h o n o r i n g t h e f a l l e n . h o n r a n d o a l o
TRANSCRIPT
HONRANDO A LOS CAÍDOS. HONORING THE FALLEN.
A N N D L O N R E P O R T O N T H E I M P A C T S O F T H EG L O B A L C O V I D 1 9 P A N D E M I C O N I M M I G R A N TW O R K E R S A N D P E O P L E O F C O L O R I N T H E U N I T E DS T A T E S
P U B L I S H E D B Y T H E N A T I O N A L D A YL A B O R E R O R G A N I Z I N G N E T W O R K( N D L O N ) O N W O R K E R S M E M O R I A L D A Y ,A P R I L 2 8 , 2 0 2 1
Workers’ Memorial Day—the Dayof the Fallen Worker—provides asomber moment to reflect onthe devastating toll the COVID-19 pandemic has taken onimmigrant workers and peopleof color throughout the UnitedStates.
In April 2021, deaths in the USfrom COVID-19 surpassed570,000, a grim milestone thatmarks the consequences ofleadership failures, mixedmessaging, and inadequateemergency preparedness.
Immigrantcommunities andpeople of colorhave shouldered adisproportionateshare of COVID-19deaths, revealingonce again howdeepsocioeconomicdivisions are thefoundation of vasthealth disparities.
INTRODUCTION
WORKERS DEEMEDESSENTIAL YET
EXCLUDED Today, undocumentedimmigrant workerssubsidize variousindustries across the USeconomy. The reality ofreliance on undocumentedlabor, predominantlyBlack, Brown, Asian, andIndigenous became evidentduring the peak of thepandemic in the US, as didthe disproportionateimpact - and number ofdeaths - of undocumentedworkers.
A report issued by theUS Congress JointEconomic Committeemakes clear both thesignificant economiccontributions made byforeign-born workersand the heightenedrisks they face duringthe ongoing pandemic:[1]
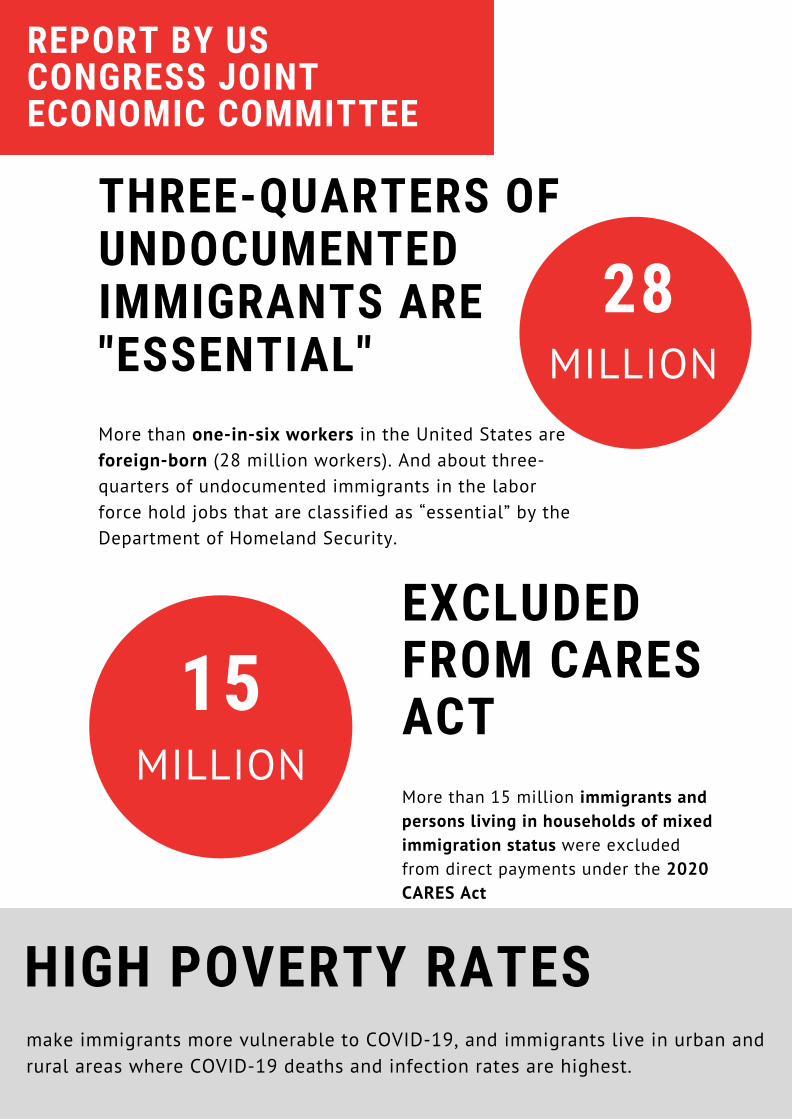
THREE-QUARTERS OFUNDOCUMENTEDIMMIGRANTS ARE"ESSENTIAL"More than one-in-six workers in the United States areforeign-born (28 million workers). And about three-quarters of undocumented immigrants in the laborforce hold jobs that are classified as “essential” by theDepartment of Homeland Security.
15MILLION
EXCLUDEDFROM CARESACTMore than 15 million immigrants andpersons living in households of mixedimmigration status were excludedfrom direct payments under the 2020CARES Act
HIGH POVERTY RATES make immigrants more vulnerable to COVID-19, and immigrants live in urban andrural areas where COVID-19 deaths and infection rates are highest.
28MILLION
REPORT BY USCONGRESS JOINTECONOMIC COMMITTEE
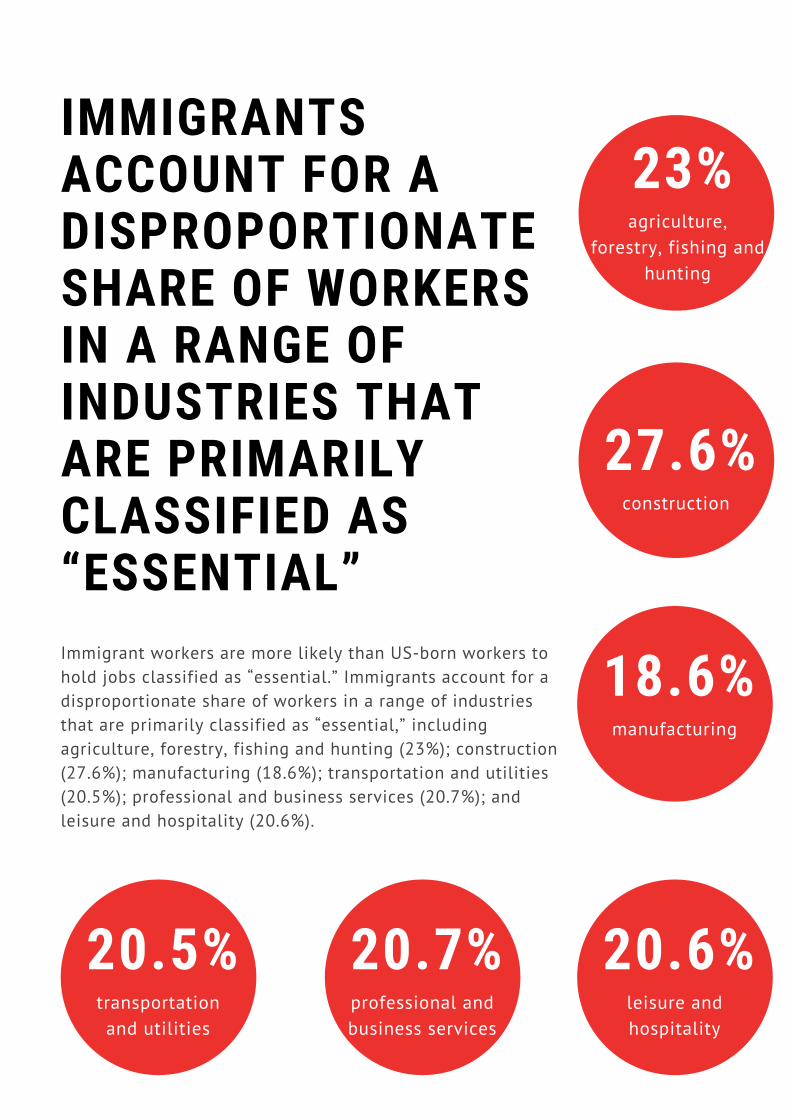
IMMIGRANTSACCOUNT FOR ADISPROPORTIONATESHARE OF WORKERSIN A RANGE OFINDUSTRIES THATARE PRIMARILYCLASSIFIED AS“ESSENTIAL”Immigrant workers are more likely than US-born workers tohold jobs classified as “essential.” Immigrants account for adisproportionate share of workers in a range of industriesthat are primarily classified as “essential,” includingagriculture, forestry, fishing and hunting (23%); construction(27.6%); manufacturing (18.6%); transportation and utilities(20.5%); professional and business services (20.7%); andleisure and hospitality (20.6%).
23%agriculture,
forestry, fishing andhunting
27.6%construction
20.5%transportationand utilities
20.7%professional andbusiness services
20.6%leisure andhospitality
18.6%manufacturing

REPORT BY US CONGRESSJOINT ECONOMIC COMMITTEE
Although the US Centers for Disease Control and Prevention (CDC) does notissue data on COVID-19 infection and mortality rates by citizenship statusor country of origin, media reports issued over the past year have signaledthat a number of industries with large shares of immigrant workers haveexperienced high rates of infection and death, as workplaces have becomecoronavirus “hotspots” where employees work in close quarters, often withwoefully inadequate protection. Undocumented immigrant workers, who areemployed in essential industries in disproportionate numbers, are withoutquestion at heightened risk of contracting COVID-19.[2]
POLICIES OF EXCLUSION UNDERMINE PUBLIC HEALTHThe vulnerabilities faced by immigrantworkers during the pandemic, however,are not restricted to theirdisproportionate rates of employmentin key economic sectors. It is widelyacknowledged that immigration statusitself is a social determinant of health,with undocumented residents andmembers of mixed-status householdsparticularly susceptible toexperiencing a range of negativehealth impacts.[3],[4],[5]
Castañeda and colleagues explain, “Being animmigrant limits behavioral choices and,indeed, often directly impacts and significantlyalters the effects of other social positioning,such as race/ethnicity, gender, orsocioeconomic status, because it placesindividuals in ambiguous and often hostilerelationships to the state and its institutions,including health services.”[6] Key behavioralchoices include health service utilization, aswell as accessing preventative care anddiagnostic procedures.

POLICIES OFEXCLUSIONUNDERMINEPUBLIC HEALTH Although behavioral models tend tofocus on individual-level decision-making, it must be recognized thatindividual decisions regardingwhether to access care, for example,are made within societal structuresthat in turn are shaped by publicpolicy, economic status, and theavailability of healthcare services.Therefore, it is likely that the“ambiguous and often hostilerelationships to the state and itsinstitutions” described by theauthors are even more damaging toimmigrants’ health outcomes.
The social positioning of immigrants,and its intersections with markers ofrace, has been incorporated intoanti-immigrant discourses thatjustify punitive public policies thatdirectly and indirectly restrictimmigrant families’ access to publicservices.[7]
Local anti-immigration policies,which have proliferated across theUS in recent years,[8] provide a casein point.
Anti-immigrationpolicies that havebeen enacted bymunicipalities andcounties have beenfound to havesignificant negativeeffects on health.[9],[10],[11],[12],[13]
There are several factors related tothe passage of restrictionist policiesthat negatively impact immigrants’health outcomes, key among theseare avoidance of healthcare servicesdue to fear and mistrust of publicinstitutions.[14],[15],[16],[17]
POLICIES OF EXCLUSIONUNDERMINE PUBLIC HEALTH
Individuals residing “inside or outsidethe U.S. who seek to either obtainLawful Permanent Resident status(apply for immigrant visas and ‘greencards’) or to extend or changenonimmigrant status (temporaryvisas) must now demonstrate thatthey have not received publicbenefits, or have received limitedpublic benefits, with [few]exceptions.”[19]
These problems are compounded bypolicies such as draconian “publiccharge” rules that have beenauthorized by the federalgovernment. On February 24, 2020,just weeks before the coronaviruspandemic struck the US, theDepartment of Homeland Security(DHS) implemented a rule stating thatindividuals applying for USimmigration authorization would beinadmissible if they are deemed“likely at any time to become a publiccharge.”[18] The public benefitsconsidered by DHS include anyfederal, state, local, or tribal cashbenefit programs for incomemaintenance, Temporary Assistancefor Needy Families, SupplementalNutrition Assistance Program(formerly known as food stamps), andSection 8 housing assistance.
The deterrence effect of publiccharge rules has been strong, as“Immigrants aspiring to becomeU.S. citizens [do] not want to riskthat they or their children mightbe considered inadmissible,deported, or unable to naturalizebecause they [are] considered‘public charges.’”[20]
ADELIBERATESTRATEGY OFATTRITION
Deterring immigrants from accessingservices is not limited to the realmof government benefits. Fears ofapprehension by immigrationauthorities have dissuaded manyimmigrants from receiving COVID-19testing and treatment, placingthemselves, their families, and thewider community at risk.[21] Indeed,after eight years of Barack Obamafailing to achieve immigration reformand four years of Donald Trumpusing the U.S. government toterrorize immigrant families, theimpact on immigrant communities ofcolor nationwide - and theirperceptions of government - aremassive and incalculable.
To be clear, many of these policiesare new manifestations of an old“attrition through enforcement”strategy promoted by anti-immigranthardliners who seek to makeresidence in the US untenable byexcluding unauthorized immigrantsand their families from publicinstitutions and community supportsystems.[22],[23]
As a result of policies ofexclusion, and the fearsthey are intended tostoke, anti-immigrationpolicy has played anoutsized role inimpeding immigrants’access to public andprivate resources thatcould help them bettercope with the pandemic.
In sum, the very idea of “attritionthrough enforcement” was toencourage self-deportation bymaking it impossible for immigrantfamilies to access the very means ofsurvival, and the pandemic brought abrutal and unconscionable goal to itslogical conclusion.
DISPROPORTIONATE IMPACTON COMMUNITIES OF COLOR
As the pandemic deepened, publichealth researchers issued direwarnings about thedisproportionate impacts COVID-19 were having on communitiesof color. For example, KaiserFamily Foundation and the EpicHealth Research Network foundthat “Black, Hispanic, and Asianpatients had significantly higherrates of infection, hospitalization,and death compared to theirWhite counterparts,” and thatracial disparities “inhospitalization and deathpersisted among positive patientseven after controlling for certainsociodemographic factors andunderlying differences inhealth.”[24] The researchersnoted,
The infection rate forHispanic patients was overthree times higher than therate in White patients (143vs. 46 per 10,000), and therate among Black patientswas over two times as high(107 per 10,000). Thehospitalization rate forHispanic patients was morethan four times as high asthe rate in White patients(30.4 vs. 7.4 per 10,000),and the rate in Black patientswas over three times as high(24.6 per 10,000). Deathrates for both groups wereover twice as high as the ratefor White patients (5.6 and5.6 compared to 2.3 per10,000). Asian patients alsofaced significant disparitiesin these measures.
DISPROPORTIONATE IMPACTON COMMUNITIES OF COLOR
Numerous studies have documented racial/ethnic disparities in COVID-19 infections, hospitalizations, deaths, testing, and now vaccinations.[25] According to a recently published report by the U.S. Department ofHealth and Human Services, “Several factors contribute to COVID-19disparities, most stemming from long-standing systemic inequalitiesand structural racism.”[26] The report authors further note, “COVID-19disparities should be studied in the context of resource deprivationcaused by historical and ongoing discrimination, low socioeconomicstatus, and place-based risk factors.”[27] Racial discrimination, fears ofdeportation, crowding in the workplaces of essential industries withoutadequate protection – all are stressors and risk factors that directlysubject immigrants and people of color to premature death.

FINALREFLECTIONSAND REMEDIES The disparities detailed in this report arenot an inevitable result of the COVID-19pandemic. They stem from anti-workerand anti-immigrant public policies andpolitics deliberately advanced at thefederal, state, and local levels thatfacilitate worker abuse and superexploitation, and value profits aboveworker health. It is an agenda that hasensured entire groups of people aredehumanized, demonized, and excluded,implicitly and explicitly, from standardhealth protections.
In order to change this shamefulsituation, federal policymakers mustacknowledge the exclusion and injusticescommitted to undocumented workers andtheir families over the course of multipleadministrations - and govern accordingly.Many of the following recommendationscan be immediately implemented throughadministrative action by President JoeBiden without need for additionalCongressional approval:
1.Protection fromdeportation for workers
who have labored duringthe pandemic, and for the
families of those whohave died.
Society owes a debt of gratitude tothose workers who exposed their
health and to those who lost theirlives in the pandemic. The least that
this country can do is to providethem and their families with a
recognition of their legal personhood- issuing work authorization - as ameaningful recognition of the truly
“essential” nature of their work.
FINAL REFLECTIONS ANDREMEDIES 2.Protection from deportation and workauthorization for undocumented workers whoreport workplace abuse. Workers’ own reports about workplace labor violations to labor agenciesare crucial for enforcement, and to prevent further abuse. However,employers constantly wield the threat, explicitly or implicitly, of ICEdetention and deportation against workers who speak out. Laborwhistleblower protections for immigrants will end the contradictionsand mixed messages that come from a government that punishesworkers that speak out about unsafe workplaces.
3.Worker protection policies such as the overdueCOVID Emergency Temporary Standard must havebroad coverage and aggressive enforcement in order to protect all workers who most need it, with particular focuson industries such as construction, cleaning, restaurant, poultry, andothers that rely on the labor of undocumented immigrant workers. Therecan be no excuse for exploiting workers or endangering their livesduring a crisis.
4.Equal access to all in COVID economic relief,unemployment insurance, funeral support, andvaccination programs.Excluding undocumented workers and families from economic relief isnot only inhumane, but unfair, considering the billions of dollars thatthey have been contributing for years. Immigrant workers and familiesshould be able to access all emergency aid programs without fear ofretaliation or “public charge” repercussions. There should be norequirement to show Social Security numbers or restrictiveidentification requirements for health measures such as testing andvaccines. As a matter of basic public health, society must protect itsmost vulnerable members, in order to ensure that all are protected.
FINAL REFLECTIONS ANDREMEDIES 5.Recognition of the role of workers centers inworkers rights enforcement. Throughout the pandemic, day labor and other workers centers havebeen small but indispensable local hubs for mutual aid, information,food distribution, cash assistance, health referrals, workers rightsenforcement, and now, vaccine distribution. By recognizing theirvaluable role and strategizing together with workers centers, the DOLcan accomplish more: creative coordination of resources, informationgathering for complaints, strategic enforcement against the worstemployers, effective workplace monitoring, and much more.
6.Additional data.It is imperative that a full accounting of the deliberate cruelty imposedby the Trump Administration on immigrant families be documented. Inorder to measure and appreciate the disproportionate impact onimmigrant workers, the Biden Administration should commission anintergovernmental agency to publish data on infection and death ratessuffered specifically by immigrant communities of color.
The pandemic has painfully exposed deep socioeconomicdivisions that fall along lines of race and nationality, evenas it has revealed the country’s reliance on immigrantworkers and people of color to produce goods and servicesthat are essential to the health of the nation. On thisWorkers’ Memorial Day, the losses experienced byimmigrants and communities of color must be honored, andpolicymakers must resolve to end the politics of hate anddivision that have exacted their deadly toll on this country.
For more information on immigrant workers efforts to defend their
dignity, human rights, and workplace protections, visit www.ndlon.org

[1] US Congress Joint Economic Committee. Immigrants, theEconomy and the COVID-19 Outbreak. Washington, DC: U.S.Congress Joint Economic Committee (2020).[2] Kerwin, Donald and Robert Warren. "US Foreign-born workers inthe global pandemic: Essential and marginalized." Journal onMigration and Human Security 8, no. 3 (2020): 282-300.[3] Castañeda, Heide, Seth M. Holmes, Daniel S. Madrigal, Maria-Elena DeTrinidad Young, Naomi Beyeler, and James Quesada."Immigration as a social determinant of health." Annual Review ofPublic Health 36 (2015): 375-392.[4] Gurrola, Maria A., and Cecilia Ayón. "Immigration policies andsocial determinants of health: Is immigrants’ health at risk?" Raceand Social Problems 10, no. 3 (2018): 209-220.[5] Hill, Jessica, Darlene Xiomara Rodriguez, and Paul N. McDaniel."Immigration Status as a Health Care Barrier in the USA duringCOVID-19." Journal of Migration and Health (2021): early view.[6] Castañeda et al., p. 378.[7] Chavez, Leo R. Latino Threat: Constructing Immigrants, Citizens,and the Nation. Stanford, CA: Stanford University Press.[8] Morse, Ann. Report on 2019 State Immigration Laws. Denver:National Conference of State Legislatures (2020).[9] Crookes, Danielle M., Kaitlyn K. Stanhope, Ye Ji Kim, ElizabethLummus, and Shakira F. Suglia. "Federal, state, and local immigrant-related policies and child health outcomes: A systematic review."Journal of Racial and Ethnic Health Disparities (2021): 1-11.[10] Martinez, Omar, Elwin Wu, Theo Sandfort, Brian Dodge, AlexCarballo-Dieguez, Rogeiro Pinto, Scott Rhodes, Eva Moya, and SilviaChavez-Baray. "Evaluating the impact of immigration policies onhealth status among undocumented immigrants: A systematicreview." Journal of Immigrant and Minority Health 17, no. 3 (2015):947-970.
[11] Philbin, Morgan M., Morgan Flake, Mark L. Hatzenbuehler, andJennifer S. Hirsch. "State-level immigration and immigrant-focusedpolicies as drivers of Latino health disparities in the United States."Social Science & Medicine 199 (2018): 29-38.[12] Vargas, Edward D., Gabriel R. Sanchez, and Melina D. Juárez."The impact of punitive immigrant laws on the health of Latina/opopulations." Politics & Policy 45, no. 3 (2017): 312-337.[13] Vernice, Nicholas A., Nicola M. Pereira, Anson Wang, MichelleDemetres, and Lisa V. Adams. "The adverse health effects of punitiveimmigrant policies in the United States: A systematic review." PloSone 15, no. 12 (2020): 1-19.[14] Desai, Sarah, Jessica Houston Su, and Robert M. Adelman."Legacies of marginalization: System avoidance among the adultchildren of unauthorized immigrants in the United States."International Migration Review 54, no. 3 (2020): 707-739.[15] Hagan, Jacqueline, Nestor Rodriguez, Randy Capps, and NikaKabiri. "The effects of recent welfare and immigration reforms onImmigrants' access to health care." International Migration Review37, no. 2 (2003): 444-463.[16] Rhodes, Scott D., Lilli Mann, Florence M. Simán, Eunyoung Song,Jorge Alonzo, Mario Downs, Emma Lawlor et al. "The impact of localimmigration enforcement policies on the health of immigrantHispanics/Latinos in the United States." American Journal of PublicHealth 105, no. 2 (2015): 329-337.[17] Yoshikawa, Hirokazu, and Jenya Kholoptseva. UnauthorizedImmigrant Parents and their Children’s Development. Washington,DC: Migration Policy Institute (2013).[18] US Citizen and Immigration Services [USCIS] (2020) PublicCharge Fact Sheet. Washington, DC: USCIS.[19] Khalid, Najia S. and Ashley Moore. "Immigration and compliancebriefing: COVID-19 summary of government relief and potential“Public Charge Rule” impact on nonimmigrant and immigrant visaapplications." National Law Review 10, no. 133 (2020): May 12.[20] Perreira, Krista M., Robert Crosnoe, Karina Fortuny, JuanPedroza, Kjersti Ulvestad, Christina Weiland, Hirokazu Yoshikawa,and Ajay Chaudry. “Barriers to immigrants’ access to health andhuman services programs." ASPE Issue Brief. Washington, DC: Officeof the Assistant Secretary for Planning and Evaluation (2012).
[21] McFarling, Usha Lee (2020) “Fearing deportation, manyimmigrants at higher risk of Covid-19 are afraid to seek testing orcare,” Stat News (April 15), accessed at:https://www.statnews.com/2020/04/15/fearing-deportation-many-immigrants-at-higher-risk-of-covid-19-are-afraid-to-seek-testing-or-care/.[22] Theodore, Nik. "Policing borders: Unauthorized immigration andthe pernicious politics of attrition." Social Justice 38, no. 1/2 (2011):90-106.[23] Waslin, Michele. Discrediting ‘Self-Deportation’ as ImmigrationPolicy. Washington, DC: Immigration Policy Center (2012).[24] Rubin-Miller, Lily, Christopher Alban, Samantha Artiga andSean Sullivan. COVID-19 Racial Disparities in Testing, Infection,Hospitalization, and Death: Analysis of Epic Patient Data. SanFrancisco: Kaiser Family Foundation (2020).[25] Simmons Adelle, Andre Chappel, Allison R. Kolbe, Laina Bush,and Benjamin D. Sommers. Health Disparities by Race and EthnicityDuring the COVID-19 Pandemic: Current Evidence and PolicyApproaches. Washington, DC: Office of the Assistant Secretary forPlanning and Evaluation, U.S. Department of Health and HumanServices (2021), emphasis added.[26] Ibid., p. 5.[27] Ibid.