good morning!!. common causative agents: procainamide hydralazine penicilliamine (but you can also...
TRANSCRIPT
Good Morning!!
Morning Report
Tuesday, September
13th
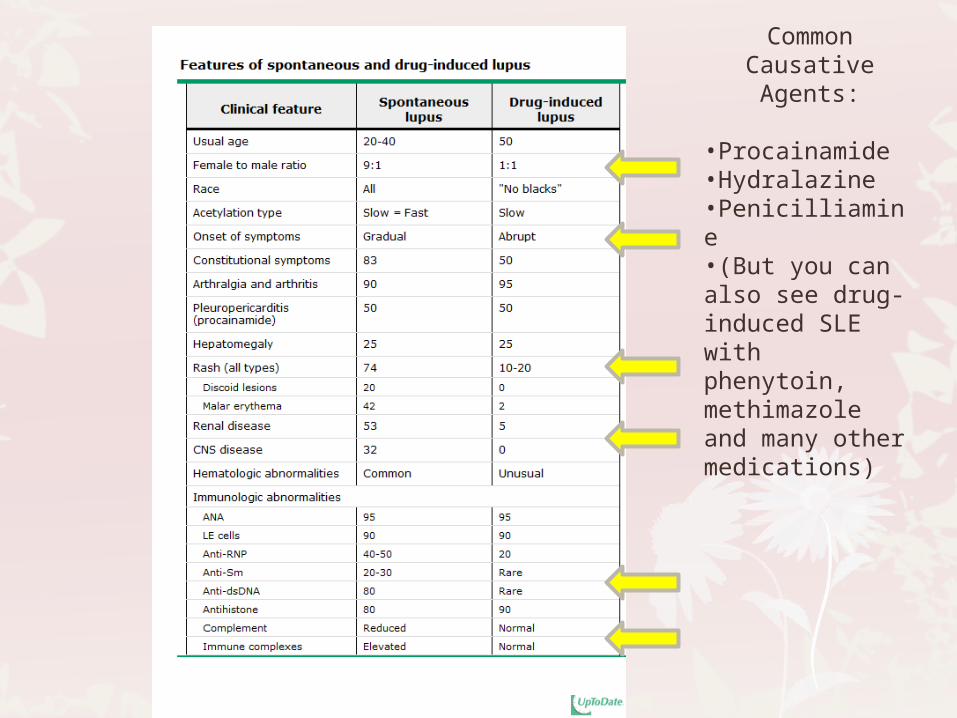
Common Causative Agents:
•Procainamide•Hydralazine•Penicilliamine•(But you can also see drug-induced SLE with phenytoin, methimazole and many other medications)
Hypothyroidism
Congenital Hypothyroidism
Why worry?
T4 is critical to the myelinization of the CNS during the first 3 years after birth
Most preventable cause of potential intellectual disability (so you don’t want to miss it!!!)
Definition
In healthy newborns:
Abrupt rise in TSH within 30-60 mins of delivery stimulates T4 secretion
TSH levels peak early, while T4 levels peak 24-36h after delivery
In premature newborns:
Smaller increases in TSH lower T4 values
Immaturity of the hypothalamic-pituitary axis
Concurrent non-thyroid illnesses
Epidemiology
85% cases sporadic, 15% hereditary (AR)
Incidence 1:4000 infants
More common in Hispanics and Caucasians
More common in females (2:1)
More common in twins
Longer the diagnosis and treatment are delayed, the lower the IQ

*Etiology
Thyroid dysgenesis (most common)
Ectopic thyroid
Thyroid aplasia
Thyroid hypoplasia
Inborn errors of thyroxine synthesis
Defects in thyroid peroxidase activity
Abnormalities in iodine transport
Production of abnormal thyroglobulin
Iodotyrosine deiodinase deficiency
*Etiology (con’t)
Maternal antibody-mediated
Central
Won’t be detected on NBS using TSH screening
Iodine deficiency/ Iodide excess
Transient
Non-thyroid illness (euthyroid-sick syndrome)
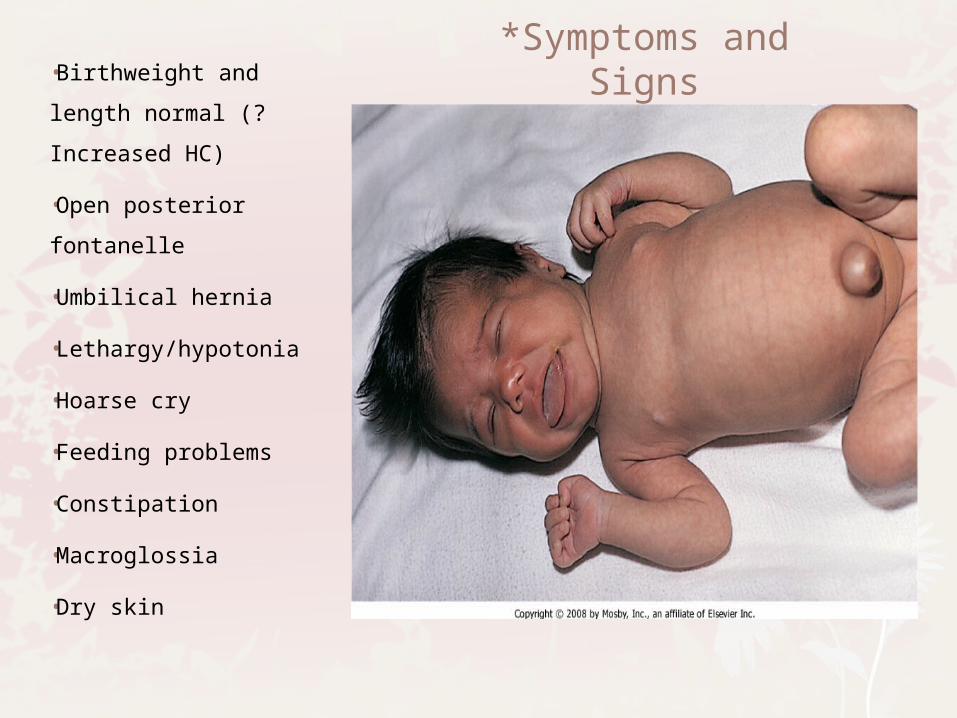
*Symptoms and Signs•Birthweight and
length normal (?
Increased HC)
•Open posterior
fontanelle
•Umbilical hernia
•Lethargy/hypotonia
•Hoarse cry
•Feeding problems
•Constipation
•Macroglossia
•Dry skin
Laboratory TestingNewborn Screen
Most states use initial T4 testing with f/u TSH
Initial labs
Free T4
Total T4
T3
TSH
In all forms of congenital hypothyroidism, serum T4 is low and TSH is elevated, except for central hypothyroidism where both T4 and TSH are low

*Management
Goals are normal growth and good cognitive outcome
Levothyroxine
10-15 mcg/kg/day
50mcg/day recommended for all term and full-sized infants
10-15mcg/kg for preterm infant using the higher range for infants with lower T4
Tablets only
Do not mix with soy formula or any preparation with iron or calcium
*Management (con’t)
Quicker correction is better!
Goal to keep serum TT4 or fT4 in upper half of normal range for age and have normal TSH
Serum T4 (or free T4) and TSH
At 2 and 4 weeks after initiation of therapy
Q1-2 mos during 1st 6 postnatal mos
Q6mos from 6mos-3yrs
Q6-12 mos until growth is complete

*Prognosis
Babies born with congenital hypothyroidism who are appropriately treated within the first 2-6 postnatal weeks grow and develop NORMALLY!
Children who are treated inadequately in the first 2-3 years after birth have IQs below those of unaffected children
6-15 point lower IQ in the severely affected
Even if IQ was not affected, difficulties with gross/fine motor coordination, ataxia, altered muscle tone, strabismus, decreased attention span and speech
Acquired Hypothyroidism
Onset after 6 mo old
Caused by failure of the hypothalamic-pituitary-thyroid axis
Primary: thyroid
Secondary: pituitary
Tertiary: hypothalamus
Epidemiology
Most cases are sporadic
Only 10-15% are inherited
More common in females (2:1)
Hashimoto thyroiditis most common cause
May occur by itself or in association with other AI diseases
Occurs more commonly in patients with Down syndrome or Turner syndrome
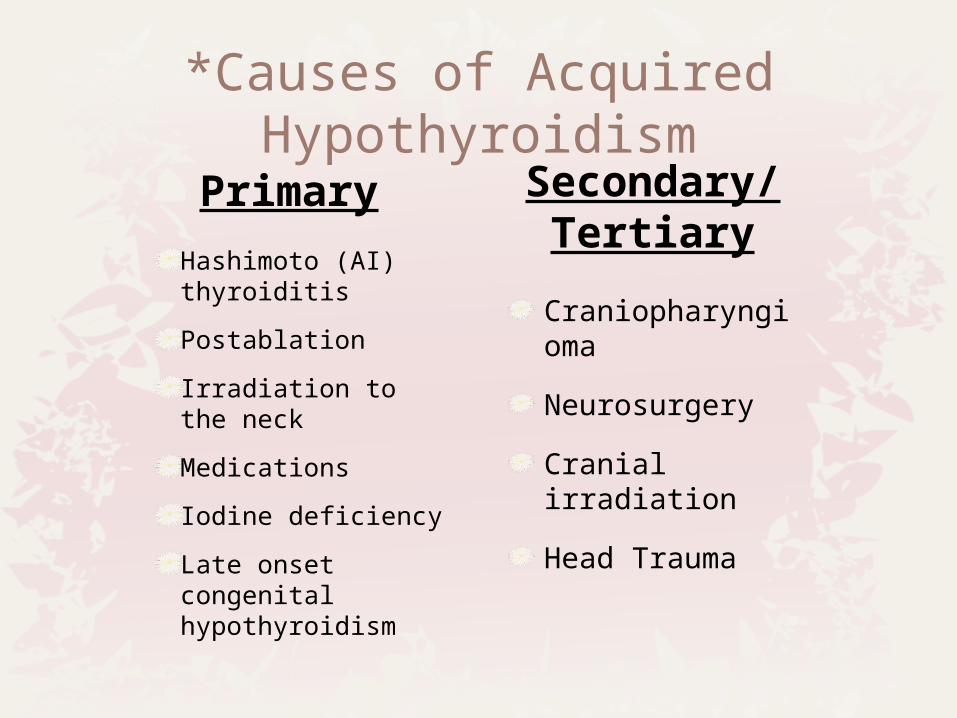
*Causes of Acquired Hypothyroidism
Primary
Hashimoto (AI) thyroiditis
Postablation
Irradiation to the neck
Medications
Iodine deficiency
Late onset congenital hypothyroidism
Secondary/ Tertiary
Craniopharyngioma
Neurosurgery
Cranial irradiation
Head Trauma
*Signs and Symptoms
Decline in linear growth
Fatigue
Constipation
Cold intolerance
Decline in school performance
Weight gain
Irregular menstrual periods
Dry skin
Hair loss

Growth failure
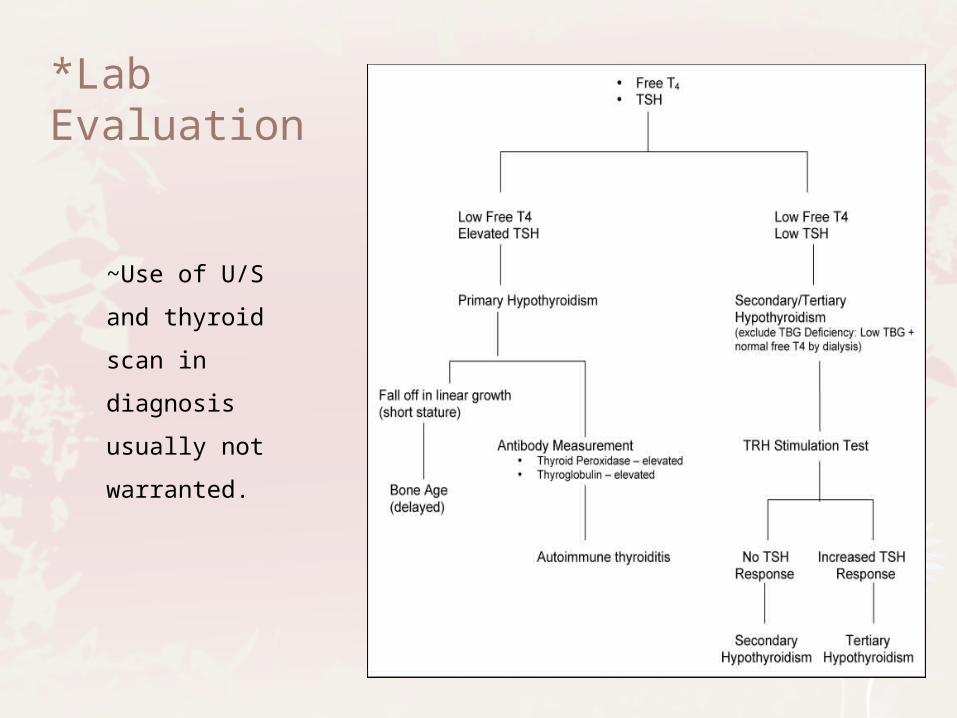
*Lab Evaluation
~Use of U/S and
thyroid scan in
diagnosis
usually not
warranted.
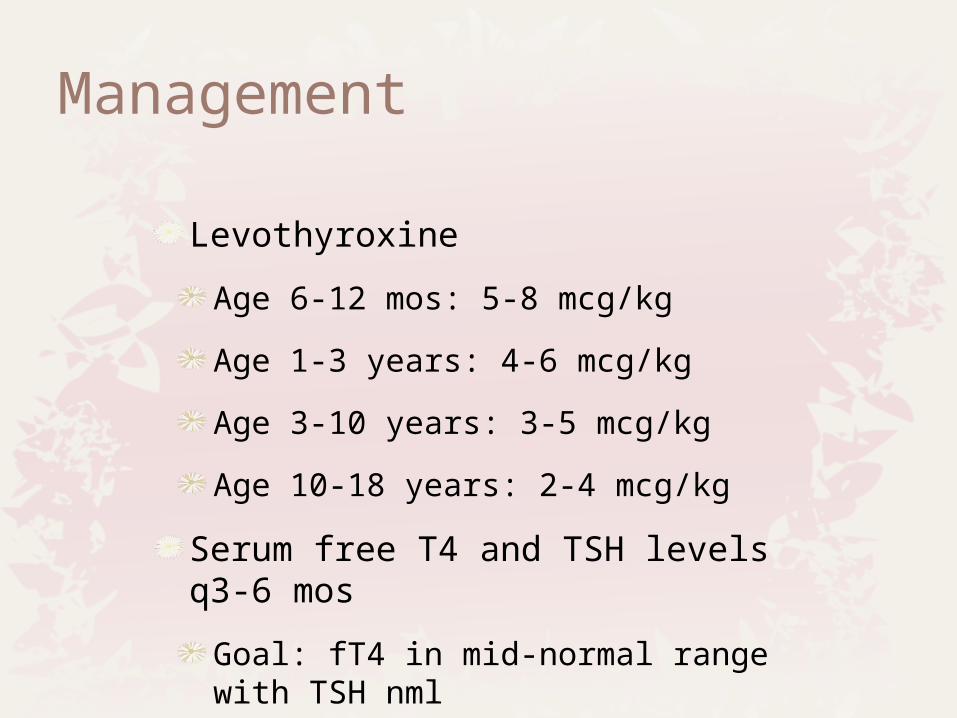
Management
Levothyroxine
Age 6-12 mos: 5-8 mcg/kg
Age 1-3 years: 4-6 mcg/kg
Age 3-10 years: 3-5 mcg/kg
Age 10-18 years: 2-4 mcg/kg
Serum free T4 and TSH levels q3-6 mos
Goal: fT4 in mid-normal range with TSH nml
Prognosis
Growth may not recover if:
Hypothyroidism longstanding
Diagnosed during puberty
Cognitive/ neurologic deficits unlikely if onset is after 2-3 yo
Other entities…Thyroid-binding globulin deficiency
Low TT4, low or normal serum fT4, normal TSH
Normal free T4 by equilibrium dialysis
Corrects for low TBG
Low TBG
Thyroid hormone resistance
Normal labs with clinical features of hypothyroidism
Thanks for your attention!
Noon Conference: Neonatal Surgical Emergencies, Dr.
Mumphrey!!!