gyorgy frendl, md, phd peri-operative management of patients for complex thoracic surgery gyorgy...
TRANSCRIPT

Gyorgy Frendl, MD, PhD
Peri-Operative Management ofPatients for Complex Thoracic Surgery
Gyorgy Frendl, MD, PhD, FCCM
Associate Professor of Anesthesiology and Critical Care, Harvard Medical School
Director of Research, Surgical Critical Care, Brigham and Women’s Hospital
November 21-22, 2014Kuwait

Gyorgy Frendl, MD, PhD
Ann Intern Med. 2006;144:581-595.

Gyorgy Frendl, MD, PhD
Types of Thoracic Surgical ProceduresEsophageal Procedures:• Esophagoscopy/PEG/Esophageal Dilation
• Laparoscopic Nissen Fundal Plication/Myotomy
• Zenker's Diverticulectomy
• Esophagectomy (Iwory-Lewis vs Three Hole)
Other:• Pericardial Window
Intra-Thoracic/Airway Procedures: Minor procedures:
• Flexible Bronchoscopy• Photodynamic Therapy (PDT)• Tracheal Stents
Procedures with moderate stress:· Ridgid Bronchoscopy· Mediastinoscopy (Cervical or Anterior)· Thoracoscopic/Video Assisted Thoracoscopic (VAT) Wedge Resection· Bronchoscopic LASER Surgery· Tracheostomy· Thoracoscopic Sympathectomy
Major procedures:· Anterior Mediastinal mass/Thymectomy· Thoracoscopic/Video Assisted Thoracoscopic (VAT) Lobectomy· Open Thoracotomy for Lobectomy/Segmentectom· Tracheal Resection and Reconstruction/Carinal Resection· Pneumonectomy, Extrapleural Pnuemonectomy (EPP), Pleurectomy· EPP with Heated Chemotherapy and Protocol· Volume Reduction/Bullectomy· Bronchopleural Fistula Repair· Pleuroscopy, Pleurodesis, Poudrage, and Decortication· Clagget Window· Lung Transplantation
Gyorgy Frendl, MD, PhD
Most Common Thoracic Surgical Procedures
Bronchoscopy & Cervical Mediastinoscopy
Thoracoscopy and/or VATS
Thoracotomy for Lobectomy or Pneumonectomy
Laproscopic GE Junction procedures (Nissen Fundoplication, Heller Myotomy)
Esophagectomy

Gyorgy Frendl, MD, PhD
Peri-Operative Atrial Fibrillation after Thoracic Surgery
Atrial Fibrillation
Wedge Resection < 4%Lobectomy/Pneumonactomy
12.5-33%
Esophagectomy 13-25%Lung Transplant 39%

Gyorgy Frendl, MD, PhD
Risk of 30 Day Mortality after Lung Cancer Resection
Risk Variable OR
Sex Male > Female 1.76
Age
>70 3.38
>80 9.94
Side Rt > Lt 1.73
Procedure Bi-Lobectomy 3.92
Pneumonectomy 4.66
Volume > 20/year 0.76
Gyorgy Frendl, MD, PhD
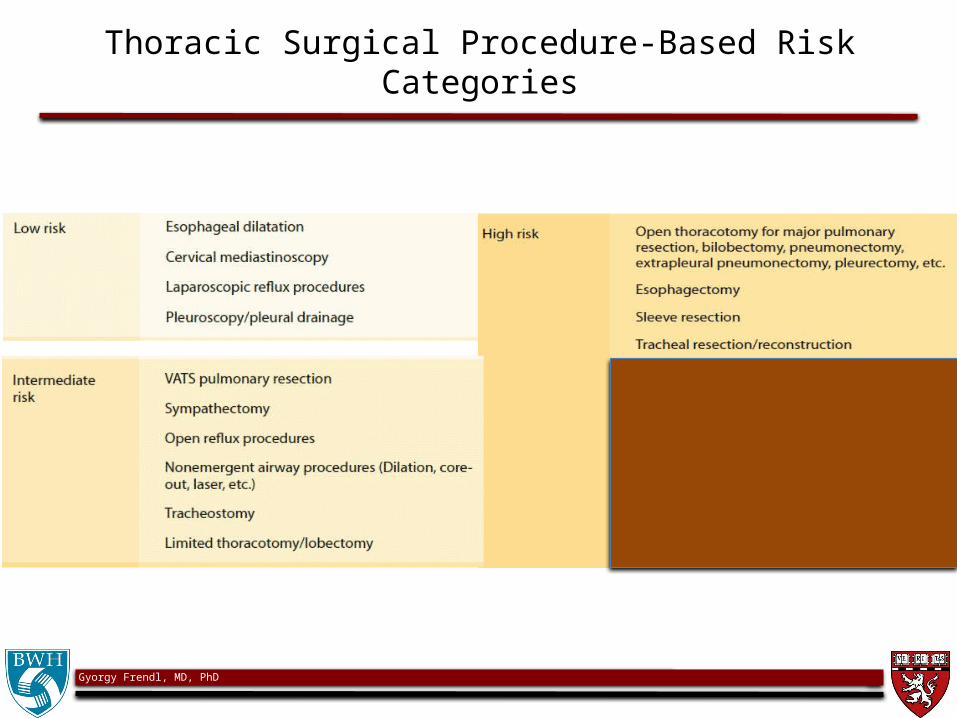
Thoracic Surgical Procedure-Based Risk Categories

Gyorgy Frendl, MD, PhD
FEV1 < 40% N=70/600

Gyorgy Frendl, MD, PhD
Focus of Pre-Operative Evaluation

Gyorgy Frendl, MD, PhD
Preoperative Evaluation for Major Thoracic Surgery
J Cardiothorac Vasc Anesth 14:202, 2000
• “Three-Legged”• Stool of
• Pre-Thoracotomy• Respiratory • Assessment
• Respiratory
• Mechanics
• Cardio-Pulmonary• Reserve
• Lung Parenchymal• Function
1. FEV1 (ppo>40%)*
2. MVV, RV/TLC, FVC
1. VO2 max (>15 ml/kg/min)*
2. Stair climb > 2 flights3. 6min Walk Test• Exercise SpO2 <4%
1. DLCO (ppo >40%)*2. PaO2 >60
3. PaCO2<45

Gyorgy Frendl, MD, PhD

Gyorgy Frendl, MD, PhD
Complete Pre-Operative Review
Review:
– The cardio-pulmonary status
– PFTs, level of physical activity, use of inhalers, steroids, home O2
– Chest radiograms, CTs (tumor size, location, degree of COPD, abscess, etc)• pictures can tell a thousand words!
– Prior anesthetic (also airway) history
Gyorgy Frendl, MD, PhD
Preoperative Management Prior to Major Thoracic Surgery
• Smoking cessation (6-8 weeks prior)• Increase physical activity, teach deep breathing exercise• Cardiac evaluation (Peri-op beta blockade, ?EF, RV, PAP)
– Risk for arrhythmias?• Degree of COPD – effective treatment (inhalers, abx)• Manage symptoms of paraneoplastic syndromes• Pre-operative imaging
– Airway compression?– Local extension?
• Predisposition to hypoxemia• Pulmonary consolidation, atelectasis, pleural effusions

Gyorgy Frendl, MD, PhD
Intra-Operative Management
• Induction and maintenance of anesthesia– appropriate for pt’s condition and surgery
• Airway – effective lung isolation techniques• Monitoring strategies• IV access• Fluid management• Pain management (intra-op, post-op)

Gyorgy Frendl, MD, PhD
Inhalational Agents vs. TIVA

Gyorgy Frendl, MD, PhD
Absolute indications for lung isolation
Gyorgy Frendl, MD, PhD
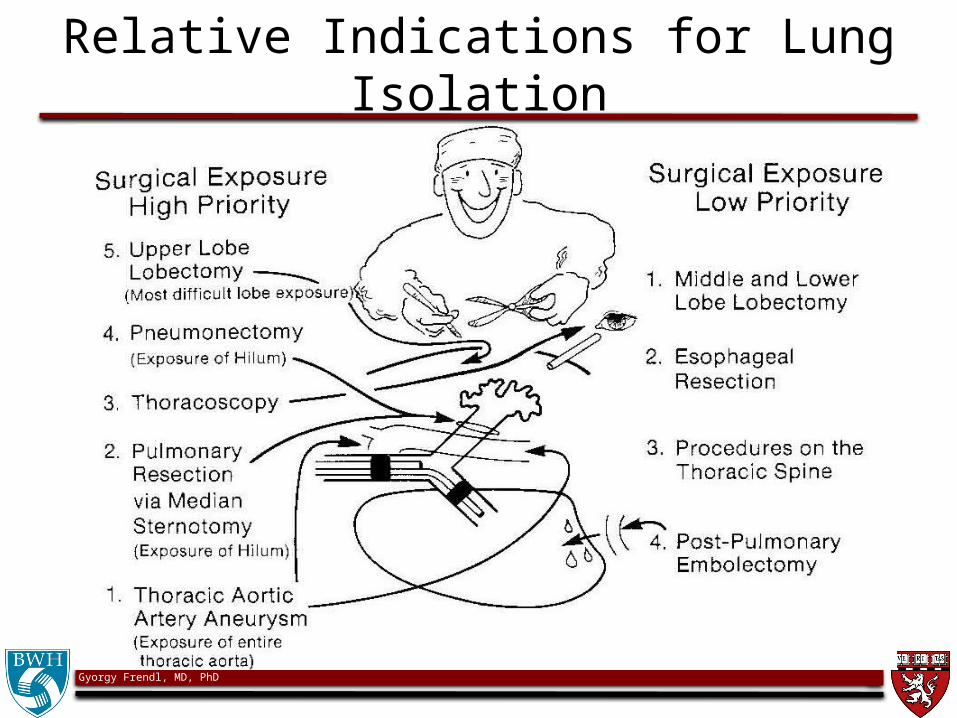
Relative Indications for Lung Isolation

Gyorgy Frendl, MD, PhD

Gyorgy Frendl, MD, PhD
Physiology of Hypoxic Pulmonary Vasoconstriction
• Localized pulmonary vasoconstriction occurs in response to alveolar hypoxia
• Diverts blood away from poorly ventilated areas
• Exposure to chronic hypoxia (e.g. chronic lung disease) results in chronic vasoconstriction, vascular remodeling, and pulmonary hypertension

Gyorgy Frendl, MD, PhD
Factors Inhibiting HPVNote: This will Increase Blood Flow to Operative Lung
• Very high PA pressures– Already bilaterally vasoconstricted
• Hypocapnia (low PaCO2)• Acidosis • High mixed venous PO2
• Intravenous vasodilators– TNG, SNP, Beta-agonists, Ca-channel blockers, Minoxidil, Theophylline,
Prostaglandin E1
– (Contrast: B-blockers and COX-inhibitors enhance HPV)• Inhalational anesthetics (esp. when > 1 MAC)
• All of these may inhibit vasoconstriction in the operative lung, leading to increased shunt
Gyorgy Frendl, MD, PhD
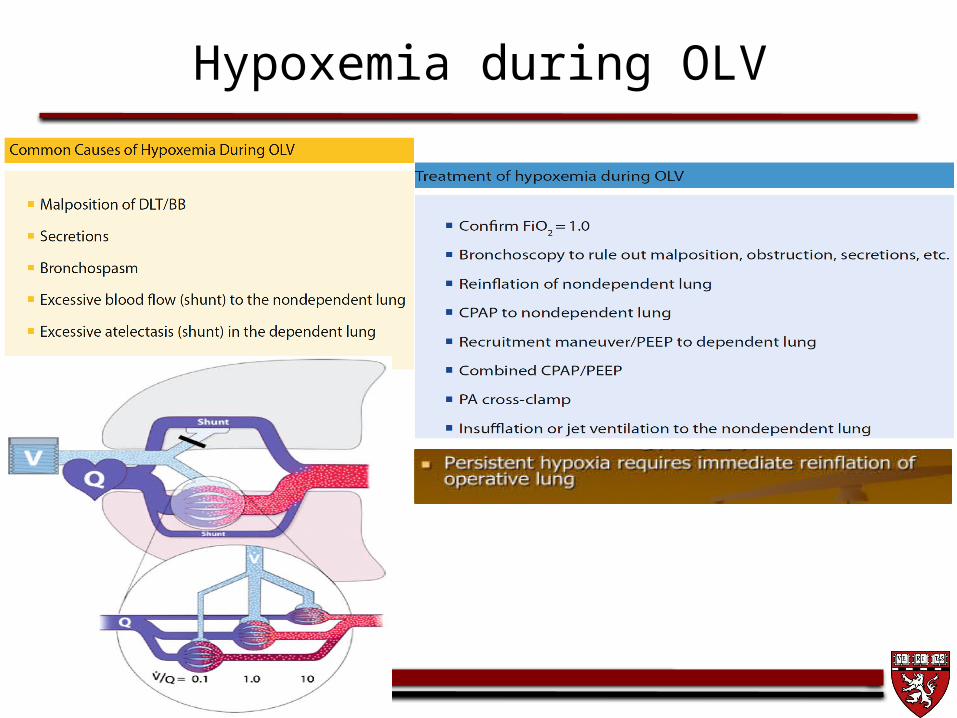
Hypoxemia during OLV

Gyorgy Frendl, MD, PhD
Anesthetic Goals for ALL Pulmonary Resections
• Safe induction – Avoid hypoxemia, hypercarbia, HD instability
• Isolate lungs to provide motionless operative field• Satisfactory oxygenation and ventilation – Using the non-operative lung
• Appropriate invasive monitors and access• Appropriate management of FEN and blood products• Hemodynamic stability• Prompt wean from mechanical ventilation• Effective postoperative pain management

Gyorgy Frendl, MD, PhD
Lung Transplantation

Gyorgy Frendl, MD, PhD
Laparoscopic GE Junction Procedures
• Similar to other intra-abdominal laparoscopic procedures
• Often done for pre-transplant patients, chronic aspirators (NB: poor lung function)– Epidurals are mandatory for patients that are
pulmonary “cripples” (adjuncts like a-line, bronchodilators, TIVA, reverse-able level of muscle relaxation maybe needed)

Gyorgy Frendl, MD, PhD
Lung Volume Reduction Surgery (LVRS)• Performed for severe COPD• Patients have – Severe airway obstruction– Enlarged thorax >> disrupts respiratory mechanics
• Increased TLC, RV• Decreased FEV1• Increased work of breathing
• Severe emphysema– FEV1 < 0.75 L – 1 year mortality 30%

Gyorgy Frendl, MD, PhD
Anesthetic Technique for LVRS
• Premedications: minimal to none• Lung isolation mandatory
– DLETT allows for both lungs to be sequentially operated on• Large dead space results in anesthetic agent trapping
– Propofol/Remifentanyl TIVA is our standard of care• Despite thoracoscopic incisions, epidural is necessary, may
supplement with NSAIDs• Ventilation parameters:
– Slow RR– Long I:E– Permissive hypercapnia
• May require intermittent reinflation of operative lungs

Gyorgy Frendl, MD, PhD
Overall Risk Mitigation Strategies
• Poor pre-op lung function or very poor functional status– Is the procedure necessary, can the patient improve if procedure is delayed?– Consider regional anesthesia (alone or with GA), minimize narcotics– TIVA, Minimal muscle relaxants – wait for full recovery– Higher level of criteria for extubation (alert, cooperative, good strength,
adequate MV and ET CO2)– If not meeting criteria, delay extubation (PACU, ICU) – If acceptable, consider post-op NIPPV
• Major blood loss– Sufficient IV / central access– A-line for monitoring/labs– Blood in the OR, readily available– High flow systems to transfuse with temperature control– Helping hands
Gyorgy Frendl, MD, PhD
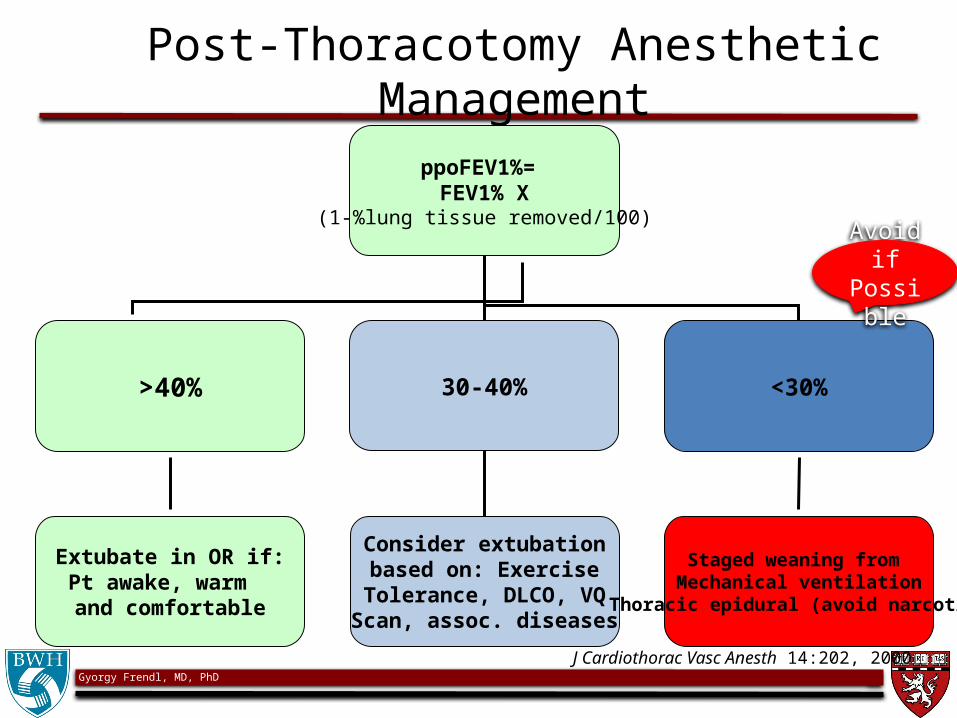
Post-Thoracotomy Anesthetic Management
ppoFEV1%= FEV1% X
(1-%lung tissue removed/100)
>40% 30-40% <30%
Extubate in OR if:Pt awake, warm and comfortable
Consider extubationbased on: Exercise
Tolerance, DLCO, VQScan, assoc. diseases
Staged weaning from Mechanical ventilation
Thoracic epidural (avoid narcotics)
J Cardiothorac Vasc Anesth 14:202, 2000
Avoid if Possible

Gyorgy Frendl, MD, PhD
Post-Op

Gyorgy Frendl, MD, PhD
Summary
• The patients usually have complex co-morbidities• The procedures are complex• Patients almost never improve their pulmonary
function (often worsen) post procedure• Communication with surgeons, pulmonary
specialists, and nurses is essential• Set realistic expectations for patients and families• Pre- and post-op physico-therapy and pulmonary
rehab is essential• Just do your best!

Gyorgy Frendl, MD, PhD
Thank You!
Questions?
Gyorgy Frendl, MD, PhD
Anesthetic Goals for BPF Patients
• Minimize airflow across the fistula
– decrease airway pressures during inspiration, decrease mean intra-thoracic pressures
• Adequate gas exchange in the un-affected lung
• Avoid tension PTX
• Protect the remaining (healthy) lung from contamination (as BPF spaces are always infected)
• Expansion of the remaining ipsilateral lung after the procedure

Gyorgy Frendl, MD, PhD
Broncho-Pleural Fistula – Anesthetic Strategies

Gyorgy Frendl, MD, PhD
Anesthetic Considerations for BPFs
• Water seal chest tubes for induction – Large BPF may make ventilation impossible ( risk of PTX)
• Chose appropriate induction strategy– inhalation induction vs. awake fiberoptic ETT insertion vs. awake
LMA vs. asleep induction (short acting meds)– Single lumen ETT vs. DLT
• Place ETT so it excludes (isolates) fistula to:– Allow Independent lung ventilation– Allow positive pressure ventilation (bronchoscopy for ETT position)– Avoid cross-contamination (turn fistula-side down/dependent
position)
• Consider high frequency ventilation if safe lung isolation is not feasible

Gyorgy Frendl, MD, PhD
Recommended Risk Reduction Strategies

Gyorgy Frendl, MD, PhD
Bronchoscopy / Cervical Mediastinoscopy
• These are “chip-shot” ambulatory cases, right?– About once a year, they biopsy the pulmonary artery
• The mediastinoscope can compress the right innominate artery– Obtain large bore IV access (even though they go home
the same day) & ensure Blood Type & Screen is done– Place the IV and pulse oximeter on the RIGHT, BP cuff can
go on the left– IV will need extension tubing– You won’t have access to the patient to monitor twitches
• Err on the side of deep paralysis – the patients should not move at the time of the surgeon biopsying near vital organs

Gyorgy Frendl, MD, PhD
Thoracoscopic Lung Resection and VAT
• Generally small incisions, VAT incisions can be larger– Thoracoscopic Lung Resection >> keyhole– VAT >> keyhole + mini thoracotomy
• Maybe segmentectomy or lobectomy
• Depending on pulmonary function, may consider:– A-line pre-op (or after induction)– Placing pre-op epidural, especially for VAT– Consider TIVA (based on residual lung function)
Gyorgy Frendl, MD, PhD
Strategies for Open Lobectomies and Pneumonectomies
• Strategies:– Pre-op large bore IVs, thoracic epidural and a-line– Test the level after test dose, before you induce– Central venous or Swan-Gants/PA catheter– Lung isolation (DLL ETT)
• Plan an anesthetic most likely to extubate from– Proprofol / Vecuronium / Desflurane /
Remifentanil / Epidural analgesia

Gyorgy Frendl, MD, PhD
Anterior Mediastinal Mass

Types of Masses
• Anterior Mediastinum1. Thymoma2. Mesenchymal tumors3. Dermoid cysts4. Lymphoma 5. Thyroid/parathyroid tumors
• Middle Mediastinum1. Pericardial cysts2. Bronchogenic cysts3. Lymphomas
• Posterior Mediastinum1. Neurogenic and enterogenous tumors/cysts2. Aortic aneurysms3. Paravertebral abscesses
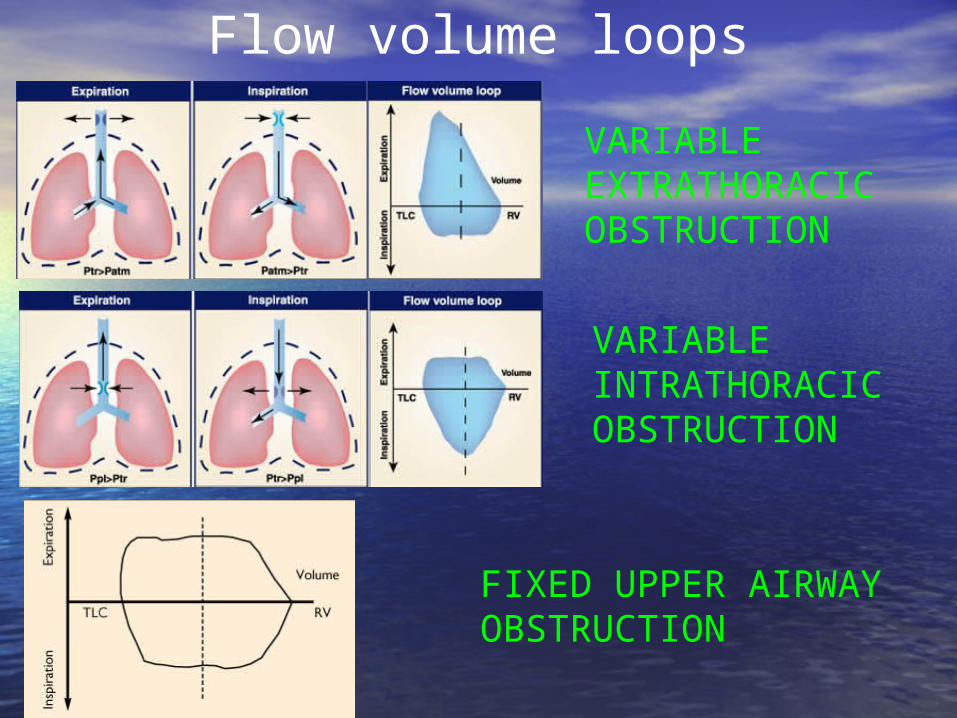
Flow volume loops
VARIABLE EXTRATHORACIC OBSTRUCTION
VARIABLE INTRATHORACIC OBSTRUCTION
FIXED UPPER AIRWAY OBSTRUCTION
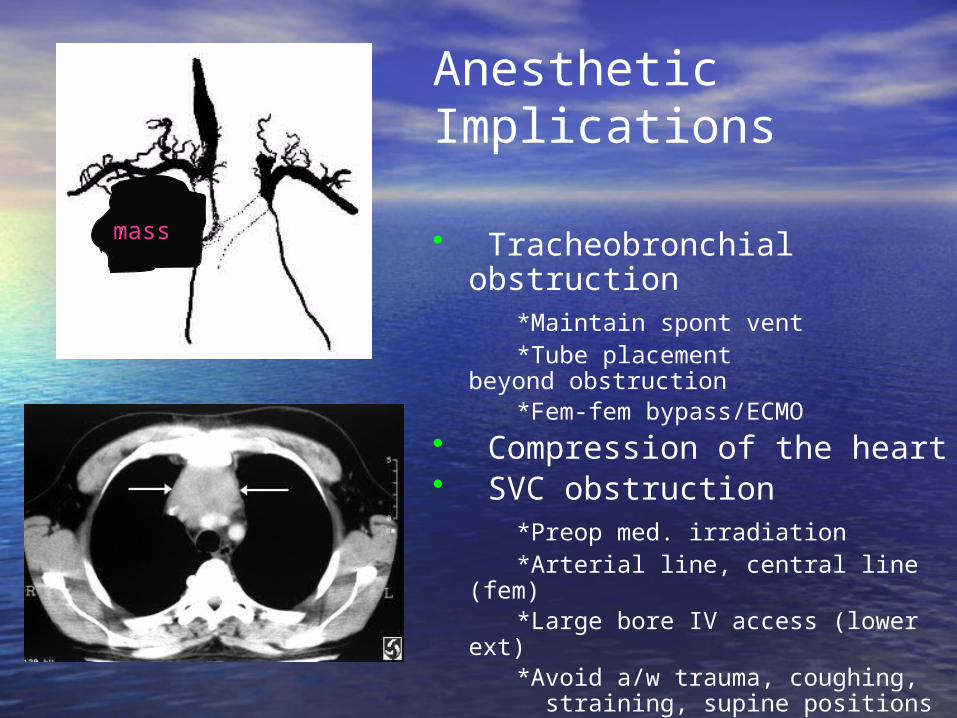
Anesthetic Implications
• Tracheobronchial obstruction*Maintain spont vent*Tube placement
beyond obstruction*Fem-fem bypass/ECMO
• Compression of the heart• SVC obstruction
*Preop med. irradiation*Arterial line, central line (fem)*Large bore IV access (lower
ext)*Avoid a/w trauma, coughing,
straining, supine positions• Myasthenia Gravis
mass
Gyorgy Frendl, MD, PhD
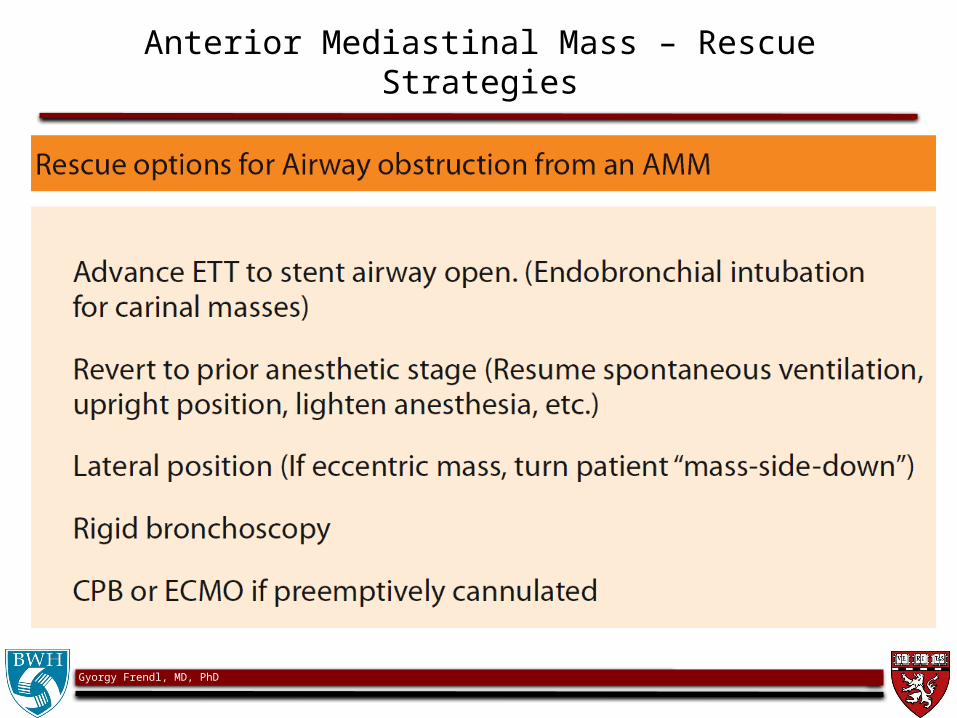
Anterior Mediastinal Mass – Rescue Strategies

Gyorgy Frendl, MD, PhDAnn Intern Med. 2006;144:581-595.

Gyorgy Frendl, MD, PhD
Outcomes after Thor Surg Procedures