gynec. 4 g. - postgraduate medical journalpmj.bmj.com/content/postgradmedj/35/409/644.full.pdf ·...
TRANSCRIPT
644 POSTGRADUATE MEDICAL JOURNAL November I99
rectal tube should be left for a few days for con-tinuous drainage of urine, and after this timefrequent evacuation should be encouraged. Thefluid intake must be high, and 4 g. of sodiumbicarbonate taken daily. If thirst or lethargy areexperienced, a salt-free diet is prescribed and8 g. of bicarbonate given. If dehydration is pro-gressive and nausea and vomiting occur,; thepatient must be admitted to hospital for full bio-chemical investigation. Marked acidosis or hypo-kalaemia will require careful intravenous replace-ment therapy. In hypocalcaemia, in addition tocorrection of acidosis, vitamin D2 should be givenby mouth in adequate dosage to restore a positivecalcium balance, that is, Io,ooo to Ioo,ooo unitsa day (Harrison, 1958).Cutaneous Ureterostomy
Bilateral cutaneous ureterostomy has had fewadvocates because storage of the urine dependsupon an external appliance worn over each stoma.It has not proved easy to carry out the operationwithout sloughing of the ureter or stricture forma-tion. Those most adept in its performance haveadvised against any indwelling drain, and someadvocate a spout fashioned as a skin pedicle forneat collection of the ureteric efflux. The expecta-tion that the method might avoid deleteriouseffects upon the kidney does not seem to berealized, and its advantage in cases of renaldeterioration from ureteric obstruction is equallyoffered by an isolated intestinal segment.
BIBLIOGRAPHYBAIRD, J. S., SCOTT, R. L., and SPENCER, R. D. (1917),
Surg. Gynec. Obstet., 24, 482.BOLLMAN, J. L., and MANN, F. C. (1927), Proc. Soc. exp.
Biol. Med., 24, 923.BOYCE, W. H. (I95I),.. Urol., 65, 241.BOYD, J. D. (I93I), Amer. J. Dis. Child., 42, 366.
BRICKER, E. M. (I950), Surg. Clin. N. Amer., 30, IxSI.COFFEY, R. C. (I9I ), J. Amer. med. Ass., 56, 397.CORDONNIER, J. J. (i949), Surg. Gynec. Obstet:, 88, 441.CORDONNIER, J. J., and SPJUT, H. J. (s957),-. Urol., 78. 242.CORTES, S. T. (x946), BoL Trab. Acad. Argent: Cir., 30, 558.DANIEL, 0., and SHACKMAN, R. (1952), Brit. J. Urol., 24, 334.DEPAGE, A., and MAYER, L. (1904), Arch. klin. Chir., 74, 7I.FERRIS, O. D., and ODEL, H. M. (195o), J. Amer. med. Ass., x42,
634.GEER, W. A., and DRAGSTEDT, L. R. (1938), Ann. Surg., xo8,
263.GERSUNY, R. (1898), Wien. klin. Wschr., Ix, 990, quoted by
Foges.GOODWIN, W. E., HARRIS, A. P., KAUFMAN, J. J., and
BEAL, J. M. (I953), Surg. Gynec. Obstet., 97, 295.HARRISON, A. R. (1958), Brit. J. Urol., 30, 455.HARTMAN, F. W. (1933), J. exp. Med., 58, 649.HARVARD, B. M., and THOMPSON, G. J. (I95I), .. Urol.,
65, 223.HINMAN, F. A., and WEYRAUCH, H. (!936), Trans. Amer.
Ass. gen.-urin. Surg., 29, I5.HOPEWELL, J. P. (I959), Ann. Roy. CoU. Surg. of Eng., 24, 159.JACOBS, A., and STIRLING, W. B. (1952), Brit... Urol., 24, 259.JOHNSON, T. H. (1956), J. Urol., 76, 380.KINMAN, L. M., SAUER, D., HOUSTON, W. T., and
MELICK, W. F. (I953), A.M.A. Arch. Surg., 66, 53I.LAPIDES, J. (I95I), Sur Gec.yne. Obstet.,. 93, 691.LEADBETTER, W. F. (I95g), J. Urol., 65, 8i8.LOWSLEY, O. S., and JOHNSON, T. H. (I955), .. Urol,, 73, 83.MARTIN, F. H. (1900), Amer. Gynec. Obstet. J., I6, 395.MAUCLAIRE, P. (1895), Ann. Mal. Org. gen.-urin., x3, io8o.MERSHEIMER, W., KOLARSICK, A., and KAMMANDEL, H.
(1950), Bull. N.Y. med. Coll., 13, 71.NASH, D. F. ELLISON (1956), Brit. J. Urol., 28, 387.NESBIT, R. M. (1949), .. Urol., 6x, 728.PARSONS, F. M., PYRAH, L. N., POWELL, F. J. N., REED,
G. W., and SPEIRS, F. W. (I952), Brit. J. Urol., 24, 3I7.POWELL, K. A. (I949), Brit. J. Surg., 36, 421.PYRAH, L. N. (I957), J. Urol., 78, 683.RICKHAM, P. P. (I956), Brit. J. Urol., 28, 394.SIMON, J. (I852), Lancet, ii, 568.SMITH, G. I., and HINMAN, F. Jnr. (I955), 7. Urol., 74, 354.STAMEY, T. A. (1956), Surg. Gynec. Obstet., 103, 736.STEVENS, A. R. (I94I), J. Urol., 46, 57.STILES, H. (I9II), Surg. Gynec. Obstet., 13, 127.TICHOFF, P. I. (I908), Zbl. Chir., 35, 109.TIZZONI, G., and FOGGI, A. (i888), Zbl. Chir., 15, 92I.VERHOOGEN, J. (I908), Assoc. franc. Urol., 12, 352.VERMOOTEN, V. (I934), J. Urol., 32, 273.WELLS, C. A. (I956), Brit. J. Urol., 28, 335.WITZEL, 0. (I891), Zbl. Chir., 18, 6o0.
Bibliography continued from bpage 648-Kenneth Owen. M.S.. F.R.C.S.BIBLIOGRAPHY
DE CAMP, P. T., and BIRCHALL, R: (I958), Surgery, 43, I34.FREEMAN, N. E., LEEDS, F. H., ELLIOTT, W. G., and
ROLAND, S. I. (I954), J. Amer. med. Ass., 1S6, 1077.GELLMAN, D. D. (I958), Quart. J. Med., 27, 105.GOLDBLATT, H., LYNCH, J., HANZEL, R. F., and SUM-
MERVILLE, W. W. (1934), J. exp. Med., 59, 347.HOWARD, J. E, CONNOR, T. B,, and THOMAS, W. C. (1956),Trans. Ass. Amer. Phys., 69, 291.
PEART, W. S. (I959), personal commuhication.POUTASSE, E. F. (0956), Circulation (N Y.), 13, 37.POUTASSE, E. F., and DUSTAN, H. (i956), Cleveland Clin.
Quart., 23, 3.POUTASSE, E. F., HUMPHRIES, A. W., McCORMACK, L. J.,and CORCORAN, A. C. (x956), J. Amer. med. Ass., Xs6, 419.ROB, C. G., EASTCOTT, H. H. E., and OWEN, K. (x956),Brit. . Surg., 43, I8x.THOMPSON, J. E., and SMITHWICK, P. J. (195z), .Aniplogy
3, 493.
by copyright. on 12 July 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.409.644 on 1 Novem
ber 1959. Dow
nloaded from

645
RENAL ARTERY STENOSISBy KENNETH OWEN, M.S., F.R.C.S.
Consultant Surgeon to St. Mary's Hospital and to St. Peter's Hospital
Since the discovery by Goldblatt, Lynch,Hanzel and Summerville (I934) that hypertensionin the dog can be caused by partial occlusion ofthe renal artery there has been an endless searchby physicians and surgeons for surgically curablerenal lesions in patients with hypertension.Patients with clinical hypertension have beencured by nephrectomy in such diseases as pyelo-nephritis, hydronephrosis, and renal tuberculosis,but there is no clear relationship between theseconditions and the Goldblatt lesion and resultshave, on the whole, been unpredictable anddisappointing.
Recently, however, it has been recognized thatpartial occlusion of a renal artery may be respon-sible for hypertension in man, either as a singlelesion or as a complication of the Leriche syndromeof aortic thrombosis (Thompson and Smithwick,1952; Poutasse, 1956; Freeman, Leeds, Elliottand Roland, 1954; Fig. i). The most commoncause of such lesions is atheroma, but a number ofcases of congenital stenotic lesions have been re-ported in children. There are numbers of isolatedexamples of many other types of pathology, suchas thromboangeitis, emboli, tumour and hydatidcysts.The majority of the atheromatous lesions occur
at the extreme proximal end of the renal arteryalthough occasional lesions have been reportedmore distally (De Camp and Birchall, I958). Thepresumably humoral hypertension produced bythese lesions progresses rapidly to produce thecharacteristic changes of malignant hypertension,and the raised pressure produces necrotizing ar-teriolitis in the opposite kidney. The kidney onthe affected side is protected from the raised pres-sure by the arterial obstruction and may, therefore,be potentially the better kidney. This is of obviousimportance when considering treatment and is areason for favouring reconstruction of the arteryas opposed to nephrectomy, despite the greatermagnitude of the former operation. When greaterexperience has been gained of the results of ar-terial surgery in this situation it may even be thatan indication might arise for reconstructive surgery
on the affected side followed by nephrectomy onthe contralateral side should extensive arteriolarchanges have occurred.
Diagnosis and Selection of CasesThe definitive diagnosis of these cases depends
upon aortography but it would seem unjustifiableto subject all hypertensive patients to this majorinvestigation. It is, therefore, of importance tofind clinical criteria for selecting patients foraortography. Hypertension due to renal arteriallesions does not usually have the family historywhich frequently occurs with malignant hyperten-sion, which is commonest in the fourth and fifthdecades, and it is rapidly progressive. There maybe a slight diminution in the kidney size on intra-venous pyelography. Evidence of vascular in-sufficiency in the lower limbs and inability tomaintain an erectionmay suggest aortic thrombosis.Gellman (1958), in summarizing the views of
Poutasse and Dustan (1956), gives the followingindications for aortography:-
I. Patients with unexplained disparity in renalsize or function on intravenous pyelo-graphy.
2. Young patients with no family history ofhypertension and no other primary cause.
3. Elderly patients with rapidly progressivehypertension.
4. Patients with rapidly progressive hyperten-sion, particularly when associated withpain in the flank.
These indications are only relative in the lightof present rather small experience and it isprobable that they will need modification asfurther experience is gained. As atheroma is socommon in patients of the malignant-hypertensionage-group it might be expected that atheromatousplaques in the renal artery would be common andthe indication for aortography may becomewidened in this group. Selective renal functiontests following bilateral ureteric catheterizationmay be of value, with the measurement of plasmaclearances, water and electrolyte excretion.Howard, Connor and Thomas (1956) found that
by copyright. on 12 July 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.409.644 on 1 Novem
ber 1959. Dow
nloaded from
646 POSTGRADUAT'E MEDICAL JOURNAL November 1959
... ...
...........:ie.:X,..:.
.::~.. ... ...:
..:..::..:
:. i.(.......
.i............Z.C: . :: '·
~~. .... ....., ', ,^.i:.:. :: .i.i......
.....? .:.:...;...
!!: - - .. ..;;..:
j-..."0;-IX~~~O ilP
~~~~~~~~~·r-,>...>,,,-t'iX.
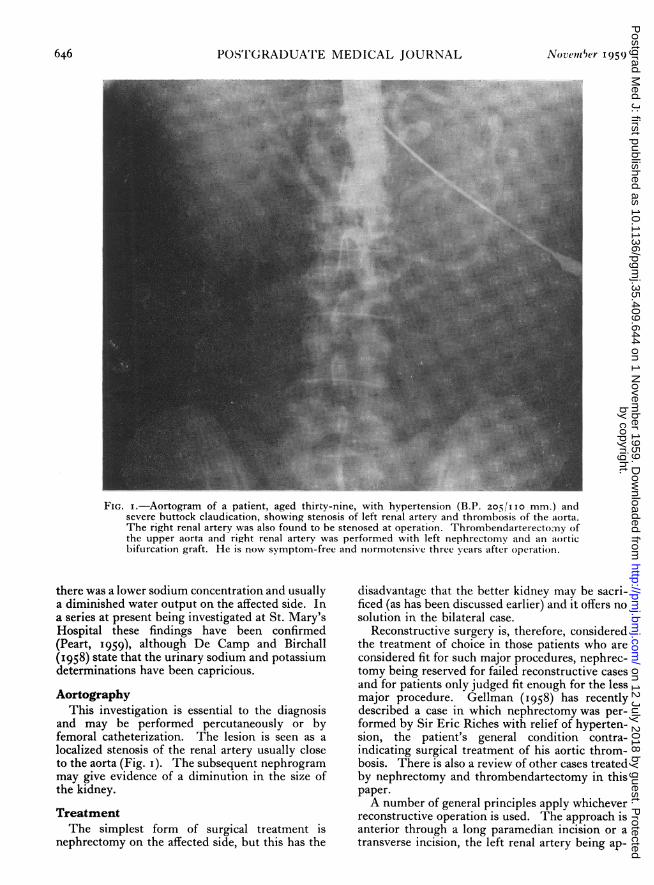
FIG. i.-Aortogram of a patient, aged thirty-nine, with hypertension (B.P. 205/IO mm.) andsevere buttock claudication, showing stenosis of left renal artery and thrombosis of the aorta.The right renal artery was also found to be stenosed at operation. Thrombendarterectomv ofthe upper aorta and right renal artery was performed with left nephrectomv and an aorticbifurcation graft. He is now symptom-free and normotensive three years after operation.
there was a lower sodium concentration and usuallya diminished water output on the affected side. Ina series at present being investigated at St. Mary'sHospital these findings have been confirmed(Peart, I959), although De Camp and Birchall(1958) state that the urinary sodium and potassiumdeterminations have been capricious.Aortography
This investigation is essential to the diagnosisand may be performed percutaneously or byfemoral catheterization. The lesion is seen as alocalized stenosis of the renal artery usually closeto the aorta (Fig. i). The subsequent nephrogrammay give evidence of a diminution in the size ofthe kidney.TreatmentThe simplest form of surgical treatment is
nephrectomy on the affected side, but this has the
disadvantage that the better kidney may be sacri-ficed (as has been discussed earlier) and it offers nosolution in the bilateral case.
Reconstructive surgery is, therefore, consideredthe treatment of choice in those patients who areconsidered fit for such major procedures, nephrec-tomy being reserved for failed reconstructive casesand for patients only judged fit enough for the lessmajor procedure. Gellman (1958) has recentlydescribed a case in which nephrectomy was per-formed by Sir Eric Riches with relief of hyperten-sion, the patient's general condition contra-indicating surgical treatment of his aortic throm-bosis. There is also a review of other cases treatedby nephrectomy and thrombendartectomy in thispaper.A number of general principles apply whichever
reconstructive operation is used. The approach isanterior through a long paramedian incision or atransverse incision, the left renal artery being ap-
by copyright. on 12 July 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.409.644 on 1 Novem
ber 1959. Dow
nloaded from

OWEN: Renal Artery Ste;osis
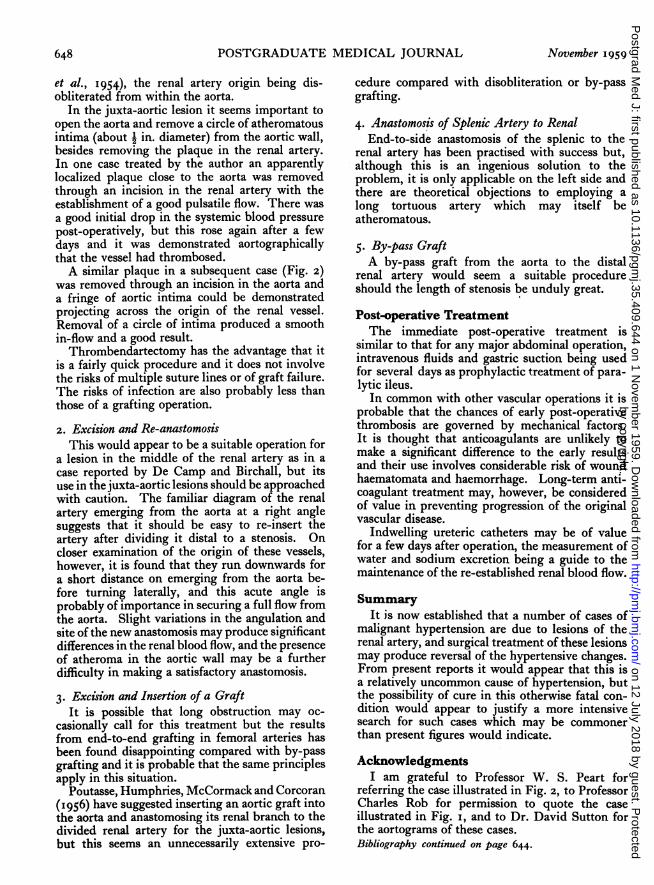
FIG. 2.-Right renal arteriogram of a patient, aged forty-eight, who presentedwith visual changes and had a severe hypertension (B.P. 290/150 mm.).There was a diminution in the size and excretory power of the right kidneyon intravenous pyelography, and the renal arteriogram shows a stenosis of theright renal artery. This vessel was disobliterated from within the aorta with amarked post-operative drop in the blood pressure (B.P. 170/100 mm.).
proached by dissecting between the spleen andsplenic flexure and retracting the spleen and pan-creas upwards and to the right. The right renalartery is displayed by reflecting the duodenum andpancreas to the left.The pressures in aorta and renal artery are
measured, the demonstration of a pressure dropacross the stenosis being the final step in thediagnosis. If a pressure drop is not found, thehypertension is unlikely to be due to the arteriallesion. It seems wise to take biopsy specimensfrom both kidneys in order to assess prognosisand the advisability of any further treatment suchas nephrectomy should the reconstructive opera-tion fail. Hypothermia is not necessary in mostcases, although its use may be considered shoulda long grafting operation be considered. Theupper aortic clamp is applied obliquely so that theblood flow to the opposite kidney is not affected.
The following surgical procedures have beensuggested and successes have been recorded withmost of them:-
I. Thrombendarectomy.2. Excision of stenosed segment and end-to-end
anastomosis or re-anastomosis to aorta.3. Excision and insertion of a graft.4. Anastomosis of splenic or colic artery, end-
to-side, to the renal artery distal to thestenosis.
5. By-pass arterial homograft from aorta todistal renal artery.
I. ThrombendarectomyThis is the operation of choice in cases of
Leriche syndrome (Rob, Eastcott and Owen, 1956)and has given some of the earlier successes inconcomitant renal artery obstruction (Freeman
November 1959 647
by copyright. on 12 July 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.409.644 on 1 Novem
ber 1959. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
et al., 1954), the renal artery origin being dis-obliterated from within the aorta.
In the juxta-aortic lesion it seems important toopen the aorta and remove a circle of atheromatousintima (about i in. diameter) from the aortic wall,besides removing the plaque in the renal artery.In one case treated by the author an apparentlylocalized plaque close to the aorta was removedthrough an incision in the renal artery with theestablishment of a good pulsatile flow. There wasa good initial drop in the systemic blood pressurepost-operatively, but this rose again after a fewdays and it was demonstrated aortographicallythat the vessel had thrombosed.A similar plaque in a subsequent case (Fig. 2)
was removed through an incision in the aorta anda fringe of aortic intima could be demonstratedprojecting across the origin of the renal vessel.Removal of a circle of intima produced a smoothin-flow and a good result.Thrombendartectomy has the advantage that it
is a fairly quick procedure and it does not involvethe risks of multiple suture lines or of graft failure.The risks of infection are also probably less thanthose of a grafting operation.2. Excision and Re-anastomosis
This would appear to be a suitable operation fora lesion in the middle of the renal artery as in acase reported by De Camp and Birchall, but itsuse in the juxta-aortic lesions should be approachedwith caution. The familiar diagram of the renalartery emerging from the aorta at a right anglesuggests that it should be easy to re-insert theartery after dividing it distal to a stenosis. Oncloser examination of the origin of these vessels,however, it is found that they run downwards fora short distance on emerging from the aorta be-fore turning laterally, and this acute angle isprobably of importance in securing a full flow fromthe aorta. Slight variations in the angulation andsite of the new anastomosis may produce significantdifferences in the renal blood flow, and the presenceof atheroma in the aortic wall may be a furtherdifficulty in making a satisfactory anastomosis.
3. Excision and Insertion of a GraftIt is possible that long obstruction may oc-
casionally call for this treatment but the resultsfrom end-to-end grafting in femoral arteries hasbeen found disappointing compared with by-passgrafting and it is probable that the same principlesapply in this situation.
Poutasse, Humphries, McCormack and Corcoran(1956) have suggested inserting an aortic graft intothe aorta and anastomosing its renal branch to thedivided renal artery for the juxta-aortic lesions,but this seems an unnecessarily extensive pro-
cedure compared with disobliteration or by-passgrafting.4. Anastomosis of Splenic Artery to Renal
End-to-side anastomosis of the splenic to therenal artery has been practised with success but,although this is an ingenious solution to theproblem, it is only applicable on the left side andthere are theoretical objections to employing along tortuous artery which may itself beatheromatous.
5. By-pass GraftA by-pass graft from the aorta to the distal
renal artery would seem a suitable procedureshould the length of stenosis be unduly great.Post-operative TreatmentThe immediate post-operative treatment is
similar to that for any major abdominal operation,intravenous fluids and gastric suction being usedfor several days as prophylactic treatment of para-lytic ileus.
In common with other vascular operations it isprobable that the chances of early post-operativethrombosis are governed by mechanical factors.It is thought that anticoagulants are unlikely tomake a significant difference to the early resultsand their use involves considerable risk of woundhaematomata and haemorrhage. Long-term anti-coagulant treatment may, however, be consideredof value in preventing progression of the originalvascular disease.
Indwelling ureteric catheters may be of valuefor a few days after operation, the measurement ofwater and sodium excretion being a guide to themaintenance of the re-established renal blood flow.
SummaryIt is now established that a number of cases of
malignant hypertension are due to lesions of therenal artery, and surgical treatment of these lesionsmay produce reversal of the hypertensive changes.From present reports it would appear that this isa relatively uncommon cause of hypertension, butthe possibility of cure in this otherwise fatal con-dition would appear to justify a more intensivesearch for such cases which may be commonerthan present figures would indicate.
AcknowledgmentsI am grateful to Professor W. S. Peart for
referring the case illustrated in Fig. 2, to ProfessorCharles Rob for permission to quote the caseillustrated in Fig. i, and to Dr. David Sutton forthe aortograms of these cases.Bibliography continued on page 644.
648 November 1959
by copyright. on 12 July 2018 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.35.409.644 on 1 Novem
ber 1959. Dow
nloaded from