handbook on assessment and evaluation in early childhood … · the handbook on assessment and...
TRANSCRIPT

i
Handbook on Assessment and Evaluation in Early Childhood
Special Education
ProgramsCalifornia Department of Education • Sacramento • 2000

ii
Prepared for publicationby CSEA members.
Publishing Information
STATE
OF CALIFORNIA
DE
PA
RTMENT OF EDUCATION
The Handbook on Assessment and Evaluation in Early Childhood SpecialEducation Programs was developed by the Special Education Division,California Department of Education. This publication was edited by FayeOng working in cooperation with Ellen Broms, Consultant, SpecialEducation Division, California Department of Education. It was designedand prepared for printing by the staff of CDE Press, with the cover andinterior design created and prepared by Paul Lee. Typesetting was done byGloria Barreiro and Carey Johnson. It was published by the Department ofEducation, 721 Capitol Mall, Sacramento, California (mailing address: P.O.Box 944272, Sacramento, CA 94244-2720). It was distributed under theprovisions of the Library Distribution Act and Government Code Section11096.
© 2000 by the California Department of EducationAll rights reserved
ISBN 0-8011-1463-2
Special AcknowledgmentThe Special Education Division extends its appreciation to Jan Kearns,Early Childhood Services, Shasta County Office of Education, principalauthor, and to field reviewers Deborah Chen, California State University,Northridge; Janine Swanson, Chris Drouin, and Margaret Benavides,Consultants, Early Education Unit; Maureen Ballard-Rosa; Pamm Shaw;Robin Reves; and Shirley Stihler.
Ordering InformationCopies of this publication are available for $13.50 each, plus shipping andhandling charges. California residents are charged sales tax. Orders maybe sent to CDE Press, Sales Office, P.O. Box 271, Sacramento, CA 95812-0271; FAX (916) 323-0823. Prices on all publications are subject to change.
A partial list of educational resources available from the Departmentappears on page 69. In addition, an illustrated Educational ResourcesCatalog describing publications, videos, and other instructional mediaavailable from the Department can be obtained without charge by writing tothe address given above or by calling the Sales Office at (916) 445-1260.
Photo CreditsThe California Department of Education gratefully acknowledges MichaelSalcedo of the SEEDS project for the use of the photos in this document.
NoticeThe guidance in Handbook on Assessment and Evaluation in EarlyChildhood Special Education Programs is not binding on local educationalagencies or other entities. Except for the statutes, regulations, and courtdecisions that are referenced herein, the document is exemplary, andcompliance with it is not mandatory. (See Education Code Section33308.5.)

iii
Contents
Preface ................................................................................................................................. v
Introduction ......................................................................................................................... 1
Teams Assessing Preschool-Age Children .......................................................................... 4
Types of Assessment Teams ............................................................................................ 4
Composition of the Team................................................................................................. 8
Eligibility of Infants and Toddlers ..................................................................................... 11
Disabling Conditions ..................................................................................................... 11
Need for Intensive Special Education and Services ...................................................... 12
Infants and Toddlers with a Solely Low-Incidence Disability ...................................... 13
Assessment of the Developmental Domains of Infants and Toddlers ............................... 14
Cognitive Domain ......................................................................................................... 14
Physical Development Domain ..................................................................................... 15
Health Domain............................................................................................................... 15
Communication Domain ............................................................................................... 15
Social–Emotional Domain............................................................................................. 16
Adaptive Domain........................................................................................................... 16
Family Assessments........................................................................................................... 17
Eligibility of Preschool-Age Children ............................................................................... 19
Assessment of All Areas of the Suspected Disability of Preschool-Age Children........ 21
Assessment for Autism .................................................................................................. 22
Assessment for Speech and Language Disorders .......................................................... 22
Assessment for a Specific Learning Disability.............................................................. 23
Assessment for Visual Impairments .............................................................................. 23
Assessment for Hearing Impairments............................................................................ 24
Assessment for Orthopedic Impairments ...................................................................... 24
Assessment for Emotional Disturbance......................................................................... 25

iv
Preparation for the Assessment.......................................................................................... 26
Information from Parents or Guardians ......................................................................... 28
Information from Other Sources.................................................................................... 28
Cultural Diversity in Assessment .................................................................................. 30
Assessment Methods ......................................................................................................... 31
Screening Tools ............................................................................................................. 31
Traditional Methods....................................................................................................... 32
Alternative Methods ...................................................................................................... 33
Assessment of Children with Low-Incidence Disabilities ................................................ 36
Hearing Impairment ....................................................................................................... 36
Visual Impairment ......................................................................................................... 37
Severe Orthopedic Impairment ...................................................................................... 38
Deaf-Blind .....................................................................................................................38
Report of the Findings ....................................................................................................... 39
Program Planning .............................................................................................................. 42
Staff Development for Assessors ....................................................................................... 44
Conclusion ......................................................................................................................... 46
Appendixes
A. Pertinent Legal Citations .......................................................................................... 48
B. Qualifications of Interpreters .................................................................................... 51
C. Guidelines for Working with Interpreters ................................................................. 52
D. Parent Interview Strategies ....................................................................................... 54
E. Sample Cover Letter and Interagency Consent to Share Information ...................... 55
F. Resources for Technical Assistance ........................................................................... 57
Glossary ............................................................................................................................. 60
Selected References ........................................................................................................... 66

v
Preface
The early years are the foundationfor a child’s healthy develop-
ment and readiness forlifelong learning. For youngchildren with disabilities,development and learning in
the early years depend on thequality of early intervention services.This handbook provides information onthe development and maintenance ofquality programs, the statutory andregulatory requirements, and the re-sources available to local educationalagencies to support those programs.
Background
Infant and toddler and preschool specialeducation programs and services havechanged substantially in recent years. Theimplementation of Senate Bill 1085 in1993 established the Early Start inter-agency program in collaboration with theCalifornia Department of DevelopmentalServices (DDS). This program providesearly intervention services that are indi-vidually designed for infants and toddlersfrom birth through two years of age andtheir families. Funding is provided underPart C of the Individuals with DisabilitiesEducation Act (20 USC Section 1471 etseq.) to develop innovative ways of
providing family-focused, coordinatedservices that are built on existing systems.
Preschool special education pro-grams received a boost from the federalgovernment with the increased funds andexpansion of eligibility categories forchildren with disabilities between the agesof three and five years under Title II of theEducation of the Handicapped ActAmendments of 1986, Public Law 99-457(20 USC sections 1411, 1412, 1413, and1419).
California state law, Chapter 311(AB 2666, Hannigan, Statutes of 1987),established program standards for allpreschoolers with exceptional needs inCalifornia. Prior to enactment of this law,public schools in California were man-dated to serve only preschool childrenrequiring intensive special education andservices.
Principles of Early ChildhoodSpecial Education ServiceDelivery
The handbooks in the Early ChildhoodSpecial Education series are based on thefollowing principles:• Early childhood special education
programs must be child-centered.• Programs should be family-focused.

vi
• Programs should be culturally sensitive.
• Collaborative interagency coordinationis the most efficient and effective wayto provide services to families.
• Programs should provide transdisciplin-ary approaches to the assessment ofchildren and delivery of services.
• Programs should provide opportunitiesfor staff development.
• Program evaluation is a necessarycomponent of special education pro-grams and services.
Purpose of the Handbook
The Early Education Unit of the SpecialEducation Division, California Depart-ment of Education, is providing staff inthe field with a resource that presentsquality criteria for best practices in pro-gram development, ideas, and concepts inthe context of the statutory requirements
for early childhood special educationprograms. New federal and state statutesand changed regulations and fundingmechanisms have affected the provision ofservices for young children with disabili-ties. Such changes make it necessary toupdate and expand the Preschool SpecialEducation Program Handbook (publishedin 1988) to include information on theinfant and toddler early interventionprograms.
Each handbook in the Early Child-hood Special Education series describescore concepts and best practices that arebased on an in-depth review of currentliterature, statutes, and regulations. Thesehandbooks may be accessed on theDepartment’s Web site.
We thank the parents and educatorswho contributed the ideas in this handbookto make it a valuable resource for adminis-trators, teachers, and family members.
HENRY DER
Deputy SuperintendentEducation Equity, Access, and Support Branch
ALICE D. PARKER
DirectorSpecial Education Division

1
Introduction
T his handbook provides informa-tion that reflects the preferred
practices in the field of evaluationand assessment of children agesbirth through five years. It presents
guidelines with references togive service providers direction
in how to accurately evaluate and assessthis age group. The requirements of theindividualized family service plan (IFSP)under the Individuals with DisabilitiesEducation Act (IDEA), Part C, and thosefor the individualized education program(IEP) under IDEA, Part B, are included.Appendix A contains the statutory andregulatory requirements regarding theevaluation and assessment of youngchildren.
Evaluation may be defined as the actof determining a child’s eligibility forspecial education. Assessment is a processthrough which one determines the child’sabilities and need for services. Evalua-tions and assessments of infants, toddlers,and preschoolers are conducted differ-ently from those of older children. Duringdevelopment a young child will act differ-ently from one situation to another andeven from one time of day to another.Changes in the environment, the child’sphysical state, and the interactions that a
The process of screening and as-sessment goes beyond scores, stan-dard deviations, and levels offunctioning. It is often a family’sfirst introduction to the humanservice or educational system andit is potentially a short-term thera-peutic experience in itself. Forexaminers, tests and other proce-dures may be used to organizeobservations about a child andfamily rather than merely as away to control eligibility for ser-vices. Assessment, in particular,should be approached as an ongo-ing, dynamic process with multiplecomponents, including case man-agement, family support, transi-tional programs, and thedevelopment of the IFSP/IEP.
—Samuel Meisels and Sally Provence,Screening and Assessment: Guidelines forIdentifying Young Disabled and DevelopmentallyVulnerable Children and Their Families

2
child has with significant people in his orher life may have a critical impact on howa young child will react to evaluation set-tings and procedures.
To address the differences betweenyoung children and older children, pro-grams may use a multidisciplinary, inter-disciplinary, or transdisciplinary teamapproach. A child may not respond to tra-ditional evaluation and assessment meth-ods; consequently, alternative proceduresmay be the only way in which to obtainaccurate information. Tools may includestandardized assessment measures andalternative approaches, including play-based assessments and clinical observa-tions of the child in a variety of settings.(See the glossary for definitions of termsthat are used regarding evaluation andassessment.)
The following concepts represent thepreferred practices in early childhoodevaluation and assessment:1
• A collaborative evaluation/assessmentprocess includes families as providersof information and as team members.
• A transdisciplinary team knowledgeablein all areas of child development,including typical and atypical develop-ment and family systems, conducts theassessments. As part of the assessmentteam, families are given the opportunityto learn about the procedures, observa-tions of the professionals, and interpre-tations of the data. The result of theassessment is a coordinated interventionplan.
• The evaluation/assessment team looksat the child in the context of the family,culture, and community, interpretinginformation about the child in thechild’s environment. According to theCalifornia Code of Regulations,
Title 17, Section 52084(e), evaluationsand assessments must be conducted innatural environments whenever pos-sible. An ecological model of assess-ment allows the interaction between achild and the environment to be judgedin the context of his or her daily activi-ties and routines and to be enhanced byenvironmental support. The assessormust focus ongoing assessment on thechild’s developmental skills, chal-lenges, and individual differences andon the child’s responses alone and insocial interactions in different experi-ences and settings and with differentpeople throughout the day.
• The assessment team focuses on theconcerns of the family, referral sources,service providers, and specific require-ments regarding the child’s eligibilityfor programs.
• The assessment team considers thereliability and validity of the variousprocedures for the child and the familywhen choosing observation strategiesand assessment measures.
• The evaluation or assessment teamdesigns procedures to obtain appropri-ate information for determining achild’s eligibility for programs and hisor her progress and for planning inter-vention strategies.
• The team provides a written report thatcommunicates the results and recom-mendations in lay terms without jargonto parents and program providers.
Personnel who assess children agesbirth to five years should adopt a philoso-phy about assessment practices. Thepublication Guidelines and RecommendedPractices for the Individualized FamilyService Plan identifies the following
1 Adapted from Linda Brekken, “Key Points in Assessing Preschoolers and Their Families,” in Preschool SpecialEducation Program Handbook. Sacramento: California Department of Education, 1988.

3
principles regarding the evaluation andassessment of young children:2
• Informed consent must be obtainedfrom a family for all initial evaluationand assessment activities.
• Assessment must be nondiscriminatory.Children should be assessed for theirstrengths and needs, with the assess-ment team showing sensitivity to theimpact of the disability on the child.
• The evaluation/assessment processshould be conducted in the languagepreferred by the family wheneverpossible. (See the Code of FederalRegulations, Section 300.532 [a] [1][ii], in Appendix A.)
2 Guidelines and Recommended Practices for the Individualized Family Service Plan (Second edition). Edited byMary McGonigel and others. Bethesda, Md.: National Early Childhood Technical Assistance System (NECTAS)and Association for the Care of Children’s Health (ACCH), 1991, p. 40.
• The child’s assessment should beshaped by the family’s priorities andneed for information as well as by thechild’s characteristics and by diagnosticconcerns.
• The evaluation/assessment processmust reflect a respect for family valuesand different styles of decision making.
• In a team assessment process, allinformation is shared freely among theteam members.
• Family members are an integral part ofany team and have the opportunity toattend evaluation/assessment sessionsand participate in all discussions.

4
Team Assessment ofPreschool-Age Children
M any early childhood programsuse some form of collaborationto assess and plan an appropri-
ate program for young children. In a studyof preschool assessment practices inCalifornia, researchers found variationsin team composition; namely, multidisci-plinary, interdisciplinary, and transdisci-plinary. Many programs that were beingstudied were changing, reflecting anincrease in team-based assessment practices.3
Types of Assessment Teams
Team approaches differ in theamount of direct contact and
interaction that team membershave with one another during theassessment process. In the multi-
disciplinary team approach, there is verylittle contact between professionals.Children are assessed, and decisions andrecommendations are made by profession-als independently.
The interdisciplinary team approachis one in which professionals maintaintheir role in a specific discipline but work
3 Maureen Ballard-Rosa and others, PreschoolAssessment Practices in California: Characteristics andIssues of Alternative Approaches. Sacramento:California Department of Education, 1996.
5
together with the child and family. Theteam makes decisions and recommenda-tions as a group, but each professional onthe team has a role in implementing theprogram once it is determined.
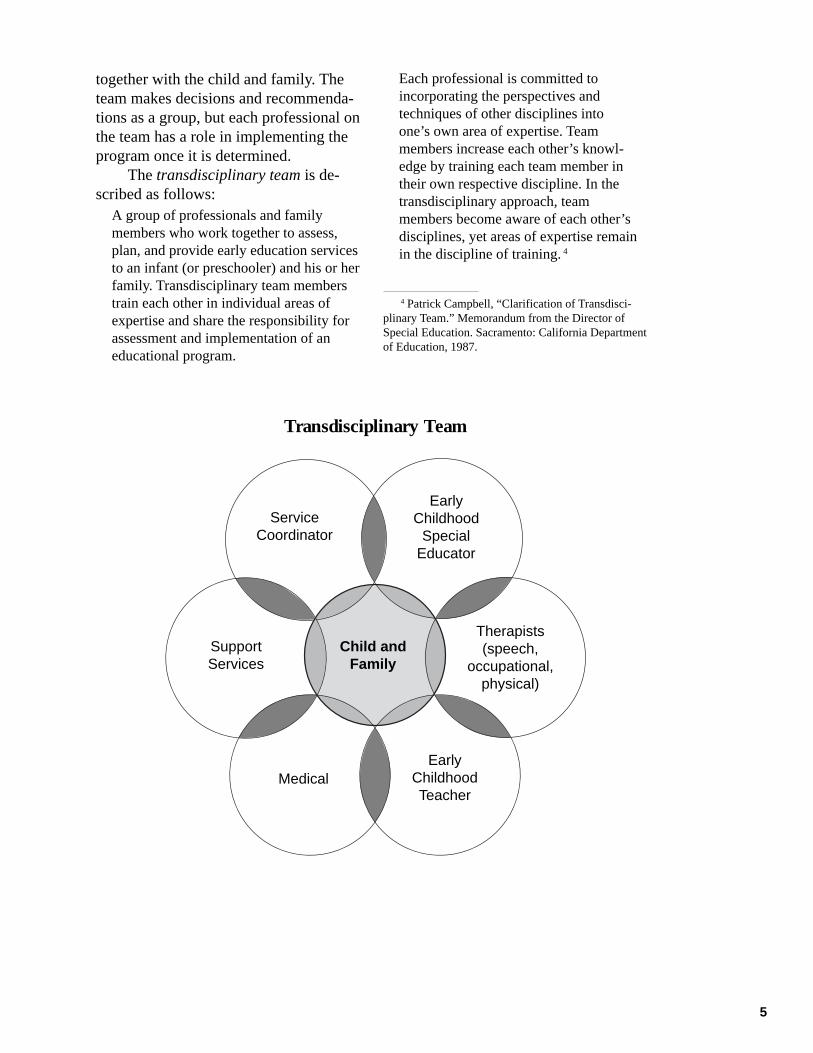
The transdisciplinary team is de-scribed as follows:
A group of professionals and familymembers who work together to assess,plan, and provide early education servicesto an infant (or preschooler) and his or herfamily. Transdisciplinary team memberstrain each other in individual areas ofexpertise and share the responsibility forassessment and implementation of aneducational program.
Each professional is committed toincorporating the perspectives andtechniques of other disciplines intoone’s own area of expertise. Teammembers increase each other’s knowl-edge by training each team member intheir own respective discipline. In thetransdisciplinary approach, teammembers become aware of each other’sdisciplines, yet areas of expertise remainin the discipline of training.4
4 Patrick Campbell, “Clarification of Transdisci-plinary Team.” Memorandum from the Director ofSpecial Education. Sacramento: California Departmentof Education, 1987.
Transdisciplinary Team
ServiceCoordinator
EarlyChildhood
SpecialEducator
Child andFamily
SupportServices
Therapists(speech,
occupational,physical)
MedicalEarly
ChildhoodTeacher

6
Transdisciplinary Early Childhood Assessment Teams
The early childhood special education assessment team is a well-established component of quality early intervention programs. Implementinga transdisciplinary team assessment model requires additional staff training,reallocation of staff time, and revision of schedules to conduct team assess-ments. These initial investments in staff training and time yield many benefitsto the children and families served. The reasons for implementing a trans-disciplinary team assessment model in early childhood special education andinfant and preschool programs are as follows:
• The various areas of development overlap in the young child and are lessdifferentiated than in the older child. Therefore, behaviors are more difficultto separate into discipline-specific realms. A single behavior may involveaspects of cognitive, motor, language, and emotional development. When ateam observes the same behavior, each member can provide a unique per-spective and interpretation based on expertise in a particular discipline.Thus, a total picture of the child emerges.
• The whole [assessment result] is greater than the sum of its parts. The teamprocess provides a more valid and complete synthesis of assessment resultsthan individual reports put together.
• Teaming is an efficient process that saves time for both staff and families byreducing the duplication of assessment services.
• The quality of the observations, assessments, and reports is improved.Teaming improves the accuracy of the observations, assists in the recall ofspecific behaviors, allows synthesis of the information, and provides valida-tion of the observations and recommendations regarding the child’s func-tioning.
• Observations and recommendations are consistent, and the family does notreceive conflicting information. The team process allows one of the teammembers to work with the family to explain the process and clarify assess-ment activities, providing an educational experience for the family duringthe assessment. The development of a parent–professional partnership at theinitial contact establishes the family’s trust in the system and allows forimmediate verification and validation of the assessment results.
• Team members receive the benefit of learning from one another so that theyare all enriched in their knowledge of child development.
• Team assessment provides an integrated picture of the whole child withinthe family system and community. The synthesis of information provides amuch broader and more accurate view of the child and family.
The composition of the transdisciplinary early childhood special educa-tion assessment team is dependent on the program’s resources, the skills of thestaff, and the family’s and child’s needs. The assessment team should developa philosophy and service delivery model that reflects and responds to thesevariables.

7
Examples of the composition and functions of a transdisciplinary assess-ment team model are as follows:
• Two to three team members assess all children. Consultants in specialareas are added to the team as needed.
• The team composition is developed individually for each child and familyto meet individual needs.
• An interagency team (i.e., consisting of Head Start and local educationalagency staff) assesses all children.
• The entire team assesses all children.
These models are not inclusive. Each program should develop atransdisciplinary early childhood special education assessment model thatmeets the particular needs of the program, family, and community.
Adapted from Linda Brekken and Gina Guarneri, “Rationale for Transdisciplinary Early ChildhoodAssessment Teams,” in Preschool Special Education Program Handbook. Sacramento: CaliforniaDepartment of Education, 1988.
It is important for the staff to exam-ine the current practices of itsprogram by asking the followingquestions:
• What approach is being used (e.g.,individual professional or a multi-disciplinary, interdisciplinary, trans-disciplinary, or transitional team) forassessment?
• Does the current approach match thephilosophy of the program?
• Does administrative support exist for ateam model?
• What is the goal of the program?• What changes need to be made to
develop a stronger team?• What barriers hinder implementation of
the new approach?• What staff development should occur
for the program to be successful?• What is the timeline for implementing
the change?
Radford and Wolfe identified somecommon concerns in the development of
successful teams.5 Although most effec-tive in developing transdisciplinary teams,these concerns apply to interdisciplinaryteams as well:
• Develop an assessment philosophy.• Establish team goals.• Clarify team priorities.• Identify the specific steps and actions
to be included in assessments.• Allocate sufficient time to share obser-
vations, results, and recommendations.• Define the skills needed by the team.• Define roles and responsibilities of
team members.• Create a system of team support.• Define the process for team decision
making.• Establish linkages with other programs
and services.• Plan for ongoing team development.
Even in programs that operatetransdisciplinary teams, teaming issuesshould be revisited on a regular basis to
5 Adapted from Linda Radford and Sheila Wolfe, “Development of an Early Childhood Assessment Team,” inPreschool Special Education Program Handbook. Sacramento: California Department of Education, 1988.
8
maintain continuity. Some factors that mayaffect a team include the following:
• Changes in personnel• Changes in laws and regulations that
may require altering established proce-dures
• Allocation of adequate time for the teamprocess
• Changes in workload or assignments ofindividual team members
• Changes in the assessment approach
Composition of the Team
Administrators should consider whowill participate and how the team
will function. The followingguidelines should be kept in
mind:
• The core infant and preschool assess-ment personnel are qualified and areinterested, experienced, and trained inthe assessment of infants and preschool-age children.
• To maintain continuity of the trans-disciplinary team, administrators shouldmake a commitment to stable staffingwhen assigning core assessment per-sonnel.
• The assessment team must include theparent or guardian and may consist ofthe following members:
—General education teacher or childcare provider
—Early childhood special educationteacher
—School nurse—School psychologist—Speech, language, and hearing
therapist
• If a child is suspected of having a low-incidence disability, an assessor who iscertified in the specific low-incidencedisability is required to participate aspart of the team (pursuant to EducationCode Section 56320[g]).
• Qualified school personnel who shouldbe involved in the assessment of a childwith a low-incidence disability (de-pending on the disability) are asfollows:
—Interpreter/translator—Adaptive physical education teacher—Occupational or physical therapist—Teacher of children who are visually
impaired—Orientation-and-mobility specialist—Teacher of children who are deaf or
hard of hearing—Teacher of children who are orthope-
dically impaired—Program specialist—Assistive technology specialist
• The size and makeup of the team mayvary, depending on the age and needsof the child, family preferences, andlocation of the evaluation.
• Sufficient clerical support is necessaryto coordinate referrals, set up IEP/IFSPmeetings, and prepare necessary reportsand documents.
• Others who may be involved in assess-ment, when appropriate, include thefollowing:
—Community service providers—Medical specialists—Personnel from such agencies as the
regional center, a public healthdepartment, or a mental healthcenter; Women, Infants, and Chil-dren (WIC) Nutrition Program; andCalifornia Children Services (CCS)
• The child’s teacher or child care pro-vider may be a valuable source ofinformation.
The roles among preschool assessmentpersonnel may be considerably blurred,depending on the skills of the assessmentpersonnel, the amount of time available,and established staff agreements. Theselection of participants in the assessmentprocess is determined in part by the type

9
of assessment required and the suspecteddisability. However, the assessment teamalways includes the parents and otherpersons requested by the parents for theirknowledge of the child and family. Teammembers are selected on the basis of theirspecial expertise, the preference of thefamily, and language skills.
Parents or guardians: The child’s parentsor guardians are central to the assessmentof young children. IDEA ’97 requires theparents to be a part of the team thatdetermines their child’s eligibility forspecial education services. The parentsparticipate in the development of theassessment plan to ensure that familyconcerns are addressed; to determine theamount of assessment that will take placein the home; to determine the family’slevel of participation; to provide assess-ment information; and to help link assess-ment to their concerns, resources, andpriorities for their child. Parents whoaccept a specific responsibility, such asengaging the child in a play activity,become more directly involved in theassessment process.
Early childhood general educationteacher or care provider: In a preschool,child care center, or family child carehome, the general education teacher’s orcare provider’s responsibility may includescreening the child, providing a referral,consulting with team members, and actingas a liaison between the parent and theschool and between the parent and assess-ment personnel. The classroom or groupsituation is often the setting of the child’sinitial school experience. The teacher orcare provider is frequently the first trainedobserver of a child’s growth and develop-ment. His or her informal assessmentsprovide valuable documentation of achild’s skills, talents, abilities, and needsthat lead to referral for further assessmentwhen appropriate. After receiving aparent’s signed consent, the general
education teacher or care provider in-cludes the developmental informationwhen making the referral to the assess-ment team. He or she can facilitate theflow of information to parents, helping toincrease the family’s understanding of andinvolvement in the assessment process.
Early childhood special educationteacher: The teacher’s responsibility mayinclude assisting in identifying andaddressing the individual needs of a child.The teacher may provide observations ofthe child in a variety of settings andactivities and participate with the assess-ment team in assessing the child. Theteacher assists in writing realistic goalsand objectives or outcomes for each childand monitors the progress of the childwithin the placement setting.
Nurse: The nurse’s responsibility mayinclude obtaining a relevant health anddevelopmental history from the child’sparents, the medical community, andother community agencies. A nurse willtypically evaluate the child’s currenthealth and nutritional status (includingdental health), vision, hearing, immuniza-tions, and sleep patterns and, when rel-evant, screen the child’s self-help skills,fine and large motor skills, and social–emotional development, including parent–child interactions. Evaluating the special-ized health care needs of a child and theimpact of those needs on educationalplacement and learning is of criticalimportance. Because health issues mayhave a significant impact on a youngchild’s development, all infants andtoddlers referred are required to receive atthe minimum an assessment for hearingand vision as part of the health statusdetermination. Nurses should also com-municate with primary care physiciansand specialists to obtain the most currentinformation on medications, equipment,technology, and special services neededby the child.

10
Psychologist: The school psychologist’sresponsibility involves both formal andinformal assessment of a child’s overallfunctional level. The psychologist as-sesses a child’s coping skills, social–emotional skills, parent–child interaction,school readiness skills, cognitive develop-ment, and general adaptive behavior. Heor she may assist in integrating evalua-tions from other persons participatingin the assessment and take the majorresponsibility for preparing the psycho-educational team report. The psychologistalso assists in identifying the child’spreferred learning style.
Speech, language, and hearing therapist:The speech, language, and hearingtherapist’s responsibility is to assess thechild’s speech, language, and other com-munication development and determinewhat interventions, if any, are necessaryto correct identified problems. A speechand language evaluation needs to beconsidered for nearly all children in thisage range because speech and languagedevelopment is a critical developmentalarea for young children. The speech andlanguage developmental level ascertainedby the therapist represents essential infor-mation in determining a child’s overalldevelopmental and educational needs.In many cases the decision to seek addi-tional assessment information is based onthe results of the speech and languageevaluation.
Interpreter/translator: The responsibilityof the interpreter/translator is to assist theassessment personnel in gathering infor-mation from the family, explaining theassessment process, administering theevaluation, and translating written infor-mation between the program personneland the family. An interpreter primarily
exchanges the information between thefamily and staff orally, and the translatorprovides the required information in writ-ten form. A sign language interpreterprovides visual interpretation of the infor-mation that was presented orally. The in-terpreter/translator may be an invaluableresource in identifying cultural issues andvalues and in training personnel to recog-nize them and their potential impact on theassessment process for the child and fam-ily. See Appendixes B and C for additionalinformation about using interpreters.
Auxiliary personnel: Auxiliary personnelin assessment may include the adaptivephysical education teacher; occupationalor physical therapist; audiologist; andspecialists in the areas of visual, orthope-dic, and hearing impairments. Dependingon the nature of the referral, the suspecteddisability of the child, and the makeup ofthe assessment team, those individualsmay participate in the assessment. Theirprimary responsibility in assessment is toprovide evaluation and expertise related totheir specific discipline; assist the team indetermining the child’s and family’seligibility and making recommendationsabout placement and services; and developgoals, objectives, and outcomes suited tothe child and family.
Administrator or service coordinator: Theadministrator or service coordinator isresponsible for overseeing the assessmentprocess and for ensuring that the team hasadequate training, materials, and time forthe appropriate assessment of youngchildren. Although some administrativeresponsibilities may be delegated, theprogram administrator or service coordi-nator must ensure accountability in, andcoordination of, the assessment process.

11
The law states that an infant ortoddler must have a disability tobe eligible for special education
and related services and need intensivespecial education and services because ofthat disability (Education Code, Part 30,Section 56026). California Code of Regu-lations (CCR), Title 5, Section 3030, ismore specific about the definition of adisability, and Section 3031 details whichchildren are considered in need of inten-sive special education and services.
Disabling Conditions
An infant or toddler is qualified toreceive special education and related
services if he or she has one ormore of the following condi-tions (5 CCR 3030):
a. Hearing impairmentb. Hearing and visual impairmentc. Language or speech disorderd. Visual impairmente. Severe orthopedic impairmentf. Other health impairmentg. Autisticlike behaviorsh. Mental retardationi. Emotional disturbancej. Specific learning disability
Eligibility of Infantsand Toddlers

12
These categories are somewhatdifferent from those used to report thenumber of children served in CASEMIS(California Special Education Manage-ment Information System). The reportableconditions of children served correspondto federal requirements for children whoare three to twenty-two years of age.CASEMIS contains data on the followingcategories of disabilities: autism, deaf-blindness, deafness, hearing impairment,mental retardation, multiple disabilities,orthopedic impairment, other healthimpairment, emotional disturbance,specific learning disability, speech orlanguage impairment, traumatic braininjury, and visual impairment. The eligi-bility of children under three years of agedoes not fall under the federal require-ments of Part B of IDEA and is deter-mined by using the categories in 5 CCR3030. However, program administratorsshould also be prepared to disaggregatedata on those children who are deaf orwho have a traumatic brain injury, ahearing impairment, or multiple disabili-ties (for the purposes of reporting pupilcounts).
Need for Intensive SpecialEducation and Services
An infant or toddler is considered inneed of intensive special educationand services if he or she alsomeets the requirements set forth in
5 CCR 3031 in combination with 5 CCR3030. There are three ways in which achild may meet those requirements:
• The child is functioning at or below 50percent in any one skill area for thechild’s chronological age. The skillareas are gross and fine motor develop-ment, receptive and expressive lan-guage, social and emotional develop-ment, cognitive development, andvisual development.
• The child is functioning between 51percent and 75 percent of his or herchronological age in any two (or more)of the skill areas (listed above).
• The child has a disabling medical condi-tion, such as a visual impairment, deaf-blindness, a hearing impairment, asevere orthopedic impairment, or acongenital syndrome that the individual-ized family service plan (IFSP) teamdetermines has a high predictability ofrequiring intensive special educationand services.
If an infant or toddler is eligible forspecial education services, she or he is alsoeligible for services under state and federalEarly Start requirements. In 1993 Califor-nia enacted the California Early Interven-tion Services Act, implementing Part H(now Part C) of IDEA. This program isknown as Early Start in California. Therequirements for Early Start may be foundin the Government Code, Part 14, Section95000, and in the California Code ofRegulations, Title 17, Section 52000.Under state and federal requirements, thethree categories of eligibility for EarlyStart are as follows:
1. Developmental delay. An infant ortoddler is considered to have a develop-mental delay when there is a significantdifference between the expected level ofdevelopment and the current level offunctioning in one or more of the fol-lowing developmental areas: cognitivedevelopment, physical and motor devel-opment (including vision and hearing),communication development, social oremotional development, or adaptivedevelopment. Most children foundeligible for special education have adisability and a significant developmen-tal delay. Therefore, they meet theeligibility requirements for Early Start.
2. Established risk conditions. An estab-lished risk condition is a condition that

13
has a known origin (etiology) and hasa high probability of resulting in adevelopmental delay even thoughthe delay is not evident at the timeof diagnosis. Children who have adisability and have a disablingmedical condition or syndrome thatthe IFSP team determines has a highpredictability of requiring intensivespecial education and services qualifyfor Early Start under this category.Low-incidence disabilities are estab-lished risk conditions.
3. At risk of a developmental disability(regional centers only). An infant ortoddler is considered at risk of a devel-opmental disability when a multi-disciplinary team determines that achild has a combination of two or morerisk factors that require early interven-tion services. The risk factors are listedin Early Start regulations (17 CCR52022 [c]). Children identified as atrisk of a developmental disability arenot considered eligible for specialeducation unless they also meet therequirements contained in the Educa-tion Code and 5 CCR. Being found atrisk is not considered a disablingmedical condition or a congenitalsyndrome requiring intensive specialeducation and related services under5 CCR 3031. Children meeting thedefinition of being at risk of a develop-mental disability are considered eligiblefor services from the regional center.
Infants and Toddlers witha Solely Low-IncidenceDisability
With the enactment of theCalifornia Early Intervention
Services Act in 1993, LEAs becameresponsible for serving all infants andtoddlers who have a solely low-incidencedisability. Under state law and regulationsfor Early Start, a solely low-incidencedisability means one disability or a com-bination (vision, hearing, orthopedicimpairment) that is the primary disabilityand has a significant impact on the child’slearning and development. The determi-nation of a solely low-incidence disabilityis made by the IFSP team of the LEA. Theinfant or toddler who has a solely low-incidence disability is not eligible forservices from a regional center.
To be considered to have a solelylow-incidence disability, a child mustmeet the appropriate eligibility criteriaunder 5 CCR 3030 and 3031. All childrenwho meet criteria under Section 3030 forone or more of the low-incidence disabili-ties (and for whom the low-incidencedisability is considered the primary dis-ability) are considered eligible for specialeducation and related services as well asEarly Start because, under state EarlyStart regulations (17 CCR 52022[b][2],the existence of a low-incidence conditionconstitutes an established risk condition.

14
A ssessment serves several pur-poses: It helps to determine thechild’s eligibility for programs
and services, ascertains the strengths andconcerns of the child and family, estab-lishes the child’s present levels of function-ing, directs the development of a plan forintervention, and notes the child’s progress.All areas of development and health statusof children ages birth to three years mustbe assessed. Additional Education Coderequirements state that all children as-sessed must have a hearing and visionassessment before the first IFSP and IEPare developed unless parental consent isdenied.
The following sections describe eachdevelopmental domain and include sugges-tions for assessment strategies. In alldomains the results will be most accuratewhen the assessment is completed in avariety of contexts, including the home,and when each domain is viewed in rela-tion to others.
Cognitive Domain
The cognitive domain encompasses achild’s ability to learn from past andnovel experiences. Infants’ skills
include early object use, interactionwith the environment, object permanence,and understanding of cause and effect. The
Assessment of the DevelopmentalDomains of Infants and Toddlers
15
skills of older toddlers and preschoolersinclude verbal and nonverbal problemsolving, symbolic play, memory, attention,discrimination, classification, sequencing,numeric reasoning, visual perception, andvisual motor integration. A profile of achild’s cognitive development should beobtained by incorporating informationcollected from various sources, includinginformation from parents and caregiver,formal and informal observations in avariety of settings, play-based and stan-dardized assessment, when appropriate,and a review of developmental concerns.
Physical Development Domain
The physical development domainencompasses both large and fine
motor abilities. Large motor skills includerolling; creeping; crawling; and balanceand mobility in standing, walking, run-ning, and hopping. Other aspects assessedas part of this domain are the child’s rangeof motion and quality and integration ofmovement and muscle tone. Fine motorskills include oral motor movement forfeeding and speech; manual grasp andrelease; and the ability to reach and to usesmall muscles for self-help and drawing.Assessment takes into account the youngchild’s regulatory and sensory system bydetermining patterns of consistency insleeping and eating and the ability to com-fort himself or herself. Information is ob-tained through formal and informal obser-vations or a report of a child’s skills andabilities in those areas.
Health Domain
The health domain includes the child’sbirth and developmental history,current health information, current
diagnoses, medications and possibleeffects, required medical procedures,current medical supplies and technologicaldevices, primary and specialty care pro-viders, neurological status, nutrition,
feeding and oral health, immunizations,hearing, and vision. Qualified assessmentteam members evaluate the impact of thechild’s health problems on his or herdevelopment and assess prenatal, perinatal,and general health conditions that mayincrease the child’s vulnerability and risk.Information on physical development andhealth is obtained from parents, health careproviders, medical records, and othersources as well as by direct assessment andobservation of the child. Because accuratescreening of young children’s hearing andvision may be difficult, specific procedureshave been developed for this age group.The recommended procedures are outlinedin the publications Ear-Resistible: HearingTest Procedures for Infants, Toddlers, andPreschoolers, Birth Through Five Years ofAge (1998) and First Look: Vision Evalua-tion and Assessment for Infants, Toddlers,and Preschoolers, Birth Through FiveYears of Age (1998).
Communication Domain
The communication domain coversboth verbal and nonverbalmodes. It encompasses preinten-
tional and intentional communication,speech development, receptive and expres-sive language development, gestures, bodymovement, and posture. Areas of languageand speech development encompassarticulation (sound development), seman-tics (word meaning), morphology (gram-mar), syntax (word order), pragmatics(how language is used in relation to oth-ers), voice, and fluency. Communicationand language should be assessed in aninteractive, meaningful context in whichthe child is encouraged to initiate commu-nication. Differences in communicationbetween home and school or other lessfamiliar surroundings should be noted. Theassessment should be based on informationprovided by parents, other caregivers, anda variety of sources, including structured

16
and unstructured conversations, play-based assessment, and standardizedassessment, when appropriate.
Social–Emotional Domain
Identifying infants and toddlers withemotional disturbance requires the
participation of professionalswith expertise in mental healthand behavioral interventions.
The Infant Mental Health WorkGroup has made recommendations regard-ing screening, assessment, and interven-tions for children from birth to threeyears. It urges team members, in thefamily-centered assessment, to discuss thefollowing areas with parents:6
• Emotional and social vulnerabilities ofinfants/toddlers who are at risk or whohave developmental disabilities, and therole they may play
• Infant/toddler cues and special develop-mental needs that affect social and emo-tional well-being
• Characteristics of the caregivingenvironment
• Family strengths, concerns, needs, andresources
• Social support networks• Significant life stressors
The comprehensive assessmentincludes information on the presentingbehavior, the infant’s temperament,parent-child interaction patterns, and thefull-scale developmental assessment com-ponents for young children.
Social–emotional developmentmeans the acquisition of capacities forhuman relationships, emotional expres-sion, communication, and learning.Social–emotional development is based onthe motivation to engage in positive inter-action and to sustain personal relation-
ships and precedes the development ofeffective coping skills, self-esteem, and theability to take advantage of opportunitiesfor learning. Differences in temperament,self-regulation, range and intensity of af-fect, and modulation of one’s response tothe environment are additional factors in-fluencing social–emotional development.
An assessment of a child’s social–emotional development includes observa-tions of the attachment of the child to theparents or guardians; relationships andinteraction with other adults and peers;and the child’s temperament, awarenessof social roles and conventions, initiationof reciprocity, and motivation. Social–emotional skills are assessed by observingor reporting a child’s ability to gain atten-tion appropriately from and respond toothers, express affection and protest, askfor help when a task is too difficult, andengage in interactions with adults andthen with peers.
Adaptive Domain
Assessment of the adaptive domaintakes into consideration the various
abilities of a child to adapt andfunction within the environment
(for example, self-help skills; in-teraction with toys, other objects, and fam-ily members and peers; activity level;attention span; and motivation). Use of astandardized form or informal interview/questionnaire with one or more parents orfamily members may be an effective wayin which to acquire information about thechild’s functioning in the home environ-ment. The information should reflect thevalues and culture of the family. When achild is in child care or a school program,information may also be obtained by con-sulting an adult who has knowledge of thechild in that setting.
6 Adapted from The California Infant Mental Health Work Group Report. Sacramento: California Department ofDevelopmental Services, 1996, p. 17.

17
A family assessment, which identi-fies the family’s strengths andneeds, is a required component of
the assessment process for childrenages birth to three years. Thisinformation is required underIDEA, Part C, as part of the
child’s individualized familyservice plan (IFSP). The family
assessment is a voluntary process that hasbeen established, not to rate or evaluate afamily, but rather to assist the team inunderstanding the outcomes that familieswant for themselves and their childrenand the ways in which the team can assistthem in achieving those outcomes. Thecategories that have been defined for thefamily assessment are family concerns,family priorities, and family resources.
Family concerns are the issues orproblems that the family wishes to ad-dress as a part of the IFSP. Priorities aredefined as the family’s determination ofwhat is the most important to them—howservices and outcomes noted on the IFSPfit into the family’s daily life. Resourcesare those items that the family identifiesas providing support related to the childand the family’s concerns. It is importantto give families multiple opportunities to
Family Assessments

18
identify their concerns, priorities, andresources during the assessment process.The following principles should be con-sidered when team members help thefamily to identify concerns, priorities, andresources: 7
• The inclusion of family information inthe IFSP is voluntary on the part offamilies.
• The family identifies its concerns,priorities, and resources in accordancewith the aspects of family life that arerelevant to the child’s development.
• A family need or concern exists only ifthe family perceives that the need orconcern exists.
• Families have a broad array of formaland informal options in determininghow they will identify their concerns,priorities, and resources.
• Assessment personnel respect familyconfidences and refrain from casuallydiscussing information shared by thefamily with other staff members.
The methods that professionals usewith families to gather this informationcan make a difference in the relationshipthat is established between program staffand the family. It is important to view theassessment process as collaborative andnonintrusive and to allow the family totake the lead in sharing information andexpressing its opinions about importantissues and resources. Respecting thefamily’s ability to identify its ownstrengths, concerns, and needs, as well asbeing sensitive to the family’s cultural andchild-rearing values, fosters a strongreciprocal relationship between theprofessionals and the family. Althoughmany areas of need may be identified,they should always be limited to thosethat the family decides are important to
the development of the child. The follow-ing principles should be considered:• Establish open, two-way communica-
tion.• Allow ample time to discuss the issues
that the family member introduces.• Be an active listener.• Be willing to meet with the family as
often as necessary throughout theprocess.
Identifying concerns, priorities, andresources may be difficult for a family,particularly if this is the family’s firstencounter with the IFSP process. The useof a self-assessment checklist or surveymay be helpful in bringing up and clarify-ing issues that a family might not havethought about before. The checklist orsurvey may be completed privately orwith the help of a team member. It shouldnot be used as the sole method of collect-ing this information and should never beconsidered a written evaluation of thefamily.
Sometimes, families are initiallyunable to disclose much information inthe assessment process. A service coordi-nator may assist by focusing on thefamily’s strengths and supports, whichinclude human and financial resources.An example of a question asked to iden-tify human supports is, “If your child tookhis first steps, whom would you call?”
One objective of this process is forfamily members to leave with the knowl-edge that they have control over decisionsregarding their child and the identifiedsystems of support. Families need toknow that it is acceptable to ask for helpand for the names of individuals who canprovide assistance. Appendix D containssuggestions for teachers and administra-tors gathering information from families.
7 Adapted from Roxane Kaufmann and Mary McGonigel, “Identifying Family Concerns, Priorities, andResources,” Chapter 6 in Guidelines and Recommended Practices for the Individualized Family Service Plan(Second edition). Edited by Mary McGonigel and others. Bethesda, Md.: National Early Childhood TechnicalAssistance System (NECTAS) and Association for the Care of Children’s Health (ACCH), 1991, pp. 48–51.
19
Criteria regarding the eligibility ofchildren ages three through fiveyears of age are established in
Education Code Section 56441.11.Under this section a child is eligible
for special education and relatedservices if he or she meets criteria
for the following conditions:
• Autism• Deaf-blindness• Deafness• Hearing impairment• Mental retardation• Multiple disabilities• Orthopedic impairment• Other health impairment• Emotional disturbance• Specific learning disability• Speech or language impairment in one
or more areas of voice, fluency, lan-guage, or articulation
• Traumatic brain injury• Vision impairment• Established medical disability
Established medical disability isdefined under Education Code Section56441.11 as a disabling medical condition
Eligibility of Preschool-AgeChildren

20
or congenital syndrome that the IEP teamdetermines has a high probability ofrequiring special education and relatedservices. A child who has been diagnosedas such but is not currently exhibiting adelay may be found eligible under thiscategory. In an effort to make this cat-egory consistent with federal law, theCalifornia Department of Education isreconsidering this category; state statutorychanges may be made.
The IEP team must also determinethat the child needs specially designed
instruction or services; that the needscannot be met with modification of aregular environment at home or in school;and that he or she meets the eligibilityrequirement under 5 CCR 3030. Althoughthe current language in 5 CCR 3031 de-fines the eligibility requirements for chil-dren up to the age of four years, ninemonths, Education Code Section 56441.11supersedes that section. Therefore, childrenover the age of three years do not have tomeet the requirement for intensive specialeducation under 5 CCR 3031.

21
The assessment process forpreschoolers is similar to the onefor infants and toddlers. One key
similarity is the need to use multiplemeasures when determining a child’s
eligibility and planning the servicesneeded. The statute (IDEA Section
614[b]) requires that a variety ofassessment tools and strategies be used togather relevant functional and develop-mental information, including informationfrom the parent. Preschoolers, however, donot have to be assessed in all areas of de-velopment; only areas of the suspecteddisability are assessed.
A key difference between the assess-ment process for preschoolers and theprocess for infants/toddlers is that pre-academic performance is assessed. IDEA,Part B, Section 300.532(g), requires chil-dren to be assessed in all areas of the sus-pected disability, including (if appropriate)health, vision, hearing, social and emo-tional status, general intelligence, aca-demic performance, communicative status,and motor abilities. IDEA Section 614(b)requires the assessment of preschoolers toinclude information related to enabling thechild to be involved and progress in appro-priate activities for preschool children.State requirements regarding the eligibility
Assessment of All Areas of theSuspected Disability ofPreschool-Age Children

22
of young children for special educationinclude all the disability categories con-tained in IDEA, Part B.
Assessment for Autism
Autistic spectrum disorders is a cat-egory of disorders that includes autis-tic disorder, Asperger disorder, perva-
sive developmental disorder nototherwise specified (PDD-NOS), Rett’sdisorder, and childhood disintegrativedisorder. These disorders are all charac-
terized by impairments in social interac-tion and communication and by a limitedrange of interests and activities. Theassessment should emphasize the areas ofcommunication, social interaction, behav-ior, play, attention and activity, cogni-tion, and sensorimotor functioning. Thepublications Diagnostic Classificationof Mental Health and DevelopmentalDisorders of Infancy and Early Childhoodand Diagnostic and Statistical Manual ofMental Disorders: DSM-IV (see SelectedReferences) may provide guidelines fordiagnosis. In school districts a team maydetermine a child is eligible for specialeducation under the provision forautisticlike behaviors specified in 5 CCR3030(g).
A child suspected of having autism ora pervasive developmental disordersimilar to autism will exhibit severedifficulties in relating and communicatingwith others and in regulating his or herphysiological, sensory, attentional, motor,cognitive, somatic, and affective pro-cesses.
Methods of assessment are tailoredaccording to a child’s age, developmentallevel, diagnosis, and areas of need. Themethods may include the use of standard-ized assessment tools, developmental as-sessment approaches, a developmentalhistory, a medical history, a family inter-view, a review of records, natural andstructured observations in multiple set-
tings, a functional analysis of behavior,documentation of symptomatology, and afamily assessment. Several instruments areavailable to assess the characteristics ofautism, although few standardized instru-ments for children under the age of fiveexist.
For more information, review thepublication Best Practices for Designingand Delivering Effective Programsfor Individuals with Autistic Spectrum Dis-orders (1997).
Assessment for Speech andLanguage Disorders
A speech or language disorder isdemonstrated by a child’s diffi-
culty in understanding or usingspoken language to such anextent that it adversely affects
his or her educational perfor-mance and cannot be corrected withoutspecial education and related services. Theassessment team includes a speech, lan-guage, and hearing specialist who deter-mines that the difficulty results from anyof the following disorders: articulation;abnormal voice; fluency; inappropriate orinadequate acquisition, comprehension, orexpression of spoken language; or hearingloss (Education Code Section 56333). Aspeech, language, and hearing specialistoften uses a language sample in assessingverbal expression in young children.
For more information, refer to thepublication Program Guidelines for Lan-guage, Speech, and Hearing SpecialistsProviding Designated Instruction andServices (1989).
Assessment for a SpecificLearning Disability
A preschool child with a specificlearning disability may be eligible forspecial education and related services
when the assessment results indicate

23
that there is a significant developmentallag between the child and children of thesame age. The IEP team determines whatis significant. Federal law does not requirea minimum threshold (i.e., percentage ofdevelopmental delay) for preschoolers asit does for infants. Preschoolers maydemonstrate differences or lags in devel-opment that represent extremes within thenormal range. Many educators believethat it is inappropriate to call such varia-tions disabilities and that it is inaccurateto diagnose a preschool child aslearning disabled because of thosevariations.
Many assessors feel uncomfort-able labeling a preschool child with aspecific learning disability because theyare unable to establish a severe discrep-ancy between the child’s intellectualability and achievements in academicareas.
Although IDEA permits the option ofidentifying young children with disabili-ties under the category of developmentaldelay, the California Department ofEducation has not adopted developmentaldelay as a criterion of preschoolers’eligibility for special education (Educa-tion Code Section 56337).
Informed observation (based onknowledge of typical and atypical childdevelopment) and clinical opinion are theprimary assessment tools to be used forchildren under five years suspected ofhaving a learning disability. Standardizedtests for young children of this age areoften not valid or reliable.
Attention deficit and hyperactivitydisorders may adversely affect a pre-school child’s development or educationalperformance or both. Children diagnosedwith attention deficit or attention deficithyperactivity disorder can meet eligibilitycriteria under the following categories:specific learning disability, serious emo-tional disturbance, or other health impair-
ment (Education Code Section 56339).For more information, refer to
Mainstreaming Preschoolers: Childrenwith Learning Disabilities and I CanLearn: A Handbook for Parents, Teachers,and Students (see Selected References).
Assessment for VisualImpairments
Every child is required tohave a vision and hearingassessment prior to thefirst IEP (Education CodeSection 56320). The termvisually impaired includes,
for educational purposes,functionally blind students
(who because of the severity of their visualimpairment rely basically on senses otherthan vision as their major channels forlearning) and low-vision students (who usevision as a major channel for learning). Avisual impairment does not include visualperceptual or visual motor dysfunctionresulting solely from a learning disability.
Assessments for children with asuspected visual impairment typicallybegin with an eye report from an ophthal-mologist or optometrist. This reportdescribes the child’s near and distantvisual acuity with and without best pos-sible correction; field of vision; the etiol-ogy of and prognosis for the visualimpairment; and the eye specialist’s rec-ommendations for school personneland parents.
A teacher of the visually impaired,the orientation-and-mobility specialist, andthe child’s family conduct a functionalvision assessment. The functional visionassessment determines what the studentsees functionally in a variety of educa-tional situations and settings; is used toevaluate how or when the vision impair-ment might adversely affect the studenteducationally; is used to evaluate thestudent’s ability to move efficiently, safely,

24
and independently in multiple environ-ments; provides one criterion for the de-termination of the appropriate reading andlearning media; and is used to identifyvision-related needs.
For further information, refer to theDepartment publication Program Guide-lines for Students Who Are Visually Im-paired (1997).
Assessment for HearingImpairments
The preferred practice for conductinghearing evaluations and assessmentsof preschoolers with a suspectedhearing loss includes reviewing thechild’s medical or case history; mak-ing informal observations of the
child’s behavior; listening to parental con-cerns; reviewing reports; and beginninghearing test procedures appropriate for theage, development, and unique needs ofthe child. Hearing test procedures mayinclude electrophysiological testing,otoacoustic emission response measures,and behavioral assessment measures. Op-tional procedures include tympanometryin conjunction with electrophysiological,acoustic emittance, or behavioral assess-ments, and a visual inspection of the ex-ternal ears.
For further information, refer to theDepartment publication Ear-Resistible:Hearing Test Procedures for Infants, Tod-dlers, and Preschoolers, Birth ThroughFive Years of Age (1998).
Assessment for OrthopedicImpairments
The term orthopedic impairmentincludes those impairments caused bycongenital anomalies, diseases, and
other conditions. Conditions resultingin severe orthopedic impairmentsinclude, but are not limited to, cerebral
palsy, muscular dystrophy, spina bifida,
spinal cord injuries, head traumas, juve-nile rheumatoid arthritis, and tumors. Asevere orthopedic impairment is persistentand significantly restricts an individual’sphysical development, movement, andactivities of daily living. As a result, thisimpairment may affect the pupil’s educa-tional performance. Accompanyingsensory, intellectual, behavioral, learning,and medical problems often occur thatmay also affect the pupil’s school perfor-mance.
The assessment team must include ateacher of individuals who are orthopedi-cally impaired and other persons who areknowledgeable about the implications ofthe orthopedic condition on the pupil’sability to learn. Assessment data aregathered from the family physician andprofessionals representing other publicand private service agencies, such asregional centers, the California ChildrenServices branch of the Department ofHealth Services, hospitals, and rehabilita-tion centers. When preparing the assess-ment plan, the assessors must considerwhether the child:
• Has sensory impairments, limitedphysical movements, or severe speechimpairments
• Needs speech aids or an augmentativemode of communication
• Has a primary language other thanEnglish
• Needs assistive technological devicesor specialized services
• Needs specialized physical health careservices
Assessment team members mayinclude a vision specialist, an occupa-tional therapist or physical therapist, and aspecialist in assistive technology.
For more information, refer to theDepartment publication Program Guide-lines for Individuals Who Are SeverelyOrthopedically Impaired (1992).

25
Assessment for EmotionalDisturbance
In an assessment for a suspectedemotional disturbance, the teammust determine whether the childhas one or more of the conditions
named in IDEA and assess thenature of the child’s social malad-justment. The IEP team member
who conducts the mental health portion ofthe emotional disturbance assessmentmust have training and experience inassessing emotional function and use avariety of instruments and procedures.
The psychoeducational assessmentof the child should include assessment inthe following areas:
• Health background (developmentalhistory, emotional history, medications,major illnesses and hospitalizations,and current health status)
• Functioning in the home and commu-nity (socioeconomic background;language; cultural and educationalbackground; family experiences,including losses and stresses)
• Functioning in school (attendance,achievement, adjustment, behavior inacademic and nonacademic situations)
• Behavior (assessment of the student’sbehavior in the context in which itoccurs, exact description and definitionof the problem, function of the behav-
ior, analysis of what happens beforeand after the behavior occurs)
• Social–emotional status (includesspecific tests and techniques validatedto determine the extent of conditionssuch as depression)
• Previous evaluations (record review,parent report, and information fromother agencies)
• Interviews and self-reports (interviewor structured self-report instrumentcompleted by the parent, teacher, orstudent and observation of the studentin a different setting)
• Pervasive nature of the condition (thepresence of the condition and its perva-siveness in the student’s environmentas cross-validated by observation andinterviews with parents, teachers, andstaff personnel)
• Educational performance (assessmentof the child’s ability to function in thelearning environment to determinewhether the condition adversely affectsthe preschool child’s educationalperformance)
• Cultural differences (a determinationthat the child’s conduct is not dueto cultural, ethnic, or language differ-ences)
For more information on assessment,refer to the publication California Pro-grams and Services for Students withSerious Emotional Disturbances.8
8 California Programs and Services for Students with Serious Emotional Disturbances. Sacramento: Resourcesin Special Education, California State University, Sacramento, 1991, pp. 35–36.

26
Planning is necessary for a success-ful assessment of a young child.Many assessment teams conductplanning meetings, either regularlyor on a case-by-case basis. Settingaside time regularly for planningassessments is recommended tomaintain continuity and to buildthe working relationship of those
conducting the assessments. Ifconflicting schedules make this optionimpossible, a conference call for discussion,at a minimum, is imperative to conduct anaccurate assessment. A team of profession-als can provide transdisciplinary expertiseand interagency coordination for childrenserved by multiple agencies. After the firstcommunication with the parent, the teammeets to discuss an assessment plan basedon the needs of the child and family. Thismeeting includes a comparison of testprotocols and identification of commonitems to ensure nonduplication by profes-sionals and the comfort of the family.
For each child referred, the assess-ment team answers the following questions:
• What are the concerns of the family andthe referral source?
• What information exists regarding thischild? What additional information isneeded?
Preparation for the Assessment
Awareness of one’s ownculture is a first step inrecognizing the culturaldiversity of others.
—Barbara Lowenthal, “TrainingEarly Interventionists to Workwith Culturally Diverse Families,”Infant–Toddler Intervention

27
• Who will be involved in the assess-ment?
• Where will the assessment be con-ducted (at home, in the family childcare home, preschool center, assessmentcenter, or a combination)?
• What needs to be in place to ensureaccurate information on the child’sabilities and needs?
• What tools and procedures will be usedto gather information?
• What role does the child’s health orphysical disability play?
• Are other agencies currently involvedwith the child and family?
• Who will be the primary contact withthe parent?
Once those questions have beenanswered, the designated case manager orservice coordinator contacts the parent tobegin the assessment process. It is themanager’s or coordinator’s responsibilityto explain the process and the rights of theparent and child regarding assessment, togather the information that has beenidentified during planning, and to help putthe family at ease. This initial communica-tion with the family ensures that thefamily is comfortable with the assessment,that the process proceeds smoothly, andthat it is completed within a time framethat meets legal requirements and thefamily’s needs. Planning with the parent iscritical to the success of an assessment.Successful preparation takes time; thefamily may need help to understand theassessment content and procedures andfeel comfortable with the assessmentprocess.
At the planning meeting with theparent or guardian, make sure that thefollowing tasks are accomplished:
• Determine whether an interpreter isneeded and provide one if necessary.
• Acquire written parental consent toconduct the assessment.
• Provide information about the purpose,steps, and time frame of the assessment.
• Explain the parent’s and child’s rightsrelated to the assessment and answer anyquestions the parent may have.
• Discuss the parent’s role in the assess-ment process and encourage parentalparticipation in the process to the extentthat the parent is comfortable and iswilling to participate.
• Obtain the consent of the parent for therelease of needed medical, therapy, anddevelopmental records.
• Agree on the best time, location, meth-ods, and sequence for the assessmentthat are suited to the child’s feeding andsleeping patterns and temperament.
• Agree on adaptations that may be neces-sary in the assessment environment.
• Gather information regarding legalcustody, if necessary.
• Gather background information that maybe useful, such as other agency involve-ment, prior assessments, and culturalissues.
In addition, take into account thefollowing information to establish theassessment setting:
• Ask questions and solicit the concernsof other persons knowledgeable aboutthe child (e.g., clinic, preschool, or childcare personnel).
• Determine the parent’s preference forplaces in which the child should beobserved (e.g., home, preschool, childcare setting, hospital).
• Determine the time of day that is bestfor the parents and when the child ismost alert.
• Identify toys or activities that will helpthe child to be focused, motivated, andcomfortable.
• Determine the role that the parentwishes to take during the assessment.
Establishing rapport with the child iscritical to the success of the assessment
28
process. The California Association ofSchool Psychologists has identified thefollowing ways to build rapport:9
• Take cues from the child during theassessment process.
• Use the child’s favorite toys or intereststo engage him or her.
• Know and use the parent’s vocabularywith the child.
• Involve the parents in the assessment ifthey agree to do so.
• Sit down at the child’s level rather thanhave the child sit at an adult-sizedtable.
• Allow the child to play and explore theenvironment.
• Make transitions quickly and smoothlybetween materials and activities.
Information from Parentsor Guardians
Typically, the information thataccompanies the initial referral isonly a small portion of what isneeded in a comprehensive
developmental history. More informationmay be obtained through written ques-tionnaires sent or given to the family. Oneof the best methods of gathering informa-tion about a child age birth to five years isthrough a conversation with the parent.
9 Best Practices in Early Childhood Assessment Manual. Edited by Diane Ashton. Millbrae, Calif.: CaliforniaAssociation of School Psychologists, 1990, p. 13.
The kind of questions asked and themethod used for gathering this informationare important in determining the depth ofinformation to be obtained. In most inter-views about a child’s developmentalhistory, specific questions are asked, suchas, “When did your baby first roll over?”or “Does your baby have differentiatedcries for different needs?” These questionsmay be difficult for a parent to answer and,at best, will provide only limited specificinformation. The use of conversation andopen-ended questions will be more likelyto set a parent at ease and elicit in-depthinformation. See Appendix D for furtherinformation on questions to ask parents ininterviews.
Information from Other Sources
To accurately assess the developmentallevels of a young child, gatherinformation from as many different
sources as possible. Ask parents about thefollowing sources:
• Birth records and any other hospitaliza-tions
• Names and locations of the primaryhealth provider and all physicians,including specialists
• Child development, Head Start, or childcare program staff

29
• Past and current regional center records• California Children Services (CCS)• Clinics or service providers, such as
Shriner’s Hospitals for Children or theEaster Seal Society
• County public health department records• Women, Infants, and Children (WIC)
nutrition program• Audiologist(s)• Private service providers, such as a
speech therapist or occupational orphysical therapist
• Social services agencies• Mental health providers• Former school district programs
Find out whether any of the current orprevious providers already have copies ofthe records mentioned above that may besent directly to the assessment team. Forexample, if a child is a current or pastclient of the regional center, the medicalrecords may be sent at the request of theparent. Contacting the regional centerrather than all the physicians and hospitalsindividually may save considerable timeand effort.
Once information sources have beenidentified, the parent or guardian mustprovide written consent to release therecords to the assessment team. In someinstances there may be reports that theparent does not wish to have included. Inother instances it may be the first opportu-nity the parent has had to review writtenrecords from other agencies. To make theassessment process easier and more timelyfor all involved, many school districts andagencies in communities have developedan interagency authorization form for theexchange of confidential information. SeeAppendix E for a sample form for aninteragency exchange of information.
Information about a child’s medicaldiagnosis and health status is a centralelement in the assessment process and inthe development of the IEP/IFSP. It isimportant to note the influence of healthconditions on the child’s development andto determine whether any health conditionsplace restrictions on the child or requirespecialized health care services. Bermanand Shaw describe the importance of two-way communication between the healthcare community and other professionalsworking with young children. “Informationfrom a health evaluation can enable staff todesign more appropriate programming fora child and may uncover a physical basisfor learning difficulties or lack ofprogress.”10 Similarly, the sharing ofdevelopmental information may help thehealth care provider plan appropriatemedical care for the child.
The following strategies enhanceregular communication between health careproviders, early intervention specialists,and preschool program staff:11
• Provide written information free ofjargon.
• Incorporate health status information inthe IFSP and the IEP.
• Encourage health care providers’ partici-pation in the assessment and IFSPprocess.
• Pursue mechanisms to reimburse medi-cal and health personnel for their partici-pation in these processes.
• Plan to implement and integrate healthinterventions within the educationalsetting
When background information is notreadily available, the team should so notethat omission in the written assessmentrecords.
10 Carol Berman and Evelyn Shaw, “Family-Directed Child Evaluation and Assessment under the Individualswith Disabilities Education Act (IDEA),” in New Visions for the Developmental Assessment of Infants and YoungChildren. Edited by Samuel Meisels and Emily Fenichel. Washington, D.C.: Zero to Three, 1996, p. 373.
11 Ibid, pp. 373–374.

30
Cultural Diversity in Assessment
The more the assessment teamunderstands the culturalvalues of the family, themore successful the interac-tions and assessment will be.Each assessment team
member brings his or her ownset of beliefs, customs, and values
to any situation. It is important to recog-nize one’s own values and assumptionsfirst before one can begin to understandthe cultural differences of another family.Lowenthal cites important issues for staffto recognize in working with families ofdiverse cultures: differences in familystructures, diverse child-rearing practicesand styles of communication, differentperspectives about the cause of the dis-abilities and the value of interventions,and socioeconomic difficulties.12
It is also important to recognize thata family may or may not hold the generalviewpoints that are attributed to its ethnicculture. Each family’s cultural practiceswill vary.
When working with families fromdiverse cultures, keep in mind the follow-ing guidelines:
• Recognize the language, ethnicity,culture, structure, and preferences ofthe family.
• Conduct the assessment in the family’slanguage of choice (use an interpreter/translator if necessary).
• Consider whether the normativesamples included members of thefamily’s cultural group before using aparticular instrument.
• Recognize differences in child-rearingpractices that may affect a child’sperformance in a particular area.
12 Barbara Lowenthal, “Training Early Interventionists to Work with Culturally Diverse Families,” Infant–Toddler Intervention, Vol. 6, No. 2 (1996), p. 146.

31
A ssessment practices with youngchildren encompass a variety ofgeneral methods, perspectives,
and tools. As mandated by law, no singletest measurement may be used in theassessment process. A brief description oftypes of assessment tools follows. Foradditional information on specific assess-ment tools, contact the Early Start Re-sources office at (916) 492-9990 or (800)869-4337 or CalSTAT (California Servicesfor Technical Assistance and Training) at(707) 664-3160.
Screening Tools
Screening tools are used primarily toidentify a suspected area of concernrelated to a child’s development thatmay warrant further evaluation. These
tools are not appropriate to use for thedetermination of eligibility for specialeducation programs and related services.
Screening measures take a sampling of afew skills that may indicate a need for adiagnostic assessment. The measures aregenerally more reliable when used withchildren ages three to five years than withinfants and toddlers.13 Because of thesmall sample of behaviors that they mea-
Assessment Methods
13 Samuel Meisels and Sally Provence, Screening andAssessment: Guidelines for Identifying Young Disabledand Developmentally Vulnerable Children and TheirFamilies. Washington, D.C.: Zero to Three, 1992.

32
sure, screening tools may not identify allchildren in need of referral. Screeningtools should not be the only method forsuch identification, or child find; rather,the use of ongoing observation, parentinterview, and information from othercare providers along with a screeningmeasure increases the accuracy of theidentification procedure.
Traditional Methods
Traditional assessment methodsinclude standardized tests andsystematic observations. Assess-
ment tools may be norm-referenced orcriterion-referenced and may measure oneor more developmental domains. Thepurpose of an early childhood assessmentis to gather information about a child’sperformance in order to plan an educa-tional and developmental program thatmeets a child’s specific needs.
Norm-Referenced Assessment Tools
These tools are used to evaluate variousdevelopmental areas while the child isengaged in specific activities. Test itemsmust be administered in a prescribed wayto be valid. A child’s responses are com-pared with those of a normative sample ofsame-age peers. The child’s raw score isconverted to a standard score within arange or a percentile rank. The validity ofthe measurement should be judged, inpart, by comparing the makeup of thechildren in the normative sample with thecharacteristics of the child being tested.The California Association of SchoolPsychologists has determined that:
Traditional instruments are inappropriatefor assessing certain groups of childrenwith disabilities or who are from cultur-ally or linguistically diverse back-grounds. School psychologists whoassess young children often make
adaptations to the standardized instru-ments and interpret their findings basedon item analysis. This use of item analysismust be described in the assessmentreport. Reliability and validity of thesetraditional tools with the preschoolpopulation are, at best, generally low.Under non-standardized conditions ofadministration, results need confirmationby use of a multimeasure approach, usingother assessment tools, as well as obser-vational and interview data.14
Criterion-Referenced Assessment Tool
These tools are used to evaluate a child’sperformance against a specific criterion.Skills are typically assessed according to ascale on the assumption that skill acquisi-tion follows a sequential pattern. Thesetests are used to determine a child’s levelof functioning within a developmentaldomain. Test results are typically reportedwithin an age range, and a list is presentedof the specific tasks a child is or is not ableto perform.
Curriculum-Based Assessment Tools
These tools are criterion-referenced butuse the child’s natural environment andongoing activities and materials in thehome, classroom, or child care setting asthe source of information collected. Ratherthan measure a child’s achievement againstexternal norm-referenced data, these toolsrate skills against previous performancealong a developmental continuum ofinstructional objectives. These tools arebest used for planning the child’s instruc-tional program or intervention. This typeof assessment generally uses a single set ofobservations at specified times for datacollection rather than the informationgathered during ongoing observations. Theassessment can be used to determine achild’s rate of learning, ability to makegeneralizations, and learning style.
14 Best Practices in Early Childhood Assessment Manual. Edited by Diane Ashton. Millbrae, Calif.: CaliforniaAssociation of School Psychologists, 1990, p. 16.

33
Alternative Methods
Alternative assessment approachesare highly recommended forchildren ages birth through fiveyears. Such approaches are a more
realistic way to obtain valid informationabout a child’s knowledge, skills, andabilities. Greenspan and Meisels identi-fied several issues regarding assessmentdesign:15
Assessment approaches that rely onstructured tasks or questions in earlychildhood are marked by recurrentpractical problems, which contribute toerror in determining early childhoodcapacities:
• Young children have a restricted abilityto comprehend assessment cues.
• Young children’s verbal and percep-tual-motor response capabilities arelimited.
• Some types of questions requirecomplex information-processing skillsthat young children do not possess.
• Young children may have difficultyunderstanding what is being asked ofthem in an assessment situation, andthey may not be able to control theirbehavior to meet these demands.
In addition, children who havedisabilities may not develop according tothe usual sequential pattern. Alternativeassessment approaches are describedbelow.
Play-Based Assessment
This method is a highly recommendedform of alternative assessment. All devel-opmental areas can be assessed, and thereis a greater likelihood that the child willdemonstrate his or her true abilities in thissetting. Play-based assessments yieldinformation to develop a plan for inter-
vention, to make recommendations forgoals or outcomes for the child andfamily, and to evaluate progress. Theassessment may be conducted in any playsetting, depending on the needs of thechild, family, and assessment team. Playis a process for intervention as well as forassessment.
The observation of play provides anunderstanding of the child’s developmentin various areas. Play is generally associ-ated with social–emotional developmentand the development of relationshipsbetween the child and his or her peers andadults. Although there are developmentaltrends in play, not all children acquire theplay skills in the same order or experiencethem with the same intensity.
Psychologist Diane Ashton describesthe following categories of play: 16
• Solitary play (all ages): The childplays alone. This type of play is notnecessarily an indicator of immaturity.High-level play may occur.
• Onlooker play (all ages): The childwatches other people play. This typeof play appears to be a passive processwhereby the child observes the playlevels of other children. The examinershould use caution in interpreting thistype of play.
• Parallel play (one to three years):Two children pursue similar activitiesbut do not always engage in eyecontact or social behavior. Childrenplay alongside each other.
• Associative play (two to three years):Children engage in the same or similaractivity and may exchange toys ormake occasional comments to eachother. This type of play lacks organi-zation and organized reciprocity.
• Cooperative play (four to five plusyears): This type of play is organized
15 Stanley Greenspan and Samuel Meisels, “Toward a New Vision for the Developmental Assessment of Infantsand Young Children,” Zero to Three, Vol. 14, No. 6 (June/July 1994).
16 Best Practices in Early Childhood Assessment Manual. Edited by Diane Ashton. Millbrae, Calif.: CaliforniaAssociation of School Psychologists, 1990, p. 22.

34
reciprocal play with rules, roles, andindividual functions well defined.Give and take is evident. Themes arereadily observable.
In addition to social play with peers,as noted, a child develops through othertypes of play: social play with adults,exploration and functional play withobjects, and symbolic and social pretendplay. Wolfberg and Schuler characterizethe following forms of play:17
• Social play with adults: Consists ofgive and take, attachment, and sharedattention
• Exploration and functional play withobjects: Involves simple explorationand shifts to increased organization inthe use of toys and other objects
• Symbolic pretend play: A highlyimaginative play form that movesfrom simple reenactment of events tothe creation of new roles and the useof objects in new ways
• Social pretend play: Includes make-believe play that is interactive, with acomplex language, social scripts, andrules
Play may be evaluated through directobservation in natural settings or in aformal, established assessment environ-ment. Information may also be obtainedfrom the observations of others andreported to the team. Assessment of playmay be a useful way to gather informationin various play settings.
Portfolio-Based Authentic Assessment
This method embeds assessment in thechild’s curriculum and involves gatheringinformation from events throughout thechild’s school day. Because this methodof assessment is not used in an artificial
setting, the data collected present a truerpicture of the child’s skills and abilities.The “Program Advisory on AppropriateAssessment Practices of Young Children,”developed by the California Departmentof Education’s Child Development Divi-sion, outlines the following ways ofdocumenting children’s strengths, devel-opmental needs, and evolving understand-ing of the world:18
• Informal and formal observation:Observations may be focused on aspecific concept or learning domain(e.g., observing whether the child isable to pedal a tricycle) or on ageneral record of actions that wereobserved throughout the course of theday (e.g., the types of interactions thattook place with other children over athree-hour class period). Records thatare made at regular intervals through-out the year focus on changes andoutstanding highlights. For example,observations may focus on play withpeers, highlighting the increase inpositive interactions with otherchildren in the program. Structuredteam observations of play in develop-mentally appropriate settings arevaluable to include along with infor-mal observations.
• Developmental profile: All publiclyfunded child development programsrequire a developmental profile to bemaintained on each child enrolled.The profile must record the child’sgrowth in emotional, social, physical,and cognitive domains. It should alsoinclude anecdotal records. Data shouldbe gathered during the course of thecurriculum rather than through anartificial testing situation.
• Portfolio: This is a collection of mate-rials organized to document a child’s
17 Pamela Wolfberg and Adriana Schuler, Integrated Play Groups. San Francisco: San Francisco State University,Department of Special Education, 1992, pp. 37–40.
18 Bill B. Honig, “Program Advisory on Appropriate Assessment Practices of Young Children: Implementing theRecommendations” of Here They Come: Ready or Not! Report of the School Readiness Task Force and It’sElementary! Elementary Grades Task Force Report. Sacramento: California Department of Education, 1992.

35
growth in all developmental domains. Itmay contain the following:
– Developmental profiles– Examples of the child’s developing
fine motor skills (drawings, paint-ings, cutting)
– Photographs and audio or videotaperecordings documenting activitiesin all domains
– Materials showing developingnumber skills
– Material showing an interest in lan-guage and literacy
– Notes of personal and socialdevelopment
– Parent/teacher conference notes– Children’s observations about
themselves– Teachers’ observations of uniqueness
Performance Assessment
This method is similar to the portfolio-based method. Meisels describes it as away of depicting a child’s performance ina developmental area by recording withindaily contexts the child’s knowledge,skills, changes in temperament, andachievements in relation to specificdevelopmental goals. The child’s familyand service providers may set goals oroutcomes based on developmental expec-tations for the child’s age. Performanceassessments are different from other typesof assessments because assessment andintervention are combined into one set ofprocedures.19
19 Samuel Meisels, “Charting the Continuum of Assessment and Interventions,” in New Visions for the Develop-mental Assessment of Infants and Young Children. Edited by Samuel Meisels and Emily Fenichel. Washington,D.C.: Zero to Three, 1996, pp. 38–39.

36
The principles of assessment dis-cussed in this handbook reflect thepreferred practices for the evalua-
tion and assessment of all children. Forsome disabilities, however, the assessorrequires additional knowledge and skillsto accurately evaluate the child’s currentdevelopmental levels and to determine theappropriate program for the child’s educa-tional needs. The team must includeindividuals with training and expertise inthe specific area of disability. This sectionoutlines the characteristics of various low-incidence disabilities and the needs thatthe assessment team must address. TheCalifornia Department of Education haspublished guidelines that contain in-depthinformation and list the resources pertain-ing to each disability (see Selected Refer-ences).
Hearing Impairment
The Department of Education publi-cation Program Guidelines forHearing Impaired Individuals
(1986) outlines the characteristics ofassessments for this population. Theassessment of a child who is deaf or
hard of hearing must take into account theconditions that may affect the child’sneeds. These conditions include the
Assessment of Children withLow-Incidence Disabilities

37
amount of residual hearing, cause of thehearing loss and age of onset, communi-cation skills, first language, other disabili-ties, and cultural and linguistic back-ground. Any standardized testmeasurement will need to be administeredin a nonstandardized mode for the hear-ing-impaired child unless the measure-ment has been standardized for the deafpopulation. Specialized assessment instru-ments and techniques have been devel-oped specifically for the very younghearing-impaired child. These are de-scribed in the California Departmentof Education publication Ear-Resistible(1998).
The assessment team must includean audiologist—a person with knowledgeand expertise in assessing and interveningwith infants, toddlers, and preschool-agechildren who are deaf or have hearing loss(Education Code Section 56320[g]).Some causes of hearing loss, includingmeningitis, rubella, and neurologicallybased deafness, may impair the vestibularsystem. This impairment may result in anadverse effect on equilibrium, bodyawareness, and visual/motor functioning.
Audiological assessments determinea person’s functional hearing level andappropriate amplification needs. It isrecommended that children ages birththrough three years have their hearingexamined by an audiologist every sixmonths and more often if speech orlanguage problems are identified or ifthey have frequent ear infections. Chil-dren over three years of age need anaudiogram once a year.
The Program Guidelines for HearingImpaired Individuals also identifiesconsiderations regarding the family’s rolein the assessment and program planningprocess and notes: “Parental involvementduring the assessment process is crucial in
obtaining both the quantity and quality ofinformation required to make the besteducational and communication decisionsfor the hearing impaired child.”20 Informa-tion on how parents currently communi-cate with their child to meet basic needsand socialize and interact with themshould be elicited.
Visual Impairment
Determining the vision of youngchildren may begin with a brief vision
assessment by the school nurse.The California Department of
Education’s publication First Look (1998)provides in-depth information on visionassessments for children ages birththrough five years. When a visual impair-ment is suspected, the child should bereferred to an eye specialist, preferably apediatric ophthalmologist. Additionalinformation should be obtained from thepediatrician and other medical personnel.State guidelines recommend a functionalvision assessment for children ages birthto three years who fail the initial visionassessment given by the nurse. Thisassessment is also beneficial for childrenwith multiple impairments or for thosewho are unable to respond to traditionalassessment procedures.
The assessment team must include aperson with knowledge and expertise inassessing and intervening with infants,toddlers, and preschool-age children whoare blind or have low vision (EducationCode Section 56320[g]). This staff mem-ber is responsible for conducting thefunctional vision assessment to determinethe way the child is using his or her sight,the child’s vision-related needs, and theinterventions and compensations that arerequired for the child to function as inde-pendently as possible. The publicationProgram Guidelines for Students Who Are
20 Program Guidelines for Hearing Impaired Individuals. Sacramento: California Department of Education,1986, p. 6.

38
Visually Impaired (1997) recommendsthis practice.
The guidelines also state that assess-ment should include the areas of conceptdevelopment, sensorimotor development,adaptive development, communicationskills, and social–emotional developmentfor assessment of children ages birththrough five years.
Severe Orthopedic Impairment
A child with a severe orthopedicimpairment may have been re-ferred or identified by another
agency, such as the regional center orCalifornia Children Services (CCS). Aphysician may refer a child to CCS ifthe cause of the impairment is a musculo-skeletal or neuromuscular condition thatmay require occupational or physicaltherapy. The occupational therapist, thephysical therapist, or both, assess thechild’s areas of orthopedic function andfine and gross motor functional skills.When the child is referred to the schoolprogram, the school staff should workwith other agencies on the additional as-sessment, sharing of current information,and program planning for the child andfamily. The assessment team must includea person who is knowledgeable aboutorthopedic impairments and trained toprovide intervention for such disabilities(Education Code Section 56320[g]). Con-sult Program Guidelines for IndividualsWho Are Severely Orthopedically Im-paired (1992) for more information.
Of particular importance during as-sessment is the recognition that a child
with an orthopedic impairment may nothave typical motor responses. In that caseextra time, positioning, and technologicaldevices should be considered. The use ofalternative assessment methods will notinvalidate the results for a child who can-not produce a motor, speech, or move-ment response that is required in mosttraditional evaluation measurements.
Deaf-Blind
“The assessment of students whoare deaf-blind must be a
transdisciplinary effortconducted by persons whoare knowledgeable in this
area. This approach requires thatassessment personnel share and exchangeinformation and skills across traditionaldisciplinary lines.”21 Assessment takesinto consideration the age of onset, degreeof hearing and visual impairment, otherdisabling conditions, and environmentalsituations and expectations. Specializedhealth needs should also be determined.Few formal assessment instruments havebeen standardized for the deaf-blindpopulation. The child’s developmentallevels and educational needs should beinformally assessed in the child’s naturalenvironment with accurate informationprovided by the parent or guardian. Deaf-blindness is a low-incidence disability andrequires a specialized assessment toobtain meaningful data (Education CodeSection 56320[g]).
21 Program Guidelines for Individuals Who Are Deaf-Blind. Sacramento, California Department of Education,1990, p. 4.

39
A lthough a written report is notspecifically required for the EarlyStart program, sharing the infor-mation with the family is animportant element in the assess-ment process:
Traditionally, assessments of thechild were conducted by profes-
sionals according to their profes-sional disciplines and were followed bya time during which staff synthesizedresults to share with family members ata later meeting. Best practice in recentyears, however, has shifted towardsharing information and results withfamilies as soon as they are gathered. Theprocess of gathering information aboutthe child should be intermingled with thereciprocal process of sharing it.22
Delivering assessment resultsthroughout the process and at the end ofthe testing sessions gives the parent time toassimilate the information and helpsalleviate worry and stress during thetraditional waiting period before the IEP or
Report of the Findings
22 Ann Turnbull, “Identifying Children’s Strengthsand Needs,” in Guidelines and Recommended Practicesfor the Individualized Family Service Plan (Secondedition). Edited by Mary McGonigel and others.Bethesda, Md.: NECTAS and ACCH, 1991, p. 45.

40
IFSP meeting. The parent may ask ques-tions and receive clarification about theassessment process immediately. Ifpossible, provide a short, written sum-mary of findings along with the oralreport. Immediate feedback also gives thefamily the opportunity to observe andnote any changes that may occur betweenthe assessment and the IEP/IFSP meeting.An oral report does not replace a writtensummary of the assessment findings;however, it is the first step in ensuringthat accurate information is shared withthe family.
The assessment information isgleaned from parents’ reports, directobservation, and a review of records. It isthen compiled into a framework thatintegrates the data and is discussed withthe parents. The process of reporting theinformation becomes a parent educationintervention itself that will lead to formalservices when appropriate. The way inwhich this information is reported andshared with parents is a part of the foun-dation for the relationship between par-ents and program staff. The report mayalso set the stage for future home-schoolrelationships. If the report is not presentedin a way that is understandable andrespects the parents’ values, perspectives,language, and culture, it may become abarrier. Technical terms should be accom-panied by a written explanation.
Section 56327 of the EducationCode requires that the following items, ata minimum, be included in the reportabout a preschool child:
• Background information• A comprehensive developmental
history• Family concerns and priorities• Recommendation for eligibility• Assessment finding
• A statement about the validity and reli-ability of the methods and procedures
• Recommendations to address thechild’s areas of need
Test results should be accompaniedby explanations so that scores may beinterpreted correctly. The Departmentpublication Program Guidelines forIndividuals Who Are Severely Orthopedi-cally Impaired (1992) recommends thatthe following factors be included whenreporting assessment and backgroundinformation: the time of day and length ofcontact with the child, the type of envi-ronment in which the child was assessed,the presence or absence of family mem-bers, the child’s familiarity with theevaluator, and observations of the child’sbehavior. The report must account for anyvariance or factors that may have contrib-uted to the results obtained. These factorsinclude, but are not limited to, the use ofan interpreter/translator, standardized testsgiven outside the required protocol, thefamiliarity of the child with the situation,the physical state of the child during theevaluation, and cultural customs of thefamily.
Only the information that is neces-sary and relevant to the evaluation of thechild and to the services and placementdecisions for the child should be reported.According to the Best Practices in EarlyChildhood Assessment Manual, “Thedignity and privacy of the parents shouldbe respected, and information which theymay have shared with you in confidence(e.g., history of substance abuse, incar-cerations) should be omitted if not perti-nent to relevant educational decisions.”23
Traditionally, assessment reportswere written separately by each teammember and reflected individual areas ofprofessional expertise. As teams move
23 Best Practices in Early Childhood Assessment Manual. Edited by Diane Ashton. Millbrae, Calif.: CaliforniaAssociation of School Psychologists, 1990, p. 23.

41
from the traditional model to a trans-disciplinary model, there is a shift towardcompiling a single assessment report thatincludes the evaluation results and recom-mendations of all team members. Chang-ing to this model requires time and on-going communication among the teammembers. One person should be desig-nated to compile all the informationprovided by the team members and toensure that the final report is clear and
concise. The transdisciplinary model hasseveral advantages:
• There is less duplication of pertinentinformation, such as background,observations of behavior, and so forth,by all writers.
• A single report simplifies the data andreduces the amount of reading materialfor the family and others.
• Teaming is enhanced through theprocess.
Communication of Results
Even when caring and skilled professionals have conducted the assessment andteamed well with the young child’s parents, sharing the assessment results isoften a difficult experience. Parents understandably may approach the assess-ment with conflicting feelings. Often, the family members not only are in themidst of coping with the emotional dynamics of having a child with a disabilitybut also are struggling with the anxiety of not knowing how disabled their childmay be. To see in writing what they may or may not know to be fact or to hearout loud for the first time the extent to which their child’s disability has affectedhis or her development may cause parents extreme stress and sometimes unex-pected shock. Professional sensitivity around the impact of the assessment andthe means of conveying the assessment results to the family are vitally importantin helping the young child.
Presenting information to parents about their young child’s special needs is themost difficult task professionals involved with the early childhood assessmentwill be required to perform. Rarely are individuals in early education prepared towork with parents in this manner. And rarely are professionals prepared for thepersonal impact these experiences may have on their own feelings. There is noeasy way in which to convey this sensitive information to another individual;consequently, the team may feel varying degrees of inadequacy and discomfortin this role. Parents, however, need to receive concise, accurate informationabout their child’s development and be told with sensitivity and support.
By being empathic and nonjudgmental and allowing the parents to openly sharetheir feelings, professionals help facilitate the growth of the families with whomthey are working.
Remember:• Provide concise, accurate, and honest information with care and sensitivity.• Ask questions frequently and be a good listener.• Offer families time to express grief and support them in that experience.
Source: Adapted from Linda Cranor, “Foundations for a Family Approach to Early Childhood Assessment,”in Preschool Special Education Program Handbook. Sacramento: California Department of Education,1988.

42
From the beginning of the assess-ment process, parents usually want
to know what services areavailable and appropriate fortheir child. Keeping parentsinformed and involvedthroughout the assessment,helping them to identify the
options, and focusing on thoseappropriate for their child are importantparts of program planning after the assess-ment is completed. Parents who provideimportant observations of a child’s needscontribute much to the assessment. Chart-ing observations of a child’s skill level andbehavior will help parents develop goalsand objectives for their child.
Program planning is based on athorough assessment. For example, acurriculum-based assessment would iden-tify many developmental skills of childrenages three through five years. Such anassessment helps to focus on children’sstrengths as well as their needs. The set-ting, procedures, and equipment areadapted for each skill; and expectations aredelineated for all the developmental do-mains. This type of learning program maybe an extension of the infant/toddler pro-gram in the developmental sequence forspecific skills.
Program Planning

43
Assessors participate in the planningof comprehensive services. Special educa-tors, therapists, classroom teachers, andpsychologists work together to promote anintegrated program that focuses on thewhole child. Assessment procedures andinstructional activities may be adapted to aclassroom or other setting. The IFSP/IEPteam helps families to consider both themost appropriate services to meet thechild’s needs and the variety of settings inwhich services are delivered.
To make the best choice for theirchild, parents may want to visit the variousprograms. A member of the assessmentteam should be available to assist parents.Educational placement decisions need totake into account the priorities of the familyand its vision for the child. Parents need tosee the types of special education class-rooms and understand the regular earlychildhood education alternatives. Parentshave a legal right to be informed of all pro-gram options for their child so that they canmake meaningful, informed decisions dur-ing the IFSP or IEP team meetings.
Program planning includes making thedecision to place the infant or toddler in asetting that is a natural environment for himor her or, for preschoolers, in the leastrestrictive environment. Natural environ-ments, according to federal law (34 CFR303.18), means settings that are natural ornormal for the child’s peers who are thesame age and who have no disabilities. PartC regulations of IDEA (34 CFR 303.12[b])require that early intervention services beprovided to the maximum extent appropri-ate to meet the needs of the child in naturalenvironments, including the home andcommunity settings in which childrenwithout disabilities participate.
Program planning for preschoolersrequires consideration of education in theleast restrictive environment. The termleast restrictive environment (LRE) underIDEA, Part B, means:
Children with disabilities, to the maxi-mum extent appropriate, including chil-dren in public or private institutions orother care facilities, are educated withchildren who are not disabled. Specialclasses, separate schooling, or other re-moval of children with disabilities fromthe regular educational environment oc-curs only when the nature or severity ofthe disability is such that education inregular classes with the use of supplemen-tary aids and services cannot be achievedsatisfactorily. (34 CFR 300.550)
The regulation about LRE also re-quires a continuum of placement optionsfor all children three to twenty-one yearsold. The options include regular classplacement, a resource specialist program,designated instruction and services, specialclasses and centers, nonpublic nonsectarianschool services, state special schools, set-tings other than the classroom where spe-cially designed instruction may occur, andhome or hospital instruction.
Placement decisions must always takeinto account the relationship of the servicesto the outcomes, goals, and objectivesagreed on in the IEP for the child. The as-sessment team should consider the child’sneeds when determining the frequency andduration of services and consider thefamily’s needs when determining the loca-tion of a program and the hours of programoperation. Lack of transportation is fre-quently an issue for parents.
Several service delivery options maybe available to meet a child’s needs. Thefamily is an integral part of the post-assessment process for determining thechild’s educational placement and the ser-vices needed. Parents must be providedwith all facts to be informed decision mak-ers for their child. The goal is to meet thechild’s specific needs by developing a ser-vice plan that fits the child, the family, andthe local educational agency.

44
Staff Developmentfor Assessors
The administration must ensure thatthe staff has knowledge ofeffective assessment practices for
young children and the expertise toconduct an accurate evaluation orassessment. The needs identifiedby the teams determine specificareas for training and support. Staff
members may wish to consider indi-vidual or team needs in the followingareas:
• Transdisciplinary or multidisciplinaryteaming
• Means of incorporating the family inthe evaluation and assessment process
• Methods of assessing play skills• Play-based assessments• Developmentally appropriate practices
related to the evaluation and assess-ment of young children
• Typical and atypical development• Informal observations and recording
data• Disability-specific assessment, evalua-
tion, and services—Hearing impairment—Vision impairment—Severe orthopedic impairment—Autistic spectrum disorders—Mental retardation

45
—Language and speech disorder—Specific learning disability—Traumatic brain injury—Deaf-blind—Emotional disturbance—Other health impairment
• Nutrition and feeding assessments• Specialized health care needs and
procedures• Occupational and physical therapy
assessments
The following activities are low costand may be incorporated into the programto address staff development needs on anongoing basis:
• Establish time for staff to plan togetherand discuss assessments.
• Share observations.• Videotape the assessment and review it
with the entire team.• Observe other team assessment pro-
cesses.• Network with other assessment teams,
if possible.
The following statewide organiza-tions and agencies regularly providetraining in the assessment of youngchildren:
Infant Development AssociationCalifornia Association for the Educa-
tion of Young ChildrenSupporting Early Education Delivery
Systems (SEEDS) ProjectColleges and universities
California Early Intervention TechnicalAssistance Network (CEITAN)
Information on forthcoming trainingmay be provided to programs directly orthrough the SELPA, the school district’sdirector of special education, or thedistrict staff development committee. Thestaff should establish a link with otherdepartments in the school district or otherregionalized school district trainingprograms to ensure that information ontraining reaches the program in a timelyway. Early in the program year, staffshould identify professional developmentneeds and set aside funds for those activi-ties. See Appendix F for statewide re-sources for technical assistance and staffdevelopment related to assessment.
The administration can supportprofessional training in the followingways:
• Make a commitment to send teams toassessment training. The interactionwithin the team increases the learningand the likelihood that new informationwill be incorporated and leads to peersupport.
• Provide on-site follow-up to anytraining.
• Set aside time at staff meetings forteam members who attend training toshare information with others.
• Provide opportunities for cross-trainingamong staff members.

46
A ssessment and evaluation duringearly childhood are critical to achild’s development. This hand-
book seeks to assist professionals inearly childhood special education whoare challenged by recent changes instate and federal law to examine theway in which they conduct assess-
ments and evaluations.Making a commitment to incorporate
and maintain the best practices in assess-ment and evaluation requires profession-als to stay current in research and trendsin the field. Such a commitment leads tomore accurate assessments and evalua-tions of children and better planning forintervention. In addition, positive relation-ships are established between families andprofessionals that set the framework forfuture collaboration between the homeand the school.
Professionals in early childhoodspecial education should review theassessment/evaluation protocol in theirschool district or county early childhoodspecial education program. The indicatorsof a viable, child-focused, and family-friendly assessment/evaluation processare as follows:
• Assessment and evaluation are viewedas a part of the intervention process and
Conclusion

47
not just as a means of determiningeligibility and services.
• Flexible procedures are designed tofacilitate collaboration with parents orother caregivers. Parents are no longerlimited to the role of informant; in-stead, they are active participants in theassessment/evaluation process.
• The assessment/evaluation report isreadable and free of jargon and reflectsthe child’s functional abilities ratherthan mere test scores. Assessmentparticipants are identified in the report.Oral reports are followed by a writtenreport. Reports are shared with theparents. Confidentiality of reports is aconsideration when sharing informationwith other agencies; parents determinewho may be permitted to receive acopy of a report.
• Family involvement and informedconsent are recognized as an importantpart of the evaluation and assessmentprocess.
• The evaluation and assessment processuses multiple measures, such as assign-
ing the child familiar tasks, in a settingthat is comfortable for the child and thechild’s family. Using multiple measureswill increase the likelihood that theresults will be valid.
• The measures are reviewed on severaloccasions in various settings.
• Developmental assessments are ongo-ing. It is important to reassess onseveral occasions after services havebeen initiated rather than rely on a one-time-only evaluation.
• The evaluation/assessment team con-sists of qualified individuals.
• The staff training program is effective,and administrators are supportive of theneed for both regular evaluation oftraining and technical assistance.
The family assessment process isanother new challenge for professionals inthe early intervention (Early Start) pro-gram. It is hoped that local educationalagencies develop additional measures offamily functioning.
48
Appendix APertinent Legal Citations
The following sections of the Code ofFederal Regulations pertain to thishandbook:
Section 300.532 Evaluation procedures.
Each public agency shall ensure, at a mini-mum, that the following requirements are met:
(a)(1) Tests and other evaluation materialsused to assess a child under Part B of theAct—
(i) Are selected and administered so as not tobe discriminatory on a racial or cultural basis;and
(ii) Are provided and administered in thechild’s native language or other mode of com-munication, unless it is clearly not feasible todo so; and
(2) Materials and procedures used to assess achild with limited English proficiency areselected and administered to ensure that theymeasure the extent to which the child has adisability and needs special education, ratherthan measuring the child’s English languageskills.
(b) A variety of assessment tools and strate-gies are used to gather relevant functional anddevelopmental information about the child,including information provided by the parent,and information related to enabling the childto be involved in and progress in the generalcurriculum (or for a preschool child, to par-ticipate in appropriate activities), that mayassist in determining—
(1) Whether the child is a child with a disabil-ity under Section 300.7; and
(2) The content of the child’s IEP.
(c)(1) Any standardized tests that are given toa child—
(i) Have been validated for the specific pur-pose for which they are used; and
(ii) Are administered by trained and knowl-edgeable personnel in accordance with anyinstructions provided by the producer of thetests.
(2) If an assessment is not conducted understandard conditions, a description of the extentto which it varied from standard conditions(e.g., the qualifications of the person adminis-tering the test, or the method of test adminis-tration) must be included in the evaluationreport.
(d) Tests and other evaluation materials includethose tailored to assess specific areas of educa-tional need and not merely those that are de-signed to provide a single general intelligencequotient.
(e) Tests are selected and administered so asbest to ensure that if a test is administered to achild with impaired sensory, manual, or speak-ing skills, the test results accurately reflect thechild’s aptitude or achievement level or what-ever other factors the test purports to measure,rather than reflecting the child’s impaired sen-sory, manual, or speaking skills (unless thoseskills are the factors that the test purports tomeasure).
(f) No single procedure is used as the sole cri-terion for determining whether a child is achild with a disability and for determining anappropriate educational program for the child.
(g) The child is assessed in all areas related tothe suspected disability, including, if appropri-ate, health, vision, hearing, social and emo-tional status, general intelligence, academicperformance, communicative status, and motorabilities.
(h) In evaluating each child with a disabilityunder Sections 300.531-300.536, the evalua-tion is sufficiently comprehensive to identifyall of the child’s special education and related
49
services needs, whether or not commonlylinked to the disability category in which thechild has been classified.
(i) The public agency uses technically soundinstruments that may assess the relative contri-bution of cognitive and behavioral factors, inaddition to physical or developmental factors.
(j) The public agency uses assessment toolsand strategies that provide relevant informa-tion that directly assists persons in determiningthe educational needs of the child.
(Authority: 20 U.S.C. 1412(a)(6)(B),1414(b)(2) and (3))
Section 303.322 Evaluationand assessment.
(a) General. (1) Each system must include theperformance of a timely, comprehensive,multidisciplinary evaluation of each child,birth through age two, referred for evaluation,including assessment activities related to thechild and the child’s family.
(2) The lead agency shall be responsible forensuring that the requirements of this sectionare implemented by all affected public agen-cies and service providers in the State.
(b) Definitions of evaluation and assessment.As used in this part—
(1) Evaluation means the procedures used byappropriate qualified personnel to determine achild’s initial and continuing eligibility underthis part, consistent with the definition of “in-fants and toddlers with disabilities” in Section303.16, including determining the status of thechild in each of the developmental areas inparagraph (c)(3)(ii) of this section.
(2) Assessment means the ongoing proceduresused by appropriate qualified personnelthroughout the period of a child’s eligibilityunder this part to identify—
(i) The child’s unique strengths and needs andthe services appropriate to meet those needs;and
(ii) The resources, priorities, and concerns ofthe family and the supports and services neces-sary to enhance the family’s capacity to meetthe developmental needs of their infant ortoddler with a disability.
(c) Evaluation and assessment of the child.The evaluation and assessment of each childmust—
(1) Be conducted by personnel trained to uti-lize appropriate methods and procedures;
(2) Be based on informed clinical opinion;and
(3) Include the following:
(i) A review of pertinent records related to thechild’s current health status and medical his-tory.
(ii) An evaluation of the child’s level of func-tioning in each of the following developmen-tal areas:
(A) Cognitive development.
(B) Physical development, including visionand hearing.
(C) Communication development.
(D) Social or emotional development.
(E) Adaptive development.
(iii) An assessment of the unique needs of thechild in terms of each of the developmentalareas in paragraph (c)(3)(ii) of this section,including the identification of services appro-priate to meet those needs.
(d) Family assessment. (1) Family assess-ments under this part must be family-directedand designed to determine the resources, pri-orities, and concerns of the family related toenhancing the development of the child.
(2) Any assessment that is conducted must bevoluntary on the part of the family.
(3) If an assessment of the family is carriedout, the assessment must—
(i) Be conducted by personnel trained to uti-lize appropriate methods and procedures;
(ii) Be based on information provided by thefamily through a personal interview; and
(iii) Incorporate the family’s description of itsresources, priorities, and concerns related toenhancing the child’s development.
(e) Timelines. (1) Except as provided in para-graph (e)(2) of this section, the evaluation andinitial assessment of each child (including thefamily assessment) must be completed within

50
the 45-day time period required in Section303.321(e).
(2) The lead agency shall develop proceduresto ensure that in the event of exceptional cir-cumstances that make it impossible to com-plete the evaluation and assessment within 45days (e.g., if a child is ill), public agencieswill—
(i) Document those circumstances; and
(ii) Develop and implement an interim IFSP,to the extent appropriate and consistent withSection 303.345 (b)(1) and (b)(2).
(Approved by the Office of Management andBudget under control number 1820-0550)
(Authority: 20 U.S.C. 1476(b)(3); 1477(a)(1), (a)(2), (d)(1), and (d)(2))
Note: This section combines into one overallrequirement the provisions on evaluation andassessment under the following sections ofthe Act: (1) section 676(b)(3) (timely, com-prehensive, multidisciplinary evaluation), and(2) section 677(a)(1) and (2) (multidisciplin-ary and family-directed assessments).
The section also requires that the evaluation-assessment process be broad enough to obtaininformation required in the IFSP concerning(1) the family’s resources, priorities, and con-cerns related to the development of the child(section 677(d)(2)); and (2) the child’s func-tioning level in each of the five developmen-tal areas (section 677(d)(1)).
Section 303.323 Nondiscriminatoryprocedures.
Each lead agency shall adopt nondiscrimina-tory evaluation and assessment procedures.The procedures must provide that publicagencies responsible for the evaluation andassessment of children and families under thispart shall ensure, at a minimum, that—
(a) Tests and other evaluation materials andprocedures are administered in the nativelanguage of the parents or other mode ofcommunication, unless it is clearly not fea-sible to do so;
(b) Any assessment and evaluation proceduresand materials that are used are selected andadministered so as not to be racially or cultur-ally discriminatory;
(c) No single procedure is used as the solecriterion for determining a child’s eligibilityunder this part; and
(d) Evaluations and assessments are con-ducted by qualified personnel.
(Approved by the Office of Management andBudget under control number 1820-0550)
(Authority: 20 U.S.C. 1476(b)(3); 1477(a)(1),(d)(2), and Individualized Family ServicePlans (IFSPs))

51
A n interpreter working to facilitatecommunication between a familyand a professional should possess the
following qualifications:
• High degree of oral proficiency in both thelanguage of the family and that of theprofessional– Has frequent exposure to both languages
to maintain proficiency in each
• Ability to translate from one language tothe other– Avoids word-for-word interpreting but
is cognizant of possible omissions, addi-tions, substitutions, and transformationsthat may distort or inaccurately repre-sent the speaker’s intended meaning
– Is sensitive to the subtleties and nuancesof the language; may need to reword/rephrase interpretations for both parties(certain words/phrases may have differ-ent meanings for different subgroupsthat may be offensive or inappropriate)
– Avoids use of unnecessary words andexcessive professional jargon
• Sensitivity to the speaker’s style– Watches tone, inflection, body move-
ments (Sometimes the intonation of thewords can totally change their meaning.)
• Ability to adjust to linguistic variations indifferent communities– Understands the varying grammar and
syntax (including slang and dialects) ofsubgroups
• Respect for and familiarity with thefamily’s national origin, indigenous com-munity, and culture
Appendix B
Qualifications of Interpreters
– Knows family’s nationality and corre-sponding ethnic group history (includingmigration experience and local commu-nity history and characteristics)
– Knows specific cultural orientationsand traditional views (e.g., towarddisabilities, child rearing, health andhealing)
• Familiarity with the culture and languageof the professional and the field– Knows the procedures and practices of
the field, relevant policies, currentterminology, and subject matter
• Understanding of the role and function ofthe interpreter on the team– Accepts and is comfortable with the role
of communicator of information– Provides accurate interpretations and
maintains neutrality (Does not offersubjective interpretations, personalopinions, or evaluations of situationsunless asked to do so)
– May assist professional or team mem-bers in identifying possible cultural biasor inappropriateness in various state-ments, questions, or interventions thatare presented as part of the interaction
• Significant experience (and training) as aninterpreter with corresponding professionaland personal attributes– Is able to remain objective and non-
judgmental and maintain confidentiality– Demonstrates good listening skills; is
respectful, patient, flexible, and appro-priately empathetic but does not getemotionally overinvolved
Source: Adapted from D. E. Randall, Strategies for Working with Culturally Diverse Communities and Clients.Washington, D.C.: Association for the Care of Children’s Health, 1989.

52
1. Learn proper protocols and forms ofaddress (including a few greetings andsocial phrases) in the family’s primarylanguage and the names family memberswish to be called and the correct pronun-ciation.
2. Introduce yourself and the interpreter,describe your representative roles, andclarify mutual expectations and thepurpose of the encounter. Assure thefamily member(s) of confidentiality andbe sensitive to the family’s needs andrequests for privacy.
3. Learn basic words and sentences in thefamily’s language and become familiarwith special terminology family mem-bers may use so you can selectivelyattend to them during interpreter-familymember interchanges.
4. Address remarks and questions directlyto the family member during the interac-tion; look at and listen to the familymember as he or she speaks. Observe theperson’s nonverbal communication andbe alert to indications of anxiety, confu-sion, or difficulty in understanding.
5. Avoid body language or gestures thatmay be offensive or misunderstood aswell as side conversations, whispering,
Appendix C
Guidelines for Workingwith Interpreters
or writing while the interpreter is inter-preting.
6. Use a positive tone of voice and facialexpressions that sincerely convey respectand interest in the family member(s).Address the family member(s) in a calm,unhurried manner.
7. Speak clearly and somewhat moreslowly (but not loudly); allow adequatetime for the interpreter to interpret andlisten carefully to the family member’sresponse.
8. Limit your remarks and questions to afew sentences between interpretationsand avoid giving too much informationof long, complex discussions of severaltopics in a single session.
9. Avoid technical jargon, colloquialisms,idioms, slang, and abstractions.
10. Keep words and phrases as simple aspossible, but avoid oversimplifying andcondensing important explanations.
11. Give information in a clear, logicalsequence; emphasize important words orpoints; and repeat vital information.Clarify and rephrase information whennecessary.
12. Check periodically on the familymember’s understanding and the accu-racy of the translation by asking him orher to repeat instructions, or whateverhas been communicated, in his or herown words with the interpreter facilitat-
The following guidelines are of- fered to help make the interview more productive and comfortablefor all concerned:
Source: Adapted from D. E. Randall, Strategies for Working with Culturally Diverse Communities and Clients.Washington, D.C.: Association for the Care of Children’s Health, 1989.

53
ing; however, avoid literally asking, “Doyou understand?” (In many culturalgroups, a “no” response would make allparties lose face and is thus unlikely tobe admitted.)
13. Offer explanations for specific recom-mendations and summarize the outcomeof the meeting, session, or visit.
14. Reinforce verbal information, whenpossible, with materials written in the
family’s language and with visual aids orbehavioral modeling, if appropriate.Before introducing written materials,tactfully determine the family member’sliteracy level through the interpreter.
15. Be patient and be prepared for theadditional time inevitably required forcareful interpretations.

54
M uch information may be gathered from parents by engaging them in a conversationabout their child. Ask open-ended questions that elicit information about the child’shabits and ways of relating. The following are suggested conversation starters that
will elicit information about parent and child interactions, the child’s temperament, andhis or her strengths and needs.
If possible, begin by trying to engage the child so that the parent can observe therelationship you are building with the child. Make positive comments about what the
child is doing or how he or she interacts with the parent. For example, watch for the nuances ofbody language or tone of voice that provides clues about the child-parent relationship. Observethe engagement because it establishes a link with the baby and a link with the parents, thenshare the observation during the conversation. Let them know you value what they say abouttheir child, that they have credibility.
Examples of open-ended questions are as follows:
1. If you wanted to do the dishes and Susie were 10 feet away, what would you give her toamuse herself? Would she play happily? For how long?
2. If you are on the phone and Jamie is awake, what happens?
3. What helps soothe your child?
4. How do you know when your child is hungry or thirsty?
5. What are the things that make your child happy/sad/angry? How does he or she let youknow that?
6. Can you tell me some of the ways that Sam lets you know that he is enjoying something?Whether he is really hungry? When he wants to play? When he wants to stop?
7. What is the favorite thing your child likes to play with?
8. If there were one thing that you could do during the day that you know would make yourchild smile or laugh, what would it be? Could you show me how you do that?
9. Can you remember something that happened yesterday that makes your heart warm?
10. Give the parents an opportunity to teach you about their child by asking them:
—What can I do to make your child smile the way that you do?
—Show me how I can do that same thing.
11. How do you know what makes your child sad?
Always follow this question with a conversation that explores the reasons the child is sad.For example, ask, “Do you think that sometimes she is trying to tell you something andyou’re not getting it?”
Appendix DParent Interview Strategies
55
Sample Form
A school district may permit access to pupil records to any person to whom a parent of the pupil has given writtenconsent specifying the records to be released and identifying the party or class of parties to whom the records may bereleased. The recipient must be notified that the transmission of the information to others without the written consentof the parent is prohibited. The consent notice shall be permanently kept with the record file. California EducationCode Section 49075
Date Requested: ___________________
TO: ___________________________________________________________
___________________________________________________________
____________________________________________________________
____ Enclosed is the following confidential information on the infant or toddler named below.
____ We would appreciate receiving the following confidential information on the infant or toddler named below:
____ Psychological ____ Hearing/Audiological
____ Medical (Medical Record #: _____________________ ) ____ Vision
____ Health and Developmental ____ Speech and Language
____ Educational ____ Other: _____________________
Child Name: ______________________________________________________ Date of Birth: _____________________
Residence Address: __________________________________________________________________________________ Number Street City ZIP Code
Current Program Site: ________________________________________________________________________________
The confidential information identified above has been requested or is being sent by:
Signature:__________________________________________________________________________________________
Name:_______________________________________________________ Title:_____________________________
Program Site:_________________________________________________ Phone No.: ________________________
Address: _______________________________________________________________________________________ Number Street City ZIP Code
A copy of the Interagency Consent to Share Information form has been appropriately signed by the parent(s),guardian, or surrogate parent and is attached.
_____________________________________________________ ______________________________________ Signature Date
Appendix ESample Cover Letter andInteragency Consent to Share Information
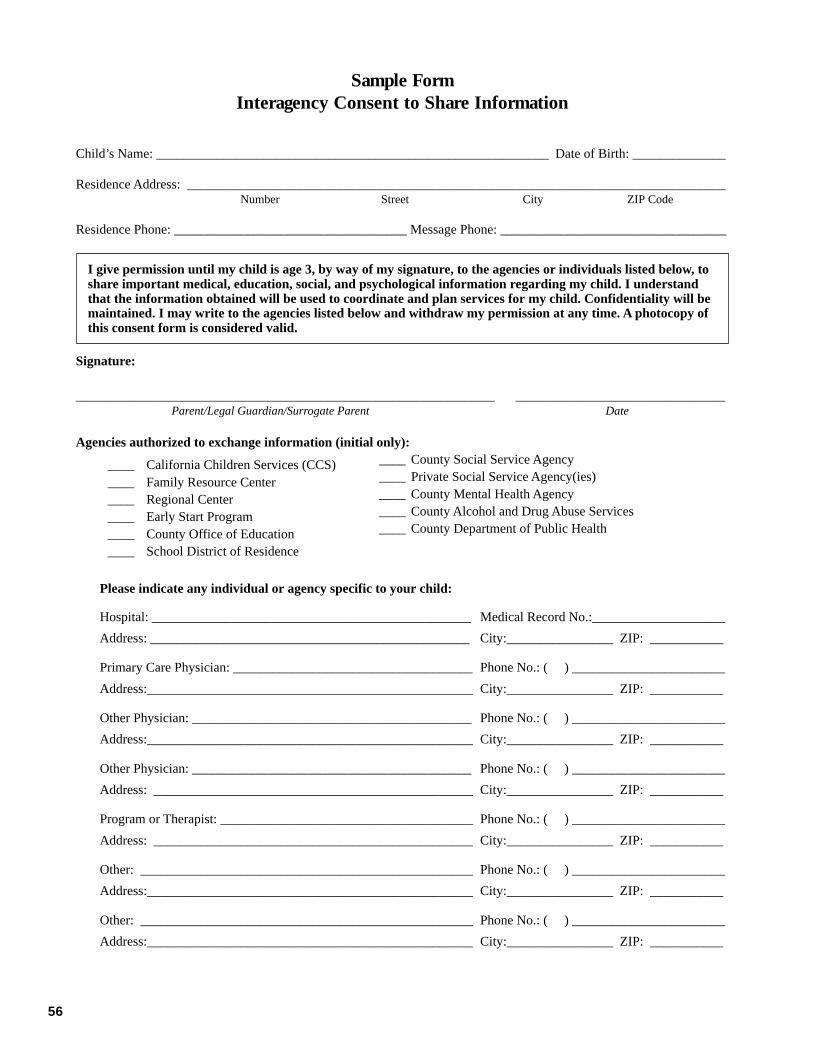
56
Sample FormInteragency Consent to Share Information
Child’s Name: ___________________________________________________________ Date of Birth: ______________
Residence Address: _________________________________________________________________________________ Number Street City ZIP Code
Residence Phone: ___________________________________ Message Phone: __________________________________
I give permission until my child is age 3, by way of my signature, to the agencies or individuals listed below, toshare important medical, education, social, and psychological information regarding my child. I understandthat the information obtained will be used to coordinate and plan services for my child. Confidentiality will bemaintained. I may write to the agencies listed below and withdraw my permission at any time. A photocopy ofthis consent form is considered valid.
Signature:
______________________________________________________________________ ___________________________________Parent/Legal Guardian/Surrogate Parent Date
Agencies authorized to exchange information (initial only):
____ California Children Services (CCS)____ Family Resource Center____ Regional Center____ Early Start Program____ County Office of Education____ School District of Residence
Please indicate any individual or agency specific to your child:
Hospital: ________________________________________________ Medical Record No.:____________________
Address: ________________________________________________ City:________________ ZIP: ___________
Primary Care Physician: ____________________________________ Phone No.: ( ) _______________________
Address:_________________________________________________ City:________________ ZIP: ___________
Other Physician: __________________________________________ Phone No.: ( ) _______________________
Address:_________________________________________________ City:________________ ZIP: ___________
Other Physician: __________________________________________ Phone No.: ( ) _______________________
Address: ________________________________________________ City:________________ ZIP: ___________
Program or Therapist: ______________________________________ Phone No.: ( ) _______________________
Address: ________________________________________________ City:________________ ZIP: ___________
Other: __________________________________________________ Phone No.: ( ) _______________________
Address:_________________________________________________ City:________________ ZIP: ___________
Other: __________________________________________________ Phone No.: ( ) _______________________
Address:_________________________________________________ City:________________ ZIP: ___________
____ County Social Service Agency____ Private Social Service Agency(ies)____ County Mental Health Agency____ County Alcohol and Drug Abuse Services____ County Department of Public Health

57
Excellent resources are available to assist staff in improving the quality ofassessments and evaluations. Many of these are projects funded through Cali-
fornia state departments. Others, in the form of professional organizations andresearch journals, provide a rich source of written materials or consultantservices to assist programs. Some are identified below; however, the list is notexhaustive. The descriptions are taken from information provided by each
respective project or organization.
Appendix FResources for Technical Assistance
California Early InterventionTechnical Assistance Network
The California Early Intervention Techni-cal Assistance Network (CEITAN) iscontracted through the California Depart-ment of Developmental Services (DDS)to ensure a comprehensive system ofpersonnel development. Each year DDShosts Early Start statewide institutesentitled “Building Blocks for Early Start:Supporting the Professional Developmentof Persons Who Serve Infants and Tod-dlers with Special Needs and TheirFamilies.” Flyers regarding these trainingopportunities are widely disseminated toeach SELPA.
In addition, CEITAN providesscholarships and training grants to earlyintervention direct service providers forpersonnel development activities. Thereare attendance scholarships (conferencesor other training), college course workscholarships, grants for local trainingevents, and start-up grants to establishlocal Early Start personnel developmentprograms or innovative systems change.For information regarding CEITANactivities, call (916) 492-9999.
CalSTAT
CalSTAT is a program of the CaliforniaInstitute on Human Services at SonomaState University and a special project ofthe Special Education Division, CaliforniaDepartment of Education. In addition tothe regularly scheduled trainings,CalSTAT also provides professionals andfamilies with customized technical assis-tance, leadership and system changesupport, and Internet resources. ContactCalSTAT by calling (707) 664-3062 orvisit the Web site <http://www.sonoma.edu/cihs/calstat/calstat.html>.
CONNECTIONS: LearningCommunities for All Children
This program is an 18-month to two-year in-service training model designed toprovide an innovative and individualizedapproach to early childhood and earlychildhood special education programs. Inresponding to current and emerging needsof professionals, children, and families,CONNECTIONS combines both researchand information on quality practices fromthe fields of early childhood education

58
and early childhood special education.The approach to supporting administra-tors, educators, and family members in-corporates a model of interagency andcross-discipline training combined withon-site follow-up and technical assistance.For information, contact the CaliforniaInstitute on Human Services (CIHS),Sonoma State University at (707) 664-4230.
Diagnostic Centers
Diagnostic Centers of the CaliforniaDepartment of Education provide high-quality, individualized services to specialeducation students, their families, andschool districts. The telephone numbers ofthe centers, which are located in southern,central, and northern California, are asfollows:
• Los Angeles: (323) 222-8090• Fresno: (209) 445-5982• Fremont: (510) 794-2500
Expert interdisciplinary teams ofdiagnostic professionals, including educa-tion specialists, speech/language special-ists, transition specialists, school psy-chologists, clinical psychologists,pediatricians, and motor skill specialists,address the unique needs of children en-rolled in special education programs.Referrals for an assessment of an eligiblestudent must be made by the child’slocal school district or county office ofeducation.
Local district special educationadministrators, SELPA directors, andcounty office special education adminis-trators may request technical assistanceand professional staff developmentservices. Diagnostic services are providedat no charge.
Early Start Information Line
The toll-free information line puts parentsand professionals working with infants
and toddlers with disabilities in touchwith local Early Start resources in Califor-nia. Information may be obtained bycontacting the DDS Early Interventionoffice at (800) 515-BABY.
NECTAS
NECTAS stands for the National EarlyChildhood Technical Assistance Systemin Chapel Hill, North Carolina. Docu-ments on assessment and evaluation is-sues may be viewed on the NECTAS Website <www.nectas.unc.edu/>. To orderthese documents, call (919) 962-2001.
Project EXCEPTIONAL
The primary focus of this project is todevelop a replicable statewide model totrain the child care staff on ways toinclude young children with disabilities(from birth to five years) in communitychild care settings. In addition, trainingmaterials have been developed for com-munity college instructors. Along withCalifornia, five states in the Outer Pacifichave participated in EXCEPTIONALoutreach trainings. For information ontraining and the purchase of materials,call the California Institute on HumanServices at Sonoma State University at(707) 664-2051.
Region IX, Quality Improvementfor Disabilities Services,Head Start
Located at the California Institute of Hu-man Services, at Sonoma State Univer-sity, this project supports Head Start pro-grams throughout Region IX by providingquality services to children with disabili-ties and their families. Consultants pro-vide technical assistance in developingstate and local interagency agreements,developing and implementing disabilitiesservice plans, and visiting Head Startgrantees on site upon request. In addition,

59
the project provides training on requestedtopics and develops and disseminates re-source materials. The office may bereached at CIHS, Sonoma State Univer-sity, 1801 E. Cotati Avenue, Rohnert Park,CA 94928; telephone (707) 664-4230; orthrough the Internet <http://www.sonoma.edu/CIHS>.
Special Education EarlyChildhood Administrators Project
The Special Education Early ChildhoodAdministrators Project (SEECAP) is aproject of the California Department ofEducation, Special Education Division,and the HOPE Infant and Family SupportProgram, San Diego County Office ofEducation. The project sponsors symposiaannually for experienced and emergingleaders and administrators in the field ofearly childhood special education. Ses-sions are held in the northern and south-ern areas of the state. The symposia covera wide range of topics, including forumson current issues in the field, funding,updates on laws and regulations, and ex-emplary program models. Attendees re-ceive a variety of written material andresources that support each session. Addi-tional information may be obtained bycalling (619) 292-3800.
Supporting Early EducationDelivery Systems Project
The Supporting Early Education DeliverySystems (SEEDS) project is funded
through the California Department ofEducation, Special Education Division,and is coordinated by the SacramentoCounty Office of Education. Its mission isto help provide technical assistance toearly childhood special education pro-grams by using a network of consultantsand visitation sites. The SEEDS project isdesigned for administrators, staff, andfamilies involved in early childhoodspecial education programs in localeducational agencies. The priorities fortechnical assistance have been establishedin cooperation with the California Depart-ment of Education.
Support activities include individualconsultation on site or by telephone,small- and large-group training, programassessment and recommendations, referralto other resources or programs, help inarranging trips to visitation sites, identifi-cation of print or audiovisual materials, orhelp in providing or arranging for speak-ers as a part of a conference or workshop.Technical assistance includes but is notlimited to assessment and evaluation;collaboration with families; curriculum,IFSP, and IEP development and imple-mentation; interagency collaboration;development of educational programspertinent to specific disabilities; referraland intake; and information on servicedelivery models, staffing models, systemschange, and transitions to other programs.For more information or to request techni-cal assistance, call (916) 228-2379.

60
Glossary
achievement test. A test that measures theextent to which an individual has acquiredcertain information or mastered certain skills.
advocate. One who pleads the cause of an-other or takes action on someone’s behalf.
affective. Pertaining to the domain of feelingsor emotions.
amino acid(s). One of the chief componentsof proteins; they are obtained from theindividual’s diet or are manufactured by liv-ing cells.
amniocentesis. A medical procedure in whicha hollow needle is inserted into the uterus toobtain amniotic fluid for detecting any ge-netic abnormalities of the fetus.
anemia. A reduced number of red blood cellsusually resulting from inadequate nutrition.The patient is often characterized by listless-ness and lack of color.
aphasia. The inability to express oneself or tocomprehend spoken or written language, usu-ally due to damage or disease in the languagearea of the cortex.
aptitude. A combination of characteristics,whether genetic or acquired, known or be-lieved to be indicative of a child’s ability tolearn in some particular area.
assessment. “Ongoing procedures used byappropriate qualified personnel throughoutthe period of a child’s eligibility to identify(i) the child’s unique needs; (ii) the family’sstrengths and needs related to development ofthe child; and (iii) the nature and extent ofearly intervention services that are needed bythe child and the child’s family” (PL 99-457Regulations, Section 300.322).
attachment. The process of building positiveand trusting bonds between individuals, usu-ally infant and parents or major caregiver;closeness and affectionate interacting.
attention deficits (or attention deficit disor-der). A learning disability characterized by achild’s short attention span, distractibility, andheightened level of movement and physicalactivity.
atypical development. Any aspect of achild’s physical or psychological makeup thatis different from what is generally accepted asnormal in early childhood.
audiologist. A certified professional whoconducts testing of hearing and is skilled indetecting hearing impairments.
auditory. Pertaining to the sense of hearing.
autism. A developmental disability that sig-nificantly affects a child’s verbal and nonver-bal communication and social interaction andis generally evident before age three; it ad-versely affects educational performance(Code of Federal Regulations, Section1308.15).
autonomy. Self-directing and acting and re-acting independently; the ability and willing-ness to make choices and decisions.
behavior modification. A system by whichparticular environmental events are intention-ally arranged to produce specified behavioralchanges.
cerebral palsy. A condition caused by injuryto certain parts of the brain; usually results inparalysis and uncontrollable muscle move-ment in particular parts of the body.

61
child find. A series of public awareness ef-forts designed to alert the community at largeabout the availability of and rationale forearly childhood intervention programs andservices.
chromosomal disorder. A vast number ofdevelopmental problems that come about atthe moment of conception when the geneticinformation from each parent is merged andmapped out.
cochlea. A bony, snail-shaped structure in theinner ear that allows hearing to occur.
cochlear implant. A device, surgically placedby opening the mastoid structure of the skull,that allows electrical impulses (sound) to becarried directly to the brain.
conductive hearing loss. Refers to problemsin the mechanical transmission of soundsthrough the outer or middle inner ear.
cognition, cognitive skills. Thinking skills,sometimes referred to as preacademic orproblem-solving skills in young children.
congenital anomaly. A developmental differ-ence that is present at birth and is not neces-sarily genetic in origin.
cumulative deficits. An adding on or layeringon of developmental problems as in an undi-agnosed hearing loss, which can result in anaccumulation of additional problems (e.g., asin language, cognitive, and social).
criterion-referenced test. A test that mea-sures a specific level of performance or aspecific degree of mastery.
developmental assessment. Standardizedtests that are intended to document the emer-gence of a sequence of behaviors, skills, orabilities over a period of time.
developmental continuum. The range ofskills or behaviors among children in any onearea of development; for example, from noball-throwing skill to spinning out a hard balloverhand. The child who can play catch issomewhere in the middle on that continuum.Developmental delay is a term that describeschildren who are not able to perform the skillsthat other children of the same age are able toperform.
diagnostic evaluation. An examination usedto ascertain conclusively whether a child hasspecial needs, determine the nature of thechild’s problems, and suggest the cause of theproblems and possible remediation strategies.
disequilibrium. Out of balance or out of har-mony; a way of describing a child who seemsto be experiencing temporary developmentalirregularities.
dyad. A pair of individuals whose relationshiphas social significance, such as a husband andwife or mother and child.
dysfluency. Hesitations, repetitions, and omit-ted or extra sounds in speech patterns.
dyslexia. An impaired ability to read; may alsorefer to an inability to understand what is read.
earmold. That part of an amplification device(hearing aid) that is fitted to the individual’sear.
echolalic. Describes an individual whose lan-guage is characterized by meaningless repeti-tion of words and sentences used intelligentlyby others; a condition often associated withautism and schizophrenia.
egocentric. In reference to young children, itimplies a restricted view of the world from oneperspective only: the child’s own.
etiology. The cause or origin of a handicap-ping condition.
evaluation. “Procedures used by appropriatequalified personnel to determine a child’s ini-tial and continuing eligibility for services” (PL99-457 Regulations, Section 300.322).
failure-to-thrive. Refers to undersized infantswhose bodies, for various reasons (organic,genetic, or environmental), either do not re-ceive or cannot utilize the nurturance neces-sary for proper growth and development.
fine motor skills. Those skills involving handuse or the use of small-muscle groups.
functional. When referring to children’s learn-ing, functional refers to the child acquiringskills that are useful in everyday living.
generalization. The spread of a learned re-sponse from the training situation to an every-day, real-life situation.

62
generalize. To apply what has been learned inone situation to a variety of other related situ-ations.
gross motor skills. Those skills involving theuse of large-muscle groups.
hydrocephalus. A medical condition in whichundrained spinal fluids leads to an enlargedhead and ultimate deterioration of the brain.The condition is often relieved by the inser-tion of a shunt.
immune system. That aspect of body func-tioning responsible for warding off diseases.
incidence. The frequency of occurrence of aproblem at a particular point in time.
incremental step. A step added to a series ina regular order; often a very small increase.
individualized education program (IEP): Awritten document prepared by the IEP team,which includes the parents and the local edu-cational agency staff, that indicates the cur-rent level of the child’s educational perfor-mance (at age three and older), annual goals,short-term objectives, and appropriate ser-vices needed to meet the goals.
individualized family service plan (IFSP).A written document that states the family’sstrengths and needs related to enhancing thedevelopment of the child (birth to threeyears), including specific statements aboutoutcomes, criteria, and timelines regardingprogress; specific services; provisions forcase management; and dates for initiation,duration, and reevaluation of service.
individual program plan (IPP). A writtenplan prepared by regional center staff andparents for persons with developmental dis-abilities to describe the provision of servicesand supports to meet the written goals andobjectives for the child.
interdisciplinary team. A group of profes-sionals who substitute for one another; theydetermine their roles in relation to the charac-teristics of each child and family. They relyon each other to build on the range ofstrengths found among different types of childdevelopment experts.
interpreter. An individual who translatesspoken language into sign language for thosewho are deaf.
in utero. Unborn; literally, in the uterus.
irreversible developmental damage. A con-dition that results in damage from which thereis no recovery, such as a missing arm or achild with Down syndrome; the irreversibilityof the problem does not mean the individualcannot find ways of living life more normally.
jargon. Refers to the specialized language ofa particular profession that is not easily un-derstood by the ordinary person. URI, forexample, refers to the common cold (upperrespiratory infection).
juvenile rheumatoid arthritis. Inflammationof the joints with stiffness, swelling, and lim-ited motion; may be accompanied by inflam-mation of the eyes, which can have seriousconsequences.
learning theory. Emphasizes the dominantrole of environment and reinforcing experi-ences in all learning. Social learning theoryadds other dimensions: that learning also oc-curs through observing and imitating and thatindividuals can generate their own satisfac-tion (intrinsic reinforcement).
meningocele. Hernial protrusion of themeninges through a defect in the skull; usu-ally causes little or no neurological impair-ment.
metabolize. The chemical process in livingcells by which energy is manufactured so thatthe body can carry out its many functions.
multidisciplinary assessment. An evaluationof a child’s strengths and weaknesses from avariety of professional viewpoints using anumber of different sources of informationand involving the child’s parents. Typically,the child’s present level of physical, neuro-logical, cognitive, speech and language, psy-chosocial development, and self-help skills isassessed.
multidisciplinary team. A group of profes-sionals who work independently of each otherin a kind of parallel play format; each disci-pline is viewed as important, but the profes-

63
sional takes responsibility only for his or herown area of clinical expertise.
muscle tone. The interaction between the cen-tral nervous system and motor activity. It doesnot mean the same thing as muscle strength.Without muscle tone there is no voluntarymovement.
mutual gaze. The steady looking at eachother’s face that goes on between intact neo-nates and their mother or primary caregiver.
myelomeningocele. A congenital protrusionof the spinal cord through the vertebrae, oftenresulting in paralysis of the lower trunk andlegs.
neonatal. Pertaining to the first four weeksfollowing birth.
neural. Pertaining to a nerve or the nerves.
neurological. Pertaining to the nervous systemin general.
nonambulatory. The inability to move one-self about; usually the inability to walk.
normalization. The act of making normal.The care and education of the handicappedshould be as culturally normal as possible withservices provided in regular community facili-ties rather than in segregated institutions.
norms. Statistics that describe the test perfor-mance of specified groups, such as children ofvarious ages or handicapping conditions in thestandardization sample of a test.
occlusion. An obstruction; something used toprevent vision. Occluder would be the objectthat the examiner used to prevent the childfrom seeing (usually one eye at a time istested).
oral muscular dysfunction. Weak or faultymovement or muscle tone of the mouth andtongue.
organic. A condition in the individual’s ownbody or neurological system.
orientation-and-mobility specialist. A thera-pist who teaches vision-impaired individualsawareness of their position in the environmentand of significant objects in the environment(orientation) as well as how to move aboutsafely and efficiently (mobility) by utilizing
their remaining senses (including any usefulvision).
orthopedic. Pertaining to the branch of medi-cine concerned with the bones and joints;osteogenesis imperfecta (brittle bones) is anorthopedic problem.
paraprofessional. A trained person who as-sists a certified professional as a teacher’saide.
pediatric ophthalmologist. A physician whois an expert on eye diseases and malfunction-ing of the eyes in children.
peripheral vision. That degree of visionavailable at the outer edges of the eyes.
pervasive developmental disorder. A severeand pervasive impairment in the developmentof reciprocal social interaction or verbal andnonverbal communication skills or the pres-ence of stereotyped behavior, interests, andactivities. This category includes atypicalautism.
physical prompt. Providing physical assis-tance to help a child perform a task. For ex-ample, positioning the teacher’s hand aroundthe learner’s hand and actually putting thelearner through the motions is a physicalprompt.
pincer grasp. The ability to pick up a smallobject by using the forefinger and thumb (adevelopmental skill that does not emerge untilthe latter part of the infant’s first year).
play-based assessment. A form of assess-ment that involves observation of a child atplay and provides understanding of a child’sdevelopment.
prerequisite skills. Skills that must be ac-quired before a next higher level skill can beattempted. For example, children must beable to stand before they can walk and be ableto walk before they can run.
prevalence. The number or proportion ofindividuals in a community or populationwith a given condition or problem.
primitive reflexes. Involuntary responses of anewborn infant, such as grasping, rooting, andsucking. When the infant is around fourmonths of age, the responses are replaced by

64
similar but voluntary behaviors as in the suck-ing response.
psychometric test. Quantitative assessmentsof an individual’s psychological and otherdevelopmental traits or abilities.
readiness test. A test that measures the extentto which a child has acquired certain skills orinformation for successfully undertaking somenew learning activity.
reflexive. An involuntary body reaction tospecific kinds of stimulation (e.g., a tap on theknee precedes the knee jerk). Infants are bornwith reflexes that decrease as the nervous sys-tem matures.
reinforcement. A general term for a conse-quence, an event, or procedure that rewards ormaintains the behavior it follows; for example,paychecks are reinforcement for working.
reinforcers. A consequence, event, or proce-dure that increases the behaviors it follows;however, reinforcers differ according to indi-viduals. For example, candy is a reinforcer formany children, but for some it is not.
reliability. The extent to which a test yieldsthe same results on repeated trials.
reliable and valid tests. Reliable relates toconsistency: how accurate, dependable, andpredictable a test is. Valid refers to tests thatmeasure what they say they are measuring. Forexample, a low score on a verbal IQ test for achild with an undiagnosed hearing impairmentis not likely to be valid. The test is not measur-ing the child’s intelligence, although it pur-ports to be doing so; instead, it is a measure ofhow well the child’s faulty hearing allows forinterpretation of the questions.
repertoire. The sum total and range of anindividual’s social skills.
residual hearing. The remaining degree ofhearing in a person who is deaf or hearingimpaired.
residual vision. The remaining vision afterdisease or damage to a person’s visual system.
respiratory distress syndrome (RDS). Aproblem commonly found among prematureinfants because of the immature developmentof their lungs; may also occur in about one
percent of full-term infants during the firstdays of life.
respite care. Temporary caregiving so thatregular caregivers (usually the mother) getsome relief and time away from the sick ordisabled individual.
rote memorization. Memorizing things with-out understanding them; the ability to recitesomething from memory without havinglearned the meaning.
screening. A brief assessment procedure de-signed to identify children who should re-ceive more intensive diagnosis or assessment.Screening is designed to help children whoare at risk of health and developmental prob-lems, handicapping conditions, or schoolfailure so that they may receive ameliorativeintervention services as early as possible.
sensorimotor. Piaget’s term for the first ma-jor stage of cognitive development, from birthto about eighteen months, when the infantmoves from reflexive to voluntary behavior.
sensorineural hearing loss. A malfunction-ing of the cochlea or auditory nerve.
sensory system. Any one of several ways inwhich individuals receive information fromtheir environment; the most familiar sensorysystems are vision, hearing, tasting, smelling,and touch or feeling.
separation protest. The fussing or displea-sure that an infant displays between eight andtwelve months (approximately) when themother or principal caregiver tries to leave.
shunting. A process for implanting a tube(shunt) into the brain to allow proper circula-tion and drainage of fluids within the skull.
signing. Nonoral communication systems,such as finger spelling, SEE (signing exactEnglish), or ASL (American sign language, inwhich fingers, hands, arms, and upper torsoare used to communicate ideas).
speech pathologist. A certified professionalexpert in speech-related problems.
sphincter muscles. Those muscles that deter-mine bowel and bladder control (the retentionand release of urine and fecal material).

65
standardized IQ test. A test for which thenorms or averages for intellectual perfor-mance have been established by the testing oflarge numbers of individuals of the same age(ideally, of the same socioeconomic back-ground too). Generally, it is not reliable oruseful for young children.
standardized norms. Norms based on a largenumber of averaged scores of similar-agedchildren on the same test items. For example,the average seventeen-month-old can build atower of three cubes.
standardized test. A systematic sample ofperformance obtained under prescribed condi-tions, scored according to definite rules, andcapable of evaluation by reference to norma-tive information.
stigmata (stigma). An identifying mark, char-acteristic, or sign of a disease or disability.
surrogate parent. A person appointed to actin the place of a parent in exercising educa-tional rights during the IEP process.
symptom. A sign or indication of a problem.(Sneezing and a runny nose often are symp-toms of an allergy problem.)
tactile. What is learned or perceived throughtouch.
tangible reinforcers. Material things that anindividual likes and that can be used to rein-force a particular behavior; in children, rein-forcers may be favorite foods and drinks, toys,
stickers, and so on (older children usually likemoney).
temperament. An individual’s psychologicalmakeup or personality traits.
therapeutic. Treatment of a disease or dis-ability.
threshold. The physical or psychologicalpoint at which an individual begins to respondto certain kinds of stimulation.
transdisciplinary team. A group of profes-sionals who cross discipline borders, acquireknowledge from the other professionals onthe team, and incorporate skills from the otherdisciplines into their own practice (similar inways to the interdisciplinary model).
validity. The overall degree of justificationfor interpreting and using a test’s findings. Itconcerns a test’s accuracy. Different kinds ofvalidity evidence are appropriate for differentkinds of tests.
visual acuity. How well an individual is ableto see; keenness of vision.
voluntary motor responses. Those responsesthat an individual controls, such as when theinvoluntary or primitive sucking reflex givesway to an infant deciding when and whethershe or he will suck.
wedges, bolsters, and prone boards. Thera-peutic positioning devices used by physical(developmental) therapists in treating indi-viduals with impaired motor skills.
66
Selected References
Some of the references cited in thisdocument may no longer be in printor otherwise available. The publica-tion data were supplied by the Spe-cial Education Division. Questionsabout the materials should be ad-dressed to the division at (916) 445-
4613.
Ballard-Rosa, Maureen, and others. PreschoolAssessment Practices in California: Char-acteristics and Issues of Alternative Ap-proaches. Sacramento: California Depart-ment of Education, 1996.
Berman, Carol, and Evelyn Shaw. “Family-Directed Child Evaluation and AssessmentUnder the Individuals with DisabilitiesEducation Act (IDEA),” in New Visions forthe Developmental Assessment of Infantsand Young Children. Edited by SamuelMeisels and Emily Fenichel. Washington,D.C.: Zero to Three National Center forInfants, Toddlers, and Families, 1996.
Best Practices for Designing and DeliveringEffective Programs for Individuals withAutistic Spectrum Disorders. Sacramento:California Department of Education, 1997.
Best Practices in Early Childhood AssessmentManual. Edited by Diane Ashton. Millbrae,Calif.: California Association of SchoolPsychologists, 1990.
Brekken, Linda. “Key Points in AssessingPreschoolers and Their Families,” in Pre-school Special Education Program Hand-book. Sacramento: California Departmentof Education, 1988.
The California Infant Mental Health WorkGroup Report. Sacramento: CaliforniaDepartment of Developmental Services,1996.
California Programs and Services for Stu-dents with Serious Emotional Distur-bances. Sacramento: Resources in SpecialEducation, California State University,1991.
Campbell, Patrick. “Clarification ofTransdisciplinary Team.” Memorandumfrom the Director of Special Education.Sacramento: California Department ofEducation, 1987.
Cranor, Linda. “Foundations for a FamilyApproach to Early Childhood Assess-ment,” in Preschool Special EducationProgram Handbook. Sacramento: Califor-nia Department of Education, 1988.
Diagnostic Classification of Mental Healthand Developmental Disorders of Infancyand Early Childhood. Washinton D.C.:Zero to Three, 1994.
Diagnostic and Statistical Manual of MentalDisorders: DSM-IV (Fourth edition).Washington, D.C.: American PsychiatricPress, 1994.
Ear-Resistible: Hearing Test Procedures forInfants, Toddlers, and Preschoolers, BirthThrough Five Years of Age. Sacramento:California Department of Education, 1998.
Early Intervention for Special Populations ofInfants and Toddlers. Edited by LouisRossetti and Jack Kile. San Diego, Calif.:Singular Publishing, 1997.
First Look: Vision Evaluation and Assessmentfor Infants, Toddlers, and Preschoolers,Birth Through Five Years of Age. Sacra-mento: California Department of Educa-tion, 1998.

67
Greenspan, Stanley, and Samuel Meisels.“Toward a New Vision for the Develop-mental Assessment of Infants and YoungChildren,” Zero to Three, Vol. 14, No. 6(June/July 1994).
Guidelines and Recommended Practices forthe Individualized Family Service Plan(Second edition). Edited by MaryMcGonigel and others. Bethesda, Md.:National Early Childhood Technical Assis-tance System (NECTAS) and Associationfor the Care of Children’s Health (ACCH),1991.
Honig, Bill. Program Advisory on Appropri-ate Assessment Practices of Young Chil-dren: Implementing the Recommendationsof Here They Come: Ready or Not! Reportof the School Readiness Task Force andIt’s Elementary! Elementary Grades TaskForce Report. Sacramento: California De-partment of Education, 1992.
I Can Learn: A Handbook for Parents, Teach-ers, and Students. Sacramento: CaliforniaDepartment of Education, 1994.
Kaufmann, Roxane, and Mary McGonigel.“Identifying Family Concerns, Prioritiesand Resources,” in Guidelines and Recom-mended Practices for the IndividualizedFamily Service Plan (Second edition).Edited by Mary McGonigel and others.Bethesda, Md.: National Early ChildhoodTechnical Assistance System (NECTAS)and Association for the Care of Children’sHealth (ACCH), 1991.
Linder, Toni. Transdisciplinary Play-basedAssessment: A Functional Approach toWorking with Young Children (Revisededition). Baltimore, Md.: Paul H. BrookesPublishing Co., 1993.
Linder, Toni. Transdisciplinary Play-basedAssessment: Guidelines for Developing aMeaningful Curriculum for Young Chil-dren. Baltimore, Md.: Paul H. BrookesPublishing Co., 1993.
Lowenthal, Barbara. “Training Early Inter-ventionists to Work with CulturallyDiverse Families,” Infant–Toddler Inter-vention, Vol. 6, No. 2 (1996).
McWilliam, P. J., and Pamela Winton. APractical Guide to Family-CenteredEarly Intervention. Chapel Hill, N.C.Contact [email protected] toorder a copy through the Internet.
Mainstreaming Preschoolers: Children withLearning Disabilities. DHEW PublicationNo. (OHDS) 79-31117. Washington, D.C.:U.S. Department of Health, Education, andWelfare, 1979.
Meisels, Samuel. “Charting the Continuum ofAssessment and Interventions,” in NewVisions for the Developmental Assessmentof Infants and Young Children. Edited bySamuel Meisels and Emily Fenichel. Wash-ington, D.C.: Zero to Three National Cen-ter for Infants, Toddlers, and Families,1996.
Meisels, Samuel, and Sally Provence. Screen-ing and Assessment: Guidelines for Identi-fying Young Disabled and DevelopmentallyVulnerable Children and Their Families.Washington, D.C.: Zero to Three NationalCenter for Infants, Toddlers, and Families,1992.
Program Guidelines for Hearing ImpairedIndividuals. Sacramento: California De-partment of Education, 1986.
Program Guidelines for Individuals Who AreSeverely Orthopedically Impaired. Sacra-mento: California Department of Educa-tion, 1992.
Program Guidelines for Language, Speech,and Hearing Specialists Providing Desig-nated Instruction and Services. Sacra-mento: California Department of Educa-tion, 1989.
Program Guidelines for Students Who AreVisually Impaired (Revised edition). Sacra-mento: California Department of Educa-tion, 1997.
Project EXCEPTIONAL: A Guide for Train-ing and Recruiting Child Care Providers toServe Young Children with Disabilities.Volumes 1 and 2. Sacramento: CaliforniaDepartment of Education, 1996.

68
Radford, Linda, and Sheila Wolfe. “Develop-ment of an Early Childhood AssessmentTeam,” in Preschool Special EducationProgram Handbook. Sacramento: CaliforniaDepartment of Education, 1988.
Randall, D. E. Strategies for Working withCulturally Diverse Communities and Cli-ents. Washington, D.C.: Association for theCare of Children’s Health, 1989.
Turnbull, Ann. “Identifying Children’sStrengths and Needs,” in Guidelines andRecommended Practices for the Individual-ized Family Service Plan (Second edition).Edited by Mary McGonigel and others.Bethesda, Md.: NECTAS and ACCH, 1991.
Wetherby, Amy M., and Barry Prizant. CSPSCaregiver Questionnaire. N.p.: RiversidePublishing Co., 1993.
Wolfberg, Pamela, and Adriana Schuler. Inte-grated Play Groups. San Francisco: SanFrancisco State University, Department ofSpecial Education, 1992.
Zeitlin, Shirley, and Gordon Williamson.Coping in Young Children: Early Interven-tion Practices to Enhance Adaptive Behav-ior and Resilience. Baltimore, Md.: Paul H.Brookes Publishing Co., 1994.
69
Publications Available from the Department of Education
This publication is one of over 600 that are available from the California Department of Education. Some of themore recent publications or those most widely used are the following:
Item no. Title (Date of publication) Price
1379 Assessing and Fostering the Development of a First and a Second Language in Early Childhood—TrainingManual (1998) ......................................................................................................................................................................... 19.00
1356 Best Practices for Designing and Delivering Effective Programs for Individuals with Autistic Spectrum Disorders (1997) .....10.001436 California Department of Education Early Start Program Guide (1998) ..................................................................................... 10.001285 Continuity for Young Children (1997) ........................................................................................................................................... 7.501431 Early Identification/Early Intervention of Young Children with Emotional and Behavioral Issues: Trainer
of Trainers Manual (1998) ....................................................................................................................................................... 30.001410 Ear-Resistible: Hearing Test Procedures for Infants, Toddlers, and Preschoolers, Birth Through Five Years of Age (1998) ....10.001430 Every Little Bite Counts: Supporting Young Children with Special Needs at Mealtime (1998) ................................................. 14.751475 First Class: A Guide for Early Primary Education (1999) ............................................................................................................ 12.501388 First Look: Vision Evaluation and Assessment for Infants, Toddlers, and Preschoolers, Birth Through Five Years
of Age (1998) .......................................................................................................................................................................... 10.001378 Fostering the Development of a First and a Second Language in Early Childhood: Resource Guide (1998) ............................. 10.751365 Fresh Fruit and Vegetable Photo Cards (1997) ............................................................................................................................ 30.001464 Handbook on Family Involvement in Early Childhood Special Education Programs (1999) ...................................................... 11.250737 Here They Come: Ready or Not—Report of the School Readiness Task Force (summary report) (1988) ................................. $5.001252 Just Kids: A Training Manual for Working with Children Prenatally Substance-Exposed (1996) ............................................. 22.251227 Keeping Kids Healthy: Preventing and Managing Communicable Disease in Child Care (1995) .............................................. 15.001384 Observing Preschoolers: Assessing First and Second Language Development (video) (1998) ................................................... 12.000309 Program Guidelines for Hearing Impaired Individuals (1986) ..................................................................................................... 10.000886 Program Guidelines for Individuals Who Are Deaf-Blind (1990) ............................................................................................... 10.001032 Program Guidelines for Individuals Who Are Severely Orthopedically Impaired (1992) ........................................................... 10.001289 Program Guidelines for Students Who Are Visually Impaired, 1997 Revised Edition ............................................................... 10.001256 Project EXCEPTIONAL: A Guide for Training and Recruiting Child Care Providers to Serve Young Children
with Disabilities, Volume 1 (1996) ......................................................................................................................................... 20.001257 Project EXCEPTIONAL: A Guide for Training and Recruiting Child Care Providers to Serve Young Children
with Disabilities, Volume 2 (1996) ......................................................................................................................................... 30.751399 Ready to Learn—Quality Preschools for California in the 21st Century: The Report of the Superintendent’s Universal
Preschool Task Force (1998) ..................................................................................................................................................... 8.001315 Reducing Exceptional Stress and Trauma: Curriculum and Intervention Guidelines (1997) ...................................................... 17.001316 Reducing Exceptional Stress and Trauma: Facilitator’s Guide (1997) ........................................................................................ 18.001318 Room at the Table: Meeting Children’s Special Needs at Mealtimes (video and guide) (1997) ................................................. 17.001383 Talking with Preschoolers: Strategies for Promoting First and Second Language Development (video) (1998) ........................ 12.001255 Taking Charge: A Disaster Preparedness Guide for Child Care and Development Centers (1996) ............................................ 10.251260 Today’s Special: A Fresh Approach to Meals for Preschoolers (video and guide) (1996) .......................................................... 17.00*
* Also available in a Spanish edition of both video and guide (item no. 1262) at same price.
Program for Infant/Toddler CaregiversItem no. Price
0869 It’s Not Just Routine - English video .......................................................................................................................................... $65.000881 It’s Not Just Routine - Spanish video ........................................................................................................................................... 65.000882 It’s Not Just Routine - Chinese (Cantonese) video ....................................................................................................................... 65.009955 It’s Not Just Routine - 50 video magazines .................................................................................................................................. 17.500753 Respectfully Yours - English video .............................................................................................................................................. 65.000773 Respectfully Yours- Spanish video .............................................................................................................................................. 65.000774 Respectfully Yours - Chinese (Cantonese) video ......................................................................................................................... 65.009958 Respectfully Yours - 50 video magazines .................................................................................................................................... 17.500752 Space to Grow - English video ..................................................................................................................................................... 65.000775 Space to Grow- Spanish video ...................................................................................................................................................... 65.000776 Space to Grow - Chinese (Cantonese) video ................................................................................................................................ 65.009959 Space to Grow - 50 video magazines ............................................................................................................................................ 17.501044 Together in Care - English video .................................................................................................................................................. 65.000888 Together in Care- Spanish video .................................................................................................................................................. 65.001051 Together in Care - Chinese (Cantonese) video ............................................................................................................................. 65.009873 Together in Care - 50 video magazines ........................................................................................................................................ 17.500877 Infant/Toddler Caregiving: A Guide to Routines ......................................................................................................................... 12.500879 Infant/Toddler Caregiving: A Guide to Setting Up Environments ............................................................................................... 12.501076 Module II Trainer’s Manual ......................................................................................................................................................... 20.00
Prices and availability are subject to change without notice. Please call 1-800-995-4099 for current prices and shipping charges.

70
Item no. Module II Price
Module II: Group Care Special Price(The package price includes 4 videos, 4 accompanying video magazines,
2 curriculum guides, and 1 trainer’s manual.)9931 English videos ........................................................................................................................................................................... $269.009932 Spanish videos ............................................................................................................................................................................ 269.009933 Chinese (Cantonese) videos ........................................................................................................................................................ 269.00
______Note: The video magazines and the curriculum guides are in English.
97-069 02-2723-376 2-00 5M
VISA®
MasterCardMasterCard
®
Order Form Date
School/District
Name/Attention
Address
City State ZIP code
Telephone ( )
To: California Department of EducationCDE Press, Sales OfficeP.O. Box 271Sacramento, CA 95812-0271(916) 445-1260 • FAX (916) 323-0823
■■ Check made payable to California Department of Education
■■ VISA ■■ MasterCard
/Card Number (Please write clearly.) Expiration Date: Month Year
Name on Card
Authorized Signature
$
Item Number of Price pernumber Title of publication copies or sets copy or set Total
Total number ofcopies
$
$
$
$
Subtotal
California residentsadd sales tax.
Shipping and handlingcharges (See chart.)
TOTAL AMOUNT
Shipping and Handling Charges
Numberof copies Add
1 $ 5.952–4 7.955–8 9.959–12 14.95
Numberof copies Add
13–16 $15.9517–20 17.9521–24 19.9525–28 21.95
Numberof copies Add
29–32 $23.9533–36 26.9537–40 28.9540+ call 1-800-995-4099
Note: Mail orders must be accompanied by a check, a purchase order, or aVISA or MasterCard credit card number, including expiration date and yoursignature. Purchase orders without checks are accepted from educationalinstitutions, businesses, and governmental agencies. Purchase orders and credit cardorders may be placed by FAX (916) 323-0823. Telephone orders will be acceptedtoll-free (1-800-995-4099) for credit card purchases. Please do not send cash.Stated prices are subject to change. Please order carefully; include correct itemnumber and quantity for each publication ordered. All sales are final.
Prices and availability are subject to change without notice. Please call 1-800-995-4099 for current prices and shipping charge s.
■■ Please send me a free copy of the currentEducational Resources Catalog.