going the distance: food and fluid going the distance
TRANSCRIPT

44thth Medical Conference on Medical Conference on UltrarunningUltrarunning, May 10, May 10thth 2013, 2013, SteenbergenSteenbergen, Netherlands, Netherlands
Going the distance: food and fluid Going the distance: food and fluid iintake ntake to optimize performance and minimize diseaseto optimize performance and minimize disease
HyponatremiaHyponatremia, , RhabdomyolysisRhabdomyolysisd R ld R l FF il iil iand Renal and Renal FFailure in ailure in
UUltradistanceltradistance RunnersRunnersUUltradistanceltradistance RunnersRunnersTamara HewTamara Hew--Butler DPM PhD FACSMButler DPM PhD FACSMTamara HewTamara Hew Butler DPM, PhD, FACSMButler DPM, PhD, FACSMOakland University, Rochester, USAOakland University, Rochester, USA

HyponatremiaHyponatremiaypyp
RhabdomyolysisRhabdomyolysis & Renal Failure& Renal FailureRhabdomyolysisRhabdomyolysis & Renal Failure& Renal Failure
Fluid IntakeFluid Intake
Sodium IntakeSodium IntakeSodium IntakeSodium Intake
RecommendationsRecommendations

EAH DEFINITIONEAH DEFINITIONEAH DEFINITIONEAH DEFINITIONExerciseExercise associatedassociated hyponatremiahyponatremia (EAH)(EAH)ExerciseExercise--associated associated hyponatremiahyponatremia (EAH)(EAH)
is the occurrence ofis the occurrence ofh t ih t i i i di id l di i di id l dhyponatremiahyponatremia in individuals engagedin individuals engaged
in prolonged physical activityin prolonged physical activityd i d fi d b ld i d fi d b land is defined by a serum or plasmaand is defined by a serum or plasmasodium concentration below thesodium concentration below the
l f f thl f f thnormal reference range of the normal reference range of the laboratory performing the testlaboratory performing the test

Serum Serum [Na+][Na+]
((mmolmmol/L)/L)
150
155 HYPERNATREMIA
145
140 NORMONATREMIA135
130
125 HYPONATREMIA

EFFECTIVE OSMOLALITY
HYPERNATREMIAHYPERNATREMIAHYPERNATREMIAHYPERNATREMIA
NORMONATREMIANORMONATREMIA
HYPONATREMIAHYPONATREMIA

pulmonary edemapulmonary edema
HYPONATREMIAHYPONATREMIA NORMONATREMIANORMONATREMIAHYPONATREMIAHYPONATREMIA NORMONATREMIANORMONATREMIA
encephalopathyencephalopathy normalnormal
Ayus JC et al. Ann Intern Med 2000

IncidenceIncidenceIncidenceIncidenceStandard marathon:Standard marathon:
Asymptomatic: 0Asymptomatic: 0 13%13%Asymptomatic: 0Asymptomatic: 0--13%13%Clinically symptomatic : 1%Clinically symptomatic : 1%
Deaths (confirmed): 5Deaths (confirmed): 5
UltramarathonUltramarathon::A t ti 0A t ti 0 51%51%Asymptomatic: 0Asymptomatic: 0--51%51%
Clinically symptomatic: <1%Clinically symptomatic: <1%Ironman Triathlon:Ironman Triathlon:
Asymptomatic: 0Asymptomatic: 0--18%18%y py pClinically Symptomatic: 12%Clinically Symptomatic: 12%

PATHOPHYSIOLOGYPATHOPHYSIOLOGYDILUTIONAL
HYPONATREMIADEPLETIONAL
HYPONATREMIA:HYPONATREMIA:Too much water
(drinking too much)
HYPONATREMIA:Losing too much salt
(sweating)
AUTOREGULATIONAUTOREGULATIONAUTOREGULATIONAUTOREGULATION

EAH: etiologic possibilities
mixed solute“pure” water “pure” solutemixed solute loss and water
retention
pretention from
SIADH
pure solute depletion from sodium loss
+H2O -NaCl-NaCl +H2O
?Exercise-inducedExercise induced
antidiuretic hormone secretion
?

Relationship between weight changes and post-race serum [Na+] in 2154 endurance athletes.
154154158158160160
OverhydrationOverhydration Increasing % Increasing % DehydrationDehydrationEuhydrationEuhydration
142142146146150150154154
HypernatremiaHypernatremia
m [N
am
[Na+
]+]
130130134134138138142142
NormonatremiaNormonatremia
BiochemicalBiochemicalHyponatremiaHyponatremiae
seru
me
seru
m
118118122122126126130130 ypyp
n = 21540 33Po
st r
ace
Post
rac
e
Clinically Clinically significantsignificant
hyponatremiahyponatremiaEAHEEAHE
110110114114118118 r = 0.33
P < 0.0001
PP ypyp
--1010--99--88--77--66--55--44--33--22--1100112233445566778899 --1515--1414--1313--1212--1111
EAHEEAHE
Body Weight change (Body Weight change (%)%)Noakes TD et al. PNAS 2005;102: 18550Noakes TD et al. PNAS 2005;102: 18550--18555 18555

Hoffman MD et al 2013 MSSE
Measuring fluid losses during exercise:Measuring fluid losses during exercise:B d i ht ≠ T t lB d i ht ≠ T t l BB dd WW ttBody weight ≠ Total Body weight ≠ Total BBody ody WWaterater
BodyBody weight changesweight changesBody Body weight changes weight changes during exerciseduring exercise
b l li blb l li blbecome less reliablebecome less reliableindicators of fluid balanceindicators of fluid balance
as race distance progressesas race distance progresses
Lee JKW unpublished

EAH: signs and symptoms
mixed solute“pure” water “pure” solutemixed solute loss and water
retention
pretention from
SIADH
pure solute depletion from sodium loss
+H2O -NaCl-NaCl +H2O
h/o overdrinkingbloating
“Dehydration”thirsty, dry mouth
i dvomiting↔↑ BP
↑ body weight
skin tentingorthostatic hypotension↓ body weight
mixed
↑ body weight↑↔↓urination? ↓urination
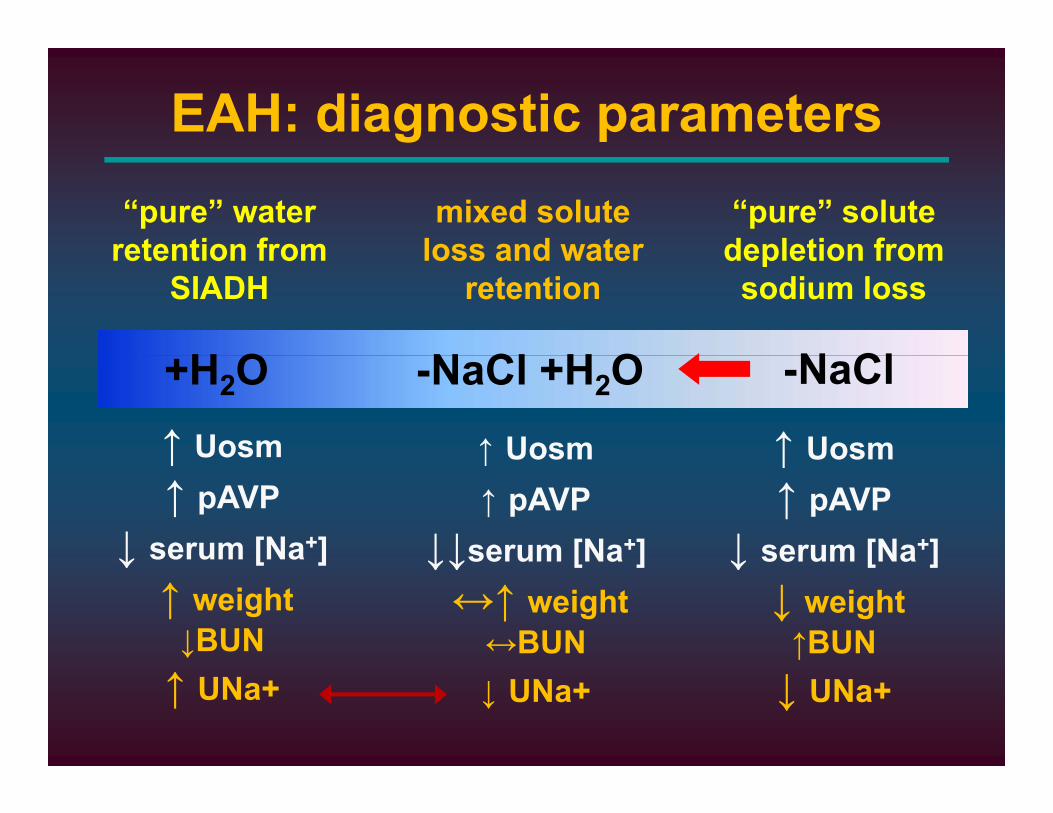
EAH: diagnostic parametersmixed solute
loss and water“pure” water
retention from“pure” solute depletion fromloss and water
retentionretention from
SIADH
H O
depletion from sodium loss
N ClN Cl H O↑ Uosm
+H2O
↑ Uosm
-NaCl-NaCl +H2O
↑ Uosm↑↑ pAVP
↓ serum [Na+]
↑ Uosm↑ pAVP
↓ serum [Na+]
↑ Uosm↑ pAVP
↓↓serum [Na+]↓ [ ]↑ weight↓BUN
↓ serum [Na ]↓ weight↑BUN
↓↓serum [Na ]↔↑ weight↔BUN
↑ UNa+ ↓ UNa+↓ UNa+

Summary: Summary: HyponatremiaHyponatremiayy ypypEAH is a EAH is a lifelife--threateningthreatening
fluid and sodium imbalancefluid and sodium imbalance
EAH b di d lEAH b di d lEAH can be diagnosed onlyEAH can be diagnosed onlyby a by a blood testblood test
EAH is caused by a EAH is caused by a combinationcombination of of fl id ti dfl id ti dexcess fluid consumption and excess fluid consumption and
sweat sodium losses during sweat sodium losses during ultraenduranceultraendurance runningrunning

HyponatremiaHyponatremia
RhabdomyolysisRhabdomyolysis & Renal Failure& Renal FailureRhabdomyolysisRhabdomyolysis & Renal Failure& Renal Failure
Fluid IntakeFluid Intake
Sodium IntakeSodium IntakeSodium IntakeSodium Intake
RecommendationsRecommendations

Skeletal MuscleSkeletal Muscle40% Bod Weight40% Bod Weight40% Body Weight 40% Body Weight
50% Total Body Water50% Total Body Water70% Total Body K+70% Total Body K+
Extracellular Volume Extracellular Volume 35% Total Body Water35% Total Body Water
11--2% Total Body K+2% Total Body K+

RhabdomyolysisRhabdomyolysisRhabdomyolysisRhabdomyolysisDissolution of skeletal muscleDissolution of skeletal muscle
from direct or indirect injury from direct or indirect injury (ATP depletion, unregulated ↑intracellular calcium)(ATP depletion, unregulated ↑intracellular calcium)
Characterized by leakage ofCharacterized by leakage ofmuscle cell contents into the circulationmuscle cell contents into the circulationmuscle cell contents into the circulationmuscle cell contents into the circulation
(electrolytes, (electrolytes, myoglobinmyoglobin, , sarcoplasmicsarcoplasmic proteins)proteins)
Acute kidney injury is a direAcute kidney injury is a direAcute kidney injury is a direAcute kidney injury is a direcomplication of severe complication of severe rhabdomyolysisrhabdomyolysis
from ↑from ↑ myoglobinmyoglobinfrom ↑ from ↑ myoglobinmyoglobinBosch X et al NEJM, 2009

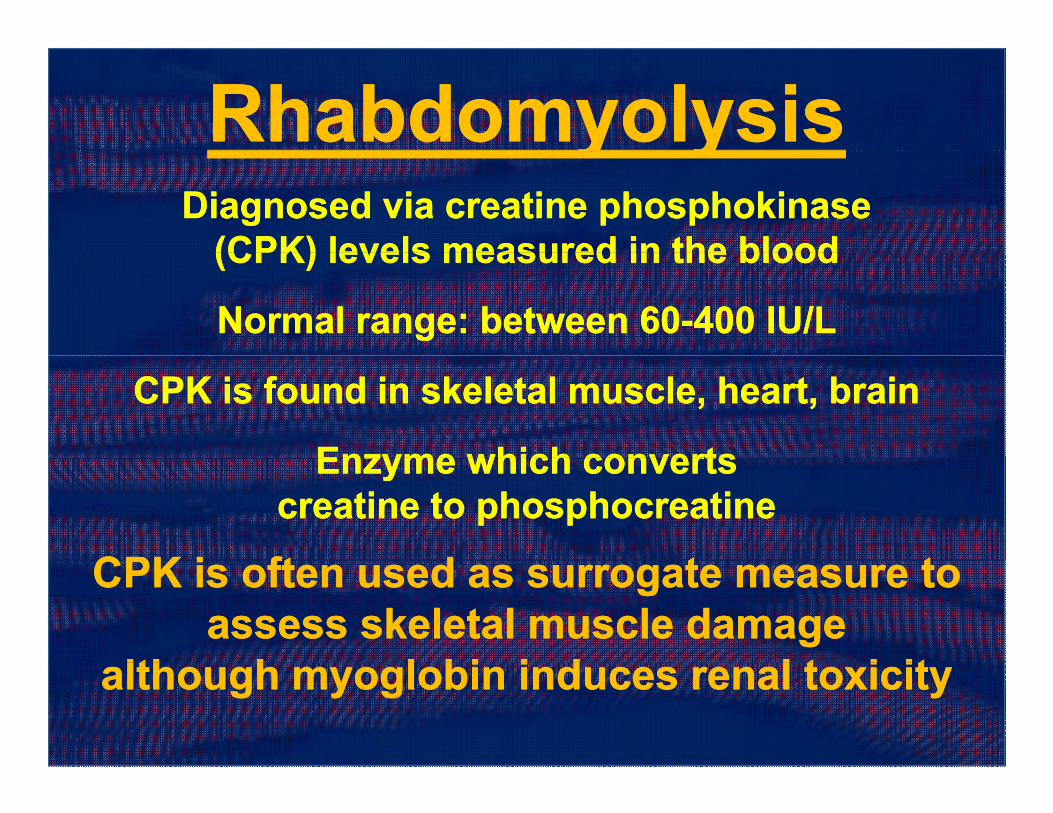
RhabdomyolysisRhabdomyolysisy yy yDiagnosed via Diagnosed via creatinecreatine phosphokinasephosphokinase
(CPK) levels measured in the blood(CPK) levels measured in the blood(CPK) levels measured in the blood(CPK) levels measured in the blood
NNormal range: between 60ormal range: between 60--400 IU/L400 IU/L
CPK is found in skeletal muscle, heart, brain CPK is found in skeletal muscle, heart, brain
Enzyme which convertsEnzyme which convertsEnzyme which converts Enzyme which converts creatinecreatine to phosphocreatineto phosphocreatine
CPK i ft d t tCPK i ft d t tCPK is often used as surrogate measure to CPK is often used as surrogate measure to assess skeletal muscle damageassess skeletal muscle damage
lth h l bi i d l t i itlth h l bi i d l t i italthough myoglobin induces renal toxicityalthough myoglobin induces renal toxicity

WSER 2011WSER 2011
FogardFogard K et al ACSM 2012K et al ACSM 2012

Low incidence renal failure with Low incidence renal failure with exertional rhabdomyolysisexertional rhabdomyolysis
0% of 35 males developed acute renal
exertional rhabdomyolysisexertional rhabdomyolysis0% of 35 males developed acute renal
failure in a retrospective study spanning 5 years
225,000 annual ER visits225,000 annual ER visits (Sinert R et al Ann Emerg Med 1994)
Population-based analysis military base22.2 cases per 100,000 per year
(Alpers JP Muscle and Nerve 2010)
Women have lower serum CK activitiesWomen have lower serum CK activities than men in response to same
amount of exercise(Noakes T, Sports Med 1987)( , p )

Myoglobin-induced acute kidney injuryrequires nephrotoxic cofactorsnephrotoxic cofactorsrequires nephrotoxic cofactorsnephrotoxic cofactors
HypovolemiaHypovolemia AciduriaAciduriaypypIntraIntra--renal vasoconstrictionrenal vasoconstriction
concentrates myoglobin concentrates myoglobin MyoglobinMyoglobin dissociatesdissociates
y gy galong renal tubulesalong renal tubules
Renal tubular Renal tubular
Precipitates with Precipitates with TammTamm--HorsfallHorsfall proteins proteins
to form caststo form castse a tubu ae a tubu aobstructionobstruction
Liberates Liberates ferrihemateferrihematewhich is nephrotoxicwhich is nephrotoxicwhich is nephrotoxicwhich is nephrotoxic

HyponatremiaHyponatremiaypyp
Is there a link?Is there a link?Is there a link?Is there a link?
RhabdomyolysisRhabdomyolysis

WSER 2011WSER 2011
FogardFogard K et al ACSM 2012K et al ACSM 2012

14000
16000
18000
HypoNa+
10000
12000
14000
K] U
/L
Mean [CPK] excluding severe EAH athlete
HypoNaat Checkpoint 2
6000
8000
[CPK
Severe EAH athlete
0
2000
4000
Start 2 4 Post
Checkpoint
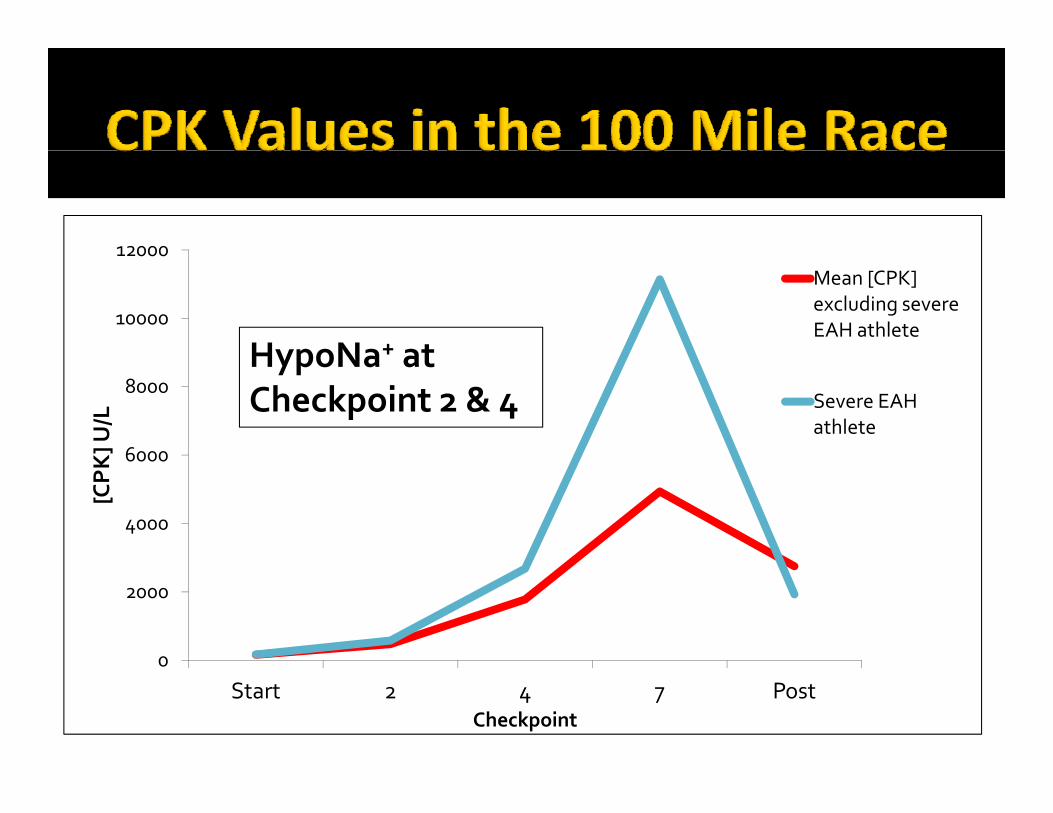
12000
10000
12000Mean [CPK] excluding severe EAH athlete
HypoNa+ at
6000
8000
K] U
/L
Severe EAH athlete
HypoNa at Checkpoint 2 & 4
4000
6000
[CPK
0
2000
0
Start 2 4 7 PostCheckpoint
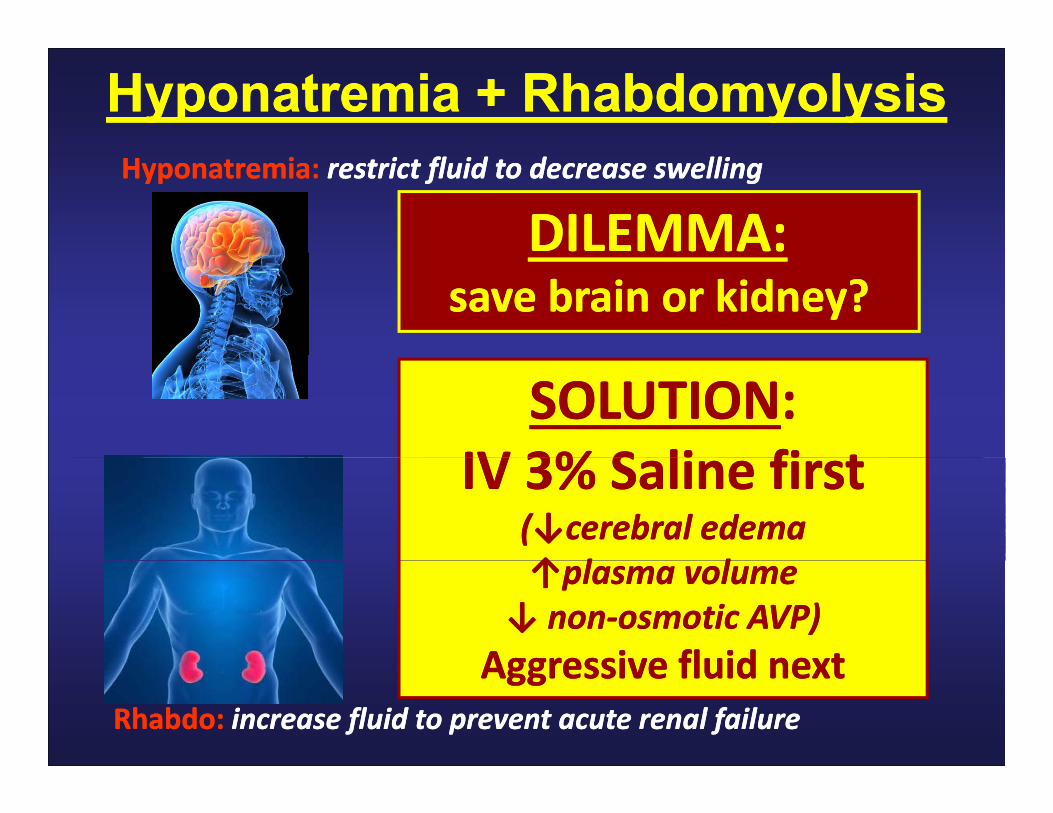
Hyponatremia Hyponatremia + Rhabdomyolysis+ RhabdomyolysisHyponatremiaHyponatremia: restrict fluid to decrease swellingrestrict fluid to decrease swelling
DILEMMA:DILEMMA:save brain or kidney?save brain or kidney?
SOLUTIONSOLUTION::IV 3%IV 3% S li fi tS li fi tIV 3% IV 3% Saline firstSaline first
(↓cerebral edema (↓cerebral edema ↑ l l↑ l l↑plasma volume↑plasma volume
↓ non↓ non‐‐osmotic AVP)osmotic AVP)Aggressive fluidAggressive fluid nextnext
Rhabdo:Rhabdo: increase fluid to prevent acute renal failureincrease fluid to prevent acute renal failure
Aggressive fluid Aggressive fluid nextnext

Summary:Summary: RhabdomyolysisRhabdomyolysisSummary: Summary: RhabdomyolysisRhabdomyolysisRhabdomyolysisRhabdomyolysis is common afteris common afterRhabdomyolysisRhabdomyolysis is common after is common after
ultradistanceultradistance racesraces
Acute renal failure is rareAcute renal failure is rare
EAH, EAH, rhabdorhabdo andand renal failurerenal failuret b i blt b i blappears to be a unique problem appears to be a unique problem
inin ultraenduranceultraendurance runnersrunnersin in ultraenduranceultraendurance runnersrunners
HyponatremiaHyponatremia
RhabdomyolysisRhabdomyolysis & Renal Failure& Renal FailureRhabdomyolysisRhabdomyolysis & Renal Failure& Renal Failure
Fluid IntakeFluid Intake
Sodium IntakeSodium IntakeSodium IntakeSodium Intake
RecommendationsRecommendations

RUNNERSRUNNERS SWEAT
11°° THERMOREGULATIONTHERMOREGULATION
Exercise >40% VO2 Max92% water92% water and 87% sodium87% sodium
flosses derived from sweat
A t [N ] 35 E /LAverage sweat [Na+]: ~35mEq/L (range: 10-70)
hypotonic to plasmay
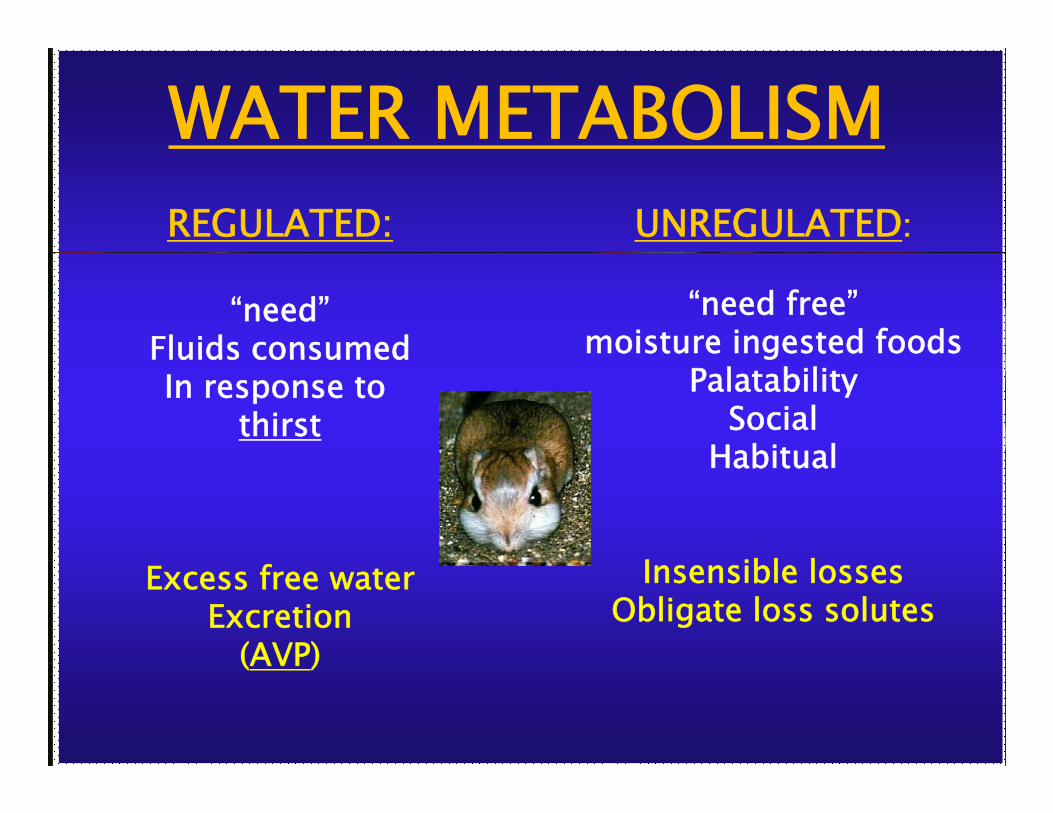
WATER METABOLISMUNREGULATED:REGULATED:
“need free”moisture ingested foods
“need”Fluids consumed g
PalatabilitySocial
Habitual
Fluids consumedIn response to
thirstHabitual
I ibl lInsensible lossesObligate loss solutes
Excess free waterExcretion
(AVP)(AVP)

THIRST“Thirst is one of the more powerful
of the beha ioral dri esof the behavioral drives.When maximally stimulated in humans,
the craving for water cannotthe craving for water cannotbe ignored and can become
sufficiently intense to dominate allyother thoughts and sensations”
I h l h d l hi i l dIn healthy adults, thirst is regulatedlargely, if not exclusively, by the
effective osmotic pressure of plasmaeffective osmotic pressure of plasma
Robertson GL, Kidney Int 1984
The ph siological sensation of thirstThe physiological sensation of thirstis designed to protect
plasma osmolality and volume- not total body water –y
within the normal physiological rangeDrinking to thirst will prevent both
dsynatremias associated with exercise
Prescribed drinking is appropriateunder steady state controlled conditionsunder steady-state, controlled, conditions

POsm( k )
Thirst is stimulated in humans when thekidneys can no longer protect osmolalityI d d f b d i h h(mosm/kg)
300Independent of bodyweight change
THIRST
295Normal [Na+]
290
285
280 AVP
Robertson GL, Recent Prog Horm Res 1977
Subject #

Field Study Data: Replacing bodyweightYearYear AuthorsAuthors RaceRace
(km)(km)Na+ preNa+ pre(mmol/L)(mmol/L)
Na+ postNa+ post(mmol/L)(mmol/L)
Na+Na+changechange
% BW% BWlossloss
TimeTime(hr)(hr)
20032003 137137±±11 133133±±22 --44 +2+2 44TwerenboldTwerenbold 41 Run41 Run
20052005 HewHew--ButlerButler 109 Bike109 Bike 139139±±33 138138±±33 --11 --22 55
20022002 GlaceGlace 160 Run160 Run 144144 140140 --44 --11 262620022002 GerthGerth 100 Run100 Run 137137±±55 131131±±22 --66 --11 1414
20032003 StuempfleStuempfle 161 Snow161 Snow 141141±±11 138138±±22 --33 --22 383819891989 NelsonNelson 42 Run42 Run 139139±±00 142142±±00 33 --33 4419731973 RefsumRefsum 90 Ski90 Ski 142142 141141 --11 --33 8819781978 C hC h 42 R42 R 139139±±22 142142±±22 33 33 3319781978 CohenCohen 42 Run42 Run 139139±±22 142142±±22 33 --33 3319771977 Kavanagh et al.Kavanagh et al. 42 Run42 Run 146146±±22 148148±±22 33 --33 4419761976 NoakesNoakes 160 Run160 Run 144144±±11 140140±±33 --44 --33 161620052005 HewHew--ButlerButler 56 Run56 Run 139139±±33 138138±±33 --11 --44 6620052005 HewHew--ButlerButler 56 Run56 Run 139139±±33 138138±±33 --11 --44 6620062006 HewHew--ButlerButler 226 Tri226 Tri 141141±±22 141141±±33 00 --44 121219751975 MaronMaron 42 Run42 Run 141141±±11 141141±±11 00 --44 3319891989 Rocker et al.Rocker et al. 42 Run42 Run 144144 149149 55 --55 3319541954 BecknerBeckner 42 Run42 Run 141141 156156 77 --5519641964 AstrandAstrand 85 Ski85 Ski 144144 152152 88 --66 99
33
Hew-Butler et al, CJSM 2006
Summary: Fluid IntakeSummary: Fluid IntakeyyWater intake is Water intake is highly regulated highly regulated g y gg y g
governed cooperatively by governed cooperatively by osmoticallyosmotically--drivendrivenosmoticallyosmotically--driven driven
thirst stimulation thirst stimulation and and
antianti--diuretic hormone secretiondiuretic hormone secretionantianti diuretic hormone secretion diuretic hormone secretion (arginine vasopressin; AVP) (arginine vasopressin; AVP)

HyponatremiaHyponatremia
RhabdomyolysisRhabdomyolysis & Renal Failure& Renal FailureRhabdomyolysisRhabdomyolysis & Renal Failure& Renal Failure
Fluid IntakeFluid Intake
Sodium IntakeSodium IntakeSodium IntakeSodium Intake
RecommendationsRecommendations

Sodium supplementation has beenSodium supplementation has beenshown to be beneficial:
HHigh intensity work inigh intensity work ing yg yhot ambient temperatureshot ambient temperatures
Exercisers unExercisers un--acclimatized to heatacclimatized to heat
LLong duration (<24) exerciseong duration (<24) exercise

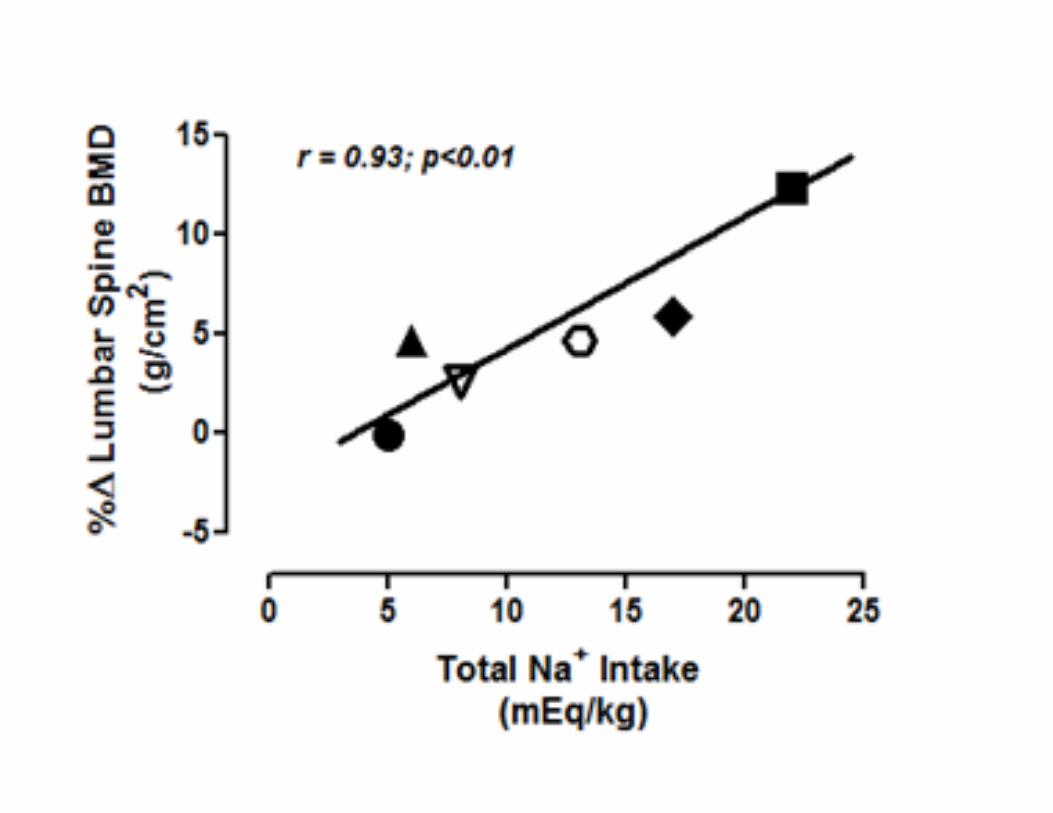
Longer distance + hotter temperature = ↑ contribution sweat [Na+] losses
Hoffman MD et al MSSE 2013

The IOM in 2004 set theThe IOM in 2004 set theadequate index for daily sodium
intake at 1.5g (60mmol) forintake at 1.5g (60mmol) forsufficient for physically active people
Th di t i t k i th USAThe mean dietary intake in the USAis 3.1-4.7g (135-204mmol) for males and
2 3 3 1g (100 135mmol) for females2.3 – 3.1g (100-135mmol) for females
thus, for those ingesting a western diet, , g g ,sodium supplementation seems unnecessary
during exercise <24 hours in temperate climates

VARIABLEVARIABLE2424--hour hour DuringDuring 2424--hourhour
VARIABLEVARIABLE PrePre--racerace(N = 18)(N = 18)
RaceRace(N = 18)(N = 18)
PostPost--racerace(n = 8)(n = 8)
T t l V lT t l V l 3 33 3 ±± 1 71 7 0 30 3 ±± 0 30 3 1 71 7 ±± 1 71 7Total VolumeTotal Volume(liters)(liters)
3.3 3.3 ±± 1.71.7(0.9 (0.9 –– 6.2)6.2)
0.3 0.3 ±± 0.30.3(0.03 (0.03 –– 1.6)1.6)
1.7 1.7 ±± 1.71.7(0.5 (0.5 –– 5.6)5.6)
Specific Specific GravityGravity
1.009 1.009 ±± 0.000.00(1.003 (1.003 –– 1.019)1.019)
1.017 1.017 ±± 0.010.01(1.003 (1.003 –– 1.030)1.030)
1.021 1.021 ±± 0.000.00(1.005 (1.005 –– 1.029)1.029)
Total Na+Total Na+(mEq)(mEq)
195.0 195.0 ±± 79.679.6(40.4 (40.4 –– 322.5)322.5)
8.8 8.8 ±± 5.95.9(0.3 (0.3 –– 26.2)26.2)
44.5 44.5 ±± 39.539.5(11.1 (11.1 –– 118.1)118.1)
Total K+Total K+(mEq)(mEq)
83.5 83.5 ±± 33.533.5(32.4 (32.4 –– 135.0)135.0)
25.4 25.4 ±± 17.517.5(2.2 (2.2 –– 74.9)74.9)
55.7 55.7 ±± 33.733.7(15.4 (15.4 –– 104.0)104.0)
* Unpublished data*
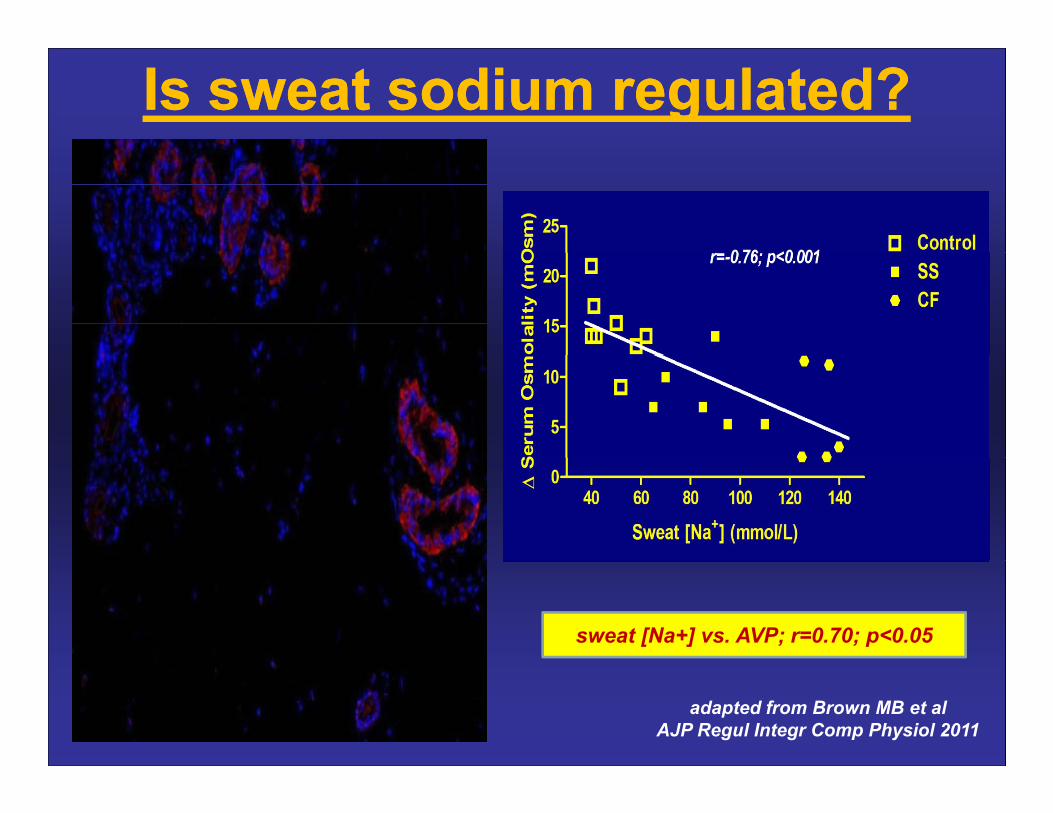
Is sweat sodium regulated?Is sweat sodium regulated?
sweat [Na+] vs. AVP; r=0.70; p<0.05
adapted from Brown MB et al AJP Regul Integr Comp Physiol 2011
SODIUM APPETITE:D i i i h ?Does it exist in humans?
15 20% Addisonian patients relate true salt cravings15-20% Addisonian patients relate true salt cravingsPerinatal sodium loss increases salt appetite
Sodium Palatability Sodium Palatability increases with:increases with:increases with:increases with:
Exercise with sweat lossExercise with sweat lossH di l iH di l iHemodialysisHemodialysis
Experimental sodium depletionExperimental sodium depletion

Palatability Rating% of full scale
palatability ratingto 1 M NaCl solution
40
60to 1 M NaCl solution
as a function of [Na+]p
20
40
20
0rehydration
-40
-20
l
148 150 152 154 156 158-60
control
Takamata A et al, Appl Physiol 1994
[Na+]pmEq/kg H2O

8
10placebo (r=0.74; p0<001)
V2 agonist (r=0.59; p<0.01)
V2 antagonist (r=0.15;NS)
Combined Data(r=0.46;p<0.001)
Rat
ing
4
6
8 g ( )
alat
abili
ty
(0-1
0)
0
2
Sod
ium
P
0 50 100
Sweat [Na+](mmol/L)( )
Sweat [Na+] accounted for 21% of variance Sweat [Na+] accounted for 21% of variance in sodiumin sodium palatabilitypalatability (55% placebo)(55% placebo)in sodium in sodium palatability palatability (55% placebo)(55% placebo)
The “saltier” the sweat, the more the subject “craved” salty beveragesThe “saltier” the sweat, the more the subject “craved” salty beverages(increased palatability)(increased palatability)

Hew-Butler T et al HMR (in press)

CONFLICTING DATACONFLICTING DATACONFLICTING DATACONFLICTING DATASODIUMSODIUMSODIUM SODIUM
SUPPLEMENTATIONSUPPLEMENTATIONSUPPLEMENTATIONSUPPLEMENTATIONB fit D t i tBenefits vs. Detriments
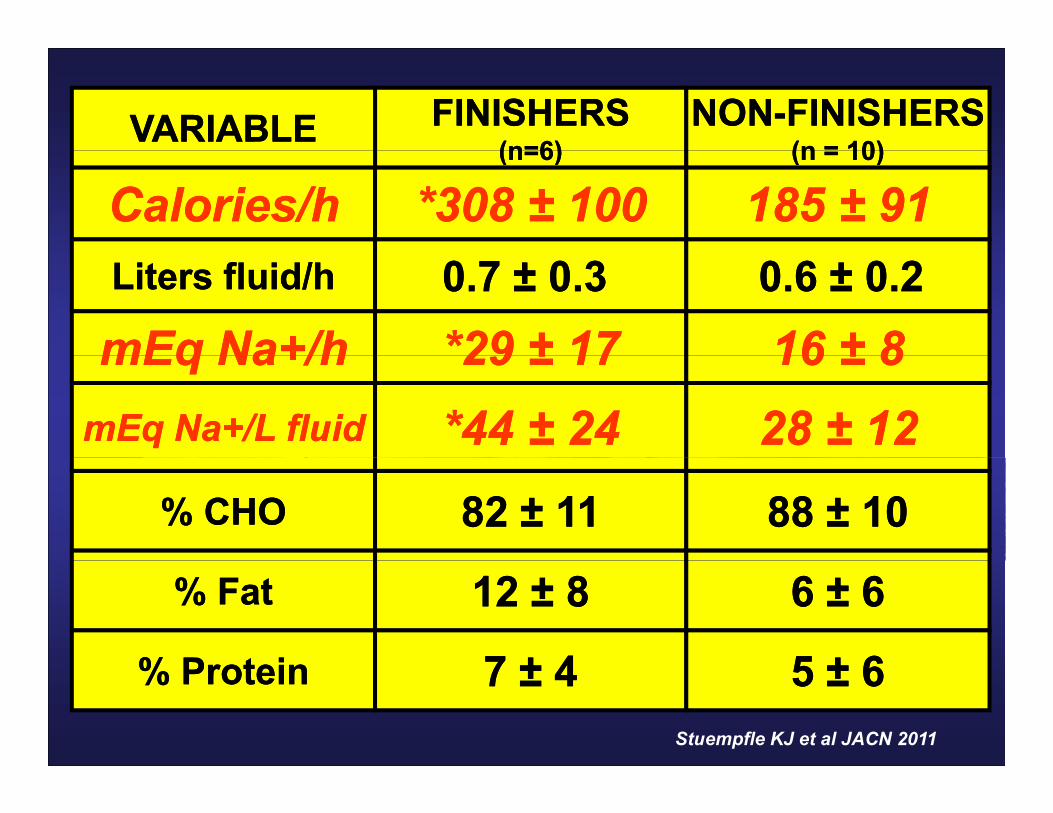
FINISHERSFINISHERS(n=6)(n=6)
NONNON--FINISHERSFINISHERS(n = 10)(n = 10)VARIABLEVARIABLE (n=6)(n=6) (n = 10)(n = 10)
Calories/hCalories/h *308 *308 ±± 100100 185 185 ±± 9191Liters fluid/hLiters fluid/h
mEq Na+/hmEq Na+/h0.7 0.7 ±± 0.3 0.3 *29*29 ±± 1717
0.6 0.6 ±± 0.20.21616 ±± 88mEq Na+/hmEq Na+/h 29 29 ±± 1717 16 16 ±± 88
mEq Na+/L fluidmEq Na+/L fluid *44 *44 ±± 2424 28 28 ±± 1212% CHO% CHO 82 82 ±± 1111 88 88 ±± 1010
% Fat% Fat
% P t i% P t i
12 12 ±± 88
77 ±± 44
6 6 ±± 66
55 ±± 66% Protein% Protein 7 7 ±± 44 5 5 ±± 66Stuempfle KJ et al JACN 2011
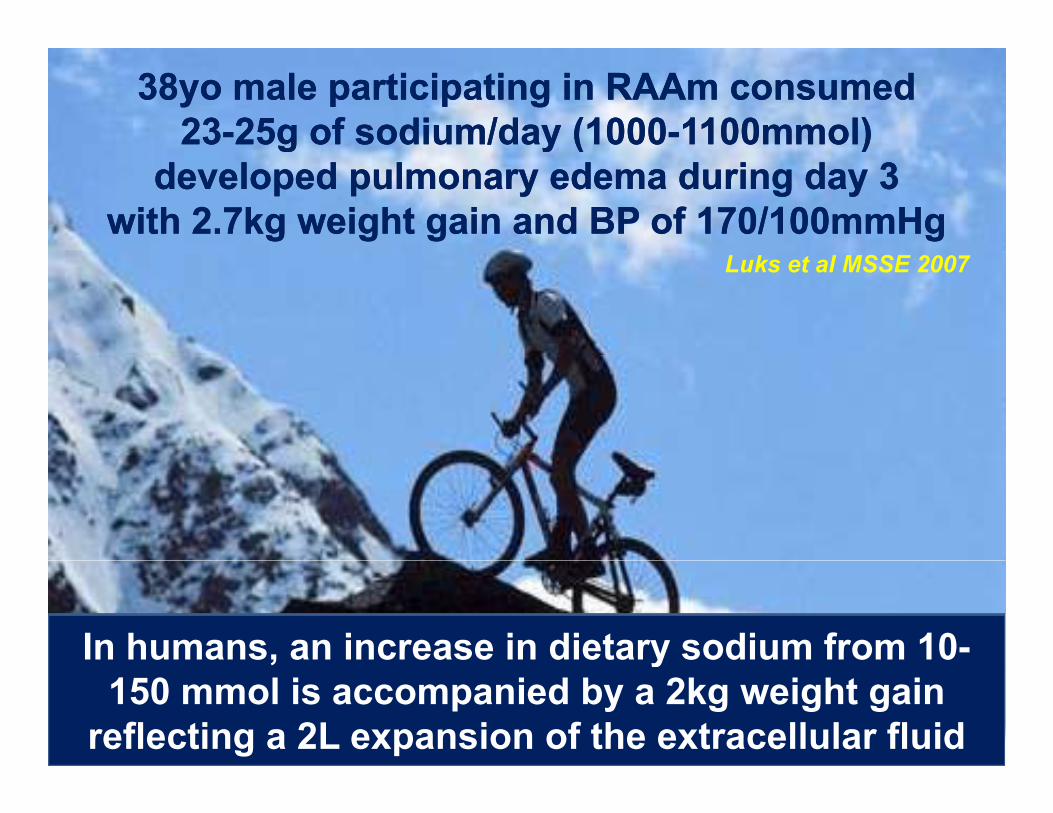
38yo male participating in 38yo male participating in RAAmRAAm consumed consumed 2323--25g of sodium/day (100025g of sodium/day (1000--1100mmol)1100mmol)g y (g y ( ))
developed pulmonary edema during day 3developed pulmonary edema during day 3with 2.7kg weight gain and BP of 170/100mmHgwith 2.7kg weight gain and BP of 170/100mmHg
Luks et al MSSE 2007
In humans, an increase in dietary sodium from 10-, y150 mmol is accompanied by a 2kg weight gain
reflecting a 2L expansion of the extracellular fluid
Salt Supplementation:Salt Supplementation:
↑ weight gain↑ g g↑ Tc↑
↑Heart ratehypervolemic effects on
respiration?respiration?performance?
Konikoff F et al Biomed and Pharmacol1986
hypervolemic normonatremia?
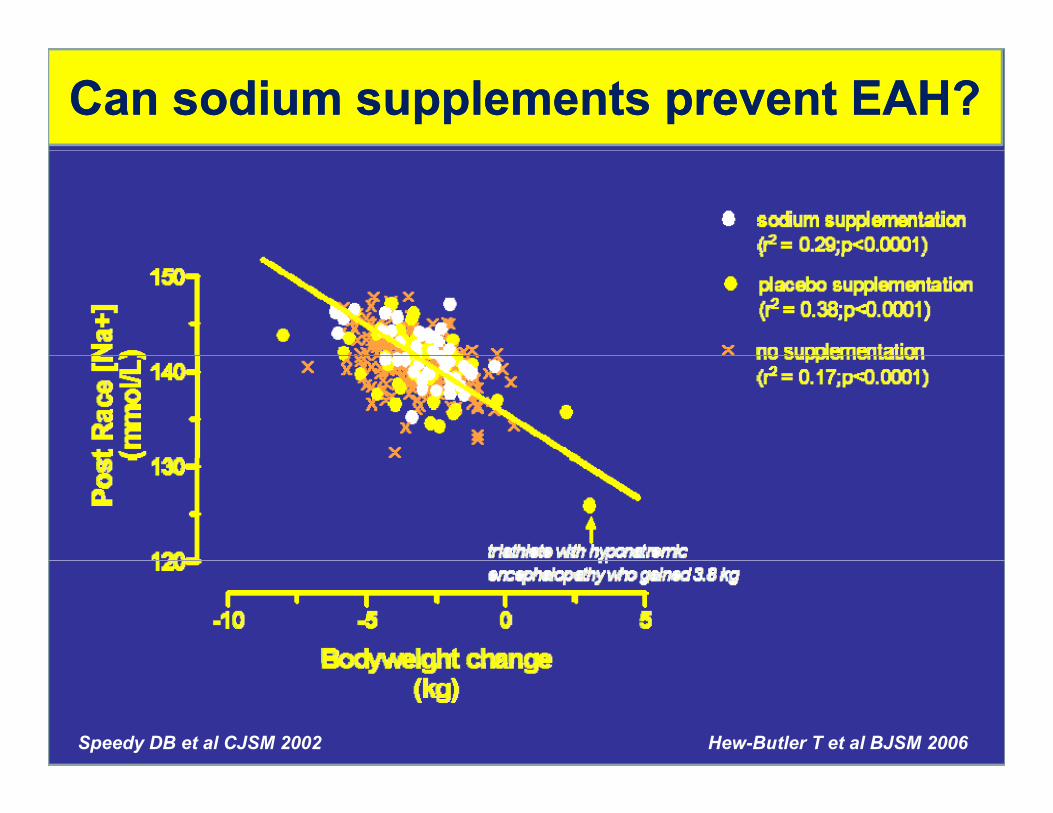
Can sodium supplements prevent EAH?Can sodium supplements prevent EAH?
Hew-Butler T et al BJSM 2006Speedy DB et al CJSM 2002

13 females running 3 hours ingesting 1L/h of high (680mg/L), low (410mg/L) or no sodium beverages
VARIABLE HIGH LOW WATERPre-run [Na+]p
(mmol/L)
Post-run [Na+]p
137.3 (1.2)
134 8 (2 5)
137.2 (1.2)
132 8 (1 7)
137.5 (1.6)
131 3 (1 7)*Post run [Na+]p(mmol/L)
∆ [Na+]p(mmol/L)
134.8 (2.5)
-2.5 (2.5)
132.8 (1.7)
-4.4 (2.5)
131.3 (1.7)*
-6.2 (2.1)*(mmol/L)
∆ Body weight(kg)
( )
2.1 (1)
( )
1.8 (1.2)
( )
1.9 (1.9)
Performance(km) 39.9 (4.3) 42.0 (4.8) 40.6 (5.2)
adapted from Twerenbold R et al, BJSM 2003

Summary: Sodium IntakeSummary: Sodium Intake
Sweat sodium losses appear to beSweat sodium losses appear to be regulated during exercise
Electrolyte beverages may attenuateblood [Na+] decline when fluid intakeblood [Na+] decline when fluid intake
matches or exceeds body mass losses
Hot weather and long duration exerciseincreases the need for sodium

HyponatremiaHyponatremia
RhabdomyolysisRhabdomyolysis & Renal Failure& Renal FailureRhabdomyolysisRhabdomyolysis & Renal Failure& Renal Failure
Fluid IntakeFluid Intake
Sodium IntakeSodium IntakeSodium IntakeSodium Intake
RecommendationsRecommendations

Fluid and sodium balanceFluid and sodium balanceFluid and sodium balanceFluid and sodium balanceare highly regulatedare highly regulatedg y gg y gthrough redundant, through redundant,
evolutionarily conserved, evolutionarily conserved, physiological mechanismsphysiological mechanismsphysiological mechanismsphysiological mechanisms
aimed to protect aimed to protect ppplasma sodium/osmolalityplasma sodium/osmolalityduring and after exercise during and after exercise

RecommendationsRecommendationsUse body weight as aUse body weight as a guideguide not a rulenot a ruleUse body weight as a Use body weight as a guideguide not a rulenot a rule
Drink to thirstDrink to thirstDrink to thirstDrink to thirstSalt to tasteSalt to tasteSalt to tasteSalt to taste
particularly in hot weather and unparticularly in hot weather and un--acclimatizedacclimatizedsalt may attenuate development of EAH but doessalt may attenuate development of EAH but doesy py p
NOT PREVENT ITNOT PREVENT IT
Listen to o r bodListen to o r bodListen to your bodyListen to your body
CONCLUSIONCONCLUSIONCONCLUSIONCONCLUSIONEAH, EAH, rhabdomyolysisrhabdomyolysis and acute renal failureand acute renal failurey yy y
are more common in are more common in ultrarunnersultrarunners..
Alth h lifAlth h lif th t ith t iAlthough lifeAlthough life--threatening threatening consequences are rare (<1%), consequences are rare (<1%),
thethe ↑↑risk forrisk for ltrar nnersltrar nners nderscoresnderscoresthe the ↑↑risk for risk for ultrarunnersultrarunners underscores underscores the importance of maintaining water and the importance of maintaining water and
sodium homeostasis during exercisesodium homeostasis during exercisesodium homeostasis during exercisesodium homeostasis during exerciseby by abidingabiding rather than outsmartingrather than outsmartingthe body’s regulatory mechanismsthe body’s regulatory mechanismsthe body’s regulatory mechanismsthe body’s regulatory mechanisms

ThankThank--youyouyyGGood luckood luckGGood luckood luck
EEnjoy the racenjoy the raceEEnjoy the racenjoy the race