grant beardsley, ms, mt(ascp) - oregonpa.orgoregonpa.org/resources/2015cme/speaker...
TRANSCRIPT

10/12/2015
1
Interpreting:
Urine Drug Test Results in
Chronic Opioid Therapy
and Drugs of Abuse
Grant D. Beardsley, M.S., MT(ASCP)
Clinical Toxicologist,
Grant Beardsley, MS, MT(ASCP)
• I have nothing to disclose.
• I work for PeaceHealth Laboratories and
will share some of our processes, but I
have no commercial interest.
What Americans Believe
• 70% of opioid users do not know sharing
painkillers is a felony
• 90% of opioid users are unconcerned about
addiction
• Only 20% Americans consider prescription
pain medication to be a serious safety threat.
From: 2015 National Safety Council – Opioid Painkiller Media Briefing (n=427)
http://www.nsc.org/NewsDocuments/031115-Public-Opinion-Poll.pdf

10/12/2015
2
People who abuse or are dependent on
prescription opioids are 40x more likely to
be abusing or dependent on heroin.
From: Frieden, T. Heroin: The Epidemic That Knows No Boundaries; Medscape CDC Expert Commentary.
July 27, 2015. See: www.medscape.com/viewarticle/848294
From: http://www.agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf
Over 60% of patients taking opioids for
at least 3 months are still on opioids five
years later.
Source of Prescription Drugs for Nonmedical Use
5
Free from
friend/relative
53 %Bought/took from
friend/relative
15 %
Other
5%
Rx from one
doctor
21 %
Drug Dealer
4 %Internet
0.1%
Source (2014): The National Survey on Drug Use and Health 2013
www.samhsa.gov/data/NSDUH/2013SummNatFindDetTables/NationalFindings/NSDUHresults2013.htm
Sources Where Users Obtained
Pain-Relievers for Nonmedical Use
The purpose of urine drug testing:
� Identify undisclosed drug use and/or abuse
� Identify aberrant behavior
� Verify compliance with treatment
Source: Washington State Agency Medical Directors’ Group. Interagency Guideline on
Prescribing Opioids for Pain. 3rd edition, June 2015.
10/12/2015
3
Urine drug testing can not do…..
There is no scientifically validated relationship
between the amount of drug taken and urine drug
concentration.
Therefore, a urine drug test cannot indicate the
amount of drug taken, when the last dose was
administered, or the source of that drug.
Source: Douglas L. Gourlay, MD, Yale H. Caplan, Ph.D., and Howard A. Heit, MD. Urine Drug
Testing in Clinical Practice, 4th Edition, 2010
Nationally Recognized Guidelines & Recommendations
• American Academy of Family Practitioners
• Centers for Disease Control & Prevention
• Washington State Agency Medical Directors’ Group
• Institute for Clinical Systems Improvement (ICSI)
• American Academy of Pain Medicine & American Pain Society in Opioid Treatment Guidelines
• Department of Veteran’s Affairs
• Center for Medicare & Medicaid Services (CMS)
• Physicians for Responsible Opioid Prescribing
All of the above organizations endorse periodic patient assessment with urine drug testing.
Updated Guidelines:
June 2015
http://www.agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf

10/12/2015
4
Questions Confronting Providers
“Is my patient taking the medications I did prescribe ?”
� Adherence, non-adherence, diversion
“Is my patient taking drugs I did not prescribe ?”
� Non-medical use of scheduled prescriptions
� Scheduled prescriptions from other providers
� Illicit drug use
“What is the reliability of a urine drug test ?”
� How accurate are the tests
� Potential for misinterpretation
� How often should a patient be tested
Adherence vs. Non-adherence
� Retrospective study of 470 non-cancer COT patients.
� Urine drug tests included confirmation.
� Drug test results compared to Rx records:
From: Michna, E., et al., Clin J Pain 23:173-179, Feb 2007
54%
10%
14%
20%
2% Expected opioid present
(Normal)
Missing prescribed opioid
Unexpected drug present
Illicit drug
Adulterated specimen
Incidence of Aberrant UDT Results
StudyCOT patients with
aberrant UDT results
Cook RF, 1995 50%
Fishbain DA, 1999 46.5%
Hariharin J, 2007 38%
Ives TJ, 2006 32%
Berndt S, 1993 32%
Katz NP, 2003 29%
Michna E, 2007 45%
West R, 2010 9-33%
Manchikanti L, 2006 16%
From: Owen, Graves T., et al. Urine Drug Testing: Current Recommendations and Best Practices, Pain Physician 2012.
15:ES119-ES133, ISSN 2150-1149

10/12/2015
5
Recommendation for Frequency of UDT (1)
Risk Category (by ORT) UDT Frequency
• Low Risk 1 per year
• Moderate Risk 2 per year
• High Risk or Opioid dose > 120 mg
MED/d)
3 - 4 per year
• Aberrant Behavior(Lost Rx, multiple requests for early refill, opioids
from multiple providers, unauthorized dose
escalation, apparent intoxication, etc.)
At time of visit(Address aberrant behaviors in person,
not by telephone.)
Source: Washington State Agency Medical Directors’ Group. Interagency Guideline on Prescribing Opioids for
Pain. 3rd edition, June 2015.
Patient Risk Status/ Profile Frequency of Opioid Monitoring
• Stable opioid treatment
• Low risk for adverse outcome* Once every 3-6 months
• History of addictive disorder
• Occupation requiring high mental activity
• Older adults
• Unstable/dysfunctional social environment
• Psychiatric or medical comorbidities
More frequent after treatment
initiation; changes in opioid dose
• Very high risk for adverse outcome* Once weekly
Source: Chou R, Fanciullo GJ, Fine PG, et al; American Pain Society-American Academy of Pain Medicine Opioids
Guidelines Panel. Clinical guidelines for the use of opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113-130.
*Undesirable effects associated with opioid use (misuse, abuse, addiction or diversion).
Recommendation for Frequency of UDT (2)
Drug/ Drug Class to Test
• Prescribing drug (if not listed)
• Amphetamines
• Opioids
• Cocaine
• Benzodiazepines
• Alcohol
• Barbiturates
• Oxycodone
• Methadone
• Fentanyl
• Marijuana
Source: Washington State Agency Medical Directors’ Group. Interagency Guideline on
Prescribing Opioids for Pain. 3rd edition, page 63. June 2015. .

10/12/2015
6
Laboratory Analysis in Pain Management
• Drug screen (“initial test”, “UDS”)• Immunoassays (Emit, ELISA, others)
• Specimen Validity Test
– pH, creatinine, specific gravity, oxidants, etc.
– Check for dilution, interference, adulterants
• Confirmation Testing (mass spectrometry)• GC-MS
• LC-MS/MS
• LC-TOF/MS
• Directed (mass spectrometry)• LC-MS/MS or GC/MS
16From: Clinical Toxicology, A Guide for Laboratory Professionals. CAP Press (2012)
Screen vs. Confirmation Tests
• Screen test: – Detect drugs or drug classes
– Qualitative: positive or negative result
– Result confidence � variable
– Lab-based multichannel instrument or Instant-test (POC)
• Confirmation test: – Chromatography with mass spectrometry methods
– Result confidence � very high
– Highly sensitive and specific
– Quantitative or qualitative
Note:
Repeating an immunoassay on the same or another urine specimen is not an acceptable confirmation strategy.
17
Analytical Requirements
• Drugs of Abuse– Commercial reagents on automated immunassay analyzer
• Confirmation using GC-MS
• Pain Management Analgesics – Commercial immunoassay reagents are generally not sensitive
enough to detect opioids at lower concentrations
– GC-MS or LC-MS-MS
• LC-MS-MS required for lower cutoffs– Lower cutoffs are required for pain management
• Negative result is a red flag
Lab immunoassay Screen

10/12/2015
7
Point-of-Care Drug Test (POC)
� POC testing in clinical practice:
� Detects some pain medications and many illicit drugs
� Convenient, rapid turn-around-time
� Adjunct to clinical laboratory testing
� Device must be CLIA waived
� Allows provider-patient discussions
� Confirmation of positive (and negative) tests
� Disadvantages:� False-positive results (cross-reactivity)
� False-negative results (fails to detect)
� Subjective interpretation
� Non-specific drug classes (opiates, amphetamines, benzodiazepines)
� Not Detected: alcohol, oxymorphone, hydrocodone (+/-), hydromorphone, buprenorphine, fentanyl, carisoprodol, tapentadol and tramadol.
Question:
Which of the following might explain a positive
opiate screen (unconfirmed)?
(a) codeine use
(b) heroin use
(c) morphine use
(d) poppy-seed ingestion
(e) hydrocodone use (variable cross-reactivity)
(f) all the above
Caution: Opiate Immunoassay Screen Test
� Situation: Patients may be dismissed from the practice based on a negative drug test result for a prescribed medication.
� Background: Opiate Screen is designed to detect morphine
� Assessment: Opiate screen does not detect:
� Oxycodone� Methadone� Fentanyl� Hydrocodone (+/- ?) � Hydromorphone � Oxymorphone� Tramadol, buprenorphine, carisoprodol
� Recommendation:
Be aware most prescription opioid analgesics are not “opiates” and will test negative on an Opiates Screen.
http://www.painphysicianjournal.com/2008/march/2008;11;S155-S180.pdf

10/12/2015
8
Immunoassay: Potential for False-Negative
Does Opiate Screen detect Hydrocodone or
Hydromorphone?
Using 112 urine specimens from patients prescribed HC or HM
where all urines had negative Opiate Screens by immunoassay:
� 81 specimens (71%) were positive for hydrocodone /
hydromorphone by mass spectrometry.
From: R Bertholf, et al: Journal of Analytical Toxicology (2015);39:24-28
Immunoassay: Potential for False-Negative (continued)
Hydromorphone detection problems with Opiates Screen?
69% of specimens found positive for hydromorphone by mass spec
were negative with Opiate Screen immunoassay.
From: Mikel et al. LC-MS/MS Extends the Range of Drug Analysis in Pain Patients. Ther Drug
Monit., 2009 December; Volume 31, Number 6.
Immunoassay: Potential for False-Negative (continued)
In a study where 77,881 urine specimens were positive for opioids using LC-MS/MS:
• 59% were opioid negative by point of care (POC) test
• 23% opioids missed by routine tests used in many clinical, hospital and reference laboratories
Evans M, Kriger S, Gunn J, Schwilke G. (2009) Effective monitoring of opiates in chronic pain patients.
Practical Pain Management. (6):32-33.
10/12/2015
9
Immunoassay: Potential for False-Negative (continued)
Benzodiazepines and instant POC tests ……..
• Point of Care (POC) tests showed 24% false-negative rate in urine from patients taking benzodiazepines.
• 10% false-positive rate in patients not taking benzodiazepines.
Manchikanti,L, et al. Comparative Evaluation of the Accuracy of Benzodiazepine Testing in Chronic
Pain Patients Utilizing LC/MS/MS of Urine Drug Testing. Pain Physician (2011);14:259-270.
Instant POC tests ……..
The simplicity of use and access to rapid results of the on-site drug testing can lead to serious medical or social consequences if unexpected
results are not confirmed by secondary analysis.
Chia-Ni Lin, et al. Evaluation of the NexScreen and DrugCheck Waive RT Urine Drug Detection Cups.
J Anal Toxicol (2013) 37 (1): 30-36.
Immunoassay Limitations
“Drug screening by immunoassay does not allow
for complete adherence-monitoring in those
patients who are prescribed drugs that are not
detected by common immunoassay screens.”
J. Dickerson, et al. Improved detection of opioid use in chronic pain patients through monitoring of opioid
glucuronides in urine. Journal of Analytical Toxicology. 36:541-547 (2012).
10/12/2015
10
Confirmation Testing
Because of cross-reactivity and different sensitivity
and specificity between immunoassays, a second
confirmatory test is required unless a screen result is
expected or the patient has disclosed drug use.
Confirmation Testing:
� Confirm a positive drug/ drug group
� Confirm a negative drug/ drug group
Source: Washington State Agency Medical Directors’ Group. Interagency Guideline on Prescribing Opioids for
Pain. 3rd edition, June 2015.
.
GC/MS Confirmation
LC-MS/MS
Tandem Mass Spectrometer

10/12/2015
11
Liquid
Chromatography
Tandem Mass
Spectrometer
Direct Testing of Opiates & Opioids by LC-MS/MS (Tandem Mass Spectrometry)
Quantitative Analysis � Codeine� Morphine� Hydrocodone� Hydromorphone� Oxycodone� Oxymorphone� Meperidine� Fentanyl� Norfentanyl� 6-Monoacetyl morphine
Gourlay, DL, Heit, HA. Patient Centered Approach to UDT in the Chronic Pain Patient. PainWeek, Las Vegas, NV; Sept 9, 2011.
The Laboratory’s Challenge:
Specimen Matrix
Biological specimens are mostly
made of what we are not
interested in measuring.

10/12/2015
12
� A mixture of 95 drug standards injected into LC-MS/MS (top).
� Patient specimen (bottom).
Chromatography (LC-MS/MS)

10/12/2015
13
SECOND: Multiple Reaction Monitoring
170 210 250 290
210
222
268 280165
Spectrum with
background ions
Q1 lets only
drug ion 210
pass through
190 210
210
Q2 Collision Cell
breaks ion 210
apart
150 170 190 210
210158
191
Q3 filters specified
product ions 158 and
191 from precursor
ion 210 to detector.
160
158
190
191
no chemical background
Ions

10/12/2015
14
Interpretation of Opiate/Opioid Test Results
� Understanding opiate-opioid metabolism is essential for
interpretation of test results.
� Historical knowledge of metabolism is data based on standard
opiate-opioid doses.
� New findings in high dose pain medication challenges historical
knowledge.
Oxycodone 5 mg tablet Oxycodone 80 mg tablet
Pharmacokinetics
Major and Minor Metabolic Pathways for Opiates & Opioids
MorphineCodeine 6-Monoacetylmorphine
Poppy Seeds and Morphine Drugs
Minor Metabolism
(high dose codeine)Minor Metabolism
(high dose morphine)
Hydrocodone Hydromorphone Heroin
Norhydrocodone (CYP3A4)
SB Karch. Pathology of Drug Abuse. CRC Press, 4th Ed. (2009)
Clinical Toxicology, A Guide for Laboratory Professionals. CAP Press (2012)

10/12/2015
15
Major and Minor Metabolic Pathways Opioids (cont.)
Methadone Methadone Metabolite (EDDP)
Buprenorphine Norbuprenorphine
Tramadol O-desmethyl tramadol
Oxycodone Oxymorphone
Oxycodone Noroxycodone (CYP3A4)
SB Karch. Pathology of Drug Abuse. CRC Press, 4th Ed. (2009)
Clinical Toxicology, A Guide for Laboratory Professionals. CAP Press (2012)
Benzodiazepines
• Complicated metabolism for many benzodiazepines
• Parent benzodiazepine frequently not found in urine
– Immunoassays may target the parent medication and have poor cross-reactivity to the metabolites
• Patients may be taking more than one benzodiazepine
• Significant patient safety issue when taken with opiate/opioids
Benzodiazepine Metabolism & Elimination
Clorazepate (Tranxene)
Diazapam (Valium) Temazepam (Restoril)
Nordiazepam Oxazepam (Serax)Halazepam (Paxipam)
Chlordiazepaxide (Librium)
Flurazepam (Dalmane) N-hydroxyethylflurazepam
7-aminoclonazepam
α-hydroxyalprazolamAlprazolam (Xanax)
Lorazepam (Ativan)
Clonazepam (Klonopin)
Glu
cu
ron
ida
tio
n
Flunitrazepam (Rohypnol)
Source: Clinical Toxicology Testing; CAP Press (2012)
7-Aminoflunitrazepam

10/12/2015
16
Example:
Rx - Clonazepam
Benzodiazepines Screen - Positive by instant cup test
Is confirmation test necessary?
Confirmation shows patient taking lorazepam and alprazolam in
addition to clonazepam
Benzodiazepines in Urine
Drug Urine Metabolites Half-life, plasma (hr)
Detection Time in
Urine (d)
Alprazolamα-Hydroxyalprazolam
11 to 15 2 to 5
Chlordiazepoxide Nordiazepam
Oxazepam5 to 30 2 to 5
Clonazepam7-Aminoclonazepam
20 to 40 2 to 5
DiazepamNordiazepam
Oxazepam
Temazepam
20 to 40 7 to 10
Flunitrazepam (not in US)7-Aminoflunitrazepam
6 to 24 2 to 5
FlurazepamHydroxyethylflurazepam
2 to 3 1 to 2
LorazepamLorazepam
9 to 24 2 to 5
Nordiazepam (not in US)Oxazepam
> 24 7 to 10
OxazepamOxazepam
4 to 15 2 to 5
Clorazepate
(prodrug) Nordiazepam
Oxazepam
> 24 7 to 10
Source: Clinical Toxicology Testing; CAP Press (2012).
Negative result for a prescribed medication:
� Non-adherence, possible diversion
� Medication used incorrectly:
o Less than prescribed dose used
o Less frequently used than prescribed
� Variable drug delivery, or not well absorbed
� Rapid metabolism/elimination
� Dilute urine or adulterated urine specimen
� Immunoassay screen failed to detect drug concentration
� Clerical or analytical error

10/12/2015
17
Positive result for a drug not prescribed
� Drug was used:
� Previous prescription
� Illicit use (street purchase, theft)
� Prescription obtained from another provider
� Incorrect prescription was filled
� Non-medical use (“shared prescription”)
� Metabolite detected from a legitimate prescription
o Codeine (high dose) ⇒ hydrocodone
o Morphine (high dose) ⇒ hydromorphone
� Poor test method specificity (immunoassay)
� Prescription manufacturing impurity
Commercial Active Pharmaceutical
Ingredient
Process Impurities Allowable Limit (%) Typical Observed (%)
Codeine Morphine 0.15 0.01-0.1
Hydrocodone Codeine 0.15 0-0.1
Hydromorphone Morphine
Hydrocodone
0.15
0.1
0-0.025
0-0.025
Morphine Codeine 0.5 0.01-0.05
Oxycodone Hydrocodone 1.0 0.02-0.12
Oxymorphone Hydromorphone
Oxycodone
0.15
0.5
0.03-0.1
0.05-0.4
Acceptable Opioid Process Impurities in Commercial Drug Substances
NB: New methods eliminate these impurities for hydrocodone and hydromorphone; Both varieties are available. Information from API
Manufacturers’ Certificates of Analysis.
Ethanol Testing in Urine
From: JA Gudin, et al. Risks, management, & monitoring of combination opioid, benzodiazepines, and/or
alcohol use. Postgrad Med. July (2013) 125(4): 115-130.

10/12/2015
18
Testing for Methadone:
High inter-individual variability
• Absorption and metabolism make its clinical
effects and toxicity difficult to predict
– Oral bioavailability: 41 – 95%
– Peak plasma (Tmax) levels from 1 - 6 hours
– Prolonged elimination T½ : 7 – 65 hours
Testing for Methadone & Metabolite (EDDP)
• Immunoassay Screen (IA):
� Specific test needed to detect methadone
� Metabolite (EDDP) is not detected by IA
� Methadone excretion increased in acid urine
• Confirmation by mass spectrometry
� Methadone & EDDP targeted for analysis
� Confirm unexpected IA negative screens
� Suspect: methadone positive, EDDP negative
� Detection time after last dose: 3 – 11 days
Case study:
A patient receiving SR-morphine 30 mg tid for chronic pain requests an increase in dose. The physician orders a urine pain management drug test panel that shows:
Urine Drug Test Results: Morphine 8250 ng/mLHydromorphone 325 ng/mL Oxymorphone 110 ng/mLEthanol 0.077 g/dL
What is the interpretation?

10/12/2015
19
Interpretation Urine Drug Test Results
Morphine 8250 ng/mLHydromorphone 325 ng/mL Oxymorphone 110 ng/mL
Ethanol 0.077 g/dL
� Morphine consistent with use of prescribed morphine.
� Hydromorphone source from metabolism of morphine and is consistent with use of prescribed morphine.
� Oxymorphone positive result ���� discrepant, unexpected.
� Beverage alcohol used within 14 hours of urine sample collection.
Follow-up:
Patient admits occasionally taking a relative’s oxymorphone;
also regularly drinks wine with dinner.
Actions:
� Patient informed about the danger from taking non-prescribed medicines; discontinue oxymorphone use immediately.
� Reduce or even eliminate alcohol intake.
� The aberrant UDT escalates patient to high-risk status.
�Add unannounced monthly UDT to monitor adherence.
Amphetamine

10/12/2015
20
Amphetamine confirmed positive test:
What are the sources of amphetamine in urine?
Prescription brand names:
� Adderall® - racemic of amphetamine salts
� Dexedrine®, Dextrostat®
� Vyvanse® is l-Lysine-d-amphetamine (lisdexamfetamine), a prodrug metabolized to amphetamine.
� NOT Methylphenidate (Ritalin®, Concerta®)
Methylphenidate and metabolite (ritanilic acid) are not detected by immunoassay screens and routine GC/MS confirmation tests.
58
Methamphetamine
Methamphetamine confirmed positive test:
What are the sources of methamphetamine in urine?
Amphetamine is a metabolite of methamphetamine, after methamphetamine use both are often found in urine.
� D-Methamphetamine sources:
� illicit methamphetamine
� Desoxyn® (methamphetamine HCl)
� Didrex® (benzphetamine) metabolite
� L-Methamphetamine sources:
� Selegiline metabolite (Eldepryl®, Emsam®, Zelapar®)
� Vick’s Vapor-Inhaler® (desoxyephedrine, levo-methamphetamine)
� D/L-Methamphetamine sources:
� illicit methamphetamine
� NOT Methylphenidate (Ritalin®, Concerta®) Methylphenidate and metabolite (ritanilic acid) are not detected by immunoassay screens and routine GC/MS confirmation tests. 60
10/12/2015
21
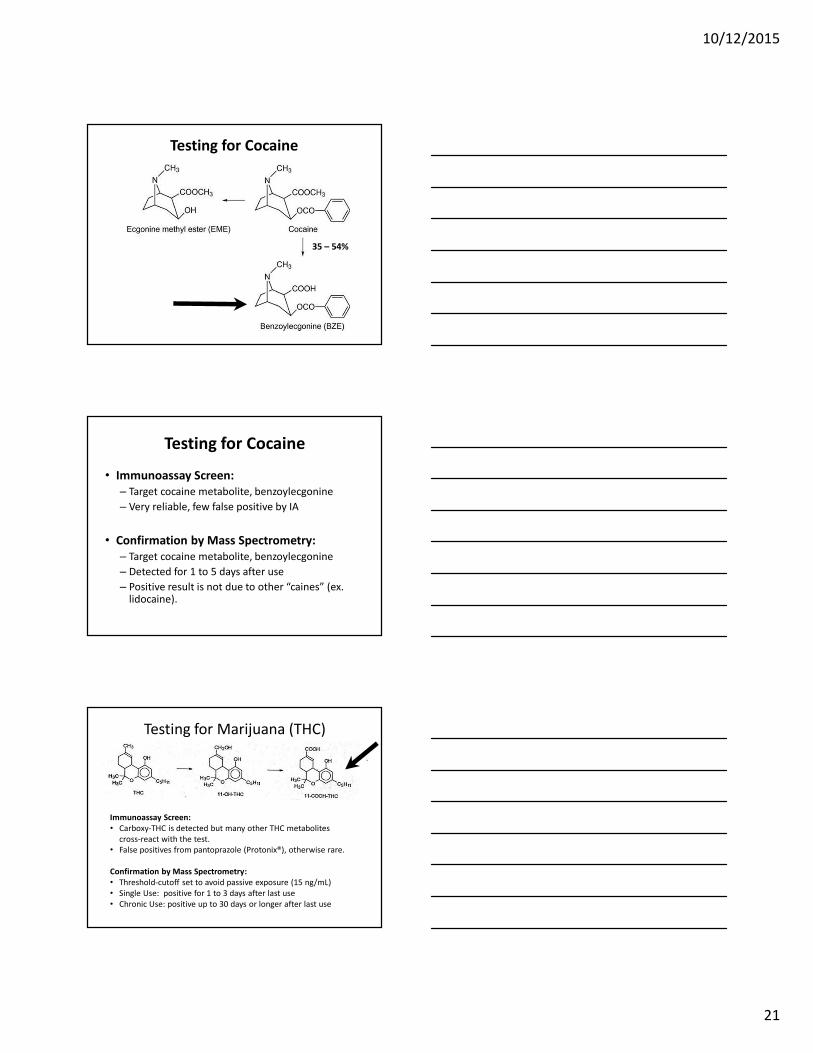
Testing for Cocaine
35 – 54%
Testing for Cocaine
• Immunoassay Screen:
– Target cocaine metabolite, benzoylecgonine
– Very reliable, few false positive by IA
• Confirmation by Mass Spectrometry:
– Target cocaine metabolite, benzoylecgonine
– Detected for 1 to 5 days after use
– Positive result is not due to other “caines” (ex. lidocaine).
Testing for Marijuana (THC)
Immunoassay Screen:
• Carboxy-THC is detected but many other THC metabolites
cross-react with the test.
• False positives from pantoprazole (Protonix®), otherwise rare.
Confirmation by Mass Spectrometry:
• Threshold-cutoff set to avoid passive exposure (15 ng/mL)
• Single Use: positive for 1 to 3 days after last use
• Chronic Use: positive up to 30 days or longer after last use

10/12/2015
22