goiter
TRANSCRIPT

SMS 2023SMS 2023
Dr. Mohanad R. A lwanDr. Mohanad R. A lwan
GoiterGoiter

TSH• Produced by Adenohypophysis Thyrotrophs• Upregulated by TRH • Downregulated by T4, T3
• Stimulates several processes• Iodine uptake• Colloid endocytosis• Growth of thyroid gland

Thyroid Hormone
Majority of circulating hormone is T4 98.5% T4 1.5% T3
Total Hormone load is influenced by serum binding proteins Albumin 15% Thyroid Binding Globulin 70% Transthyretin 10%
Regulation is based on the free component of thyroid hormone
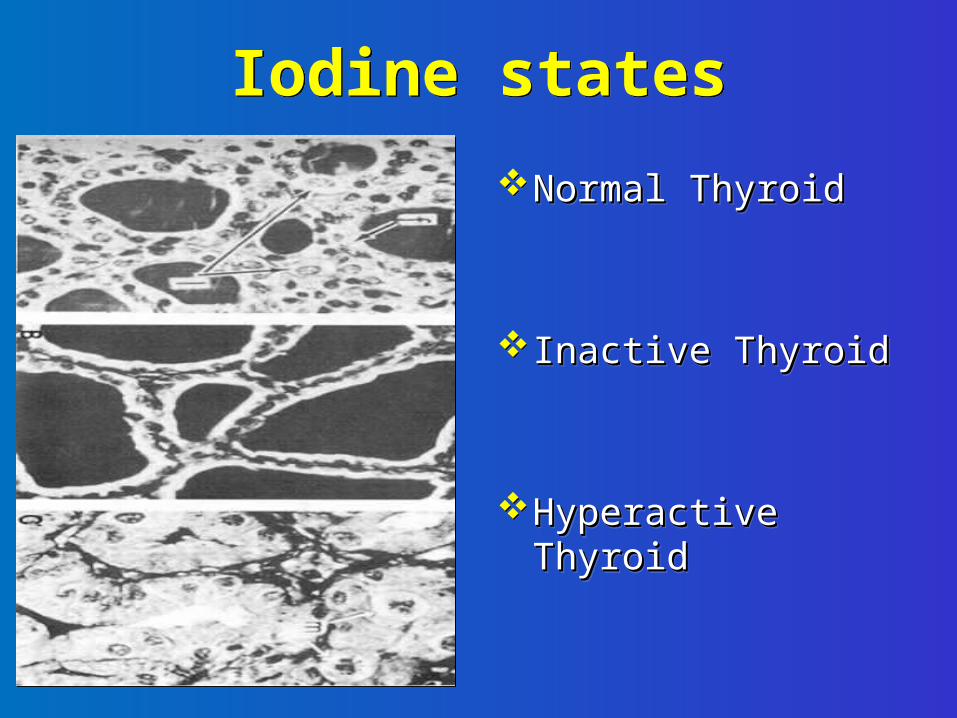
Iodine statesNormal ThyroidNormal Thyroid
Inactive ThyroidInactive Thyroid
Hyperactive ThyroidHyperactive Thyroid

Iodine deficiency
Iodine deficiency most common cause of goiter & hypothyroidism worldwide
Effect of I deficiency aggravated by goitrogens foods, with anti-thyroid properties (Africa, South America)

Goitrogens

Clinical Expression of Iodine Deficiency
• Miscarriages• Stillbirths• Neurological
cretinism• Impaired
intellectual function
• Increased perinatal mortality
• Increased infant mortality
• Neonatal goiter• Cretinism• Impaired
intellectual function
FetusNeonate
Clinical Expression of Iodine Deficiency
• Goiter• Hypothyroidism• Impaired
intellectual function
• Retarded physical development
• Goiter• Hypothyroidism
and poor intellectual and physical performance
Child & adolescent Adult

* Definition: Non-inflammatory, non-neoplastic
enlargement of the thyroid gland.
GOITERS

GoiterEtiology
Diet: Iodine deficiency Brassica (cabbage, turnips, cauliflower, broccoli)
Hashimoto’s thyroiditis Early stages only, late stages show atrophic
changesMay present with hypo, hyper, or euthyroid states
Graves’ diseaseDue to chronic stimulation of TSH receptor
Chronic Iodine excessIodine excess leads to increased colloid formation
and can prevent hormone releaseMedications
Immunosuppressants, antiretrovirals, heart drug prevents release of hormone, causes goiter in 6% of chronic users

Goiter Classification Goiter: Chronic enlargement of the thyroid
gland not due to neoplasm• Endemic goiter
• Areas where > 5% of children 6-12 years of age have goiter
• Common in China and central Africa• Sporadic goiter
• Areas where < 5% of children 6-12 years of age have goiter
• Familial

Morphology Classification Regarding morphology, goiters may be classified either as the growth pattern or as the size of the growth:•Growth pattern •1. Uninodular (struma uninodosa) - can be either inactive or a toxic nodule•2. Multinodular (struma nodosa) - can likewise be inactive or toxic, the latter called toxic multinodular goiter•3. Diffuse (struma diffuse), with the whole thyroid appearing to be enlarged.•Size Class I - palpation struma - in normal posture of the head, it cannot be seen; it is only found by palpation.•Class II - the struma is palpative and can be easily seen.•Class III - the struma is very large and is retrosternal; pressure results in compression marks.

* Pathogenesis:a. Parenchymatous goiter:•Iodine deficiency → decreased thyroid hormone synthesis → increases TSH secretion → thyroid glands hyperplasia.•The acini are increased in number and lined by tall columnar cells and contain little colloid.•If iodine deficiency is corrected after a short time, the acini return to the normal state.
DIFFUSE NONTOXIC (SIMPLE) GOITER
GROSS Diffuse symmetrical
enlargement of the gland
SIZE: Rarely exceeds 100-150gm
C/S: Brown, glassy, translucent
MICROSCOPYFollicles lined by low cuboidal or flattened epithelial cellsAbundant colloid during involution

DIFFUSE NONTOXIC (SIMPLE) GOITER
CLINICAL FEATURES:Majority: EuthyroidMass effect

Multinodular Goiter (MNG)
• MNG is an enlarged thyroid gland containing multiple nodules– The thyroid gland becomes more nodular with
increasing age– In MNG, nodules typically vary in size
• MNG may be toxic or nontoxic– Toxic MNG occurs when multiple sites of autonomous
nodule hyperfunction develop, resulting in THYROTOXICOSIS– Toxic MNG is more common in the elderly

Toxic Multinodular Goiter
• Asymmetric enlargement
• Multinodular• Haemorrhage• Calcification• Fibrosis• Cystic degeneration

Toxic Multinodular Goiter
• Numerous follicles varying in size
• Recent haemorrhage• Haemosiderin • Calcification• Cystic degeneration• +/- dominant nodule

TMNG and Graves
Huge Toxic MNG Diffuse Graves Thyroid

MICROSCOPY
Colloid rich follicles lined by low cuboidal to flattened cells Fibrous bands Hemorrhage Calcification


Toxic Multinodular Goiter (TMG)

Grade IV Toxic MNG
Huge Toxic MNG Huge Toxic MNG

Clinical Manifestations
• If thyroid function is preserved, most goiters are asymptomatic
• If the thyroid is markedly enlarged, it can
cause tracheal or esophageal compression

•Swollen front of the neck
•Protruding (popping out) eyes
•A tight feeling in the throat
•Coughing
•Difficulty in swallowing & breathing

• Substernal goiter – May obstruct the thoracic inlet– Respiratory flow measurements and CT or MRI
should be used to evaluate substernal goiter in patients with obstructive signs or symptoms
• Pemberton's sign – Symptoms of faintness with evidence of facial
congestion and external jugular venous obstruction when the arms are raised above the head, a maneuver that draws the thyroid into the thoracic inlet

Symptoms also include:•Fatigue•Frequent bowel movements•Heat intolerance•Increased appetite•Increased sweating•Menstrual irregularities (in women)•Muscle cramps•Nervousness•Restlessness•Weight loss

• Symmetrically enlarged, nontender, generally soft gland without palpable nodules

Enlargement
• 0 – the gland is not palpated• I – some part of the gland can be palpated• II- the gland can be seen although the neck is in a
normal shape• III – shape of the neck is being changed• IV – configuration of the neck is being changed• V – an giant goiter with complications

Thyroid Evaluation
TRHTSHTotal T3, T4
Free T3, T4
ThyroglobulinAntibodies: Anti-TPO, Anti-TSHr

Treatment Options
1. Symptom relief medications
2. Anti Thyroid Drugs – ATD Methimazole, Carbimazole Propylthiouracil (PTU)
3. Radio Active Iodine treatment – RAI Rx.
4. Thyroidectomy – Subtotal or Total
5. NSAIDs and Corticosteroids – for SAT

•The use of iodized table salt •Avoid goiter promoting foods such as cabbage, Brussels sprouts, & soy•Thyroid Replacement Therapy•Thyroidectomy- surgery to remove part or all of the thyroid.


Complications
• Heart complications:• Atrial fibrillation• Congestive heart failure• Rapid heart rate• Superior vena cava obstruction• Other complications:• Bone loss leading to Osteoporosis
Questions???