hai proceedings of hai summit clin infect dis.-2008-kollef-s55-99
DESCRIPTION
Conference Proceedings of Hospital Acquired Infection SummitTRANSCRIPT

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S55
S U P P L E M E N T A R T I C L E
Health Care–Associated Infection (HAI): A CriticalAppraisal of the Emerging Threat—Proceedings ofthe HAI Summit
Marin H. Kollef,1,2 Lena M. Napolitano,3 Joseph S. Solomkin,4 Richard G. Wunderink,5 In-Gyu Bae,7
Vance G. Fowler,7 Robert A. Balk,6 Dennis L. Stevens,8 James J. Rahal,9,10 Andrew F. Shorr,11,12 Peter K. Linden,13
and Scott T. Micek1,2
1Washington University School of Medicine and 2Barnes-Jewish Hospital, St. Louis, Missouri; 3University of Michigan Health Center, Ann Arbor;4University of Cincinnati College of Medicine, Cincinnati, Ohio; 5Feinberg School of Medicine, Northwestern University, and 6Rush UniversityMedical Center and Rush Medical College, Chicago, Illinois; 7Duke University Medical Center, Durham, North Carolina; 8Veterans Affairs MedicalCenter, Boise, Idaho; 9New York Hospital Queens, Flushing, and 10Weill Medical College of Cornell University, New York, New York; 11WashingtonHospital Center and 12Georgetown University, Washington, DC; and 13University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania
During the Health Care–Associated Pneumonia Summit conducted in June 2007, it was found that there is a
need for educational efforts in several areas of health care–associated infections (HAI) that extend beyond
pneumonia. This supplement to Clinical Infectious Diseases represents the proceedings of the HAI Summit,
a diverse panel of clinical investigators whose goal was to assess the quality of evidence regarding issues
surrounding HAI and to discuss potential implications for its diagnosis and treatment in the future.
The classification of bacterial infections is in a state of
flux. Most of the prior classification schemes have seg-
regated these infections according to the site of infec-
tion (e.g., lung, urinary tract, soft tissue and skin, and
intra-abdominal) and the location of the patient at the
time the infection developed. The latter has historically
been divided into community-acquired and nosocomial
(hospital-acquired) infections [1, 2]. Unfortunately,
this simple classification scheme is no longer adequate,
because of changing patient demographics and risk
profiles for infection with potentially antibiotic-resis-
tant bacteria, which historically have been encountered
primarily in the hospital setting.
Patients with serious infections (e.g., pneumonia,
bacteremia, and septic shock) should be given treat-
ment initially with antibiotics active against the bac-
terial pathogens causing the infection (i.e., appropriate
antibiotic therapy). Additionally, appropriate antibiotic
Reprints or correspondence: Dr. Marin H. Kollef, Div. of Pulmonary and CriticalCare Medicine, Washington University School of Medicine, 660 S. Euclid Ave.,Campus Box 8052, St. Louis, MO 63110 ([email protected]).
Clinical Infectious Diseases 2008; 47:S55–99� 2008 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2008/4707S2-0002$15.00DOI: 10.1086/590937
therapy should be administered in a timely manner to
optimize the likelihood of a clinical response. The sup-
port for these recommendations comes from investi-
gations demonstrating that patients initially given treat-
ment with antibiotic regimens that are not active against
the causative bacterial species (i.e., inappropriate an-
tibiotic therapy) have a greater risk for in-hospital mor-
tality than do patients receiving appropriate therapy [3–
5]. Classification schemes should assist clinicians in
identifying patients at risk for antibiotic-resistant in-
fections, thereby requiring initial treatment with broad-
spectrum antimicrobials. The recognition of potentially
antibiotic-resistant infections occurring outside the
hospital setting has resulted in the formulation of the
new category, termed “health care–associated infec-
tions” (HAIs). Implicit in the definition of HAIs is that
patients will require initial therapy with more broad-
spectrum antibiotics, compared with patients with
community-acquired infections.
HAIs have been defined using various criteria (table
1). Friedman et al. [6] evaluated patients admitted to
the hospital with bloodstream infections (BSIs) and
showed that individuals with HAI risk factors were sta-
tistically more likely than were patients with commu-
nity-acquired infections to be infected with anti-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S56 • CID 2008:47 (Suppl 2) • Kollef et al.
Table 1. Risk factors used to define health care–associatedinfections.
Infection type [source] and criteria
Bacteremia [6]Health care–associated BSI was defined by a positive culture re-
sult for a blood specimen obtained from a patient at thetime of hospital admission or within 48 h after admissionif the patient fulfilled any of the following criteria:
1. Received intravenous therapy at home; received woundcare or specialized nursing care through a health careagency, family, or friends; or had self-administered intrave-nous medical therapy in the 30 days before the BSI. Pa-tients whose only home therapy was oxygen use wereexcluded.
2. Attended a hospital or hemodialysis clinic or received intra-venous chemotherapy in the 30 days before the BSI
3. Was hospitalized in an acute care hospital for �2 days inthe 90 days before the BSI
4. Resided in a nursing home or long-term-care facilityPneumonia [7]
HCAP was defined as a diagnosis of pneumonia in patients witha first positive bacterial respiratory culture finding within2 days of admission and any of the following:
1. Admission source indicates a transfer from another healthcare facility
2. Receiving long-term hemodialysis3. Prior hospitalization within 30 days for those whose condi-
tion does not meet VAP definitionPneumonia [8]
HCAP was defined as a diagnosis of pneumonia in patients ad-mitted to the hospital who met at least 1 of the followingcriteria:
1. Admission from a nursing home, rehabilitation hospital, orother long-term–nursing care facility
2. Previous hospitalization within the immediately preceding12 months
3. Receiving outpatient hemodialysis, peritoneal dialysis, or in-fusion therapy necessitating regular visits to a hospital-based clinic
4. Having an immunocompromised state
NOTE. Adapted from [6], from [7], and from [8]. BSI, bloodstream infection;HCAP, health care–associated pneumonia; VAP, ventilator-associated pneu-monia.
biotic-resistant bacteria, including methicillin-resistant Staphy-
lococcus aureus (MRSA) and antibiotic-resistant enterococci. In
an accompanying overview, the importance of the classification
of HAIs was emphasized in terms of identifying a group of
patients who would potentially benefit from initial treatment with
broad-spectrum antibiotics [9]. Similarly, Kollef et al. [7] ex-
amined 4543 patients with microbiologically confirmed pneu-
monia from a multicenter administrative database. They sepa-
rated patients into 4 categories: community-acquired pneumonia
(CAP), health care–associated pneumonia (HCAP), hospital-ac-
quired pneumonia (HAP), and ventilator-associated pneumonia
(VAP). Patients with HCAP had underlying comorbidities and
bacterial pathogens similar to those of patients with HAP and
VAP. The most common bacterial pathogen isolated in patients
with HCAP was MRSA. The in-hospital mortality rate among
patients with HCAP was similar to that observed among patients
with HAP (19.8% vs. 18.1%; ), both being almost twiceP � .005
the mortality rate observed among patients with CAP (10%;
for both comparisons) [7].P ! .001
The American Thoracic Society (ATS) and Infectious Diseases
Society of America (IDSA) guidelines for HCAP, HAP, and VAP
have summarized potential risk factors for HAIs (table 1) [1, 2].
These are the first published guidelines to recognize the category
of HCAP in terms of recommending initial broad-spectrum an-
timicrobial treatment because of the high prevalence of antibi-
otic-resistant bacteria as the causative agents of infection. Further
support for this recommendation comes from a large single-
center study evaluating patients with microbiologically confirmed
pneumonia admitted to an urban teaching hospital [8]. Among
the 639 patients with microbiologically confirmed pneumonia
evaluated in that study, HCAP made up 67.4% of the pneumonia
cases, and CAP accounted for 32.6%. Patients with HCAP were
statistically more likely to be infected with MRSA, Pseudomonas
aeruginosa, and other nonfermenting gram-negative rods, com-
pared with patients with CAP. Patients with HCAP were also
significantly more likely to have received inappropriate initial
antimicrobial therapy (28.3% vs. 13.0%; ) and hadP ! .001
greater in-hospital mortality (24.6% vs. 9.1%; ), com-P ! .001
pared with patients with CAP.
The importance of correctly classifying patients with HAI risk
profiles is demonstrated by 2 recent studies. Schramm et al. [5]
evaluated patients with MRSA sterile-site infections and showed
that patients with a positive sterile-site culture specimen obtained
during the first 48 h of hospitalization were significantly less
likely to have received empirical treatment for MRSA. This oc-
curred despite the fact that most patients had readily identifiable
risk factors for HAI, which suggests that the treating clinicians
did not recognize either the presence of these risk factors or the
associated therapeutic implications. In a prospective before-after
study using a protocol and standardized order set for the man-
agement of septic shock in the emergency department, a statis-
tically significant reduction (from 48.3% to 30%; ) inP p .04
28-day mortality was associated with the prescription of broad-
spectrum antibiotics to patients with risk factors for HAI [10].
These studies suggest that many patients evaluated during the
early periods of their hospitalization may benefit from having
their infection identified as an HAI, so that more-appropriate
initial antibiotic therapy can be prescribed.
During the HCAP Summit conducted in June 2007, it was
found that there is a need for educational efforts in several
areas of HAI that extend beyond pneumonia. This supplement
to Clinical Infectious Diseases represents the proceedings of a
diverse panel of clinical investigators whose goal was to assess
the quality of evidence in support of the clinical classification
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S57
Table 2. Health Care–Associated Infection (HAI) Summit clini-cal practice statements.
Workshop 1: Treatment by Sites of Infection (statements 1–5)1. Patients at risk for health care–associated complicated skin
and soft tissue infections are more likely to have both resis-tant gram-negative and gram-positive pathogens. (L.M.N.)
2. Patients with health care–associated intra-abdominal infec-tions should receive dual empiric therapy for resistant gram-negative and gram-positive pathogens. (J.S.S.)
3. Early aggressive, appropriate empiric treatment and de-esca-lation for HCAP reduces mortality and minimizes resistance.(R.G.W.)
4. Health care–associated BSIs require empiric coverage forMDR gram-negative bacteria and MRSA, as well as coveragefor fungal pathogens in patients with specific risk factors.(V.G.F.)
5. Initial appropriate antimicrobial therapy and source control arethe most important determinants of outcome in severe sepsisand septic shock. (R.A.B.)
Workshop 2: Treatment by Organism (statements 6–10)6. Vancomycin is obsolete for treating MRSA infections. (D.L.S.)7. Serious HAIs due to suspected gram-negative bacteria should
be treated empirically with dual coverage that includes anaminoglycoside. (J.J.R.)
8. Patients with serious HAIs who have risk factors for fungalinfections require early empiric antifungal therapy to reducemortality. (A.F.S.)
9. All infections in immunocompromised patients should be con-sidered HAIs until proven otherwise. (P.K.L.)
10. Adjunctive therapy should be utilized to prevent and treatserious HAIs. (S.T.M.)
NOTE. BSI, bloodstream infection; HCAP, health care–associated pneu-monia; MDR, multidrug resistant; MRSA, methicillin-resistant Staphylococcusaureus.
Table 3. Workshop and Health Care–Associated Infection Sum-mit panel voting schemes.
Category Nature of evidence
I Evidence obtained from at least 1 well-designed,randomized, controlled trial
II Evidence obtained from well-designed cohort orcase-control studies
III Evidence obtained from case series, case reports,or flawed clinical trials
IV Opinions of respected authorities based on clini-cal experience, descriptive studies, or reportsof expert committees
V Insufficient evidence to form an opinion
Level of workshop support for statement
A There is good evidence to support the statementB There is fair evidence to support the statementC There is poor evidence to support the statement,
but recommendations may be made on othergrounds
D There is fair evidence to reject the statementE There is good evidence to reject the statement
Individual level of support
1 Accept recommendation completely2 Accept recommendation with some reservations3 Accept recommendation with major reservations4 Reject recommendation with reservations5 Reject recommendation completely
of HAI as a distinct entity and the need for specific therapeutic
interventions for HAI. Ten clinical practice statements were
drafted by the chair (M.H.K.) and the 2 workshop leaders
(L.M.N. and D.L.S.) and were subsequently evaluated by an
11-member panel with expertise in infectious diseases, surgery,
critical care, pharmacology, and outcomes research (table 2).
Before the summit was convened, each participant was assigned
a statement and was instructed to systematically review and
summarize the evidence supporting or refuting that statement.
In the first phase of the live meeting, the simultaneously
conducted workshops “Treatment by Sites of Infection” and
“Treatment by Organism” included a leader and 4 or 5 content
experts and served as a forum for each individual to present
the evidence for his or her assigned statement. When the data
were presented, primary attention was given to the study meth-
odology, the number of patients enrolled, and the outcome
events. After the presentation of data for each statement, work-
shop members discussed the evidence, graded the strength of
the evidence, and assigned the statement a consensus numeric
grade through a voting process (table 3).
In the second phase of the live meeting, all summit panelists
reconvened as a single group, reviewed the workshop sum-
maries, and discussed each statement further. After each dis-
cussion, all participants voted on their individual levels of sup-
port, using the grading scheme shown in table 3. In addition
to defining the level of evidence available for each statement,
the panel members also outlined additional data required to
further refine the statements for future clinical uses.
Before the summit meeting, clinical perspectives of prac-
ticing physicians were measured via a Web-based survey. E-
mail polling was done to ascertain their level of support for
the same 10 statements. The e-mail invitation to participate
in the electronic survey was sent to 3300 members of the
IDSA (all active e-mail addresses). Of the IDSA members
surveyed, 744 (23%) responded. The purpose of the electronic
surveys was to provide information that would allow for the
comparison of data-driven responses from the content “ex-
perts” at the summit with those from clinicians practicing in
the field. The summit participants and the surveyed physicians
used the same voting scheme for “Individual Level of Sup-
port” to grade the 10 statements (table 3).
This exercise was performed to determine the prevailing cur-
rent opinions regarding HAIs and areas where additional re-
search and knowledge is required. In this era of increasing
antimicrobial resistance, clinical decision making regarding the
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S58 • CID 2008:47 (Suppl 2) • Kollef et al.
management of suspected bacterial infections has become in-
creasingly complex. Given factors such as the aging of our
population, the increasing use of immunomodulating therapies,
and the practice of caring for patients with more-complicated
cases outside of the hospital setting, it is very likely that the
prevalence of HAIs will increase. Research to better define this
category of infection and its management appears to be very
relevant.
STATEMENT 1: PATIENTS AT RISK FOR HEALTHCARE–ASSOCIATED COMPLICATED SKIN ANDSOFT-TISSUE INFECTIONS ARE MORE LIKELYTO HAVE BOTH RESISTANT GRAM-NEGATIVEAND GRAM-POSITIVE PATHOGENS
Rationale and Definition of Statement
Presently, there is no standard definition for health care–as-
sociated complicated skin and soft-tissue infection (cSSTI). The
terminology of HAIs was first devised as a new classification
scheme for BSIs to distinguish patients with community-ac-
quired, health care–associated, and nosocomial infections [6].
Skin and soft-tissue infections (SSTIs) have traditionally been
categorized as either uncomplicated or complicated infections,
by use of the US Food and Drug Administration (FDA) criteria
[11]. Uncomplicated skin infections include simple abscesses,
impetiginous lesions, furuncles, and cellulitis. Complicated skin
infections include deeper soft-tissue infections or those re-
quiring significant surgical intervention, such as infected ulcers,
burns, and major abscesses or a significant underlying disease
state that complicates the response to treatment. Superficial
infections or abscesses in an anatomical site, such as the rectal
area, where the risk of anaerobic or gram-negative pathogen
involvement is higher, should be considered complicated
infections.
The microbiology of uncomplicated and complicated skin
infections is not the same. In uncomplicated skin infections,
S. aureus and Streptococcus pyogenes are the 2 most commonly
seen pathogens. Among complicated skin infections, the pos-
sible pathogens are numerous, may be monomicrobial or po-
lymicrobial, and are dependent on the clinical situation, the
location of the infection, and the medical history of the indi-
vidual patient.
Because no standard definition for health care–associated
cSSTI is available, we will review data regarding HAIs in general
and the changing epidemiology of cSSTIs. This section aims to
assess the strength of evidence supporting the assertion that
patients at risk for health care–associated cSSTI are more likely
to be infected with both resistant gram-negative and gram-
positive pathogens.
Methods
A PubMed database search to identify studies related to the
clinical and microbiological features of health care–associated
cSSTIs was completed on 4 September 2007. The search term
“skin infections” yielded a total of 78,866 articles. The search
term “complicated skin and skin structure infection (cSSSI)”
yielded 244 articles, and the search term “complicated skin and
soft tissue infection (cSSTI)” yielded 100 articles. The search
terms “health care associated,” “healthcare associated,” and
“healthcare-associated” yielded 51,504, 38,460, and 288 articles,
respectively. Combining the search terms “health care associ-
ated,” “healthcare associated,” and “healthcare-associated” with
“infection,” using the “AND” function, produced 5154, 3759,
and 250 articles, respectively. Combining the search terms
“health care associated,” “healthcare associated,” and “health-
care-associated” with “skin infections,” using the “AND” func-
tion, produced 138, 109, and 5 articles, respectively. After lim-
iting these articles to the English language, a total of 147 articles
were reviewed, and 2 articles were deemed relevant to the
statement.
Evidence
Prevalence of health care–associated cSSTI. No studies were
identified as specifically focusing on the prevalence of health
care–associated cSSTI. One study specifically addressed the is-
sue of overall prevalence of HAIs in general and included a
cohort of patients with skin infections. This study involved a
cross-sectional population survey of patients, aged �19 years,
admitted to 25 acute-care hospitals participating in the Ca-
nadian Nosocomial Infection Surveillance Program, to deter-
mine the prevalence of HAIs. A 1-day HAI point-prevalence
survey was conducted in February 2002. Adult patients who
had been admitted at least 48 h before the day of the survey
were identified, and the primary outcome was the presence of
an HAI, which was identified as an infection not present at
admission and with onset at least 72 h after admission. Some
would consider these nosocomial infections. The study was
limited to the following infections: pneumonia, urinary-tract
infection, BSI, surgical-site infection, and Clostridium difficile
infection. Centers for Disease Control and Prevention (CDC)
definitions were used for all HAIs. A total of 5750 adults were
surveyed, 2086 (36%) of whom were receiving at least 1 sys-
temic antimicrobial agent; 601 patients had 667 HAIs, giving
a prevalence of 10.5% for infection and 11.6% for HAI. The
only skin infection reported was surgical-site infection, which
was identified in 146 patients (2.5%). In the multivariate logistic
regression model for HAI, the following characteristics were all
independently associated with HAI: extended hospital stays of
17 days before the day of the survey, having a central venous
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S59
catheter, having an indwelling urinary catheter, or having an
endotracheal tube with or without mechanical ventilation [12].
Epidemiology and microbiology of health care–associated
cSSTI. No studies were identified that specifically focused on
the microbiology of health care–associated cSSTI. However,
multiple studies reported the microbiology of SSTIs in hos-
pitalized patients and patients presenting to the emergency
department.
The SENTRY Antimicrobial Surveillance Program, estab-
lished in 1997 by the Jones Group/JMI laboratories and funded
by SmithKline Beecham, is designed to monitor antimicrobial
resistance among various pathogens around the globe [13]. The
SENTRY program recently reported data regarding causative
isolates from SSTIs from 3 continents during a 7-year period
(1998–2004) [14]. Each year, participating medical centers sent
50 consecutive pathogens from hospitalized patients that were
determined to be significant causes of pyogenic wound infec-
tions. The isolates were from an SSTI or surgical-site infection
and were either community acquired or nosocomial in origin.
The predominant pathogens included S. aureus (ranked first
in all geographic regions), P. aeruginosa, Escherichia coli, and
Enterococcus species. On the global scale, S. aureus was the most
frequently occurring pathogen from an SSTI, with MRSA being
the greatest resistance concern. Considerable variation in the
MRSA rate was noted between countries and continents, with
the overall rate highest in North America (35.9%), followed by
Latin America (29.4%) and Europe (22.8%). It was noted that
the rate of MRSA in North America increased from 26.2% of
isolates in 1998 to 47.4% of isolates in 2004. Gram-negative
isolates as causes of SSTIs were common, and, among non-
Enterobacteriaceae gram-negative bacilli, P. aeruginosa had the
highest occurrence in SSTIs in all geographic regions.
Community-associated MRSA has increased markedly to be-
come the greatest problem facing treatment of SSTIs in the
outpatient setting. A comparison of community-associated and
health care–associated MRSA infections was performed as a
prospective cohort study of patients with MRSA infection iden-
tified at 12 Minnesota laboratory facilities from 1 January
through 31 December 2000. Of 1100 MRSA infections, 131
(12%) were community associated, and 937 (85%) were health
care associated. SSTIs were more common among community-
associated cases (75%) than among health care–associated cases
(37%) (OR, 4.25; 95% CI, 2.97–5.90) [15].
A prospective, observational study examined patients with
SSTIs presenting to the emergency department in an urban public
hospital in Oakland, California. Among the 137 patients enrolled,
MRSA was present in 51% of infection-site cultures. Of 119 S.
aureus isolates (from infection site and nares), 89 (75%) were
MRSA, and almost all (99%) of the MRSA isolates possessed the
staphylococcal cassette chromosome (SCC) mec type IV allele
(typical of community-associated MRSA). Among predictor var-
iables independently associated with MRSA infection, the stron-
gest was presence of furunculosis (OR, 28.6). In this urban pop-
ulation, MRSA was the leading pathogen in SSTIs [16].
The CDC and 3 sites participating in the Emerging Infections
Program began a specialized, prospective MRSA surveillance
project in 2001 using the Active Bacterial Core Surveillance
program, a population-based surveillance component of the
Emerging Infections Program Network designed to study the
epidemiologic features of invasive bacterial disease and to track
drug resistance in the United States. The MRSA Active Bacterial
Core Surveillance project monitored all MRSA isolates from all
body sites from patients in select hospitals in Baltimore, Atlanta,
and Minnesota. From 2001 through 2002, 1647 cases of com-
munity-acquired MRSA infections were reported, and 77% in-
volved skin and soft tissue. Overall, 23% of patients were hos-
pitalized for the MRSA infection. This study concluded that
community-associated MRSA skin infections were now a com-
mon problem [17].
A prospective multicenter study confirmed this finding.
Adult patients with acute, purulent SSTIs presenting to 11 uni-
versity-affiliated emergency departments during the month of
August 2004 were enrolled to determine the causative bacterial
isolates. S. aureus was isolated from 320 (76%) of 422 patients
with SSTIs. The prevalence of MRSA was 59% overall, and USA
300 isolates accounted for 97% of MRSA isolates; SCC mec
type IV and the Panton-Valentine leukocidin toxin gene were
detected in 98% of MRSA isolates, consistent with community-
associated MRSA infection. Methicillin-susceptible S. aureus
(MSSA) was identified in only 17% of patients with SSTIs. In
this study, MRSA was the most common identifiable cause of
SSTIs among patients presenting to emergency departments in
11 US cities [18].
None of these studies specifically differentiate between the
epidemiologic characteristics of community-associated (i.e.,
with no established risk factors) versus health care–associated
(i.e., with health care–associated risk factors) SSTIs. They do,
however, address the issue of differences in the microbiological
characteristics between the community-associated and health
care–associated MRSA isolates (table 4) [19].
An active, prospective, laboratory surveillance study con-
ducted at a 1000-bed urban hospital and its affiliated outpatient
clinics in Atlanta, Georgia, identified S. aureus that was recov-
ered from SSTIs in 384 persons and 389 episodes of infection,
with MRSA accounting for 72% (279 of 389 episodes). Among
all S. aureus isolates, 63% (244 of 389 isolates) were commu-
nity-acquired MRSA. Among MRSA isolates, 87% (244 of 279
isolates) were community-acquired MRSA, and 99% were USA
300 clones. Factors independently associated with community-
acquired MRSA infection were black race (prevalence ratio,
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S60 • CID 2008:47 (Suppl 2) • Kollef et al.
Table 4. Comparison of community-associated and health care–associated methicillin-resistantStaphylococcus aureus (MRSA).
Characteristic Community-associated MRSA Health care–associated MRSA
Susceptibility, drugChloramphenicol Usually susceptible Frequently resistantClindamycin Usually susceptible Frequently resistantErythromycin Usually resistant Usually resistantFluoroquinolone Geographic variability Usually resistantTMP-SMZ Usually susceptible Usually susceptible
SCC mec type IV IILineage USA 300, USA 400 USA 100, USA 200Toxin producing More FewerPanton-Valentine leukocidin producing Common RareHealth care exposure Less frequent More frequent
NOTE. SCC, staphylococcal chromosome cassette; TMP-SMZ, trimethoprim-sulfamethoxazole. Adapted from [19].
1.53; 95% CI, 1.16–2.02), female sex (prevalence ratio, 1.16;
95% CI, 1.02–1.32), and hospitalization within the previous 12
months (prevalence ratio, 0.80; 95% CI, 0.66–0.97). Inadequate
initial antibiotic therapy was statistically significantly more
common among those with community-acquired MRSA (65%)
than among those with MSSA (1%) SSTI. This study concluded
that the community-acquired MRSA USA 300 clone was the
predominant cause of community-onset S. aureus SSTIs, and
therefore empirical use of agents active against community-
acquired MRSA is warranted for patients presenting with se-
rious SSTIs. The study setting was a 1000-bed, urban hospital
and its affiliated outpatient clinics in Atlanta, Georgia [20].
Epidemiology and microbiology of cSSTI. Because no pub-
lished data are available for health care–associated cSSTIs, we
reviewed recent studies that served as FDA registration trials
for antimicrobials used to treat cSSTI. In 2 randomized inter-
national trials involving 1092 patients with cSSTI, daptomycin
was compared with conventional antibiotics (penicillinase-re-
sistant penicillin or vancomycin). S. aureus was the leading
causative pathogen, isolated in ∼70% of patients; MRSA ac-
counted for only 10% of the S. aureus isolates. Streptococci
and enterococci were also common causative pathogens [21].
In another phase 3 cSSTI study, patients ( ) weren p 854
randomized to receive dalbavancin or linezolid. Baseline cul-
tures yielded at least 1 gram-positive pathogen for 550 patients
(64%; the microbiological intent-to-treat population). Of these,
90% presented with a single gram-positive pathogen. S. aureus
was predominant (89% of all patients). Of the S. aureus isolates,
278 (57%) of 492 were MRSA. Overall, 51% of patients pre-
sented with cSSTI that involved MRSA [22].
Two phase 3, double-blind studies randomized hospitalized
adults with cSSTI to receive tigecycline or vancomycin-az-
treonam ( ). S. aureus, with a majority of isolates beingn p 1116
MSSA, was the leading pathogen, and streptococci were also
common. Gram-negative isolates (only E. coli) were uncommon
and were isolated in only 59 patients [23].
Two large, multinational, double-blind, randomized, phase 3
clinical studies (ATLAS 1 and ATLAS 2) enrolled 1867 patients
with cSSTI, 719 of whom were infected with MRSA, and deter-
mined that televancin was not inferior to vancomycin. S. aureus
was the primary pathogen isolated in these studies, as it was in
the 2 prior phase 2 trials (FAST 1 and FAST 2) [24–26].
A multicenter, global, randomized, double-blind trial com-
pared ceftobiprole with vancomycin for patients ( )n p 784
with cSSTI and confirmed the noninferiority of ceftobiprole,
and S. aureus was the primary causative isolate [27]. A second
cSSTI trial also included patients with diabetic foot infections,
and gram-negative pathogens were more common. Gram-pos-
itive pathogens were isolated from 79% of patients and MRSA
was the most common pathogen (42.4%). Gram-negative path-
ogens were isolated from 29% of patients, and E. coli (11.0%)
and Pseudomonas isolates (6.6%) were the most common [28].
All these studies confirm that the most common causative
pathogens in cSSTIs are aerobic gram-positive cocci, with S.
aureus and MRSA as the leading isolates.
Epidemiology and microbiology of surgical-site infections.
Surgical-site infections are also included in the cSSTI category.
In a report from the National Nosocomial Infections Surveil-
lance System from 1986–2003, an analysis of 1410,000 bacterial
isolates associated with hospital-acquired infections (BSIs,
pneumonia, surgical-site infection, and urinary-tract infection)
in intensive care units (ICUs) were reported. For surgical-site
infections, the percentage of bacterial isolates that were gram
negative decreased during the study period (from 56.5% in
1986 to 33.8% in 2003). By the mid-1990s, gram-positive bac-
terial pathogens were more commonly reported as causative
isolates in surgical-site infections, with S. aureus as the leading
pathogen [9]. MRSA has emerged as the most common isolate
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S61
Figure 1. Voting comparison for statement 1 (“Patients at risk for health care–associated complicated skin and soft tissue infections are morelikely to have both resistant gram-negative and gram-positive pathogens”). “IDSA” refers to the members of the Infectious Diseases Society of Americawho responded to a Web-based survey; “Summit” refers to the Health Care–Associated Infection Summit panel.
causing surgical-site infections in most institutions [29]. MRSA
surgical-site infections are associated with significantly in-
creased mortality (OR, 3.4; ), length of hospital stay,P p .003
and costs, compared with MSSA surgical-site infections [30].
Community-associated MRSA strains are increasingly recov-
ered from hospital settings, and a recent retrospective review
of surgical-site infection in 2004–2005 in Alabama determined
that 57% of MRSA strains from surgical-site infections were of
the USA 300 genotype, confirming that community-associated
MRSA was a prominent cause of surgical-site infection at that
institution [31].
Epidemiology and microbiology of diabetic foot infection.
The bacteriology of diabetic foot infections was assessed in a
recent study of 371 patients (infected ulcer and cellulitis were
the most common types of infection). Overall, one-half of all
patients had only gram-positive cocci isolated (355 isolates).
Of these, S. aureus, coagulase-negative staphylococci, strepto-
cocci, and enterococci were the most common isolates. Gram-
negative bacteria, predominantly Pseudomonas and Enterobac-
teriaceae species, were isolated in 105 patients, and 32% had
mixed infections with both gram-positive and gram-negative
pathogens [32]. In the SIDESTEP study (of ertapenem vs. pi-
peracillin/tazobactam for treatment of diabetic foot infection;
), infections were polymicrobial in 47% of evaluablen p 586
patients, and 9% had both gram-positive and gram-negative
aerobic organisms isolated by culture. The most commonly
isolated pathogens were gram-positive aerobic cocci (257 iso-
lates), with S. aureus as the leading isolate, followed by gram-
negative aerobic bacilli isolates (102 isolates), with Enterobac-
teriaceae species as the leading isolates [33].
The IDSA guidelines for diagnosis and treatment of diabetic
foot infection state, “Aerobic gram-positive cocci (especially S.
aureus) are the predominant pathogens in diabetic foot infec-
tions. Patients who have chronic wounds or who have recently
received antibiotic therapy may also be infected with gram-
negative rods, and those with foot ischemia or gangrene may
have obligate anaerobic pathogens” [34, p. 885].
Grading of Evidence
On the basis of a review of the studies cited above, the workshop
members agreed that there was substantial evidence available
to reject this statement. In evaluating the nature of the evidence,
20% voted category I, 60% voted category II, and 20% voted
category III (table 3).
Level of Support
When voting on the individual level of support for this statement,
0% of the summit participants voted to accept the statement
completely, 18% voted to accept the statement with some res-
ervations, 9% voted to accept the statement with major reser-
vations, 45% voted to reject the statement with reservations, and
27% voted to reject the statement completely. In comparison, of
the 744 IDSA members who participated in the online survey,
32% voted to accept the statement completely, 42% voted to
accept the statement with some reservations, 11% voted to accept
the statement with major reservations, 12% voted to reject the
statement with reservations, and 3% voted to reject the statement
completely (figure 1).
Discussion
Presently, there is no true category or definition of health care–
associated cSSTI, and no studies were identified in the published
literature. The traditional categories of SSTI include uncompli-
cated versus complicated (initially proposed by the FDA for the
conduct of clinical trials for SSTIs) and community acquired or
community onset versus hospital acquired or nosocomial.
The leading causative pathogen of SSTIs in both community
and hospitalized patients is MRSA. This has been confirmed
with an in-depth review of the recent registration trials for
cSSTIs that discusses the microbiology of new antimicrobials
(daptomycin, dalbavancin, telavancin, tigecycline, and cefto-
biprole). S. aureus was the leading pathogen in all studies, with
rising rates of MRSA. The SENTRY Antimicrobial Surveillance
Program has documented that the rate of MRSA in SSTIs in
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S62 • CID 2008:47 (Suppl 2) • Kollef et al.
Table 5. Definitions used for epidemiologic classification of invasive methicillin-resistantStaphylococcus aureus (MRSA) infections.
Classification Definition
Health care associatedCommunity onset Cases with at least 1 of the following health care risk factors: (1)
presence of an invasive device at time of admission; (2) historyof MRSA infection or colonization; (3) history of surgery, hospitali-zation, dialysis, or residence in a long-term-care facility in previ-ous 12 months preceding culture date
Hospital onset Cases with positive culture result from a normally sterile site ob-tained 148 h after hospital admission. These cases might alsohave �1 of the community-onset risk factors.
Community associated Cases with no documented community-onset health care risk factor
NOTE. Reprinted from JAMA 2007;298:1763–71 [39]. Copyright �2007, American Medical Association.All rights reserved.
North America increased substantially, from 26.2% of isolates
in 1998 to 47.4% of isolates in 2004. Community-associated
MRSA is the primary pathogen in patients without health care–
associated risk factors. S. aureus is also the leading pathogen
in surgical-site infections, with rising rates of MRSA.
Given the high prevalence of MRSA cSSTI at present, is it
important to standardize the classification of these invasive
MRSA infections? Several methods are used to classify MRSA
as health care associated or community associated, including
(1) genotypic testing, based on the results of PFGE or other
molecular techniques; (2) phenotypic testing, based on anti-
microbial susceptibility testing; and (3) epidemiologic analysis,
based on the time from hospital admission to a positive culture
result. Definitions of community-associated MRSA often use
time-based criteria in which the recovery of MRSA isolates
within 48 or 72 h after hospital admission is considered in-
dicative of community-associated MRSA. However, time-based
criteria do not consider patients with MRSA infection after
recent health care exposure. Furthermore, community-associ-
ated MRSA has emerged as a health care–associated and nos-
ocomial pathogen [35–38]. Community-associated MRSA
strains differ from hospital-acquired MRSA strains in that they
are generally susceptible to most antibiotics, whereas nosoco-
mial strains are generally multidrug resistant (MDR). However,
these data are not available to the prescribing clinician when
empirical antibiotics are selected.
The recent epidemiologic reports of invasive MRSA infec-
tions ( ) in the United States, which were associatedn p 8987
with 1598 in-hospital deaths, classified cases into mutually ex-
clusive groups (health care associated vs. community associ-
ated), first on the basis of health care risk factors. HAIs, in
turn, were classified as either community onset or hospital onset
(table 5) [39].
In contrast, in diabetic foot infections, gram-negative path-
ogens and polymicrobial infections are more common than are
surgical-site infections and cSSTIs. There are, however, some
additional cSSTI categories in which resistant gram-positive and
gram-negative pathogens would be likely. These include peri-
neal infections, necrotizing soft-tissue polymicrobial infections,
pressure ulcer and decubitus infections, and surgical-site in-
fections related to abdominal and genitourinary surgical
procedures.
Future Directions
Future directions discussed by the summit members include
the need to evaluate whether a category of health care–asso-
ciated cSSTIs is appropriate at this time. The use of HAI cat-
egories in bacteremia and pneumonia are thought to be im-
portant for improving the recognition of those patients who
may be infected with MDR pathogens and therefore warrant
more broad-spectrum empirical antimicrobial therapy. There
is minimal evidence to suggest that the addition of health care–
associated cSSTIs would have significant implications for the
selection of empirical antimicrobial therapy for these patients
with skin infections. Other potential classification schemes
could be considered for cSSTIs, such as monomicrobial versus
polymicrobial, necrotizing versus nonnecrotizing, and pyogenic
versus nonpyogenic. Additional detailed studies of SSTIs are
warranted to further delineate changes in the microbial etiology
of cSSTIs, to optimize treatment strategies and also to evaluate
risk factors for recurrence.
STATEMENT 2: PATIENTS WITH HEALTH CARE–ASSOCIATED INTRA-ABDOMINAL INFECTIONSSHOULD RECEIVE DUAL EMPIRIC THERAPYFOR RESISTANT GRAM-NEGATIVE AND GRAM-POSITIVE PATHOGENS
Rationale and Definition of Statement
Complicated intra-abdominal infections (cIAIs) are defined as
infections that extend beyond the hollow viscus of origin into
the peritoneal space and are associated with either abcess for-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S63
mation or peritonitis [40]. Intra-abdominal infections pose se-
rious challenges to the treating physicians, and mortality rates
approach 60% [41]. Rapid diagnosis, appropriate intervention,
and timely and efficacious anti-infective therapy are of critical
importance and have been shown to lead to improved patient
outcomes.
The traditional binary classification scheme for cIAIs has
consisted of nosocomial and community-acquired infections.
At present, there is no defined category for health care–asso-
ciated cIAI, unlike the distinction that has been made recently
with BSI and pneumonia. Many of the data regarding epide-
miology and antimicrobial treatment of cIAI are derived from
antimicrobial trials, and most patients who entered into those
trials had community-acquired infections, such as perforated
or complicated appendicitis, and have not been severely ill.
It is estimated that ∼80% of all intra-abdominal infections
(IAIs) are acquired in a community setting [42]. In com-
munity-acquired infections, the location of the gastrointes-
tinal perforation defines the infecting flora: infections that
occur beyond the proximal small bowel are caused by fac-
ultative and aerobic gram-negative organisms; infections that
occur past the proximal ileum can be caused by a variety of
anaerobic microorganisms.
The IDSA guidelines for cIAI used the term “health care–
associated infections” to describe nosocomial infections, in-
cluding cIAIs acquired postoperatively. HAIs were specifically
defined as infections that “are most commonly acquired as
complications of previous elective or emergent intra-abdominal
operations and are caused by nosocomial isolates particular to
the site of the operation and to the specific hospital and unit”
[40, p. 997].
In the context of the HAI Summit’s reference to other in-
fections, the term HAI was used to describe infections in in-
dividuals who regularly interact with the health care environ-
ment. It has been suggested that HAIs represent a unique
population of patients. These patients are thought to be infected
not only with a different spectrum of pathogens but also with
potentially more-resistant flora.
The term HAI was first used to characterize a spectrum of
BSIs [6]. Similarly, patients with cIAI with these same risk
factors for HAI may have ample opportunity to acquire resis-
tant bacteria. It is undetermined at present whether an ex-
panded classification scheme, to include health care–associated
cIAI, may be necessary for patients with IAIs. There is currently
no standard category or definition for HAIs in the broader
category of IAIs.
This review focuses on the available literature that charac-
terizes the microbiology of cIAIs (both community acquired
and nosocomial), the importance of appropriate initial empir-
ical therapy, and the incidence of MDR organisms. By assess-
ment of the strength of this evidence, it is possible to ascertain
whether an expanded classification system that includes health
care–associated cIAI is needed and would benefit a potential
new subgroup of patients.
Methods
A PubMed database search was conducted on 4 September 2007
to identify relevant reports involving the treatment and mi-
crobiological features of health care–associated IAIs. The search
term “intra-abdominal infections” yielded a total of 2347 ar-
ticles. The search terms “health care associated,” “healthcare-
associated,” and “healthcare associated” yielded 51,504, 38,460,
and 288 articles, respectively. When these terms were combined
with “intra-abdominal infections,” using the “AND” function,
22 articles were found. After the results were limited to the
English language, 0 articles were found to be relevant to the
statement.
In a second PubMed database search, the search term “post-
operative peritonitis OR secondary peritonitis” yielded 9237
articles. This term was combined with “microbiology,” using
the “AND” function, yielding 168 articles; with the search term
“drug resistance,” yielding 198 articles; and with the search term
“appropriate therapy,” yielding 220 articles. After results were
limited to humans and the English language, 5 articles were
found to be relevant to the statement. The IDSA and the Sur-
gical Infection Society guidelines for the treatment of cIAIs were
also reviewed.
Evidence
No studies specifically related to “health care–associated intra-
abdominal infections” were identified. The 2 issues of empirical
antibiotic therapy and dual empirical therapy for treatment of
infection with resistant gram-positive and gram-negative path-
ogens will be addressed separately.
Empirical antimicrobial therapy for cIAI. The first portion
of the statement recommends that patients with health care–
associated IAI should receive empirical antimicrobial therapy.
A retrospective case study by Krobot et al. [43] assessed the
effect of inappropriate initial empirical antibiotic therapy in
425 patients with “community-acquired” secondary peritonitis.
E. coli was the most commonly isolated pathogen. A total of
54 patients (13%) received inappropriate initial therapy. Clin-
ical success, predefined as resolution of infection with initial
or step-down therapy after primary surgery, was achieved for
322 patients (75.7%). However, patients were more likely to
have clinical success if the initial antibiotic therapy was appro-
priate than if it was inappropriate (75.7% vs. 53.4%). Patients
who had clinical success had a mean length of stay of 13.9
days, compared with 19.8 days for those who had clinical fail-
ure. Furthermore, multinomial analyses (with adjustment for
patient age, sex, and comorbidities) revealed that inappropriate
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S64 • CID 2008:47 (Suppl 2) • Kollef et al.
antimicrobial therapy was associated with the need for second-
line antibiotic therapy and repeated operation.
A more recent multicenter study of 425 patients with com-
munity-acquired IAI in Spain examined the consequences of
inappropriate initial empirical parenteral antibiotic therapy
[44]. Initial empirical therapy was classified as appropriate if
all isolates were susceptible to at least 1 of the antibiotics ad-
ministered. A total of 387 patients (92%) received appropriate
initial empirical therapy. Patients receiving inappropriate ther-
apy were less likely to have clinical success (79% vs. 26%;
), more likely to require additional antibiotic therapyP ! .001
(40% vs. 7%; ), and more likely to be rehospitalizedP ! .01
within 30 days after discharge (18% vs. 3%; ). Multi-P ! .01
variate analyses also showed that inappropriate therapy was
associated with an almost 16% increase in length of stay and
a 26% increase in the number of days of antibiotic therapy.
Inappropriate initial antibiotic therapy was associated with a
significantly higher proportion of unsuccessful patient out-
comes, including death, repeated operation, rehospitalization,
additional antibiotic therapy, and increased length of stay. Other
studies have confirmed similar findings [45–47]. These data
clearly confirm that patients with IAI should receive appropriate
empirical antimicrobial therapy.
Dual empirical antimicrobial therapy for cIAI with resis-
tant gram-positive and gram-negative pathogens. The sec-
ond portion of the statement recommends that dual empirical
therapy for resistant gram-positive and gram-negative patho-
gens should be used for patients with health care–associated
cIAI.
The IDSA guidelines for cIAI separate the recommendations
regarding selection of anti-infective agents into 2 categories—
“mild-to-moderate” and “high-severity” infections—and these
may occur in both patients with community-acquired and pa-
tients with nosocomial infections [40]. Similarly, the Surgical
Infection Society guidelines for cIAI separate the recommen-
dations into “lower-risk patient” and “higher-risk patient” [48].
In general, for less severely ill patients with community-ac-
quired infections, antimicrobial agents with a narrow spectrum
of activity are adequate.
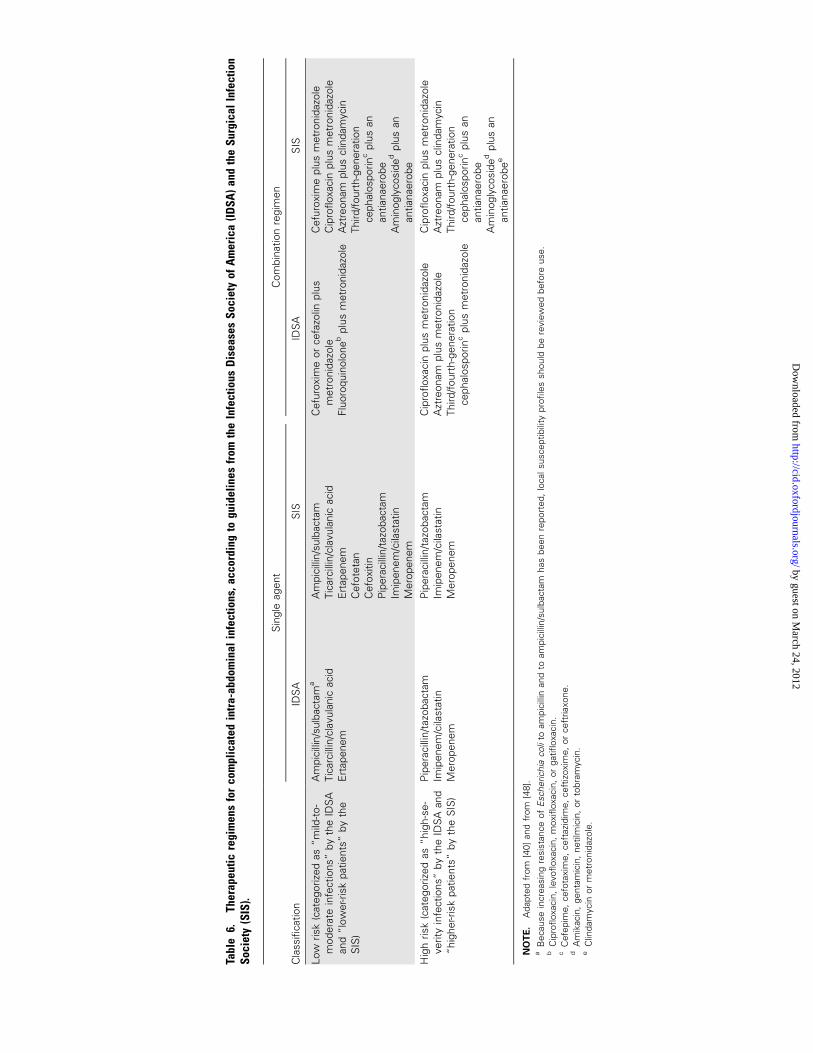
The IDSA recommends that community-acquired infections
may be managed with a variety of single- and multiple-agent
therapeutic regimens that are based, in part, on in vitro activ-
ities. The IDSA advises that no particular antimicrobial regimen
has consistently been demonstrated to be superior or inferior
(table 6).
For higher-risk patients or for those with high-severity IAIs,
broader-spectrum empirical antimicrobial therapy is recom-
mended to cover potential MDR pathogens. Nosocomial IAIs
are typically caused by a more-resistant flora, which may in-
clude P. aeruginosa, Acinetobacter species, Enterobacter species,
Proteus species, MRSA, enterococci, and Candida species. The
IDSA’s treatment recommendations for nosocomial cIAI sug-
gest multidrug regimens guided by knowledge of nosocomial
flora and susceptibility patterns.
Several studies have documented that infections involving
resistant organisms, particularly those likely to be acquired in
the health care setting, are associated with an increased risk of
treatment failure, morbidity, and mortality [49–52]. Prolonged
preoperative length of stay and prolonged (12 days) preoper-
ative antimicrobial therapy are significant predictors of anti-
microbial failure leading to recurrent infection, which suggests
that organisms resistant to the empirical antimicrobial regimen
may be responsible for infection. Patients with these risk factors
should be given treatment for nosocomial infection.
Montravers et al. [52] evaluated the incidence of resistant
bacterial strains among patients with postoperative peritonitis,
as well as the efficacy of empirical antimicrobial therapy. In
this study, 100 resistant pathogens were isolated from 70 pa-
tients who underwent repeated operation for generalized post-
operative peritonitis. Candida species and both gram-negative
and gram-positive anaerobic bacteria were isolated (table 7)
[52]. The relative frequencies of different pathogens cultured
in this patient population differed from those typically found
in patients with “community-acquired peritonitis.” Further-
more, the authors determined that 54% of the patients who
received inadequate initial empirical therapy for these resistant
pathogens had poorer outcomes, compared with patients who
received adequate therapy ( ).P ! .05
Roehrborn et al. [53] examined the microbiology of postop-
erative peritonitis in a prospective case study involving 67 pa-
tients. The most common isolates from patients with postop-
erative peritonitis were E. coli and Enterococcus, Enterobacter,
Bacteroides, and Klebsiella species. In addition, patients with post-
operative peritonitis were significantly more likely than were pa-
tients with community-acquired infections to have the following
isolates: enterococci (23 vs. 6), Enterobacter species (13 vs. 4), S.
aureus (7 vs. 1), and coagulase-negative staphylococci (7 vs. 1).
Patients with community-acquired infections were significantly
more likely to have streptococci and E. coli isolated.
The Study for Monitoring Antimicrobial Resistance Trends,
begun in 2002 and developed by the Merck research program,
is designed to monitor resistance patterns among aerobic and
facultative gram-negative bacilli isolated worldwide from intra-
abdominal bacterial clinical isolates collected from multiple
centers (including both teaching and community hospitals)
[54]. Data from the 2004 report [55] were used in the evaluation
of 6156 unique aerobic and facultatively anaerobic gram-neg-
ative bacilli isolated from IAIs. Enterobacteriaceae composed
86% of the total isolates, with E. coli (48%), Klebsiella species
(16%), and Enterobacter species (9%) comprising the majority
of isolates. Quinolone susceptibility rates for E. coli were sig-
nificantly reduced (60%–70% susceptible), with the lowest rates
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from
Tabl
e6.
Ther
apeu
ticre
gim
ens
for
com
plic
ated
intr
a-ab
dom
inal
infe
ctio
ns,a
ccor
ding
togu
idel
ines
from
the
Infe
ctio
usD
isea
ses
Soci
ety
ofA
mer
ica
(IDSA
)and
the
Surg
ical
Infe
ctio
nSo
ciet
y(S
IS).
Cla
ssifi
catio
n
Sin
gle
agen
tC
ombi
natio
nre
gim
en
IDS
AS
ISID
SA
SIS
Low
risk
(cat
egor
ized
as“m
ild-t
o-m
oder
ate
infe
ctio
ns”
byth
eID
SA
and
“low
er-r
isk
patie
nts”
byth
eS
IS)
Am
pici
llin/
sulb
acta
ma
Tica
rcill
in/c
lavu
lani
cac
idE
rtap
enem
Am
pici
llin/
sulb
acta
mTi
carc
illin
/cla
vula
nic
acid
Ert
apen
emC
efot
etan
Cef
oxiti
nP
iper
acill
in/ta
zoba
ctam
Imip
enem
/cila
stat
inM
erop
enem
Cef
urox
ime
orce
fazo
linpl
usm
etro
nida
zole
Fluo
roqu
inol
oneb
plus
met
roni
dazo
le
Cef
urox
ime
plus
met
roni
dazo
leC
ipro
floxa
cin
plus
met
roni
dazo
leA
ztre
onam
plus
clin
dam
ycin
Third
/fou
rth-
gene
ratio
nce
phal
ospo
rinc
plus
anan
tiana
erob
eA
min
ogly
cosi
ded
plus
anan
tiana
erob
eH
igh
risk
(cat
egor
ized
as“h
igh-
se-
verit
yin
fect
ions
”by
the
IDS
Aan
d“h
ighe
r-ris
kpa
tient
s”by
the
SIS
)
Pip
erac
illin
/tazo
bact
amIm
ipen
em/c
ilast
atin
Mer
open
em
Pip
erac
illin
/tazo
bact
amIm
ipen
em/c
ilast
atin
Mer
open
em
Cip
roflo
xaci
npl
usm
etro
nida
zole
Azt
reon
ampl
usm
etro
nida
zole
Third
/fou
rth-
gene
ratio
nce
phal
ospo
rinc
plus
met
roni
dazo
le
Cip
roflo
xaci
npl
usm
etro
nida
zole
Azt
reon
ampl
uscl
inda
myc
inTh
ird/f
ourt
h-ge
nera
tion
ceph
alos
porin
cpl
usan
antia
naer
obe
Am
inog
lyco
side
dpl
usan
antia
naer
obee
NO
TE
.A
dapt
edfr
om[4
0]an
dfr
om[4
8].
aB
ecau
sein
crea
sing
resi
stan
ceof
Esc
heric
hia
coli
toam
pici
llin
and
toam
pici
llin/
sulb
acta
mha
sbe
enre
port
ed,
loca
lsus
cept
ibili
typr
ofile
ssh
ould
bere
view
edbe
fore
use.
bC
ipro
floxa
cin,
levo
floxa
cin,
mox
iflox
acin
,or
gatifl
oxac
in.
cC
efep
ime,
cefo
taxi
me,
ceft
azid
ime,
ceft
izox
ime,
orce
ftria
xone
.d
Am
ikac
in,
gent
amic
in,
netil
mic
in,
orto
bram
ycin
.e
Clin
dam
ycin
orm
etro
nida
zole
.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S66 • CID 2008:47 (Suppl 2) • Kollef et al.
Table 7. Organisms reported in a study of postoperative peri-tonitis by Montravers et al. [52].
OrganismNo. of
isolates
Gram negativeEscherichia coli 53Proteus/Morganella species 25Pseudomonas species 21Klebsiella species 14Enterobacter cloacae 10Acinetobacter/Citrobacter/Serratia species 10
Gram positiveMethicillin-resistant Staphylococcus species 24Enterococcus faecalis 19Enterococcus faecium 19
AnaerobeBacteroides species 13Candida species 23
NOTE. Adapted from [52], with permission from the University of ChicagoPress. Some patients had 11 isolate.
in the Asia/Pacific region and Latin America. Extended-spec-
trum b-lactamases (ESBLs) were detected phenotypically in
10% of E. coli, 17% of Klebsiella species, and 22% of Entero-
bacter species worldwide, representing an increase from the 2
previous years.
In this large surveillance program, an additional analysis of
7002 E. coli isolates documented that increasing resistance rates
have been seen in both community-acquired and hospital-ac-
quired E. coli infections [56]. Ampicillin-sulbactam was the least
active agent (45.1%–67.6% of isolates were susceptible). Quin-
olones (ciprofloxacin and levofloxacin) also demonstrated low
activity (69%–75% susceptible). E. coli isolated !48 h after
hospital admission (presumed to be community acquired) were
more often susceptible to the agents tested than were E. coli
isolated 148 h after hospitalization (presumed to be hospital
acquired). There were small differences in susceptibility rates
between community-acquired and hospital-acquired E. coli for
the carbapenems and amikacin, but there were more sizable
differences for other agents, including ampicillin-sulbactam
(60.3% vs. 48.4%), ciprofloxacin (83.7% vs. 71.6%), and levo-
floxacin (83.8% vs. 73.5%). Antimicrobial resistance among
gram-negative bacteria isolated from IAIs, both community
acquired and nosocomial, is emerging as a more significant
problem worldwide.
Although resistance rates are of growing concern, there are
rare studies that examine the consequences of resistance and
adequate empirical treatment for outcomes. A retrospective co-
hort study by Peralta et al. [57] analyzed patients with E. coli
bacteremia to identify associations between antibiotic resistance,
adequacy of empirical therapy, and mortality. Of the 663 patients
included in the study, those with MDR E. coli bacteremia had a
significantly lower frequency of correct empirical treatment than
did patients with non-MDR E. coli bacteremia (relative risk [RR],
0.53; 95% CI, 0.48–0.67), coupled with a considerably higher
mortality rate (RR, 3.31; 95% CI, 1.72–6.36).
A prospective observational study by Seguin et al. [58] re-
ported factors associated with MDR bacteria in secondary peri-
tonitis. Forty-four cases of community-acquired peritonitis and
49 cases of nosocomial peritonitis (35 postoperative cases) were
reported. In univariate analysis, the risk of acquiring an MDR
organism was significantly associated with a higher Acute Phys-
iology and Chronic Health Evaluation (APACHE) II score. In
addition, preoperative length of hospital stay, previous anti-
microbial therapy, and the duration and modification of post-
operative antimicrobial therapy were significantly associated
with the presence of MDR bacteria. Multivariate analysis confir-
med that patients with a preoperative length of hospital stay
of �5 days had a higher risk for developing an MDR IAI,
especially if antibiotics had been used previously. The authors
concluded that knowledge of these 2 risk factors for acquiring
MDR bacteria (preoperative length of stay and prior use of
antibiotics) enables the use of expanded-spectrum empirical
antimicrobial therapy for these specific high-risk patients.
No studies were identified that specifically focused on the
epidemiology and/or incidence of MDR organisms of “health
care–associated” IAIs. Additional discussion regarding the po-
tential definition of health care–associated IAIs and patients
who would be included in such a category suggested that it
could include patients with cIAIs such as peritoneal dialysis-
catheter infections, patients with spontaneous bacterial peri-
tonitis with multiple prior episodes, and patients in nursing
homes or long-term-care facilities who develop cIAIs including
appendicitis, cholecystitis, and diverticulitis. There is no con-
sensus as to whether this category of “health care–associated
cIAI” should be created.
Grading of Evidence
On the basis of a review of the studies cited above, the workshop
members agreed that there was substantial evidence to accept
the statement. In evaluating the nature of the evidence, 40%
voted category II, 20% voted category III, and 40% voted cat-
egory IV (table 3).
Level of Support
When voting on the support for this statement, 0% of the
summit participants voted to accept the statement completely,
27% voted to accept the statement with some reservations, 64%
voted to accept the statement with major reservations, 9% voted
to reject the statement with reservations, and 0% voted to reject
the statement completely. In comparison, of the 744 IDSA
members who participated in the online survey, 30% voted to
accept the statement completely, 38% voted to accept the state-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S67
Figure 2. Voting comparison for statement 2 (“Patients with health care–associated intra-abdominal infections should receive dual empiric therapyfor resistant gram-negative and gram-positive pathogens”). “IDSA” refers to the members of the Infectious Diseases Society of America who respondedto a Web-based survey; “Summit” refers to the Health Care–Associated Infection Summit panel.
ment with some reservations, 11% voted to accept the state-
ment with major reservations, 18% voted to reject the statement
with reservations, and 3% voted to reject the statement com-
pletely (figure 2).
Discussion
In summary, a review of the literature produced very limited
retrospective studies in general support of the statement. How-
ever, in practice, patients suspected of having risk factors for
a “health care–associated” infection typically receive empirical
therapy for MDR gram-positive and gram-negative organisms.
On the basis of the presented studies of patients with secondary
peritonitis, it is reasonable to assume that certain patient sub-
groups were infected with a different spectrum of bacteria, as
well as with MDR bacteria. The current studies of patients with
secondary peritonitis document that appropriate empirical an-
tibiotic coverage as well as coverage for MDR organisms lead
to improved outcomes.
Future Directions
Traditional categorization of IAIs has segregated them as nos-
ocomial or community-acquired infections. In recent years,
epidemiologic studies have identified that pathogens associated
with cIAI demonstrate rising levels of drug resistance in both
groups. It has also been shown that inadequate initial empirical
therapy is associated with a significantly higher rate of failures
and death. On the basis of studies of patients with postoperative
peritonitis, it is reasonable to suggest that select patients may
benefit from broad-spectrum empirical therapy. For patients
with peritonitis, several attempts have been made to identify
clinical features that increase the risk of adverse outcomes. For
these patients, the IDSA suggests that antimicrobial regimens
with expanded spectra may be warranted. Finally, given the
different spectrum of pathogens and the varying levels of re-
sistance seen in patients with peritonitis, an effort should be
made to identify other patient types and specific risk factors
for IAIs due to resistant pathogens. Because unnecessary broad-
spectrum therapy is associated with its own problems, caution
should be exercised. Future studies will need to be conducted
to examine whether health care–associated cIAI should be de-
lineated as a separate category of IAIs before specific recom-
mendations can be made.
STATEMENT 3: EARLY AGGRESSIVE,APPROPRIATE EMPIRIC TREATMENTAND DE-ESCALATION FOR HCAP REDUCESMORTALITY AND MINIMIZES RESISTANCE
Rationale and Definition of Statement
A designation of “health care–associated” infection was first
used for cases of bacteremia in which patients who acquired
bacteremia as outpatients were found to have pathogens usually
associated with hospital-acquired infections [6]. Of significance,
the term referred only to patients who were hospitalized with
an infection, not to those who remained in their nonhospital
setting. The term “health care associated” seemed to apply to
a variety of infections, including pneumonia, with a similar
propensity to be caused by typically nosocomial pathogen. The
concept of HCAP was therefore readily embraced. For this
reason, HCAP was included in the latest statement on HAP
from the ATS and IDSA [1] and was essentially excluded from
discussion in the recent IDSA-ATS consensus guidelines on the
management of CAP [2].
Because several principals of treatment have been thought
to be important for outcomes among patients with HAP and
VAP, logic would suggest that these principals are applicable to
HCAP as well. These principals include: (1) early initiation of
empirical antibiotic treatment; (2) use of broad-spectrum, em-
pirical, antibiotic therapy to avoid inappropriate therapy; and
(3) narrowing or “de-escalation” of empirical antibiotic therapy
on the basis of results of respiratory-tract cultures [1]. The
purported benefits of such an approach were to decrease the
mortality associated with inappropriate initial antibiotics while,
at the same time, lessening the emergence of antibiotic-resistant
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S68 • CID 2008:47 (Suppl 2) • Kollef et al.
pathogens. Although it may be logical to assume that these
principals and expected results apply to HCAP, this section aims
to assess the strength of evidence supporting this assertion.
Methods
A PubMed search was performed on 1 October 2007. With the
search limited to the English language, the term “health care
associated OR healthcare associated OR health care-associated
OR healthcare-associated” gave a total of 33,408 articles. This
result combined with the term “pneumonia” resulted in a total
of 333 articles. This result combined with the term “treatment”
yielded 309 articles. The abstracts were reviewed for pertinence,
and additional “related articles” were also screened. The text
word “antibiotic” was also combined with the 333 health care–
associated/pneumonia articles, resulting in 87 common articles.
Abstracts of all these articles were examined, as were the “related
articles” for each. One apposite article was found.
As a consequence of the overlap of HCAP with other pneu-
monia terms, additional searches were performed. Combina-
tion of the terms “nursing home AND pneumonia AND treat-
ment” resulted in 262 English language articles and 1 relevant
article.
Evidence
No randomized, controlled trials of treatment specific to hos-
pitalized patients with HCAP were found. No concurrent co-
hort studies of antibiotic treatment in general for hospitalized
patients with HCAP were found. Only 1 randomized, controlled
trial involving nursing home patients that specifically addressed
treatment in the nursing home was available [59].
No category I evidence for any aspect of the statement.
Because the entity of HCAP has been defined only recently,
studies of either CAP or HAP may have bearing on the state-
ment; therefore, this evidence will also be reviewed. Further-
more, because the statement is multifaceted, each statement
component will be discussed separately.
Appropriate empirical therapy. Only 1 study specifically
addressed the issue of appropriate empirical therapy for HCAP
[59]. This was a preintervention and postintervention study of
the management of nursing home–acquired pneumonia with
either oral or parenteral antibiotic therapy. The actual inter-
vention was a guideline for the indication for parenteral an-
tibiotics in a randomized study of 10 skilled-nursing facilities
involving either a multidisciplinary or a physician-only training
program. After the intervention, use of parenteral antibiotics,
when indicated by guidelines, increased significantly ( )P ! .02
without differences by randomization. No overall mortality
benefit was seen. Emergence of resistance was not addressed.
Because 35%–40% of patients ultimately required hospitali-
zation, the results have some pertinence to the issue of HCAP.
The issue of appropriate antibiotic therapy for HCAP re-
volves around the microbial etiology of HCAP, specifically
whether broad-spectrum antibiotic therapy is needed to em-
pirically cover MDR pathogens, such as P. aeruginosa, MRSA,
and ESBL-producing Enterobacteriaceae. Surprisingly, only 3
epidemiologic studies address this issue specifically. Two ret-
rospective US studies focused on culture-positive cases; the first
study examined a large administrative database [7], and the
second analyzed a single large tertiary care referral hospital [8].
Both studies demonstrated that HCAP was more common than
CAP, with a high frequency (20%–25%) of each of the MDR
pathogens listed above. Conversely, another study involving a
Spanish, multicenter, prospective, observational cohort of pa-
tients admitted with pneumonia found that only 17.3% of cases
could be classified as HCAP and that the incidences of cases
of pneumonia caused by gram-negative organisms (other than
Legionella species and Hemophilus influenzae, typical CAP path-
ogens) and S. aureus were both !5% [60]. However, 32% of
patients with HCAP in this study did not receive a microbi-
ological diagnosis, and an additional 20% received a diagnosis
of aspiration pneumonia, which left a positive microbiological
diagnosis for !50%.
Several explanations for these major differences in etiology
of HCAP exist. By far the most important is the inclusion of
HCAP cases without a microbiological diagnosis. Others in-
clude differences in criteria (all immunocompromised patients
included vs. only severely immunocompromised patients in-
cluded; previous hospitalization in the past 12 months vs. the
past 3 months), different types of hospitals (major referral cen-
ters vs. smaller local hospitals), and study design (retrospective
vs. prospective).
Even if MDR pathogens occur at high frequency, the use of
broad-spectrum therapy is still of unclear benefit with regard
to mortality. Two studies, both using the before-after interven-
tion format, specifically addressed this issue. Ibrahim et al. [61]
found that the use of a 3-drug, broad-spectrum protocol for
late-onset VAP was able to decrease the percentage of patients
administered inappropriate initial empirical antibiotic therapy
to 5.8%, as opposed to 52% before protocol introduction. Mor-
tality was unaffected, although the incidence of recurrent VAP
and subsequent infection with MDR pathogens decreased. The
second study [62], which used a similar type of empirical pro-
tocol, also demonstrated that the use of inappropriate initial
antibiotic therapy was decreased significantly, and broader-
spectrum therapy resulted in decreased mortality at 14 days
after treatment (27% vs. 8%; ). However, the statisticallyP p .03
significant reduction in mortality was not maintained for 30-
day or in-hospital mortality.
An additional article from the CAP literature on cases of
pneumonia caused by gram-negative pathogens from a pro-
spective CAP database was pertinent and thus was reviewed
[63]. Most patients with CAP caused by gram-negative path-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S69
ogens had risk factors that would likely qualify them for HCAP
status. Provision of appropriate initial therapy was not asso-
ciated with a significant improvement in mortality (32% vs.
13%; ).P p .27
In summary, despite being intuitively logical and supported
by multiple retrospective studies, no prospective study of VAP,
nursing home–acquired pneumonia, HCAP, or CAP has dem-
onstrated a mortality benefit from broader-spectrum proto-
colized antibiotic regimens, despite efforts made to consistently
decrease rates of inappropriate therapy to low levels. Thus, the
support for a mortality benefit of aggressive broad-spectrum
therapy for HCAP cannot even be extrapolated from studies
of other types of pneumonia.
Aggressive empirical therapy. The use of the broad-spec-
trum multiple-drug regimens discussed above can be considered
aggressive empirical therapy. However, the only published study
specifically addressing HCAP is a retrospective review of van-
comycin dosing for patients with HAP and HCAP [64]. The
authors compared dosing that was adjusted to achieve a serum
trough level of 115 mg/mL, as recommended by the ATS-IDSA
guidelines because of poor outcomes with standard dosing. The
group that achieved trough levels greater than this threshold did
not have a mortality benefit and had more adverse effects [65].
Early empirical therapy. The timing of appropriate antibi-
otic therapy has received significant attention. No study of HCAP
has specifically examined the timing of antibiotic therapy. How-
ever, 2 large retrospective reviews of Medicare patients suggested
a survival advantage when there was earlier provision of anti-
biotics [66, 67]. Many of these patients were likely to have HCAP.
Although significant differences in mortality among patients re-
ceiving antibiotics in the first 4–8 h were documented, the trend
toward increased mortality was heterogeneous, with some of the
highest mortality rates found among those who received anti-
biotics in the first 2 h after presentation to the emergency de-
partment. More importantly, prospective studies of CAP guide-
line implementation have demonstrated that mortality is
unchanged despite significant increases in the proportion of
patients receiving antibiotics within 4 or 8 h [68].
The only prospective trial involving VAP did not show a
difference in mortality if antibiotics were started empirically
when VAP was suspected, compared with when the culture
results were returned [69]. However, the study was limited to
trauma patients for whom an attributable mortality due to VAP
was unclear and VAP was less likely to have been caused by
MDR pathogens. Duration of ventilation was increased for pa-
tients randomized to receive culture-directed treatment. Ret-
rospective data from a medical ICU population suggest that a
delay of 24 h in initiating therapy is associated with excess
mortality [70].
The strongest evidence in favor of early antibiotic therapy is
from a retrospective review of septic shock, in which every 1-
hour delay in initiation of antibiotic therapy was associated
with a 7.6% increase in mortality [4]. In this study, 37% of
patients had pneumonia.
Early de-escalation of empirical therapy. De-escalation has
a variety of definitions. The most accepted definition is a de-
crease in the number of different antibiotics being used for
treatment; however, de-escalation may also include switching
to a narrower-spectrum agent, shortening the duration of ther-
apy, or even ceasing the administration of antibiotics altogether
when culture results are negative.
Both before-after antibiotic treatment protocols included de-
creasing the number of empirical antibiotics (once culture re-
sults were known), as well as the duration of use [61, 62].
Although neither protocol was associated with a mortality ben-
efit, the use of very-broad-spectrum antibiotics and de-esca-
lation was associated with a decrease in the subsequent occur-
rence of colonization or infection with MDR pathogens [61,
62, 71]. Some evidence of antibiotic pressure was seen in the
study by Soo Hoo et al. [62], in which 6 of the 7 imipenem-
resistant isolates occurred in patients given the more aggressive
empirical regimen (which included imipenem). Two additional
randomized trials are significant. Singh et al. [71] demonstrated
that, among patients with HAP or VAP who have a persistently
low clinical pulmonary infection score, the discontinuation of
antibiotic therapy after 3 days was associated with a decrease
in the percentage of pathogens that were MDR (14% vs. 38%;
) and a trend toward mortality differences. Chastre etP p .017
al. [72] demonstrated that patients with VAP randomized to
receive 8 days of therapy had lower rates of emergence of MDR
pathogens than did those who received 15 days of therapy
(42.1% vs. 62%; ). A randomized, controlled trial ofP p .04
diagnostic methods also demonstrated that, when fewer anti-
biotics were used, the 14-day mortality (16.2% vs. 25.8%;
) and severity-adjusted 28-day mortality were de-P p .022
creased, although no differences in the emergence of MDR
pathogens was demonstrated (61.3% vs. 59.8%; ) [73].P 1 .2
In summary, early de-escalation of therapy has an unclear
association with decreased mortality. The strongest support
comes from avoiding or discontinuing antibiotic therapy com-
pletely, rather than narrowing the spectrum or decreasing the
number of antibiotics. Conversely, any type of de-escalation is
associated with a decrease in the emergence of MDR pathogens.
The major benefit appears to occur with a decrease in the overall
duration of therapy, rather than de-escalation per se.
Grading of Evidence
On the basis of a review of the studies cited above, 83% of the
members of this workshop agreed that the nature of the evi-
dence available to support this statement was category II for
the statement in general, with the remainder grading the evi-
dence as category III (table 3).
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S70 • CID 2008:47 (Suppl 2) • Kollef et al.
Figure 3. Voting comparison for statement 3 (“Early aggressive, appropriate empiric treatment and de-escalation for HCAP reduces mortality andminimizes resistance”). “IDSA” refers to the members of the Infectious Diseases Society of America who responded to a Web-based survey; “Summit”refers to the Health Care–Associated Infection Summit panel. HCAP, health care–associated pneumonia.
Level of Support
When voting on the support for this statement, 55% of the
workshop members voted to accept the statement with some
reservations, and 45% voted to accept the statement with major
reservations. In comparison, of the 744 IDSA members who
participated in the online survey, 56% voted to accept the state-
ment completely, 36% voted to accept the statement with some
reservations, 5% voted to accept the statement with major res-
ervations, 2% voted to reject the statement with reservations,
and 1% voted to reject the statement completely (figure 3).
Discussion
The difference between the voting of the workshop participants
and that of the IDSA members is striking. The most likely
explanation is an overestimation of the literature support for
the concept of HCAP. Only 3 studies have specifically addressed
HCAP [7, 8, 60]. Most of the other information is extrapolated
from either HAP/VAP or CAP literature.
The second major issue is the over-reliance on retrospective
studies, which is particularly true for data on inappropriate
initial empirical therapy, for which multiple retrospective stud-
ies consistently show excess mortality among patients receiving
inappropriate initial empirical therapy [1]. The prospective tri-
als of broad-spectrum empirical therapy with de-escalation do
not demonstrate that providing appropriate initial antibiotics
is sufficient to improve mortality [61, 62]. One explanation for
this seemingly paradoxical finding between retrospective and
prospective trials is that antibiotics for MDR pathogens may
frequently be ineffective, despite being appropriate [1].
Another explanation may be that the patient’s host response
is unable to cure the pneumonia despite antibiotic therapy.
Here, the difference between CAP and HAP, especially VAP, is
likely to be great. Many VAP cases occur during a period of
relative immunoparalysis after initial ICU admission for a crit-
ical illness [74]. In contrast, most CAP cases are characterized
by a proinflammatory state. Although the pathogens associated
with HCAP may resemble HAP and/or VAP, it is unclear
whether the physiologic response will vary in the same way.
Future Directions
No prospective, randomized trial comparing appropriate versus
inappropriate initial antibiotic therapy for HCAP has been per-
formed. Therefore, the only information regarding the benefit
of early appropriate initial therapy will have to come from
studies of alternative empirical regimens, such as those for VAP.
Given the wide discrepancy in the frequencies of MDR path-
ogens in HCAP cases in recent studies, this type of study is
clearly needed.
STATEMENT 4: HEALTH CARE–ASSOCIATEDBSIs REQUIRE EMPIRIC COVERAGE FOR MDRGRAM-NEGATIVE BACTERIA AND MRSA,AS WELL AS COVERAGE FOR FUNGALPATHOGENS IN PATIENTSWITH SPECIFIC RISK FACTORS
Rationale and Definition of Statement
BSI is a common and potentially lethal complication of health
care contact. A significant minority of hospitalized patients
develop a BSI. Among these patients, mortality rates are high.
This high mortality may be caused in part by the emergence
of antimicrobial resistance in pathogens associated with the
health care system. Such antimicrobial resistance increases the
possibility of inadequate empirical antimicrobial therapy, which
can delay the time until effective antimicrobial therapy is
administered.
The entity of health care–associated BSI was first defined by
Friedman et al. [6] as involving a positive culture result from
a blood specimen that was obtained from a patient within 48
h after admission if the patient received intravenous therapy,
wound care, or specialized nursing care or did any of the fol-
lowing: received self-administered intravenous medical therapy
in the 30 days before the BSI; attended a hospital or hemo-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S71
dialysis clinic or received chemotherapy in the 30 days before
the BSI; was hospitalized in an acute care hospital for �2 days
in the 90 days before the BSI; or resided in a nursing home or
long-term-care facility. A key finding of this study was that the
prevalence of antimicrobial-resistant pathogens among patients
with non-nosocomial health care–associated BSI (i.e., BSI that
did not originate in the hospital setting) resembled that among
patients with nosocomial BSI. Thus, for the purposes of the
present article, HAIs are defined as both nosocomial and non-
nosocomial HAIs.
Methods
A PubMed search related to health care–associated BSI was
completed on 28 September 2007. The search terms “health
care associated,” “health care-associated,” “healthcare associ-
ated,” and “healthcare associated OR health care-associated OR
health care associated OR healthcare-associated” gave a total
of 54,638 articles. The search terms “blood stream infection,
bloodstream infection, bacteremia,” “bloodstream infection,”
and “blood stream infection,” combined using the “OR” func-
tion, yielded a total of 27,839 articles. The search term “inef-
fective therapy OR ineffective antibiotic therapy OR delayed
antibiotic treatment OR delayed receipt of effective antimicro-
bial therapy OR inadequate antimicrobial treatment OR delay
in effective therapy” yielded a total of 24,230 articles. Com-
bining the “bloodstream infection…” search with the “ineffec-
tive therapy…” search, using the “AND” function, resulted in
a total of 232 articles. All these articles were reviewed; 13 were
relevant to the statement.
Evidence
Health care–associated status is a risk factor for ineffective an-
tibiotic therapy of BSI. One study specifically focused on the
impact of health care–associated status on the likelihood of in-
effective therapy for patients with BSI [75]. In this prospective,
multicenter, cohort study of 466 adults with BSI, only 132 (28%)
had community-acquired BSI. The most common pathogens in
BSI were E. coli (14.2%) and MRSA (13.1%). Although the mi-
crobiological characteristics of nosocomial and non-nosocomial
health care–associated BSIs were similar, microbiological char-
acteristics of both groups differed significantly from those of
community-associated BSI. In multivariable logistic regression
analysis, both health care–associated (OR, 3.1; 95% CI, 1.6–6.1)
and nosocomial (OR, 4.3; 95% CI, 2.2–8.3) status were inde-
pendently associated with ineffective initial antibiotic therapy.
Specific causes of BSI, including MRSA (OR, 1.7; 95% CI, 1.0–
2.8) and Enterococcus species (OR, 2.3; 95% CI, 1.3–4.1), were
also associated with ineffective initial therapy.
Assessment of association between appropriate antibiotic
therapy and mortality in patients with bacteremia. Studies
of the association between inappropriate therapy and mortality
among patients with bacteremia have yielded conflicting results.
One recent article [76] systematically reviewed the published
literature evaluating the association between inappropriate an-
tibiotic therapy and mortality among patients with bacteremia.
The authors found that 51 studies meeting their inclusion cri-
teria exhibited significant heterogeneity in design, definition,
measurement of variables, and statistics. Thirty-four studies
(67%) measured the severity of illness, but only 6 (12%) spec-
ified when it was assessed. Only 8 studies (16%) defined in-
appropriate antibiotic therapy as that which was inactive in
vitro against the isolated organism and was not consistent with
current clinical practice recommendations and also distin-
guished between empirical and definitive treatment. McGregor
et al. [76] identified key methodological recommendations to
improve the validity and generalizability of future studies, in-
cluding a robust, consistent definition of “inappropriate” ther-
apy based on in vitro susceptibility data; separate consideration
of empirical and definitive therapy; and appropriate statistical
adjustment for the baseline severity of illness of the patient.
Association between patient outcome and antibiotic therapy
for BSI caused by MDR gram-negative pathogens. A recent
meta-analysis of 16 peer-reviewed studies examined associa-
tions between ESBL production in Enterobacteriaceae species
causing bacteremia, time to effective antibiotic therapy, and
patient mortality [77]. Meta-analysis of crude RR demonstrated
a significantly increased incidence of delay in effective therapy
(pooled RR, 5.56; 95% CI, 2.94–10.51; ) and signifi-P ! .001
cantly increased mortality (pooled RR, 1.85; 95% CI, 1.39–2.47;
) in bacteremia caused by ESBL-producing bacteria.P ! .001
The meta-analysis was unable to evaluate adjusted mortality,
because only 1 of the 16 included studies reported these data.
A total of 7 additional reports were published after the en-
rollment period for the meta-analysis [78–84]. All were ret-
rospective, and all but 1 was a single-center study [80]. Most
[1, 5, 7, 10,78, 81, 82, 84] but not all [79, 83] of the 7 additional
studies found an association between delayed effective therapy
for BSI caused by MDR gram-negative pathogens and mortality.
Consistent with the report by McGregor et al. [76], significant
heterogeneity existed among the 7 studies in patient population,
definitions of delayed antibiotic therapy, follow-up period, and
statistical methodology. Moreover, establishing the risks of at-
tributable mortality remains difficult.
Using classification and regression tree (CART) analysis,
Lodise et al. [81] evaluated the relationship between delayed
appropriate antibiotic therapy and risk of 30-day mortality in
100 patients with nosocomial P. aeruginosa bacteremia. Delayed
antibiotic therapy was defined using CART analysis as receipt
of effective antibiotic therapy 152 h after the culture result was
obtained. Mortality was significantly higher among patients
with delayed appropriate antibiotic therapy than among pa-
tients whose therapy was not delayed (44% vs. 19%; P p
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S72 • CID 2008:47 (Suppl 2) • Kollef et al.
). Appropriate antibiotic therapy delayed 152 h was in-.008
dependently associated with resistance to 13 antibiotic classes
(adjusted OR [AOR], 4.6; 95% CI, 1.9–11.2; ), chronicP p .001
obstructive pulmonary disease (AOR, 5.4; 95% CI, 1.5–19.7;
), and 30-day mortality (OR, 4.1; 95% CI, 1.2–13.9;P p .01
) among patients with P. aeruginosa BSI.P p .03
Tumbarello et al. [84] sought to identify the impact of in-
adequate initial antibiotic therapy (defined as initiation of treat-
ment with active antimicrobial agents 172 h after collection of
the first positive blood culture specimen) on 21-day mortality
in 186 hospitalized patients with BSI caused by ESBL-producing
organisms. Patients receiving inadequate treatment had a 3-fold
increase in mortality, compared with the group receiving ade-
quate treatment (59.5% vs. 18.5%; 95% CI, 1.76–3.22; ).P ! .001
In multivariate analysis, the significant predictors of mortality
were inadequate initial antimicrobial therapy (OR, 6.28; 95% CI,
3.18–12.42; ) and unidentified primary infection siteP ! .001
(OR, 2.69; 95% CI, 1.38–5.27; ). The antibiotic regimensP p .004
most frequently classified as inadequate were based on oxyimino
cephalosporin or fluoroquinolone therapy.
Using a multicenter, nested, case-control study, Hyle et al.
[80] evaluated the association of inadequate initial antimicro-
bial therapy with mortality in 187 patients with BSI caused by
ESBL-producing organisms. Initial antimicrobial therapy was
defined as inadequate when there was 148 h between the time
a culture specimen was obtained and the initiation of therapy
with an agent to which the infecting organism was susceptible.
Infection with MDR ESBL-producing E. coli or Klebsiella species
(AOR, 14.58; 95% CI, 1.91–111.36) and health care–acquired
infection with ESBL-producing E. coli or Klebsiella species
(AOR, 4.32; 95% CI, 1.49–12.54) were independent risk factors
for inadequate initial antimicrobial therapy, and inadequate
initial antimicrobial therapy was an independent risk factor for
mortality among patients with nonurinary infection with ESBL-
producing E. coli or Klebsiella species (AOR, 10.04; 95% CI,
1.90–52.96).
Anderson et al. [78] used multivariable logistic regression to
identify predictors of all-cause in-hospital mortality among 60
patients with bacteremia due to ceftazidime-resistant Klebsiella
pneumoniae. Only 72% of patients received effective therapy
within 5 days after the diagnosis of BSI. Delay in the initiation
of effective therapy for 172 h after diagnosis of BSI was an
independent predictor of mortality (OR, 3.32; 95% CI, 1.07–
10.3; ).P p .04
Micek et al. [82] evaluated 305 patients with P. aeruginosa
BSI to determine whether the administration of appropriate
initial antimicrobial treatment was associated with a better clin-
ical outcome and to examine the relationship between the em-
pirical administration of combination antimicrobial therapy for
gram-negative pathogens and appropriate treatment for P. aeru-
ginosa BSI [82]. In-hospital mortality was statistically greater
for patients receiving inappropriate initial antimicrobial treat-
ment than for patients receiving appropriate initial treatment
(30.7% vs. 17.8%; ). Multiple logistic regression anal-P p .018
ysis identified inappropriate initial antimicrobial treatment
(AOR, 2.04; 95% CI, 1.42–2.92; ) as an independentP p .048
predictor of in-hospital mortality. An appropriate initial anti-
microbial regimen was administered more often to patients
receiving empirical combination antimicrobial treatment for
gram-negative bacteria than to those receiving empirical mono-
therapy (79.4% vs. 65.5%; ).P p .011
Two studies found no increased risk with delayed effective
therapy for BSI caused by MDR gram-negative pathogens. Osih
et al. [83] assessed the effect of appropriate empirical therapy
on in-hospital mortality and length of stay among 167 patients
with P. aeruginosa BSI. Adequate empirical antibiotic therapy
was defined on the basis of in vitro susceptibility testing from
8 h before the first positive blood culture to the time the sus-
ceptibility results were known. After adjustment for age, severity
of illness, and time at risk, appropriate empirical antibiotic
therapy was not significantly associated with mortality (OR,
0.96; 95% CI, 0.31–2.9; ). Deal et al. [79] sought toP p .58
identify predictors of in-hospital mortality among 124 patients
with bacteremia caused by Enterobacter or Citrobacter species
from 1998 through 2004. Appropriate empirical antibiotic ther-
apy was administered to three-quarters of the patients and was
similar among survivors and nonsurvivors (74% vs. 81%;
). An important limitation to this investigation wasP p .51
sample size.
Association between patient outcome and antibiotic therapy
for MRSA bacteremia. Two meta-analyses involving 16000
staphylococcemic patients have shown that the mortality rate
among patients with MRSA bacteremia was significantly greater
than that among patients with MSSA bacteremia [85, 86]. Using
data from 13900 patients from 30 studies, Cosgrove et al. [85]
showed that mortality was significantly higher among patients
with MRSA bacteremia than among patients with MSSA bac-
teremia (36% vs. 23%; RR, 1.42; 95% CI, 1.25–1.63; ).P ! .001
Whitby et al. [86] reviewed 9 studies of nosocomial S. aureus
bacteremia published in 1990–2000. In this analysis, the RR of
death also was significantly higher among patients with MRSA
bacteremia (29% vs.12%; RR, 2.12; 95% CI, 1.76–2.57; P !
)..001
Several investigations have sought to quantify the impact of
delayed effective therapy on outcomes for patients with MRSA
bacteremia [87–90]. Results have varied, with 2 studies finding
no difference in mortality, and 2 studies finding higher mortality
rates among patients with MRSA bacteremia receiving delayed
antibiotic therapy. Roghmann et al. [90] retrospectively evaluated
132 episodes in 128 patients with MRSA bacteremia to estimate
the impact of delayed initiation of vancomycin on clinical out-
comes. Patients with MRSA bacteremia were significantly less
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S73
likely to receive effective antibiotic therapy during the first 48 h
of hospitalization (45% vs. 98%; ) than were patients withP ! .01
MSSA bacteremia. However, this ineffective empirical therapy
was not significantly associated with an increased mortality risk
(RR, 0.82; 95% CI, 0.36–1.88) and did not change significantly
when adjusted for age, occurrence of sepsis, or nosocomial in-
fection. Kim et al. [88] evaluated 238 retrospectively identified
patients with MRSA bacteremia who received vancomycin or
ineffective therapy. Using a propensity-matching case-control de-
sign to adjust for confounding introduced by the clinician’s
choice of antibiotic, these investigators compared the outcomes
for patients with MRSA bacteremia who received inappropriate
empirical therapy with those of control patients with a similar
score but who received vancomycin. In the matched case-control
analysis of 50 propensity score–matched pairs with MRSA bac-
teremia, inappropriate empirical antibiotic therapy was not as-
sociated with a statistically significant difference in mortality (OR,
1.15; 95% CI, 0.51–2.64).
By contrast, 2 investigations found higher mortality among
patients receiving delayed effective therapy for S. aureus bac-
teremia. Using CART analysis, Lodise et al. [89] evaluated the
impact of delayed effective therapy on 167 retrospectively iden-
tified patients with nosocomial S. aureus bacteremia. The break-
point between delayed and early therapy by use of CART anal-
ysis was 44.75 h. In a multivariate analysis, delayed treatment
was found to be an independent predictor of infection-related
mortality (OR, 3.8; 95% CI, 1.3–11.0; ) and was as-P p .01
sociated with longer hospital stay when compared with early
treatment (20.2 vs. 14.3 days; ). The authors concludedP p .05
that delay of therapy has deleterious effects on clinical outcomes
and underscores the importance of early appropriate therapy.
Similar conclusions were reached by Khatib et al. [87], who
found that, in a cohort of 342 retrospectively identified patients
with S. aureus bacteremia, the time to effective antibiotic ther-
apy was longer for MRSA-infected patients than for MSSA-
infected patients (25.5 vs. 9.6 h; ) and all-cause mor-P ! .0005
tality was higher among patients receiving inappropriate
therapy than among those receiving appropriate therapy (35.0%
vs. 20.9%; ).P p .02
Association between patient outcome and antimicrobial
therapy for fungal BSI in patients with specific risk factors.
Two studies evaluated the risk of delayed effective therapy in
fungemic patients. Garey et al. [91] evaluated the relationship
between treatment delay and mortality in 230 retrospectively
identified patients with Candida BSI. Although the mortality
was the lowest among patients who began therapy on day 0
(15%), day 1 (24%), day 2 (37%), or day 3 or later (41%)
( for trend), only 40% of patients received antifungalP p .0009
therapy within the first day. By multivariate modeling, increased
time (per day) to administration of fluconazole was indepen-
dently associated with mortality (AOR, 1.5; 95% CI, 1.09–2.09;
). In the second study, Morrell et al. [92] evaluatedP p .0138
157 candidemic hospitalized patients to identify the influence
of delayed empirical antifungal treatment on clinical outcome.
By multivariable analysis, administration of antifungal treat-
ment 112 h after the first positive blood culture specimen was
drawn (AOR, 2.09; 95% CI, 1.53–2.84; ) was inde-P p .018
pendently associated with in-hospital mortality. Of note, only
5.7% of patients received antifungal therapy within 12 h after
the initial positive result of blood culture. Investigators in both
of these studies concluded that delay in initiation of fluconazole
therapy for hospitalized patients with candidemia had a sig-
nificant impact on mortality. Delayed treatment of Candida BSI
could be minimized by the development of more-rapid diag-
nostic techniques for the identification of Candida BSI or
through increased use of empirical antifungal treatment for
selected patients at risk for fungemia.
Grading of Evidence
On the basis of a review of the studies cited above, the workshop
members considered the nature of the evidence supporting this
statement to be category II (67% of votes) or category III (33%
of votes) (table 3).
Level of Support
When voting on the support for this statement, 9% of the
summit participants voted to accept the statement completely,
73% voted to accept the statement with some reservations, and
18% voted to accept the statement with major reservations. In
comparison, of the 744 IDSA members who participated in the
online survey, 25% voted to accept the statement completely,
38% voted to accept the statement with some reservations, 16%
voted to accept the statement with major reservations, 17%
voted to reject the statement with reservations, and 4% voted
to reject the statement completely (figure 4).
Discussion
This statement is critically important, given the growing prob-
lems of sepsis, bacteremia [93], and antimicrobial resistance
[94]. The majority of the studies reviewed for this statement
support the assertion that delayed appropriate antibiotic ther-
apy is associated with higher mortality among patients with
BSIs. Although none of the studies were able to accurately
establish causal relationships between delayed appropriate an-
timicrobial therapy and increased mortality and most suffered
in one way or another from methodologic limitations [76],
their conclusions are generally consistent with current treat-
ment guidelines for other HAIs [1] and with previous reports
evaluating the impact of such treatment delays for patients with
sepsis [3]. As evidenced by the results of the IDSA membership
poll related to this statement, the important influence of time
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S74 • CID 2008:47 (Suppl 2) • Kollef et al.
Figure 4. Voting comparison for statement 4 (“Health care–associated BSIs require empiric coverage for MDR gram-negative bacteria and MRSA,as well as coverage for fungal pathogens in patients with specific risk factors”). “IDSA” refers to the members of the Infectious Diseases Society ofAmerica who responded to a Web-based survey; “Summit” refers to the Health Care–Associated Infection Summit panel. BSI, bloodstream infection;MDR, multidrug resistant; MRSA, methicillin-resistant Staphylococcus aureus.
to administration of effective antimicrobial therapy on the clin-
ical outcome also makes intuitive sense to many clinicians.
The primary “rate-limiting steps” to effective antimicrobial
therapy for health care–associated BSI remain diagnostics and
susceptibility testing. Even when guided by local antimicrobial
susceptibility, empirical therapy often becomes little more than
an educated guess. Until diagnostic strategies emerge to provide
real-time, point-of-care information on the identification and
susceptibility of a bloodstream pathogen, clinicians will be
forced to make important decisions about initial antibiotic se-
lection without the luxury of definitive data. In this light, ob-
servations from these studies are important.
Among patients with BSI caused by gram-negative patho-
gens, early effective therapy was usually associated with reduced
mortality, and the likelihood of accomplishing early effective
therapy was higher when combination empirical antimicrobial
therapy was employed. Obviously, clinicians should consider
both the risks and benefits of adding a second antibiotic—often
an aminoglycoside—to an empirical regimen to treat gram-
negative pathogens in individual patients. However, the pre-
dominance of MRSA as a cause of health care–associated bac-
teremia, the availability of an FDA-approved agent for the
treatment of S. aureus bacteremia and right-sided endocarditis
(e.g., daptomycin), and the prospects of several anti-MRSA
agents in late stages of clinical development emphasize the need
for appropriately designed clinical studies to better address this
important issue. Significant controversy remains over the role
of vancomycin for treatment of MRSA bacteremia—whether
empirical or targeted [95, 96].
Finally, the emerging importance of fungi as a cause of BSI
and sepsis is a potentially important change to consider in the
management of BSI. For example, in an evaluation of the hos-
pital discharge records of 110 million cases of sepsis in the
United States over 22 years, there was an annualized increase
in the incidence of sepsis of 8.7%, from ∼164,000 cases (82.7
per 100,000 population) to nearly 660,000 cases (240.4 per
100,000 population). During this time, the rate of sepsis due
to fungal organisms increased by 207% [93]. Given the in-
creasing importance of fungemia and the suggestion that early
empirical antifungal therapy may reduce mortality among pa-
tients with this infection, further studies are clearly needed to
help determine which patients, if any, should receive empirical
antifungal treatment.
Future Directions
Future directions discussed by the summit members reflected
many of the limitations indicated by McGregor et al. [76].
Appropriately designed epidemiologic studies with rigorous at-
tention to important design details are required, including a
consistent definition of “inappropriate” therapy based on in
vitro susceptibility data, separate consideration of empirical and
definitive therapy, and appropriate statistical adjustment for the
baseline severity of illness of the patient. The need for more-
rapid diagnostic tests was emphasized. Finally, until such bed-
side diagnostic technologies are available, additional studies to
identify patients at risk for colonization or infection with MDR
pathogens—especially the fungi—are required to best balance
the dual needs for judicious and effective empirical antimicro-
bial therapy for patients with BSIs.
STATEMENT 5: INITIAL APPROPRIATEANTIMICROBIAL THERAPY AND SOURCECONTROL ARE THE MOST IMPORTANTDETERMINANTS OF OUTCOME IN SEVERESEPSIS AND SEPTIC SHOCK
Rationale and Definition of Statement
Severe sepsis and septic shock are commonly encountered con-
sequences of severe infection, both community acquired and
hospital acquired [97]. Sepsis and its adverse sequelae, shock
and organ dysfunction, are currently the 10th leading cause of
death in the United States and one of the most common causes
of death in the noncoronary ICU [97, 98]. Martin et al. [93]
found that the incidence of sepsis in the United States has
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S75
dramatically increased over a 22-year period (1979–2000), from
82.7 cases per 100,000 population to 240.4 cases per 100,000
population, for an annualized increase of 8.7%. The incidence
of severe sepsis is predicted to continue to rise in the next 2
decades [99].
To prevent the progression to organ dysfunction and other
adverse sequelae of severe sepsis and septic shock, it is impor-
tant to identify the patient with sepsis as early as possible and
to institute effective therapy [97, 98, 100]. Representatives from
11 societies proposed a consensus guideline for severe sepsis
and septic shock management [101], and they recommended
the following actions: the early administration of effective an-
tibiotics, source control when appropriate, provision of early
goal-directed fluid resuscitation and vasopressor support when
required, maintenance of adequate oxygenation and ventilation
as necessary, use of physiologic steroid-replacement therapy for
vasopressor-dependent patients with relative adrenal insuffi-
ciency, antithrombotic therapy when warranted and not con-
traindicated, and prevention of the various complications of
critical illness [101]. The Surviving Sepsis Campaign recently
published an update to these recommendations [102] that ad-
vises institution of early, effective antibiotic therapy; evaluation
of the need for source control; early, goal-directed fluid resus-
citation with either crystalloid or colloid norepinephrine or
dopamine as needed to maintain a mean arterial blood pressure
�65 mm Hg; dobutamine for patients with myocardial de-
pression; packed RBCs to treat hemoglobin levels of !7.0 g/dL;
use of lung-protective ventilatory support strategies when
needed; weaning from ventilatory support by protocol and
spontaneous breathing trials; prevention of complications of
critical illness (insulin to maintain blood sugar levels at !150
mg/dL); deep vein thrombosis prophylaxis; stress ulcer pro-
phylaxis; and use of sedation protocols [102].
The use of early, effective antibiotic therapy and source con-
trol, when indicated, has been considered the cornerstone of
sepsis therapy. Conventional wisdom would suggest that ap-
propriate (effective) antibiotic therapy is essential for an im-
proved outcome. This hypothesis will never be clinically tested
because it would be considered unethical to deprive a patient
of timely or effective antibiotic treatment.
Most of our current evidence in support of early, effective
antibiotic therapy is based on retrospective outcome analysis
comparing early, effective antibiotic therapy with initially in-
effective antibiotic agents. Because the definition of sepsis has
varied over time and, in the older literature, often required the
presence of bacteremia and hypotension, it is difficult to make
comparisons with some of the current data [103]. However, it
is still apparent that, regardless of the definition, mortality rates
improve with timely use of effective, appropriate antibiotic
therapy. Other important aspects of antibiotic effectiveness re-
late to the timing of antibiotic therapy (early vs. delayed ad-
ministration). Studies that are amenable to prospective, ran-
domized clinical trials involve the use of single versus multiple
antibiotic agents and the effects on outcome parameters.
The adequacy of source control is also a difficult topic to
evaluate with the published literature [104]. Few studies have
commented on the adequacy of drainage or debridement. The
adequacy of source control is evaluated primarily by retro-
spective review of the clinical course or by a post hoc adju-
dication committee. As in investigations evaluating the effec-
tiveness of antibiotic therapy, ethical concerns preclude a study
of adequate versus inadequate source control. Therefore, to
answer both of these important questions, we must turn our
attention to an analysis of the limited available literature, with
emphasis on clinical trials that have evaluated or commented
on the adequacy of either antibiotic therapy or source control,
as it relates to outcome for patients with sepsis.
Methods
A PubMed search to identify studies related to appropriate
antibiotic use and source control in sepsis outcome was per-
formed on 14 September 2007. The search was limited to 1996
through September 2007, and all searches were restricted to the
English language, adult humans, and full-text articles. The text
words “adequate antibiotics” yielded 18,240 articles, “sepsis/
septic shock” yielded 14,423 articles, and “survival/mortality”
yielded 93,638 articles. When the search for “adequate anti-
biotics” was combined with that for “sepsis/septic shock,” the
result was 1209 articles. The combination of the search for
“adequate antibiotics” and the search for “survival/mortality”
yielded 7744 articles. When the search was limited to “adequate
antibiotics AND sepsis/septic shock AND survival/mortality,”
the result was 680 articles. A review of the titles and abstracts
of the 680 articles resulted in 16 articles that were relevant to
the statement. In addition, an evidence-based review from the
Surviving Sepsis Campaign on the topics of adequate antimi-
crobial therapy and adequate source control was examined
along with the references from these articles [100, 104].
Evidence
To evaluate evidence concerning appropriate antibiotic therapy
for severe sepsis and septic shock, we must first acknowledge
that no clinician would intentionally give a patient ineffective
antibiotic therapy. It is convention to classify appropriate or
effective antibiotic therapy on the basis of the culture and sus-
ceptibility results; however, not all patients with sepsis will have
positive culture results. Most large clinical trials report that
approximately one-third of patients have positive blood culture
results and approximately one-quarter of patients will have no
positive culture result of any type [105]. It is also disappointing
to find that several large epidemiologic studies and clinical trials
involving patients with sepsis do not give any data concerning
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S76 • CID 2008:47 (Suppl 2) • Kollef et al.
the administration of effective antibiotic therapy or the ade-
quacy of source control [106, 107]. Other important questions
(related to the use of culture and susceptibility results) surround
the ability of in vitro culture results to reflect in vivo effects of
antibiotics, as well as the debate about the thresholds differ-
entiating a true pathogen from a colonizing organism. A ret-
rospective review of 612 patients with bacteremia caused by
gram-negative bacteria demonstrated a significant reduction in
mortality when appropriate antibiotic therapy was administered
[108]. Fish [109] reviewed mortality differences between pa-
tients receiving appropriate antimicrobial therapy and patients
receiving inappropriate antimicrobial therapy in 11 studies and
demonstrated an association between a significant reduction in
mortality and appropriate antibiotic treatment.
Furthermore, in the Surviving Sepsis Campaign, the 11 so-
cieties used a modified Delphi method to define the role of
effective antimicrobial therapy in the management of severe sep-
sis and septic shock [100]. The consensus committee concluded
that prompt institution of effective antimicrobial therapy is one
of the most important predictors of outcome; unfortunately,
most of the evidence in support of their recommendations re-
flects category III, IV, or V evidence (table 3). Using the same
modified Delphi method to assess source control in the man-
agement of severe sepsis and septic shock, the same group con-
cluded that source control represents a key component for suc-
cessful sepsis management and should be used when indicated
[104]. Source control includes drainage of infected fluids, de-
bridement of infected soft tissues, and removal of infected devices
or foreign bodies. Source control should correct anatomic de-
rangements resulting in ongoing contamination and restore func-
tion [104].
In Spain, Garnacho-Montero et al. [110] conducted a pro-
spective cohort study of 406 critically ill patients with sepsis in
a tertiary care hospital, to determine the impact of effective,
empirical antibiotic therapy on early, 28-day, and 60-day mor-
tality. The administration of inadequate antibiotic therapy was
associated with an RR of 1.55 (95% CI, 1.20–2.02) for increased
mortality, compared with effective antibiotic therapy. An ob-
servational, prospective cohort study of 3413 patients with BSI
also demonstrated an increased mortality RR (1.6; 95% CI,
1.3–1.9) associated with the administration of inadequate an-
tibiotic therapy [111]. Ineffective antibiotic therapy was found
to increase all-cause mortality (52.1% vs. 23.5%; RR, 2.22; 95%
CI, 1.79–2.76; ) and infection-related mortality (42%P ! .001
vs. 17.7%; RR, 2.37; 95% CI, 1.83–3.08; ) in 2000 con-P ! .001
secutive ICU patients included in a prospective, observational,
cohort study [3]. In this study, the use of ineffective antibiotics
was greater in the setting of nosocomial infection with or with-
out prior antibiotic therapy. A prospective study of 707 patients
with bacteremia and/or fungemia evaluated the impact of ef-
fective versus ineffective antimicrobial therapy administered
initially, after results of cultures were obtained, and after the
susceptibility results were available; this study noted an increase
of up to 3.18 in the RR for death, when effective therapy was
compared with ineffective therapy at all time points [112].
The investigation of innovative therapies to improve the out-
come of severe sepsis and septic shock seems a perfect oppor-
tunity to evaluate the relationship between effective antibiotic
therapy and outcome. Unfortunately, this important variable
is often not assessed as part of a trial. Typically, the evaluation
of effective antibiotic and/or source control therapy involves
the use of a post hoc adjudication committee to evaluate the
culture and susceptibility results in relation to the antimicrobial
agents administered. A multicenter, prospective, randomized,
double-blind, controlled trial of high-dose intravenous im-
munoglobulin (IVIG), in addition to antibiotic therapy, given
to patients with sepsis undergoing surgery, found that overall
mortality increased from 20.4% with effective antibiotic therapy
to 87.5% with ineffective therapy [113].
In the PROWESS trial, drotrecogin alfa (activated) signifi-
cantly reduced mortality among patients with severe sepsis, but
148 patients (8.8%) in the intention-to-treat population (pa-
tients given drotrecogin alfa [activated], ; patients givenn p 74
placebo, ) received inadequate antibiotic therapy [114].n p 74
In a subsequent analysis, it was noted that the observed mor-
tality rates for patients given drotrecogin alfa (activated) and
patients given placebo who did not receive adequate antibiotic
therapy (29.7% and 43.2%, respectively) were higher the ob-
served mortality rates for those who received adequate anti-
infective therapy (24.2% and 29.6%, respectively) [115]. The
provision of adequate antimicrobial treatment, when evaluated,
has been quite variable, with reported values ranging from 75%
[116] to 88% [117].
The timing of antibiotic administration has also been found
to be an extremely important factor in outcome. A retrospective
cohort study of 2731 patients with hypotension and sepsis
found that mortality increased 7.6% for each 1-hour delay in
antibiotic administration after the onset of hypotension [4].
When antibiotics were administered within 30 min after the
onset of hypotension, the survival rate was 82.7%, but it fell
to 42% when the antibiotics were delayed 6 h after the onset
of hypotension. To improve the timely administration of an-
tibiotics and other diagnostic and therapeutic aspects of sepsis
management, clinicians have incorporated recommended ther-
apies into bundles of care [118]. Nguyen et al. [118] conducted
a 2-year, prospective, observational cohort study of 330 patients
who presented to the emergency department with severe sepsis
or septic shock, and they found a significant reduction (from
20.8% to 39.5%; ) in mortality when bundles were usedP ! .01
and, specifically, when antibiotics were administered within 4
h after presentation (OR, 0.38; 95% CI, 0.18–0.80; ).P p .03
Adequacy of source control is evaluated even less frequently
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S77
than is antimicrobial therapy. Among patients requiring surgery
for source control in a multicenter, prospective, randomized,
double-blind, placebo-controlled trial of platelet-activating fac-
tor acetylhydrolase for treatment of severe sepsis and septic
shock, adequate source control occurred in 190% of both treat-
ment groups [117]. In contrast, in the PROWESS trial of dro-
trecogin alfa (activated) for severe sepsis, the initial source-
control procedure was judged to be adequate in only 90 (50.8%)
of 177 patients receiving drotrecogin alfa (activated) and 86
(47.3%) of 182 patients receiving placebo. Initial source control
was inadequate for 38 (21.5%) of 177 patients receiving dro-
trecogin alfa (activated) and 51 (28.0%) of 182 patients re-
ceiving placebo and was indeterminate for 49 (27.7%) and 45
(24.7%), respectively. In patients with adequate or inadequate
source control, no reduction in mortality was noted for dro-
trecogin alfa (activated). In patients with indeterminate source
control, drotecogin alfa (activated) was associated with a re-
duction in mortality (37.0% vs. 56.6%; OR, 0.65; 95% CI, 0.43–
1.00; absolute risk reduction, 19.6%) [119].
Grading of Evidence
On the basis of a review of the 12 studies cited above, 67% of
the workshop members agreed that the nature of the evidence
available to support this statement was category II, whereas
17% voted category III, and 17% voted category V (table 3).
Level of Support
When voting on the support for this statement, 9% of the
summit participants voted to accept the statement completely,
82% voted to accept the statement with some reservations, 9%
voted to accept the statement with major reservations, and 0%
voted to reject the statement. In comparison, of the 744 IDSA
members who participated in the online survey, 50% voted to
accept the statement completely, 35% voted to accept the state-
ment with some reservations, 10% voted to accept the state-
ment with major reservations, 5% voted to reject the statement
with reservations, and 0% voted to reject the statement com-
pletely (figure 5).
Discussion
Consideration of the statement concerning the importance of
effective antibiotics and source control in outcomes for patients
with severe sepsis and septic shock caused the vast majority
(180%) of the summit participants to support the statement
either completely or with some reservations. This conclusion
was reached by the participants despite the lack of multicenter,
prospective, randomized, placebo-controlled, double-blind
clinical trials substantiating the importance of effective anti-
biotic therapy in outcomes for patients with severe sepsis and
septic shock. Despite this lack of evidence, most clinicians be-
lieve that administration of early, effective antimicrobial therapy
and source control, when indicated, are among the key com-
ponents of management of severe sepsis and septic shock. Other
key components of effective sepsis management include fluid
resuscitation, restoration and maintenance of hemodynamic
function, support of oxygenation and ventilation as necessary,
and prevention of the complications of critical illness [97, 98,
101, 102]. Ethical considerations and common sense prohibit
conducting clinical trials to establish the key role for effective
antibiotics and source control in the management of severe
sepsis. It is also impossible to establish the relative value of one
key component compared with another. The various compo-
nents of effective sepsis management may be viewed as links
in a chain, and the chain is only as strong as its weakest link.
Therefore, without provision of all necessary aspects of sepsis
management, the outcome will be less than optimal.
Unfortunately, technology has not progressed to the point
where the clinician can rapidly diagnose the microbial cause
of the infection leading to sepsis or determine the susceptibility
of the organism at an early point in time and thus enable
provision of effective antibiotics at the time of diagnosis. Even
the diagnosis of sepsis is often not confirmed until the results
of cultures are available for review. This process typically takes
hours to days, and, to date, is not available during the “golden
hour” of initial management when the best outcome can be
expected [4]. The use of markers for sepsis (e.g., procalcitonin
levels, soluble triggering receptors expressed on myeloid cells,
and peptide nucleic acid fluorescence in situ hybridization) and
other techniques for early diagnosis may improve the diagnosis
of sepsis, but we still lack an early indicator of organism sus-
ceptibility to various antibiotics [120–122]. For now, clinicians
have directed their attention to the implementation of sepsis
bundles, to ensure the early administration of effective sepsis
therapy, including antibiotics, to achieve the best possible out-
comes for patients [118].
Future Directions
Although not necessarily the major determinant of outcome in
severe sepsis and septic shock, early, effective antibiotic therapy
and source control, when indicated, are among the key com-
ponents necessary for optimal outcome. Future efforts will
likely focus on uses of advanced diagnostic techniques to iden-
tify specific bacterial and fungal pathogens, such as fluorescence
in situ hybridization and PCR. These tests will help facilitate
early diagnosis of sepsis and will direct more-appropriate early
therapy. In addition, the efficacy of antibiotic treatment should
be more definitively investigated in terms of the MIC of the
microbe and the blood level and, potentially, the mechanism
of action of the antibiotic. Relying only on the categories “sus-
ceptible” or “resistant” may not adequately define “appropri-
ate” antibiotic treatment. This has particular relevance to an-
tibiotics such as vancomycin and aminoglycosides. This strategy
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S78 • CID 2008:47 (Suppl 2) • Kollef et al.
Figure 5. Voting comparison for statement 5 (“Initial appropriate antimicrobial therapy and source control are the most important determinants ofoutcome in severe sepsis and septic shock”). “IDSA” refers to the members of the Infectious Diseases Society of America who responded to a Web-based survey; “Summit” refers to the Health Care–Associated Infection Summit panel.
not only will result in better sepsis outcome but also will assist
with antibiotic stewardship and potentially minimize the de-
velopment of bacterial resistance.
STATEMENT 6: VANCOMYCIN IS OBSOLETEFOR TREATING MRSA INFECTIONS
Rationale and Definition of Statement
Vancomycin has been the workhorse antimicrobial for the treat-
ment of MRSA infections for 140 years. In the past decade,
the prevalence of hospital-associated MRSA infections has
reached 64% in most US hospitals [123]. In addition, there has
been a virtual explosion of community-onset MRSA infections
among young, healthy individuals in a wide variety of situa-
tions, including high school, college, and professional football
teams; prisons; and so forth. Although vancomycin was pre-
scribed sporadically and infrequently 20–30 years ago, its use
has increased exponentially over the past decade. As a conse-
quence, there is increasing evidence that vancomycin is not
currently as effective as it once was; this evidence results from
frank treatment failures as well as growing concern related to
the emergence of various types of vancomycin resistance. The
current epidemics of hospital-associated MRSA and commu-
nity-onset MRSA infections have developed rapidly, and there
are no concrete guidelines addressing the current problems
associated with treatment of MRSA infections. The purpose of
the current investigation is to examine the mounting evidence
regarding treatment failures and reduced in vitro activity of
vancomycin against MRSA.
Methods
A PubMed database search to identify studies related to van-
comycin was concluded on 26 September 2007. The search term
“vancomycin” yielded 13,064 articles. “Vancomycin” limited to
the English language resulted in 11,528 articles and, when com-
bined with “last ten years,” yielded 4181 articles. When these
elements were combined with “human,” 3166 articles were
found. Further narrowing of the field was accomplished by
combining the elements “failure” (162 articles), “Staphylococcus
aureus” (74 articles), and “MRSA” (30 articles). Excluding case
reports yielded 10 articles. Finally, 3 abstracts on in vitro sus-
ceptibility were added from abstracts from the annual meetings
of the IDSA and the Interscience Conference on Antimicrobial
Agents and Chemotherapy.
Evidence
Changes in the susceptibility of MRSA to vancomycin.
There have been 3 studies performed in the United States that
evaluated the in vitro susceptibility of MRSA strains to van-
comycin over time, with the objective of identifying trends in
the susceptibility of MRSA to vancomycin. In the first study,
the MIC90 values for vancomycin among MRSA strains were
compared in vitro at M. D. Anderson Hospital across a 20-
year period; 25 strains from 1985 and 28 strains from 2004
were examined. This study demonstrated that the MIC90 in-
creased from 0.2 mg/mL to 2.0 mg/mL during this nearly 20-
year time span [124]. The second study compared the in vitro
susceptibility of blood isolates of MRSA in 2002 with that of
blood isolates of MRSA in 2005 at the New England Medical
Center (Boston, MA) and demonstrated a dramatic increase in
the MICs for vancomycin (figure 6) [125]. The third study was
an in vitro investigation of MICs for vancomycin among 945
strains of S. aureus from 2000 and 1418 strains of S. aureus
from 2004. In 2000, 79.9% of strains had vancomycin MICs
of �0.5 mg/mL, and 19.9% ( ) had vancomycin MICs ofP ! .01
1.0 mg/mL. In contrast, in 2004, 28.8% had vancomycin MICs
of �0.5 mg/mL, whereas 70.4% ( ) had vancomycin MICsP ! .01
of 1.0 mg/mL [126]. According to this study, a marked increase
in vancomycin MICs was apparent for MRSA isolates in Los
Angeles from 2000 through 2004.
Clinical failure of vancomycin in patients with bacteremia
caused by MRSA strains with MICs of 4 mg/mL. An obser-
vational series of 14 case reports of clinical failures of vanco-
mycin for treatment of bacteremia caused by MRSA strains
with MICs of vancomycin 4 mg/mL were compiled [127]. These
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S79
Figure 6. In vitro comparison of vancomycin MICs at the New EnglandMedical Center (Boston, MA), in 2002 and 2005. Adapted from [125].
Figure 7. Clinical failures of vancomycin treatment for vancomycin-susceptible Staphylococcus aureus: the role of MICs. Data are from [134].
failures were the primary evidence compelling the Clinical and
Laboratory Standards Institute to lower the vancomycin-sus-
ceptible MRSA MIC breakpoint to 2 mg/mL.
Vancomycin-resistant MRSA. Absolute resistance of
MRSA strains has been described [128]. These strains are called
“vancomycin-resistant MRSA” and have been defined as strains
with MIC of 116 mg/mL for vancomycin. Thus far, 7 vanco-
mycin-resistant MRSA strains have been described in Japan and
the United States [129].
Vancomycin-intermediate MRSA (VISA) and heteroresis-
tant VISA (hVISA). The first descriptions of emergence of
vancomycin-intermediate strains of MRSA [130] or glycopep-
tide-intermediate S. aureus [131] were from Japan, and these
are defined as having MICs of 4–8 mg/mL [130]. Soon there-
after, clinical failures of vancomycin for patients with MRSA
bacteremia caused by vancomycin-intermediate strains were re-
ported. In a retrospective study in Australia, 76% of 25 patients
with MRSA bacteremia who were given treatment with van-
comycin experienced failed therapy, as defined as persistence
of bacteremia for 17 days. Interestingly, these MRSA strains
were relatively susceptible to vancomycin, with MICs of 2–4
mg/mL [132]. Although these strains were defined as being VISA
strains, they contained populations of microbes that were re-
sistant to vancomycin. Because of the heterogenous population
of MRSA, these strains are called “hVISA.” In the laboratory,
demonstration of heteroresistance requires a large inoculum of
107 MRSA organims per mL because ∼1 in 100,000 bacteria is,
in fact, resistant to vancomycin. It likely has clinical relevance
for cases in which the “load” of MRSA is high, as one might
expect in a large abscess, necrotizing fasciitis, consolidative
pneumonia, bacteremia, and endocarditis. Because most clinical
laboratories are standardized to use inocula of 105 MRSA or-
ganisms for susceptibility testing, newer methods must be de-
veloped to alert clinicians of this phenomenon.
Failure of vancomycin in bacteremia caused by hVISA.
A retrospective study of isolates from all patients with MRSA
bacteremia ( ) in a hospital in Australia evaluated a 12-n p 53
month period (July 2001–June 2002), with the objective of
identifying the prevalence of hVISA and the outcomes for these
patients given treatment with vancomycin [133]. No VISA iso-
lates were recovered; however, 5 (9.4%) of 53 MRSA isolates
were heteroresistant to vancomycin. Patients infected with
hVISA were more likely to have high bacterial loads (P p
), compared with patients infected with vancomycin-sus-.001
ceptible MRSA, and patients with hVISA infections were more
likely to experience a failure of vancomycin treatment (P !
), compared with patients infected with vancomycin-sus-.001
ceptible MRSA [133].
Failure rate of vancomycin treatment as a function of rising
MICs in patients with infection caused by vancomycin-sus-
ceptible MRSA. A total of 122 S. aureus isolates, 63 of which
were MRSA with vancomycin MICs of 0.5–2.0 mg/mL, from
87 patients given treatment with vancomycin were analyzed.
Of the 87 patients, 45 had no clinical or bacteriological response
to vancomycin. Among the 36 clinically evaluable patients in-
fected with S. aureus strains that had the accessory gene
regulator (agr) group II polymorphism, 31 had an infection
that failed to respond to vancomycin, whereas only 5 had an
infection that responded successfully to vancomycin. There was
a significant association between vancomycin treatment failure
(45 of 63) and MIC increase ( ) (figure 7) [134].P p .004
Failure of vancomycin as a function of the rapidity of bac-
terial killing. This investigation analyzed isolates ( )n p 30
from patients with bacteremia in 24 US hospitals, with the ob-
jective of correlating clinical failure with in vitro vancomycin
susceptibility and bactericidal activity. For MRSA isolates with
vancomycin MICs �0.5 mg/mL, vancomycin was 55.6% suc-
cessful in the treatment of bacteremia, whereas vancomycin was
only 9.5% ( ) effective in cases in which MRSA MICs forP p .02
vancomycin were 1–2 mg/mL. In addition, the failure rate for
vancomycin was 100% if !4.71 log of bacteria were killed in 72
h ( ); 77% if 4.71–6.26 log of bacteria were killed in 72 hn p 9
( ); and 50% if 16.27 log of bacteria were killed in a 24-n p 13
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S80 • CID 2008:47 (Suppl 2) • Kollef et al.
h period ( ). The differences between treatment groups weren p 8
statistically significant ( ) [135].P p .05
Vancomycin tolerance among MRSA isolates. Another
cause of failure of antimicrobial treatment is the phenomenon
of bacterial tolerance, which is defined as a minimum bacte-
ricidal concentration (MBC)/MIC ratio of �32 or an MBC of
�16. Of 207 evaluated strains of S. aureus, 102 were MRSA;
14.7% of wild-type MRSA demonstrated tolerance, whereas
69.3% of hVISA and 100% of VISA isolates demonstrated tol-
erance. Thus, even large doses of vancomycin may not reach
bactericidal blood and tissue levels sufficient to kill tolerant
strains of MRSA [136].
Does increasing the dose of vancomycin to achieve serum
trough levels of 115 mg/mL increase efficacy, or does it increase
nephrotoxicity? The rationale for this study was a perceived
increase in vancomycin treatment failures for infections caused
by vancomycin-susceptible MRSA strains with high MICs and
the general practice to recommend a higher vancomycin target
trough level of 15–20 mg/mL, in an effort to increase efficacy.
However, there are no data regarding potentially increased renal
toxicity associated with these higher doses.
In a prospective cohort study of patients with MRSA infec-
tions ( ), investigators sought to correlate the distribu-n p 95
tion of vancomycin MICs and treatment outcomes with trough
levels at least 4 times the MIC. There was no nephrotoxicity
when trough levels were !15 mg/mL. However, 11 (12%) of 63
patients developed nephrotoxicity with trough levels �15 mg/
mL. Multivariate analysis implicated concomitant nephrotox-
ins, such as aminoglycosides and amphotericin B. In the high-
trough-level group, only 2% (in the absence of nephrotoxins)
developed nephrotoxicity [137]. Of the 95 patients in the study,
51 (54%) were infected with high-MIC strains and had pneu-
monia (77%) and/or bacteremia. An initial response rate of
74% was achieved when the target trough level was attained,
irrespective of MIC. However, despite achieving the target
trough level, the group infected with high-MIC strains had
fewer end-of-treatment responses (24 [62%] of 39 vs. 34 [85%]
of 40; ) and higher infection-related mortality (11P p .02
[24%] of 51 vs. 4 [10%] of 44; ), compared with theP p .16
group infected with low-MIC strains. Infection with a high-
MIC strain ( ) and high APACHE II score ( )P p .03 P p .009
were independent predictors of poor response in multivariate
analysis. Nephrotoxicity occurred only in the high-trough-level
group (11 [12%] of 63); this was significantly predicted by
concomitant therapy with other nephrotoxic agents.
A high prevalence of clinical MRSA strains with elevated
vancomycin MICs (2 mg/mL) requires aggressive empirical van-
comycin dosing to achieve a trough level of 115 mg/mL. The
rationale for this recommendation is obvious, yet there is little
clinical experience with high vancomycin dosages, and toxicity
becomes an important issue, as discussed below. Combination
or alternative therapy should be considered for invasive infec-
tions caused by these strains.
Will higher trough levels of vancomycin be associated with
a higher incidence of renal toxicity? In a prospective review
of patients with HAP, 43 patients were followed up for changes
in creatinine clearance ( ). Overall, there was a 25% de-n p 43
crease in creatinine clearance among all patients receiving van-
comycin. There was a 30% decrease in creatinine clearance
among patients with a low trough level (5–15 mg/mL), com-
pared with a 60% decrease in creatinine clearance among pa-
tients with high trough levels of 115 mg/mL ( ) [65].P p .006
Grading of Evidence
Of the workshop participants, 83% voted that the evidence to
support the statement was category III, and 17% voted that it
was category II (table 3).
Level of Support
Interestingly, 36% of the summit participants voted to accept
the statement with some reservations, 36% voted to accept the
statement with major reservations, 18% voted to reject the
statement with reservations, and 9% voted to reject the state-
ment completely. In comparison, of the 744 IDSA members
who participated in the online survey, 1% accepted the state-
ment completely, 9% accepted the statement with some res-
ervations, 7% accepted the statement with major reservations,
38% rejected the statement with reservations, and 45% rejected
the statement completely (figure 8).
Discussion
This statement is of key importance, given the emerging data
regarding reduced susceptibility of MRSA to vancomycin and
the increasing reports of failure of vancomycin in the treatment
of clinical infections. Recognition of this problem is not yet
widespread, as evidenced by the IDSA membership’s diverse
responses to this statement that vancomycin is obsolete in the
treatment of MRSA infections. Summit participants’ responses
were diverse yet more accepting of the statement.
The quality of the evidence supporting emerging resistance
to vancomycin and so-called MIC creep is not robust, largely
because it reflects regional differences and is not yet on a na-
tional scale. Still, these small studies are compelling because
the studies were done in several different geographical regions
by independent investigators. There may be some bias, since
many of the sites are large hospitals in densely populated
regions of the United States where vancomycin use may be
greater. In addition, some studies are retrospective and start
with patients who experienced failure of vancomycin treatment.
Not surprisingly, some of the isolates from these cases have
reduced susceptibility to vancomycin. Still, all studies presented
here support the contention that strains of MRSA are emerging
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S81
over time with reduced susceptibility to vancomycin and that
this phenomenon is associated with or causes treatment failures.
Thus, although the quality and size of these studies are not
robust, it is clear that vancomycin susceptibility among MRSA
isolates is changing rapidly, and these preliminary studies are
providing early warning of larger problems to come. It is also
true that very large doses of vancomycin may be necessary to
achieve an area under the concentration-time curve/MIC ratio
for MRSA infections caused by strains with vancomycin MICs
of 1–2 mg/mL [138].
Future Directions
Future directions discussed by the summit members clearly
involve additional studies. Prospective studies that evaluate the
in vitro susceptibility of MRSA strains to vancomycin on re-
gional and national scales are sorely needed. New assays to
detect heteroresistance among clinical isolates of MRSA need
to be developed and correlated with clinical outcomes. Finally,
prospective studies that evaluate clinical responses of MRSA
infections, in terms of susceptibility issues and vancomycin
trough levels, should be done immediately. Until then, if van-
comycin is to be used, these data mandate increased knowledge
of the MICs and vancomycin trough levels, to ensure that pa-
tients are given appropriate treatment. Specifically, clinical lab-
oratories need to provide clinicians with the actual vancomycin
MIC of the MRSA strain, because clinical failure increases pro-
portionally to the MIC, even among “susceptible” strains.
STATEMENT 7: SERIOUS HAIs DUE TOSUSPECTED GRAM-NEGATIVE BACTERIASHOULD BE TREATED EMPIRICALLY WITHDUAL COVERAGE THAT INCLUDES ANAMINOGLYCOSIDE
Rationale and Definition of Statement
The terminology of HAIs is rapidly permeating the classification
of various infection types. Classification schemes for both BSIs
and pneumonia have already been adopted. These classifica-
tions identify specific patients at risk, as well as treatment rec-
ommendations. “HAIs” can describe a wide variety of infection
types; therefore, it is important to focus recommendations on
the basis of patient-specific circumstances. The evaluation of
this statement was insupportable in its entirety; therefore, the
review of the literature centered on the use of dual empirical
coverage as well as the use of an aminoglycoside in combination
therapy. The use of dual empirical coverage is well supported
in the literature; however, the selection of an aminoglycoside
is problematic because it is not necessarily appropriate in all
clinical situations. There are 5 inherent issues that will be ad-
dressed in the evaluation of this statement: the role of adequate
empirical therapy for serious HAI in the determination of out-
come [139], the potential value of combination antimicrobial
therapy in the determination of outcome [140], the potential
efficacy of aminoglycosides as a component of combination
antimicrobial therapy for serious HAI [3], the potential efficacy
of quinolones as a component of combination therapy for se-
rious HAI [141], and the influence of antibiotic-resistance sur-
veillance on selection of therapeutic agents [46]. Each of these
issues will be discussed with respect to evidence in favor of or
against acceptance of the statement.
Methods
A PubMed literature search was conducted on 4 September
2007 to identify studies related to dual empirical coverage of
infections with gram-negative pathogens. The search term
“cross infection/drug therapy or cross infection therapy” was
combined using the “AND” function with “antibiotic therapy
and gram-negative.” Results were limited to the English lan-
guage and studies published within the past 5 years. The search
yielded 204 articles, 2 of which were relevant to the statement.
A second PubMed search was conducted using the search terms
“gram-negative bacterial infections/drug therapy” and “cross
infection,” combined using the “AND” function. This search
yielded 200 articles, 10 of which were relevant to the statement.
Twelve additional articles were also reviewed from previous
searches.
Evidence
The role of adequate empirical therapy for serious HAI in the
determination of outcome. The outcome of serious HAI is
improved by selection of adequate empirical antibiotic therapy,
as defined by susceptibility of the infecting organism(s) to the
agent(s) selected. Several retrospective and prospective clinical
studies since the mid-1990s have provided statistical evidence
of the positive effect of adequate empirical antibiotic therapy
on clinical outcome. These studies have also concluded that
adjustment of therapy when susceptibility data become avail-
able does not reverse the unfavorable effect of inadequate em-
pirical therapy.
In 1997, Luna et al. [139] described a prospective cohort
study of 132 patients with VAP to determine the impact on
outcome of a change in antibiotic therapy based on the results
of culture of specimens collected by early bronchoalveolar lav-
age (BAL). Among patients from whom a pathogen was re-
covered by BAL, mortality was 91% after inadequate initial
therapy and 38% after adequate initial therapy ( ). WhenP ! .001
therapy was changed according to BAL culture results, mortality
was comparable to that among patients who continued to re-
ceive inadequate therapy. Kollef and Ward [140] reported the
results of a similar study in 1998 to determine the influence
of mini-BAL cultures on subsequent changes in antibiotic ther-
apy and outcomes in 130 patients with suspected VAP. Mortality
among patients for whom therapy was either begun or changed
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S82 • CID 2008:47 (Suppl 2) • Kollef et al.
Figure 8. Voting comparison for statement 6 (“Vancomycin is obsolete for treating MRSA infections”). “IDSA” refers to the members of the InfectiousDiseases Society of America who responded to a Web-based survey; “Summit” refers to the Health Care–Associated Infection Summit panel. MRSA,methicillin-resistant Staphylococcus aureus.
at the time of BAL culture results was 60.8%, compared with
33.3% among patients requiring no change in initial antibiotic
therapy ( ). Thus, a delay in initiation of adequate ther-P ! .001
apy was associated with greater mortality.
A prospective cohort study by Kollef et al. [3] was subse-
quently reported in 1999; the report described 655 critically ill
infected patients admitted to the ICU. The overall mortality
was 15.6%. Mortality among patients receiving inadequate ini-
tial antimicrobial treatment was 52.1%, compared with 12.2%
among patients who received adequate initial treatment (P !
). The effects of inappropriate initial antimicrobial therapy.001
on outcomes for 286 patients with bacteremia due to antibiotic-
resistant organisms were reported by Kang et al. in 2005 [141].
In a study of patients with a high-risk source of bacteremia,
inappropriate initial antibiotic therapy was independently as-
sociated with increased mortality (mortality among those given
appropriate therapy, 27.4%; mortality among those given in-
appropriate therapy, 38.4%; ) (OR, 3.64; 95% CI,P p .049
1.13–11.72; ). Fraser et al. [46] reported similar resultsP p .030
in a study published in 2006 involving 920 patients with mi-
crobiologically documented infections. Thirty-day all-cause
mortality was 20.1% among those who received inappropriate
initial empirical antibiotic therapy and was 11.8% among those
who received appropriate therapy ( ). In a study ofP p .001
patients with bacteremia published in 2007 by Tumbarello et
al. [84], 186 patients infected with ESBL-producing organisms
had 21-day mortality of 59% after inadequate initial antimi-
crobial therapy, compared with 18.5% among those who re-
ceived adequate initial therapy ( ).P ! .001
The potential value of combination antimicrobial therapy
in the determination of outcome. The potential benefit of
combination antibiotic therapy, compared with effective single-
drug therapy, remains ill defined. However, in a retrospective
study of 115 patients with P. aeruginosa bacteremia, Chamot
et al. [142] found that adequate empirical combination therapy
yielded lower 30-day mortality than did adequate empirical
monotherapy, inadequate empirical monotherapy, or inade-
quate empirical combination therapy. In addition, adequate
definitive combination therapy given when susceptibility results
became available did not improve survival, compared with ad-
equate definitive monotherapy. These results support the ben-
efit of adequate empirical monotherapy or combination ther-
apy, compared with delayed definitive therapy for bacteremia
due to P. aeruginosa. Adequate combination empirical therapy
was also more effective than adequate empirical monotherapy.
Neutropenic patients accounted for 30% (34 of 115 patients)
of the study population.
A prospective, observational study of 230 patients with Kleb-
siella bacteremia showed no difference (20% vs. 18%; )P 1 .05
in 14-day mortality between those given monotherapy and
those given combination therapy (b-lactam plus aminoglyco-
side) [143]. However, for the subgroup of patients who ex-
perienced hypotension (systolic blood pressure, �90 mm Hg)
within 72 h before or on the day of the positive blood culture,
those who received combination therapy experienced signifi-
cantly lower mortality (24%) than did those who received
monotherapy (50%).
A meta-analysis published in 2004 reviewed 17 studies that
compared combination therapy and monotherapy for bacter-
emia caused by gram-negative organisms [144]. The authors
found no mortality benefit with combination therapy. However,
analysis of only P. aeruginosa bacteremia showed a significant
mortality benefit (OR, 0.50; 95% CI, 0.30–0.79).
In the above-mentioned studies, most of the effective com-
bination therapies used b-lactam and aminoglycoside agents to
which common isolates were susceptible. In the more recent
era of MDR gram-negative bacilli, use of novel empirical an-
tibiotic combinations may be dictated by advanced local resis-
tance patterns. In certain areas of New York City and Morocco,
effective empirical combination therapy requires use of a poly-
myxin alone or in combination with other agents, according
to special in vitro susceptibility tests [145–147].
The potential efficacy of aminoglycosides as a component
of combination antimicrobial therapy for serious HAIs.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S83
The potential efficacy of aminoglycosides as a component of
combination antibacterial therapy is illustrated by the studies
described above. Guidelines for the management of HAP, VAP,
and HCAP in adults were published jointly by the ATS and the
IDSA in 2005 [1]. Suggested antibiotic combinations included
either an aminoglycoside or quinolone, chosen on the basis of
local susceptibility data. Early evidence that aminoglycoside
therapy for serious pneumonia caused by gram-negative path-
ogens is relatively ineffective because of poor tissue penetration
is contradicted by more-recent pharmacokinetic/pharmaco-
dynamic studies indicating that optimal aminoglycoside ther-
apy is achieved by once-daily administration, not divided daily
doses [148].
The potential efficacy of quinolones as a component of com-
bination therapy for serious HAIs. The potential efficacy of
quinolones as a component of adequate empirical combination
therapy depends on the intensity of local use and likely the
degree of resistance among invading gram-negative pathogens.
A surveillance study published by Neuhauser et al. [149] ex-
amined fluoroquinolone resistance in 1994–2000. They found
that overall susceptibility to ciprofloxacin decreased from 86%
in 1994 to 76% in 2000 and was significantly associated with
increased use of fluoroquinolones. Other studies published dur-
ing the past decade have documented the rising use of fluo-
roquinolones in various areas of the United States and its as-
sociation with increasing resistance among gram-negative
bacilli [149–151].
The influence of antibiotic resistance surveillance on selec-
tion of therapeutic agents. Increasing antibiotic resistance
among gram-negative bacilli in the United States and inter-
nationally has been well documented in the past few decades.
Its local incidence should influence the selection of empirical
therapy for serious infections with gram-negative bacilli. Na-
tional surveillance studies in the United States have indicated
a greater degree of quinolone resistance than aminoglycoside
resistance among P. aeruginosa and Acinetobacter isolates, par-
ticularly from ICUs [152–154]. Routine colonization surveil-
lance in an ICU has demonstrated that knowledge of coloni-
zation status before infection is associated with higher rates of
appropriate therapy for patients with bacteremia caused by an-
tibiotic-resistant gram-negative bacilli [155]. A retrospective co-
hort study notes the clinical implications of resistance and the
value of accurate susceptibility information. In that study, Tam
et al. [156] examined 34 bacteremia episodes involving P. aeru-
ginosa isolates with reduced susceptibility to piperacillin-ta-
zobactam, which was given empirically for 7 episodes. Thirty-
day mortality was found to be 85.7% in the group receiving
piperacillin-tazobactam, compared with 22.2% in the group
receiving other antipseudomonal agents ( ). Tam et al.P p .004
[156] observed an increase in mortality among patients infected
with an isolate that had increased resistance, despite the fact
that these patients had received appropriate therapy. Currently,
there is no real clinical data supporting a synergistic effect of
dual coverage for P. aeruginosa or any other gram-negative
bacilli. The same is true for resistance. The main rationale for
dual coverage of gram-negative bacilli is to increase the like-
lihood of the administration of appropriate therapy. On another
note, in 2007, Livermore and Pearson [157] analyzed the utility
of international, national, and local resistance surveys. They
concisely summarized the essence of their findings in the title
“Antibiotic resistance: location, location, location,” emphasiz-
ing that “for patient management, good local data are essential”
[157, p. 7]. They highlighted the complexity of issues and large
variances in resistance rates according to country, patient char-
acteristics, and unit of care (i.e., nursing home vs. ICU). The
authors concluded that, although these surveys help to illustrate
trends, local susceptibility data are essential to good clinical
management.
Grading of Evidence
On the basis of a review of the studies cited above, 33% of the
workshop members voted that the evidence to support the
statement was category II, 50% voted that it was category III,
and 17% voted that it was category V (table 3).
Level of Support
Overall, 27% of the workshop members voted to accept the
statement with some reservations, 64% voted to accept the
statement with major reservations, and 9% voted to reject the
statement with reservations. None of the summit members
voted to accept or reject the statement completely. In com-
parison, of the 744 IDSA members who participated in the
online survey, 30% voted to accept the statement completely,
38% voted to accept the statement with some reservations, 11%
voted to accept the statement with major reservations, 18%
voted to reject the statement with reservations, and 3% voted
to reject the statement completely (figure 9).
Discussion and Future Directions
In conclusion, this statement can be supported by evidence that
microbiologically adequate empirical treatment of serious HAIs
due to gram-negative bacteria provides optimal clinical out-
come. Evidence also supports the use of dual therapy to provide
broad empirical coverage, as well as improved mortality for
patients with bacteremia caused by P. aeruginosa. National sur-
veillance data from the United States provide evidence that
aminoglycosides retain greater susceptibility than do quino-
lones as potential second agents in combination therapy. How-
ever, in selected and expanding geographic areas, antimicrobial
resistance has progressed to include all aminoglycosides and
quinolones, as well as all b-lactams. This phenomenon pre-
cludes the use of a definitive general statement that includes a
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from
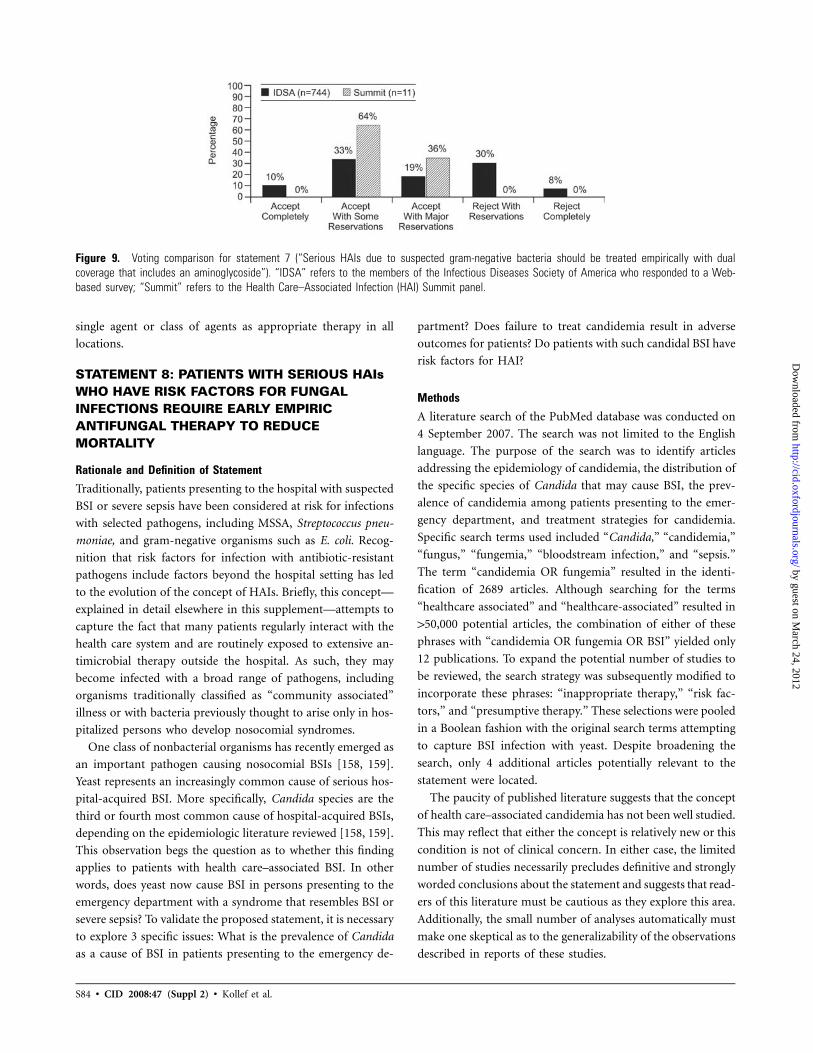
S84 • CID 2008:47 (Suppl 2) • Kollef et al.
Figure 9. Voting comparison for statement 7 (“Serious HAIs due to suspected gram-negative bacteria should be treated empirically with dualcoverage that includes an aminoglycoside”). “IDSA” refers to the members of the Infectious Diseases Society of America who responded to a Web-based survey; “Summit” refers to the Health Care–Associated Infection (HAI) Summit panel.
single agent or class of agents as appropriate therapy in all
locations.
STATEMENT 8: PATIENTS WITH SERIOUS HAIsWHO HAVE RISK FACTORS FOR FUNGALINFECTIONS REQUIRE EARLY EMPIRICANTIFUNGAL THERAPY TO REDUCEMORTALITY
Rationale and Definition of Statement
Traditionally, patients presenting to the hospital with suspected
BSI or severe sepsis have been considered at risk for infections
with selected pathogens, including MSSA, Streptococcus pneu-
moniae, and gram-negative organisms such as E. coli. Recog-
nition that risk factors for infection with antibiotic-resistant
pathogens include factors beyond the hospital setting has led
to the evolution of the concept of HAIs. Briefly, this concept—
explained in detail elsewhere in this supplement—attempts to
capture the fact that many patients regularly interact with the
health care system and are routinely exposed to extensive an-
timicrobial therapy outside the hospital. As such, they may
become infected with a broad range of pathogens, including
organisms traditionally classified as “community associated”
illness or with bacteria previously thought to arise only in hos-
pitalized persons who develop nosocomial syndromes.
One class of nonbacterial organisms has recently emerged as
an important pathogen causing nosocomial BSIs [158, 159].
Yeast represents an increasingly common cause of serious hos-
pital-acquired BSI. More specifically, Candida species are the
third or fourth most common cause of hospital-acquired BSIs,
depending on the epidemiologic literature reviewed [158, 159].
This observation begs the question as to whether this finding
applies to patients with health care–associated BSI. In other
words, does yeast now cause BSI in persons presenting to the
emergency department with a syndrome that resembles BSI or
severe sepsis? To validate the proposed statement, it is necessary
to explore 3 specific issues: What is the prevalence of Candida
as a cause of BSI in patients presenting to the emergency de-
partment? Does failure to treat candidemia result in adverse
outcomes for patients? Do patients with such candidal BSI have
risk factors for HAI?
Methods
A literature search of the PubMed database was conducted on
4 September 2007. The search was not limited to the English
language. The purpose of the search was to identify articles
addressing the epidemiology of candidemia, the distribution of
the specific species of Candida that may cause BSI, the prev-
alence of candidemia among patients presenting to the emer-
gency department, and treatment strategies for candidemia.
Specific search terms used included “Candida,” “candidemia,”
“fungus,” “fungemia,” “bloodstream infection,” and “sepsis.”
The term “candidemia OR fungemia” resulted in the identi-
fication of 2689 articles. Although searching for the terms
“healthcare associated” and “healthcare-associated” resulted in
150,000 potential articles, the combination of either of these
phrases with “candidemia OR fungemia OR BSI” yielded only
12 publications. To expand the potential number of studies to
be reviewed, the search strategy was subsequently modified to
incorporate these phrases: “inappropriate therapy,” “risk fac-
tors,” and “presumptive therapy.” These selections were pooled
in a Boolean fashion with the original search terms attempting
to capture BSI infection with yeast. Despite broadening the
search, only 4 additional articles potentially relevant to the
statement were located.
The paucity of published literature suggests that the concept
of health care–associated candidemia has not been well studied.
This may reflect that either the concept is relatively new or this
condition is not of clinical concern. In either case, the limited
number of studies necessarily precludes definitive and strongly
worded conclusions about the statement and suggests that read-
ers of this literature must be cautious as they explore this area.
Additionally, the small number of analyses automatically must
make one skeptical as to the generalizability of the observations
described in reports of these studies.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S85
Evidence
Epidemiology of health care–associated candidemia. Two re-
ports either directly or indirectly explored this question [160,
161]. In general, these studies suggest that health care–asso-
ciated candidemia exists as a distinct entity. In a large surveil-
lance project focused on patients with candidemia presenting
to the emergency department, Sofair et al. [161] prospectively
evaluated all cases of candidal BSI in several hospitals in various
regions of the United States. This project was sponsored by the
CDC and represented a specific effort to grapple with the notion
of community-onset candidemia. These investigators had clear
criteria for defining a BSI caused by Candida as community
onset in origin. Of 1143 cases of candidemia evaluated, the
authors determined that 356 (31%) were community-onset in-
fections [161].
More importantly, these investigators determined the prev-
alence of select risk factors for candidemia in persons with
community-onset disease. A review of the distribution of these
risk factors reveals that the vast majority of these community-
onset cases of candidemia did, in fact, represent HAIs. For
example, 1 in 5 subjects had underlying malignancy, and more
than a quarter of the 365 persons were receiving immunosup-
pressive therapy [161]. More strikingly, approximately half of
patients with community-onset infection had central venous
catheters in place. With respect to the distribution of specific
species causing candidemia, patients with community-onset in-
fection were less likely than were persons with traditional nos-
ocomial infection to have Candida albicans implicated. Addi-
tionally, 25% of community-onset infections were due to
Candida glabrata—a rate no different from the one seen in the
traditional nosocomial candidemia cases.
Exploring the question of health care–associated candidemia
from a different perspective, Shorr et al. [160] reviewed a large
administrative database to determine the general prevalence of
health care–associated BSIs. They defined health care–associ-
ated BSI as a BSI case diagnosed within 2 days after infection
that had any of the following conditions: the patient was ad-
mitted from a nursing home, had been hospitalized in the past
30 days, was being given treatment with immunosuppressive
therapy, had active malignancy, or was receiving chronic he-
modialysis. Among nearly 7000 blood-culture–confirmed cases
of BSI, health care–associated processes accounted for nearly
55% [160]. Nearly 2% of health care–associated BSIs were due
to yeast [160]. This rate of fungal BSI was lower than the rate
of fungemia noted in nosocomial BSI. However, since the rate
was not zero, it indicated that the proposed definition for health
care–associated fungemia does capture a unique population of
patients. Conversely, these data underscore the relative infre-
quency of this condition, given the huge number of BSI cases
seen annually in emergency departments in the United States.
Implications of failure to treat candidemia. Over the past
5 years, multiple analyses have documented that failure to
promptly treat serious infections increases a patient’s proba-
bility of death [70, 79, 82, 162]. This finding has been confirmed
for multiple disease states, from VAP to severe sepsis and septic
shock [70, 79, 82, 162]. The relationship between mortality and
either a delay in initial antibiotic therapy or the administration
of inadequate therapy also applies if one focuses on specific
pathogens (e.g., MRSA), rather than on clinical syndromes [5].
The definitions used for inadequate therapy generally categorize
this as the administration of an anti-infective agent to which
the culprit pathogen is resistant in vitro.
For candidemia, only 2 reports attempted to address the
relationship between inadequate or delayed antifungal therapy
and survival [91, 92]. A potential explanation for the existence
of so few reports dealing with this topic is the fact that in vitro
susceptibilities for antifungal agents are not well described and
that controversy exists regarding what represents in vitro
“resistance.”
In a retrospective analysis, Morrell et al. [92] reviewed 157
cases of candidemia. Their aims were to determine predictors
of outcome in this disease and to describe the relationship
between survival and both delays in antifungal therapy and
inadequate antifungal treatment. Two analyses were conducted;
the primary analysis included all antifungals, and a secondary
analysis evaluated patients infected with C. albicans, Candida
parapsilosis, or Candida tropicalis generally susceptible to flu-
conazole. The results were not stratified by organism type. Ap-
proximately half of the patients were infected with a non–C.
albicans species, and nearly 1 in 5 cases was attributed to either
Candida krusei or C. glabrata [92]. They defined delayed ther-
apy as administration of an antifungal agent 112 h after the
patient’s initial blood culture specimen was drawn. Inadequate
therapy represented use of fluconazole for infections due to C.
krusei. Specific MIC90 breakpoints were not determined. Overall
mortality approached 30%, which is similar to the death rate
for candidemia described in other reports [92]. For example,
in the analysis by Sofair et al. [161] noted above, the death rate
for candidemia exceeded 25%.
Of the 157 patients, only 5 received timely and adequate
antifungal therapy. Strikingly, the death rate among patients
given adequate treatment within 12 h after the blood culture
specimens were drawn was only 10% [92]. Among persons
given antifungal therapy beyond this 12-h window, the mor-
tality rate increased to 33% ( ) [92]. More importantly,P p .169
when stratifying the time to therapy into the periods of 12–24
h, 24–48 h, and 148 h after blood culture specimens were
drawn, these authors saw no difference in mortality. In mul-
tivariate analysis, a delay in antifungal treatment independently
doubled a patient’s risk of death.
Confirming these observations, Garey et al. [91] reviewed
230 cases of candidemia at 4 different centers. The crude mor-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S86 • CID 2008:47 (Suppl 2) • Kollef et al.
tality rate in this cohort was 30%. Of note, all subjects were
given treatment with fluconazole. These authors determined
that persons given fluconazole on the day the culture specimen
was obtained faced a mortality risk of 15%. They also observed
a stepwise increase in probability of death as time progressed
( ). Specifically, persons given treatment on the dayP p .0009
after the culture specimen was drawn had a mortality rate of
25%, whereas those who were finally given fluconazole �3 days
after the culture specimen was drawn had a 40% unadjusted
chance for in-hospital death [91]. In their logistic regression,
delay in therapy heightened the potential for death by 50%
(AOR, 1.50; 95% CI, 1.09–2.09) [91]. This relationship per-
sisted even after exclusion of persons for whom fluconazole
may have been inadequate on the basis of a definition similar
to the one employed by Morrell et al. [92].
Is risk stratification possible? Numerous reports detail po-
tential risk factors for fungemia [158, 159]. These range from
patient variables, such as a history of recent abdominal surgery
and underlying malignancy, to process of care issues, including
presence of a central venous catheter or receipt of parenteral
nutrition [158, 159]. Unfortunately, efforts to develop a specific
risk score that identifies persons with fungemia as the likely
cause of their syndrome have been fraught with limitations.
Often 2 approaches are employed—one relying on the presence
of certain risk factors, and the other using surveillance for
Candida colonization. Use of risk scores tends to compromise
specificity for the sake of sensitivity. In other words, although
a proposed score may identify a cohort of persons more likely
to have candidemia, the rate of candidemia remains sufficiently
low, and it can be presumed that clinicians would need to give
treatment to many patients without candidal infection to ensure
that they were capturing cases of candidemia. Alternatively,
surveillance-based strategies are necessarily cumbersome and
are unlikely to be of value for treatment of health care–asso-
ciated candidemia, because the patient is, by definition, pre-
senting to the emergency department and has not been in the
hospital long enough to have had surveillance cultures
performed.
A report by Leon et al. [163] represents a recent attempt to
refine the risk-score paradigm. In a multicenter trial in Spain,
these investigators studied 1669 persons who stayed in the ICU
for at least 7 days. The overall rate of candidemia was 6%
[163]. Specific variables associated with subsequent ICU-onset
candidemia included recent surgery, underlying severe sepsis,
use of parenteral nutrition, and known Candida colonization
[163]. Researchers developed a complex point-scoring tool
based on logistic regression, which employed good screening
characteristics for candidemia. Based on the plot of the receiver
operating curve, their score had an area under the curve of
0.85 [163]. However, this score has not been independently
validated in other settings or in other studies. Furthermore, for
the purposes of determining who might be at greater risk for
health care–associated fungemia, their score may not be ap-
plicable, because it incorporates the findings from surveillance
cultures.
Addressing colonization in particular, Pairroux et al. [164]
explored a role for the colonization index in determining the
potential for candidemia. Again, admittedly, this strategy will
not be helpful in the emergency department. However, for
completeness, readers should familiarize themselves with this
paradigm. These researchers completed a before-after study re-
lying on the colonization index. They computed the coloni-
zation index as the number of sites on a patient that tested
positive for Candida divided by the total number of sites
swabbed. Swabbing was done biweekly. If the colonization in-
dex was 10.4, these patients were given preemptive therapy
with fluconazole. With this technique and strategy, they were
able to significantly reduce rates of proven ICU-acquired can-
didemia (from 2.2% to 0%; ) [164].P ! .001
There were no specific reports investigating risk stratification
in health care–associated or community-onset fungemia. This
is perhaps not surprising, given the overall limited literature
on this topic.
Grading of Evidence
On the basis of a review of the studies cited above, the workshop
members agreed that the nature of the evidence available to
support this statement was category II (table 3).
Level of Support
When voting on the support for this statement, 0% of the
summit participants voted to accept the statement completely,
64% voted to accept the statement with some reservations, 27%
voted to accept the statement with major reservations, and 9%
voted to reject the statement with reservations. None rejected
the statement completely. In comparison, of the 744 IDSA
members who participated in the online survey, 27% voted to
accept the statement completely, 44% voted to accept the state-
ment with some reservations, 17% voted to accept the state-
ment with major reservations, 10% voted to reject the statement
with reservations, and 2% voted to reject the statement com-
pletely (figure 10).
Discussion
This statement should be viewed as complementary to the oth-
ers in this supplement, addressing both particular pathogens
and specific HAI syndromes. For the concept of HAI to prove
meaningful, it must be internally consistent. Thus, if one lim-
ited the health care–associated stratification to bacterial path-
ogens only, the entire notion might prove both difficult to apply
and unhelpful. Therefore, recognition that, even for fungal BSI,
the health care–associated concept is unique reinforces the sup-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S87
Figure 10. Voting comparison for statement 8 (“Patients with seriousHAIs who have risk factors for fungal infections require early empiricantifungal therapy to reduce mortality”). “IDSA” refers to the membersof the Infectious Diseases Society of America who responded to a Web-based survey; “Summit” refers to the Health Care–Associated Infection(HAI) Summit panel.
port for the need to adopt HAIs as distinct syndromes. Al-
though there is certainly overlap between community-acquired,
health care–associated, and nosocomial processes, the evidence
consistently underscores the need to break our traditional di-
chotomous classification scheme into 3 distinct components.
Unfortunately, there are only 2 analyses that specifically ad-
dress the epidemiology of health care–associated candidal BSIs
[160, 161]. These studies, however, were internally valid and
well conducted. Thus, clinicians should at least recognize the
potential for candidemia to be a cause of BSI in patients pre-
senting to the emergency department. This statement is not
meant to imply that physicians should prescribe antifungal
treatment either routinely or reflexively. Instead, local epide-
miologic information must be gathered to facilitate the devel-
opment of local protocols to determine whether Candida spe-
cies are an issue of concern. Readers should also note that there
are no data suggesting that health care–associated candidemia
does not exist. In other words, there are no studies that spe-
cifically disprove this assertion.
For risk stratification, one must rely on clinical judgment.
No reliable tool exists to help determine which patients face
an elevated potential for candidemia. Given the pathophysi-
ology of the process, it appears that immunosuppression or
presence of a central venous catheter is necessary, but neither
is a sufficient condition for this disease. Perhaps, therefore, in
giving treatment to persons presenting with a syndrome con-
sistent with severe sepsis but not showing evidence of pul-
monary infection (or other evident infection), clinicians should
consider more formally candidal BSI in the differential diag-
nosis, particularly if multiple risk factors, including those noted
above, are present. However, this recommendation represents
opinion more than fact but does acknowledge that failure to
promptly and adequately treat fungal BSI leads to substantial
excess mortality. Conversely, one cannot hope to begin anti-
fungal therapy promptly if one presupposes that yeast can never
be a cause of health care–associated BSI. Given that it seems
that the vast majority of patients are not given prompt treat-
ment, it appears there is ample room for improvement.
Future Directions
Certainly, more broadly designed prospective epidemiologic re-
search is required. Such projects must include a range of in-
stitutions, rather than a focus exclusively on academic centers.
With such information, geographic variations may become ap-
parent. More importantly, these surveillance studies can si-
multaneously collect information that allows for the develop-
ment and validation of risk-stratification tools. Finally, other
diagnostic measures are needed. Since cultures for Candida may
take several days to grow, clinicians require more-rapid diag-
nostic interventions to determine whether to continue or stop
presumptive antifungal treatment.
STATEMENT 9: ALL INFECTIONS INIMMUNOCOMPROMISED PATIENTS SHOULDBE CONSIDERED HAIs UNTIL PROVENOTHERWISE
Rationale and Definition of Statement
Infection due to a diverse spectrum of pathogens is the most
common and well-recognized complication in patients with
compromised immunologic host defenses as well as a native
disease and/or iatrogenic interventions. The microbial etiology
for such infections may vary across different specific immune
defects, severity and duration, and other modifiers, including
the patient’s prior and present geographic location, prior ex-
posure to anti-infectives for prophylaxis or treatment, and ex-
ogenous exposures (e.g., transfused blood products or donor
organs). The orthodox view pertaining to the origin of infec-
tions in immunocompromised hosts recognizes that the incit-
ing organism(s) may originate from (1) the patient’s native
endogenous flora or dormant organisms, which become re-
activated with failed immune defenses; (2) endogenous flora,
which has been modified principally by exposure to anti-in-
fective agents or the animate and inanimate nosocomial en-
vironment; (3) exogenous reservoirs; and (4) as-yet-unknown
sources. Among organ transplant recipients, the donor organ
represents another reservoir for pathogen transmission. Al-
though much of the important clinical management of im-
munocompromised patients occurs within the hospital unit or
the critical care setting, some of the management has shifted
to the parahospital or outpatient health care facilities. Promi-
nent examples include outpatient chemotherapy for oncologic
disease, management of HIV-associated illness, and long-term–
acute care facilities that receive organ transplant recipients for
ventilator dependence or rehabilitation. HAIs within this ex-
panded sphere might have a greater impact on the immuno-
compromised host than on immunocompetent patients and
also may be caused by a different spectrum of pathogens. With
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S88 • CID 2008:47 (Suppl 2) • Kollef et al.
respect to MDR bacteria, the duration of antecedent coloni-
zation and the incidence of progression to infection are 2 pa-
rameters that may have a greater impact on immunocompro-
mised patients. This section focuses on whether there is
evidence in the literature confirming that the health care en-
vironment is the exclusive source of all infections in the im-
munocompromised host.
Methods
A literature search of the PubMed database was performed on
15 September 2007, and results were narrowed to the English
language and human subjects. The purpose of the search was
to identify published articles on the epidemiology of infection
among immunocompromised hosts and, specifically, to deter-
mine whether the inciting pathogens were acquired in a com-
munity, health care, or hospital setting. The initial search terms
and combinations included “immunocompromise AND
healthcare-associated infection,” which yielded 656 articles;
“immunocompromise AND infection AND epidemiology,”
which yielded 1971 articles; and “immunocompromise AND
community-acquired infection,” which yielded 127 articles.
Only articles that included major immunocompromised host
categories (bone marrow or solid organ transplant recipients
and patients with cancer, neutropenia, granulocytopenia, or
AIDS) were selected for further review. After examinination of
all articles for these criteria, a total of 12 articles were deemed
relevant to the statement.
A second PubMed search for specific MDR pathogens of
interest (S. aureus, Enterococcus, P. aeruginosa, Candida, and
Aspergillus) was combined with “immunocompromised” and
was limited to the English language only. The search terms
“immunocompromise AND antimicrobial resistance” yielded
225 articles, “methicillin-resistant Staphylococcus aureus”
yielded 110 articles, “immunocompromise AND Enterococcus”
yielded 84 articles, “immunocompromise AND Candida”
yielded 970 articles, and “immunocompromise AND Aspergil-
lus” yielded 904 articles. Since prolonged colonization with such
organisms may represent a more sensitive end point when the
presence of health care acquisition is discerned, all the organ-
ism-specific searches were also combined with the term
“colonization.”
Evidence
Is the health care environment the exclusive source for all
infections in immunocompromised patients? Not all infec-
tions in immunocompromised patients are the result of health
care exposures; some patients become colonized and infected
with pathogenic organisms as a result of their weakened im-
mune status. Kotton et al. [165] mentioned numerous reports
of transmission of zoonosis to humans during and after solid-
organ and hematopoietic stem cell transplantation. The ma-
jority of zoonoses cases are acquired after transplantation. Cer-
tain occupations (e.g., veterinarian, farmer, and forestry
worker), pet ownership, hobbies (e.g., hunting), and travel also
increase the risk of acquisition [166]. Lamaris et al. [167] also
reported the incidence of Scedosoprium infections among 21
patients with cancer in 1989–2006. The authors concluded that
these infections were associated with typical immunologic de-
fects, such as hematologic cancer, neutropenia, lymphopenia,
and systemic steroid use. Although an increase in the incidence
was seen in the last 5 years of the study, there was no evidence
of nosocomial transmission.
Does immunocompromise contribute independently to the
alteration of the epidemiology of HAI? Several articles in-
vestigated whether there are significant differences in the eti-
ology of infection between immunocompromised and non-
immunocompromised hosts. A study by Shorr et al. [160] of
a 2-year database of BSIs, which were subsequently classified
as community-acquired, health care–acquired, or hospital-ac-
quired infection, demonstrated only minimal differences in the
etiology between immunocompromised patients ( )n p 2140
and immunocompetent patients ( ). When all acqui-n p 4557
sition categories were analyzed, no significant differences in the
incidence of any gram-positive pathogen were observed.
Among gram-negative organisms, the incidences of Pseudo-
monas species (4.0% vs. 2.3%; ) and Klebsiella speciesP p .001
(8.2% vs. 5.1%; ) were significantly higher among im-P ! .001
munocompromised patients than among nonimmunocom-
promised patients [160].
A study by Dimiopoulos et al. [168] compared the charac-
teristics of candidemia between immunocompromised (n p
) and immunocompetent ( ) patients. The mean time9 n p 15
from hospitalization to diagnosis of candidemia was 9 days
(range, 5–11 days). With respect to risk factors, no important
differences were observed between the 2 cohorts [168].
Immunosuppression was not found to be a significant risk
factor for all MDR bacterial infections in the ICU in a retro-
spective, matched, case-control study of 256 medical/surgical
ICU patients [169]. With the notable exception of MRSA, which
was significantly more frequent in the immunosuppressed co-
hort (25 of 44 vs. 10 of 26; ), there was no independentP p .01
association between immunosuppression and ICU-acquired
MDR organisms.
Does immunocompromise contribute to a higher incidence
of MDR colonization and thus act as a precursor to HAI?
Several studies have examined the incidence of MDR coloni-
zation among immunocompromised patients. In a prospective
observational study of 2347 admissions in 14 French ICUs,
nasal and cutaneous swab screening was performed to deter-
mine the variables associated with MRSA carriage at the time
of ICU admission [170]. Immunosuppression was not associ-
ated with an increased risk of MRSA carriage. Furuno et al.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S89
[171] confirmed that risk factors other than immunosuppres-
sion identified patients colonized with antibiotic-resistant bac-
teria. They found that previous hospital admission occurring
within 1 year before the time of current hospitalization was
independently associated with a high risk of carriage of anti-
biotic-resistant bacteria. Nseir et al. [169] conducted a retro-
spective case-control study to determine the relationship be-
tween immunosuppression and ICU-acquired MDR bacteria
(MRSA, ESBL-producing organisms, and MDR P. aeruginosa,
Acinetobacter baumannii, and Stenotrophonmonas maltophilia).
In univariate analysis, immunosuppressed patients had a higher
incidence of colonization with these organisms than did im-
munocompetent patients (22 per 1000 patient-days vs. 12 per
1000 patient-days; ); however, in multivariate analysis,P p .004
antibiotic treatment administered before or during the ICU stay
remained a significant factor. A 6-year study by Reddy et al.
[172] examined the results of rectal swab screening for ESBL-
producing gram-negative bacilli in 17,872 patients hospitalized
in high-risk units. Notably, the medical ICU service had the
highest incidence of colonization with ESBL-producing organ-
isms during the study period, whereas the hematology/oncology
and solid-organ transplant units experienced significantly lower
incidences.
Does immunocompromise contribute to a prolongation of
MDR colonization and thus act as a precursor to HAI?
There is limited evidence examining the duration of MDR col-
onization in immunocompromised patients. Most of the avail-
able evidence focuses on duration of colonization with van-
comycin-resistant enterococci (VRE). The reports that have
demonstrated a prolonged duration of VRE gastrointestinal col-
onization have studied immunocompromised patients, such as
abdominal solid-organ recipients and oncologic patients with
or without neutropenia [173–175]. One study by Montecalvo
et al. [173] determined that 86 oncologic patients with VRE
colonization were identified. Colonization was persistent for 17
weeks in the majority of patients. Of 34 colonized patients
discharged from and then readmitted to the hospital after a
mean of 2.5 weeks, 22 (61%) were still colonized with VRE.
PFGE further demonstrated that VRE colonization with the
same strain could persist for at least 1 year. In a similar patient
population, Roghmann et al. [175] found a 44% rate of per-
sistent VRE colonization. Patel et al. [174] reported the results
of serial rectal surveillance cultures from 52 liver and kidney
transplant recipients during both inpatient and outpatient pe-
riods and followed up for a median of 306 days. Persistent VRE
colonization was present in 150% of the initial cohort.
Are there infections in immunocompromised hosts that arise
from distinct community reservoirs or from shared reservoirs
between the community and the health care setting? There
is ample evidence that the same pathogen can originate from
both community and health care settings. Representative ex-
amples found in the search included Legionella species, My-
cobacterium tuberculosis, Aspergillus species and other mycelial
organisms, influenzae viruses, varicella-zoster virus, and respi-
ratory syncytial virus [167, 176–178]. Pneumocystis, on oc-
casion, can be acquired as a nosocomial pathogen. Organisms
that appear to be acquired exclusively in the community setting
include Listeria monocytogenes, Nocardia species, Cryptococcus
neoformans, endemic mycoses, Pneumocystis jiroveci, Toxo-
plasma gondii, Strongyloides stercoralis, and other parasites, as
well as pathogens causing zoonotic infections [165].
Grading of Evidence
On the basis of a review of the studies cited above, 20% of the
workshop members voted that the evidence to support the
statement was category II, 20% voted category III, and 60%
voted category V (table 3).
Level of Support
Overall, 0% of the summit participants voted to accept the state-
ment completely, 0% voted to accept the statement with some
reservations, 27% voted to accept the statement with major res-
ervations, 45% voted to reject the statement with reservations,
and 27% voted to reject the statement completely. In comparison,
of the 744 IDSA members who participated in the online survey,
11% voted to accept the statement completely, 28% voted to
accept the statement with some reservations, 15% voted to accept
the statement with major reservations, 27% voted to reject the
statement with reservations, and 19% voted to reject the state-
ment completely (figure 11).
Discussion
Although the epidemiology of infection among immunocom-
promised patients has been studied intensively and reported
for decades, there are few, if any, studies that pinpoint the
precise time and location when the pathogen is acquired (other
than rare and well-documented epidemic outbreaks). Thus,
many of the diverse organisms that can cause infection in the
immunocompromised host are presumptively classified as com-
munity associated, hospital associated, or health care associated,
on the basis of the known ecology (i.e., natural reservoirs and
vectors), biology (i.e., incubation period and latency), and ep-
idemiology (i.e., presence of geographic or temporal clusters
supported by molecular typing methods that match the or-
ganism patient-to-patient or between a patient and an envi-
ronmental source) of the pathogen in question.
The paucity of precise investigations in this area necessitated
a somewhat oblique approach to the literature search. Not sur-
prisingly, the search effort produced a very low level of evidence
in support of the statement that all infections should be con-
sidered health care–associated among immunocompromised
patients. It is reasonable to assume that (1) immunocompro-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S90 • CID 2008:47 (Suppl 2) • Kollef et al.
Figure 11. Voting comparison for statement 9 (“All infections in immunocompromised patients should be considered HAIs until proven otherwise”).“IDSA” refers to the members of the Infectious Diseases Society of America who responded to a Web-based survey; “Summit” refers to the HealthCare–Associated Infection (HAI) Summit panel.
mised patients are exposed more intensively to the health care
setting after or between hospitalizations than are immunocom-
petent patients and (2) residual effects of health care exposure
could lead to health care acquisition of a finite number of
pathogens and infections attributable to those pathogens. How-
ever, with regard to MDR bacteria, the available literature fails
to show an independent association of immunocompromised
states with either colonization or infection with such pathogens.
Instead, such observations were mediated by more-dominant
mechanisms, such as antimicrobial exposure, intensity, and du-
ration of health care exposures, in which “immunocompro-
mise” was a surrogate marker. Although colonization-to-infec-
tion ratios may be quite high (particularly for low-virulence
pathogens, such as VRE), it was important to direct part of
the search effort to a “colonization” end point because mod-
ification of the patient’s endogenous microbial reservoirs is a
well-recognized antecedent condition to an overt infection
[179].
Future Directions
The idealized study prototype, which would allow a clear and
scientific conclusion as to whether a pathogen was health care
associated or non–health care associated among immunocom-
promised patients, requires sequential testing with a highly sen-
sitive and specific assay for the presence of the pathogen of
interest performed throughout periods of health care exposure
and non–health care exposure. The rapid development and
deployment of gene-based and other molecular diagnostic
methods as investigative tools to detect the presence of resis-
tance could be valuable in answering this intriguing question.
STATEMENT 10: ADJUNCTIVE THERAPYSHOULD BE UTILIZED TO PREVENT ANDTREAT SERIOUS HAIs
Rationale and Definition of Statement
Serious infections are a leading cause of death in hospitalized
patients, with a mortality rate of up to 60% among patients
manifesting septic shock [180]. Adjunctive therapies targeted
to control the immunologic, inflammatory, and procoagulant
response elicited by infection have been researched and pre-
scribed for decades. In this section, we specifically review the
level of evidence supporting tight glycemic control, avoidance
of RBC transfusion, IVIG, and drotrecogin alfa (activated) as
adjunctive therapies for the treatment of HAIs, with emphasis
on the critically ill population.
Methods
A PubMed database search was conducted to identify relevant
reports involving each adjunctive therapy. The search strategy
was limited to humans, the English language, clinical trials,
randomized controlled trials, and meta-analyses. Text terms for
each adjunctive therapy—that is, “IVIG,” “IGIV,” “intravenous
immune globulin,” and “intravenous immunoglobulin”—were
combined using the “OR” function and then were combined
using the “AND” function with search terms describing HAI,
including “bacteremia,” “bloodstream infection,” “pneumo-
nia,” “nosocomial infection,” and “infection.” The search
yielded 88 articles for “tight glycemic control,” 29 articles for
“red blood cell transfusion avoidance,” 87 articles for “IVIG,”
and 88 articles for “drotrecogin alfa (activated).” Bibliographies
of selected articles were also reviewed to identify relevant
reports.
Evidence
Tight glycemic control. Hyperglycemia is a common occur-
rence in patients in the critical care setting, regardless of history
of diabetes mellitus. The etiology of hyperglycemia is multi-
factorial and may adversely affect immune function, such that
an inflammatory state is promoted and granulocyte adherence,
chemotaxis, phagocytosis, and intracellular killing are nega-
tively altered [181]. Control of hyperglycemia in the acute care
setting has been associated with prevention of sternal wound
infection and survival in patients undergoing cardiac surgery
procedures [182, 183].
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S91
Limited data are available on controlling glucose levels and
outcomes in critically ill patients with HAI. Compelling data
on critically ill patients with or without infection were reported
in a prospective, randomized, controlled trial that considered
whether intensive insulin therapy (defined by targeted blood
glucose levels of 80–110 mg/dL) reduced ICU mortality among
1548 surgical ICU patients [184]. Compared with patients who
received conventional treatment (targeted blood glucose levels,
180–200 mg/dL), patients randomized to receive intensive in-
sulin therapy had significantly decreased rates of ICU mortality
(8.0% vs. 4.6%; ) and in-hospital mortality (10.9% vs.P ! .04
7.2%; ). The greatest reduction in mortality appearedP p .01
to be limited to patients who required �5 days of ICU care
and may have been linked to infection prevention, as indicated
by a marked reduction in deaths due to multiple organ failure
secondary to sepsis and in rates of septicemia. Not surprisingly,
hypoglycemia occurred in 39 patients in the intensive-treatment
group and in 6 patients in the conventional-treatment group.
A follow-up trial involving 1200 adult medical ICU patients
conducted by the same group of investigators using identical
methodology revealed similar findings [184, 185]. Although the
intention-to-treat in-hospital mortality was not statistically dif-
ferent between groups, the subgroup of patients requiring �3
days of ICU care and randomized to receive intensive insulin
therapy had significantly increased hospital survival, compared
with patients in the conventional arm (57% vs. 47%; P p
). The occurrence of hypoglycemia, defined as a blood.009
glucose level !40 mg/dL, was alarmingly high in the group
receiving intensive insulin therapy (25.1% vs. 3.9%; ).P ! .001
A retrospective evaluation of the effects of tight glycemic con-
trol on critically ill patients with sepsis at the time of admission
found no difference in the in-hospital or ICU mortality among
all patients; however, a survival advantage was observed among
patients requiring �3 days of ICU care plus intensive insulin
therapy (OR, 2.9; 95% CI, 1.8–4.6; ) [186]. FurtherP ! .001
evaluation of the impact of hypoglycemia in the subgroup of
patients with sepsis at ICU admission found it to be indepen-
dently associated with in-hospital mortality (AOR, 2.8; 95%
CI, 1.8–4.2; ). This finding has been confirmed in aP ! .001
separate evaluation [187].
Avoidance of RBC transfusions. Transfusion of packed
RBCs (PRBCs) is a common intervention for critically ill pa-
tients. For patients with severe sepsis, PRBC transfusion has
become part of a widely adopted resuscitation algorithm used
in many hospitals and endorsed by the Surviving Sepsis Cam-
paign guidelines [10, 188–191]. The basis of this recommen-
dation and its subsequent implementation at the local level
stems from significantly improved survival in the landmark trial
of early goal-directed therapy [192]. However, whether trans-
fusion therapy is a key ingredient of improved outcomes for
patients with severe sepsis remains uncertain, and, when closely
scrutinized in all critically ill patients, this form of therapy may
be correlated with major nosocomial complications, most no-
tably infection.
The strongest evidence linking PRBC transfusion and nos-
ocomial infection comes from large observational trials and,
therefore, should not be interpreted as absolute proof of hy-
pothesis. Nonetheless, the accumulated data consistently point
to a direct relationship between transfusion and infectious com-
plications. The CRIT trial—a prospective, observational study
of transfusion practices in the United States conducted over a
10-month period in 2000 and 2001—evaluated 4892 patients
in 284 distinct ICUs [193]. Within this population, 3502 pa-
tients were free of BSI at baseline, as well as 48 h after en-
rollment, and were secondarily evaluated for the development
of BSI [194]. Of the patients, 49% received transfusion and
3.3% developed a BSI during the 30-day evaluation. Patients
who were found to develop BSI were significantly more likely
to receive PRBC transfusion (76.1% vs. 48.7%; ) andP ! .001
to have a greater number of units transfused (4.0 � 4.6 U vs.
2.3 � 4.3 U; ), compared with patients without thisP ! .001
infectious complication. In multivariable analysis, transfusion
was found to significantly increase the likelihood of BSI (AOR,
2.23; 95% CI, 1.43–3.52; ), and the probability increasedP ! .001
as the number of PRBC units transfused increased. Using the
same CRIT study population, a subgroup of 1518 patients who
required mechanical ventilation for at least 48 h were evaluated
for the development of VAP [195]. Overall, 52.7% of patients
receiving mechanical ventilation received transfusion, and
22.6% received a diagnosis of VAP. Similar to findings of the
aforementioned BSI analysis, patients with VAP were signifi-
cantly more likely to receive transfusion (58.2% vs. 51.4%;
), and transfusion was an independent predictor of VAPP p .03
development in the multivariable analysis (AOR, 1.89; 95% CI,
1.33–2.68; ). A single-center, prospective, observa-P p .0004
tional cohort of 2085 mixed medical/surgical ICU patients
found that patients who received transfusion ( ) had an p 428
significantly higher incidence of nosocomial infection (14.3%
vs. 5.8%; ), longer length of ICU stay (8.2 � 11.7 daysP ! .001
vs. 3.3 � 5.1 days; ), longer length of hospital stayP ! .001
(18.3 � 18.7 days vs. 9.9 � 9.5 days; ), and higher in-P ! .001
hospital mortality rate (10.2% vs. 21.8%; ), comparedP ! .001
with patients who did not receive transfusion [196].
Drotrecogin alfa (activated). The use of drotrecogin alfa
(activated), the recombinant form of human activated protein
C, as an adjunctive therapy for infections manifesting as severe
sepsis and septic shock has been widely studied. The question
of which patient subgroup is most likely to benefit from the
therapy and, at the same time, be protected from drug toxicity,
most notably bleeding, remains largely unresolved. Collectively,
4 large industry-sponsored trials form the basis for bedside
decision-making regarding the use of drotrecogin alfa (acti-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S92 • CID 2008:47 (Suppl 2) • Kollef et al.
vated) for adults [114, 197–199]. In each trial, ∼75% of patients
presented from the community, and among 50% of these pa-
tients, the lung was the site of infection. The FDA-approved
labeling for drotrecogin alfa (activated) is derived from the
initial landmark trial, PROWESS [114]. In this trial of 1690
patients with severe sepsis or septic shock, a 6.1% absolute risk
reduction in mortality was observed that favored drotrecogin
alfa (activated) over placebo; however, the benefit appeared to
be limited to the patient subgroup that had a higher severity
of illness, as indicated by an APACHE II score of �25 [200,
201]. Additional subgroup analysis of this trial revealed that
patients with severe CAP given treatment with drotrecogin alfa
(activated) were also statistically more likely to survive [202].
The lack of efficacy for patients with a low severity of illness,
as indicated by an APACHE II score of !25 or by single-organ
dysfunction, was confirmed in a follow-up trial that was halted
because of therapeutic futility found by an interim analysis
[197].
Two initial, randomized, placebo-controlled trials demon-
strated consistent bleeding rates. In contrast, an open-label trial
of 2375 patients who received drotrecogin alfa (activated) re-
vealed higher rates of serious bleeding during the 96-h infusion
period and the 28 days after drug initiation in a noncontrolled
setting [199]. These results, coupled with a higher number of
CNS bleeding events observed with administration of drotre-
cogin alfa (activated), compared with placebo, during the in-
fusion (27 events vs. 3 events) and after 28 days (60 events vs.
6 events) in the accumulation of the 4 largest trials to date,
indicate that the serious bleeding risk posed by drotrecogin alfa
(activated) requires careful consideration before prescribing,
particularly for patients with severe thrombocytopenia or men-
ingitis [203].
IVIG. IVIG in polyclonal form has been extensively studied
as an adjuvant therapy for severe infections. The complete
mechanism of action is unknown, but the fundamental phar-
macology of IVIG is activity against bacterial products, includ-
ing endotoxin, other superantigens, and host cytokines. Re-
cently, 3 meta-analyses have been published on the use of
polyclonal IVIG for critically ill adult patients with sepsis, severe
sepsis, or septic shock [204–206]. Despite the heterogeneous
patient populations, as well as variable dosing, duration, and
product composition, each evaluation found IVIG to be as-
sociated with a significant survival benefit. However, when only
high-quality trials (randomized, double-blind, placebo-con-
trolled trials) are considered in the meta-analysis, the associ-
ation with improved survival does not exist [205, 206]. This
finding is consistent with recently published high-quality trials.
The Score-Based Immunoglobulin Therapy of Sepsis study
found no difference in 28-day mortality between patients given
a 2-day course of intravenous IgG and patients given placebo
(39.3% vs. 37.3%; ) [207]. Likewise, a trial of IgMA-P p .67
enriched immunoglobulin compared with placebo for neutro-
penic patients with sepsis caused by gram-negative organisms
( ) found no difference in mortality at 28 days (26.2%n p 211
vs. 28.2%; ) [208]. Additionally, it appears that poly-P p .93
clonal IVIG is of limited benefit relative to placebo in targeting
specific populations, including patients with streptococcal toxic
shock syndrome and intra-abdominal sepsis [113, 209].
Grading of Evidence
On the basis of a review of the literature cited above, workshop
members voted that the nature of evidence for the statement
ranged from category I to category IV (table 3).
Level of Support
Overall, 9% of the summit participants voted to accept the state-
ment with some reservations, 73% voted to accept the statement
with major reservations, and 18% voted to reject the statement
with reservations. In comparison, of IDSA members who com-
pleted the online survey, 18% voted to accept the statement
completely, 40% voted to accept the statement with some res-
ervations, 23% voted to accept the statement with major res-
ervations, 18% voted to reject the statement with reservations,
and 0% voted to reject the statement completely (figure 12).
Discussion and Future Directions
This role of adjunctive therapies for the treatment of HAI re-
mains unclear, as demonstrated by the summit participants and
IDSA membership. Summit participants did concede that there
is evidence that tight glycemic control reduces ICU mortality
and that the incidence of bacteremia, VAP, and mortality is
related to RBC transfusions. However, there is inadequate evi-
dence for and controversy regarding the use of activated protein
C and IVIG as adjunctive therapies for the treatment of HAI.
The lack of consensus can be traced to the heterogeneous nature
of infections and patient populations. Therefore, translation of
the results of the cumulative literature for bedside care remains
a patient-by-patient decision. The practice of tight glycemic
control, avoidance of PRBC transfusion, and use of drotrecogin
alfa (activated) or IVIG for patients with HAI will become more
universal only with more succinctly defined clinical targets,
standardized preparations, and, perhaps, disease-state bio-
markers identifying patients who would most likely benefit
from adjunctive therapies.
CONCLUSIONS
HAIs should be viewed as distinct infections that identify in-
dividuals with an increased risk of infection with MDR path-
ogens. The current level of evidence is such that this idea ap-
pears to be best supported for HCAP and health care–associated
BSIs. Other infections, including intra-abdominal, skin, uri-
nary-tract, CNS, and pediatric infections, have not been as well
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S93
Figure 12. Voting comparison for statement 10 (“Adjunctive therapy should be utilized to prevent and treat serious HAIs”). “IDSA” refers to themembers of the Infectious Diseases Society of America who responded to a Web-based survey; “Summit” refers to the Health Care–AssociatedInfection (HAI) Summit panel.
studied, and definitive statements regarding HAI for these cat-
egories await the findings of future studies. However, it appears
prudent to identify patients at risk for infection with MDR
pathogens or any other type of infection, to increase the like-
lihood of administration of appropriate empirical antimicrobial
therapy.
Initial treatment with an appropriate antimicrobial regimen
is associated with reduced risk of death and more–cost-effective
medical care during hospitalization. To provide appropriate
empirical therapy, clinicians must actively identify risk factors
for colonization or infection with MDR pathogens in the pa-
tients for whom they provide treatment. Classification of the
patient as at risk for HAI is a surrogate marker for increased
risk of colonization and infection with MDR bacteria. At the
same time, clinicians must develop and implement strategies
in their hospitals to ensure that unnecessary antimicrobial usage
is avoided, to minimize the emergence of antibiotic resistance.
The de-escalation strategy is one that attempts to accomplish
this dual goal by providing for the administration of broad-
spectrum empirical antimicrobial therapy to patients at risk for
MDR infection while modifying the empirical antimicrobial
regimens on the basis of microbiological, antimicrobial-sus-
ceptibility, and clinical-response data. De-escalation also im-
plies that the shortest antimicrobial regimen deemed appro-
priate for a patient’s infection and clinical response should be
employed. This strategy is intended to improve short-term out-
comes for individual patients and long-term outcomes for the
general population.
The goal of the HAI Summit was to critically appraise ex-
isting literature, to assess the relative strengths and limitations
of our current knowledge in this area. A recurring theme, re-
gardless of which statement was being discussed, was the pau-
city of specific data concerning HAIs and the frequent extrap-
olation of data from studies of nosocomial infections. The
“Treatment by Sites of Infection” workshop showed that only
HCAP and health care–associated BSI have been directly eval-
uated as separate distinct clinical entities. However, even for
these infections, it is apparent that additional studies are needed
to define the criteria for and definition of HAI. For other in-
fections, including skin and intra-abdominal infections, inves-
tigations evaluating patients at risk for HAI are needed. One
assumption made by the HAI Summit members is that the
criteria for HAI are similar for all the infections examined.
However, this may not be correct, and there is room for debate
regarding which patient subsets should be included. For ex-
ample, the presence of a device such as a joint prosthesis could
be an unexplored criterion for health care–associated BSI, but
this might not be the case for HCAP. Clearly, there is overlap
among all these infections in terms of distinguishing HAI from
community-acquired infection. Nevertheless, additional studies
are needed to validate these statements.
In the “Treatment by Organism” workshop, these complex
concerns translated into discrepant opinions regarding the op-
timal approach to the administration of empirical therapy to
patients at risk for HAI. Again, the theme of antimicrobial de-
escalation emerged as a unifying concept, regardless of infection.
However, the specific agents employed for initial antimicrobial
treatment of HAI could vary, depending on the site of infection.
Additionally, the need to provide specific coverage for distinct
pathogens (MRSA and Candida species) in patients at risk for
HAI also led to much discussion and debate. These discussions
focused on the need to balance empirically covered MDR path-
ogens through the use of broad-spectrum therapy while mini-
mizing the generation of more resistance through unnecessary
antibiotic use. An example is the need to provide double coverage
for suspected HAI caused by gram-negative bacteria. Adding an
aminoglycoside to a b-lactam or carbapenem is likely to increase
overall coverage, compared with the addition of a fluoroquin-
olone. However, unnecessary use of dual coverage could also
promote more antimicrobial resistance.
At the summit’s conclusion, participants identified several
areas of research that merit priority to refine our care of patients
with HCAP. Large-scale, multicenter, observational cohort
studies with rigorous microbiological data are needed to better
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S94 • CID 2008:47 (Suppl 2) • Kollef et al.
define the precise subsets of patients at risk for infection with
MDR pathogens, as well as to better delineate risk factors for
specific pathogens. Similar studies are needed regarding the
implications of severity of illness for outcomes. In addition, a
clear need exists for specific studies on antibiotic therapy de-
escalation, specifically according to pathogen species, and the
optimal duration of therapy. Investigators should be actively
encouraged to pursue these lines of investigation in the future.
Acknowledgments
Supplement sponsorship. This article was published as part of a sup-plement entitled “Health Care–Associated Infection (HAI): A Critical Ap-praisal of the Emerging Threat—Proceedings of the HAI Summit,” sponsoredby Medical Education Resources and Consensus Medical Communicationsand supported by an unrestricted educational grant from Ortho-McNeil, Inc.,administered by Ortho-McNeil Janssen Scientific Affairs, LLC.
Potential conflicts of interest. M.H.K. has received grants/researchsupport from Pfizer, Merck, and Bard. V.G.F. has received grants/researchsupport from Cubist, Theravance, Merck, and Nubi Inhibitex; has been aconsultant for Astellas, Cubist, Biosynexur, Theravance, Merck, and John-son & Johnson; and has been a speakers’ bureau participant for Cubistand Pfizer. S.T.M. has received grants/research support from Pfizer,AstraZeneca, Astellas, and Ortho-McNeil. J.J.R. has been a consultant forWyeth and Ortho-McNeil and has been a speakers’ bureau participant forWyeth and Ortho-McNeil. A.F.S. has received grants/research support formAstellas, GlaxoSmithKline, Johnson & Johnson, Pfizer, and Sanofi; has beena consultant for Astellas, GlaxoSmithKline, Johnson & Johnson, Pfizer, andSanofi; and has been a speakers’ bureau participant for Astellas, Glaxo-SmithKline, Johnson & Johnson, Pfizer, Sanofi, and Merck. J.S.S. has re-ceived grants/research support from Pfizer and has been a consultant forJohnson & Johnson, Roche, Novartis, Schering-Plough, and Bayer. D.L.S.has received grants/research support from Pfizer, Arpida, Cubist, andRoche. All other authors: no conflicts.
References
1. American Thoracic Society, Infectious Diseases Society of America.Guidelines for the management of adults with hospital-acquired, ven-tilator-associated, and healthcare-associated pneumonia. Am J RespirCrit Care Med 2005; 171:388–416. Available at: http://www.thoracic.org/sections/publications/statements/pages/mtpi/guide1-29.html.Accessed 26 December 2007.
2. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious DiseasesSociety of America/American Thoracic Society consensus guidelineson the management of community-acquired pneumonia in adults.Clin Infect Dis 2007; 44(Suppl 2):S27–72.
3. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate antimicrobialtreatment of infections: a risk factor for hospital mortality amongcritically ill patients. Chest 1999; 115:462–74.
4. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension beforeinitiation of effective antimicrobial therapy is the critical determinantof survival in human septic shock. Crit Care Med 2006; 34:1589–96.
5. Schramm GE, Johnson JA, Doherty JA, Micek ST, Kollef MH. Meth-icillin-resistant Staphylococcus aureus sterile-site infection: the im-portance of appropriate initial antimicrobial treatment. Crit Care Med2006; 34:2069–74.
6. Friedman ND, Kaye KS, Stout JE, et al. Health care–associated blood-stream infections in adults: a reason to change the accepted definitionof community-acquired infections. Ann Intern Med 2002; 137:791–7.
7. Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Ep-idemiology and outcomes of health-care–associated pneumonia: re-sults from a large US database of culture-positive pneumonia. Chest2005; 128:3854–62.
8. Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health
care-associated pneumonia and community-acquired pneumonia: asingle-center experience. Antimicrob Agents Chemother 2007; 51:3568–73.
9. Gaynes R, Edwards JR. Overview of nosocomial infections caused bygram-negative bacilli. Clin Infect Dis 2005; 41:848–54.
10. Micek ST, Roubinian N, Heuring T, et al. Before-after study of astandardized hospital order set for the management of septic shock.Crit Care Med 2006; 34:2707–13.
11. US Department of Health and Human Services, Food and Drug Ad-ministration, Center for Drug Evaluation and Research. Guidance forindustry: uncomplicated and complicated skin and skin structure in-fections—developing antimicrobial drugs for treatment. Draft guid-ance. July 1998. Available at: http://www.fda.gov/ohrms/dockets/98fr/2566dft.pdf. Accessed 2 January 2007.
12. Gravel D, Taylor G, Ofner M, et al. Point prevalence survey for health-care-associated infections within Canadian adult acute-care hospitals.J Hosp Infect 2007; 66:243–8.
13. Jones RN, ed. Global aspects of antimicrobial resistance among keybacterial pathogens: results from the 1997–1999 SENTRY Antimicro-bial Program. Clin Infect Dis 2001; 32(Suppl 2):S81–167.
14. Moet GJ, Jones RN, Biedenbach DJ, Stilwell MG, Fritsche TR. Con-temporary causes of skin and soft tissue infections in North America,Latin America, and Europe: report from the SENTRY AntimicrobialSurveillance Program (1998–2004). Diagn Microbiol Infect Dis2007; 57:7–13.
15. Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of com-munity- and health care–associated methicillin-resistant Staphylococ-cus aureus infection. JAMA 2003; 290:2976–84.
16. Frazee BW, Lynn J, Charlebois ED, Lambert L, Lowery D, Perdreau-Remington F. High prevalence of methicillin-resistant Staphylococcusaureus in emergency department skin and soft tissue infections. AnnEmerg Med 2005; 45:311–20.
17. Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistantStaphylococcus aureus disease in three communities. N Engl J Med2005; 352:1436–44.
18. Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S.aureus infections among patients in the emergency department. NEngl J Med 2006; 355:666–74.
19. Weber JT. Community-associated methicillin-resistant Staphylococcusaureus. Clin Infect Dis 2005; 41(Suppl 4):S269–72.
20. King MD, Humphrey BJ, Wang YF, Kourbatova EV, Ray SM, Blum-berg HM. Emergence of community-acquired methicillin-resistantStaphylococcus aureus USA 300 clone as the predominant cause ofskin and soft-tissue infections. Ann Intern Med 2006; 144:309–17.
21. Arbeit RD, Maki D, Tally FP, Campanaro E, Eisenstein BI. The safetyand efficacy of daptomycin for the treatment of complicated skin andskin-structure infections. Clin Infect Dis 2004; 38:1673–81.
22. Jauregui LE, Babazadeh S, Seltzer E, et al. Randomized, double-blindcomparison of once-weekly dalbavancin versus twice-daily linezolidtherapy for the treatment of complicated skin and skin structureinfections. Clin Infect Dis 2005; 41:1407–15.
23. Ellis-Grosse EJ, Babinchak T, Dartois N, Rose G, Loh E. The efficacyand safety of tigecycline in the treatment of skin and skin-structureinfections: results of 2 double-blind phase 3 comparison studies withvancomycin-aztreonam. Clin Infect Dis 2005; 41(Suppl 5):S341–53.
24. Stryjewski ME, Chu VH, O’Riordan WD, et al. Telavancin versusstandard therapy for treatment of complicated skin and skin structureinfections caused by gram-positive bacteria: FAST 2 study. AntimicrobAgents Chemother 2006; 50:862–7.
25. Stryjewski ME, O’Riordan WD, Lau WK, et al. Telavancin versusstandard therapy for treatment of complicated skin and soft-tissueinfections due to gram-positive bacteria. Clin Infect Dis 2005; 40:1601–7.
26. Corey R, Stryjewski M, O’Riordan W, et al. Telavancin for the treat-ment of complicated skin and skin structure infections (cSSSI): resultsof the ATLAS I study [poster LB-17]. In: Program and abstracts ofthe 44th Annual Meeting of the Infectious Diseases Society of America
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S95
(Toronto). Alexandria, VA: Infectious Diseases Society of America,2006:239.
27. Noel GJ, Strauss RS, Amsler K, Heep M, Pypstra R, Solomkin JS.Results of a double-blind, randomized trial of ceftobiprole treatmentof complicated skin and skin structure infections caused by gram-positive bacteria. Antimicrob Agents Chemother 2008; 52:37–44.
28. Strauss RS, Amsler K, Vazquez JA, Jacobs MR, Noel GJ, Bush K.Microbiological eradication of gram-positive and gram-negative bac-teria with ceftobiprole (BPR) in complicated skin and skin structureinfections (cSSSI) [presentation L-1143, poster 409]. In: Program andabstracts of the 47th Interscience Conference on Antimicrobial Agentsand Chemotherapy (Chicago). Washington, DC: American Society forMicrobiology, 2007.
29. Anderson DJ, Sexton DJ, Kanafani ZA, Auten G, Kaye KS. Severesurgical site infection in community hospitals: epidemiology, key pro-cedures, and the changing prevalence of methicillin-resistant Staph-ylococcus aureus. Infect Control Hosp Epidemiol 2007; 28:1047–53.
30. Kaye KS, Engemann JJ, Mozaffari E, Carmeli Y. Reference groupchoice and antibiotic resistance outcomes. Emerg Infect Dis 2004; 10:1125–8.
31. Patel M, Kumar RA, Stamm AM, Hoesley CJ, Moser SA, Waites KB.USA300 genotype community-associated methicillin-resistant Staph-ylococcus aureus as a cause of surgical site infections. J Clin Microbiol2007; 45:3431–3.
32. Lipsky BA, Itani K, Norden C. Treating foot infections in diabeticpatients: a randomized, multicenter, open-label trial of linezolid versusampicillin-sulbactam/amoxicillin-clavulanate. Clin Infect Dis 2004;38:17–24.
33. Lipsky BA, Armstrong DG, Citron DM, Tice AD, Morgenstern DE,Abramson MA. Ertapenem versus piperacillin/tazobactam for diabeticfoot infections (SIDESTEP): prospective, randomised, controlled,double-blinded, multicentre trial. Lancet 2005; 366:1695–703.
34. Lipsky BA, Berendt AR, Deery HG, et al. Diagnosis and treatment ofdiabetic foot infections. Clin Infect Dis 2004; 39:885–910.
35. Gonzalez BE, Rueda AM, Shelburne SA III, Musher DM, Hamill RJ,Hulten KG. Community-associated strains of methicillin-resistantStaphylococccus aureus as the cause of healthcare-associated infection.Infect Control Hosp Epidemiol 2006; 27:1051–6.
36. Kourbatova EV, Halvosa JS, King MD, Ray SM, White N, BlumbergHM. Emergence of community-associated methicillin-resistant Staph-ylococcus aureus USA 300 clone as a cause of health care-associatedinfections among patients with prosthetic joint infections. Am J InfectControl 2005; 33:385–91.
37. Saiman L, O’Keefe M, Graham PL III, et al. Hospital transmission ofcommunity-acquired methicillin-resistant Staphylococcus aureusamong postpartum women. Clin Infect Dis 2003; 37:1313–9.
38. Zaoutis TE, Toltzis P, Chu J, et al. Clinical and molecular epidemiologyof community-acquired methicillin-resistant Staphylococcus aureus in-fections among children with risk factors for health care-associatedinfection: 2001–2003. Pediatr Infect Dis J 2006; 25:343–8.
39. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resis-tant Staphylococcus aureus infections in the United States. JAMA2007; 298:1763–71.
40. Solomkin JS, Mazuski JE, Baron EJ, et al. Guidelines for the selectionof anti-infective agents for complicated intra-abdominal infections.Clin Infect Dis 2003; 37:997–1005.
41. Pacelli F, Doglietto GB, Alfieri S, et al. Prognosis in intra-abdominalinfections: multivariate analysis on 604 patients. Arch Surg 1996; 131:641–5.
42. Solomkin JS, Hemsell DL, Sweet R, Tally F, Bartlett J. Evaluation ofnew anti-infective drugs for the treatment of intraabdominal infec-tions. Infectious Diseases Society of America and the Food and DrugAdministration. Clin Infect Dis 1992; 15(Suppl 1):S33–42.
43. Krobot K, Yin D, Zhang Q, et al. Effect of inappropriate initial empiricantibiotic therapy on outcome of patients with community-acquiredintra-abdominal infections requiring surgery. Eur J Clin MicrobiolInfect Dis 2004; 23:682–7.
44. Tellado JM, Sen SS, Caloto MT, Kumar RN, Nocea G. Consequencesof inappropriate initial empiric parenteral antibiotic therapy amongpatients with community-acquired intra-abdominal infections inSpain. Scand J Infect Dis 2007; 39:947–55.
45. Bare M, Castells X, Garcia A, Riu M, Comas M, Egea MJ. Importanceof appropriateness of empiric antibiotic therapy on clinical outcomesin intra-abdominal infections. Int J Technol Assess Health Care2006; 22:242–8.
46. Fraser A, Paul M, Almanasreh N, et al. Benefit of appropriate empiricalantibiotic treatment: thirty-day mortality and duration of hospitalstay. Am J Med 2006; 119:970–6.
47. Sturkenboom MC, Goettsch WG, Picelli G, et al. Inappropriate initialtreatment of secondary intra-abdominal infections leads to increasedrisk of clinical failure and costs. Br J Clin Pharmacol 2005; 60:438–43.
48. Mazuski JE, Sawyer RG, Nathens AB, et al. The Surgical InfectionSociety guidelines on antimicrobial therapy for intra-abdominal in-fections: an executive summary. Surg Infect (Larchmt) 2002; 3:161–73.
49. Barie PS, Vogel SB, Dellinger EP, et al. A randomized, double-blindclinical trial comparing cefepime plus metronidazole with imipenem-cilastatin in the treatment of complicated intra-abdominal infections.Cefepime Intra-abdominal Infection Study Group. Arch Surg 1997;132:1294–302.
50. Christou NV, Turgeon P, Wassef R, Rotstein O, Bohnen J, Potvin M.Management of intra-abdominal infections: the case for intraoperativecultures and comprehensive broad-spectrum antibiotic coverage. TheCanadian Intra-abdominal Infection Study Group. Arch Surg 1996;131:1193–201.
51. Hopkins JA, Lee JC, Wilson SE. Susceptibility of intra-abdominalisolates at operation: a predictor of postoperative infection. Am Surg1993; 59:791–6.
52. Montravers P, Gauzit R, Muller C, Marmuse JP, Fichelle A, DesmontsJM. Emergence of antibiotic-resistant bacteria in cases of peritonitisafter intraabdominal surgery affects the efficacy of empirical anti-microbial therapy. Clin Infect Dis 1996; 23:486–94.
53. Roehrborn A, Thomas L, Potreck O, et al. The microbiology of post-operative peritonitis. Clin Infect Dis 2001; 33:1513–9.
54. Study Monitoring Antimicrobial Resistance Trends (SMART). Avail-able at: http://www.merck.com/mrl/studies/smart.html. Accessed 20May 2008.
55. Rossi F, Baquero F, Hsueh PR, et al. In vitro susceptibilities of aerobicand facultatively anaerobic gram-negative bacilli isolated from pa-tients with intra-abdominal infections worldwide: 2004 results fromSMART (Study for Monitoring Antimicrobial Resistance Trends). JAntimicrob Chemother 2006; 58:205–10.
56. Bochicchio GV, Baquero F, Hsueh PR, et al. In vitro susceptibilitiesof Escherichia coli isolated from patients with intra-abdominal infec-tions worldwide in 2002–2004: results from SMART (Study for Mon-itoring Antimicrobial Resistance Trends). Surg Infect (Larchmt)2006; 7:537–45.
57. Peralta G, Sanchez MB, Garrido JC, et al. Impact of antibiotic resis-tance and of adequate empirical antibiotic treatment in the prognosisof patients with Escherichia coli bacteraemia. J Antimicrob Chemother2007; 60:855–63.
58. Seguin P, Laviolle B, Chanavaz C, et al. Factors associated with mul-tidrug-resistant bacteria in secondary peritonitis: impact on antibiotictherapy. Clin Microbiol Infect 2006; 12:980–5.
59. Naughton BJ, Mylotte JM, Ramadan F, Karuza J, Priore RL. Antibioticuse, hospital admissions, and mortality before and after implementingguidelines for nursing home–acquired pneumonia. J Am Geriatr Soc2001; 49:1020–4.
60. Carratala J, Mykietiuk A, Fernandez-Sabe N, et al. Healthcare–associated pneumonia requiring hospital admission: epidemi-ology, antibiotic therapy, and clinical outcomes. Arch Intern Med2007; 167:1393–9.
61. Ibrahim EH, Ward S, Sherman G, Schaiff R, Fraser VJ, Kollef MH.Experience with a clinical guideline for the treatment of ventilator-associated pneumonia. Crit Care Med 2001; 29:1109–15.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from
S96 • CID 2008:47 (Suppl 2) • Kollef et al.
62. Soo Hoo GW, Wen YE, Nguyen TV, Goetz MB. Impact of clinicalguidelines in the management of severe hospital-acquired pneumonia.Chest 2005; 128:2778–87.
63. Arancibia F, Bauer TT, Ewig S, et al. Community-acquired pneumoniadue to gram-negative bacteria and Pseudomonas aeruginosa: incidence,risk, and prognosis. Arch Intern Med 2002; 162:1849–58.
64. Jeffres MN, Isakow W, Doherty JA, et al. Predictors of mortality formethicillin-resistant Staphylococcus aureus health-care–associatedpneumonia: specific evaluation of vancomycin pharmacokinetic in-dices. Chest 2006; 130:947–55.
65. Jeffres MN, Isakow W, Doherty JA, Micek ST, Kollef MH. A retro-spective analysis of possible renal toxicity associated with vancomycinin patients with health care–associated methicillin-resistant Staphy-lococcus aureus pneumonia. Clin Ther 2007; 29:1107–15.
66. Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG. Timing of an-tibiotic administration and outcomes for Medicare patients hospi-talized with community-acquired pneumonia. Arch Intern Med2004; 164:637–44.
67. Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process,and outcomes in elderly patients with pneumonia. JAMA 1997; 278:2080–4.
68. Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensityof implementing pneumonia guidelines: a randomized, controlledtrial. Ann Intern Med 2005; 143:881–94.
69. Baker A, Meredith J, Chang M, Dunagan D, Smith A, Haponik E.Bronchoscopically guided management of ventilator-associated pneu-monia in trauma patients. J Bronchol 2003; 10:7–16.
70. Iregui M, Ward S, Sherman G, Fraser VJ, Kollef MH. Clinical im-portance of delays in the initiation of appropriate antibiotic treatmentfor ventilator-associated pneumonia. Chest 2002; 122:262–8.
71. Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-courseempiric antibiotic therapy for patients with pulmonary infiltrates inthe intensive care unit: a proposed solution for indiscriminate anti-biotic prescription. Am J Respir Crit Care Med 2000; 162:505–11.
72. Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days ofantibiotic therapy for ventilator-associated pneumonia in adults: arandomized trial. JAMA 2003; 290:2588–98.
73. Fagon JY, Chastre J, Wolff M, et al. Invasive and noninvasive strategiesfor management of suspected ventilator-associated pneumonia: a ran-domized trial. Ann Intern Med 2000; 132:621–30.
74. Wunderink RG. Nosocomial pneumonia, including ventilator-asso-ciated pneumonia. Proc Am Thorac Soc 2005; 2:440–4.
75. McDonald JR, Friedman ND, Stout JE, Sexton DJ, Kaye KS. Riskfactors for ineffective therapy in patients with bloodstream infection.Arch Intern Med 2005; 165:308–13.
76. McGregor JC, Rich SE, Harris AD, et al. A systematic review of themethods used to assess the association between appropriate antibiotictherapy and mortality in bacteremic patients. Clin Infect Dis 2007;45:329–37.
77. Schwaber MJ, Carmeli Y. Mortality and delay in effective therapyassociated with extended-spectrum b-lactamase production in Enter-obacteriaceae bacteraemia: a systematic review and meta-analysis. JAntimicrob Chemother 2007; 60:913–20.
78. Anderson DJ, Engemann JJ, Harrell LJ, Carmeli Y, Reller LB, KayeKS. Predictors of mortality in patients with bloodstream infection dueto ceftazidime-resistant Klebsiella pneumoniae. Antimicrob AgentsChemother 2006; 50:1715–20.
79. Deal EN, Micek ST, Ritchie DJ, Reichley RM, Dunne WM Jr, KollefMH. Predictors of in-hospital mortality for bloodstream infectionscaused by Enterobacter species or Citrobacter freundii. Pharmaco-therapy 2007; 27:191–9.
80. Hyle EP, Lipworth AD, Zaoutis TE, Nachamkin I, Bilker WB, Lau-tenbach E. Impact of inadequate initial antimicrobial therapy on mor-tality in infections due to extended-spectrum b-lactamase–producingEnterobacteriaceae: variability by site of infection. Arch Intern Med2005; 165:1375–80.
81. Lodise TP Jr, Patel N, Kwa A, et al. Predictors of 30-day mortalityamong patients with Pseudomonas aeruginosa bloodstream infections:impact of delayed appropriate antibiotic selection. Antimicrob AgentsChemother 2007; 51:3510–5.
82. Micek ST, Lloyd AE, Ritchie DJ, Reichley RM, Fraser VJ, Kollef MH.Pseudomonas aeruginosa bloodstream infection: importance of ap-propriate initial antimicrobial treatment. Antimicrob Agents Che-mother 2005; 49:1306–11.
83. Osih RB, McGregor JC, Rich SE, et al. Impact of empiric antibiotictherapy on outcomes in patients with Pseudomonas aeruginosa bac-teremia. Antimicrob Agents Chemother 2007; 51:839–44.
84. Tumbarello M, Sanguinetti M, Montuori E, et al. Predictors of mor-tality in patients with bloodstream infections caused by extended-spectrum-b-lactamase-producing Enterobacteriaceae: importance ofinadequate initial antimicrobial treatment. Antimicrob Agents Che-mother 2007; 51:1987–94.
85. Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, KarchmerAW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia:a meta-analysis. Clin Infect Dis 2003; 36:53–9.
86. Whitby M, McLaws ML, Berry G. Risk of death from methicillin-resistant Staphylococcus aureus bacteraemia: a meta-analysis. Med JAust 2001; 175:264–7.
87. Khatib R, Saeed S, Sharma M, Riederer K, Fakih MG, Johnson LB.Impact of initial antibiotic choice and delayed appropriate treatmenton the outcome of Staphylococcus aureus bacteremia. Eur J Clin Mi-crobiol Infect Dis 2006; 25:181–5.
88. Kim SH, Park WB, Lee CS, et al. Outcome of inappropriate empiricalantibiotic therapy in patients with Staphylococcus aureus bacteraemia:analytical strategy using propensity scores. Clin Microbiol Infect2006; 12:13–21.
89. Lodise TP, McKinnon PS, Swiderski L, Rybak MJ. Outcomes analysisof delayed antibiotic treatment for hospital-acquired Staphylococcusaureus bacteremia. Clin Infect Dis 2003; 36:1418–23.
90. Roghmann MC. Predicting methicillin resistance and the effect ofinadequate empiric therapy on survival in patients with Staphylococcusaureus bacteremia. Arch Intern Med 2000; 160:1001–4.
91. Garey KW, Rege M, Pai MP, et al. Time to initiation of fluconazoletherapy impacts mortality in patients with candidemia: a multi-in-stitutional study. Clin Infect Dis 2006; 43:25–31.
92. Morrell M, Fraser VJ, Kollef MH. Delaying the empiric treatment ofCandida bloodstream infection until positive blood culture results areobtained: a potential risk factor for hospital mortality. AntimicrobAgents Chemother 2005; 49:3640–5.
93. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology ofsepsis in the United States from 1979 through 2000. N Engl J Med2003; 348:1546–54.
94. Spellberg B, Guidos R, Gilbert D, et al. The epidemic of antibiotic-resistant infections: a call to action for the medical community fromthe Infectious Diseases Society of America. Clin Infect Dis 2008; 46:155–64.
95. Mohr JF, Murray BE. Point: vancomycin is not obsolete for the treat-ment of infection caused by methicillin-resistant Staphylococcus au-reus. Clin Infect Dis 2007; 44:1536–42.
96. Deresinski S. Counterpoint: vancomycin and Staphylococcus aureus—an antibiotic enters obsolescence. Clin Infect Dis 2007; 44:1543–8.
97. Russell JA. Management of sepsis. N Engl J Med 2006; 355:1699–713.98. Balk RA. Optimum treatment of severe sepsis and septic shock: evi-
dence in support of the recommendations. Dis Mon 2004; 50:168–213.99. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J,
Pinsky MR. Epidemiology of severe sepsis in the United States: analysisof incidence, outcome, and associated costs of care. Crit Care Med2001; 29:1303–10.
100. Bochud PY, Bonten M, Marchetti O, Calandra T. Antimicrobial ther-apy for patients with severe sepsis and septic shock: an evidence-basedreview. Crit Care Med 2004; 32(Suppl 11):S495–512.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S97
101. Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaignguidelines for management of severe sepsis and septic shock. CritCare Med 2004; 32:858–73.
102. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign:international guidelines for management of severe sepsis and septicshock: 2008. Crit Care Med 2008; 36:296–327.
103. Balk RA. Severe sepsis and septic shock: definitions, epidemiology,and clinical manifestations. Crit Care Clin 2000; 16:179–92.
104. Marshall JC, Maier RV, Jimenez M, Dellinger EP. Source control inthe management of severe sepsis and septic shock: an evidence-basedreview. Crit Care Med 2004; 32(Suppl 11):S513–26.
105. Bochud PY, Glauser MP, Calandra T. Antibiotics in sepsis. IntensiveCare Med 2001; 27(Suppl 1):S33–48.
106. Engel C, Brunkhorst FM, Bone HG, et al. Epidemiology of sepsis inGermany: results from a national prospective multicenter study. In-tensive Care Med 2007; 33:606–18.
107. Vincent JL, Sakr Y, Sprung CL, et al. Sepsis in European intensivecare units: results of the SOAP study. Crit Care Med 2006; 34:344–53.
108. Kreger BE, Craven DE, Carling PC, McCabe WR. Gram-negativebacteremia. III. Reassessment of etiology, epidemiology and ecologyin 612 patients. Am J Med 1980; 68:332–43.
109. Fish DN. Optimal antimicrobial therapy for sepsis. Am J Health SystPharm 2002; 59(Suppl 1):S13–9.
110. Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A,Jimenez-Jimenez FJ, Perez-Paredes C, Ortiz-Leyba C. Impact of ad-equate empirical antibiotic therapy on the outcome of patients ad-mitted to the intensive care unit with sepsis. Crit Care Med 2003;31:2742–51.
111. Leibovici L, Shraga I, Drucker M, Konigsberger H, Samra Z, PitlikSD. The benefit of appropriate empirical antibiotic treatment in pa-tients with bloodstream infection. J Intern Med 1998; 244:379–86.
112. Weinstein MP, Towns ML, Quartey SM, et al. The clinical significanceof positive blood cultures in the 1990s: a prospective comprehensiveevaluation of the microbiology, epidemiology, and outcome of bac-teremia and fungemia in adults. Clin Infect Dis 1997; 24:584–602.
113. Rodriguez A, Rello J, Neira J, et al. Effects of high-dose of intravenousimmunoglobulin and antibiotics on survival for severe sepsis under-going surgery. Shock 2005; 23:298–304.
114. Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of re-combinant human activated protein C for severe sepsis. N Engl J Med2001; 344:699–709.
115. Dhainaut JF, Laterre PF, LaRosa SP, et al. The clinical evaluationcommittee in a large multicenter phase 3 trial of drotrecogin alfa(activated) in patients with severe sepsis (PROWESS): role, meth-odology, and results. Crit Care Med 2003; 31:2291–301.
116. Annane D, Vignon P, Renault A, et al. Norepinephrine plus dobu-tamine versus epinephrine alone for management of septic shock: arandomised trial. Lancet 2007; 370:676–84.
117. Opal S, Laterre PF, Abraham E, et al. Recombinant human platelet-activating factor acetylhydrolase for treatment of severe sepsis: resultsof a phase III, multicenter, randomized, double-blind, placebo-con-trolled, clinical trial. Crit Care Med 2004; 32:332–41.
118. Nguyen HB, Corbett SW, Steele R, et al. Implementation of a bundleof quality indicators for the early management of severe sepsis andseptic shock is associated with decreased mortality. Crit Care Med2007; 35:1105–12.
119. Barie PS, Williams MD, McCollam JS, et al. Benefit/risk profile ofdrotrecogin alfa (activated) in surgical patients with severe sepsis. AmJ Surg 2004; 188:212–20.
120. Clec’h C, Fosse JP, Karoubi P, et al. Differential diagnostic value ofprocalcitonin in surgical and medical patients with septic shock. CritCare Med 2006; 34:102–7.
121. Gibot S, Cravoisy A, Levy B, Bene MC, Faure G, Bollaert PE. Solubletriggering receptor expressed on myeloid cells and the diagnosis ofpneumonia. N Engl J Med 2004; 350:451–8.
122. Tenover FC. Rapid detection and identification of bacterial pathogens
using novel molecular technologies: infection control and beyond.Clin Infect Dis 2007; 44:418–23.
123. Centers for Disease Control and Prevention. About VISA/VRSA.Available at: http://www.cdc.gov/ncidod/dhqp/ar_visavrsa_FAQ.html.Accessed 9 October 2007.
124. Kapadia M, Coyle E, Prince R, Rolston KVI. Declining in vitro activityof vancomycin against Staphylococcus aureus isolates from cancer pa-tients [poster E-807]. In: Program and abstracts of the 45th Inter-science Conference on Antimicrobial Agents and Chemotherapy(Washington, DC). Washington, DC: American Society for Micro-biology, 2005:44.
125. Golan Y, Baez-Giangreco C, O’Sullivan C, Snydman DR. Trends invancomycin (vanco) susceptibility (S) among consecutive MRSA bac-teremic isolates [poster LB-11]. In: Program and abstracts of the 44thAnnual Meeting of the Infectious Diseases Society of America (To-ronto). Alexandria, VA: Infectious Diseases Society of America, 2006:238.
126. Wang G, Hindler JF, Ward KW, Bruckner DA. Increased vancomycinMICs for Staphylococcus aureus clinical isolates from a university hos-pital during a 5-year period. J Clin Microbiol 2006; 44:3883–6.
127. Tenover FC, Moellering RC Jr. The rationale for revising the Clinicaland Laboratory Standards Institute vancomycin minimal inhibitoryconcentration interpretive criteria for Staphylococcus aureus. Clin In-fect Dis 2007; 44:1208–15.
128. Centers for Disease Control and Prevention. Vancomycin-resistantStaphylococcus aureus—New York, 2004. MMWR Morb Mortal WklyRep 2004; 53:322–3.
129. Sievert DM, Rudrik JT, Patel JB, McDonald LC, Wilkins MJ, HagemanJC. Vancomycin-resistant Staphylococcus aureus in the United States,2002–2006. Clin Infect Dis 2008; 46:668–74.
130. Hiramatsu K, Hanaki H, Ino T, Yabuta K, Oguri T, Tenover FC.Methicillin-resistant Staphylococcus aureus clinical strain with reducedvancomycin susceptibility. J Antimicrob Chemother 1997; 40:135–6.
131. Linares J. The VISA/GISA problem: therapeutic implications. ClinMicrobiol Infect 2001; 7(Suppl 4):8–15.
132. Howden BP, Ward PB, Charles PG, et al. Treatment outcomes forserious infections caused by methicillin-resistant Staphylococcus aureuswith reduced vancomycin susceptibility. Clin Infect Dis 2004; 38:521–8.
133. Charles PG, Ward PB, Johnson PD, Howden BP, Grayson ML. Clinicalfeatures associated with bacteremia due to heterogeneous vancomy-cin-intermediate Staphylococcus aureus. Clin Infect Dis 2004; 38:448–51.
134. Moise-Broder PA, Sakoulas G, Eliopoulos GM, Schentag JJ, ForrestA, Moellering RC Jr. Accessory gene regulator group II polymorphismin methicillin-resistant Staphylococcus aureus is predictive of failureof vancomycin therapy. Clin Infect Dis 2004; 38:1700–5.
135. Sakoulas G, Moise-Broder PA, Schentag J, Forrest A, Moellering RCJr, Eliopoulos GM. Relationship of MIC and bactericidal activity toefficacy of vancomycin for treatment of methicillin-resistant Staph-ylococcus aureus bacteremia. J Clin Microbiol 2004; 42:2398–402.
136. Sader HS, Fritsche TR, Jones RN. Daptomycin bactericidal activityand correlation between disk and broth microdilution method resultsin testing of Staphylococcus aureus strains with decreased susceptibilityto vancomycin. Antimicrob Agents Chemother 2006; 50:2330–6.
137. Hidayat LK, Hsu DI, Quist R, Shriner KA, Wong-Beringer A. High-dose vancomycin therapy for methicillin-resistant Staphylococcus au-reus infections: efficacy and toxicity. Arch Intern Med 2006; 166:2138–44.
138. Craig W, Andes D. In vivo pharmacodynamics of vancomycin againstVISA, heteroresistant VISA (hVISA) and VSSA in the neutropenicmurine thigh-infection model [abstract A-644]. In: Program and ab-stracts of the 46th Interscience Conference on Antimicrobial Agentsand Chemotherapy (San Francisco). Washington, DC: American So-ciety for Microbiology, 2006.
139. Luna CM, Vujacich P, Niederman MS, et al. Impact of BAL data on
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

S98 • CID 2008:47 (Suppl 2) • Kollef et al.
the therapy and outcome of ventilator-associated pneumonia. Chest1997; 111:676–85.
140. Kollef MH, Ward S. The influence of mini-BAL cultures on patientoutcomes: implications for the antibiotic management of ventilator-associated pneumonia. Chest 1998; 113:412–20.
141. Kang CI, Kim SH, Park WB, et al. Bloodstream infections caused byantibiotic-resistant gram-negative bacilli: risk factors for mortality andimpact of inappropriate initial antimicrobial therapy on outcome.Antimicrob Agents Chemother 2005; 49:760–6.
142. Chamot E, Boffi El Amari E, Rohner P, Van Delden C. Effectivenessof combination antimicrobial therapy for Pseudomonas aeruginosabacteremia. Antimicrob Agents Chemother 2003; 47:2756–64.
143. Korvick JA, Bryan CS, Farber B, et al. Prospective observational studyof Klebsiella bacteremia in 230 patients: outcome for antibiotic com-binations versus monotherapy. Antimicrob Agents Chemother1992; 36:2639–44.
144. Safdar N, Handelsman J, Maki DG. Does combination antimicrobialtherapy reduce mortality in gram-negative bacteraemia? A meta-anal-ysis. Lancet Infect Dis 2004; 4:519–27.
145. Bratu S, Tolaney P, Karumudi U, et al. Carbapenemase-producingKlebsiella pneumoniae in Brooklyn, NY: molecular epidemiology andin vitro activity of polymyxin B and other agents. J Antimicrob Che-mother 2005; 56:128–32.
146. Motaouakkil S, Charra B, Hachimi A, et al. Colistin and rifampicinin the treatment of nosocomial infections from multiresistant Aci-netobacter baumannii. J Infect 2006; 53:274–8.
147. Yoon J, Urban C, Terzian C, Mariano N, Rahal JJ. In vitro doubleand triple synergistic activities of polymyxin B, imipenem, and rif-ampin against multidrug-resistant Acinetobacter baumannii. Antimi-crob Agents Chemother 2004; 48:753–7.
148. Drusano GL, Ambrose PG, Bhavnani SM, Bertino JS, Nafziger AN,Louie A. Back to the future: using aminoglycosides again and howto dose them optimally. Clin Infect Dis 2007; 45:753–60.
149. Neuhauser MM, Weinstein RA, Rydman R, Danziger LH, Karam G,Quinn JP. Antibiotic resistance among gram-negative bacilli in USintensive care units: implications for fluoroquinolone use. JAMA2003; 289:885–8.
150. Gasink LB, Fishman NO, Weiner MG, Nachamkin I, Bilker WB, Lau-tenbach E. Fluoroquinolone-resistant Pseudomonas aeruginosa: as-sessment of risk factors and clinical impact. Am J Med 2006; 119:526.e19–25.
151. Polk RE, Johnson CK, McClish D, Wenzel RP, Edmond MB. Predictinghospital rates of fluoroquinolone-resistant Pseudomonas aeruginosafrom fluoroquinolone use in US hospitals and their surrounding com-munities. Clin Infect Dis 2004; 39:497–503.
152. Friedland I, Gallagher G, King T, Woods GL. Antimicrobial suscep-tibility patterns in Pseudomonas aeruginosa: data from a multicenterIntensive Care Unit Surveillance Study (ISS) in the United States. JChemother 2004; 16:437–41.
153. Karlowsky JA, Draghi DC, Jones ME, Thornsberry C, Friedland IR,Sahm DF. Surveillance for antimicrobial susceptibility among clinicalisolates of Pseudomonas aeruginosa and Acinetobacter baumannii fromhospitalized patients in the United States, 1998 to 2001. AntimicrobAgents Chemother 2003; 47:1681–8.
154. Manikal VM, Landman D, Saurina G, Oydna E, Lal H, Quale J.Endemic carbapenem-resistant Acinetobacter species in Brooklyn, NewYork: citywide prevalence, interinstitutional spread, and relation toantibiotic usage. Clin Infect Dis 2000; 31:101–6.
155. Blot S, Depuydt P, Vogelaers D, et al. Colonization status and ap-propriate antibiotic therapy for nosocomial bacteremia caused by an-tibiotic-resistant gram-negative bacteria in an intensive care unit. In-fect Control Hosp Epidemiol 2005; 26:575–9.
156. Tam VH, Gamez EA, Weston JS, et al. Outcomes of bacteremia dueto Pseudomonas aeruginosa with reduced susceptibility to piperacillin-tazobactam: implications on the appropriateness of the resistancebreakpoint. Clin Infect Dis 2008; 46:862–7.
157. Livermore DM, Pearson A. Antibiotic resistance: location, location,location. Clin Microbiol Infect 2007; 13(Suppl 2):7–16.
158. Bennett JE. Echinocandins for candidemia in adults without neutro-penia. N Engl J Med 2006; 355:1154–9.
159. Pappas PG. Invasive candidiasis. Infect Dis Clin North Am 2006; 20:485–506.
160. Shorr AF, Tabak YP, Killian AD, Gupta V, Liu LZ, Kollef MH. Health-care-associated bloodstream infection: a distinct entity? Insights froma large U.S. database. Crit Care Med 2006; 34:2588–95.
161. Sofair AN, Lyon GM, Huie-White S, et al. Epidemiology of com-munity-onset candidemia in Connecticut and Maryland. Clin InfectDis 2006; 43:32–9.
162. Shorr AF, Micek ST, Jackson WL Jr, Kollef MH. Economic implica-tions of an evidence-based sepsis protocol: can we improve outcomesand lower costs? Crit Care Med 2007; 35:1257–62.
163. Leon C, Ruiz-Santana S, Saavedra P, et al. A bedside scoring system(“Candida score”) for early antifungal treatment in nonneutropeniccritically ill patients with Candida colonization. Crit Care Med2006; 34:730–7.
164. Piarroux R, Grenouillet F, Balvay P, et al. Assessment of preemptivetreatment to prevent severe candidiasis in critically ill surgical patients.Crit Care Med 2004; 32:2443–9.
165. Kotton CN. Zoonoses in solid-organ and hematopoietic stem celltransplant recipients. Clin Infect Dis 2007; 44:857–66.
166. Centers for Disease Control and Prevention, Infectious Diseases So-ciety of America, American Society of Blood and Marrow Transplan-tation. Guidelines for preventing opportunistic infections among he-matopoietic stem cell transplant recipients. MMWR Recomm Rep2000; 49(RR-10):1–125 (erratum: MMWR Morb Mortal Wkly Rep2004; 53:396).
167. Lamaris GA, Chamilos G, Lewis RE, Safdar A, Raad II, KontoyiannisDP. Scedosporium infection in a tertiary care cancer center: a reviewof 25 cases from 1989–2006. Clin Infect Dis 2006; 43:1580–4.
168. Dimopoulos G, Karabinis A, Samonis G, Falagas ME. Candidemia inimmunocompromised and immunocompetent critically ill patients:a prospective comparative study. Eur J Clin Microbiol Infect Dis2007; 26:377–84.
169. Nseir S, Di Pompeo C, Diarra M, et al. Relationship between im-munosuppression and intensive care unit-acquired multidrug-resis-tant bacteria: a case-control study. Crit Care Med 2007; 35:1318–23.
170. Lucet JC, Chevret S, Durand-Zaleski I, Chastang C, Regnier B. Prev-alence and risk factors for carriage of methicillin-resistant Staphylo-coccus aureus at admission to the intensive care unit: results of amulticenter study. Arch Intern Med 2003; 163:181–8.
171. Furuno JP, McGregor JC, Harris AD, et al. Identifying groups at highrisk for carriage of antibiotic-resistant bacteria. Arch Intern Med2006; 166:580–5.
172. Reddy P, Malczynski M, Obias A, et al. Screening for extended-spec-trum b-lactamase–producing Enterobacteriaceae among high-risk pa-tients and rates of subsequent bacteremia. Clin Infect Dis 2007; 45:846–52.
173. Montecalvo MA, de Lencastre H, Carraher M, et al. Natural historyof colonization with vancomycin-resistant Enterococcus faecium. InfectControl Hosp Epidemiol 1995; 16:680–5.
174. Patel R, Allen SL, Manahan JM, et al. Natural history of vancomycin-resistant enterococcal colonization in liver and kidney transplant re-cipients. Liver Transpl 2001; 7:27–31.
175. Roghmann MC, Qaiyumi S, Schwalbe R, Morris JG Jr. Natural historyof colonization with vancomycin-resistant Enterococcus faecium. InfectControl Hosp Epidemiol 1997; 18:679–80.
176. Kim YJ, Boeckh M, Englund JA. Community respiratory virus infec-tions in immunocompromised patients: hematopoietic stem cell andsolid organ transplant recipients, and individuals with human im-munodeficiency virus infection. Semin Respir Crit Care Med 2007;28:222–42.
177. Lee I, Barton TD. Viral respiratory tract infections in transplant pa-
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from

HAI Summit Critical Appraisal • CID 2008:47 (Suppl 2) • S99
tients: epidemiology, recognition and management. Drugs 2007; 67:1411–27.
178. Vonberg RP, Gastmeier P. Nosocomial aspergillosis in outbreak set-tings. J Hosp Infect 2006; 63:246–54.
179. Donskey CJ. The role of the intestinal tract as a reservoir and sourcefor transmission of nosocomial pathogens. Clin Infect Dis 2004; 39:219–26.
180. Annane D, Aegerter P, Jars-Guincestre MC, Guidet B. Current epi-demiology of septic shock: the CUB-Rea Network. Am J Respir CritCare Med 2003; 168:165–72.
181. Montori VM, Bistrian BR, McMahon MM. Hyperglycemia in acutelyill patients. JAMA 2002; 288:2167–9.
182. Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin in-fusion reduces mortality in patients with diabetes undergoing coro-nary artery bypass grafting. J Thorac Cardiovasc Surg 2003; 125:1007–21.
183. Furnary AP, Zerr KJ, Grunkemeier GL, Starr A. Continuous intra-venous insulin infusion reduces the incidence of deep sternal woundinfection in diabetic patients after cardiac surgical procedures. AnnThorac Surg 1999; 67:352–60.
184. Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulintherapy in the critically ill patients. N Engl J Med 2001; 345:1359–67.
185. Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulintherapy in the medical ICU. N Engl J Med 2006; 354:449–61.
186. Van Cromphaut S, Wilmer A, Van den Berghe G. Management ofsepsis. N Engl J Med 2007; 356:1179–81.
187. Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients:risk factors and outcomes. Crit Care Med 2007; 35:2262–7.
188. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign:international guidelines for management of severe sepsis and septicshock: 2008. Intensive Care Med 2008; 34:17–60.
189. Jones AE, Focht A, Horton JM, Kline JA. Prospective external vali-dation of the clinical effectiveness of an emergency department-basedearly goal-directed therapy protocol for severe sepsis and septic shock.Chest 2007; 132:425–32.
190. Shapiro NI, Howell MD, Talmor D, et al. Implementation and out-comes of the multiple urgent sepsis therapies (MUST) protocol. CritCare Med 2006; 34:1025–32.
191. Trzeciak S, Dellinger RP, Abate NL, et al. Translating research toclinical practice: a 1-year experience with implementing early goal-directed therapy for septic shock in the emergency department. Chest2006; 129:225–32.
192. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy inthe treatment of severe sepsis and septic shock. N Engl J Med2001; 345:1368–77.
193. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: anemiaand blood transfusion in the critically ill—current clinical practice inthe United States. Crit Care Med 2004; 32:39–52.
194. Shorr AF, Jackson WL, Kelly KM, Fu M, Kollef MH. Transfusion
practice and blood stream infections in critically ill patients. Chest2005; 127:1722–8.
195. Shorr AF, Duh MS, Kelly KM, Kollef MH. Red blood cell transfusionand ventilator-associated pneumonia: a potential link? Crit Care Med2004; 32:666–74.
196. Taylor RW, O’Brien J, Trottier SJ, et al. Red blood cell transfusionsand nosocomial infections in critically ill patients. Crit Care Med2006; 34:2302–8.
197. Abraham E, Laterre PF, Garg R, et al. Drotrecogin alfa (activated) foradults with severe sepsis and a low risk of death. N Engl J Med2005; 353:1332–41.
198. Levi M, Levy M, Williams MD, et al. Prophylactic heparin in patientswith severe sepsis treated with drotrecogin alfa (activated). Am JRespir Crit Care Med 2007; 176:483–90.
199. Vincent JL, Bernard GR, Beale R, et al. Drotrecogin alfa (activated)treatment in severe sepsis from the global open-label trial ENHANCE:further evidence for survival and safety and implications for earlytreatment. Crit Care Med 2005; 33:2266–77.
200. Siegel JP. Assessing the use of activated protein C in the treatmentof severe sepsis. N Engl J Med 2002; 347:1030–4.
201. Warren HS, Suffredini AF, Eichacker PQ, Munford RS. Risks andbenefits of activated protein C treatment for severe sepsis. N Engl JMed 2002; 347:1027–30.
202. Laterre PF, Garber G, Levy H, et al. Severe community-acquired pneu-monia as a cause of severe sepsis: data from the PROWESS study.Crit Care Med 2005; 33:952–61.
203. Ely EW, Laterre PF, Angus DC, et al. Drotrecogin alfa (activated)administration across clinically important subgroups of patients withsevere sepsis. Crit Care Med 2003; 31:12–9.
204. Kreymann K, de Heer G, Nierhaus A, Kluge S. Use of polyclonalimmunoglobulins as adjunctive therapy for sepsis or septic shock.Crit Care Med 2007; 35:2677–85.
205. Laupland KB, Kirkpatrick AW, Delaney A. Polyclonal intravenousimmunoglobulin for the treatment of severe sepsis and septic shockin critically ill adults: a systematic review and meta-analysis. Crit CareMed 2007; 35:2686–92.
206. Turgeon AF, Hutton B, Fergusson DA, et al. Meta-analysis: intrave-nous immunoglobulin in critically ill adult patients with sepsis. AnnIntern Med 2007; 146:193–203.
207. Werdan K, Pilz G, Bujdoso O, et al. Score-based immunoglobulin Gtherapy of patients with sepsis: the SBITS study. Crit Care Med2007; 35:2693–701.
208. Hentrich M, Fehnle K, Ostermann H, et al. IgMA-enriched immu-noglobulin in neutropenic patients with sepsis syndrome and septicshock: a randomized, controlled, multiple-center trial. Crit Care Med2006; 34:1319–25.
209. Darenberg J, Ihendyane N, Sjolin J, et al. Intravenous immunoglob-ulin G therapy in streptococcal toxic shock syndrome: a Europeanrandomized, double-blind, placebo-controlled trial. Clin Infect Dis2003; 37:333–40.
by guest on March 24, 2012
http://cid.oxfordjournals.org/D
ownloaded from