h pylori resistance
TRANSCRIPT

H pylori Resistance
Ahmed Alwassief, MD
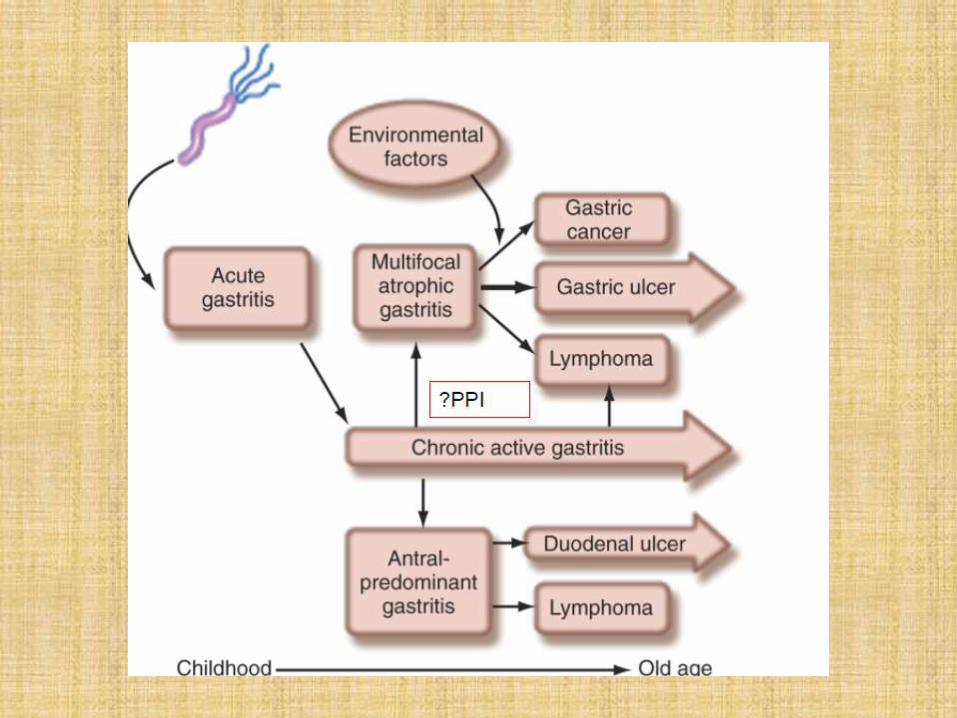
Pathogenesis: Colonization versus Infection
• Present exclusively in humans since the beginning
• Roughly 50% of the world’s population has HP
• Only 20% of this 50% will ever have any HP associated condition
• Linked to several disease processes
• Also inversely associated with some disease processes
• Is/was there some evolutionary advantage to our relationship?
Practice Challenges
• Guidelines vague and variable
• Specialists often reluctant to manage
• Patient questions difficult to answer
• What is the acceptable rate of Tx failure??
>>>> 20%
Health Impact
• Ulcers: 80-95% DU and 70-80% GU
• 80% of Gastric cancers. 6X risk for carrier.
• 3-4X risk of NSAID gastropathy.
• Gastric B-cell Lymphoma (“MALT”)
• Non-Ulcer Dyspepsia
• More suspected -vascular/migraine/autoimmune
• Colon and Pancreatic cancers?
Transmission
• Fecal-Oral
• Oral-Oral/ Dental Plaque/Kissing
• Environmental reservoirs (water/fish?)
• Iatrogenic
• Family contacts
• Still poorly understood

• Formerly Campylobacter• Ulcer link 1982 by
Australians J. Robin Warren (Pathologist), and Barry Marshall, MD.
• Marshall dramatically demonstrated Koch’s postulates by voluntary ingestion. Reportedly took more than two years to clear, trying numerous treatment regimens,.
• Not accepted as cause of ulcers until 1994.

HP resistance
• Decline in efficacy has been noted with standard triple therapy over the past 10 years.
• Newer Drugs have a higher eradication rate , however, it is likely that it will show similar phenomenon.
• Since the evolution of drug resistance will remain a problem, newer therapies must be implemented sooner rather than later.


Clarithromycin Resistance
• There are essentially three point mutations, which can occur at the positions 2142 (A2142G and A2142C) and 2143 (A2143G) I
• these mutations resulted in:
• Decrease in binding of the drug.
• No impact on bacterial Viability
• Decreased efficacy of triple therapy by 66.2%
• Problem can be induced by any type of Macrolid

levofloxacin Resistance
• More extensive loci
• No enough evidence
• Response rate is 60%

Diagnosis of CLA resistance
• Start screening if prevalence is > 20 %1- The standard methods using culture and antimicrobial susceptibility testing (e.g. Etest, AB bioMerieux, Solna, Sweden) take several days 2- Rapid molecular methods including standard polymerase chain reaction (PCR)
(Seeflex®ClaR H. pylori ACE detection, Seegene, Seoul, South Korea)
Real-time PCR (Engenetix, Vienna, Austria) fluorescence in situ hybridization (seaFAST H. pylori)

ManagementSequential treatment
• Sequential treatment =(PPI) and amoxicillin for 5 days followed by a PPI t >>>> clarithromycin and metronidazole for the next 5 days
• In resistant strain standard Tx 32% vs 72% Seqential Tx
• Theory of success that 1st phase Tx decrease bacterial load including resistant strains allowing better result with 2nd phase

ManagementBismuth-based quadruple therapy
OBMT • PPI + Bithmus salt + Metro 250 QID + Tetra 250 QID • Rational1. Bismuth salts mechanism of action is not known but appears to be more
like an antiseptic than an antibiotic, and no resistance has been described; 2. Tetracycline is an antibiotic for which resistance is rarely encountered. The
reason is that to reach a high level resistance, three adjacent point mutations are required which is rare to find in the same organism
3. Metronidazole, resistance is of low clinical impact that can be overcomedby increasing the dose and duration of treatment >>> only 14% decrease in treatment success
4. BMT three-in-one capsule (Pylera®) is commercially available Concern High doses of bismuth salts were associated with encephalopathy with reports of fatality

Management Salvage therapy
• Esomeprazole 20 mg BID + amoxicillin 500 mg BID + levofloxacin 500 mg BID.
• Success as a second line Tx is around 75%

H Pylori Reinfection
• Reappearance of H. pylori is thought to occur via two distinct mechanisms, recrudescence and re-infection. Recrudescence reflects reappearance of the original strain of H. pylori following its temporary suppression rather than successful eradication. True re-infection occurs when, after successful eradication,
• Most reinfections in the 1st year post Tx• Variable incidence world wide and look linked to the local H pylori
Incidence 1-20%• Comparison of strains of H. pylori following reappearance have shown
that 38% are identical to the pre-treatment strain in the first 6 months and none are identical following 1 year.
• Recurrence rate is less for 2nd line drugs • USA 1%• Iran 20%

Vaccine
• Difficulties include HP immune evasive mechanisms as it involves T Reg recruitment and down regulation of immune system.
• Recent breakthrough as the protective H. pylori-derived antigens have already been administered to humans and have proven their safety and immunogenicity
• Experimental H. pylori vaccination is under trial EpiVax “Phase I”

Who to test?
• Established• PUD• Gastric low-grade MALT lymphoma• Univestigated dyspepsia• After endoscopic resection of early cancer• Evaluate success of eradication therapy• Controversial• High Risk for Gastric Ca (e.g. relatives of patients who have gastric cancer)• Unexplained Iron Deficiency anemia• Nonulcer dyspepsia• Chronic nonsteroidal anti-inflammatory drug/aspirin therapy a• Chronic antisecretory drug therapy (eg, gastroesophageal reflux disease) b• Relatives of patients who have Hpylori infection• Patient desires to be tested• When planning long-term NSAID therapy • When planning long-term antisecretory therapy.
