocco I, Nilsson F, Sabel KG, et al. Trauma metabolism and the heart. Uptake of substrates and effects of insulin early after cardiac operations. J Thorac Car-diovasc Surg 1990;99(6):1063-73.
28. Szabo Z, Arnqvist H, Hakanson E, Jorfeldt L, Svedjeholm R. Ef-fects of high-dose glucose-insulin-potassium on myocardial meta-bolism after coronary surgery in patients with Type II diabetes. Clin Sci (Lond) 2001;101(1):37-43.
29. Holger JS, Engebretsen KM, Fritzlar SJ, Patten LC, Harris CR, Flottemesch TJ. Insulin versus vasopressin and epinephrine to treat beta-blocker toxicity. Clin Toxicol (Phila) 2007;45(4):396-401.
30. Lucchesi BR, Medina M, Kniffen FJ. The positive inotropic action of insulin in the canine heart. Eur J Pharmacol 1972;18(1):107-15.
31. Hsu CH, Wei J, Chen YC, Yang SP, Tsai CS, Lin CI. Cellular me-chanisms responsible for the inotropic action of insulin on failing human myocardium. J Heart Lung Transplant 2006;25(9):1126-34.
32. Steinberg HO, Brechtel G, Johnson A, Fineberg N, Baron AD. Insulin-mediated skeletal muscle vasodilation is nitric oxide de-pendent. A novel action of insulin to increase nitric oxide release. J Clin Invest 1994;94(3):1172-9.
33. Sundell J, Nuutila P, Laine H, Luotolahti M, Kalliokoski K, Raita-kari O, et al. Dose-dependent vasodilating effects of insulin on adenosine-stimulated myocardial blood flow. Diabetes 2002;51(4):1125-30.
34. Ueda S, Petrie JR, Cleland SJ, Elliott HL, Connell JM. The vasodi-lating effect of insulin is dependent on local glucose uptake: a double blind, placebo-controlled study. J Clin Endocrinol Metab 1998;83(6):2126-31.
35. Ueda S, Petrie JR, Cleland SJ, Elliott HL, Connell JM. Insulin va-sodilatation and the "arginine paradox". Lancet 1998;351(9107):959-60.
36. Gradinac S, Coleman GM, Taegtmeyer H, Sweeney MS, Frazier OH. Improved cardiac function with glucose-insulin-potassium af-ter aortocoronary bypass grafting. Ann Thorac Surg 1989;48(4):484-9.
37. Girard C, Quentin P, Bouvier H, Blanc P, Bastien O, Lehot JJ, et al. Glucose and insulin supply before cardiopulmonary bypass in cardiac surgery: a double-blind study. Ann Thorac Surg 1992;54(2):259-63.
38. Hiesmayr M, Haider WJ, Grubhofer G, Heilinger D, Keznickl FP, Mares P, et al. Effects of dobutamine versus insulin on cardiac per-formance, myocardial oxygen demand, and total body metabolism

80
after coronary artery bypass grafting. J Cardiothorac Vasc Anesth 1995;9(6):653-8.
39. Lazar HL, Chipkin S, Philippides G, Bao Y, Apstein C. Glucose-insulin-potassium solutions improve outcomes in diabetics who have coronary artery operations. Ann Thorac Surg 2000;70(1):145-50.
40. Lazar HL, Philippides G, Fitzgerald C, Lancaster D, Shemin RJ, Apstein, et al. Glucose-insulin-potassium solutions enhance recov-ery after urgent coronary artery bypass grafting. J Thorac Cardio-vasc Surg 1997;113(2):354-60.
41. Lindholm L, Nilsson B, Kirno K, Sellgren J, Nilsson F, Jeppsson A. Is skeletal muscle luxury perfusion the main hemodynamic effect of high-dose insulin in cardiac surgery? Scand Cardiovasc J 2000;34(4):396-402.
42. Ranasinghe AM, McCabe CJ, Quinn DW, James SR, Pagano D, Franklyn JA, et al. How does glucose insulin potassium improve hemodynamic performance? Evidence for altered expression of be-ta-adrenoreceptor and calcium handling genes. Circulation 2006;114(1 Suppl):I239-44.
43. Svedjeholm R, Ekroth R, Joachimsson PO, Tyden H. High-dose insulin improves the efficacy of dopamine early after cardiac sur-gery. A study of myocardial performance and oxygen consump-tion. Scand J Thorac Cardiovasc Surg 1991;25(3):215-21.
44. Svensson S, Ekroth R, Milocco I, Nilsson F, Pont‚n J, William-Olsson G. Glucose and lactate balances in heart and leg after co-ronary surgery: influence of insulin infusion. Scand J Thorac Car-diovasc Surg 1989;23:145-50.
45. Brodin LA, Dahlgren G, Ekestrom S, Settergren G, Ohqvist G. Influence of glucose-insulin-potassium on left ventricular function during coronary artery bypass grafting. Scand J Thorac Cardiovasc Surg 1993;27(1):27-34.
46. Lindholm L, Bengtsson A, Hansdottir V, Westerlind A, Jeppsson A. Insulin (GIK) improves central mixed and hepatic venous oxy-genation in clinical cardiac surgery. Scand Cardiovasc J 2001;35(5):347-52.
47. Quinn DW, Pagano D, Bonser RS, Rooney SJ, Graham TR, Wil-son IC, et al. Improved myocardial protection during coronary ar-tery surgery with glucose-insulin-potassium: a randomized con-trolled trial. J Thorac Cardiovasc Surg 2006;131(1):34-42.
48. Coleman GM, Gradinac S, Taegtmeyer H, Sweeney M, Frazier OH. Efficacy of metabolic support with glucose-insulin-potassium for left ventricular pump failure after aortocoronary bypass sur-gery. Circulation 1989;80(3 Pt 1):I91-6.
49. Koskenkari JK, Kaukoranta PK, Kiviluoma KT, Raatikainen MJ, Ohtonen PP, Ala-Kokko TI. Metabolic and hemodynamic effects
81
of high-dose insulin treatment in aortic valve and coronary sur-gery. Ann Thorac Surg 2005;80(2):511-7.
50. Svedjeholm R, Ekroth R, Joachimsson PO, Ronquist G, Svensson SE, Tyd‚n H. Myocardial uptake of amino acids and other sub-strates in relation to myocardial oxygen consumption four hours after cardiac surgery. J Thorac Cardiovasc Surg 1991;101:688-94.
51. Svensson S, Ekroth R, Nilsson F, Pont‚n J, William-Olsson G. Insulin as a vasodilating agent in the first hour after cardiopulmo-nary bypass. Scand J Thorac Cardiovasc Surg 1989;23:139-43.
52. Jeppsson A, Ekroth R, Kirno K, Milocco I, Nilsson B, Nilsson F, et al. Insulin and amino acid infusion after cardiac operations: effects on systemic and renal perfusion. J Thorac Cardiovasc Surg 1997;113(3):594-602.
53. Klein LJ, van Campen LC, Sieswerda GT, Kamp O, Visser CA, Visser FC. Glucose-insulin-potassium echocardiography detects improved segmental myocardial function and viable tissue shortly after acute myocardial infarction. J Am Soc Echocardiogr 2006;19(6):763-71.
54. Marano L, Bestetti A, Lomuscio A, Tagliabue L, Castini D, Tarri-cone D, et al. Effects of infusion of glucose-insulin-potassium on myocardial function after a recent myocardial infarction. Acta Cardiol 2000;55(1):9-15.
55. Rau EE, Shine KI, Gervais A, Douglas AM, Amos EC. Enhanced mechanical recovery of anoxic and ischemic myocardium by amino acid perfusion. Am J Physiol 1979;236:H873-H9.
56. Safer B. The metabolic significance of the malate-aspartate cycle in heart. Circ Res 1975;37:527-33.
57. Safer B, Williamson JR. Mitochondrial-cytosolic interactions in perfused rat heart. Role of coupled transamination in repletion of citric acid cycle intermediates. J Biol Chem 1973;248:2570-9.
58. Pisarenko OI. Mechanisms of myocardial protection by amino acids: facts and hypotheses. Clin Exp Pharm Physiol 1996;23(8):627-33.
59. Thomassen AR. Myocardial uptake and effects of glutamate dur-ing non-ischaemic and ischaemic conditions. A clinical study with special reference to possible interrelationships between glutamate and myocardial utilization of carbohydrate substrates. Dan Med Bull 1992;39:471-88.
60. McEntee WJ, Crook TH. Glutamate: its role in learning, memory, and the aging brain. Psychopharmacology (Berl) 1993;111(4):391-401.
61. Danbolt NC. Glutamate uptake. Prog Neurobiol 2001;65(1):1-105.
62. Daabees TT, Finkelstein MW, Stegink LD, Applebaum AE. Corre-lation of glutamate plus aspartate dose, plasma amino acid con-

80
after coronary artery bypass grafting. J Cardiothorac Vasc Anesth 1995;9(6):653-8.
39. Lazar HL, Chipkin S, Philippides G, Bao Y, Apstein C. Glucose-insulin-potassium solutions improve outcomes in diabetics who have coronary artery operations. Ann Thorac Surg 2000;70(1):145-50.
40. Lazar HL, Philippides G, Fitzgerald C, Lancaster D, Shemin RJ, Apstein, et al. Glucose-insulin-potassium solutions enhance recov-ery after urgent coronary artery bypass grafting. J Thorac Cardio-vasc Surg 1997;113(2):354-60.
41. Lindholm L, Nilsson B, Kirno K, Sellgren J, Nilsson F, Jeppsson A. Is skeletal muscle luxury perfusion the main hemodynamic effect of high-dose insulin in cardiac surgery? Scand Cardiovasc J 2000;34(4):396-402.
42. Ranasinghe AM, McCabe CJ, Quinn DW, James SR, Pagano D, Franklyn JA, et al. How does glucose insulin potassium improve hemodynamic performance? Evidence for altered expression of be-ta-adrenoreceptor and calcium handling genes. Circulation 2006;114(1 Suppl):I239-44.
43. Svedjeholm R, Ekroth R, Joachimsson PO, Tyden H. High-dose insulin improves the efficacy of dopamine early after cardiac sur-gery. A study of myocardial performance and oxygen consump-tion. Scand J Thorac Cardiovasc Surg 1991;25(3):215-21.
44. Svensson S, Ekroth R, Milocco I, Nilsson F, Pont‚n J, William-Olsson G. Glucose and lactate balances in heart and leg after co-ronary surgery: influence of insulin infusion. Scand J Thorac Car-diovasc Surg 1989;23:145-50.
45. Brodin LA, Dahlgren G, Ekestrom S, Settergren G, Ohqvist G. Influence of glucose-insulin-potassium on left ventricular function during coronary artery bypass grafting. Scand J Thorac Cardiovasc Surg 1993;27(1):27-34.
46. Lindholm L, Bengtsson A, Hansdottir V, Westerlind A, Jeppsson A. Insulin (GIK) improves central mixed and hepatic venous oxy-genation in clinical cardiac surgery. Scand Cardiovasc J 2001;35(5):347-52.
47. Quinn DW, Pagano D, Bonser RS, Rooney SJ, Graham TR, Wil-son IC, et al. Improved myocardial protection during coronary ar-tery surgery with glucose-insulin-potassium: a randomized con-trolled trial. J Thorac Cardiovasc Surg 2006;131(1):34-42.
48. Coleman GM, Gradinac S, Taegtmeyer H, Sweeney M, Frazier OH. Efficacy of metabolic support with glucose-insulin-potassium for left ventricular pump failure after aortocoronary bypass sur-gery. Circulation 1989;80(3 Pt 1):I91-6.
49. Koskenkari JK, Kaukoranta PK, Kiviluoma KT, Raatikainen MJ, Ohtonen PP, Ala-Kokko TI. Metabolic and hemodynamic effects
81
of high-dose insulin treatment in aortic valve and coronary sur-gery. Ann Thorac Surg 2005;80(2):511-7.
50. Svedjeholm R, Ekroth R, Joachimsson PO, Ronquist G, Svensson SE, Tyd‚n H. Myocardial uptake of amino acids and other sub-strates in relation to myocardial oxygen consumption four hours after cardiac surgery. J Thorac Cardiovasc Surg 1991;101:688-94.
51. Svensson S, Ekroth R, Nilsson F, Pont‚n J, William-Olsson G. Insulin as a vasodilating agent in the first hour after cardiopulmo-nary bypass. Scand J Thorac Cardiovasc Surg 1989;23:139-43.
52. Jeppsson A, Ekroth R, Kirno K, Milocco I, Nilsson B, Nilsson F, et al. Insulin and amino acid infusion after cardiac operations: effects on systemic and renal perfusion. J Thorac Cardiovasc Surg 1997;113(3):594-602.
53. Klein LJ, van Campen LC, Sieswerda GT, Kamp O, Visser CA, Visser FC. Glucose-insulin-potassium echocardiography detects improved segmental myocardial function and viable tissue shortly after acute myocardial infarction. J Am Soc Echocardiogr 2006;19(6):763-71.
54. Marano L, Bestetti A, Lomuscio A, Tagliabue L, Castini D, Tarri-cone D, et al. Effects of infusion of glucose-insulin-potassium on myocardial function after a recent myocardial infarction. Acta Cardiol 2000;55(1):9-15.
55. Rau EE, Shine KI, Gervais A, Douglas AM, Amos EC. Enhanced mechanical recovery of anoxic and ischemic myocardium by amino acid perfusion. Am J Physiol 1979;236:H873-H9.
56. Safer B. The metabolic significance of the malate-aspartate cycle in heart. Circ Res 1975;37:527-33.
57. Safer B, Williamson JR. Mitochondrial-cytosolic interactions in perfused rat heart. Role of coupled transamination in repletion of citric acid cycle intermediates. J Biol Chem 1973;248:2570-9.
58. Pisarenko OI. Mechanisms of myocardial protection by amino acids: facts and hypotheses. Clin Exp Pharm Physiol 1996;23(8):627-33.
59. Thomassen AR. Myocardial uptake and effects of glutamate dur-ing non-ischaemic and ischaemic conditions. A clinical study with special reference to possible interrelationships between glutamate and myocardial utilization of carbohydrate substrates. Dan Med Bull 1992;39:471-88.
60. McEntee WJ, Crook TH. Glutamate: its role in learning, memory, and the aging brain. Psychopharmacology (Berl) 1993;111(4):391-401.
61. Danbolt NC. Glutamate uptake. Prog Neurobiol 2001;65(1):1-105.
62. Daabees TT, Finkelstein MW, Stegink LD, Applebaum AE. Corre-lation of glutamate plus aspartate dose, plasma amino acid con-

82
centration and neuronal necrosis in infant mice. Food Chem Tox-icol 1985;23:887-93.
63. Fernstrom JD. Pituitary hormone secretion in normal male hu-mans: acute responses to a large, oral dose of monosodium gluta-mate. J Nutr 2000;130(4S Suppl):1053S-7S.
64. Sacks W, Sacks S, Brebbia DR, Fleischer A. Cerebral uptake of amino acids in human subjects and rhesus monkeys in vivo. J Neu-rosci Res 1982;7:431-6.
65. Waelsch H. Glutamic acid and cerebral function. Adv Protein Chem 1951;6:299-341.
66. Greenamyre JT, Porter RH. Anatomy and physiology of glutamate in the CNS. Neurology 1994;44(11 Suppl 8):S7-13.
67. Munro HN. Factors in the regulation of glutamate metabolism in glutamic acid. Raven Press 1979:55-68.
68. Peters JH, Lin SC, Betridge BJ, Cummings JG, Chao WR. Amino acids, including aspargine and glutamine in plasma and urine of normal human subjects. Proc Soc Expt Biol Med 1969;131:281-8.
69. Stegink LD, Filer LJ, Baker GL. Plasma amino acid concentrations in normal adults fed meals with added monosodium L-glutamate and aspartame. J Nutr 1983;113:1851-60.
70. Ikeda K. On the taste of the salt of glutamic acid. Chem Soc 1909;30:820-36.
71. Ikeda K. Method of producing a seasoning material whose main component is the salt of glutamic acid. Japanese Pat 1908;14:805.
72. Sano C. History of glutamate production. Am J Clin Nutr 2009;90(3):728S-32S.
73. Prawirohardjono W, Dwiprahasto I, Astuti I, Hadiwandowo S, Kristin E, Muhammad M, et al. The administration to Indonesians of monosodium L-glutamate in Indonesian foods: an assessment of adverse reactions in a randomized double-blind, crossover, place-bo-controlled study. J Nutr 2000;130(4S Suppl):1074S-6S.
74. Tarasoff L, Kelly MF. Monosodium L-glutamate: a double-blind study and review. Food Chem Toxicol 1993;31(12):1019-35.
75. Wilkin JK. Does monosodium glutamate cause flushing (or merely "glutamania")? J Am Acad Dermatol 1986;15(2 Pt 1):225-30.
76. Engelman RM, Dobbs WA, Rousou JH, Meeran MK. Myocardial high-energy phosphate replenishment during ischemic arrest: aero-bic versus anaerobic metabolism. Ann Thorac Surg 1982;33:453-8.
77. Engelman RM, Rousou JA, Flack JE, Iyengar J, Kimura Y, Das DK. Reduction of infarct size by systemic amino acid supplementa-tion during reperfusion. J Thorac Cardiovasc Surg 1991;101:855-9.
78. Lazar HL, Buckberg GD, Manganaro AJ, Becker H. Myocardial energy replenishment and reversal of ischemic damage by substrate
83
enhancement of secondary blood cardioplegia with amino acids during reperfusion. J Thorac Cardiovasc Surg 1980;80:350-9.
79. Weldner PW, Myers JL, Miller CA, Arenas JD, Waldhausen JA. Improved recovery of immature myocardium with L-glutamate blood cardioplegia. Ann Thorac Surg 1993;55:102-5.
80. Pisarenko OI, Novikova EB, Serebryakova LI, Tskitishvili OV, Ivanov VE, Studneva IM. Function and metabolism of dog heart in ischemia and in subsequent reperfusion: effect of exogenous glu-tamic acid. Pflugers Arch 1985;405:377-83.
81. Lazar HL, Buckberg GD, Manganaro AJ, Becker H, Maloney JV, Jr. Reversal of ischemic damage with amino acid substrate en-hancement during reperfusion. Surgery 1980;80:702-9.
82. Pisarenko OI, Solomatina ES, Studneva IM, Ivanov VE, Kapelko VI, Smirnov VN. Protective effect of glutamic acid on cardiac func-tion and metabolism during cardioplegia and reperfusion. Basic Res Cardiol 1983;78:534-43.
83. Haas GS, DeBoer LWV, O'Keefe DD, Bodenhamer RM, Geffin GA, Drop LJ, et al. Reduction of postischemic myocardial dys-function by substrate repletion during reperfusion. Circulation 1984;70(suppl I):65-74.
84. Pisarenko OI, Rosenfeldt FL, Langley L, Conyers RA, Richards SM. Differing protection with aspartate and glutamate cardiople-gia in the isolated rat heart. Ann Thorac Surg 1995;59:1541-8.
85. Pisarenko OI, Novikova EB, Serebriakova LI, Tskitishvili OV, Ivanov VE. Correction of contractile function and metabolism in canine ischemic myocardium due to exogenous glutamic acid. Biull Eksp Biol Med 1985;100:280-2.
86. Mudge GH, Mills RM, Taegtmeyer H, Gorlin R, Lesch M. Altera-tions of myocardial amino acid metabolism in chronic ischemic heart disease. J Clin Invest 1976;58:1185-92.
87. Pisarenko OI, Oleynikov OD, Shulzhenko VS, Studneva IM, Ryff IM, Kapelko VI. Association of myocardial glutamate and aspar-tate pool and functional recovery of postischemic heart. Biochem Med Metab Biol 1989;42:105-17.
88. Thomassen A, Nielsen TT, Bagger JP. Alterations in myocardial uptake of glutamate and release of alanine after propranolol, nife-dipine, and glyceryl trinitrate in coronary artery disease. J Cardio-vasc Pharmacol 1985;7:394-400.
89. Thomassen A, Nielsen TT, Bagger JP, Thuesen L. Myocardial glutamate and alanine exchanges related to carbohydrate metabol-ism in patients with normal and stenotic coronary arteries. Clin Physiol 1984;4:425-34.
90. Thomassen AR, Mortensen PT, Nielsen TT, Falstie-Jensen N, Thygesen K, Henningsen P. Altered plasma concentrations of glu-

82
centration and neuronal necrosis in infant mice. Food Chem Tox-icol 1985;23:887-93.
63. Fernstrom JD. Pituitary hormone secretion in normal male hu-mans: acute responses to a large, oral dose of monosodium gluta-mate. J Nutr 2000;130(4S Suppl):1053S-7S.
64. Sacks W, Sacks S, Brebbia DR, Fleischer A. Cerebral uptake of amino acids in human subjects and rhesus monkeys in vivo. J Neu-rosci Res 1982;7:431-6.
65. Waelsch H. Glutamic acid and cerebral function. Adv Protein Chem 1951;6:299-341.
66. Greenamyre JT, Porter RH. Anatomy and physiology of glutamate in the CNS. Neurology 1994;44(11 Suppl 8):S7-13.
67. Munro HN. Factors in the regulation of glutamate metabolism in glutamic acid. Raven Press 1979:55-68.
68. Peters JH, Lin SC, Betridge BJ, Cummings JG, Chao WR. Amino acids, including aspargine and glutamine in plasma and urine of normal human subjects. Proc Soc Expt Biol Med 1969;131:281-8.
69. Stegink LD, Filer LJ, Baker GL. Plasma amino acid concentrations in normal adults fed meals with added monosodium L-glutamate and aspartame. J Nutr 1983;113:1851-60.
70. Ikeda K. On the taste of the salt of glutamic acid. Chem Soc 1909;30:820-36.
71. Ikeda K. Method of producing a seasoning material whose main component is the salt of glutamic acid. Japanese Pat 1908;14:805.
72. Sano C. History of glutamate production. Am J Clin Nutr 2009;90(3):728S-32S.
73. Prawirohardjono W, Dwiprahasto I, Astuti I, Hadiwandowo S, Kristin E, Muhammad M, et al. The administration to Indonesians of monosodium L-glutamate in Indonesian foods: an assessment of adverse reactions in a randomized double-blind, crossover, place-bo-controlled study. J Nutr 2000;130(4S Suppl):1074S-6S.
74. Tarasoff L, Kelly MF. Monosodium L-glutamate: a double-blind study and review. Food Chem Toxicol 1993;31(12):1019-35.
75. Wilkin JK. Does monosodium glutamate cause flushing (or merely "glutamania")? J Am Acad Dermatol 1986;15(2 Pt 1):225-30.
76. Engelman RM, Dobbs WA, Rousou JH, Meeran MK. Myocardial high-energy phosphate replenishment during ischemic arrest: aero-bic versus anaerobic metabolism. Ann Thorac Surg 1982;33:453-8.
77. Engelman RM, Rousou JA, Flack JE, Iyengar J, Kimura Y, Das DK. Reduction of infarct size by systemic amino acid supplementa-tion during reperfusion. J Thorac Cardiovasc Surg 1991;101:855-9.
78. Lazar HL, Buckberg GD, Manganaro AJ, Becker H. Myocardial energy replenishment and reversal of ischemic damage by substrate
83
enhancement of secondary blood cardioplegia with amino acids during reperfusion. J Thorac Cardiovasc Surg 1980;80:350-9.
79. Weldner PW, Myers JL, Miller CA, Arenas JD, Waldhausen JA. Improved recovery of immature myocardium with L-glutamate blood cardioplegia. Ann Thorac Surg 1993;55:102-5.
80. Pisarenko OI, Novikova EB, Serebryakova LI, Tskitishvili OV, Ivanov VE, Studneva IM. Function and metabolism of dog heart in ischemia and in subsequent reperfusion: effect of exogenous glu-tamic acid. Pflugers Arch 1985;405:377-83.
81. Lazar HL, Buckberg GD, Manganaro AJ, Becker H, Maloney JV, Jr. Reversal of ischemic damage with amino acid substrate en-hancement during reperfusion. Surgery 1980;80:702-9.
82. Pisarenko OI, Solomatina ES, Studneva IM, Ivanov VE, Kapelko VI, Smirnov VN. Protective effect of glutamic acid on cardiac func-tion and metabolism during cardioplegia and reperfusion. Basic Res Cardiol 1983;78:534-43.
83. Haas GS, DeBoer LWV, O'Keefe DD, Bodenhamer RM, Geffin GA, Drop LJ, et al. Reduction of postischemic myocardial dys-function by substrate repletion during reperfusion. Circulation 1984;70(suppl I):65-74.
84. Pisarenko OI, Rosenfeldt FL, Langley L, Conyers RA, Richards SM. Differing protection with aspartate and glutamate cardiople-gia in the isolated rat heart. Ann Thorac Surg 1995;59:1541-8.
85. Pisarenko OI, Novikova EB, Serebriakova LI, Tskitishvili OV, Ivanov VE. Correction of contractile function and metabolism in canine ischemic myocardium due to exogenous glutamic acid. Biull Eksp Biol Med 1985;100:280-2.
86. Mudge GH, Mills RM, Taegtmeyer H, Gorlin R, Lesch M. Altera-tions of myocardial amino acid metabolism in chronic ischemic heart disease. J Clin Invest 1976;58:1185-92.
87. Pisarenko OI, Oleynikov OD, Shulzhenko VS, Studneva IM, Ryff IM, Kapelko VI. Association of myocardial glutamate and aspar-tate pool and functional recovery of postischemic heart. Biochem Med Metab Biol 1989;42:105-17.
88. Thomassen A, Nielsen TT, Bagger JP. Alterations in myocardial uptake of glutamate and release of alanine after propranolol, nife-dipine, and glyceryl trinitrate in coronary artery disease. J Cardio-vasc Pharmacol 1985;7:394-400.
89. Thomassen A, Nielsen TT, Bagger JP, Thuesen L. Myocardial glutamate and alanine exchanges related to carbohydrate metabol-ism in patients with normal and stenotic coronary arteries. Clin Physiol 1984;4:425-34.
90. Thomassen AR, Mortensen PT, Nielsen TT, Falstie-Jensen N, Thygesen K, Henningsen P. Altered plasma concentrations of glu-

84
tamate, alanine and citrate in the early phase of acute myocardial infarction in man. Eur Heart J 1986;7:773-8.
91. Thomassen AR, Nielsen TT, Bagger JP, Henningsen P. Myocardial exchanges of glutamate, alanine, and citrate in controls and pa-tients with coronary artery disease. Clin Sci 1983;64:33-40.
92. Thomassen A, Nielsen TT, Bagger JP, Pedersen AK, Henningsen P. Antiischemic and metabolic effects of glutamate during pacing in patients with stable angina pectoris secondary to either coronary artery disease or syndrome X. Am J Cardiol 1991;68:291-5.
93. Pisarenko OI, Lepilin MG, Ivanov VE. Cardiac metabolism and performance during L-glutamic acid infusion in postoperative car-diac failure. Clin Sci 1986;70:7-12.
94. Svedjeholm R, Vanhanen I, Hakanson E, Joachimsson PO, Jorfeldt L, Nilsson L. Metabolic and hemodynamic effects of intravenous glutamate infusion early after coronary operations. J Thorac Car-diovasc Surg 1996;112(6):1468-77.
95. Langenberg CJ, Pietersen HG, Geskes G, Wagenmakers AJ, Lange SD, Schouten HJ, et al. The effect of glutamate infusion on cardiac performance is independent of changes in metabolism in patients undergoing routine coronary artery bypass surgery. Clin Sci (Lond) 2001;101(6):573-80.
96. Pietersen HG, Langenberg CJ, Geskes G, Kester A, de Lange S, Van der Vusse GJ, et al. Myocardial substrate uptake and oxida-tion during and after routine cardiac surgery. J Thorac Cardiovasc Surg 1999;118(1):71-80.
97. Pietersen HG, Langenberg CJ, Geskes G, Soeters PB, Wagenmak-ers AJ. Glutamate metabolism of the heart during coronary artery bypass grafting. Clin Nutr 1998;17(2):73-5.
98. Pisarenko OI, Portnoy VF, Studneva IM, Arapov AD, Korostylev AN. Glutamate-blood cardioplegia improves ATP preservation in human myocardium. Biomed Biochim Acta 1987;46:499-504.
99. Svedjeholm R, Huljebrant I, Hakanson E, Vanhanen I. Glutamate and high-dose glucose-insulin-potassium (GIK) in the treatment of severe cardiac failure after cardiac operations. Ann Thorac Surg 1995;59(2 Suppl):S23-30.
100. Svedjeholm R, Vidlund M, Vanhanen I, Hakanson E. A metabolic protective strategy could improve long-term survival in patients with LV-dysfunction undergoing CABG. Scand Cardiovasc J 2010;44(1):45-58.
101. Kimose HH, Ravkilde J, Helligs” P, Knudsen MA, Thomassen AR, Nielsen TT, et al. Myocardial loss of glutamate after cold chemical cardioplegia and storage in isolated blood-perfused pig hearts. Thorac Cardiovasc Surg 1993;41:93-100.
102. Vanhanen I, Svedjeholm R, Hakanson E, Joachimsson PO, Jorfeldt L, Nilsson L, et al. Assessment of myocardial glutamate require-
85
ments early after coronary artery bypass surgery. Scand Cardio-vasc J 1998;32(3):145-52.
103. Svedjeholm R, Dahlin LG, Lundberg C, Szabo Z, Kagedal B, Ny-lander E, et al. Are electrocardiographic Q-wave criteria reliable for diagnosis of perioperative myocardial infarction after coronary surgery? Eur J Cardiothorac Surg 1998;13(6):655-61.
104. Noyez L. Influence of the definition of acute renal failure post-cardiac surgery on incidence, patient identification, and identifica-tion of risk factors. Eur J Cardiothorac Surg;39(3):e8-12.
105. Lazar HL, Buckberg GD, Foglia RP, Manganaro AJ, Maloney JV, Jr. Detrimental effects of premature use of inotropic drugs to dis-continue cardiopulmonary bypass. J Thorac Cardiovasc Surg 1981;82(1):18-25.
106. Andersson LG, Ekroth R, Bratteby LE, Hallhagen S, Wesslén. Acute renal failure after coronary surgery - a study of incidence and risk factors in 2009 consecutive patients. Thorac Cardiovasc Surg. 1993;41:237-41.
107. Kehlet H. Multimodal approach to control postoperative patho-physiology and rehabilitation. Brit J Anaesth 1997;78(5):606-17.
108. Bolli R, Becker L, Gross G, Mentzer R, Jr., Balshaw D, Lathrop DA. Myocardial protection at a crossroads: the need for transla-tion into clinical therapy. Circ Res 2004;95(2):125-34.
109. Thomassen A, B”tker HE, Nielsen TT, Thygesen K, Henningsen P. Effects of glutamate on exercise tolerance and circulating substrate levels in stable angina pectoris. Am J Cardiol 1990;65:173-8.
110. Vanhanen I, Hakanson E, Jorfeldt L, Svedjeholm R. Myocardial uptake and release of substrates in patients operated for unstable angina: impact of glutamate infusion. Scand Cardiovasc J 2003;37(2):113-20.
111. Szabo Z, Hakanson E, Maros T, Svedjeholm R. High-dose glu-cose-insulin-potassium after cardiac surgery: a retrospective analy-sis of clinical safety issues. Acta Anaesthesiol Scand 2003;47(4):383-90.
112. Lazar HL, McDonnell M, Chipkin SR, Furnary AP, Engelman RM, Sadhu AR, et al. The Society of Thoracic Surgeons practice guideline series: Blood glucose management during adult cardiac surgery. Ann Thorac Surg 2009;87(2):663-9.
113. Svedjeholm R, Hakanson E, Szabo Z. Routine SvO2 measurement after CABG surgery with a surgically introduced pulmonary artery catheter. Eur J Cardiothorac Surg 1999;16(4):450-7.
114. Holm J, Hakanson E, Vanky F, Svedjeholm R. Mixed venous oxy-gen saturation predicts short- and long-term outcome after coro-nary artery bypass grafting surgery: a retrospective cohort analysis. Br J Anaesth 2011;Epub ahead of print 2011 June 16.
84
tamate, alanine and citrate in the early phase of acute myocardial infarction in man. Eur Heart J 1986;7:773-8.
91. Thomassen AR, Nielsen TT, Bagger JP, Henningsen P. Myocardial exchanges of glutamate, alanine, and citrate in controls and pa-tients with coronary artery disease. Clin Sci 1983;64:33-40.
92. Thomassen A, Nielsen TT, Bagger JP, Pedersen AK, Henningsen P. Antiischemic and metabolic effects of glutamate during pacing in patients with stable angina pectoris secondary to either coronary artery disease or syndrome X. Am J Cardiol 1991;68:291-5.
93. Pisarenko OI, Lepilin MG, Ivanov VE. Cardiac metabolism and performance during L-glutamic acid infusion in postoperative car-diac failure. Clin Sci 1986;70:7-12.
94. Svedjeholm R, Vanhanen I, Hakanson E, Joachimsson PO, Jorfeldt L, Nilsson L. Metabolic and hemodynamic effects of intravenous glutamate infusion early after coronary operations. J Thorac Car-diovasc Surg 1996;112(6):1468-77.
95. Langenberg CJ, Pietersen HG, Geskes G, Wagenmakers AJ, Lange SD, Schouten HJ, et al. The effect of glutamate infusion on cardiac performance is independent of changes in metabolism in patients undergoing routine coronary artery bypass surgery. Clin Sci (Lond) 2001;101(6):573-80.
96. Pietersen HG, Langenberg CJ, Geskes G, Kester A, de Lange S, Van der Vusse GJ, et al. Myocardial substrate uptake and oxida-tion during and after routine cardiac surgery. J Thorac Cardiovasc Surg 1999;118(1):71-80.
97. Pietersen HG, Langenberg CJ, Geskes G, Soeters PB, Wagenmak-ers AJ. Glutamate metabolism of the heart during coronary artery bypass grafting. Clin Nutr 1998;17(2):73-5.
98. Pisarenko OI, Portnoy VF, Studneva IM, Arapov AD, Korostylev AN. Glutamate-blood cardioplegia improves ATP preservation in human myocardium. Biomed Biochim Acta 1987;46:499-504.
99. Svedjeholm R, Huljebrant I, Hakanson E, Vanhanen I. Glutamate and high-dose glucose-insulin-potassium (GIK) in the treatment of severe cardiac failure after cardiac operations. Ann Thorac Surg 1995;59(2 Suppl):S23-30.
100. Svedjeholm R, Vidlund M, Vanhanen I, Hakanson E. A metabolic protective strategy could improve long-term survival in patients with LV-dysfunction undergoing CABG. Scand Cardiovasc J 2010;44(1):45-58.
101. Kimose HH, Ravkilde J, Helligs” P, Knudsen MA, Thomassen AR, Nielsen TT, et al. Myocardial loss of glutamate after cold chemical cardioplegia and storage in isolated blood-perfused pig hearts. Thorac Cardiovasc Surg 1993;41:93-100.
102. Vanhanen I, Svedjeholm R, Hakanson E, Joachimsson PO, Jorfeldt L, Nilsson L, et al. Assessment of myocardial glutamate require-
85
ments early after coronary artery bypass surgery. Scand Cardio-vasc J 1998;32(3):145-52.
103. Svedjeholm R, Dahlin LG, Lundberg C, Szabo Z, Kagedal B, Ny-lander E, et al. Are electrocardiographic Q-wave criteria reliable for diagnosis of perioperative myocardial infarction after coronary surgery? Eur J Cardiothorac Surg 1998;13(6):655-61.
104. Noyez L. Influence of the definition of acute renal failure post-cardiac surgery on incidence, patient identification, and identifica-tion of risk factors. Eur J Cardiothorac Surg;39(3):e8-12.
105. Lazar HL, Buckberg GD, Foglia RP, Manganaro AJ, Maloney JV, Jr. Detrimental effects of premature use of inotropic drugs to dis-continue cardiopulmonary bypass. J Thorac Cardiovasc Surg 1981;82(1):18-25.
106. Andersson LG, Ekroth R, Bratteby LE, Hallhagen S, Wesslén. Acute renal failure after coronary surgery - a study of incidence and risk factors in 2009 consecutive patients. Thorac Cardiovasc Surg. 1993;41:237-41.
107. Kehlet H. Multimodal approach to control postoperative patho-physiology and rehabilitation. Brit J Anaesth 1997;78(5):606-17.
108. Bolli R, Becker L, Gross G, Mentzer R, Jr., Balshaw D, Lathrop DA. Myocardial protection at a crossroads: the need for transla-tion into clinical therapy. Circ Res 2004;95(2):125-34.
109. Thomassen A, B”tker HE, Nielsen TT, Thygesen K, Henningsen P. Effects of glutamate on exercise tolerance and circulating substrate levels in stable angina pectoris. Am J Cardiol 1990;65:173-8.
110. Vanhanen I, Hakanson E, Jorfeldt L, Svedjeholm R. Myocardial uptake and release of substrates in patients operated for unstable angina: impact of glutamate infusion. Scand Cardiovasc J 2003;37(2):113-20.
111. Szabo Z, Hakanson E, Maros T, Svedjeholm R. High-dose glu-cose-insulin-potassium after cardiac surgery: a retrospective analy-sis of clinical safety issues. Acta Anaesthesiol Scand 2003;47(4):383-90.
112. Lazar HL, McDonnell M, Chipkin SR, Furnary AP, Engelman RM, Sadhu AR, et al. The Society of Thoracic Surgeons practice guideline series: Blood glucose management during adult cardiac surgery. Ann Thorac Surg 2009;87(2):663-9.
113. Svedjeholm R, Hakanson E, Szabo Z. Routine SvO2 measurement after CABG surgery with a surgically introduced pulmonary artery catheter. Eur J Cardiothorac Surg 1999;16(4):450-7.
114. Holm J, Hakanson E, Vanky F, Svedjeholm R. Mixed venous oxy-gen saturation predicts short- and long-term outcome after coro-nary artery bypass grafting surgery: a retrospective cohort analysis. Br J Anaesth 2011;Epub ahead of print 2011 June 16.

86
115. Holm J, Hakanson RE, Vanky F, Svedjeholm R. Mixed venous oxygen saturation is a prognostic marker after surgery for aortic stenosis. Acta Anaesthesiol Scand 2010;54(5):589-95.
116. Alehagen U, Dahlstrom U. Can NT-proBNP predict risk of cardi-ovascular mortality within 10 years? Results from an epidemiolog-ical study of elderly patients with symptoms of heart failure. Int J Cardiol 2009;133(2):233-40. Epub 2008 Apr 14.
117. Alehagen U, Lindstedt G, Levin LA, Dahlstrom U. Risk of cardi-ovascular death in elderly patients with possible heart failure. B-type natriuretic peptide (BNP) and the aminoterminal fragment of ProBNP (N-terminal proBNP) as prognostic indicators in a 6-year follow-up of a primary care population. Int J Cardiol 2005;100(1):125-33.
118. Doust JA, Pietrzak E, Dobson A, Glasziou P. How well does B-type natriuretic peptide predict death and cardiac events in pa-tients with heart failure: systematic review. BMJ 2005;330(7492):625.
119. Eliasdottir SB, Klemenzson G, Torfason B, Valsson F. Brain natri-uretic peptide is a good predictor for outcome in cardiac surgery. Acta Anaesthesiol Scand 2008;52(2):182-7. Epub 2007 Oct 19.
120. Fox AA, Shernan SK, Collard CD, Liu KY, Aranki SF, DeSantis SM, et al. Preoperative B-type natriuretic peptide is as independent predictor of ventricular dysfunction and mortality after primary coronary artery bypass grafting. J Thorac Cardiovasc Surg 2008;136(2):452-61.
121. Hutfless R, Kazanegra R, Madani M, Bhalla MA, Tulua-Tata A, Chen A, et al. Utility of B-type natriuretic peptide in predicting postoperative complications and outcomes in patients undergoing heart surgery. J Am Coll Cardiol 2004;43(10):1873-9.
122. Nozohoor S, Nilsson J, Algotsson L, Sjogren J. Postoperative in-crease in B-type natriuretic peptide levels predicts adverse outcome after cardiac surgery. J Cardiothorac Vasc Anesth 2011;25(3):469-75. Epub 2010 Sep 9.
123. Nozohoor S, Nilsson J, Luhrs C, Roijer A, Algotsson L, Sjogren J. B-type natriuretic peptide as a predictor of postoperative heart failure after aortic valve replacement. J Cardiothorac Vasc Anesth 2009;23(2):161-5. Epub 2009 Jan 23.
124. Svedjeholm R, Hakanson E, Vanhanen I. Rationale for metabolic support with amino acids and glucose-insulin-potassium (GIK) in cardiac surgery. Ann Thorac Surg 1995;59(2 Suppl):S15-22.
125. Safer B. The metabolic significance of the malate-aspartate cycle in heart. Circulation Research 1975;37:527-33.
126. Peuhkurinen KJ. Regulation of the tricarboxylic acid pool size in heart muscle. J Mol Cell Cardiol 1984;16(6):487-95.
87
127. Svedjeholm R, Hakanson E, Szabo Z, Vanky F. Neurological in-jury after surgery for ischemic heart disease: risk factors, outcome and role of metabolic interventions. Eur J Cardiothorac Surg 2001;19(5):611-8.
128. Loop FD, Higgins TL, Panda R, Pearce G, Estafanous FG. Myo-cardial protection during cardiac operations. Decreased morbidity and lower cost with blood cardioplegia and coronary sinus perfu-sion. J Thorac Cardiovasc Surg 1992;104(3):608-18.
129. http://onlinelibrary.wiley.com/doi/10.1111/j.0954-6820.1964.tb18851.x/abstract. Points of Enquiry, Diagnostic Cri-teria and Material. Acta Med Scand 1964;175:8-13.
130. Dahlin LG, Kagedal B, Nylander E, Olin C, Rutberg H, Svedje-holm R. Unspecific elevation of plasma troponin-T and CK-MB af-ter coronary surgery. Scand Cardiovasc J 2003;37(5):283-7.
131. Noyez L. Influence of the definition of acute renal failure post-cardiac surgery on incidence, patient identification, and identifica-tion of risk factors. Eur 2011;39(3):e8-12. Epub 2010 Dec 16.

86
115. Holm J, Hakanson RE, Vanky F, Svedjeholm R. Mixed venous oxygen saturation is a prognostic marker after surgery for aortic stenosis. Acta Anaesthesiol Scand 2010;54(5):589-95.
116. Alehagen U, Dahlstrom U. Can NT-proBNP predict risk of cardi-ovascular mortality within 10 years? Results from an epidemiolog-ical study of elderly patients with symptoms of heart failure. Int J Cardiol 2009;133(2):233-40. Epub 2008 Apr 14.
117. Alehagen U, Lindstedt G, Levin LA, Dahlstrom U. Risk of cardi-ovascular death in elderly patients with possible heart failure. B-type natriuretic peptide (BNP) and the aminoterminal fragment of ProBNP (N-terminal proBNP) as prognostic indicators in a 6-year follow-up of a primary care population. Int J Cardiol 2005;100(1):125-33.
118. Doust JA, Pietrzak E, Dobson A, Glasziou P. How well does B-type natriuretic peptide predict death and cardiac events in pa-tients with heart failure: systematic review. BMJ 2005;330(7492):625.
119. Eliasdottir SB, Klemenzson G, Torfason B, Valsson F. Brain natri-uretic peptide is a good predictor for outcome in cardiac surgery. Acta Anaesthesiol Scand 2008;52(2):182-7. Epub 2007 Oct 19.
120. Fox AA, Shernan SK, Collard CD, Liu KY, Aranki SF, DeSantis SM, et al. Preoperative B-type natriuretic peptide is as independent predictor of ventricular dysfunction and mortality after primary coronary artery bypass grafting. J Thorac Cardiovasc Surg 2008;136(2):452-61.
121. Hutfless R, Kazanegra R, Madani M, Bhalla MA, Tulua-Tata A, Chen A, et al. Utility of B-type natriuretic peptide in predicting postoperative complications and outcomes in patients undergoing heart surgery. J Am Coll Cardiol 2004;43(10):1873-9.
122. Nozohoor S, Nilsson J, Algotsson L, Sjogren J. Postoperative in-crease in B-type natriuretic peptide levels predicts adverse outcome after cardiac surgery. J Cardiothorac Vasc Anesth 2011;25(3):469-75. Epub 2010 Sep 9.
123. Nozohoor S, Nilsson J, Luhrs C, Roijer A, Algotsson L, Sjogren J. B-type natriuretic peptide as a predictor of postoperative heart failure after aortic valve replacement. J Cardiothorac Vasc Anesth 2009;23(2):161-5. Epub 2009 Jan 23.
124. Svedjeholm R, Hakanson E, Vanhanen I. Rationale for metabolic support with amino acids and glucose-insulin-potassium (GIK) in cardiac surgery. Ann Thorac Surg 1995;59(2 Suppl):S15-22.
125. Safer B. The metabolic significance of the malate-aspartate cycle in heart. Circulation Research 1975;37:527-33.
126. Peuhkurinen KJ. Regulation of the tricarboxylic acid pool size in heart muscle. J Mol Cell Cardiol 1984;16(6):487-95.
87
127. Svedjeholm R, Hakanson E, Szabo Z, Vanky F. Neurological in-jury after surgery for ischemic heart disease: risk factors, outcome and role of metabolic interventions. Eur J Cardiothorac Surg 2001;19(5):611-8.
128. Loop FD, Higgins TL, Panda R, Pearce G, Estafanous FG. Myo-cardial protection during cardiac operations. Decreased morbidity and lower cost with blood cardioplegia and coronary sinus perfu-sion. J Thorac Cardiovasc Surg 1992;104(3):608-18.
129. http://onlinelibrary.wiley.com/doi/10.1111/j.0954-6820.1964.tb18851.x/abstract. Points of Enquiry, Diagnostic Cri-teria and Material. Acta Med Scand 1964;175:8-13.
130. Dahlin LG, Kagedal B, Nylander E, Olin C, Rutberg H, Svedje-holm R. Unspecific elevation of plasma troponin-T and CK-MB af-ter coronary surgery. Scand Cardiovasc J 2003;37(5):283-7.

PAPER I
Table 8
Patients operated for acute coronary syndrome during the study period but not included in the Glutamics trial (n=780*)
30-day mortality**
4.0%
Inotropes in OR > 30 minutes
34.2%
65.4% 29.7%
Hemodynamic state at completion of surgery -Stable without inotropes -Stable with inotropes -Unstable with inotropes / IABP
4.3%
CK-MB µg/L day 1 post op
15 (10-27)
Troponin-T µg/L day 3-4 post op
0.4 (0.1-1.4)
peak p- Creatinine µmol/L
121 ± 86
Dialysis post op
2.2%
Length of ICU stay (hours)
22 (18 -37)
Time on ventilator (hours)
5.3 (3.5-8.8)
Postoperative atrial fibrillation
32.8%
Reoperation due to bleeding/tamponade
5.8%
Reoperation sternal infection/dehiscense
1.7%
Stroke during hospital stay
2.3%
Table 8. Outcome data for patients operated for acute coronary syndrome during the study
period but not included in the Glutamics trial (median + interquartile range, mean ± SD or
count n (%) ). OR = operating room. IABP = intra-aortic balloon pump. ICU = intensive care
unit. * complete data available from two of the participating centers (n=780) ** data from all
three participating centers (n=1222)
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)
Publications in the series
Örebro Studies in Medicine
1. Bergemalm, Per-Olof (2004). Audiologic and cognitive long-term sequelae from closed head injury.
2. Jansson, Kjell (2004). Intraperitoneal Microdialysis. Technique and Results.
3. Windahl, Torgny (2004). Clinical aspects of laser treatment of lichen sclerosus and squamous cell carcinoma of the penis.
4. Carlsson, Per-Inge (2004). Hearing impairment and deafness. Genetic and environmental factors – interactions – consequences. A clinical audiological approach.
5. Wågsäter, Dick (2005). CXCL16 and CD137 in Atherosclerosis.
6. Jatta, Ken (2006). Inflammation in Atherosclerosis.
7. Dreifaldt, Ann Charlotte (2006). Epidemiological Aspects on Malignant Diseases in Childhood.
8. Jurstrand, Margaretha (2006). Detection of Chlamydia trachomatis and Mycoplasma genitalium by genetic and serological methods.
9. Norén, Torbjörn (2006). Clostridium difficile, epidemiology and antibiotic resistance.
10. Anderzén Carlsson, Agneta (2007). Children with Cancer – Focusing on their Fear and on how their Fear is Handled.
11. Ocaya, Pauline (2007). Retinoid metabolism and signalling in vascular smooth muscle cells.
12. Nilsson, Andreas (2008). Physical activity assessed by accelerometry in children.
13. Eliasson, Henrik (2008). Tularemia – epidemiological, clinical and diagnostic aspects.
14. Walldén, Jakob (2008). The influence of opioids on gastric function: experimental and clinical studies.
15. Andrén, Ove (2008). Natural history and prognostic factors in localized prostate cancer.
16. Svantesson, Mia (2008). Postpone death? Nurse-physician perspectives and ethics rounds.
17. Björk, Tabita (2008). Measuring Eating Disorder Outcome – Definitions, dropouts and patients’ perspectives.
18. Ahlsson, Anders (2008). Atrial Fibrillation in Cardiac Surgery.
19. Parihar, Vishal Singh (2008). Human Listeriosis – Sources and Routes.
20. Berglund, Carolina (2008). Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus. Epidemiological aspects of MRSA and the dissemination in the community and in hospitals.
21. Nilsagård, Ylva (2008). Walking ability, balance and accidental falls in persons with Multiple Sclerosis.
22. Johansson, Ann-Christin (2008). Psychosocial factors in patients with lumbar disc herniation: Enhancing postoperative outcome by the identification of predictive factors and optimised physiotherapy.
23. Larsson, Matz (2008). Secondary exposure to inhaled tobacco products.
24. Hahn-Strömberg, Victoria (2008). Cell adhesion proteins in different invasive patterns of colon carcinoma: A morphometric and molecular genetic study.
25. Böttiger, Anna (2008). Genetic Variation in the Folate Receptor-α and Methylenetetrahydrofolate Reductase Genes as Determinants of Plasma Homocysteine Concentrations.
26. Andersson, Gunnel (2009). Urinary incontinence. Prevalence, treatment seeking behaviour, experiences and perceptions among persons with and without urinary leakage.
27. Elfström, Peter (2009). Associated disorders in celiac disease.
28. Skårberg, Kurt (2009). Anabolic-androgenic steroid users in treatment: Social background, drug use patterns and criminality.
29. de Man Lapidoth, Joakim (2009). Binge Eating and Obesity Treatment – Prevalence, Measurement and Long-term Outcome.
30. Vumma, Ravi (2009). Functional Characterization of Tyrosine and Tryptophan Transport in Fibroblasts from Healthy Controls, Patients with Schizophrenia and Bipolar Disorder.
31. Jacobsson, Susanne (2009). Characterisation of Neisseria meningitidis from a virulence and immunogenic perspective that includes variations in novel vaccine antigens.
32. Allvin, Renée (2009). Postoperative Recovery. Development of a Multi-Dimensional Questionnaire for Assessment of Recovery.
33. Hagnelius, Nils-Olof (2009). Vascular Mechanisms in Dementia with Special Reference to Folate and Fibrinolysis.
34. Duberg, Ann-Sofi (2009). Hepatitis C virus infection. A nationwide study of assiciated morbidity and mortality.
35. Söderqvist, Fredrik (2009). Health symptoms and potential effects on the blood-brain and blood-cerebrospinal fluid barriers associated with use of wireless telephones.
36. Neander, Kerstin (2009). Indispensable Interaction. Parents’ perspectives on parent–child interaction interventions and beneficial meetings.
37. Ekwall, Eva (2009). Women’s Experiences of Gynecological Cancer and Interaction with the Health Care System through Different Phases of the Disease.
38. Thulin Hedberg, Sara (2009). Antibiotic susceptibility and resistance in Neisseria meningitidis – phenotypic and genotypic characteristics.
39. Hammer, Ann (2010). Forced use on arm function after stroke. Clinically rated and self-reported outcome and measurement during the sub-acute phase.
40. Westman, Anders (2010). Musculoskeletal pain in primary health care: A biopsychosocial perspective for assessment and treatment.
41. Gustafsson, Sanna Aila (2010). The importance of being thin – Perceived expectations from self and others and the effect on self-evaluation in girls with disordered eating.
42. Johansson, Bengt (2010). Long-term outcome research on PDR brachytherapy with focus on breast, base of tongue and lip cancer.
43. Tina, Elisabet (2010). Biological markers in breast cancer and acute leukaemia with focus on drug resistance.
44. Overmeer, Thomas (2010). Implementing psychosocial factors in physical therapy treatment for patients with musculoskeletal pain in primary care.
45. Prenkert, Malin (2010). On mechanisms of drug resistance in acute myloid leukemia.
46. de Leon, Alex (2010). Effects of Anesthesia on Esophageal Sphincters in Obese Patients.

17. Björk, Tabita (2008). Measuring Eating Disorder Outcome – Definitions, dropouts and patients’ perspectives.
18. Ahlsson, Anders (2008). Atrial Fibrillation in Cardiac Surgery.
19. Parihar, Vishal Singh (2008). Human Listeriosis – Sources and Routes.
20. Berglund, Carolina (2008). Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus. Epidemiological aspects of MRSA and the dissemination in the community and in hospitals.
21. Nilsagård, Ylva (2008). Walking ability, balance and accidental falls in persons with Multiple Sclerosis.
22. Johansson, Ann-Christin (2008). Psychosocial factors in patients with lumbar disc herniation: Enhancing postoperative outcome by the identification of predictive factors and optimised physiotherapy.
23. Larsson, Matz (2008). Secondary exposure to inhaled tobacco products.
24. Hahn-Strömberg, Victoria (2008). Cell adhesion proteins in different invasive patterns of colon carcinoma: A morphometric and molecular genetic study.
25. Böttiger, Anna (2008). Genetic Variation in the Folate Receptor-α and Methylenetetrahydrofolate Reductase Genes as Determinants of Plasma Homocysteine Concentrations.
26. Andersson, Gunnel (2009). Urinary incontinence. Prevalence, treatment seeking behaviour, experiences and perceptions among persons with and without urinary leakage.
27. Elfström, Peter (2009). Associated disorders in celiac disease.
28. Skårberg, Kurt (2009). Anabolic-androgenic steroid users in treatment: Social background, drug use patterns and criminality.
29. de Man Lapidoth, Joakim (2009). Binge Eating and Obesity Treatment – Prevalence, Measurement and Long-term Outcome.
30. Vumma, Ravi (2009). Functional Characterization of Tyrosine and Tryptophan Transport in Fibroblasts from Healthy Controls, Patients with Schizophrenia and Bipolar Disorder.
31. Jacobsson, Susanne (2009). Characterisation of Neisseria meningitidis from a virulence and immunogenic perspective that includes variations in novel vaccine antigens.
32. Allvin, Renée (2009). Postoperative Recovery. Development of a Multi-Dimensional Questionnaire for Assessment of Recovery.
33. Hagnelius, Nils-Olof (2009). Vascular Mechanisms in Dementia with Special Reference to Folate and Fibrinolysis.
34. Duberg, Ann-Sofi (2009). Hepatitis C virus infection. A nationwide study of assiciated morbidity and mortality.
35. Söderqvist, Fredrik (2009). Health symptoms and potential effects on the blood-brain and blood-cerebrospinal fluid barriers associated with use of wireless telephones.
36. Neander, Kerstin (2009). Indispensable Interaction. Parents’ perspectives on parent–child interaction interventions and beneficial meetings.
37. Ekwall, Eva (2009). Women’s Experiences of Gynecological Cancer and Interaction with the Health Care System through Different Phases of the Disease.
38. Thulin Hedberg, Sara (2009). Antibiotic susceptibility and resistance in Neisseria meningitidis – phenotypic and genotypic characteristics.
39. Hammer, Ann (2010). Forced use on arm function after stroke. Clinically rated and self-reported outcome and measurement during the sub-acute phase.
40. Westman, Anders (2010). Musculoskeletal pain in primary health care: A biopsychosocial perspective for assessment and treatment.
41. Gustafsson, Sanna Aila (2010). The importance of being thin – Perceived expectations from self and others and the effect on self-evaluation in girls with disordered eating.
42. Johansson, Bengt (2010). Long-term outcome research on PDR brachytherapy with focus on breast, base of tongue and lip cancer.
43. Tina, Elisabet (2010). Biological markers in breast cancer and acute leukaemia with focus on drug resistance.
44. Overmeer, Thomas (2010). Implementing psychosocial factors in physical therapy treatment for patients with musculoskeletal pain in primary care.
45. Prenkert, Malin (2010). On mechanisms of drug resistance in acute myloid leukemia.
46. de Leon, Alex (2010). Effects of Anesthesia on Esophageal Sphincters in Obese Patients.

47. Josefson, Anna (2010). Nickel allergy and hand eczema – epidemiological aspects.
48. Almon, Ricardo (2010). Lactase Persistence and Lactase Non-Persistence. Prevalence, influence on body fat, body height, and relation to the metabolic syndrome.
49. Ohlin, Andreas (2010). Aspects on early diagnosis of neonatal sepsis.
50. Oliynyk, Igor (2010). Advances in Pharmacological Treatment of Cystic Fibrosis.
51. Franzén, Karin (2011). Interventions for Urinary Incontinence in Women. Survey and effects on population and patient level.
52. Loiske, Karin (2011). Echocardiographic measurements of the heart. With focus on the right ventricle.
53. Hellmark, Bengt (2011). Genotypic and phenotypic characterisation of Staphylococcus epidermidis isolated from prosthetic joint infections.
54. Eriksson Crommert, Martin (2011). On the role of transversus abdominis in trunk motor control.
55. Ahlstrand, Rebecca (2011). Effects of Anesthesia on Esophageal Sphincters.
56. Holländare, Fredrik (2011). Managing Depression via the Internet – self-report measures, treatment & relapse prevention.
57. Johansson, Jessica (2011). Amino Acid Transport and Receptor Binding Properties in Neuropsychiatric Disorders using the Fibroblast Cell Model.
58. Vidlund, Mårten (2011). Glutamate for Metabolic Intervention in Coronary Surgery with special reference to the GLUTAMICS-trial.