gonzalez-the role of surgery for stage iv cancer surgery and the role of surgery for stage iv cancer...
TRANSCRIPT
Palliative Surgery and the Role of Surgery for Stage IV Cancer
Ricardo J. Gonzalez, MDAssistant Professor of Surgery
University of Colorado

Objectives• Discuss the classic management of advanced disease• Define palliation and palliative surgery• Review literature on palliative surgery and metastectomy
• Make sense of anecdote and logical conjecture by employing well-characterized information for specific patient groups in difficult situations
– “We want actual not virtual data” AH Harken 6am lab mtng 2000

“In the field of surgical oncology tumor biology is king, patient selection is queen, and technical maneuvers are the prince and princess who try, but usually fail, to usurp the throne.”
Cady Arch Surg 1997

Advanced/Incurable disease
• Classic teaching– Chemotherapy is the treatment of choice– Radiation only for symptomatic lesions– Cure or even long-term progression free
survival is not likely

Advanced/Incurable disease
• Arguments against surgery– Survival is driven by the rate and volume of
metastatic burden– Unhealthy patients that can’t tolerate surgery
• Risk benefit ratio is heavily weighted toward the risks
– Theoretical risk of “angering the tumor” or “letting the air in”
• Elaboration of VEGF or other angiogenic factors from anesthesia, surgical stress, blood transfusion and various other unknowns
Advanced/Incurable disease
• Arguments for surgery– Improving quality of life and symptom control– Debulking gives chemotherapy a fighting chance– Alter the metastatic cascade
• removing the primary tumor• removing the metastases
– Removing the inhibitory peptides/molecules that depress the local immune response to the tumor enhancing the anti-tumor immunity to the remaining tumor cells
Surgery and metastatic disease
• Must decide and discuss the goals early • What are the goals?
1. Palliation – symptoms/QOL2. Improve upon progression-free survival3. End of life goals met with surgery4. Curative intent
Is this really that important?• Cancer is the 2nd most common cause of death
(1/3 diagnosed and 1/3 die)
• End of life care consumes 12% of national health care expenditure and 27% of Medicare expenditures.
• 12.5 % of surgical procedures are for palliative reasons
Krouse Arch Surg 2001

What’s Needed?• Miner et al Am J Surg 1999 348 publications
– primarily focused on morbidity and mortality, while only 12% of studies considered pain relief, 2% considered cost, and 17% evaluated QOL.
– Curative surgery is based on robust data and evidenced-based decision making; palliative surgery is not.
• What’s needed: 1. Better define palliative surgery2. Study more meaningful end results and establish
standards for which logical and thoughtful decisions can be made
Krouse Arch Surg 2001
Palliation• Relieve symptoms for patients beyond cure when non-
surgical measures are not feasible, not effective, or not expedient
• Palliation means patient should be better at the completion of the procedure or treatment
“It is axiomatic that one cannot palliatively improve an asymptomatic patient using a scalpel.”– R. G. Martin, 1982

Palliative Care – Evolution - Early
Quotes from a palliative care doctor• “We are not team death”• “We are not a death squad”
Quotes from those who do not understand palliative care
• “Here come the grim reapers”• “Oh here they come dressed in black”• “They’ll just drug ‘em with morphine”• “If he’s not comatose now just give them a shot at him”

The Surgical Treatment of Cancer: A Comparison of Resource Utilization following Procedures Performed with Curative and Palliative Intent
Purpose - evaluate the immediate and short term resource utilization needs of patients undergoing surgical intervention with curative or palliative intent.
Methods - 302 pts identified as palliative (58) or curative (244) and followed for 6 months
Findings• Avg # of patient encounters no different
– Patients undergoing surgery for palliative intent require equal resources
• Character of resources is different:– palliative patients admitted for symptom control and had
fewer hospital free days – curative intent utilized services directed at their continued
treatment. Cullinane CA Cancer 2003
Resource utilization for ovarian cancer patients at the end of life: How much is too much?
Aim: compared hospital vs. hospice based costs during last 60 days of life for ovarian cancer patients
• Billing records were analyzed for inpatient and outpatient costs.
Lewin SN Gyn Oncol 2005
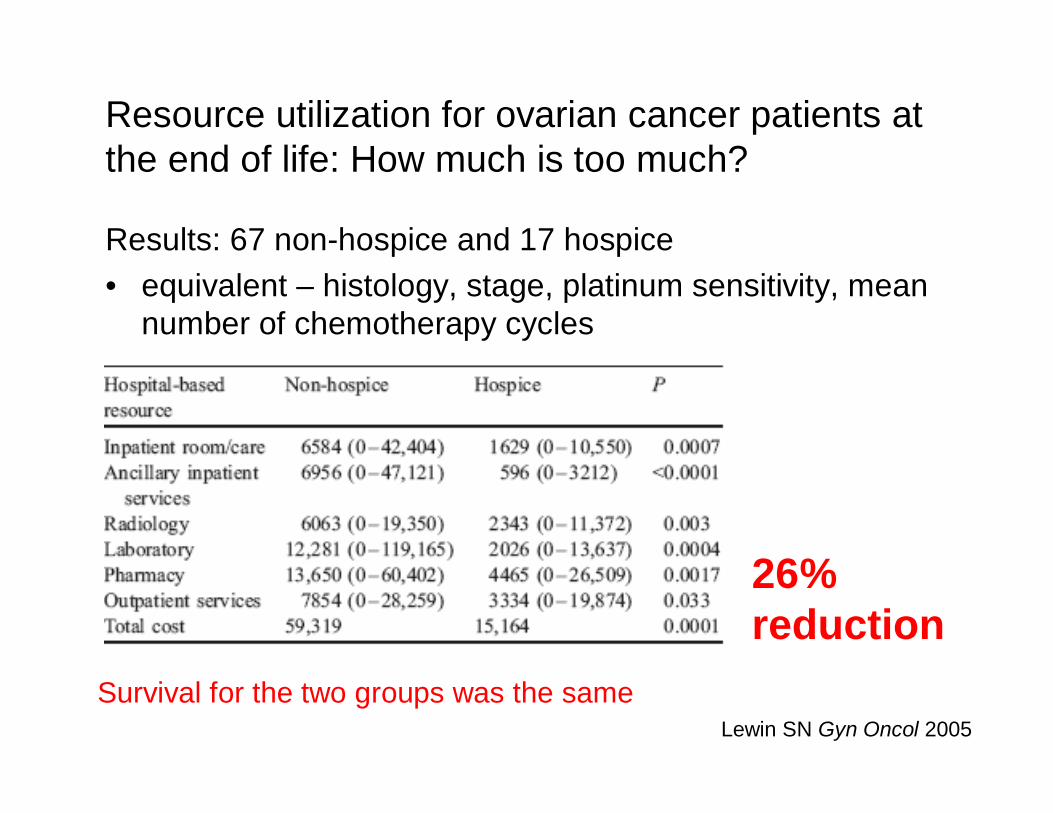
Resource utilization for ovarian cancer patients at the end of life: How much is too much?
Results: 67 non-hospice and 17 hospice• equivalent – histology, stage, platinum sensitivity, mean
number of chemotherapy cycles
Lewin SN Gyn Oncol 2005
26% reduction
Survival for the two groups was the same
Palliative Care – Evolution - Today• Establish the patients’ goals
and personalize therapy based upon those goals
• Symptom control for long term pain management in terminal patients
• Helping the family and the patient cope with and accept the situation
• Help achieve fullness of life
• Reduces end of life health care costs by 25-40%
“Mobile Happy Hour”

Palliative Care – Evolution - Today
• Have far-reaching effects outside what you see in the hospital
• Should be involved earlier and with increasing responsibility during the treatment of patients with incurable cancers
When to involve the Palliative Care Team:
1. When your attending gives you the OK
2. When the labor of symptom control outstrips the teams resources or understanding
3. Difficult social or psychological situation
Palliative Surgery
Surgeon’s role: 1. initial evaluation of the disease 2. local control 3. control of discharge and hemorrhage 4. control of pain 5. reconstruction and rehabilitation
Early stage disease
Risk
Benefit
Metastectomy/Palliative Surgery
Risk Benefit

Palliative Surgery-Defined• Primary goal is improving symptoms
caused by advanced malignancy• Effectiveness – presence and durability of
patient-acknowledged symptom resolution• Successful:
1. improvement in QOL2. minimal morbidity and mortality3. modest resource utilization
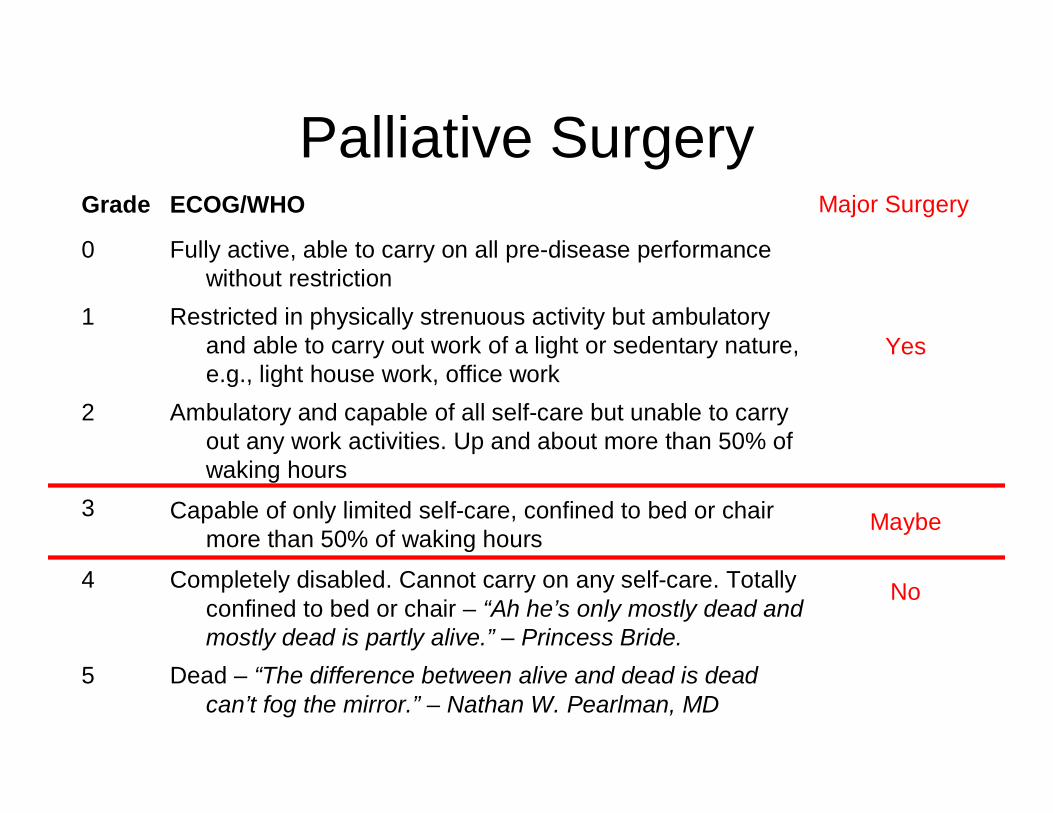
Palliative Surgery
Dead – “The difference between alive and dead is dead can’t fog the mirror.” – Nathan W. Pearlman, MD
5
Completely disabled. Cannot carry on any self-care. Totally confined to bed or chair – “Ah he’s only mostly dead and mostly dead is partly alive.” – Princess Bride.
4
Capable of only limited self-care, confined to bed or chair more than 50% of waking hours
3
Ambulatory and capable of all self-care but unable to carry out any work activities. Up and about more than 50% of waking hours
2
Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light house work, office work
1
Fully active, able to carry on all pre-disease performance without restriction
0
ECOG/WHOGrade Major Surgery
No
Maybe
Yes
• The goal:– “to prospectively follow all patients undergoing
a palliative operative or endoscopic procedure during a one year period to obtain some of the data that are required to guide sound clinical decisions and allow more adequate patient counseling.”
Miner Ann Surg 2004
A Prospective, Symptom Related, Outcomes Analysis of 1022 Palliative Procedures for advanced Cancer

A Prospective, Symptom Related, Outcomes Analysis of 1022 Palliative Procedures for advanced Cancer
• Results: – 823 initial procedures– 109 for recurrence– 90 for new sx’s.– Overall mortality – 11%– Overall morbidity – 40%
• 70% operative vs. 30% endoscopic– no difference in sx resolution– Morbidity:
39% vs. 18%, (p<0.001)– Mortality:
9% vs. 15%, (p=0.017)
• Documented improvement in 80%– Median 135 days– Complication vs. none:
67% vs. 89%, (p<0.001)– High grade complication
reduced reported symptom control to 17%
• No benefit 20%– Died due to complications or
progression– Further palliation required for
chief complaint – No documentation in the
medical record
Miner Ann Surg 2004

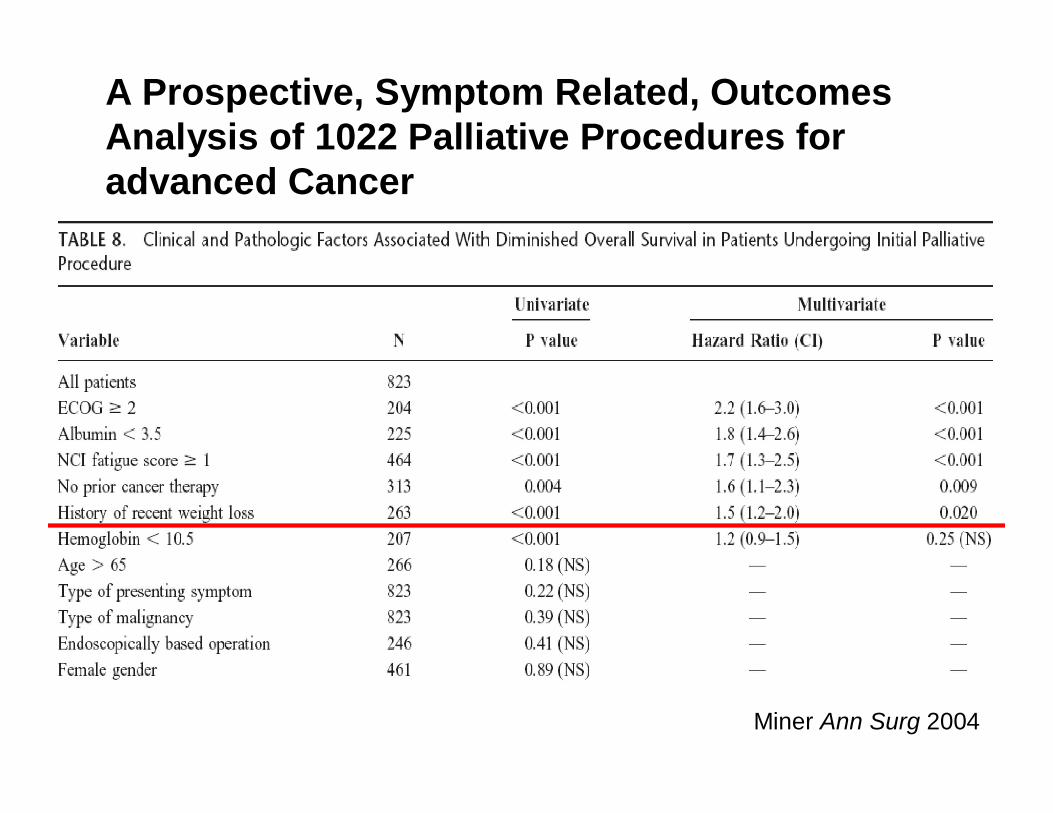
A Prospective, Symptom Related, Outcomes Analysis of 1022 Palliative Procedures for advanced Cancer
Miner Ann Surg 2004
Palliative procedure to control symptoms or improve QOL
823 patients
Improved Symptoms
80% (659/823)
No Improvement
20% (164/823)
Symptom Free
46% (303/659)
Median 135 days
Additional Symptoms
29% (191/659)
Median 58 days
Recurrent Symptoms
25% (165/659)
Median 52 days
A Prospective, Symptom Related, Outcomes Analysis of 1022 Palliative Procedures for advanced Cancer
Miner Ann Surg 2004

A Prospective, Symptom Related, Outcomes Analysis of 1022 Palliative Procedures for advanced Cancer
• Conclusions– In select patients palliation can be expected– Durability of symptom control may be limited
by the development of new symptoms– Potential benefit may be limited by poor
performance, malnutrition, and no prior cancer treatment
Miner Ann Surg 2004
Palliative Surgery• Miner TJ et al Defining
Palliative Surgery in Patients Receiving Noncurative Resections for Gastric Cancer. JACS2004
• Miner TJ et al Symptom Control in Patients With Locally Recurrent Rectal Cancer. Ann Surg Oncol2003
• Similar findings– Palliation is achievable with
great success– Durability of palliation is
short due to development of new symptoms
– Age, gross residual disease, pain and recurrence of local disease (rectal) were predictors of shortened symptom control

Case Vignettes
• “If all you ever do is discuss your successes and not your failures then you’ll never get anything out if this job.”
• “A man’s errors are his portals of discovery.”
Nathan W. Pearlman, MD
James Joyce

Palliative Surgery
• 55 yo male with RLE 1.3 mm melanoma. SNBx (-) in 2002. • Hx of recurrences every year until he developed visceral mets. • Multiple clinical trials • Worsening left upper back pain, insomnia, and early satiety. ECOG 0• OR – left adrenalectomy, known liver and pelvic nodes left behind. • Home in 5 days. No pain, eating well and can sleep.
4 mos!!
Palliative Surgery
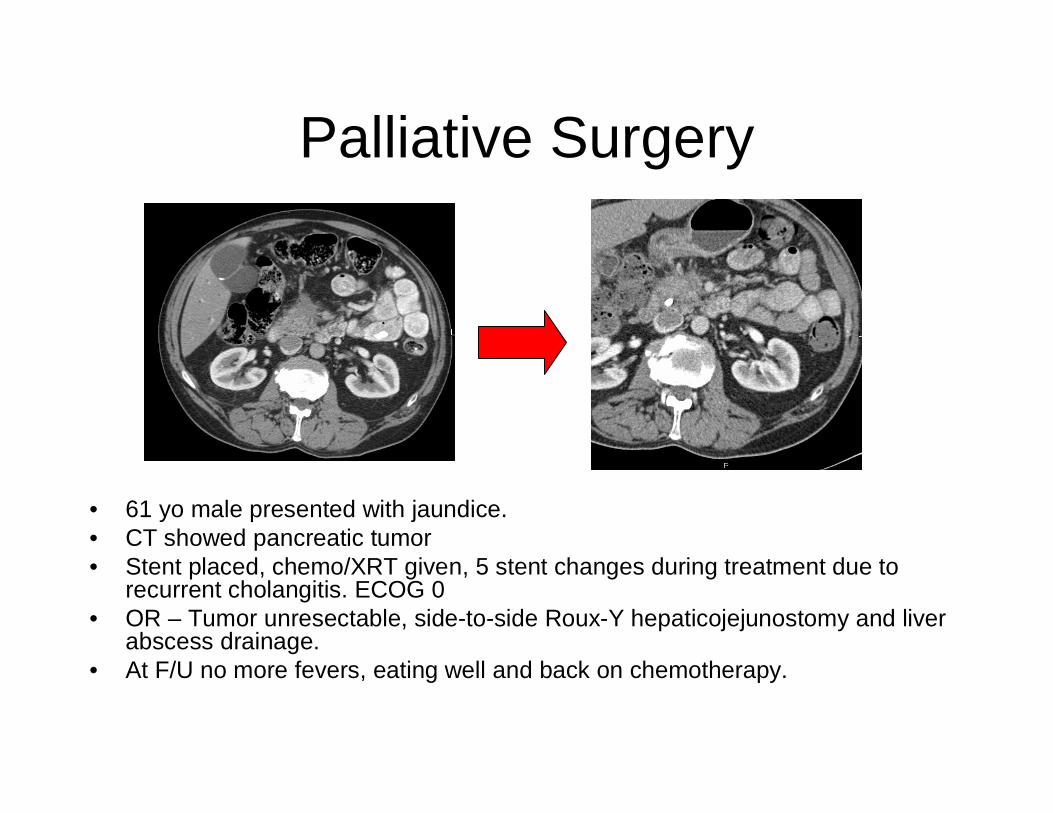
• 61 yo male presented with jaundice.• CT showed pancreatic tumor• Stent placed, chemo/XRT given, 5 stent changes during treatment due to
recurrent cholangitis. ECOG 0• OR – Tumor unresectable, side-to-side Roux-Y hepaticojejunostomy and liver
abscess drainage.• At F/U no more fevers, eating well and back on chemotherapy.

Palliative Surgery43 yo woman• Colon obstruction and low
volume lung mets. ECOG 3. • OR – Ex lap, en bloc
resection of distal panc, spleen, splenic flexure, left kidney, and diaphragm
• DC home in 2 weeks• 1 mo. later brain mets and
peritoneal recurrence• 3 weeks later died
Would she have done better with a palliative bypass?
“Whenever a man does a thoroughly stupid thing, it is always from the noblest motives.” Oscar Wilde

What about metastatic disease?
Surgery and Metastatic Disease
• Can we alter the natural history of the disease?– Does removing the primary alter progression-free or
overall survival?• Is there any benefit to Stage IV NED?• How do we select patients for surgery and keep
long term survival as our goal? – Two approaches
1. The Pragmatic approach2. The Academic approach

1. Is the patient insured?
2. Is the Oncologist a friend of mine or do I want him to be a friend of mine?
4. Any on-going studies for which I need patients?
7. Is there any patient benefit? (Last consideration)
Patient selection – Pragmatic
3. If not insured then is the patient loaded and will I get an endowed chair?
5. Should I go snowboarding instead of taking this on?
6. Do I need a break from M&M?
1. Do we have a clinical trial in our center?
2. What is this patients performance status?
3. Are there any contraindications based on comorbidities?
4. Do I understand the disease progression for this particular patients tumor prior to considering surgery?
Patient selection – Academic
5. Is there any chance for patient benefit or can I improve upon his symptoms?
(ALWAYS AT THE FOREFRONT OF THE ANALYSIS!!)
“After a while you spend so much time trying to fend off the Grim Reaper you wonder if you’re ever going to win or even why you’ve gotten yourself into this mess.”
Cady Arch Surg 1997
Nathan W. Pearlman on Rounds 2004
“In the field of surgical oncology tumor biology is king, patient selection is queen, and technical maneuvers are the prince and princess who try, but usually fail, to usurp the throne.”
The Pragmatic
The Academic

Stage IV Melanoma
• Sobering statistics– 0.76 – 1.5 mm 25% nodal mets in 3 yrs– 1.5 – 4.0 mm 60% nodal mets in 3 yrs and
15% distant mets in 5yrs• Site of distant recurrence predicts survival
– Nodal 20 – 50% at 5 yrs– Visceral 5% at 5yrs
Balch CM. J Am Acad Dermatol 1980
Stage IV Melanoma
Three criteria cited as predictive of survival after complete metastatic resection – biology is king.
1. The site of metastasis • visceral vs. nonvisceral• visceral pulmonary vs. nonpulmonary
2. The number of metastatic lesions • more is worse
3. The disease-free interval before the development of metastases • more than a year
Allen PJ ASO 2002

Stage IV Melanoma
• Patient selection is queen• 26,204 pts with melanoma• 1,750 (7%)pts with liver mets• 34/1750 (2%) explored (med DFS 58 mos
and 75% solitary mets)– 16 aborted and 18 resected– Of resected 5 (27%) were NED – 0.3% of patients with liver mets!!
Rose DM Arch Surg 2001
Stage IV Melanoma
• Complete resection is the only technical maneuver that potentially alters the natural history of the disease – the princess.
• Prior to proceeding forward with this approach you need a complete staging workup– H&P, labs (LDH), PET/CT scan– brain MRI and bone scan (symptomatic patients)
Stage IV melanoma –skin/soft tissue
• Most common (59%) initial site of distant recurrence is skin, subcutaneous tissue and regional nodes.
• Complete resection– Median survival as high as 50 months– 5 year overall survival of 38%
• DFI has highest predictive value with best prognosis if >18 months after primary resection.
• Surgical palliation is strongly encouraged because it is easily accomplished with minimal morbidity.
Balch J Clin Oncol 1983 Allen ASO 2002
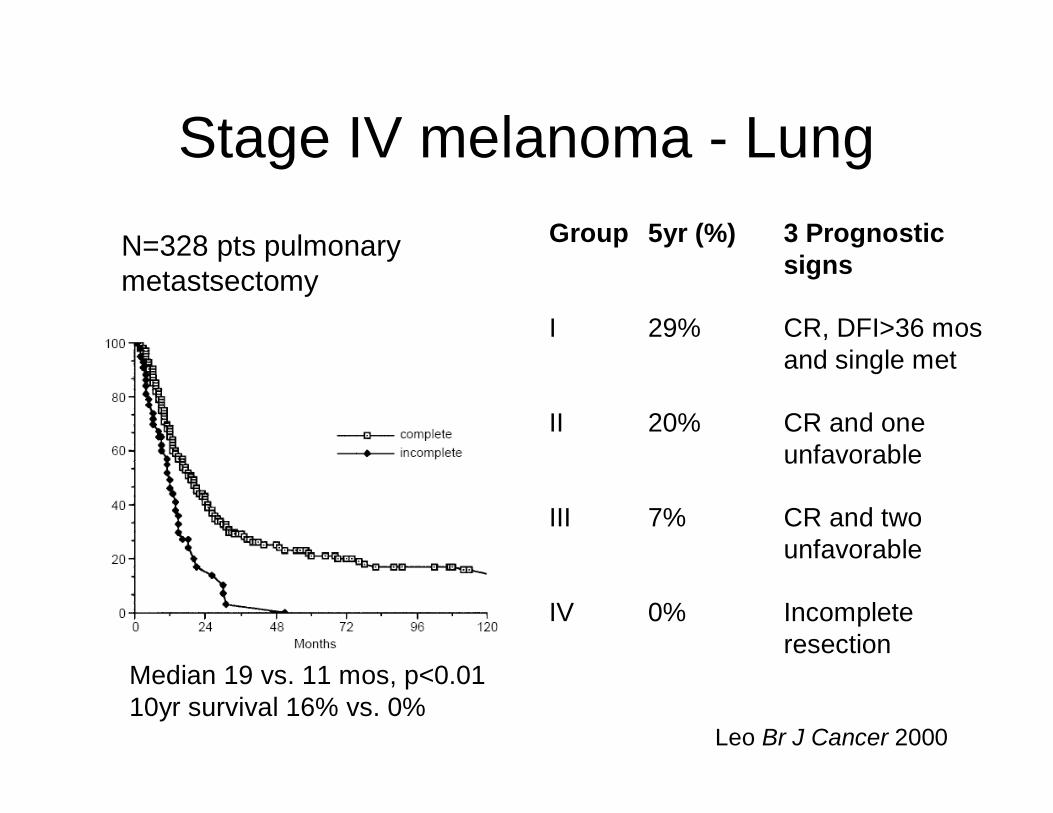
Stage IV melanoma - Lung
Leo Br J Cancer 2000
Median 19 vs. 11 mos, p<0.01 10yr survival 16% vs. 0%
N=328 pts pulmonary metastsectomy
Incomplete resection
0%IV
CR and two unfavorable
7%III
CR and one unfavorable
20%II
CR, DFI>36 mosand single met
29%I
3 Prognostic signs
5yr (%)Group

Stage IV melanoma – GI tract• N=68 pts explored• Anemia 60% and pain
59%
• Group I curative resection
• Group II residual disease
Agrawal S ASO 1999
Curative
Residual disease
Median = 6.9 mos
5 yr = 18%
14.9 vs. 6.9 mosmedian survival
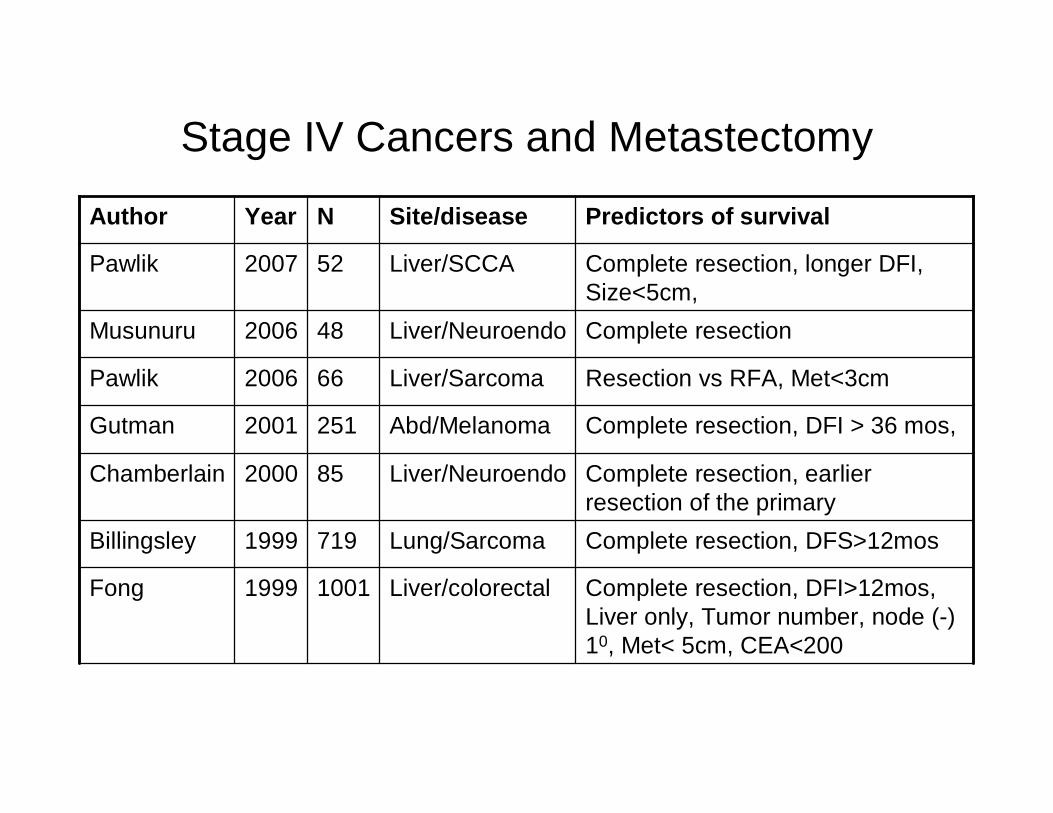
Stage IV Cancers and Metastectomy
Complete resection, longer DFI, Size<5cm,
Liver/SCCA522007Pawlik
Complete resection, DFS>12mosLung/Sarcoma7191999Billingsley
Complete resection, DFI>12mos, Liver only, Tumor number, node (-) 10, Met< 5cm, CEA<200
Liver/colorectal10011999Fong
Complete resection, earlier resection of the primary
Liver/Neuroendo852000Chamberlain
Complete resection, DFI > 36 mos, Abd/Melanoma2512001Gutman
Resection vs RFA, Met<3cm Liver/Sarcoma662006Pawlik
Complete resectionLiver/Neuroendo482006Musunuru
Predictors of survivalSite/diseaseNYearAuthor
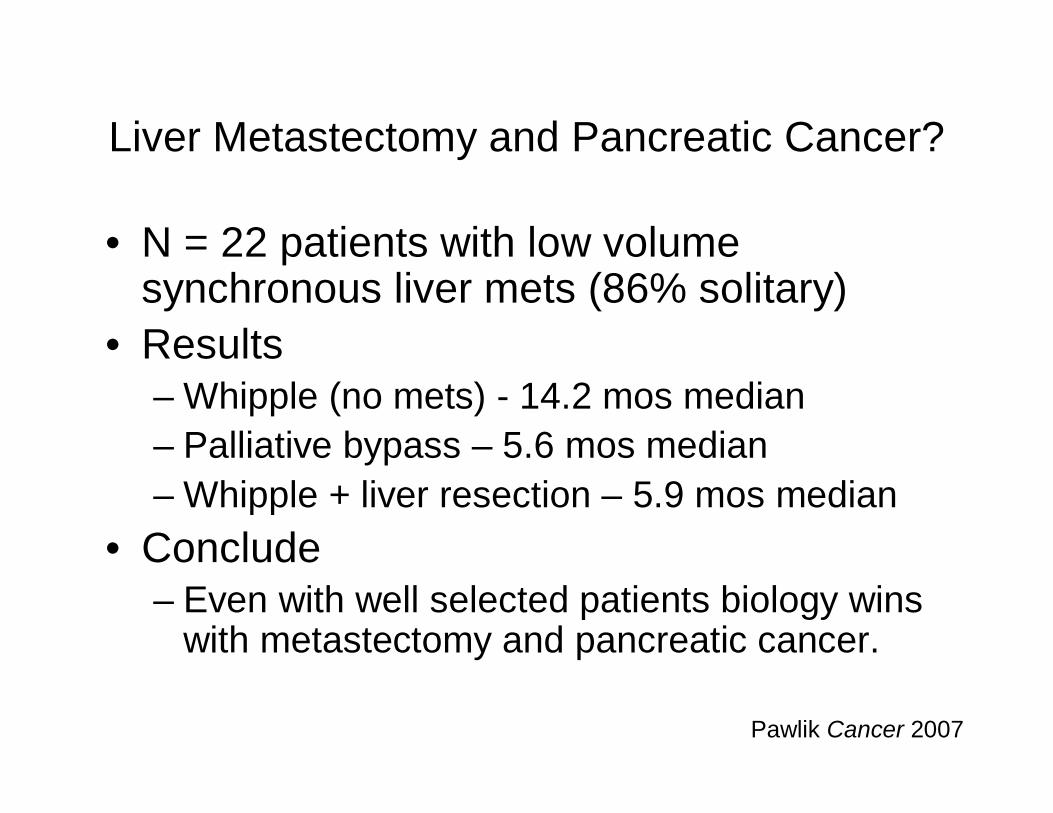
Liver Metastectomy and Pancreatic Cancer?
• N = 22 patients with low volume synchronous liver mets (86% solitary)
• Results – Whipple (no mets) - 14.2 mos median– Palliative bypass – 5.6 mos median– Whipple + liver resection – 5.9 mos median
• Conclude– Even with well selected patients biology wins
with metastectomy and pancreatic cancer.
Pawlik Cancer 2007
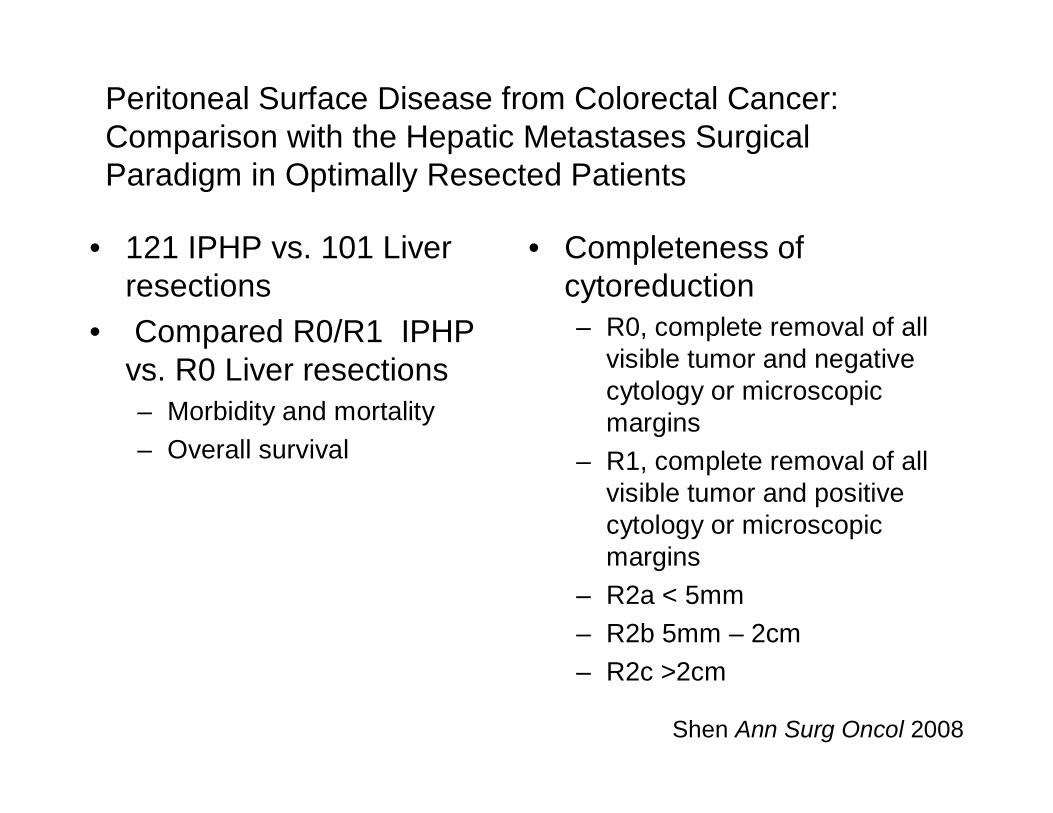
Peritoneal Surface Disease from Colorectal Cancer:Comparison with the Hepatic Metastases Surgical Paradigm in Optimally Resected Patients
• 121 IPHP vs. 101 Liver resections
• Compared R0/R1 IPHP vs. R0 Liver resections– Morbidity and mortality– Overall survival
Shen Ann Surg Oncol 2008
• Completeness of cytoreduction– R0, complete removal of all
visible tumor and negative cytology or microscopic margins
– R1, complete removal of all visible tumor and positive cytology or microscopic margins
– R2a < 5mm– R2b 5mm – 2cm – R2c >2cm

Peritoneal Surface Disease from Colorectal Cancer:Comparison with the Hepatic Metastases Surgical Paradigm in Optimally Resected Patients
• M&M (PSD vs. HM)– 48.1% vs. 33.7% (p=0.38)– 5.5% vs. 4.2% (p=0.71)
• MV predictors– Resection status,
obstruciton, malignant ascites and LOS
Shen Ann Surg Oncol 2008
34 mos41 mos
5yr OS was 26% vs. 34%
Concluded: R0/R1 resection during IPHC compared with margin-negative hepatic resection demonstrated no significant difference in OS and should be considered a viable treatment option.

Surgery and Stage IV Disease: should we remove the primary?
• Yes if– The lesion is symptomatic or will soon become
symptomatic– The disease classically responds to chemotherapy– Patients can live a long time with mets– Removing the lesion can be achieved with low
morbidity
• No if all of the above do not apply

Removing the Primary and Survival
Improves OS (27.1 vs.16.8 mos)
Breast395(242)2008Blanchard
Improves metastatic PFS (p=0.001) and trend toward OS (p=.1)
Breast224(87)2006Babiera
Improves OS(31.9 vs 15.4 mos), not metastatic PFS
Breast409 (187)2007Field
Improves OS (13.2 vs. 5.5 mos)
Gastric105(24)2006Saidi
ConclusionsDiseaseN (resected)
YearAuthor
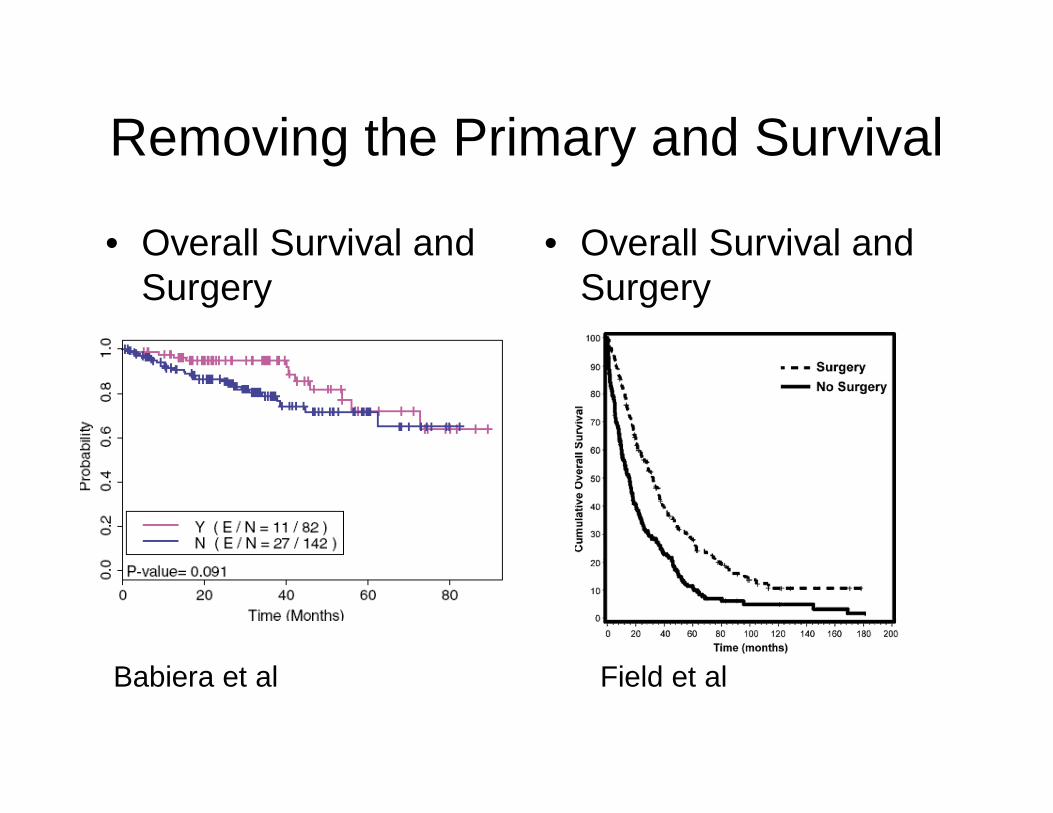
Removing the Primary and Survival
• Overall Survival and Surgery
• Overall Survival and Surgery
Babiera et al Field et al

Removing the Primary and Survival
• Metastatic PFS and Surgery - improved
• Metastatic PFS and Surgery – no difference
Babiera et al Field et al

Do tumor-bearing patients have decreased tumor immunity?
• Multiple hypotheses– immune tolerance of the host to tumor antigens1
– genetic changes in tumor cells that render the tumor cells “immune” to the host’s immune system2-4
– “ignorance”or lack of activation to tumor antigens5
– dysfunction of potentially tumor-reactive lymphocytes rendering them unresponsive to antigen6
– immune suppression mediated by tumor cell secretion of inhibitor factors and/or activation of systemically immunosuppressive cells7,8
1. Pardoll D Ann Rev Immunol 2003
2. Seliger B Immunol Today 2000
3. Marincola FM Adv Immunol 2000
4. Seliger B Semin Cancer Biol 1999
5. Ochsenbein AF Nature 20016. Fink J Immunol Today 19997. Kusmartesev S Cancer Immunol Immunotherapy 20028. Shevach EM Nature Rev Immunol 2002

SummaryGoals should be patient-directed and discussed early
Palliative surgery should be considered after careful patient selection
• Success is determined by: 1. Symptom resolution or improved QOL2. Minimal morbidity and mortality 3. Modest resource utilization
Surgery for stage IV disease can be undertaken with curative intent1. DFI > 12 months 2. Performance status <3 (at least better than “mostly dead”)3. Optimized nutrition 4. Complete resection

Thank you!