hapatobilliary trauma dr awad al dumour al basheer hospital
TRANSCRIPT

Hapatobilliary trauma
Dr awad al dumour
Al basheer hospital

Background
Largest solid abdominal organ,fixed position
Second most common injured, but most common cause of death after abdominal trauma
Blunt MVA most common 80% adults, 97% children-conservative rx

Locate your liver
Upper right quadrant deep to inferior ribs
Dome of liver abuts aganst inferior diaphragm surface
Left/right lobesGall bladder is thin muscular
sac on inferior surface where bile collects (1 above)
1. ANATOMY

Measuring liver span by percussion: variation in liver span Variation in liver span according to the vertical plane of examination. Since there is variability in where clinicians determine the mid-clavicular line to be, the inevitable consequence is that liver span may also vary even if multiple observers are perfectly accurate in measuring it.
Percuss your liverEasiest organ to percussDense tissue gives rock-
solid sound/feel on percussion
Mid-clavicular line moving inferiorly from mid-chest to lower right quadrant

Portal Triad- Common Bile duct- Common Bile duct
- Proper Hepatic Artery- Proper Hepatic Artery
- Portal Vein- Portal Vein

LIVER

Anatomy
Cantile described main divisions along a main plane from GB fossa to IVC. Divides liver into equal halves.
Couinaud developed 4 sectors and 8 segments, divided into vertical and oblique planes, defined by the 3 main hepatic veins and transverse plane thru right and left portal branches.

Anatomy
Hepatic veins lie between segments. Left hepatc vein divides left lobe into
medial and lateral segments. Middle hepatic vein divides liver into left
and right lobes.

Anatomy
Right hepatic vein divides right lobe into anterior and posterior segments.
A horizontal line thru left and right main portal veins is used to divide lobes into inferior and superior segments.
The 8 liver segments are numbers clockwise on the frontal view.
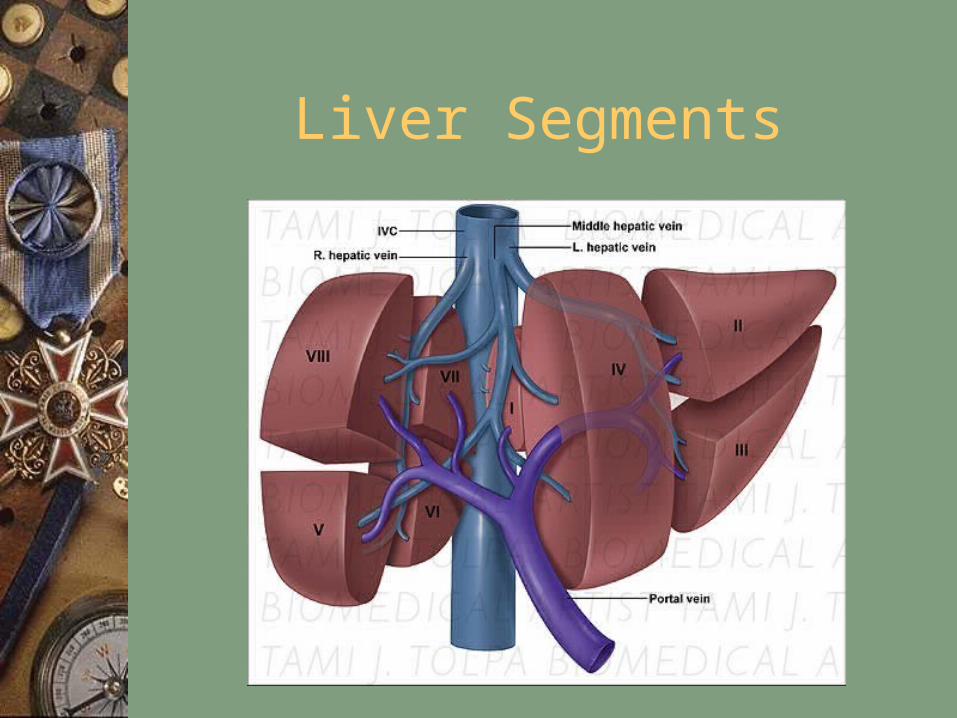
Liver Segments

Liver Segments

Injuries
Subcapsular hematoma or intrahepatic hematoma.
Laceration Contusion Hepatic vascular disruption Bile duct injury 86% of injuries have stopped bleeding at time of
exploration. Decreased transfusion req.With conservative.

Injuries
Subcapsular hematoma or intrahepatic hematoma.
Laceration Contusion Hepatic vascular disruption Bile duct injury 86% of injuries have stopped bleeding at time of
exploration. Decreased transfusion req.With conservative.
CLASSIFICATION
Penetrating wounds Stabs wounds , gunshots…. Level of injury Frequency of organ injury :1. Liver 37%2. Small bowel 26% 3. Stomach 19%4. Colon 17%5. Major vessels & retroperitoneal structures

Penetrating wounds
CLASSIFICATION
Blunt trauma RTAs , direct blows , falls , ….. Sudden application of pressure , seat belt syn Frequency of organ injury
1. Spleen 25%
2. Kidney 12%
3. Intestine 15%
4. Liver 15%
5. Retro peritoneal haematoma 13%
CLASSIFICATION
Iatrogenic injury
Due to diagnostic & therapeutic procedures
1. Endoscopy
2. External cardiac massage
3. Peritoneal dialysis
4. Paracentesis
5. PTC
6. Liver biopsy

Classification
I-Subcapsular hematoma<1cm, superficial laceration<1cm deep.
II-Parenchymal laceration 1-3cm deep, subcapsular hematoma1-3 cm thick.
III-Parenchymal laceration> 3cm deep and subcapsular hematoma> 3cm diameter.

Classification
IV-Parenchymal/supcapsular hematoma> 10cm in diameter, lobar destruction, or devasularization.
V- Global destruction or devascularization of the liver.
VI-Hepatic avulsion

LIVER INJURIES
Incidence Clinical picture Management
1. Non operative
2. Drainage of deep lacerations Sump drain
3. Removal of devitalized tissue
4. Pringle maneuver , ? HA ligation where ?
5. Segmentectomy ? Lobectomy ? Packing
6. Repair CBD over T- tube

Pathophysiology
Friable parenchyma, thin capsule, fixed position in relation to spine.
Right lobe gets hit more since its larger, and closer to ribs.
85% injuries involve segments 6,7,8 from compressioin against ribs, spine, abd wall.
Shear forces at attachments to diaphragm Transmission thru right hemithorax.

Pathophysiology
Liver injured easily in children since ribs are compliant, force transmitted.
Liver not as developed in children, with weaker connective tissue framework.
Iatrogenic injuries by biopsies, biliary drainage, TIPS, can cause capsular tears and bile leaks, fistulas, hemoperitoneum.

Clinical Details
Symptoms of injury are related to blood loss, peritoneal irritation, RUQ tenderness, and guarding.
Unrecognized delayed abcess Bilomas Signs of blood loss may dominate the
picture.

Clinical Details
Elevated liver tests Biliary peritonitis (nausea, vomiting, abd
pain). DPL has high sensitivity, 1-2%
complication rate. Plain x-rays non-specific. CT scan diagnostic procedure of choice. Hida for leaks, angio for hemorrhage.

Physical examination
Ecchymosis or abrasions ,respiratory pattern inspect urethra & perineum Examine the back ,sprung the pelvis. PR exam why ? Bowel sounds Palpation spasm & rigidity ? Rebound Foley catheter Why ? when? Re evaluations why ?

Limitations
FAST sensitivity highest (98%) for grade 3 injuries or greater. Negative findings do not exclude hepatic injury.
Emergency sono findings demonstrating free fluid, parenchymal injury, or both demonstrate overall sensitivity for detection of blunt abdominal trauma of 72%.
Angiogram may fail to detect active bleeding.
ADJUVANT STUDIES FOR ASSESSMENT
Laboratory studies
Hct , UA , S amylase , other tests baseline
Radiological studies
PFA , Erect CXR ,US , CT ? Contrast , IVU, Urethrogram , Cystogram and Angiography .
Four quadrant tap test

DIAGNOSTIC PERITONEAL LAVAGE
Indications of DPL Contraindications Technique , precautions
Results are positive IF
1. RBCs > 100,000/cubic mm
2. WBCs > 5000/cubic mm
3. Amylase >200 units
4. Presence of bacteria ,bile, faeces
5. Rough index

CT Scans
Accurate in localizing the site of liver injury, associated injuries.
Used to monitor healing. CT criteria for staging liver trauma uses
AAST liver injury scale Grades 1-6 Hematoma,laceration,vascular,acute
bleeding,gallbladder injury,biloma.

Angiography
Demonstrates active bleeding Transcatheter embolization may be the
only treatment required. Findings include contusion, laceration,
hematoma, pseudoaneurysms, fistulas. Embolization can reduce transfusion
requirements, stenting for fistulas.

Angiography

Grade I Liver Injury

Grade II Liver Injury

Grade III

Grade IV
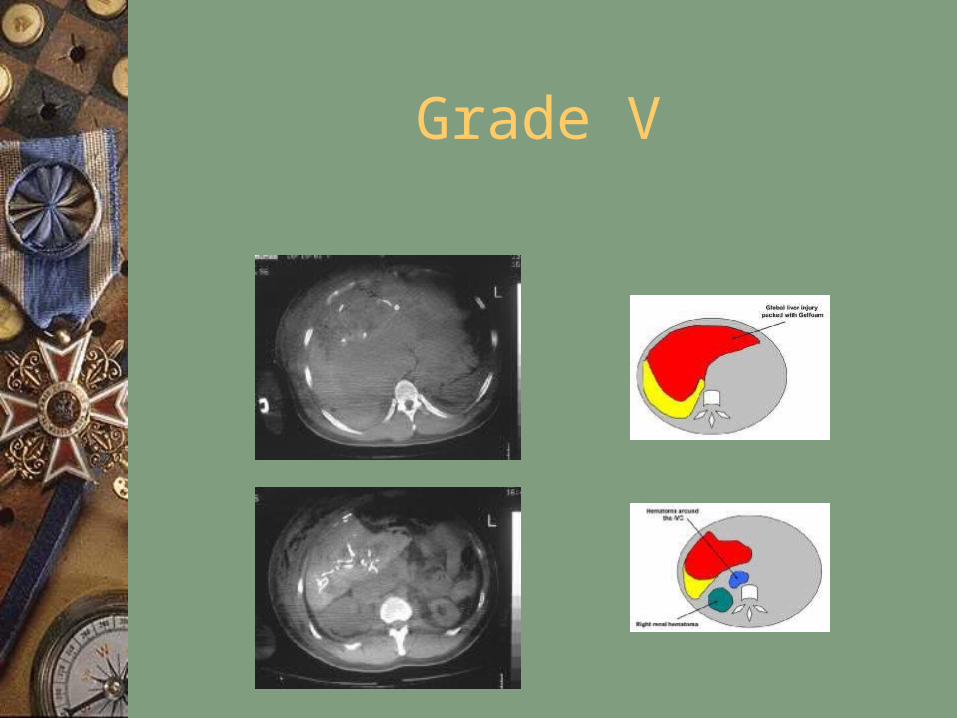
Grade V

MANAGEMENT
Pre hospital care
Little can be done ABC Sterile dressing Don't remove FB from trunk Saline dressing over evisceration
MANAGEMENT cont…
Hospital care Detailed history specially in blunt trauma Physical examination Resuscitation
1. ABC
2. Basic blood tests, cross match, amylase
3. Closed monitoring
4. If patient is stable complete investigation
Biliary Injury & Laparoscopic
Cholecystectomy

Causes of Biliary Injury in LC
Failure to properly occl. the cystic duct Injury to the ducts in the liver bed caused
by entering a plane too deep to the gallbladder
Cautery Misuse – thermal necrosisductal tissue loss
Pulling forcefully up on the gallbladder when clipping the cystic duct tenting injury to the junction of the CBD & common hepatic duct
Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180 (1) : 101-25.
Reviews revealed the incidence of biliary injury during open CCY to be 0.1-0.3%
1995 – Strasberg’s study which incl. more than 124,000 laparoscopic cholecystectomies (LC) reported in the literature found the incidence of major bile duct injury to be 0.5%.
Biliary Injuries During Cholecystectomy (CCY)

Diagnosis of Bile Leaks
Persistent fullness, anorexia, abdominal pain, fever & tenderness,jaundice, elev WBC
High level of suspicion following surgery Bile draining from a drain left in the
operative field

Radiographic Diagnosis of Biliary Injury
US/CT – detect bilomas (poss. perc drainage)

Radiographic Diagnosis of Biliary Injury
US/CT – detect bilomas (poss. perc drainage) HIDA – presence of active bile leak
(physiologic)

ERCP
Provides exact anatomical diagnosis of bile duct leak; while allowing treatment w/ decompression of the biliary tree.
Principal of treatment is to establish a pressure gradient that will favor flow into the duodenum not the leak site; may entail removal of retained stone or internal stenting +/- sphincterotomy

Internal stenting is currently the procedure of choice for treating bile duct leaks ( types A & D)
Cessation of bile extravasation in 70-95% of cases w/in 7 days

Percutaneous Transhepatic Cholangiography
Another method of non-surgical mgmt of bile leak
Usually reserved for when ERCP unsuccessful; since bile ducts of normal caliber increasing the difficulty of the procedure

Plastic surgery meets GI surgery
BOTOX injection to sphincter of Oddi

Intraoperative Injury
Strasberg D injury - (partial injury to a major duct) should be repaired at initial operation w/ T-tube drainage
Strasberg E injury - (complete transection of major duct) may be reconstructed at the initial operation w/ a R-Y hepaticojejunostomy.
*** No primary re-anastomosis secondary to ischemic factors***

Detection in post-op period
Abx, nutrition support, percutaneous drainage of bile collex (US or CT)
MRCP, PTC or ERCP to delineate location of injury.
Once sepsis and leaks are controlled, then may perform definitive reconstruction w/ R-Y hepaticojejunostomyKaman et al. Management of Major Bile Duct Injuries following
LC. Surg Endosc (2004)18:1196 –1199

Gallblader injury
Blunt trauma Penetrating injury Investigation Ultrasound CT SCAN

PANCREATIC INJURIES
Blunt or penetrating injury Associated with other injuries Persistent elevation of S. amylase Laparotomy usually for other injuries Select the surgical procedure ,
Debridment
Good drainage , Sump drain