grief and perinatal loss : a community hospital approach to support
TRANSCRIPT

principles and practice
Grief and Perinatal Loss A Community Hospital Approach to Support DONNA CARR, RN, AND CHAPLAIN SAMUEL F. KNUPP, MDIV, THM
Hospital health-care professionals sometimes fail to recognize the depth to which parents grieve over a stillbirth and to acknowledge the validity of the parents’ grief. By interacting with SHARE (Support and Help in Airing and Resolving Experiences), a parent support group for those who have experienced a perinatal loss, a hospital team was able to develop a written protocol with support measures to use when stillbirth occurs. This protocol has been in effect for three years and the staff has seen dual benefits. Staff members find constructive ways of offering support, and parents derive a sense of comfort and direction from the approach.
Brenda and Jack were like many young couples during pregnancy- looking forward to the moment of birth from the perspective of many months of planning, hoping, and dreaming. Books of names had been consulted until pages became dog-eared with use a s favorites were recorded for future selection. A room had been set aside, painted, and invested with the name “baby’s room.” A special savings bond had been taken out and jokingly referred to as the “college fund.” Arms were aching to hold the infant soon to be born. Good prenatal care had been sought. “Doing fine,” the doctor pronounced at the last prenatal visit, “Should be any time now.” Dutifully, every night Brenda and Jack practiced their Lamaze tech-
Submitted: June 1983. Revised: No- vember 1983. Accepted: December 1983.
niques learned together in class. A special suitcase was packed be- side the door waiting to be grabbed in a hurry.
In due time, the labor pains came and Brenda and Jack went to the hospital. It was an exciting time but, just the same, a little frightening. Breathing exercises were used on the long trip from the emergency room to the labor room. After so many months of waiting, everything was hurry and more hurry. The staff was smiling at the couple and warmly attentive to their needs. Things were going smoothly. Suddenly, everybody stopped smiling and the atmo- sphere in the room became coolly professional. Another nurse was sent for, then the physician ar- rived in a rush. The whole world turned upside down when the physician said, “There’s no heart- beat. The baby’s dead.”
Labor stopped being something
productive and positive and be- came a nightmare of pain. N o one talked with Brenda and Jack out- side of brief comments that fo- cused on telling them when to move and what to do. The staff seemed to talk around them. The warmth had become uncomfort- able professionalism. Silence be- came the loudest communication.
After the birth, the infant was quickly taken away to another room. Brenda was taken back to her room, her possessions were packed, and she was prepared to be transferred from the maternity unit to another floor. The route was strange, seeming to avoid any open rooms and far away from the nursery. People moved around her but really did not seem to have anything to say.
Finally, in her room on the sur- gical floor she began to feel and think again. “Why? What did my baby look like? Why can’t I cry?
130 March/April 1985 JOG”

What am I going to say to my parents? Why is Jack so distant? What did I do wrong?” Later, her parents came in and cried with her. Her mother told her, “The doctor said that it’s just like falling off a bicycle. You have to get up and try again. You can have an- other one.” Later, when Brenda went home, her crying seemed to anger her husband. She learned not to share her thoughts of how the baby looked with her husband.
* * * “Stillbirth”-who involved in
maternity care has not experi- enced the sense of dread and helplessness this term evokes? A perinatal loss causes a sense of futility for many health-care professionals. They feel frustrated with not being able to provide a successful pregnancy outcome to parents. Health-care professionals also feel inadequate in providing parents with the most helpful emotional support. Because of discomfort with the subject of death in the maternity area, many health-care providers find it diffi- cult to give consistent physical and emotional care to patients and their families. In the midst of still- birth crisis, health-care profes- sionals tend to forget the value of supporting each other as a staff so that they can better support the grieving couple. When the staff members feel inadequate in still- birth crisis, their care reflects the discomfort and staff members come across to the patient and her family as being “cool” and “distant.” Then, health-care professionals lose their ability to help structure, support, and comfort.
In 1981, Lancaster Osteopathic Hospital in Lancaster, Pennsylva- nia, engaged in an exploration of ways of supporting grieving fami- lies during perinatal death. Still- birth, as an issue, was brought to
the hospital’s attention by a local parent support group, SHARE (Source of Support and Help in Airing and Resolving Experi- ences), which assists parents in dealing with perinatal loss. In sev- eral meetings with two of SHARE’S representatives, both of whom have experienced a perinatal loss, hospital staff became aware of areas in which health-care profes- sionals could become more effec- tive in support of these parents.
After approximately six months of experimenting with several ideas, nursing staff found ap- proaches that helped both parents and staff. From this beginning, a protocol was developed outlining support measures and hospital policies concerning stillbirth to ensure sensitivity and consistency of approach.
Staff drafted a stillbirth protocol in September 1981 with input from SHARE and the hospital’s nursing, chaplaincy, and physician staff (Table 1). Included in the protocol were the technical aspects to which hospital staff must attend and guidelines for providing emo- tional support for parents. The protocol outlined for nursing staff is a step-by-step approach from admission to labor and delivery to discharge from the hospital.
The stillbirth protocol operates under the assumption that parents and family coming into the hos- pital are in crisis. How these in- dividuals and families will deal with this crisis has much to do with the crisis situation itself, the person’s habitual coping mecha- nisms, their emergency problem- solving mechanisms, and the im- pact the setting has on them. While staff has no control over the coping ability that a family brings to the stillbirth protocol, health-care providers can struc- ture the hospital setting so that as much control as possible is returned to the family.
One of the biggest frustrations parents seem to feel is a loss of control. The stress of the situation, the strangeness of the surround- ings, fear, anxiety, and shock all contribute to a sense of being out of control. The protocol functions through a process of explanation, repetition, structuring of the physical plant, and encouragement to be a real part of all decision making, thus, returning control to patients and their families. It, therefore, comforts in the im- mediate sense and lays the groundwork for realistic, guilt-free grieving.
~
PREDELIVERY SUPPORT
Nursing staff may have contact with the couple before labor when the fetal demise is diagnosed. At this time, the nurse can lay the groundwork for support when the parents return to labor. After con- sultation with the physician, the chaplain is contacted to establish a rapport with the couple. A di- agnosed fetal demise is noted on the mother’s prenatal record to assure that all staff are prepared to provide consistent care on ad- mission in labor. Parents know that the infant has died and are anxious to have that part of the process over. As one mother said, “I can’t stand it. My belly’s so big, but I don’t feel the movement any- more. I just want to get it over with so I can get back to normal. I just feel so full and empty at the same time.”
Parents need clear explanations regarding the plan for initiation of labor. However, this extended pe- riod before labor can be a very productive time when prebirth grieving can be started and rela- tionships with support staff per- sons cemented (Table 1). At Lan- caster, a positive correlation has been found between the amount
March/April 1985 JOGNN 131

Table 1. Lancaster Osteopathic Hospital Department of Nursing: Procedure for Handling Stillbirths
Purpose: To provide guidelines for handling stillbirths. Objective: To provide continuity of care to parents experiencing
a stillbirth. I. Support of Parents Prior to Delivery:
A. Encourage ventilation of feelings. B. Encourage support person to stay with mother. C. Encourage one-to-one nursing support. D. Administer order pain medications. E. Inform mother of her option of being transferred to
F. Notify clergy according to parents’ wishes. G. Note parents’ wishes on care plan.
II. Care of Infant After Delivery: A. Physical Care of Infant
another unit after delivery.
1. Take to soiled utility room to complete care. 2. Weigh and measure.
a. Save disposable tape measure for parents. 3. Cut small piece of hair for parents, tape to Infant
111. A. Memory Sheet. a. Save comb for parents.
4. Apply Hollister cord clamp to cord, remove hemostat. 5. Footprint on birth record.
a. Obtain mother’s thumbprints first. b. Footprint “Infant Memory Sheet.” c. Footprints may be deleted if infant is macerated,
note this on footprint record. 6. Identify with ID band.
a. Make two bands so that one can be given to parents.
7. Complete two crib cards. a. One for parents b. One to tag outside of blanket prior to taking infant
to morgue. 8. Baptize infant after obtaining verbal permission from
9. Save all above-mentioned baby effects to be given to parents.
parents. a. Infant Memory Sheet, hair cutting, tape measure,
comb, crib card, ID band. b. Place in manila envelope, place mother’s name
and date of infant’s birth on outside. Note: If parents do not claim belongings, save on
storage shelf in soiled utility room L/D; retain for five years; if not claimed, they will be discarded.
10. Ask parents if they want an instant picture taken of baby; obtain consent form.
11. Discuss with parents their options in viewing the baby.
12. If infant is very small (i.e., 1 Ib.; 16-20 wk.) or very macerated, a properly labeled specimen container is used to transport to morgue.
Common Sense will dictate which of above measures is appropriate and which can be used to support parents. 8. Documentation, Required Forms
1. Birth Record (footprint sheet) a. Complete as much as possible prior to delivery to
b. Obtain mother’s thumbprints prior to delivery if avoid questioning parents later.
possible.
c. Make parents aware they may name the baby. d. When complete-place in Ward Clerk’s file on
2. Stillbirth Certificate (2 certificates with carbon between) a. Required by State Law on any stillborn 16 weeks
gestation or older; if in doubt of age, follow through with procedure; the pathologist will give final determination of gestational age.
1. Coroner signs certificate on a Coronor’s case. 2. Physician signs certificate otherwise.
c. Send original signed certificate to Nursing Office; retain carbon copy on mother’s chart.
postpartum unit.
b. Physician consulted by Coroner.
3. Record of Death Sheet a. Send to Nursing Office after infant is taken to the
morgue. 4. Checklist for Assisting Parents (see Table 2)
a. Check as items are complete; place on mother’s care plan. Remove at time of discharge and file on postpartum unit.
C. Infant to Morgue 1. Be sure parents have had opportunity to hold/view
infant. 2. Be sure infant is identified. 3. Wrap infant in blanket. 4. Tag outside of blanket with crib card. 5. Notify security to meet you at morgue to open door. 6. Take infant to morgue via back stairwell. 7. Place in morgue compartment (cooler). 8. Complete record of death sheet, forward to Nursing
Office. 111. Support of Parents After Delivery:
A. Allow Parents to viewihold baby as desired. 1. In delivery room
a. Physician agrees that mother’s condition permits. b. If physically or emotionally unable, inform parents
c. It is preferrable to keep baby in soiled utility room they may view baby later.
of L/D until all family members have viewed, provided this is a reasonable period of time (i.e., 1-2 hours).
2. In immediate postpartum period after transfer from Delivery Room. a. As mother’s condition permits. b. Allow grandparents as couple desires.
a. Notify Supervisor and Security of request. b. Meet Security at Morgue to obtain baby, wrap in a
c. Use back stairwell to return baby to OB
3. After infant has been taken to Morgue.
warm blanket.
conference room for viewing. 1 a. To meet Infection Control Guidelines, all
individuals viewing the baby must wash hands prior to returning to patient’s room.
4. Stay with parents while they view baby. a. Silent support sometimes best. b. If parent’s condition warrants, you may leave them
c. Remember-some parents may never be able to alone for awhile.
be left alone.
(Continued on page 135)
132 MarchiApril 1985 JOG”
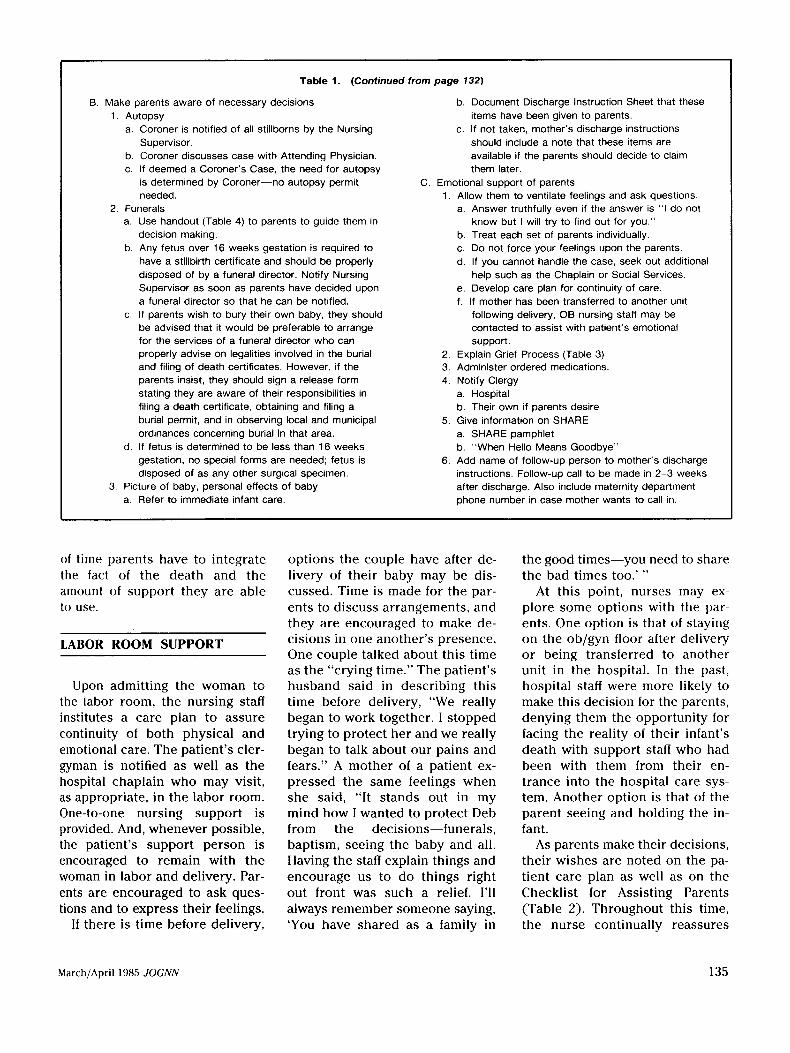
Table 1. (Continued from page 132)
B. Make parents aware of necessary decisions 1. Autopsy
a. Coroner is notified of all stillborns by the Nursing Supervisor.
b. Coroner discusses case with Attending Physician. c. If deemed a Coroner’s Case, the need for autopsy
is determined by Coroner-no autopsy permit needed.
a. Use handout (Table 4) to parents to guide them in decision making.
b. Any fetus over 16 weeks gestation is required to have a stillbirth certificate and should be properly disposed of by a funeral director. Notify Nursing Supervisor as soon as parents have decided upon a funeral director so that he can be notified.
c. If parents wish to bury their own baby, they should be advised that it would be preferable to arrange for the services of a funeral director who can properly advise on legalities involved in the burial and filing of death certificates. However, if the parents insist, they should sign a release form stating they are aware of their responsibilities in filing a death certificate, obtaining and filing a burial permit, and in observing local and municipal ordinances concerning burial in that area.
d. If fetus is determined to be less than 16 weeks gestation, no special forms are needed: fetus is disposed of as any other surgical specimen.
3. Picture of baby, personal effects of baby a. Refer to immediate infant care.
2. Funerals
b. Document Discharge Instruction Sheet that these items have been given to parents.
c. If not taken, mother’s discharge instructions should include a note that these items are available if the parents should decide to claim them later.
C. Emotional support of parents 1. Allow them to ventilate feelings and ask questions.
a. Answer truthfully even if the answer is “I do not know but I will try to find out for you.”
b. Treat each set of parents individually. c. Do not force your feelings upon the parents. d. If you cannot handle the case, seek out additional
help such as the Chaplain or Social Services. e. Develop care plan for continuity of care. f. If mother has been transferred to another unit
following delivery, OB nursing staff may be contacted to assist with patient’s emotional support.
2. Explain Grief Process (Table 3) 3. Administer ordered medications. 4. Notify Clergy
a. Hospital b. Their own if parents desire
a. SHARE pamphlet b. “When Hello Means Goodbye”
6. Add name of follow-up person to mother’s discharge instructions. Follow-up call to be made in 2-3 weeks after discharge. Also include maternity department phone number in case mother wants to call in.
5. Give information on SHARE
of time parents have to integrate the fact of the death and the amount of support they are able to use.
LABOR ROOM SUPPORT
Upon admitting the woman to the labor room, the nursing staff institutes a care plan to assure continuity of both physical and emotional care. The patient’s cler- gyman is notified as well as the hospital chaplain who may visit, as appropriate, in the labor room. One-to-one nursing support is provided. And, whenever possible, the patient’s support person is encouraged to remain with the woman in labor and delivery. Par- ents are encouraged to ask ques- tions and to express their feelings.
If there is time before delivery,
options the couple have after de- livery of their baby may be dis- cussed. Time is made for the par- ents to discuss arrangements, and they a re encouraged to make de- cisions in one another’s presence. One couple talked about this time as the “crying time.” The patient’s husband said in describing this time before delivery, “We really began to work together. I stopped trying to protect her and we really began to talk about our pains and fears.” A mother of a patient ex- pressed the same feelings when she said, “It stands out in my mind how I wanted to protect Deb from the decisions-funerals, baptism, seeing the baby and all. Having the staff explain things and encourage us to d o things right out front was such a relief. I’ll always remember someone saying, ‘You have shared a s a family in
the good times-you need to share the bad times too.’ ”
At this point, nurses may ex- plore some options with the par- ents. One option is that of staying on the ob/gyn floor after delivery o r being transferred to another unit in the hospital. In the past, hospital staff were more likely to make this decision for the parents, denying them the opportunity for facing the reality of their infant’s death with support staff who had been with them from their en- trance into the hospital care sys- tem. Another option is that of the parent seeing and holding the in- fant.
As parents make their decisions, their wishes are noted on the pa- tient care plan as well as on the Checklist for Assisting Parents (Table 2). Throughout this time, the nurse continually reassures
March/April 1985 JOGNN 135

Table 2. Checklist for Assisting Parent@) Ex1
DATE I TIME I CHECK:
I I
briencing Newborn Death, Stillbirth (Lancaster Osteopathic Hospital) I
INDICATES COMPLETION I SIGNATURE
Viewed baby when born and/or after delivery: ___ Mother -Father
Touched and/or held baby: ___ Mother - Father
Given option of being transferred off Maternity Department
Autopsy: Yes __ No __ Permit Signed ___
Clergy notified - Family -Hospital
Baptism: ___ Yes - No
Did parent(s) name the baby? ~ Yes - No
Name of baby on Death Certificate
Instant photo: Permit signed - Given to parent(@ - On file -
Footprints and Memory Certificate: Given to parent@) - On file -
I.D. band, crib card, baby belongings: Given to parent(s) -
On file -
Funeral sheet given to parent(s): - I Funeral arrangements made by: Mother __
Father ~
Informed about postponing funeral until mother able to attend ___
Grief process explained to: ___ Mother - Father
Resource information given to parent(s) about: SHARE -
"When Hello Means Goodbye" -
Follow-up person assigned: Name
Place with patient's care plan. After discharge this is to be filed on postpartum unit.
the parents that their decisions aged to think of the support pro- as they want. Sometimes, parents are not right or wrong but rather tocol as a guide to options lrom are so overwhelmed by the death have to do with feelings and which they can choose. They can of their infant that they cannot needs. Parents are also encour- use as little of it or as much of it make use of any of the protocol
136 March/April 1985 JOG"

Table 3. Grief Process’
A. Stage of Denial b. Sit with patient. c. Use touch if appropriate.
D. Stage of Acceptance 1 . Period of denial allows patient to mobilize defenses. 2. Patient will exhibit withdrawal and avoid talking about
death. 1. Patient is neither angry or depressed about loss 3. Usually a temporary defense to be replaced in time by
partial acceptance. 4. May talk of death then change topic abruptly.
2. Patient may be void of feelings
1. Fear, anxiety Normal feelings may include:
5. May be in temporary state of shock.
6. Stage of Anger 1 . Denial replaced by anger, rage, envy, and resentment. 2. Anger may be displaced and projected on environment. 3. Anger frequently directed at hospital staff. 4. Try to tolerate irrational anger-patient experiences a
sense of relief in expressing anger.
1. Patient prepares to accept loss of everything and everyone he loves.
2. May mourn loss of other meaningful people in his life. a. Allow patient to express his sorrow.
C. Stage of Depression
2. Sorrow and grief 3. Over- or suppressed hostility interwoven with guilt or self-
blame. 4. Depersonalization 5. Projection of guilt 6. Submission or excessive courtesy (may mask hostility)
1. Offer practical help-Social Services, Chaplain 2. Reassure parents they are not alone 3. Provide opportunity for ventilation of conflicts-anger,
depression, victimization-SHARE; follow-up call * Reference: The Lippincott manual of nursing practice,
Demonstrate concern for family:
Philadelphia: J.B. Lippincott, 1974: 891-4.
at the time. Parents are reassured that staff approval of them as in- dividuals is not connected to use of the support protocol.
~~ ~ ~
DELIVERY ROOM SUPPORT
In the delivery room, the phys- ical care of the infant is outlined so that articles used to care for the infant may be saved for the parents. After measuring the in- fant, the disposable tape measure is saved. If the infant has enough hair, a small lock is cut to be placed on a Memory Certificate. In applying the identification band, a duplicate is made to be given to the parents. A crib card is filled out with important information and placed with the other belong- ings. The mother’s thumb prints and infant’s footprints are ob- tained on the Memory Certificate.
The infant is bathed and dressed in an undershirt and wrapped in a soft blanket. These are removed later and placed with the other articles that had come in contact with the infant. The parents are then informed that they may hold the infant a t this time, a s well as later when they are taken back to a postpartum
room. If the parents wish the in- fant to be baptized, staff tries to d o this with support people pres- ent (grandparents, friends, etc.), making it a ceremony with the parents participating a s fully a s they wish. A baptismal certificate is filled out and signed by both the parents and the chaplain or family clergy. Again, even the signing of the certificate helps put the parents more in control of this part of the protocol.
Another option offered is an instant picture of the infant being held by its parents. Some parents find that there may be too many decisions for them to make at one time. The staff lets them know that all the infant’s belongings will be maintained in a file in labor and delivery for five years. If the parents decide at a later date that they would like the belongings, they are available.
The staff at Lancaster has found that most parents want to see their infant regardless of the condition. Parents will find something very positive about the infant. One mother ignored badly macerated skin to focus on perfect fingers and toes; another found a mouth that was just like her father’s. If
parents are prepared for what to expect when they see their infant, they seem to cope with the facts of the death, while talking about the positives of the infant’s devel- opment. If the parents are denied an opportunity to see their infant, their imaginations can envision the infant to be much more disfig- ured than it is in reality. Seeing the dead infant seems to reinforce, in a positive way, the reality of the experience that is both unfor- gettable and healing.
POSTPARTUM SUPPORT
After the recovery period, par- ents are informed of additional decisions for them to make re- garding an autopsy and funeral home. The parents need some time in which to accept the basic fact of the infant’s death before they are required to make these difficult decisions. These expec- tant parents had not thought that they would need to make these types of decisions. When the par- ents should be deciding where to buy formula and diapers, they are asked to make decisions about the burial of their infant. The unpleas- antness of this subject often leads
March/April 1985 JOCNN 137

Table 4. Funerals
Upon the death of your baby You and your family have just experienced the death of a fetus
or full-term baby. This is the time when it is difficult to think clearly or make decisions. We know that this is a painful time that you have had no time for which to prepare. We have gathered a few facts about the services available in the Lancaster area. This sheet is intended to give you some ideas which you can talk over with your family, clergyperson, friends, and staff. We encourage you to share openly with one another and to make mutual decisions.
Various funeral homes contacted in the Lancaster area are willing to offer specialized services to families experiencing fetal death or stillbirth. These funeral homes stressed their willingness to help families in the grieving process by providing sensitive, lowcost funeral arrangements. They welcome your questions and will help you in your arrangements at no obligations.
In the next few hours, you will be asked some difficult questions. We, as a hospital, need to know the name of the funeral home you will contact. We will also be approaching you about the possibility of an autopsy. After you have made those decisions, you will have more time to decide what type of funeral arrangements and services you might want. Funeral Arrangements and Services
A typical funeral might include 0 Transportation (moving the body)
d Announcements (for newspapers, memorial folders, etc.) 0 Burial container 0 Viewing (a chance to see the body before burial or cremation) 0 Preservation of body (type of embalming) 0 Opening and closing of grave site 0 Burial plot 0 Religious service (whatever you and your clergyperson have
decided upon) costs
The services offered by the various funeral homes would vary in terms of cost with regard to each situation, however, most, funeral arrangements totaled less than $1 00.00. The various funeral homes contacted stressed that cost would be kept at a minimum and that much of the expenses would be at cost or given free of charge.
Various funeral homes offer cremation services at a nominal charge. Cost would range with each individual case but would be made up of transportation and cremation charges. Planning
Making funeral plans is difficult. It must seem very final and very real. We as a staff will support you in this process. We encourage you to discuss your plans and the feelings they raise. If it becomes necessary for you to be hospitalized for a longer period of time than expected, you might want to think about postponing the actual funeral service until you can participate in it personally.
staff to make decisions for the parents. Parents were often told that “. . . the hospital will take care of the remains.” Lancaster has developed an information sheet that summarizes the basics of funerals (Table 4). The mother is informed of the option of post- poning the funeral services until she can attend. Funerals are useful in helping parents and families face the reality of the loss and begin networks of support.
In the period from delivery to discharge, the parents may or may not be able to express their grief. The stage of shock in the grief process may mask underlying emotions. During the next few hours, and days, nursing staff fol- low the care initiated in labor and delivery. Patient care assignments are arranged to allow as much time as possible for support of the couple. One of the most difficult areas the nursing staff has had to master is understanding that there is not one right thing to say to parents to comfort them. The most important thing is to be available
to the couple to listen, to reflect, and to answer their questions as truthfully a s possible. The nurses have learned that professionalism does not prevent them from showing parents how deeply the nurses feel the parents’ loss: a firm hug, a held hand, and tears shared seem to ease both parents and staff.
Nurses at Lancaster have found that there are some more helpful and some less helpful verbal re- sponses to parents during this time of loss. Some examples of statements that are definitely not helpful follow. “You can always have another.” The couple wanted this baby, not another one. “It’s better this way, you never really knew her.” The parents had begun to bond with the infant from the time of conception; the infant was a reality to them. More helpful responses are affirming and per- mission giving: “It’s okay to cry.” “ I know that this is an awfully difficult time.” “It’s hard to know what to feel sometimes.” “Let it out.” Sometimes, the nurse needs
to reassure the parents that they are not responsible for the infant’s death. Death at anytime during life raises guilt feelings. Guilt feel- ings are particularly apparent for parents experiencing a stillbirth. Parents feel an overwhelming sense of failure of their bodies to produce a perfect living child. The most common question is “Why?” and the most frequent statement is “lf only 1 had . . . .”
The parents need to find some sense of meaning and order in the face of this tragedy. As parents begin to come out of the initial stages of shock, they begin to question. At this time, the parents need the support of a trusted nurse-someone who has seen them through the whole process of admission, to sharing in the labor and delivery rooms, to post- partum care and discharge plan- ning. Through the rapport that has been established during the hospitalization, the various sup- port persons begin the process of reality education. Parents are told of the grief process and some of
138 March/April 1985 JOCNN

the normal feelings that they can expect to experience over the course of their mourning. “When Hello Means Goodbye”* is an ex- tremely useful tool to give parents. The booklet outlines emotional responses that the parents may have as well as how to deal with friends and family who d o not seem to understand the depth of their loss. Parents are also given a pamphlet from the local SHARE group and are asked to keep the group in mind if they feel they would like a support group expe- rience.
Mother’s discharge instructions include a phone number of the maternity department as well as the name of the nurse who was significant in her care. This nurse will make a follow-up call to the patient in two to three weeks to answer questions, show concern, and to listen. In many cases, par- ents have found it meaningful to have some of the nursing staff attend the infant’s funeral. This act somehow expresses how much others do care, and provides a continuing link to the hospital ex- perience. Staff attending funeral services also point to the nurses’ needs as professionals to get a sense of closure on some of the work situations. When nurses open themselves to be more emotion- ally available to patients and their familes, nurses not only become more effective care givers, but also respond to the patients’ pains and hurts. The nurses at Lancaster have become sensitive to one an-
‘“When Hello Means Goodbye” is available from the University of Ore- gon Health Sciences Center, Dept. of Ob/Cyn, 3181 S.W. Sam Jackson Park Road, Portland, OR 97201.
other in a unique way and seek out ways to support, to share ex- periences, and to comfort.
In Lancaster Osteopathic Hos- pital’s protocol (Table l), the grief that people feel in tragedy is not removed. The protocol allows them to feel the depth of their hurt with people who can support and respond with loving concern and professionalism.
SUMMARY
Lancaster Osteopathic’s still- birth protocol has been in use for approximately three years. The protocol has been used a s a guide for assisting parents and their families in crisis. Each situation calls for some fresh rethinking of why things are done the way they are. With each family that nurses assist, they try new methods of support. Families are invited to share what was most comforting and supporting to them.
The nursing staff has been look- ing into some new directions and offers patients new options. One option is for the family to make use of the birthing room in place of the more sterile, less home-like delivery room. Also, patients have less anxiety, more restful nights, and are generally more interactive with support people when they have their significant other sleep in the same room with them. Pa- tients are now offered the choice of having a family support person room-in with them.
Finally, the nursing staff has seen some positive results when siblings are invited to be a part of some of the stillbirth situations in the hospital.
Lancaster Osteopathic Hospi- tal’s stillbirth protocol is a life-
affirming structure that seeks to grow to meet the newness and uniqueness of each individual’s experience of hurt, of loss, and of hope.
BIBLIOGRAPHY
Cooper J. Reactions to stillbirth: end this conspiracy of silence. Nursing Mirror December 6, 1979;31-3.
Croucher M. Stillbirth. Nursing Mirror July 7, 1982;155.
Crout TK. Caring for the mother of a stillborn baby. Nursing 80 April
Harrington V. Bereavement and child- birth: look, listen, and support. Nursing Mirror January 13, 1982:
Lovell A. Mothers and babies in limbo . . . loss of a baby through late miscarriage, stillbirth, and perinatal death. Nursing Mirror November 3, 1982:53.
O’Donohue N. Facilitating the grief process. Journal of Nurse Midwifery. September/October 1979:16-9.
Parrish S. Letting go . . . new dimen- sions for assisting bereaved parents. Canadian Nurse March 1980:34-7.
Quirk TR. The perinatal bereavement crisis. Crisis theory, grief history and related psychosocial factors: The framework for intervention. Journal of Nurse Midwifery Septem- ber/October 1979:16-9.
Stock JM. Reproductive casualities: ef- fects on families and professional care givers. Perinatal Press March
1980:70-3.
21-4.
1982:31-6.
Address for correspondence: Donna Carr, R N , Ob/Gyn Patient Care Coor- dinator, Lancaster Osteopathic Hos- pital, 1175 Clark Street, Lancaster, PA 17604.
Donna Carr is the ob/gyn patient care co- ordinator in the Maternity Department of the Lancaster Osteopathic Hospital in Lancaster, Pennsylvania. She serves on the Board of Directors of the SHARE group of Lancaster.
Chaplain Samuel Knupp is a hospital chaplain at Lancaster Osteopathic Hospital. He is a member of the Board of Directors of SHARE.
March/April 1985 JOCNN 139