halford capstone paper
TRANSCRIPT

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTHa 1
The Role of Victimization by Peers in Aggressive Behavior Among Youths with Autism
Spectrum Disorder
Michael Halford
University of Missouri

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 2
Abstract
The elevated presence of aggression is one of the most prevalent and distressing behaviors of
youths with Autism Spectrum Disorder (ASD) (Kanne & Mazurek, 2011). Research has shown
that the severity of autistic symptoms is highly correlated with this increase in aggression
(Dominick et al., 2007; Murphy et al., 2009), though little attention has been dedicated to
examining this relation further. Additionally, literature has suggested that victimization by peers
is also significantly correlated with increased aggression in youths with ASD (Rieffe et al.,
2012). Therefore, this study sought to examine the relation between autistic symptoms and
aggression (proactive and reactive) by evaluating victimization by peers as a possible mediator.
One hundred and twenty youths and their caregivers completed a battery of measures to
assessing these variables. The Sobel Test for mediation was then performed to examine if the
relation between autistic symptoms and aggressive behaviors (reactive and proactive) was
significantly attenuated by victimization by peers. Results indicated that victimization by peers
was a significant mediator between autistic symptoms and proactive aggression (P =.05). There
was no significant result for reactive aggression. These findings suggest that victimization by
peers, as well as other social components, may play an unprecedented role in the proactively
aggressive behaviors of youths with ASD. The results of this study may further our
understanding of how social relationships impact the outcome of youths with ASD, as well as
inform ecologically based therapies as more viable treatment options.

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 3
The Role of Victimization by Peers in Aggressive Behavior among Youths with Autism
Research has indicated that approximately 50% of youths with Autism Spectrum
Disorder (ASD) engage in aggressive behavior toward other individuals, including caregivers
and peers (Farmer & Aman, 2011; Kanne & Mazurek, 2011). These elevated rates of aggression
may have a significant impact on the developmental outcomes of these youths (Kaartinen et al.,
2014). Aggression is predictive of depression, rejection among peers, delinquency, academic and
vocational failure, as well as increased adulthood criminality (Card & Little, 2006; Kanne &
Mazurek, 2011; Kaartinen et al., 2014). In addition, childhood aggression negatively impacts
multiple levels an individual’s social ecology. Parents suffer from increased levels of familial
stress and out-of-home placements, teachers suffer from widespread emotional exhaustion and
poor instructional efforts, and peers suffer from a decrease in educational opportunity (Kanne &
Mazurek, 2011). Caregivers frequently report that elevated aggression is one of the most
distressing aspects of their child’s ASD (Baker et al., 2002).
Aggressive behavior is usually conceptualized as either reactive or proactive aggression.
These two manifestations of aggression have distinct functions and motives (Card & Little,
2006). Lucinda B.C. Pouw offers an excellent description on the differences between these two
forms of aggression.
Reactive aggression is seen as defensive behavior in reaction to real or perceived external
provocation without thought to personal gain. It is a response to poor emotion regulation,
feelings of anger, and hostile (mis)attributions or misunderstandings. Proactive
aggression refers to instrumental aggression, which children engage in to reach a certain

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 4
goal (e.g., material or territorial gain or social control), without being provoked. (Pouw et
al., 2012: 1257)
Aggression in youths with ASD has thought to be predominately reactive in nature, such that
youths with ASD who are victimized by peers are likely to respond with anger and engage in
aggressive acts towards peers (Rieffe, 2012). Though most research has conceptualized
aggression in youths as being predominately reactive, research has demonstrated elevated rates
of proactive aggression as well (Pow et al., 2012).
Amid all risk factors for increased levels of aggression, social impairments are some of
the most well-documented. Research has suggested that the severity of autistic symptoms (e.g.
social communication deficits, repetitive behaviors, etc.) is positively correlated with aggressive
behaviors in youths with ASD (Dominick et al., 2007; Murphy et al., 2009). This relation is
typically attributed to the neurological deficits that are common among ASD cases. For example,
the positive correlation between autistic symptoms and aggression has frequently been attributed
to emotional dysregulation, social communication deficits, and impairments in theory of mind
(Pouw et al., 2012; Bauminger et al., 2008; Dominick et al., 2007). Little study has been devoted
to analyzing the social components that may contribute to the significance of this relation,
despite research suggesting a multitude of ecological factors that shape youth behavior
(Bronfenbrenner, 1977).
Research has also demonstrated that youths with ASD are much more likely than
neurotypical youth to be victimized by peers, which may contribute to aggressive behavior
(Rieffe et al., 2012). This may be due to the fact that autistic symptoms often include social
deficits and behaviors that are often deemed inappropriate (Rieffe, 2012; Sreckovic et al., 2014).
Youths with ASD exhibit extreme language impairment, compulsive movements and/or

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 5
behaviors (i.e. the writhing, pulling, or flapping of extremities), and intensely restricted
behaviors and interests (i.e. card games, video games, comic books, etc.; DSM-V). These
behaviors are frequently seen as unusual by peers (Lam and Aman, 2007). It is common for
youths to respond critically to things that they do not comprehend. Therefore, it is reasonable to
assume that increased autistic symptom severity in youths with ASD may predict victimization
by peers.
Studies have shown that victimization and aggression in ASD may have a bidirectional
relation. When a child is victimized, they tend to exhibit more aggression, and when a child is
aggressive, they tend to be victimized more (Rieffe, 2012). It appears that victimization by peers
may act as a catalyst for elevated rates of aggression. Although studies suggest that youths with
ASD are more likely than neurotypical youth to respond aggressively to provocation from peers
(Sreckovic et al., 2014), no prior research has investigated whether victimization by peers
mediates the relation of autistic symptoms and aggression (reactive or proactive) in youths with
ASD.
Therefore, this study sought to further examine the relation between autistic symptoms
(specifically, repetitive behaviors and restricted interests) and aggressive behavior in youths with
ASD. In order to provide the most reliable and effective treatment options for reducing
aggression (and other problem behaviors) in youths with ASD, further research must be
conducted analyzing this relation. Given the degree to which youths are impacted by social
relationships (Bronfenbrenner, 1977) and the elevated rates of victimization among youths with
ASD, this study examined victimization by peers as a possible mediator between autistic
symptoms and aggression. If this social component proves to be a significant mediator, it may
provide further evidence for the use of ecologically based treatments (specifically aimed at

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 6
reducing victimization) as a viable means to reduce aggression in youths with ASD. This
mediational model was tested for both reactively and proactively aggressive acts.
Method
Participants
Participants included youths (N =120) who were diagnosed with ASD and their
caregivers. Diagnoses were assessed via the Autism Diagnostic Observation Schedule (ADOS;
Lord et al., 2000) or Autism Diagnostic Interview-Revised (ADI-R; Lord et al., 1994), which are
considered the “gold standard” measures for ASD diagnosis. All participants met the
requirements for an ASD diagnosis. Participants ranged between 11 and 17 years of age with a
mean age of 14.2 (SD =2.1). Males constituted 77.5% of all participants (N =93), which is
representative of the rest of the population with ASD
Procedure
Youths and caregivers were recruited from a center for autism and neurodevelopmental
disorders in a medium-sized Midwestern city. They were contacted via email, telephone, and text
message. Potential participants were told that their responses would advance future research on
behavior of ASD youths, as well as inform possible ecologically based treatments. Refusal to
participate did not result in any treatment variations at the center for autism from which they
were contacted.
Youths and caregivers completed batteries of measures while at the Midwestern facility.
Youth questionnaires predominately assessed how they perceived the quality of their
relationships with parents and peers. Caregivers answered questionnaires concerning youth
behavior.

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 7
Measures
Caregiver Report
Youth Aggression. Aggressive Behavior was assessed via the Children’s Scale for
Hostility and Aggression: Reactive/Proactive (C-SHARP; Appendix A; Farmer & Aman, 2009).
The C-SHARP is designed to measure five types of aggressive acts (physical, verbal, hostility,
bullying, and covert) in youths with developmental disabilities. This measure contains 58
questions with two responses for each question. The first response measured the frequency with
which an aggressive behavior is being committed (e.g. “pinches others), rated as 0 (doesn’t
occur), 1 (mild or infrequent problem), 2 (moderately serious and/or frequent problem), or 3
(severe and/or very frequent problem). The second response measured the degree to which the
behavior was provoked or unprovoked, rated as -2 (only provoked), -1 (usually provoked), 0
(equally provoked and unprovoked), 1 (usually unprovoked), 2 (always unprovoked). Typically,
the C-SHARP sums both of these responses into one measure of aggression. However, for this
study the division between reactivity and proactivity was maintained in order to assess both types
separately.
Autistic Symptoms. Severity of autistic symptoms was measured by the Repetitive
Behavior Scale-Revised (RBS-R; Appendix B; Lam & Aman 2007). This measure assesses six
subscales of symptoms that are prevalent among ASD, which includes (a) stereotyped behavior,
(b) self-injurious behavior, (c) compulsive behavior, (d) ritualistic behavior, (e) sameness
behavior, and (f) restricted behavior. (Lam and Aman, 2007).

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 8
This measure consists of 43-items, ranking behaviors (on a Likert scale ranging from 0 (behavior
does not occur, 1 (behavior is a mild problem), 2 (behavior is a moderate problem), 3 (behavior
is a serious problem)).
Youth Report
Victimization by Peers. Victimization by peers was assessed via the Multidimensional Peer-
Victimization Scale (MPVS; Appendix C; Mynard & Joseph, 2000). Victimization was
categorized by four subscales: physical victimization, verbal victimization, social manipulation,
and attacks on property. The version of the MPVS used for this study consisted of 16 questions.
These questions listed out possible victimization experiences by peers (e.g. “called me names”),
which were rated by youths with ASD as occurring either not at all (0), once (1), more than once
(2). Responses for an individual were then tallied together as a summed victimization score. This
study has proven to have convergent validity with self-reports on being bullied.
Analyses
Regression. Regressions were conducted via the linear regression statistical macro within the
Statistical Package for the Social Sciences (SPSS). These analyses examine whether an
independent variable has a predictive effect on a dependent variable.
Mediation. Mediation analyses were performed as outlined in Zhao et al. 2010, and were
conducted using the Sobel Test for mediation (Preacher & Leonardelli, 2001). Mediation
assumes that an indirect effect between an independent variable (IV) and a dependent variable
(DV) exists due to the influence of a third variable (the mediator). This occurs when a) the IV
significantly effects the mediator, (2) the IV significantly effects the DV, without the mediator
(3) the mediator significantly effects the DV, and (4) the effect of the IV on the DV either
disappears (full mediation) or diminishes significantly (partial mediation) through the inclusion

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 9
of the mediator. This was calculated by inputting raw regression coefficients (a and b) and their
respective standard errors (sa and sb) into Preacher and Leonardelli’s online Sobel Test macro
(See Figure 1; http://quantpsy.org/sobel/sobel.htm). For the purposes of this study, the IV was
autistic symptoms, the DV was aggressive behavior (both proactive and reactive), and the
mediator was victimization by peers.
Results
A series of linear regressions were administered in order to determine if there was a
significant relation between the predictor variables (autistic symptoms and victimization by
peers) and the predicted variables (victimization by peers, proactive aggression, and reactive
aggression). As expected, results demonstrated that autistic symptoms significantly predicted
victimization (r =.24, p =.009) and proactive aggression (r =.48, p =.008), and victimization by
peers significantly predicted proactive aggression (r =.48, p =.001). However, though autistic
symptoms approached significance, it was not demonstrated to be a predictor of reactive
aggression (r =.16, p =.143). Additionally, victimization by peers was not a significant predictor
of reactive aggression (r =.08, p=.371). Therefore, reactive aggression was excluded from any
mediation testing. These results are found within Table 1.
Following these regression analyses, a mediation model was constructed in order to
assess whether the relation between severity of autistic symptoms and proactive aggression was
significantly mediated by victimization by peers (see Figure 2). Results demonstrated that the
mediation of victimization by peers was significant, diminishing the effect between autistic
symptoms and aggression (p <.05). These findings are indicative of a partial mediation.

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 10
Discussion
This study sought to further understand the relation between autistic symptoms and
aggression in youths with ASD. It was hypothesized that victimization by peers would prove to
be a significant mediator in this relation, therein reducing the effect that autistic symptoms had
on both proactive and reactive aggression.
Part of this hypothesis was confirmed; results did indicate that victimization by peers
significantly mediated the relation between autistic symptoms and proactive aggression in youths
with ASD. The results of this study place it in contrast to other literature, which found proactive
aggression being associated with less victimization by peers in neurotypical youth (Card and
Little et al., 2006). Although, this study supports research that has demonstrated elevated rates of
proactive aggression among youths with ASD (Pouw et al. 2012). There may be an attribute of
ASD that is not present in neurotypical youth that facilitates this relation between victimization
by peers and proactive aggression. However, this theory is in need of further support before any
conclusions may be drawn.
The results of this study also help to bridge the gap of past victimization research in
ASD. Victimization of ASD youths has been shown to be more prevalent than in neurotypical
youths, to be related to more severe impairment (Sreckovic et al. 2014), and to lead to increased
aggression (Rieffe et al. 2012). However, these three components have never before been
analyzed together. By examining this relation, this study is able to conclude that victimization by
peers serves as a significant variable in why ASD youths are engaging in more proactive
aggression.
Contrary to what was previously assumed, these results may suggest that social
interactions and pressures may play a pivotal role on aggression in youths with ASD. It is

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 11
possible that this social component could impact other problem behaviors of ASD (i.e. self-
injurious behaviors, tantrums, etc.) as well (Dominick et al. 2007). It has been suggested that
individuals with ASD “lack the basic ability to experience relationship-based emotions”
(Bauminger et al. 2008). However, this study’s finding may suggest that these youths are
responding to negative peer relationships in a way that is consistent with neurotypical youths
(Card & Little 2006). Apart from this study, little research has been devoted to examining the
effects of one’s social ecology on problem behaviors in individuals with ASD. There is a need
for further study on this subject.
In contrast to what was hypothesized, the results of this study did not find any support for
a model in which victimization by peers mediated the relation between autistic symptoms and
reactive aggression. Previous research has suggested that aggression toward peers in youths with
ASD is predominantly reactive, such that youths with ASD who are victimized by peers are
likely to respond with anger and engage in aggressive acts toward peers (Rieffe et al. 2012).
Though these findings were surprising, there are a wealth of factors that may have contributed to
the lack of reported reactive aggression in this study.
One such explanation could be that possible hostile attributional biases are driving
reactive aggression in youths with ASD (Dodge et al., 1990). Hostile attributional biases occur
when an individual interprets neutral cues as threatening ones. Aggression levels were indicated
by caregivers, while the experience of victimization by peers was reported by the youths
themselves. Therefore, there could be a discrepancy in how youths and their caregivers are
interpreting events. For example, youths with ASD may respond aggressively to another child
asking to play with a toy they are preoccupied with. To an observer, this may appear proactively
aggressive, but it may not feel so to the youth. It is possible that there is a discrepancy in how

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 12
this study identified reactive aggression (caregiver report) and how other literature has identified
it (youth report, teacher report; Pouw et al. 2012; Sreckovic et al., 2014).
Perhaps another explanation of the prevalence of proactive aggression as opposed to
reactive aggression has to do with Badura’s psychosocial theory of modeling (Bandura, 1973). It
is possible that many of these youths with ASD have associated aggression with instrumental
reward by modeling the behavior of those who are victimizing them. For example, if a classmate
were to threaten a child with ASD into giving them a toy they wanted, that same victim may
internalize that aggressive act as a means to an end. Viewing relationships superficially is a
common characteristic of ASD (Bauminger et al. 2008), therefore it is a real possibility that these
youths may have learned to use aggression toward their peers as a way to get what they want.
However, both the modeling theory and the hostile attributional theory are in need of testing
before any definitive conclusions can be drawn.
Informing treatment options is the most desired outcome of these results. The findings in
the present study may inform efforts aimed at reducing aggression in this clinical population of
youths. These treatments should consider that victimization by peers could lead to proactive
rather than reactive aggression. Interventions that directly target victimization by peers may be
needed to reduce aggressive behaviors in youths with ASD. However, further research may need
be dedicated to examine the effectiveness of these ecologically based treatments.
In summary, this study is the first to report victimization by peers as a mediator in the
relation between autistic symptoms and proactive aggression. Given the lack of any significant
predictive variables, no mediation model was conducted for reactive aggression. These results
reveal a large social impact on the behaviors of ASD youth, and should be considered in future
treatments efforts toward the problem behaviors of youths with ASD.
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 13
The current study has many limitations and is in need of future replication. Though there
were a considerable amount of participants involved in this study, a significantly larger sample
size is needed in order to make claims about the general population of youths with ASD.
Additionally, the C-SHARP measure was used in a way that it was not intended. This study
divided proactive and reactive aggression into separate summed scores, despite its original
purpose being devoted to consolidating responses into one aggression output. Future research
should consider using a measure designed to assess reactive and proactive aggression. The
MPVS is also limited in its ability to assess victimization by peers. It is designed to be simple
enough for youths of varying intellectual capacity to fill out accurately, but this simplicity results
in the sacrifice of intricacy. A more thorough measure of victimization by peers may also be
needed in future research.
This study is also limited in the conclusions it can make toward the mediation capacity of
victimization by peers in the relation of autistic symptoms and aggression. The regressions, as
well as the mediation model constructed afterwards, are unable to draw conclusions about the
causal direction of assessed variables. Future researchers should consider a longitudinal design in
order to assess any possible causal relations between autistic symptoms, victimization by peers,
and aggression. It is imperative that such a design begin research in early childhood in order to
properly evaluate causality, especially between victimization by peers and aggression.
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 14
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders
(5th ed). Author: Washington, DC.
Baker, B. L., Blacher, J., Crnic, K. A., & Edelbrock, C. (2002). Behavior problems and parenting
stress in families of three-year-old children with and without developmental delays. American
Journal on Mental Retardation,107(6), 433-444.
Bandura, A. (2010). Self-Efficacy. Corsini Encyclopedia of Psychology. 1–3.
Bauminger, N., Solomon, M., Aviezer, A., Heung, K., Gazit, L., Brown, J., & Rogers, S. J.
(2008). Children with autism and their friends: A multidimensional study of friendship in
high-functioning autism spectrum disorder. Journal of Abnormal Child Psychology, 36,
135-150.
Bronfenbrenner, U. (1977). The ecology of human development: Experiments by nature and
design. Cambridge, Mass.: Harvard University Press.
Card, N. A., & Little, T. D. (2006). Proactive and reactive aggression in childhood and
adolescence: A meta-analysis of differential relations with psychosocial adjustment.
International Journal of Behavioral Development, 30(5), 466–480.
Dodge, K.A., Price, J..M., Bachorowski, J., Newman, J.P. (1990). Hostile attributional biases in
severely aggressive adolescents. Journal of Abnormal Psychology, 99, 385-392.
Dominick, K.C., Davis, N.O., Lainhart, J., Tager-Flusberg, H., & Eolstein, S. (2007). Atypical
behaviors in children with autism and children with a history of language Impairment.
Research in Developmental Disabilities, 28, 145-162.
Farmer, C. A., & Aman, M. G. (2009). Development of the children's scale of hostility and
aggression: Reactive/proactive (C-SHARP). Research in Developmental Disabilities, 30,

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 15
1155-1167.
Farmer, C., & Aman, M. (2011). Aggressive Behavior in a sample of children with autism
Spectrum Disorders. Research in Autism Spectrum Disorders, 317-323.
Kaartinen, M., Puura, K., Helminen, M., Salmelin, R., Pelkonen, E., & Juujärvi, P. (2014).
Reactive aggression among children with and without autism spectrum disorder. Journal
of autism and developmental disorders,44(10), 2383-2391.
Kanne, S. M., & Mazurek, M. O. (2011). Aggression in children and adolescents with ASD:
Prevalence and risk factors. Journal of Autism and Developmental Disorders, 41, 926-
937.
Lam, K. S., & Aman, M. G. (2007). The Repetitive Behavior Scale-Revised: independent
validation in individuals with autism spectrum disorders. Journal of autism and
developmental disorders, 37(5), 855-866.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism Diagnostic Interview-Revised: a revised
version of a diagnostic interview for caregivers of individuals with possible pervasive
developmental disorders. Journal of autism and developmental disorders, 24(5), 659-685.
Lord, C., Risi, S., Lambrecht, L., Cook Jr, E. H., Leventhal, B. L., DiLavore, P. C., ... & Rutter,
M. (2000). The Autism Diagnostic Observation Schedule—Generic: A standard measure
of social and communication deficits associated with the spectrum of autism. Journal of
autism and developmental disorders, 30(3), 205-223.
Murphy, O., Healy, O., & Leader, G. (2009). Risk factors for challenging behaviors among 157
children with autism spectrum disorder in Ireland. Research in Autism Spectrum
Disorders, 3, 474-482.
Mynard, H., & Joseph, S. (2000). Development of the multidimensional peer‐victimization

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 16
scale. Aggressive Behavior, 26, 169-178.
Pouw, L. B., Rieffe, C., Oosterveld, P., Huskens, B., & Stockmann, L. (2013).
Reactive/proactive aggression and affective/cognitive empathy in children with
ASD. Research in Developmental Disabilities, 34, 1256-1266.
Preacher, K.J., & Leonardelli, G.J. (2001). Calulation for the Sobel test. Retrieved April 2016.
Rieffe, C., Camodeca, M., Pouw, L. B., Lange, A. M., & Stockmann, L. (2012). Don't anger me!
Bullying, victimization, and emotion dysregulation in young adolescents with
ASD. European Journal of Developmental Psychology, 9, 351-370.
Sreckovic, M.A., Brunsting, N.C., & Able, H. (2014). Victimization of students with autism
spectrum disorder: A review of prevalence and risk factors. Research in Autism Spectrum
Disorders, 8, 1155-1172.
Zhao, X., Lynch, J. G., & Chen, Q. (2010). Reconsidering Baron and Kenny: Myths and truths
about mediation analysis. Journal of Consumer Research, 37, 197-206.

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 17
Table 1
Predictor Variable Predicted Variable r B SE p
Autistic Symptoms
Victimization by peers .24 .011 .043 .009
Victimization by peers Proactive Aggression .24 1.016 .377 .008
Autistic Symptoms
Proactive Aggression .48 .096 .163 .001
Victimization by peers Reactive Aggression . 08 .27 .308 .371
Autistic Symptoms
Reactive Aggression .16 .216 .116 .143
Figure 1
Figure 2
Autistic
Symptoms
Proactive
Aggression
Victimization by peers
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 18
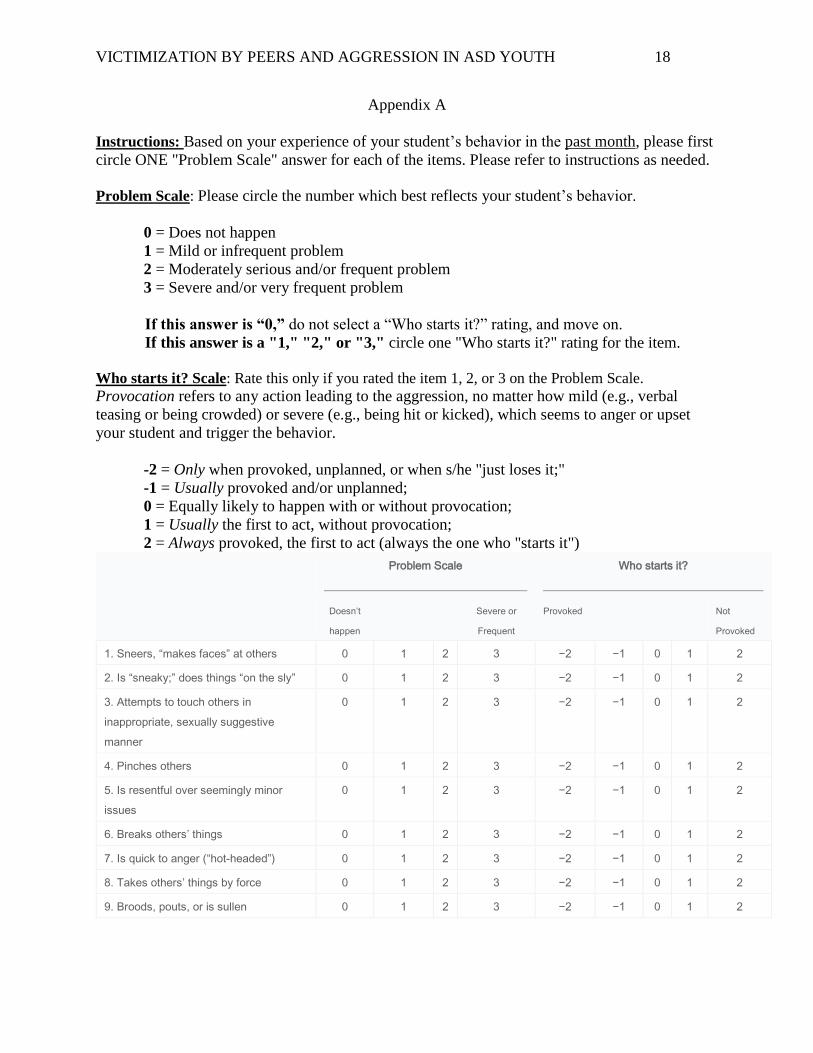
Appendix A
Instructions: Based on your experience of your student’s behavior in the past month, please first
circle ONE "Problem Scale" answer for each of the items. Please refer to instructions as needed.
Problem Scale: Please circle the number which best reflects your student’s behavior.
0 = Does not happen
1 = Mild or infrequent problem
2 = Moderately serious and/or frequent problem
3 = Severe and/or very frequent problem
If this answer is “0,” do not select a “Who starts it?” rating, and move on.
If this answer is a "1," "2," or "3," circle one "Who starts it?" rating for the item.
Who starts it? Scale: Rate this only if you rated the item 1, 2, or 3 on the Problem Scale.
Provocation refers to any action leading to the aggression, no matter how mild (e.g., verbal
teasing or being crowded) or severe (e.g., being hit or kicked), which seems to anger or upset
your student and trigger the behavior.
-2 = Only when provoked, unplanned, or when s/he "just loses it;"
-1 = Usually provoked and/or unplanned;
0 = Equally likely to happen with or without provocation;
1 = Usually the first to act, without provocation;
2 = Always provoked, the first to act (always the one who "starts it")
Problem Scale
Who starts it?
Doesn’t
happen
Severe or
Frequent
Provoked Not
Provoked
1. Sneers, “makes faces” at others 0 1 2 3 −2 −1 0 1 2
2. Is “sneaky;” does things “on the sly” 0 1 2 3 −2 −1 0 1 2
3. Attempts to touch others in
inappropriate, sexually suggestive
manner
0 1 2 3 −2 −1 0 1 2
4. Pinches others 0 1 2 3 −2 −1 0 1 2
5. Is resentful over seemingly minor
issues
0 1 2 3 −2 −1 0 1 2
6. Breaks others’ things 0 1 2 3 −2 −1 0 1 2
7. Is quick to anger (“hot-headed”) 0 1 2 3 −2 −1 0 1 2
8. Takes others’ things by force 0 1 2 3 −2 −1 0 1 2
9. Broods, pouts, or is sullen 0 1 2 3 −2 −1 0 1 2
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 19
Problem Scale
Who starts it?
Doesn’t
happen
Severe or
Frequent
Provoked Not
Provoked
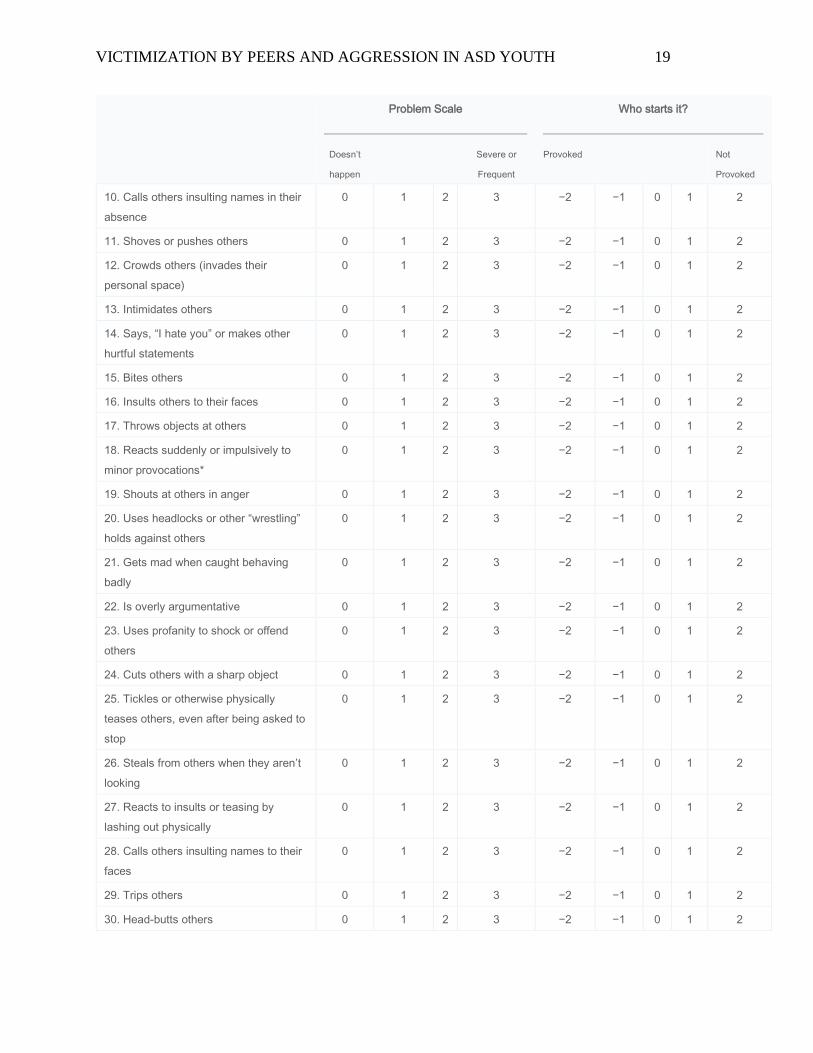
10. Calls others insulting names in their
absence
0 1 2 3 −2 −1 0 1 2
11. Shoves or pushes others 0 1 2 3 −2 −1 0 1 2
12. Crowds others (invades their
personal space)
0 1 2 3 −2 −1 0 1 2
13. Intimidates others 0 1 2 3 −2 −1 0 1 2
14. Says, “I hate you” or makes other
hurtful statements
0 1 2 3 −2 −1 0 1 2
15. Bites others 0 1 2 3 −2 −1 0 1 2
16. Insults others to their faces 0 1 2 3 −2 −1 0 1 2
17. Throws objects at others 0 1 2 3 −2 −1 0 1 2
18. Reacts suddenly or impulsively to
minor provocations*
0 1 2 3 −2 −1 0 1 2
19. Shouts at others in anger 0 1 2 3 −2 −1 0 1 2
20. Uses headlocks or other “wrestling”
holds against others
0 1 2 3 −2 −1 0 1 2
21. Gets mad when caught behaving
badly
0 1 2 3 −2 −1 0 1 2
22. Is overly argumentative 0 1 2 3 −2 −1 0 1 2
23. Uses profanity to shock or offend
others
0 1 2 3 −2 −1 0 1 2
24. Cuts others with a sharp object 0 1 2 3 −2 −1 0 1 2
25. Tickles or otherwise physically
teases others, even after being asked to
stop
0 1 2 3 −2 −1 0 1 2
26. Steals from others when they aren’t
looking
0 1 2 3 −2 −1 0 1 2
27. Reacts to insults or teasing by
lashing out physically
0 1 2 3 −2 −1 0 1 2
28. Calls others insulting names to their
faces
0 1 2 3 −2 −1 0 1 2
29. Trips others 0 1 2 3 −2 −1 0 1 2
30. Head-butts others 0 1 2 3 −2 −1 0 1 2

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 20
Problem Scale
Who starts it?
Doesn’t
happen
Severe or
Frequent
Provoked Not
Provoked
31. Makes insulting comments about
others behind their backs
0 1 2 3 −2 −1 0 1 2
32. Breaks own belongings 0 1 2 3 −2 −1 0 1 2
33. Makes threatening gestures (like
shaking fist)
0 1 2 3 −2 −1 0 1 2
34. Charges at others 0 1 2 3 −2 −1 0 1 2
35. Verbally teases others, even after
being asked to stop
0 1 2 3 −2 −1 0 1 2
36. If caught, denies having behaved
badly
0 1 2 3 −2 −1 0 1 2
37. Pulls others’ hair 0 1 2 3 −2 −1 0 1 2
38. When angry, is slow to cool off 0 1 2 3 −2 −1 0 1 2
39. Spits at others 0 1 2 3 −2 −1 0 1 2
40. Says “I hate [someone not present]”
or makes other hurtful statements in
absence of the person concerned
0 1 2 3 −2 −1 0 1 2
41. Chokes others/Grabs others’ necks 0 1 2 3 −2 −1 0 1 2
42. Lashes out at people who are in
his/her space
0 1 2 3 −2 −1 0 1 2
43. Takes offense at things others say
or do when s/he shouldn’t
0 1 2 3 −2 −1 0 1 2
44. Starts trouble by baiting others 0 1 2 3 −2 −1 0 1 2
45. If caught, makes excuses for bad
behavior
0 1 2 3 −2 −1 0 1 2
46. Is hostile, “has a chip on his/her
shoulder”
0 1 2 3 −2 −1 0 1 2
47. Scratches others with fingernails 0 1 2 3 −2 −1 0 1 2
48. Glares at others 0 1 2 3 −2 −1 0 1 2
49. Encourages others to gang up on
someone (physically OR verbally)
0 1 2 3 −2 −1 0 1 2
50. Hits others with objects 0 1 2 3 −2 −1 0 1 2
51. Is often grouchy 0 1 2 3 −2 −1 0 1 2
52. Doesn’t care about others’ feelings 0 1 2 3 −2 −1 0 1 2

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 21
Problem Scale
Who starts it?
Doesn’t
happen
Severe or
Frequent
Provoked Not
Provoked
53. Verbally threatens others with
physical harm
0 1 2 3 −2 −1 0 1 2
54. Hits or shoves others forcefully 0 1 2 3 −2 −1 0 1 2
55. Makes unwanted sexual comments
to others
0 1 2 3 −2 −1 0 1 2
56. Doesn’t seem truly sorry after
hurting someone
0 1 2 3 −2 −1 0 1 2
57. Gets revenge after some time has
passed and the other person is not on
guard
0 1 2 3 −2 −1 0 1 2
58. Tries not to get caught while doing
harmful things to others
0 1 2 3 −2 −1 0 1 2

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 22
Appendix B
Instructions:
Please rate your child’s behavior by reading each of the items listed and then choosing the score
that best describes how much of a problem the item is for the person. Be sure to read and score
all items listed. Make your ratings based on your observations and interactions with the person
over the last month. Use the definitions in the box given below to score each item.
0 = behavior does not occur
1 = behavior occurs and is a mild problem
2 = behavior occurs and is a moderate problem
3 = behavior occurs and is a severe problem
At the end of each section, there will be three questions asking you to rate that section’s
behaviors in terms of (a) how frequently they occur, (b) how upset the person becomes when
repetitive behaviors are interrupted, and (c) how much the behaviors interfere with ongoing
events. You will indicate the score by marking along each line, which represents a range of
frequencies and severities.
For example, if your child does those behaviors many times a day you may put the mark quite
close to the right side:
Never Constantly
I. Stereotyped Behavior Subscale
(DEFINITION: apparently purposeless movements or actions that are repeated in a similar
manner)
1. WHOLE BODY (Body rocking, Body swaying) 0 1 2
3
2. HEAD (Rolls head, Nods head, Turns head) 0 1 2
3
3. HAND/FINGER (Flaps hands, Wiggles or flicks fingers, Claps hands, Waves or shakes hand
or arm)
0 1 2 3
4. LOCOMOTION (Turns in circles, Whirls, Jumps, Bounces) 0 1 2
3
5. OBJECT USAGE (Spins or twirls objects, Twiddles or slaps or throws objects, Lets objects
fall out of hands) 0 1
2 3
6. SENSORY (Covers eyes, Looks closely or gazes at hands or objects, Covers ears,

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 23
Smells or sniffs items, Rubs surfaces) 0 1 2
3
Please answer the following questions about the behaviors described above (put a vertical mark (
) on the line to show your answer):
How often do they happen?
(If Never, skip to Section II) Never Constantly
How upset does your child get
when interrupted? Not at all Extremely
How much do these behaviors get
in the way of ongoing events? Not at all Severe
interference
0 = behavior does not occur
1 = behavior occurs and is a mild problem
2 = behavior occurs and is a moderate problem
3 = behavior occurs and is a severe problem
II. Self-Injurious Behavior Subscale
(DEFINITION: movement or actions that have the potential to cause redness, bruising, or other
injury
to the body, and that are repeated in a similar manner)
7. HITS SELF WITH BODY PART (Hits or slaps head, face, or other body area) 0
1 2 3
8. HITS SELF AGAINST SURFACE OR OBJECT (Hits or bangs head or other body part on
table, floor or other surface) 0
1 2 3
9. HITS SELF WITH OBJECT (Hits or bangs head or other body area with objects)
0 1 2 3
10. BITES SELF (Bites hand, wrist, arm, lips or tongue) 0 1
2 3
11. PULLS (Pulls hair or skin) 0 1
2 3
12. RUBS OR SCRATCHES SELF (Rubs or scratches marks on arms, leg, face or torso)
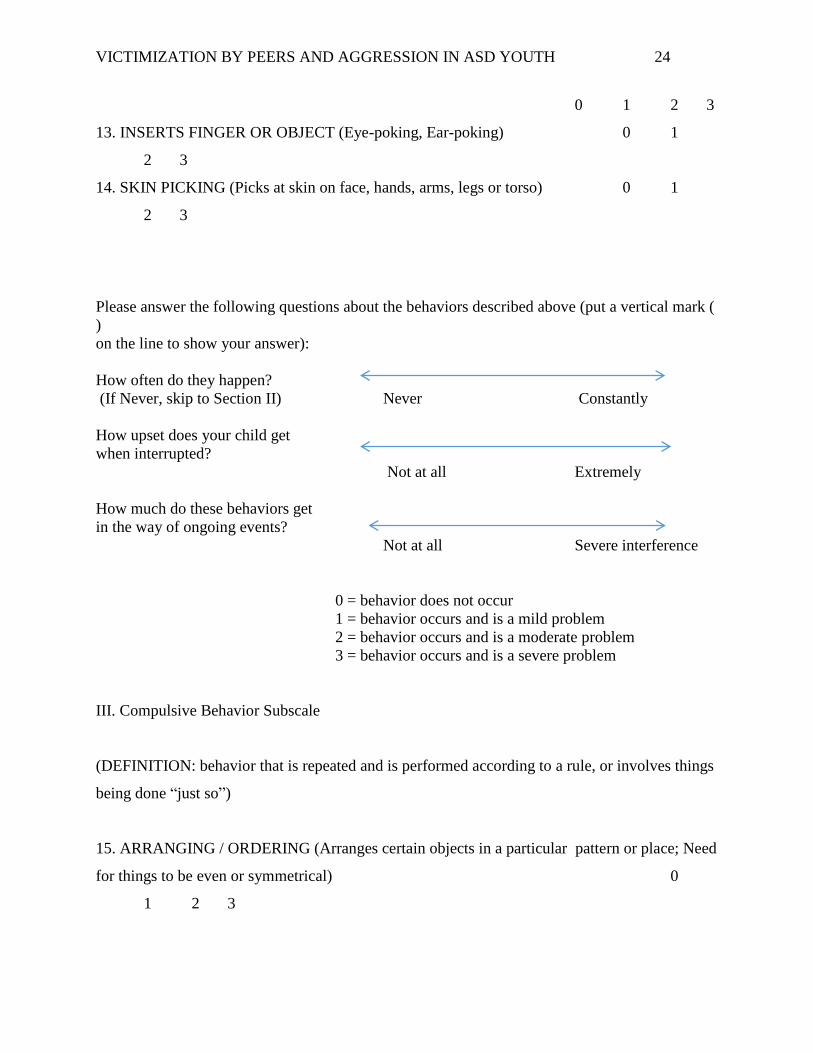
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 24
0 1 2 3
13. INSERTS FINGER OR OBJECT (Eye-poking, Ear-poking) 0 1
2 3
14. SKIN PICKING (Picks at skin on face, hands, arms, legs or torso) 0 1
2 3
Please answer the following questions about the behaviors described above (put a vertical mark (
)
on the line to show your answer):
How often do they happen?
(If Never, skip to Section II) Never Constantly
How upset does your child get
when interrupted?
Not at all Extremely
How much do these behaviors get
in the way of ongoing events?
Not at all Severe interference
0 = behavior does not occur
1 = behavior occurs and is a mild problem
2 = behavior occurs and is a moderate problem
3 = behavior occurs and is a severe problem
III. Compulsive Behavior Subscale
(DEFINITION: behavior that is repeated and is performed according to a rule, or involves things
being done “just so”)
15. ARRANGING / ORDERING (Arranges certain objects in a particular pattern or place; Need
for things to be even or symmetrical) 0
1 2 3

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 25
16. COMPLETENESS (Must have doors opened or closed; Takes all items out of a container or
area)
0 1 2 3
17. WASHING / CLEANING (Excessively cleans certain body parts; Picks at lint or loose
threads)
0 1 2 3
18. CHECKING (Repeatedly checks doors, windows, drawers, appliances, clocks, locks, etc.)
0 1 2 3
19. COUNTING (Counts items or objects; Counts to a certain number or in a certain way)
0 1 2 3
20. HOARDING/SAVING (Collects, hoards or hides specific items) 0 1
2 3
21. REPEATING (Need to repeat routine events; In / out door, up / down from chair, clothing
on/off)
0 1 2 3
22. TOUCH / TAP (Need to touch, tap, or rub items, surfaces, or people) 0 1
2 3
Please answer the following questions about the behaviors described above (put a vertical mark (
)
on the line to show your answer):
How often do they happen?
(If Never, skip to Section II) Never Constantly
How upset does your child get
when interrupted?
Not at all Extremely
How much do these behaviors get
in the way of ongoing events? Not at all Severe
interference
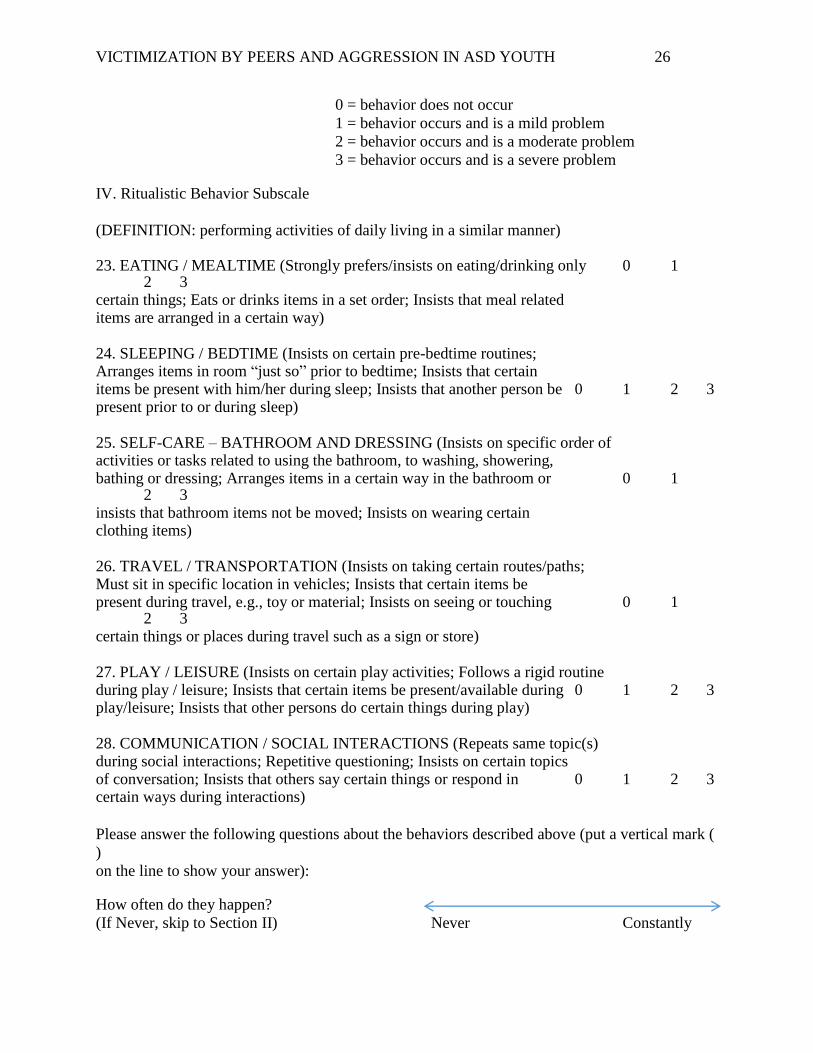
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 26
0 = behavior does not occur
1 = behavior occurs and is a mild problem
2 = behavior occurs and is a moderate problem
3 = behavior occurs and is a severe problem IV. Ritualistic Behavior Subscale
(DEFINITION: performing activities of daily living in a similar manner)
23. EATING / MEALTIME (Strongly prefers/insists on eating/drinking only 0 1 2 3 certain things; Eats or drinks items in a set order; Insists that meal related items are arranged in a certain way) 24. SLEEPING / BEDTIME (Insists on certain pre-bedtime routines; Arranges items in room “just so” prior to bedtime; Insists that certain items be present with him/her during sleep; Insists that another person be 0 1 2 3 present prior to or during sleep) 25. SELF-CARE – BATHROOM AND DRESSING (Insists on specific order of activities or tasks related to using the bathroom, to washing, showering, bathing or dressing; Arranges items in a certain way in the bathroom or 0 1 2 3 insists that bathroom items not be moved; Insists on wearing certain clothing items) 26. TRAVEL / TRANSPORTATION (Insists on taking certain routes/paths; Must sit in specific location in vehicles; Insists that certain items be present during travel, e.g., toy or material; Insists on seeing or touching 0 1 2 3 certain things or places during travel such as a sign or store) 27. PLAY / LEISURE (Insists on certain play activities; Follows a rigid routine during play / leisure; Insists that certain items be present/available during 0 1 2 3 play/leisure; Insists that other persons do certain things during play) 28. COMMUNICATION / SOCIAL INTERACTIONS (Repeats same topic(s) during social interactions; Repetitive questioning; Insists on certain topics of conversation; Insists that others say certain things or respond in 0 1 2 3 certain ways during interactions)
Please answer the following questions about the behaviors described above (put a vertical mark (
)
on the line to show your answer): How often do they happen?
(If Never, skip to Section II) Never Constantly
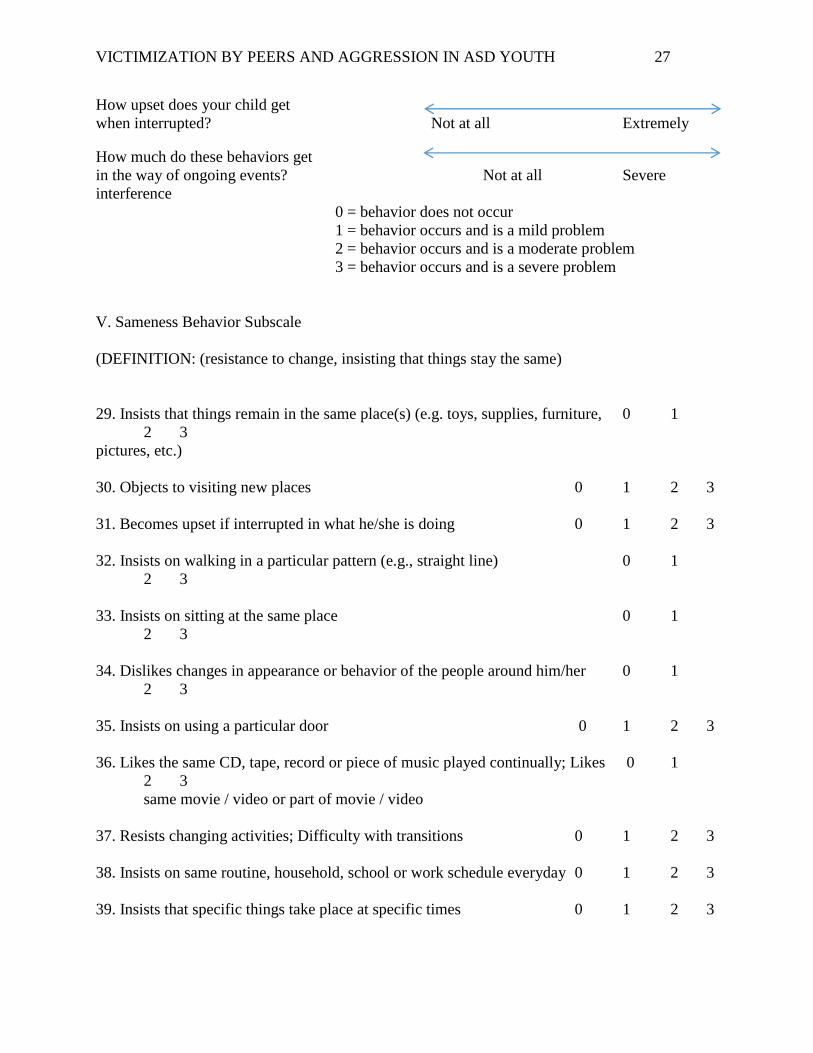
VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 27
How upset does your child get
when interrupted? Not at all Extremely How much do these behaviors get
in the way of ongoing events? Not at all Severe
interference
0 = behavior does not occur
1 = behavior occurs and is a mild problem
2 = behavior occurs and is a moderate problem
3 = behavior occurs and is a severe problem
V. Sameness Behavior Subscale
(DEFINITION: (resistance to change, insisting that things stay the same)
29. Insists that things remain in the same place(s) (e.g. toys, supplies, furniture, 0 1
2 3
pictures, etc.)
30. Objects to visiting new places 0 1 2 3
31. Becomes upset if interrupted in what he/she is doing 0 1 2 3
32. Insists on walking in a particular pattern (e.g., straight line) 0 1
2 3
33. Insists on sitting at the same place 0 1
2 3
34. Dislikes changes in appearance or behavior of the people around him/her 0 1
2 3
35. Insists on using a particular door 0 1 2 3
36. Likes the same CD, tape, record or piece of music played continually; Likes 0 1
2 3
same movie / video or part of movie / video
37. Resists changing activities; Difficulty with transitions 0 1 2 3
38. Insists on same routine, household, school or work schedule everyday 0 1 2 3
39. Insists that specific things take place at specific times 0 1 2 3

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 28
Please answer the following questions about the behaviors described above (put a vertical mark (
)
on the line to show your answer):
How often do they happen?
(If Never, skip to Section II) Never Constantly
How upset does your child get
when interrupted?
Not at all Extremely
How much do these behaviors get
in the way of ongoing events?
Not at all Severe interference
0 = behavior does not occur
1 = behavior occurs and is a mild problem
2 = behavior occurs and is a moderate problem
3 = behavior occurs and is a severe problem
VI. Restricted Behavior Subscale
(DEFINITION: Limited range of focus, interest or activity)
40. Fascination, preoccupation with one subject or activity (e.g., trains, 0 1
2 3
computers, weather, dinosaurs)
41. Strongly attached to one specific object 0 1 2 3
42. Preoccupation with part(s) of object rather than the whole object (e.g., 0 1 2 3
buttons on clothes, wheels on toy cars)
43. Fascination, preoccupation with movement / things that move (e.g., fans, 0 1
2 3
clocks)
Please answer the following questions about the behaviors described above (put a vertical mark (
)
on the line to show your answer):
How often do they happen?
(If Never, skip to Section II) Never Constantly
How upset does your child get
when interrupted?
Not at all Extremely

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 29
How much do these behaviors get
in the way of ongoing events?
Not at all Severe interference
FINAL QUESTION: Overall, if you “lump together” all of the behaviors described in this
questionnaire, how much of a problem are these repetitive behaviors (both for your child with
autism, as well as how they affect the people around them)? Please rate on a scale from 1 to 100,
where 1 = not a problem at all, and 100 = as bad as you can imagine:
Score from 1-100: ____________________

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 30
Appendix C
Please mark your answers below with an “x”. How often during the last school year has another student done these things to you?
1. Called me names _____ Not at all _____ Once _____ More than once
2. Tried to get me into trouble with my friends _____ Not at all _____ Once _____ More than once
3. Took something of mine without permission _____ Not at all _____ Once _____ More than once
4. Made fun of me because of my appearance _____ Not at all _____ Once _____ More than once
5. Made fun of me for some reason _____ Not at all _____ Once _____ More than once
6. Punched me _____ Not at all _____ Once _____ More than once
7. Kicked me _____ Not at all _____ Once _____ More than once
8. Hurt me physically in some way _____ Not at all _____ Once _____ More than once

VICTIMIZATION BY PEERS AND AGGRESSION IN ASD YOUTH 31
9. Beat me up _____ Not at all _____ Once _____ More than once
10. Tried to break something of mine _____ Not at all _____ Once _____ More than once
11. Tried to make my friends turn against me _____ Not at all _____ Once _____ More than once
12. Stole something from me _____ Not at all _____ Once _____ More than once
13. Refused to talk to me _____ Not at all _____ Once _____ More than once
14. Made other people not talk to me _____ Not at all _____ Once _____ More than once
15. Deliberately damaged some property of mine _____ Not at all _____ Once _____ More than once
16. Swore at me _____ Not at all _____ Once _____ More than once