hale et al 1988 - .net framework
TRANSCRIPT
THE LANCET No 8625 BOSTON, MASS. AND LONDON· SATURDAY DECEMBER 17 1988 VOL II FOR 1988
ORIGINAL ARTICLES Ocular Fundus Lesions in Divers 1381 P. ]. Polkinghome, FRACP, Kulwant SehnU, FRPS, M. R. Cross, MB, Darwin Minassian, FRCS, Prof A. C. Bird, FRCS
Allele Loss on Short Arm of Chromosome 17 In Breast Cancers 1384 ]. Mackay, FRCS, C. M. St«I, MRCPE, P.A. Elder, HNC, Sir Patrick Forrest, FRCS, ProfH. J. Evans, PHO
Support for Adrenaline-hypertension Hypothesis: 18 hour Pressor Effect after 6 hours Adrenaline Infusion 1386 P. J. Blankestijn, MD, A. J. Man in't Veld, MD, Joke Tulen, B SC, A.H. ven den Meiracker, PH o, Frans Boomsma, PH o, Peter Moleman, PH o, H.J. Ritscrna van Eck, MD, F. H. M. Derlcx, MD, Paul Mulder, PH o, S. ]. Lambens, MD, M.A. D. H. Schalelwnp, MD
Simultaneous Isolation of HIV-I and HIV-2 from an AIDS Patient 1389 L. A. Evans, PH o, Jacques Moreau, MD, Koudou Odehouri, MD, Deborah Seto, BA, Graeme Thomson-Honnebier, MD, Harold Legg, BA, Ashley Barboza, BA, Cecilia Oleng-Mayer, PH D, Prof J. A. Levy, MD
Improvement of Hepatic Encephalopathy Treated with Flumazenil 1392 Georg Grinun, MD, Peter Fercnci, MD, Regina Katzenschlager, Olristian Madi, Bruno Schneeweiss, MD, A. N. Laggner, MD, Kun Lenz, MD, Prof Alfred Gangl, MD
PRELIMINARY COMMUNICATION Remission Induction in Non-Hodgkin Lymphoma with Reshaped Human Monoclonal AntibodyCAMPATil-IH 1394 G. Hale, PH o, M. J. S. Dyer, MRCP, M. R. Oark, PH o, ]. M. Phillips, PH D, R. Marcus, MRC PATH, L. Riechmann, PH o, G. Winter, PHO, H. Waldmann,MtD
REVIEWS Notices of Books 1399
GENERAL PRAcnCE EvaluadonofaStructured Treatment and Teaching Programme on Non-insulin-dependent Diabetes 1407 Peter Kronsbein, PH o, Viktor Jorgens, MD, Ingrid Miihlhauser, MD, Vera Scholz, PH D, Annene Venhaus, MS, Prof Michael Berger, MD
THERAPEUTICS Reversible Ceftriaxoneassociated Biliary Pseudolithiasis in Children 1411 U. B. Schaad, MD, Joanna Wedgwood-Krucko, .\\0, Heinz Tschaeppeli;r, MD
HOSPITAL PRAGnCE Nasal Continuous Positive Airway Pressure In - ~ Pneumocystis carinii Pneumonia 1414 Steven Kesten, FRcrc, A. S. Rebuck, FRCPC
ROUND TIIE WORLD India 1415
IN ENGLAND NOW 1416
XamoteroI: Stabilising the Cardiac Beta Receptor?
Shackled, Shameful, and Shoddy
Valproate, Spina Bifida, and Binh Defect Registries
Diurnal Variation in Platelet Aggregation Responses
Recurrent Respiratory Papillomatosis
1403
1404
1406
1407
1408
LETIERS TO TIIE EDITOR Reversed Polarity of Vasculocutaneous
Potential and Neonatal Nccrotislnc Enterocolltls 1417 Dr M. R. Millar and others
Haemodllution In Renal Transplantation in Patients on Erythropoietln 1418 Dr Jan Wahlberg and others
Treatments for Neurotic Dborders 1418 Prof D. F. Klein
Ucensing Synthetic lntracervlcal Tents 1418 Mr Nicholas JohnS<lCl, MRCX>G
Birthwdght and Neonatal Monallty 1419 Dr Alfredo Pisacanc
Food Intolerance and Rheumatoid Arthritis 1419 Dr Pekka Kurki and others; Prof L. Corbec:I and others
Changes In Body Wdght between Consecutive Pregnancies 1420 Dr J. S. Samra and others
Salmonella -teritidi• Phage Type 4 and Hens' Eggs 1421 Dr John Paul, Dr Barry Batchelor
O.olinergic Side-elTecu of Tetrabydroaminoacridinc 1421 ProfR2ymond Uvy
Peripheral Facial Paralysis Indicating HIV lnrection 1421 Dr Laurent &lee and Olhers
HIV, Glue Ear, and Adenoidal Hypertrophy 1422 Mr J. W. Fairley, FRCS, and others
Cat Scratch Disease, Bartonellosls, and Kaposi Sarcoma 1422 Dr S. Dcaller
Inhibition of O.olinesterasn by Pentarnldinc 1423 Dr T. A. Alston
Italian Epidemic orW•terbornc Tulancmi8 1423 Dr E. Mignani and others
Home lntravmous lmmunoglobulin Therapy 1423 Dr H. M. O>apcl, Sister V. M. Brennan
Is Inactivated Poliovacclne more Expensive? Dr J.P. Moulia-Pdat and others
Heat-suable vcnus Heat-labile
1424
Vaccines 1424 Dr C. P. Muller, Prof Giinthcr Jung
Marlagmimt of Dysentery by Community Health Worken 1425 Dr Manin Kirl<patrick
Antibody Responses to Human Herpcsvirus 6 and other Herpcsvlruses 1425 Dr D. ] . Morris and others; Dr Martin Andre, Dr lkrtfncd Matz
Parvovlrus-associated Thrombocytopenic Purpura Dr N. K. Foreman and others
Clinical Trial Numben and Confidence Intervals of
1426
Pre-specified Sitt 1427 Mr S. J. Day, FSS
Danish Exp.rim« of Suatutory Right or Patients to Access to Hospital Records 1428 Dr T eis Andcnen Dr Georg Jergmsm
Better Surgeons get Better Results 1428 Mr Richard Novell, FRCS, and othcn
Paying for Extended Medicare 1429 Dr Brian Potter
ICRF Appeals Dr L. A. l'lia:
1429
Graves' DiseaK: the Thyroid not the Pancras 1429 Prof]. G. Scadding
Specific Detection of r.,,;,, MJ6inata Eggs by DNA Hybridisation 1429 Dr A. Flisscr and others
Non-$urglcal Lefi-atrial Aonic Bypass Dr U. U. Babic and others
1430
Screening for Aortic Aneurysm 1431 Mr Jack Collin, FRCS
Pelvic Irradiation and Tamoxlfm as Risk Facton for Carcinoma or Corpus Uteri Dr l..amart Hardell
1432
Erythromycln-raistant Streptococcw tm-monitM 1432 Dr J. Vttha<gm and Olhers; Dr R. E. Wanm and others
Naevus of Jamaica Dr Ncjat Akar
1433
MEDICINE AND 1llE LAW O>smetic Surgery: Greater Duty to
Warn of Risks 1434 Doctors and Advertising 1434
NOTES AND NEWS MRC Activities-Official 1435 Spare a Thought for the Victim 1435 Help for Sick Doctors 1435 After the Olrisanas Pany 1435 C.ancer Incidence World Wide 1435 Women's Health Concern 1436 Healers, Quacks, and Lady Doctors 1436 Postgraduate Education 1436 Training Courses for HIV/AIDS
1436 Counsellors
CORREGnON Fetal Obstructi~e Uropathy 1436
Editorial Offi«: 46 Bedford uarc, London WCIB 3SL, England. Tel: 01-436 4981. The Lan=, North American Edition ISSN 0099-5355 published wttltly by Llnlc, Brown and Company, 34 Beacon St., Boston, Mass. 02108. Annual individual subscription in U.S. 185.00, in Canada S95.00; resident and intern rate (U.S. and Canada) $48.50; Single copy $7.00. Second class postage paid at Boston, Ma .. ., and"' additional mailing offices. !) The Lancet Lld., 17 Dcconber 1988. Postmaster: Send address changes to The Lan=, 34 Beacon St, Boston, Mass. 02108 (617) 227-0730, ext 516. lliE WHOLEOFTilE 1..llCRARY .\\ATJCR IN THE LANCET IS COPYRIGHT
0189 1289LI SC IP 0400~~ °'f8 SCRIPPS C~INIC hfS FDTH:'\)".W. l ·i~~~~LT5R~·~R INES DEC:::~ 1988 LA J3LLA CA 92037
DO NOT REMOV~j
1 of 7 Celltrion, Inc., Exhibit 1132

1394
Discussion This study is the largest experience to date with the
bcnzodiazcpine antagenist flwnazcnil in the treatment of HE. The effects of the drug were assessed clinically and by SEP recordings. The late components of cortical SEPs (peaks X3 and P3) appear to be highly sensitive indicators of cortical dysfuiiction in HE.11 The results indicate that Oumazcnil may improve the HE that complicates both acute and chronic liver failure. Flumazenil treatment was IS30ciated with improvement in neurological status in 60% of episodes of HE; with one exception improvement occurred within a few minutes to an hour of drug administration. The speed of these responses contrasts with the interval of several hours that is typically necessary before HE improves after conventional therapies. The response co flumazcnil in bcmodiazcpine intoxication is also very rapid.19
The 60% improvement rate may even underesr.imate the potential efficacy of flumazeni.I in the treatment of HE since most of the patients in this study had been cncephalopathic for many days before flumazenil treatment and had not responded to conventional therapy. Furthermore all 5 patients with clinical evidence of increased intracranial pressure due to brain oedema did not respond to flwnazerul. l of these patients improved after treatment with mannitol. The remaining 4 died within 3 days of flumazcnil administration.
In 8 of the 12 episodes rcponding to flumaz.cnil there was an exacerbation of HE 0·5-4 h after stopping treatment, This transient effect of the drug is consistent with its phannacokinctics.'°.z1 To achieve a sustained response continuous administration of the dn:~ over lonecr period~ may be necessary. Although these 12 episodes unproved, no patient regained normal brain function at the end of treatment. The possibility that larger doses or a longer duration of treatment would have achieved complete improvement seems unlikely since, in bcnzodiazcpine intoxication, much lower doses are sufficient for recovery. 11
In addition an increased GABA-crgic tone may be only one of many abnormalities of brain function in patients with liver failure and correction of this particular abnormality may therefore induce incomplete improvement.
The mechanism by which flwnazcnil improves HE is uncertain. One possibility is displaccmcnt of an endogenous bcnzodiazcpinc-like substance from the GABA"bcnzodiazcpine receptor. The prcscncc of such a substance was suggested in the brains of animals with HE and in cerebrospinal fluid of patients dying with HE. 21
This srudy was supponed by the Fonds zur FOrdcnina der wwcn· schaftlichcn Fonchung (P 6169 M). Flwnaunil was provided by HoffmannLa Roche, Basel, Swilzerland.
Corttspondcnce should be oddttsscd to G. G., 1st Oepanmmt of Medicine, Uruvcniry of Vimn11, A-1090 Vimnll, Ausma.
REFERENCES
I. Scllafcr OF,P-SC, llndy LE,Jacol>I R,JonaEA. v...i~pounuab ona nbbol modd o( ._ mcephalopolhy I. _... -..... Ind mmponsara wilh dtuc lnduc.d ........ ~ 1984;"' 540-45.
2 Basil< AS, Ganvnal SH, Mullen KD, Jones EA, SkoWd< P. DilTcr<naal mponlivmcss o( ocr<bdlu: Pur!Onj< ncun>n> to GABA and bcnzodiazopu>< r«<pcor bpnds in m orurnal modd olbcpobc: mcopbolopolhy. JN- 1988;1: 2414--21.
3. Scharer OF, Jones EA H<poac mcq>halopodly and 1h< y~...ad ncwocnnsrrumr ,,_.., ~ 11182; ii: 1&-.:IO.
4. Paul SM, Ma..,..,. PJ, Skolnd P. Tbt ~-<hloride ionophote r«<pcor complct: ......-lite oCnunor innquilliza ection. Biol l'rycJr 1981; 16: 213-29
THEu.NCET,DECEMBER 17, 1988
Preliminary Communication
REMISSION INDUCTION IN NON-HODGKIN LYMPHOMA WI1H RESHAPED HUMAN
MONOO..ONAL ANTIBODY CAMPA Til-lH
G. HALE' M. R. ()JJu{I
R MARcus2
G. WrNTER1
M. J. S. DYER2
J.M. PHILLIPS' L. RIElliMA.NN1
H. WALDMANN'
/Rparrmnus of Palho/ogy1 and Haanarology,' Unn.'C'siry of Cambridge, and Labortllory of Mokcu/ar Biology,> Cambridge
Summary A genetically reshaped human IgG l monoclonal antibody (CAMPATI-1-lH.
was used to treat two patients with non-Hodgkin lymphoma. Doses of 1-20 mg daily were given intravenously for up to 43 days. In both patients lymphoma cells were cleared from the blood and bone marrow and splenomegaly resolved. One patient had lymphadenopathy which also resolved. These effects were achieved without myelosuppression, and normal haemopocisis was restored during the course of treaonent, partially in one patient and complctdy in the other. No antiglobulin response was detected in either patient. CAMPATI-1-lH is a potent lympholytic antibody which might have an important use in the treatment of lymphoprolifcrative disorders and additionally as an immunosuppressive agent.
G. GRIMM AND OTHERS; REFERENa;.s....coruinwd
5. Banldi M, Zenaoti ML, VaalW'll E, n al. Supmcnsiliviry o( bauodilzq>ane m:ep«>n in hq>oac aaaphalopelhy due to fulnunan1 bepotic failure in 1h< n1. r<venoJ by • bauodiaz<pine - Clut So 1984; 67: 167-~.
6 BauettML.Mullm KD,Skolrud<P,nal~o(hq>oacmcephalopolhyby phumoo:)lopc .,_...,. oC 1h< GABA•~ re<:<J*lr canplot., a rabbttmoddofl\olminomhq>ouc faalutt. a.,,,_,,.oloo 1987;'3: 1069-77.
7. 8ansky G, Mdcr PJ, Ziegler WH, Walser H, Sdvrud M, Huber M. Rev<nal of hepoDc coma by bcnzodiazepu>e Wlaiconi>t (Ro I 5rl788~ U..:n 1985; i• I 32+-25
8 BanslyG,MacrPJ,RiedeftrE,nal Ell'<aola~-nbepooc mcephalopolhy.,--. H'PO'olao 1987; 7: 1103
9. S<olJo.t....vw.n G, Suwvnonn E. Revenal ol hq>ooc coma by -_,. anusonist (Ro 15rl788). lanu1 1985; i: 1324.
10. Bwte DA, Milchdl KW, Al Mardini H, R<a>rd CO Rev<na1 o(hepobc coma Wldl Oumazmil .,........,..,...,,., an V>IUll ~ pocmaals. lanul 1988; ii:~
11 Su!herbnd LR, M....ia GY. Ro 15rl788 and hepobc ~A- I"''"' Mal 1988, IOI: 158.
12 Gnmm G, L<ni K, KJe.nberl<f G, n al. Ro I Sri 788 unprovcs coma on ~ out of 5 peomts with fulmananl hcpabC Ca.turc": vcnficaoon by b\a; latency auditory and soma1osauory po<mtiab. J H•paUJ/ 1987; 4 (suppl I): S21.
tl Mt... R, Gyr K. Traanen1o(hepoo< <ne<phalopotlay (HE) Wllh the btluodmepone .._.,. fNmazcrul: a plo< S<Udy. £w J A_,,ltnoo/ 1988; suppl 2 t l9-46
14 T.....W. G, Jmnm B Assesvnaat o( 1X1ma and tmpaaml a>nsc:IOU>ll<SS a pncoaJ scale. lanut 1974; u: 81-1!4.
15. Conn HO, Liebenhal M. Tbt hepotic 1X1ma syndromn and lactuloK. Baltimo«: Vlllilms & Wil<inl, 1979: 6.
16. Cnao RQ, Bodlf.Wolner I, <do. Fronlim o( dinocal """"*"""' Voll evoked poc- New Yon:: Alm R. Lm, 1966.
17. )- HH. Tbt tal/twa>ty ekarodc .,....... oC 1h< I~ Fcdcnoon. ~ClatN~1958; 10:371-75.
18. Olu NS, Yq SS. Ponal-symnuc cnaphalopolhy: ahcrations in~ and bninsccm audnory evoked pocentials. J Nnmll So 1988; 14: 41-'°
19 l'n5dU F, Donner A, Grimm G, t1 al Value o( flumazaul ., bauodiaupone ldf-poiooralns. M.J T.....i 1988;): 334-)9.
:10 L>staR,Gr.<nl>llnD,AbemoihyD,nall'bam-....oc""'1ia..,ROl5rt788,a bcNodiueptne ._ lipnd, in tbebninol,._ B,.,,Ro 1984;J90l ls:Hl6.
21. Roncanli G,ZiqlcrWH,GumienTW. --oltbencwbauodiaupine ._m Ro 15rl788 in,,_ followinc inlrwv<nousand onl ldminio<nDan. Br J °"' ~ 19961ll:421-:IS.
22. Mullen KD, M1r1111 JV, -WB,n al Could., mdopnoul bcnmdiaz<pln< ........ """"-., bepotic cna:pbalopodry? Lanut 1988; i: 457-59.
2 of 7 Celltrion, Inc., Exhibit 1132

THE U..-.:CET,DECEMBER 17, 1988
i l
A
... -· ... a UllHot•• , ........ , lttMU Ntu+IN ON I
1395
Fag 1-Efrttt ofCAMPATil-IG (A) and CAMPATil-IH (8)- blood counts in poitleat I. 4 - lymphocytes; D. • ncucrophils.
INTRODUCTION
T U.\\OUR treaanem by passive serotherapy has had a long and largely unsuccessful history .1 The advent of monoclonal antibodies gave fresh impetus to this approach, but results with unmodified antibodies are generally unremarkable. Efforts to enhance activity in vivo are now largely focused on the conjugation of antibodies to toxins or radionuclides. However, we are convinced that physiological effector mechanisms are still among the most potent and have tried to find the optimwn combinations of antibody specificity and isocype to exploit them fuJJy.
One possible specificity is the CAMPATH-1 antigen.' It does not readily undergo modulation and is abundantly expressed on virtually all lymphoid cells and monocyces, but not on other cell cypes.u These properties make it a potential target for treaanent of lymphoid malignant disorders and for immunosuppression. Several rat lgM and lgG antibodies to this antigen have been produced.•.s The lgM CAMPATH-IM) is intensely lytic with hwnan complement and is widely used for depletion ofT cells from bone marrow to prevent graft-versus-host disease."' The lgG2b (CAMPATH-lG) is the most potent for cell depletion in vivo,• probably because it binds to hwnan Fe receptors and can activate the complement system.• Patients with lymphoid malignant disorders treated with CAMPATH- lG (25-50 mg/day for 10 days) showed pronounced reduction in lymphoid infiltration of blood and bone marrow and improvement of splenomegaly.• However, treaanent with rat antibody is likely to be limited by an antiglobulin response. This problem should be reduced or eliminated by use of a hwnan antibody. A reshaped hwnan antibody (CAMPATH-lH) has been constructed-the hypervariable regions of the rat antibody were transplanted into nonnaf hwnan immunoglobulin genes.• Hwnan IgG l was chosen since it had greater activity than other hwnan isocypes both in complement lysis and in cell-mediated killing .... "
Here we describe the use of CAMP A TH-lH to treat two patients with non-Hodgkin lymphoma. Although it was possible to continue treaanent for up to 6 weeks without the development of a neutralising antiglobulin response, the main point of this report is to describe the efficacy of the antibody in clearing large masses of nunout cells. This is the first report of treaanent with a fulJy reshaped hwnan monoclonal antibody.
PATIENTS ANO MEniODS
Approval for the use of monoclonal antibodies was given by the ethical comminec of Addcnbrooke's Hospital and wrincn consent was obwncd from both paticnrs.
Antibodies were obtained from culrure supernatant of cells growing in a hollow fibre biorcactor (' Acusyst-Jr', Endorronics). CAMPATii-IG was purified by precipitation with ammonium sulphate; CAMPATH-IH was purified by affinity chromatography on prolClll-A-• Scpharosc'. They were dissolved in phosphate-buffered saline, sterile filtered, and tested for pyrogcn and sterility. Patients were prchydrated overnight and antibody, diluted in 500 ml saline, was inflHcd over 2-4 h
CAMPA TH-I expression on rumour cells was measured by flow cytomctry and complement-mediated lysis.u• Scrum ooncent12tions of CAMPATii-IH were measured by invnWlOOuorescmce with normal lympbocytcs.' Southern bk>< analysis with an imnnmoglobulin J" probe was used to detect residual rumour cdls in DNA extracted from mononuclear fractions of bone marrow.• Antiglobulin responses were sought by two techniques. Tbc first was a solid-phase cnzymc-linked assay using microtittt plates coated with CAMPATH-IH. After incubation with patients' scrum samples, the assay was devdopcd with biotin-labelled CAMPATH-IH foUowcd by Stttptavidinpcroxidasc. A mixture of monoclonal mouse antibodies against human JgG was used as a positive control and 500 ng/ml of this mixture oould be detected. In the second assay, patienrs' scrum samples were mixed with rcdcdlsoouplcd with CAMPATH-IH.11
Agglutination by 5 ng/ml of the control mixture could be detected. Inummoglobulin allotypcs were dctcrmincd by means of standard reagents and techniques from the Central Labomory of the Netherlands Red Cross blood U20Sfusion service.
RESULTS
PaLien1 I
A 69-year-old woman presented in I 983 with acute appendicitis. Massive splenomegaly was found (table) and the bone marrow was heavily infiltrated with lymphocytes, some of which had clefted nuclei and a single nucleolus. There was weak membrane expression of IgM-kappa. Computed tomography scan showed splenomegaly but no lymphadenopathy. Grade I, stage IVA non-Hodgkin lymphoma in leukaemic phase was diagnosed. Between 1983 and 1987 the patient received oral and intravenous chemotherapy with combinations of cyclophosphamide, vincristine, prednisolone, and chlorambucil, which induced partial responses, the minimwn level of marrow infiltration being 40%. Two courses of splenic radiotherapy were given,
3 of 7 Celltrion, Inc., Exhibit 1132

1396
but the second (in April 1987) was cunailed since the spleen grew larger during the course.
In September 1987 the disease progressed with increases in blood lymphocytes (24 x 109 cells/I) and spleen size. The patient was treated with CAMPATH-IG for 8 days (fig IA). This treatment completely cleared lymphoma cells from blood and marrow but only partially reduced spleen size. CAMP A TH-1 G induced fever, nausea, and vomiting, and the treatment was stopped on day 8 when it resulted in severe bronchospasm. (Such severe reactions have not been seen in twenty-one other patients who have received similar doses.) Reappearance of lymphoma cells in the blood was initially slow and the spleen size did not change for 5 months but there was little recovery of normal haemopoiesis. In March 1988 the patient began to lose weight and experienced drenching night sweats. The spleen enlarged and lymphoma cells reaccumulated in the blood. They had similar phenotype and identical rearranged immunoglobulin J" fragments to those seen before treatment. Marrow aspirate and trephine showed complete replacement of normal marrow by lymphoma cells (fig 2A); the patient became dependent on red-cell transfusions and was absolutely neutropenic.
The patient's serum did not b lock binding of CAMPATH-IH or CAMPATH-IG to normal lymphocytes and the tumour cells were still sensitive to these antibodies in vitro, so we decided to treat her with CAMPATH-IH. The starting dose was 1 mg daily and, since it was well tolerated, the dose was increased to a maximum of 20 mg/day, though the usual dose was 4 mg/day owing to the small amount available. In all the patient received 126 mg over 30 days. The response was prompt; in 6 days the night sweats had abated, by day 10 there was pronounced reduction in splenomegaly and recovery of blood neutrophils, and by day 18 lymphoma cells were cleared from the blood (fig IB). On day 28 a bone marrow aspirate and trephine were hypocellular but showed active myelopoiesis and erythropoiesis and no lymphoid cells (fig 2B). No CAMPATH-1-positive cells could be detected by flow cytometry. DNA from the mononuclear marrow cells was germline when probed with an immunoglobulin t probe under conditions where clonal rearrangements could be detected in 0·2% of cells. Thus, we conclude that lymphoma cells were cleared from the marrow. The spleen volume was reduced about eight-fold (fig 3A, B), although it was still slightly larger than normal.
Other than fever occurring about I h after the end of antibody infusions there were no adverse effects of antibody treatment until the 5th week, when severe rigors occurred after each infusion. No antiglobulin response could be detected and the rate of clearance of antibody from the serum was unchanged. For the next 3 weeks the patient continued to experience occasional fever and rigors. She was given oral cotrimoxazOfe because of her lymphopenia, but no infective cause of these symptoms could be found.
In the next 4 months lymphocytes, which appeared morphologically normal, slowly reappeared in the blood (up to 0·2 x 109/1). They did not show the characteristic rearranged immunoglobulin fragments, and both CD3-positive and CDI9-positive cells were present (table). Serum immunoglobulin levels, which had been very low since presentation, have risen towards normal (table). A marrow aspirate and trephine taken 50 days after the end of treatment were again hypocellular but had no lymphomatous infiltration. This rnai:ow sample contained
THE LANCET, DECEMBER 17, 1988
PATIENT OiARACfERISTICS BEFORE AND AFTER TREATMENT
WITH CAMPATH-IH
Patient 1 Patient 2
- Before After• lld0tt After•
Splern nu (m/Jt 4460 590 2600 440 Lymphadmoparlryt None None None
paraortic ~marrow % lymphoma cells 99 0 72 0 Southern blot analysis lg JH fragment R/R
Pm/>heral blood G/G R/R G/G
Haemoglobin (g/dl) 8·7 10·6 11·2 .12-0 Rcticulocytcs ( x 109/1) 31 135 ND ND Platelets ( x 109/1) 37 50 110 453 Lymphocytes ( x 109/1) 60 0 37 0 Neu<rophils ( x 109/1) 0 2-0 4·6 7-3 Monocytcs ( x 109/1) O· 0-04 1·5 0·5
Blood lymplwcyte phmctype I % J
CD19 97 46 93 <5 CD3 0 32 8 80 CAMPATH-lM 96 ND 95 ND CAMPATii-lH 98 ND 97 ND
Serwn immunctlobulins lg/I)
JgM <0·3 1·2 <0·3 0·7 lgA <0·5 <0·5 <0·5 0·5 JgG 5·8 8·2 n 4·7
Brna-Jtm£j None None ++ None
*Made shonly after end of antibody treatment, except for lymphocyte phcnotyping and senun inununoglobulins, which wae assessed 6 weeks later. tBy computed tomognphy. ND- not done.
4% CAMPATH-1-positive cells and showed some oligoclonal rearrangements of immunoglobulin genes. However, by day 100, lymphoma cells were again detected in the blood and the spleen size had started to increase. A second course of 12 days' therapy with CAMPATH-IH was completed with similar therapeutic benefit to the first and no adverse effects. Since the main reservoir of disease in this patient appeared to be the spleen, splenectomy was carried out at the end of this second course of treatment. At that time no rumour cells could be detected in blood or marrow. The patient is now well 37 days after the splenectomy. The lymphocyte count is low but she has normal neutrophil, platelet, and red-cell counts.
Pazient 2
A 67-year-old man presented in April 1988 with splenic pain; there was 12 cm splenomegaly, and computed tomography scan of thorax and abdomen revealed retrocrural and para-aortic lymphadenopathy, the largest node measuring 3 cm in diameter (fig 3C). A blood count revealed 36·6 x 109 lymphocytes/ml, the majority being lymphoplasmacytoid cells which expressed surface IgGkappa and were characterised by large cytoplasmic periodicacid-Schiff-positive vacuoles which could be intensely stained by anti-IgG. A marrow aspirate contained 72% lymphomatous cells (fig 2C). DNA from blood mononuclear cells showed biallelic rearrangement of immunoglobulin J" genes but was germline with various T -cell receptor and oncogene probes. The lymphoma cells expressed the CAMPATH-1 antigen in amounts comparable with normal lymphocytes but were more resistant to complement-mediated lysis. Stage IV A grade I
4 of 7 Celltrion, Inc., Exhibit 1132
THE LJ\NCET, DECEMBER 17, 1988
.. "·
.. ~·· , . . ... ·. • !
~'= ... ·~~··-...: .. ,
.. ":.
•·,~
•... ... .. ·- -
. ---· ... ·~
..A~
... · , ..:· .......... ·
• • ~ ......... "t~ .. .
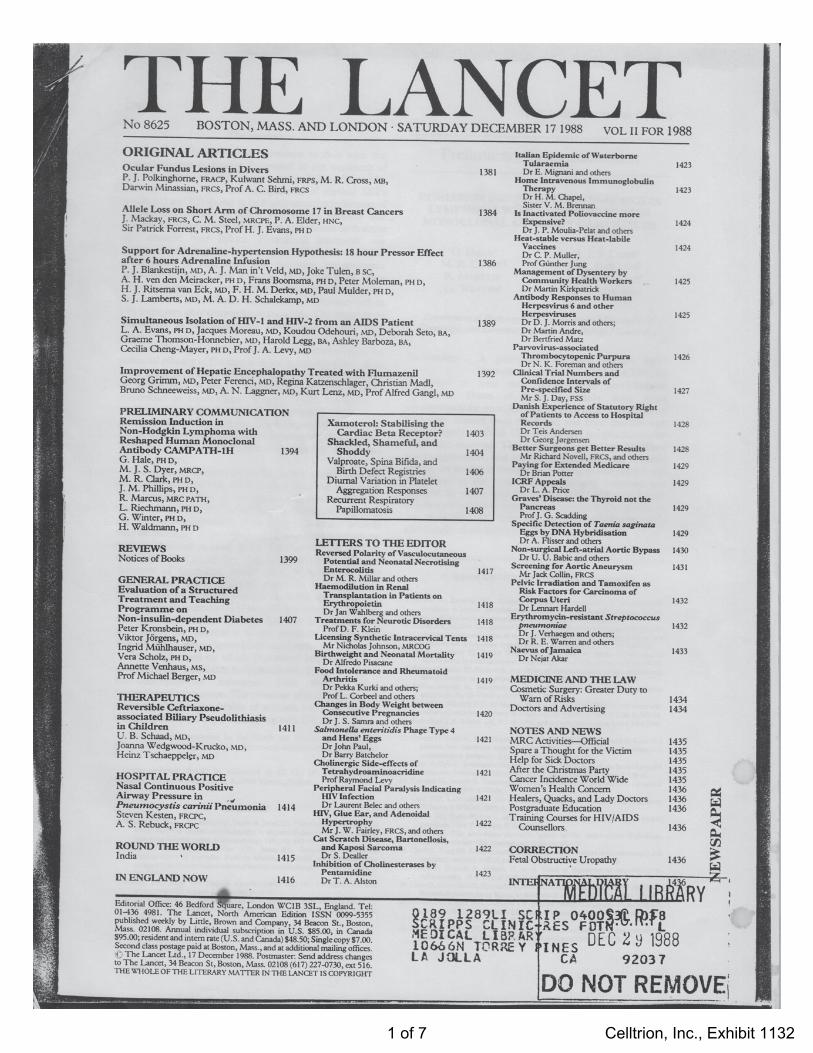
Fig 2.-Cytology of hone ma.rrnw cells.
1397
A~ patient I trcphine before trcaancnt with CAMPATH-IH; B • patient I trcphine on day 43 (ie, 16 days after trcaanent); C~ patient 2 aspirate before treatment with CAMPATH·IH; D - patient 2 aspirate on day 78 (ie, 35 days after trcauncnt). Rcdu<:<d by 58% from x IOO(A,B), x 1000 (C), x 400 (D).
A c
B D
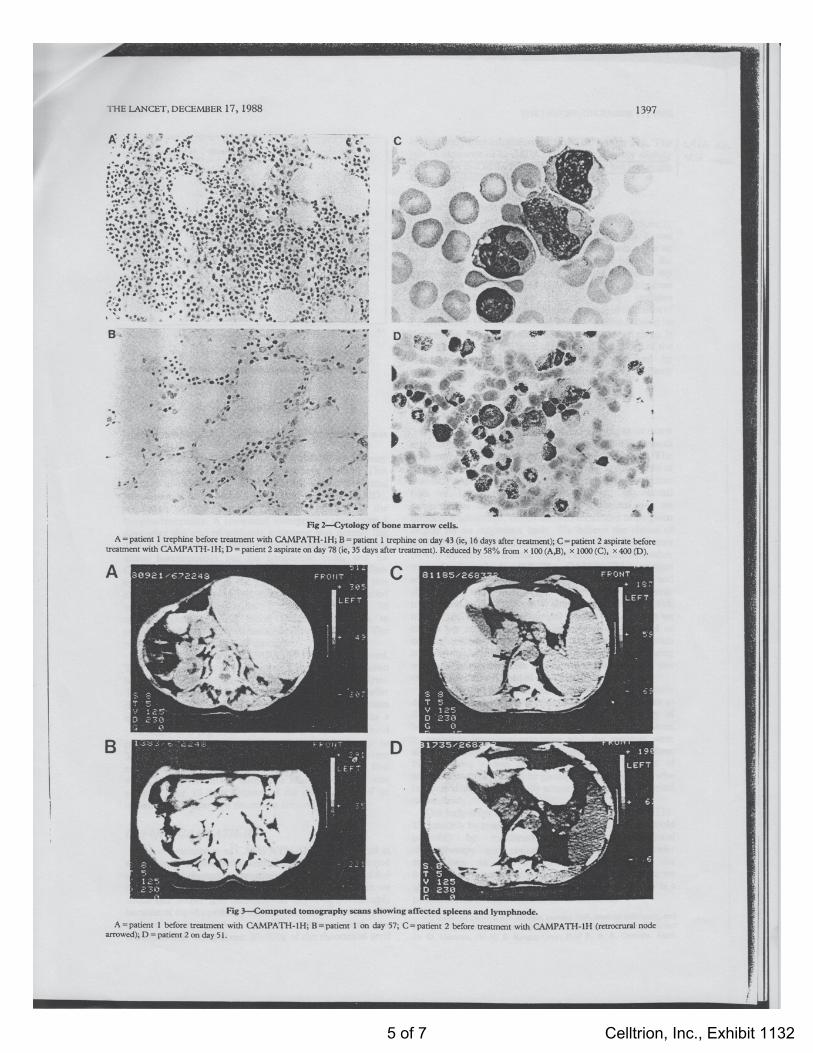
Fag 3--Computed tomography scans showing affected splttDS and lymphnode.
A•patient I before trcaoncnt with CAMPATH·IH; B•patient I on day 57; C - paticnt 2 before trcaancnt with CAMPATH-IH (tttr()CJ"llra] node arrowed); D •patient 2 on day 51.
5 of 7 Celltrion, Inc., Exhibit 1132

1398
CAMH.TH · tH ISMt totel 100 llllfltUUUUH I I f I I I t t
c 10
e
• 0 · 5
i l
0 10 20 30 •o so 10 10 10
Days since start of antJbody therapy
Fig -Effect of CAMPA TH-IH on blood counts in patient 2.
• = lymphocytes; D. = neutrophils.
to
lymphoplasmacytoid non-Hodgkin lymphoma was diagnosed.
The patient was offered CAMPATH-lH as primary therapy and received a total of 85 mg over 43 days. This resulted in clearance of the lymphoma cells and normal lymphocytes from blood (fig 4) and marrow (fig 20), resolution of splenomegaly, and improvement in the lymphadenopathy. A computed tomography scan taken 8 days after the end of antibody treaunent was normal (fig 30). A bone marrow aspirate taken at the same time showed active haemopoiesis but no lymphoma cells, and no CAMPATH-1-positive cells could be detected by flow cytometry. DNA from the mononuclear fraction of this marrow showed only germline configuration when probed with the imrnunoglobulin J H probe. By day 78 morphologically normal blood lymph0cytes began to reappear and none of the vacuolated cells could be seen. The patient remains well and off therapy.
Some toxic effects of CAMPATH-lH were observed. The first dose was stopped after 3 mg had been given because of hypotension, possibly caused by tumour lysis. This problem was subsequently avoided by giving smaller doses at a slower rate and when lymphoma cells had been cleared from the blood, the dose was increased to a maximum of 8 mg over 4 h without any effect on blood pressure. Nevertheless, all doses induced fever (up to 38·5°C), and malaise for up to 36 h, but these were not severe enough to stop antibody treaunent which, after the first week, was given on an outpatient basis. Treaunent was stopped after 43 days because of the development of an urticaria! rash after two successive antibody infusions.
Half-life of CAMPATH-IH
The concentration of CAMP A TH-1 H was measured in serum samples taken before and after antibody infusions and at other rimes throughout treaunent. In theory, a dose of 4-<i mg corresponds to about 1 µg/ml in the plasma. In fact we could not detect free antibody till day 4-<i, presumably because of rapid uptake by the tumour mass. After that, the rate of clearance was roughly constant, with the concentration being about 30-70% of the theoretical level
THE LANCET, DECEMBER 17, 1988
Lack of Antiglcbulin Response
TheallotypeofCAMPATH-lH is Glm(l,2,17),Krn(3). Patient 1 was Glm(l,3,17),Krn(3) and patient 2 was G lm(3),Krn(3), so both could theoretically have made an anti-allotype response as well as a response to the hypervariable regions. However, we failed to detect any antiglobulin to CAMPATH-lH either by the solid-phase enzyme-linked assay or by the more sensmve haemagglutination assay. In addition, the rate of clearance of CAMPA TH-IH did not change and free antibody could be detected for up to 8 days after the last dose had been given. It is possible that the reactions experienced at the end of the course of treaunent could have been provoked by contaminating non-human proteins in the antibody preparation.
DISCUSSION
The remissions achieved in these two patients show that it is possible to clear large numbers of rumour cells with small amounts of an unmodified monoclonal antibody. The effects in the first patient were far superior to the results of previous chemotherapy and radiotherapy. The selective lysis of lymphoma cells with recovery of normal haemopoiesis during the course of treaunent was an important advantage, which allowed treaunent to be given largely on an outpatient basis. We believe the· choice of antibody specificity and isotype is important; indeed, it may be why we had more success than previous effons with other monoclonal antibodies.1 ... 16 The CAMPATH-1 antigen seems to be a good target because it is widely distributed and abundant, and does not suffer from antigenic modulation.2.>"·11 This study shows that, as predicted, human IgGl can bring about cell lysis in vivo, though we cannot yet assess the relative importance of humoral or cellular mechanisms. There was no change in serum complement levels (CH50, C3, or C4 components) during antibody treatment (data not shown), but this does not exclude a role for C3 in cell clearance.
Although the two patients did not make any serologically detectable antiglobulin response, it would be premature to draw general conclusions about the imrnunogenicity of human monoclonal antibodies, since CAMPATH-IH itself is probably imrnunosuppressive and the patients were already immunosuppresscd as a result of their disease. Nevertheless, it was encouraging that two courses of antibody treaunent could be given, even in the patient who
· had previously had unusually severe reactions to the original rat antibody.
The long-term benefit of treaunent with CAMPATH-1 H can only be assessed in a much larger trial when it would probably be combined with more conventional chemotherapy and radiotherapy. It may have wider applications as an imrnunosuppressive agent for transplantation and possibly autoimmi,me disease, since we already know that the rat antibody CAMPATH-IG is a potent imrnunosuppressant in the shon-term.
We thank the patients and families, nursing sWT, medical collcaguc:s, and Prof F. G . J. Hayhoe for their coopcT3tion, encouragement and support; and Dr D. Gilmore, Dr H. S. Kruger-Gray, Prof R. R. A. Ox>rnbs, Mart.
6 of 7 Celltrion, Inc., Exhibit 1132
THE LANCET, DECEMBER 17, 1988
Frcwin, ond Caroline McHarg for their help. Thn won was Npported by !he
Medical R~ Uiunal, Wellcome Bioccdl Lid, Ind St John's Collqe
Cambrid~ (Meres studcntslup to M. J. S. D.). 'CAMPA Tif' 1$ a trade mart;
ofWelkxxne Foundaoon.
Correspondence should be addressed 10 H. W., Department of Pathology,
Uruvcmty ofCamb~, Tennis Coun ROid, Cambrid~ CB2 IQP.
REFERENO!S
I. Cumc GA. Ech'l' yean o< immunoch<npy: 1 ttVICW olimmunoloplll m<lhods used
(or treatment album.. canar. B' J c.-tr 1972; Mc 141-S).
2. !Uk G, 11nabt S, Olumblcy G, ct oL R..._.t ol T odl from ban< monow (or
cnrupbntation: a monodMal .-itilymphocytc antibody that fuccs human
compl<mau. Blood 1983; 62: 87>-82. 3. Hole G, Swinl<y O, Waldmann H, 0-LC Rcoctivity ol r11 monoclonal antibody
CAMPATH-1 -"th humon lcubcnua cdb ind its pou.blc oppticotion for
'"'""-" ban< monow c:nnsplan1>oon 8' 1 H"""""" 1985; 40: 41 ~. 4. HoleG, H_,,T,l'>oopcro T, w., SM, Waldmom H. -olT cdbfrom ban<
monow foe trw1Splan......,: ~ ol I'll monoclonal onl>-lympbocytc
onUbodit> ol d>ff<r<nt OOtypCS. Mo/ &ol Mid 1983; I: :lOS-19
5. Hale G, Cobtdd. SP, W1k1mlm H1 Easter G, Matc'itsd\uk P, c.oombs RR.A. Isolation of low·frequcncy ctass.swuch variants from rat hybrid mydonw.
J /__,,,/ Mttlr 1987; 103: 59---67.
Reviews of Books
Worse than the Disease: Pitfalls of Medical Progress -
Diana B. Dutton with cootributions by 1bomas A. Preston and Nancy E. Pfund. C.ambridgc: C.ambridgc University Press. 1988. Pp 528. {.25. ISON ~52134-0233.
Dr Dutton is a sociologist with a special interest in the development of health policy. She clearly shares Lord Salisbury's view that doctors are a variety of expen who
require to have their strong wine diluted by very large admixrure of insipid conunonsense. On the evidence of this book she has a strong case. Four detailed histories of major
medical developments are presented. Two of these initiatives caused considerable hann and suffering to a small
nwnber of people at enonnous cost and without clinical benefit. The American swine flu mass inununisarion progranune was designed to protect against an epidemic that did not occur and resulted in severe neurological disease in some unlucky recipients. The artificial hean programme conswned vast federal funds over many years and, when tested (probably prematurely) in man, failed to extend life significantly but afforded a few individuals a miserable death. A third development, diethylstilboestrol, was hailed as a wonder drug and widely put to unproven use until serious adv~· scquelae were noted in the children of women who had received it. In the founh case history, the development of recombinant DNA methods, there is no discernible evidence oft physical harm, although the safeguards introduced in the early days, after public debate, were brushed aside under conunercial and scientific pressures. In the absence of any harmful outcome, this last case is very much the odd man out; I suspect that it is
included because of the early public consultation, although this consultation had little effect upon the course of events.
In the first three examples there is an clement of being wise after the event. At least some of those involved acted from the purest of motives when there was considerable
1399
6. Waldmonn H,Or R,HalcG,ctol. Eliminationolpaft-vmus-hostduaKby in vitro
dcplcuon al - lymphocytes usinc 1 ,,_,.:lorW rat lllli-twmon lymphocyte onbl>ody (CAMPA TH· I). 1.-.r 1984, i: 483.
7. !Uk G, ColJbold S, w--... H T-all ~ WMh CAMPA TH· I on llloca>Oc
ban< - a• ..... -• Tr~""" 1988;4S. 7S}-S9. 8. Dyer MJS, HakG,Hoyhoc l'GJ, Wlldmann H. Etrcetso<CAMl'ATH·I ona"bocj;<s
in viYO in pocicnts with lymphoid malignoncics: onflucnc< o( antibody -WC·
Blood(in""'9). 9. RXduNnn L,OorkMR, WoldmannH, W'uucrG Rc>hopinch..,,...,obodi<>for
thcnpy. N.,.,.. 1988; JJ2: JU-27. 10. an_,,. M, Wilb-.>sGT,8'ndonCl,ctal. eon_,_olth<cffcaorNr..-..
olh....,~1111n11m.a1chcdscto<chunmc.,ribodi<>.J£xpMld
1987; 166< IJSl-61. II . Bindon Cl, Hale G, Bru_.,.,,, M, Waldmann H. Humm> monoclonal lgG
..Ubodlcs ctill'u inoomplcmcn1 octivotion fun.,_ 11 the l<vcl olC4 u wcll os Cl q. J Exp M<d 1988; 261: 127-52.
12.Halc G, Swni<y OM, H.,i- FGJ, Waldmom H. Elf= al .-.odonal
anu-lympbocyu ~., Y1YO in monleys ond human Mo/ B..t Mid 1983; I: 321-24
13. Mottll A, Tcrty WD, Waldnwv> TA. Mctobohc propcrucsollgG wbdasscs in man.
J Chn r_,, 1970; 49: 673. 14. Ria J. Schloamat SF. Uolmoon of monoclonal ontibodics in the trc1ancnt of
lcukmuo ond ~Blood 1982; 59: 1-11
IS. Levy R, M.Ucr RA. Biolop:al ond dwaJ implic:orionsollympbocytc hybndomos:
nmor thcnpJ wid> monoclonal ono'bodics. .t-R,., M<d 1983; )4: 107-16.
16. Stevenson GT, Glemi< MJ. Swfaoe unmunoslobuhn ol8-lymphocy,. tumoWS os a thcnpnlb< W'S<L Canur S""' 1985; 4: 21~
17. Bindon Ci, Hot< G, Waldmann H. lmpanana: of onua<n spcci(taty (oraxnplcmcnt
mcd>otcd lyus by monodonol anobodlcs. Ew J /-..a/ (in preu).
uncenainty about the paths to be taken. Later, market forces distoned clinical and scientific judgment, precipitating unjustified clinical use together with obstruction of necessary action by the regulatory authorities. h is a son:y tale, and if there is one obvious lesson it is that the marketplace is no testing ground for medical innovation of thesondiscusscdhere.Wherefinancialrerumsare involved, they only too easily corrupt scientific, clinical, and ethical judgment-in way~ uiat arc not always obvious to the
participants at the time. Dunon continues to swim against the tide by suggesting
that governments must take responsibility for safeguarding society from the consequences of regarding medical developments as saleable commodities. This philosophy she
sees as a variant of Tudor Han's inverse-care law whereby the areas of greatest need attract the least resources. The difficulty here is obvious from one of her case histories-die mass inununisation programme against swine influenza. Here an early warning system was triggered too easily, a President in an election year needed to present a decisive image, and expens lost the courage of their convictions in
the face of the high cost of possibly being proved wrong. The result was a progranune that would have failed to stern an
epidemic even if the epidemic had occurred. Where powerful govenunental machinery existed it over-reacted in an incompetent way.
Dunon recognises the shoncomings of governmental machinery. Her solution is public accountability through other mechanisms at local and national level. She
·recognises the obvious difficulty presented by the way the
popular voice is heard at present. This heavenly chorus "sings with a strong upper class accent. Probably about 90% of the people cannot get into the pressure system". One model she sees in a favourable light is the citizens' panel set up by the Cambridge (Massachusetts) City Manager to examine the potential risks of recombinant DNA research at two of the world's leading universities. This unique approach employed non-experts as a juiy. At a national level she proposes greater congressional oversight of medical innovation and perhaps the construction of an overall policy-making body within the United States Department
7 of 7 Celltrion, Inc., Exhibit 1132