goal of project to reduce adverse outcomes of warfarin therapy by developing and implementing an...
Post on 18-Dec-2015
214 views
TRANSCRIPT

Goal Of Project
To reduce adverse outcomes of warfarin therapy by developing and implementing an inpatient warfarin
dosing protocol, and by instituting an education program with regard to diet and instructions for physician follow
up at discharge.

CommitteesMed Use Team
Pharmacy and Therapeutics CommitteePatient Safety Committee
Medical Executive Committee
Team MembersSharon Lutz, Ph.D., Vice President, Quality Support Services
Colleen Wheeler, Quality Support ServicesJim Whipple, Nursing EducationDina Vankolpenberg, DietaryDaniel Malinowski, Dietary
Mary Slater, LaboratoryBruce Read, PharmD, Clinical Director
Sunny Choi, PharmD, Computer InterfaceLaura Uhl, PharmD, Computer Interface
Allan Cohen, PharmD, Director




COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol
PURPOSE:
To provide clarity and uniformity in the pharmacy directed dosing of Warfarin.
SCOPE OF SERVICE:
The Warfarin Therapy protocol must be initiated by a physician. For consulted patients, warfarin is initiated or home therapy is continued. Dosing is adjusted based upon patient condition and lab values. Dietary is informed of patients receiving warfarin. Education is provided to the patient prior to hospital discharge.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
PROCEDURE:
Prescriber orders Warfarin by Protocol order, including indication, anticipated duration of therapy and target INR range.
All doses of warfarin shall be scheduled for 1800. For consults ordered after 2300 the first dose of warfarin shall be scheduled for the following evening unless the prescriber orders it as a “now” order.
Initial Patient Assessment - Warfarin by Protocol
The pharmacist will review the patient medical record to confirm indication for therapy, determine baseline coagulation parameters including PT, INR, and Hgb, and to identify any potential interacting medication therapy or patient conditions.
If the most recent PT and INR were obtained more than 24 Hours prior to the planned initial warfarin dose, the pharmacist shall order a PT and INR per protocol and assess the results prior to administration of the initial warfarin dose.
Baseline INR should be below or within the goal INR range prior to initiation of warfarin therapy.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Initial Dosing
Baseline INR< 1.2
Age<=60: ABW>=70KG 7.5-10mg
Post CVA patients 5-7.5mg
Age>=80(all patients) No > than 5mg(Age>90 consider <5mg)
All others 5-7.5mg
Patients on amiodarone or with 3 or more risk factors, consider reducing initial dose by 2.5mg.
If not currently treated with a parenteral anticoagulant, do not exceed 7.5mg for initial dose
Baseline >=1.2 – Dose<=5mg or reduce above dose by up to 2.5mg.
Whenever INR exceeds therapeutic goal and has increased by >.8, discuss options with MD.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Monitoring
Daily PT, INR, and Hgb should be monitored. These labs would be by the pharmacist per protocol if necessary.
The pharmacist should review the clinical notes of the primary service daily to determine the presence of patient conditions that may interact with warfarin therapy and/or impact the dosing
The pharmacist should discuss with the physician those patients with significant changes in the INR or patient condition, or if appropriate dosing is outside parameters of the protocol.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Dose Adjustment
The pharmacist must assess and adjust Warfarin dosing based on lab value and patient condition according to the Dose Adjustment Tables in this protocol. Changes will be documented in pharmacy HMM clinical notes
Changes to dosing shall be ordered by the pharmacist per protocol as appropriate.
Warfarin Risk Factors:
Age >60 (moderate risk) Age >80 (high)
Actual body weight (ABW) <70kg (low)
ABW<Ideal Body Weight (IBW) (low)
IBW<50kg(low) ABW<50kg(moderate)
Significant renal failure (moderate)
DDI (variable)
Protein C or Protein S deficiency
Anti-Phospholipid Antibody Syndrome or Lupus Anticoagulant
Low Vit K intake (moderate)
Reduced Vit K absorption
Liver Disease (moderate)
Hypermetabolic states (fever)
CHF (Moderate)
Malnutrition, Low alb (moderate)
Potential Bleeding risk (high)

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Initial Dose:
Baseline INR< 1.2
Age<=60: ABW>=70KG 7.5-10mg
Post CVA patients 5-7.5mg
Age>=80(all patients) No > than 5mg(Age>90 consider <5mg)
All others 5-7.5mg
Patients on amiodarone or with 3 or more risk factors, consider reducing initial dose by 2.5mg.
If not currently treated with a parenteral anticoagulant, do not exceed 7.5mg for initial dose
Baseline >=1.2 – Dose<=5mg or reduce above dose by up to 2.5mg.
Whenever INR exceeds therapeutic goal and has increased by >.8 , discuss options with MD

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
INR Day 2 of Therapy Dose
INR increase< 0.2 Same as initial dose - Consider slight increase only if initial dose reduced
INR increase 0.2 to 0.4 ½ to ¾ dose - Consider holding if age>=80yo,risk factors
INR increase 0.4 to 0.8 ¼ to ½ previous dose - Consider holding if multiple risk factors or age >=80yo
INR increase > 0.8 Hold dose
INR Day 3 of Therapy Dose
INR increase <.4 Increase dose up to 3/2
INR increase 0.4 to 0.8 ½ to same dose
INR increase >0.8 ¼ to ½ dose - Consider holding If age>= 80yo or INR above goal
INR Day 4 of Therapy Dose (If third dose was held, use ½ of second dose as the reference)
INR<1.5 Increase by 3/2
INR 1.5 to 1.9 and INR increase<=0.4INR increase 0.4 to 0.8
Same dose to 3/2 dose½ to ¾ dose
INR 2.0 to 3.0 and INR increase <=0.4If INR increase 0.4 to 0.8If INR increase >0.8
Same dose (If INR increase <=.2 above goal, consider slight increase)½ to ¾ dose¼ to ½ dose, consider holding (using risk factors as guide)
INR > 3.0-3.5 and INR increase <=0.4If INR increase >0.4
½ to ¾ dose¼ to ½ dose - Consider holding
INR>3.5 Hold
Day 5 and onSubsequent dose should be based on trend established by the INR results from
the third and fourth doses
COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Hospital Discharge Planning
Prior to discharge the patient will be provided appropriate prescriptions for outpatient Warfarin therapy, phlebotomy for INR and physician appointment.
Notification of the Physician
The physician should be notified if there is significant changes in the INR or the patient’s condition, or if appropriate dose or dose adjustment is outside parameters of the protocol.
The physician should also be notified for the following:
INR>4.5
Hgb<9g/DL or decrease by > 2g/DL from previous result
Significant bleeding.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Patient Education
Patients should be educated by the nurse and dietician prior to discharge. Patient education should include the following:
Importance of adherence to warfarin regimen
Potential Side effects, especially the signs and symptoms of bleeding
Possible effects of diet on therapy
Potential for prescription and over-the-counter drug interactions
Written educational materials
Answers to patient’s questions and contact numbers if questions arise after discharge
COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Documentation-Rx to Dose
Pharmacy to document in a pharmacy clinical note prior to initiation of therapy.
Therapy type and home regimen (if applicable)
Indication for therapy, goal INR range, and anticipated duration.
Presence of complicating diseases
Baseline PT, INR, albumin, Hgb. After initial assessment, the note should include Medication Plan (including interacting medications, initial dosing, and monitoring plan.
Daily clinical notes will be written by the pharmacist which will include the following:
Therapy type and home regimen (if applicable)
New medication therapy and its potential effect on the INR.
Most recent PT, INR, and Hgb
Assessment and therapy management plan (including laboratory result evaluation, dosing changes, and monitoring plan)

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin Therapy Protocol (continued)
Cottage Health System
Minimum Requirements For Monitoring Warfarin Therapy
Before initiation of warfarin therapy a baseline INR, H/H and platelet count must be obtained.
INRs will be obtained daily until therapeutic for 2 consecutive draws, then at least weekly.
HgB/HCT to be drawn at least every other day until INR is stable, then at least weekly.
All INRs and coumadin doses will be documented by nursing on the Anticoagulation flow sheet (form 187)
Pharmacy will dispense coumadin in the exact dosage prescribed, check the INR before dispensing and will contact the physician if the dose does not seem appropriate. Heparin anticoagulation is to be discontinued when the patient has been on warfarin a minimum of 3 days and the INR is therapeutic.
MD will be contacted by nursing if the HgB decreases by more than 2gm/dL, for signs of bleeding or the INR is greater than 4.5
Dietary will be notified of all patients on Coumadin therapy.
All patients will be provided discharge instructions, which will include the name of the physician coordinating the coumadin dose.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyPatient Instructions
Warfarin (Oral) (Tablet)
Warfarin (By mouth)
Warfarin (WAR-far-in)
Treats or prevents blood clots. This medicine is a blood thinner (anticoagulant).
Brand Name(s):Coumadin, Jantoven, WarfarinThere may be other brand names for this medicine.
When This Medicine Should Not Be Used:
You should not use this medicine if you have had an allergic reaction to warfarin, or if you are pregnant or planning to become pregnant. Ask your doctor about using this medicine if you are having or have recently had surgery. Usually, you should not use this medicine if you are having surgery on your eyes, brain, or spine, or major surgery that will leave you with large, open wounds. This medicine should not be used if you have certain heart problems, severe or uncontrolled high blood pressure, or any condition that may cause uncontrolled bleeding (such as a stomach ulcer or hemophilia).

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyPatient Instructions (continued)
How to Use This Medicine:
Tablet
Your doctor will tell you how much of this medicine to use and how often. Your dose may need to be changed several times in order to find out what works best for you. Do not use more medicine or use it more often than your doctor tells you to.
You may take this medicine with or without food.
If a dose is missed:
If you miss a dose or forget to use your medicine, use it as soon as you can. If it is almost time for your next dose, wait until then to use the medicine and skip the missed dose. Do not use extra medicine to make up for a missed dose.
How to Store and Dispose of This Medicine:
Store the medicine in a closed container at room temperature, away from heat, moisture, and direct light.
Ask your pharmacist, doctor, or health caregiver about the best way to dispose of any leftover medicine after you have finished your treatment. You will also need to throw away old medicine after the expiration date has passed.
Keep all medicine away from children and never share your medicine with anyone.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyPatient Instructions (continued)
Drugs and Foods to Avoid:
Ask your doctor or pharmacist before using any other medicine, including over-the-counter medicines, vitamins, and herbal products.
There are many other medicines, including nonprescription (over-the-counter) medicines and herbal products, that you should not use while you are taking warfarin. Make sure your doctor knows about ALL other medicines you are using.
Carefully follow your doctor's instructions about any special diet. This medicine works best when you eat about the same amount of vitamin K in your food every day. Avoid big changes in how much vitamin K you eat. Some foods that have a high amount of vitamin K are broccoli, brussels sprouts, cabbage, and green leafy vegetables such as spinach and salad greens.
You should avoid drinking cranberry juice or any other cranberry products.
Do not drink alcohol while you are using this medicine.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyPatient Instructions (continued)
Warnings While Using This Medicine:
Using this medicine while you are pregnant can harm your unborn baby. Use an effective form of birth control to keep from getting pregnant. If you think you have become pregnant while using the medicine, tell your doctor right away.
Make sure your doctor knows if you are breastfeeding, or if you have liver disease, kidney disease, congestive heart failure, high blood pressure, diabetes, any type of infection, or any other medical problems. Also tell your doctor if you have recently had a fall or other injury.
You may bleed more easily while you are using this medicine. Stay away from rough sports or other situations where you could be bruised, cut, or injured. Brush and floss your teeth gently. Be careful when using sharp objects, including razors and fingernail clippers. Avoid picking your nose. If you need to blow your nose, blow it gently.
Carry an ID card or wear a medical alert bracelet to let any emergency caregivers know that you are using warfarin.
Make sure any doctor or dentist who treats you knows that you are using this medicine. You may need to stop using this medicine several days before having surgery or medical tests.
Your doctor will need to check your blood at regular visits while you are using this medicine. Be sure to keep all appointments.

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyWarfarin Work Flow
Order For Warfarin by MD Order By MD for Pharmacy to Dose
Pharmacist enters order for specific dose Pharmacist enters order for specific dose
Then enters “COUMD” Enters COUMRX
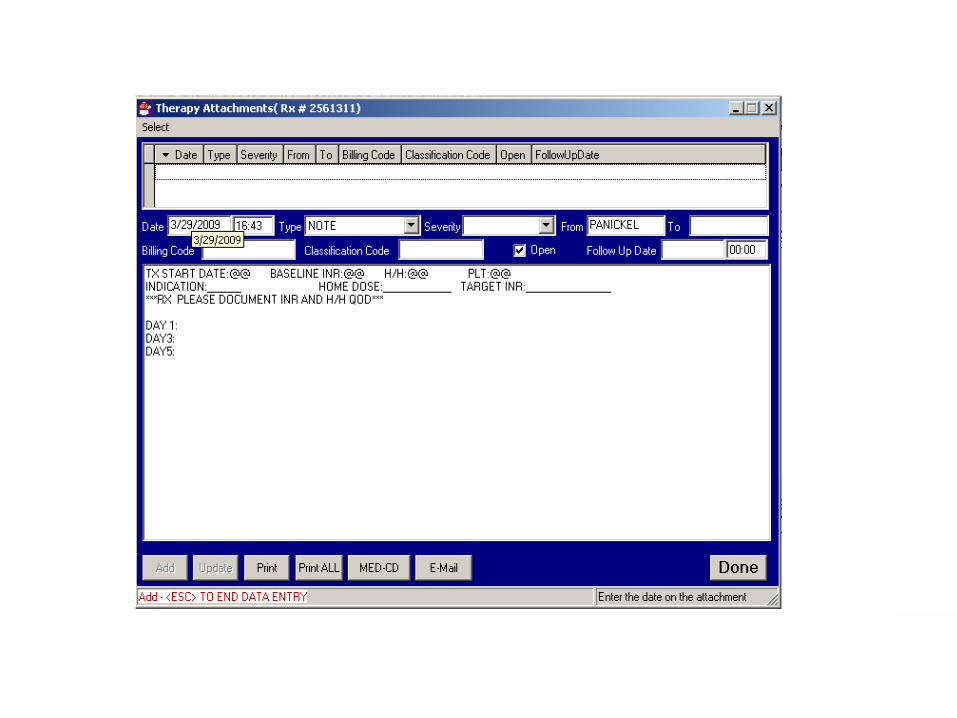
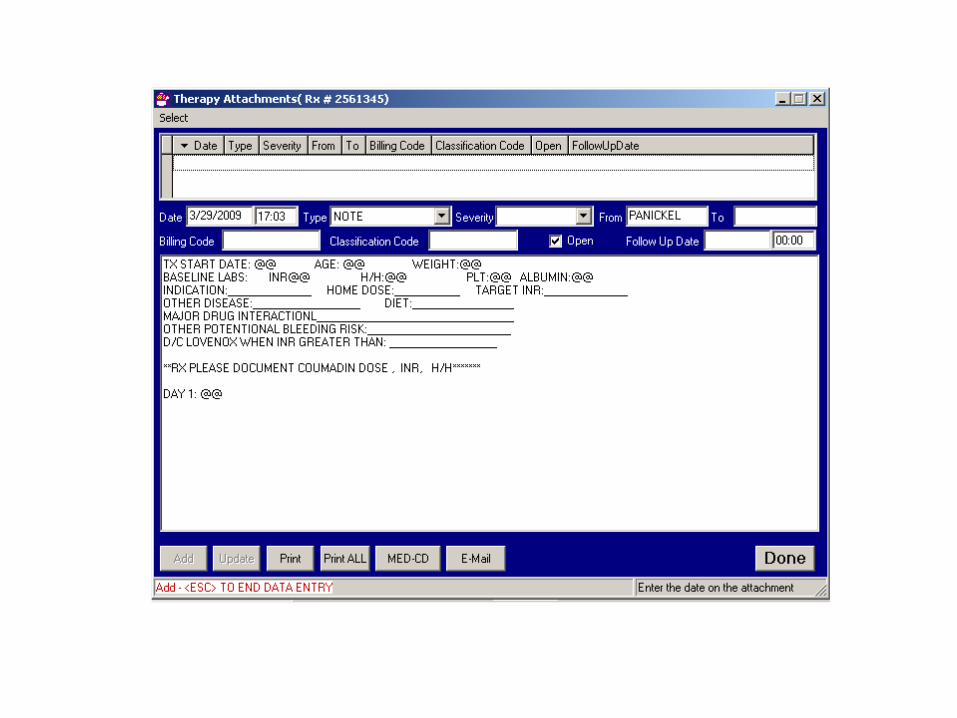
Pop up window with forced entry for required baseline data, and follow up dates
Pop up with forced entry for required criteria for dosing.
COUMD shows on MAR with message “contact physician if no routine order by 1800, chart dose on warfarin flowsheet”
RX to dose on MAR Chart on Flow sheet
Any new or continuing warfarin is summarized and printed for both pharmacy and dietary each morning for follow-up
Same summary

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyWarfarin Work Flow (continued)
For both order entry modes, pharmacy documents doses, INR, Hgb/HCT, platelets, MD interventions, drug interactions in therapy attachment for each patient.
Dietary initiates education of new and continuing patients, and documents in electronic CPOE interface. Warfarin handout given to patient.
At discharge, nurse gives written discharge instructions, including the name of physician for subsequent follow up and INR. This is also documented in CPOE electronic interface.
A copy of in-house flow sheet to go with patient to follow-up MD.


COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyMinimum requirements for warfarin dosing
Baseline Hgb/HCT, platelets must be obtained before initiation of therapy.
INR daily until two consecutive draws are therapeutic, then at least weekly.
All INR and warfarin doses will be documented on Anticoagulation Flow Sheet.
Exact doses will be dispensed, so that overdose will not occur.
MD will be contacted if Hgb drops by more than 2gm/dl, signs of bleeding, or INR>4.5.
Dietary department will be notified of all patients on warfarin therapy.
All patients will be provided discharge instructions, which will include the name of the physician coordinating the dose.


COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyGoal Measurement
7 month inpatient data collection (March 2008 to September 2008)
INR Inpatient Data
Trauma Research ”Fall on Warfarin Data”
Further research comparisons pending
Current comparison data in process
Preliminary results suggest Pharmacy department dosing reduces supratherapeutic INR’s by approximately 50%
Further comparison data ongoing
Onset to therapeutic range: Incidence of ADRs
MD vs RX dosing
Outpatient ADR’s

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyMinimum Requirements Audit (Duration 3 Weeks)
Results:
100% Compliance by Dietary Education 2 of 37 inappropriate for education (tube feeds, not cognitive)
Nursing Education at Discharge:Unknown - means of documentation by nursing at discharge not implemented: Audit resulted in new interface to be created for documentation.
36 out of 37 patients had required baseline data prior to initiation of therapy (97% compliance)
Exact Doses Dispensed (100% compliance)

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyMinimum Requirements Audit (Duration 3 Weeks) (continued)
Doses charted on flowsheet
One of 37 had warfarin flowsheet completed: 3% complianceLack of educationResistance to “charting in two places”Alternatives being investigatedMAR documentation 100% compliance
34 of 37 had baseline data, doses charted in pharmacy notes (92% compliance)
36 of 37 had daily INRs until therapeutic (97% compliance)
2 of 37 had H/H drop: Verified by pharmacy that MD aware: Progress note notation by MD (100% compliance)

COTTAGE HEALTH SYSTEMPharmacy Directed Warfarin TherapyFuture Areas of Improvement
More active participation with MD’s in dosing:Computer modelsPharmacogenetic dosing based on CYP 2C9 and VKORC1 gene variations
Standardize orthopedic dosing
Outpatient follow-up
Documentation