haploidentical hematopoietic stem cell transplantation for hematological malignancies
DESCRIPTION
Haploidentical Hematopoietic Stem Cell Transplantation for Hematological Malignancies. Xiao-Jun Huang M.D. Ph.D. Peking University Institute of Hematology, Peking University People’s Hospital & Beijing Key Laboratory of HSCT, Beijing, P.R.China. Clinic. Research. Education. 1. - PowerPoint PPT PresentationTRANSCRIPT

Haploidentical Hematopoietic Stem Cell Transplantation for Hematological Malignancies
Xiao-Jun Huang M.D. Ph.D.Peking University Institute of Hematology,
Peking University People’s Hospital &Beijing Key Laboratory of HSCT,
Beijing, P.R.China

1
EducationClinic
Research

The Cumulative Hematopoietic Stem Cell Transplantation (HSCT) Cases of PUIH
PUIHThe Largest HSCT center in AsiaNow >400 cases of HSCT per yearNow >60% Allo-HSCT cases are Unmanipulated Haploidentical HSCT
24%24%

• Current Clinical Results
• Strategy to Improve the Clinical Results
Haploidentical Hematopoietic Stem Cell Transplantation for Hematological Malignancies
11
• In vitro T-cell-depleted HSCT
22• Non-Myeloablative Haploidentical HSCT
33• Unmanipulated Myeloablative
Haploidentical HSCT

GIAC protocol
• G: donor treatment with rhG-CSF
• I: intensified immunological suppression
• A: anti-human thymocyte immunoglobulin (ATG)
for the prevention of GVHD
• C: combination of G-PB and G-BM
Huang XJ, et al. Blood, 2006, 107(8):3065-3073Huang XJ, et al. Annals of Medicine, 2008, 40,444-455Huang XJ, et al. Clin Cancer Res. 2009;15:4777-4783Huang XJ, et al. BBMT. 2011 Jun;17(6):821-30.
3. Unmanipulated Haploidentical HSCT

Effects of G-CSF on Bone Marrow in Healthy Donors
HuangXJ, et al. Clin Transplant 2011: 25: 13–23
3. Unmanipulated Haploidentical HSCT

Immunoregulatroy Effects after G-CSF Administration to Healthy Donors
Huang XJ, et al. Biol Blood Marrow Transplant.2011;17(2):197-204
3. Unmanipulated Haploidentical HSCT

400.00300.00200.00100.000.00
Days posttransplant
1.0
0.8
0.6
0.4
0.2
0.0Pro
babi
lity
of e
ngra
ftm
ent (%
)
-censored小于中位值
-censored大于等于中位值
小于中位值
大于等于中位值CD34 ? ?二分 量
400.00300.00200.00100.000.00
Days posttransplant
1.0
0.8
0.6
0.4
0.2
0.0Pro
babi
lity
of e
ngra
ftm
ent (%
)
-censored小于中位值
-censored大于等于中位值
小于中位值
大于等于中位值CD34 ? ?二分 量
Engraftment
Huang XJ, et al. Biol Blood Marrow Transplant,2009, 15(5):632-8
n=348
400.00300.00200.00100.000.00
Day posttransplant
1.0
0.8
0.6
0.4
0.2
0.0Pro
babi
lity
of e
ngra
ftm
ent (%
)
? -censored展期
-censored早期
? 展期
早期? ? ?移植 的疾病
400.00300.00200.00100.000.00
Day posttransplant
1.0
0.8
0.6
0.4
0.2
0.0Pro
babi
lity
of e
ngra
ftm
ent (%
)
? -censored展期
-censored早期
? 展期
早期? ? ?移植 的疾病
P=0.008
n=348
CD34+ cells≥2.19×106/kg
CD34+ cells<2.19×106/kg
P<0.0001
Early stageAdvanced stage
3. Unmanipulated Haploidentical HSCT
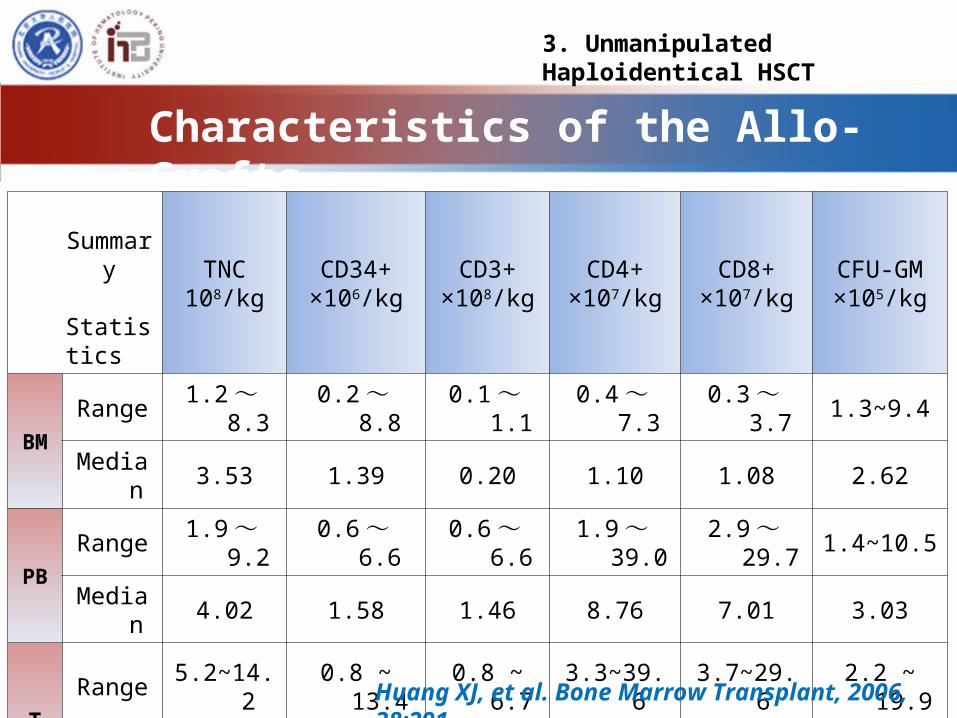
Characteristics of the Allo-Grafts
Summary Statistics
TNC108/kg
CD34+×106/kg
CD3+×108/kg
CD4+×107/kg
CD8+×107/kg
CFU-GM×105/kg
BMRange 1.2 ~ 8.3 0.2 ~ 8.8 0.1 ~ 1.1 0.4 ~ 7.3 0.3 ~ 3.7 1.3~9.4
Median 3.53 1.39 0.20 1.10 1.08 2.62
PBRange 1.9 ~ 9.2 0.6 ~ 6.6 0.6 ~ 6.6 1.9 ~ 39.0 2.9 ~ 29.7 1.4~10.5
Median 4.02 1.58 1.46 8.76 7.01 3.03
TRange 5.2~14.2 0.8 ~ 13.4 0.8 ~ 6.7 3.3~39.6 3.7~29.6 2.2 ~ 19.9
Median 7.56 2.65 1.77 10.39 7.87 5.21
Huang XJ, et al. Bone Marrow Transplant, 2006, 38:291
3. Unmanipulated Haploidentical HSCT

Huang XJ, et al. Biol Blood Marrow Transplant 2009, 15(2)Huang XJ, et al. Biol Blood Marrow Transplant 2011; 17(6)
Cumulative incidence of aGVHDafter HLA-mismatched allo-HSCT
Haplo=81
Identical=36
P=0.11
3. Unmanipulated Haploidentical HSCT

Probability of aGVHD with locus disparity
Huang XJ, et al. Bone Marrow Transplant. 2006;38(4):291-7.
3. Unmanipulated Haploidentical HSCT

DFS & OS compared with HLA Matched Donor
Huang XJ, et al. Blood, 2006, 107(8):3065-3073
3. Unmanipulated Haploidentical HSCT
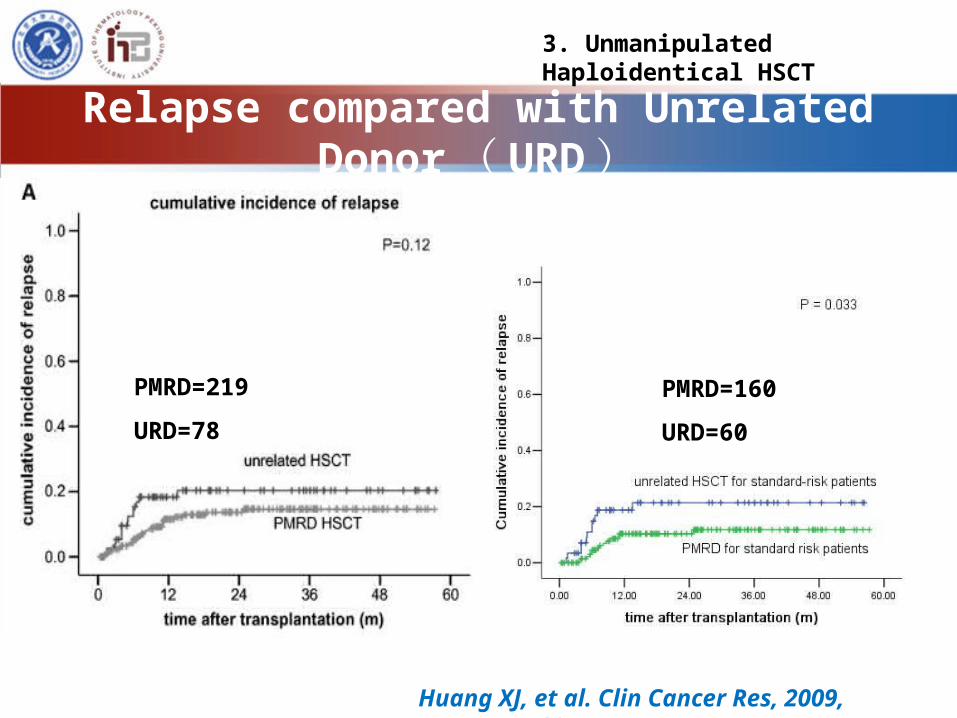
Relapse compared with Unrelated Donor ( URD)
Huang XJ, et al. Clin Cancer Res, 2009, 15:4777-4783
PMRD=219
URD=78
PMRD=160
URD=60
3. Unmanipulated Haploidentical HSCT

Relapse compared with Identical Sibling ( ISD)
HuangXJ, et al. Biol Blood Marrow Transplant. 2011;17(6)
Haplo=81
Identical=36
3. Unmanipulated Haploidentical HSCT

OS & DFS compared with ISD
PMRD=81
ISD=36P = 0.048 P = 0.029
HuangXJ, et al. Biol Blood Marrow Transplant. 2011;17(6)
Haplo=81
Identical=36
3. Unmanipulated Haploidentical HSCT

Superior Graft-versus-Leukemia effect
HaploidenticalHLA-identical
sibling
High risk acute leukemia
HuangXJ, et al. Biol Blood Marrow Transplant. 2011 ;17(6):821-30
3. Unmanipulated Haploidentical HSCT

No. of Haploidentical HSCT accumulated in PUIH
PUIH data
3. Unmanipulated Haploidentical HSCT
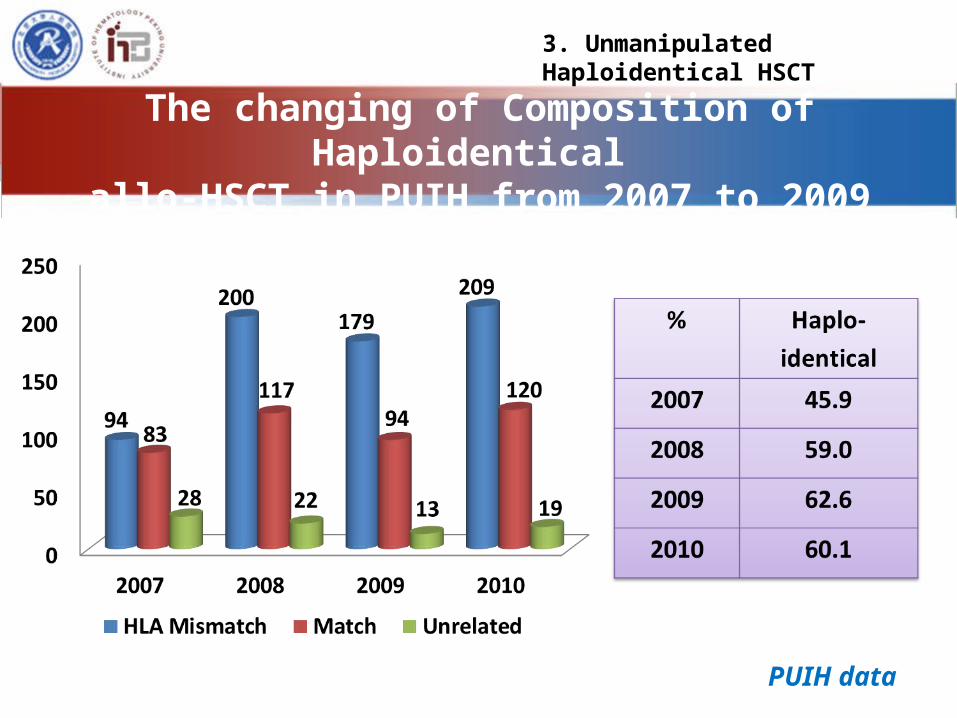
The changing of Composition of Haploidentical allo-HSCT in PUIH from 2007 to 2009
PUIH data
3. Unmanipulated Haploidentical HSCT

Studies on HLA-mismatched/haploidentical stem cell transplantation (GIAC)
Patients (n) Disease Conditioning
GVHDprophylaxis
aGHVD cGVHD TRM Relapse LFS Reference
35 AML/ALL/
CML/DLBCL/ ATL
Standard intensity±TBI
Tacrolimus based 56% 19% 11 pt 9 pt 40% Ichinohe et
al. (2004)
171 ALL/AML/CML/MDS
Bu/Cy/Ara-C/MeCCNU+
CsA/MTX/MMF 55% 21.3% 19% SR @
2yrs SR 12% SR 68% @ 2yrs
Huang et al. (2006)
135 ALL/AML/CML/MDS
Bu/Cy/Ara-C/MeCCNU+ATG
CsA/MTX/MMF
(II-IV) 40% 55% 22% 18% 64% @
yrs Lu et al. (2006)
68 AML/ALL/CML/MDS/ TBI/Cy/Flu Cy/MMF/ (II-IV) 5% * 4% @ 100
days 51% @ 1 yr 34% @ 1yr
Luznik et al. (2008)
29 AML/ALL/CML/NHL/
Flu/Mel/OKT3/thiotepa
CD3/CD19 depletion
(II-IV) 48% 3 pt 20% @ 100
days 12 pt 35% @ 1yr
Bethge et al. (2008)
42 AML/ALL/CML Bu/Cy/Ara-C/
MeCCNU+ATG
CsA/MTX/MMF 57.2% 27.2% 20.4±6.5% @
1yr 21.43% 57.3±8% @ 3yrs
Liu et al. (2008)
93 CML Bu/Cy/Ara-C/MeCCNU+
CsA/MTX/MMF 64.25% 27.16% 28.3% @ 1yr CP1 3.77% 76.5% @
1yr Huang et al.
(2008)
45 AML/ALL/CML/NHL TBI/Cy/Ara-C/ATG CsA/MTX/
MMF/ (II-IV) 9 pt 3 pt 11 pt 24 pt Wang et al. (2009)
46 AML/CML/ALL TBI/Cy/Ara-C/ATG CsA/MTX/MMF (I-II) 10.9% 8.7% @ 2yrs 23.9% @
2yr 70.6% @
2yrs Chen et al.
(2009)
250 AML/ALL Bu/Cy/Ara-C/
MeCCNU+ ATG CsA/MTX/MMF 45.8% 31.3% AML 11.9%
@ 3yrs AML 19.4%
@ 3yrs AML70.7
%3yrs Huang et al.
(2009)
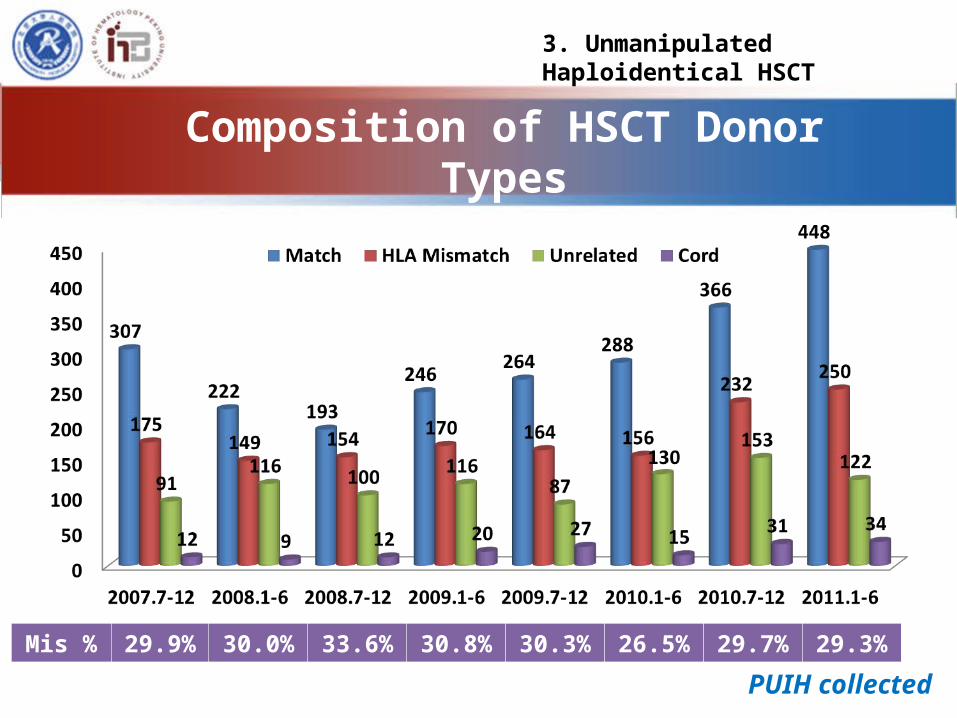
Composition of HSCT Donor Types in 24 Transplant Units in China
PUIH collected
Mis % 29.9% 30.0% 33.6% 30.8% 30.3% 26.5% 29.7% 29.3%
3. Unmanipulated Haploidentical HSCT
Huang XJ, et al. BMT, 2006, 38:291
Huang XJ, et al. Blood, 2006, 107(8):3065-3073
Huang XJ, et al. Clin Cancer Res, 2009, 15: 4777-4783
Huang XJ, et al. BBMT. 2011 Feb;17(2):197-204
Part I Conclusions
• G-BM combined with PBSC from haploidentical family donors, without in vitro TCD, may be used as a good source of stem cells for allo-HSCT
• There is no difference in OS and LFS between patients receiving allografts from PMRD and URD
3. Unmanipulated Haploidentical HSCT
3.Unmanipulated Haploidentical HSCT
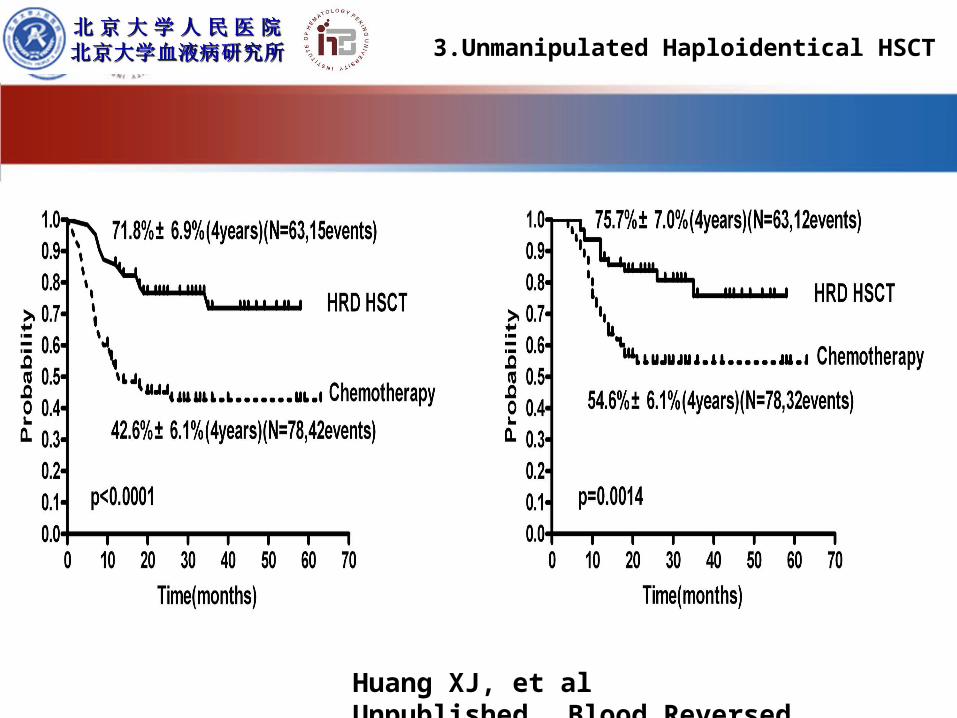
Huang XJ, et al Unpublished , Blood Reversed
Part II : Strategy to Improve the Clinical Results
1• Modified Donor Lymphocyte Infusion(DLI)
2• Manipulating the Graft
3• Optimize KIR ligand match/mismatch
4• Improve Immune Reconstitution
3. Unmanipulated Haploidentical HSCT

Relapse Remains a Problem after HSCT
High risk leukemiaHigh risk leukemia
Huang XJ et al, Biol Blood Marrow Transplant. 2009 Feb;15(2)
Especiallyfor advancedleukemia(58%- 74%)
3. Unmanipulated Haploidentical HSCT

Strategy-1 Our modified DLI
G-CSF primed peripheral blood progenitor cells instead of steady
donor lymphocyte harvests
Short-term CsA/MTX for prevention of
DLI-associated GVHD
GPBSCIGPBSCI
Huang XJ et al, LEUKEMIA, 2006 ; 20 , 365-368Huang XJ et al, Bone Marrow Transplant. 2009;44(5):309-16
3. Unmanipulated Haploidentical HSCT
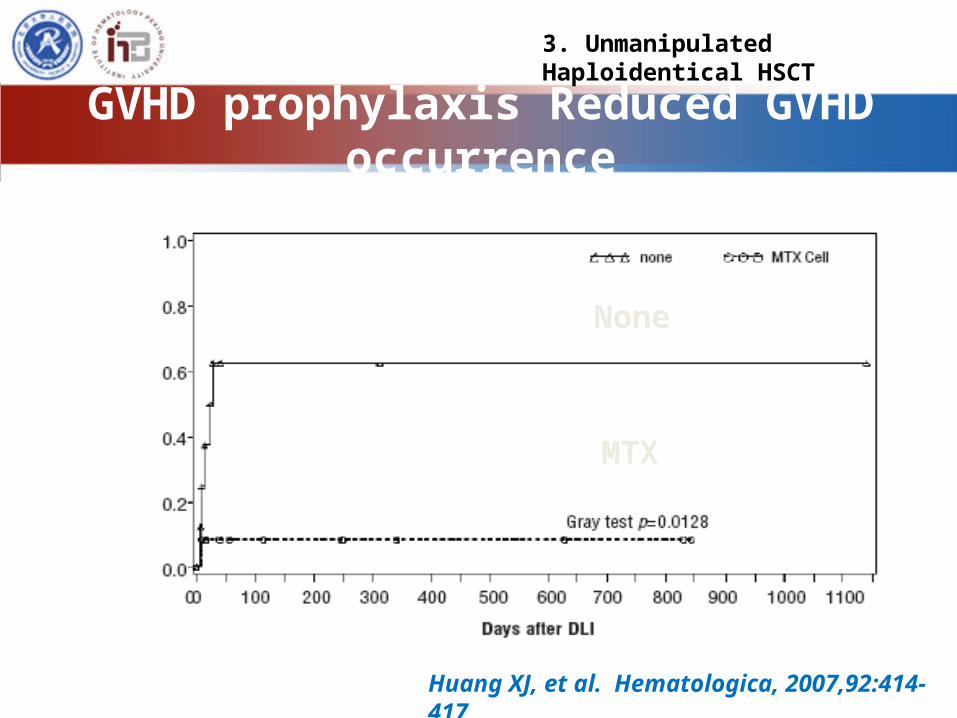
GVHD prophylaxis Reduced GVHD occurrence
Huang XJ, et al. Hematologica, 2007,92:414-417
None
MTX
3. Unmanipulated Haploidentical HSCT

Prevention of relapse using modified DLI can
significantly increase survival following HLA-
mismatched/Haplo-identical HSCT in patients
with advanced-stage, acute leukemia
3. Unmanipulated Haploidentical HSCT
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted

Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
Diagnosis N=75 Jan,2003 - Sep,2010
AMLN=42
>CR2 7
NR+REL 35
ALLN=33
>CR2 8
NR+REL 25
Patients Characteristic
3. Unmanipulated Haploidentical HSCT
Prophylactic GPBPCI
• Performed at 70 (20 ~ 314) d after HSCT
• MNC 1.0 (0.5-2.0) 108/kg • CD3+ 0.93 (0.2-2.12) 108/kg
• No patients had profound and lasting pancytopenia after the prophylactic infusion
3. Unmanipulated Haploidentical HSCT

Cumulative incidence of grade to acute Ⅲ ⅣGVHD
GVHD prophylaxis < 2w: 49.5%
GVHD prophylaxis 2 ~4w: 31.6%
GVHD prophylaxis 4 ~6w: 14.4%
GVHD prophylaxis >6w: 9.3%
The risk factor of DLI-associated acute GVHD
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
3. Unmanipulated Haploidentical HSCT
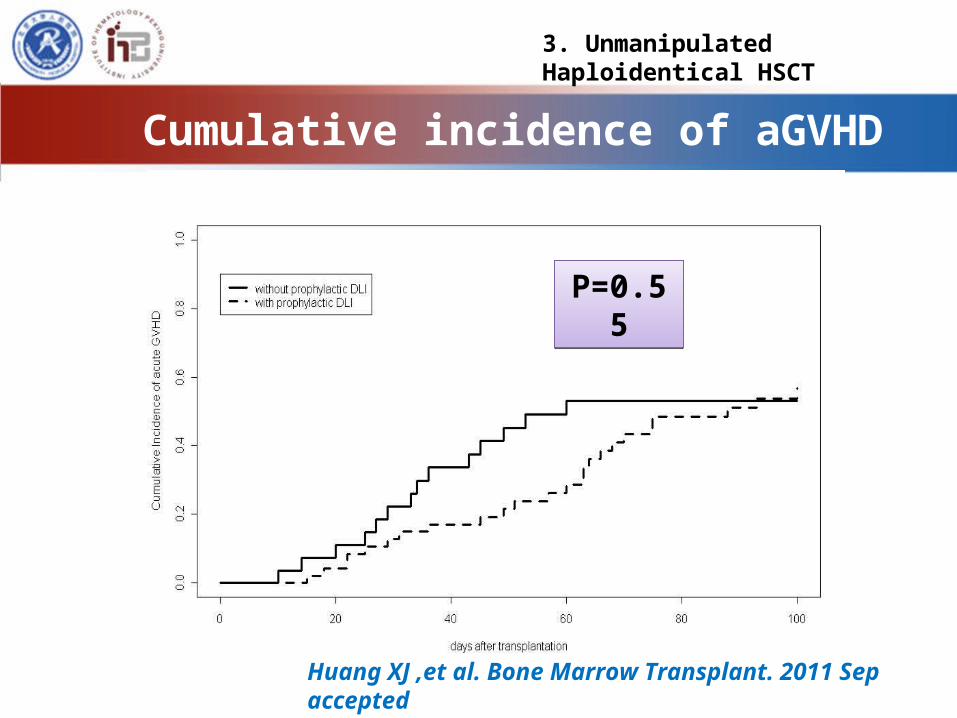
Cumulative incidence of aGVHD
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
P=0.55P=0.55
3. Unmanipulated Haploidentical HSCT
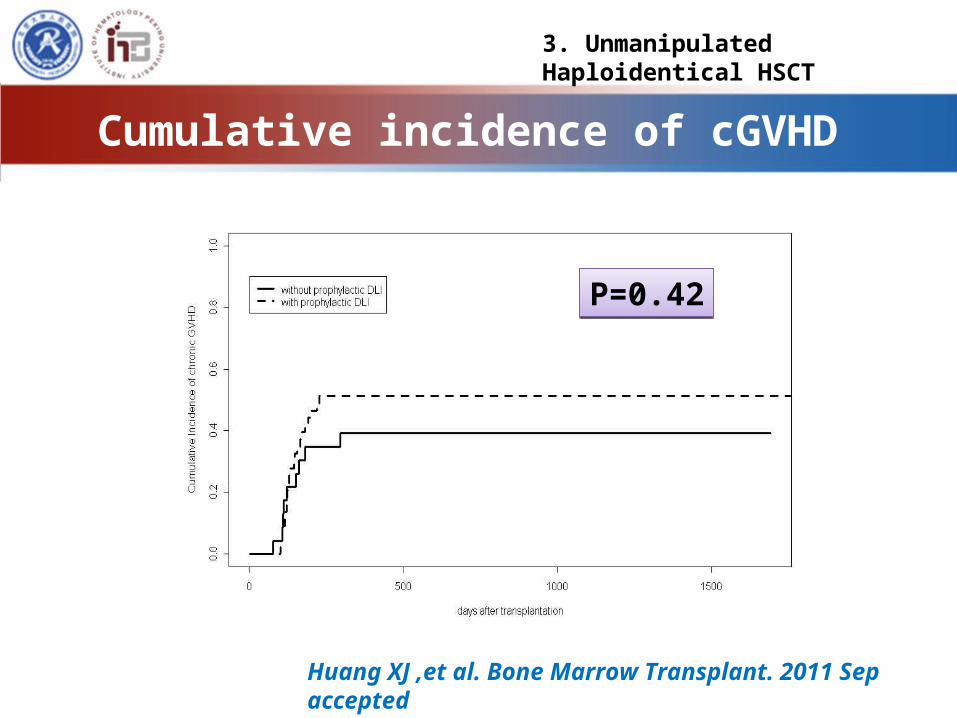
Cumulative incidence of cGVHD
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
P=0.42P=0.42
3. Unmanipulated Haploidentical HSCT

Cumulative incidence of TRM
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
P=0.95P=0.95
3. Unmanipulated Haploidentical HSCT
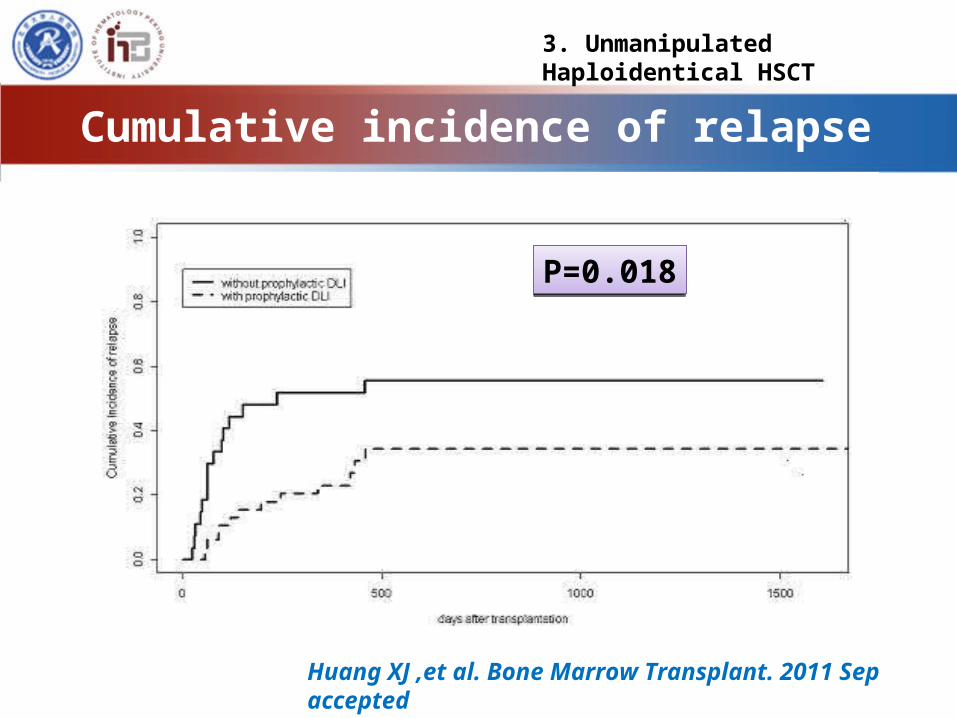
Cumulative incidence of relapse
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
P=0.018P=0.018
3. Unmanipulated Haploidentical HSCT

Probability of OS
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
(P=0.013)(P=0.013)
3. Unmanipulated Haploidentical HSCT

Lower relapse rate, a similar NRM, and a higher
survival probability compared with non-DLI
Can significantly increase the survival of
patients with advanced-stage, acute leukemia
even after HLA-mismatched, T-cell-replete HSCT
Modified prophylactic DLI after HLA-mismatched/Haplo-identical HSCT
Huang XJ ,et al. Bone Marrow Transplant. 2011 Sep accepted
3. Unmanipulated Haploidentical HSCT

Risk stratification-directed DLI could reduce relapse of standard-risk acute
leukemia after allo-HSCT
Institute of Hematology Peking UniversityBeijing, China
ASH 2111 Oral Presentation

Efficacy of intervention
Groups 3yr-Relapse TRM OS LFSA 18.1% 19.7% 66.0% 61.6% B 68.0% 11.2% 23.9% 20.8% C 29.8% 15.6% 55.4% 52.5%
ASH 2111 Oral Presentation
Strategy-1 Conclusion
m-DLI can be used for the
treatment and prophylaxis of relapse
after haplo-identical HSCT
3. Unmanipulated Haploidentical HSCT

Dose of Th17 and GVHD
0 50 100 1500
20
40
60
80
Low Th17 groupHigh Th17 group
days after transplantation
Cu
mu
lati
ve in
cid
en
ce Dose of Th17 and GVHD
0 50 100 1500
20
40
60
80
Low Th17 groupHigh Th17 group
days after transplantation
Cu
mu
lati
ve in
cid
en
ce
Tc17 dose and GVHD
0 50 100 1500
20
40
60
80Low Tc17 groupHigh Tc17 group
days after transplantation
Cu
mu
lati
ve in
cid
en
ce Tc17 dose and GVHD
0 50 100 1500
20
40
60
80Low Tc17 groupHigh Tc17 group
days after transplantation
Cu
mu
lati
ve in
cid
en
ce
0 50 100 1500
20
40
60
80
100
Low dose
other dose
High dose
days after transplantation
Cum
ulat
ive
inci
denc
e0 50 100 150
0
20
40
60
80
100
Low dose
other dose
High dose
days after transplantation
Cum
ulat
ive
inci
denc
ep=0.005
p=0.00017
p=0.001
( n=12)
( n=17)
( n=12)
HuangXJ , et al,
Eur J Immunol. 2011 Feb;41(2):514-26
Predictive value of Th17 cells and Tc17 cells in allo-graft on acute GVHD

Treating donor mice with rhIL-11 and rhG-CSF promotes transplant-tolerance and preserves the effects of GVL after allogeneic bone
marrow transplantation
HuangXJ, et al. Leuk Res. 2009 Jan;33(1):123-8
Effects of different cytokines treatment on the recipients’ T cells proliferation activity in response to host alloantigens +14 d after BMT.
Effects of different cytokines treatment on the recipients’ T cells proliferation activity in response to host alloantigens +14 d after BMT.
Strategy-2 Conclusion
We may decrease the incidence of GVHD by manipulating the cell contents or function of graft? Mobilization with IL-11 plus G-CSF ?
3. Unmanipulated Haploidentical HSCT

Strategy-3 KIR ligand match/mismatch to outcome on pretransplantation category
aGVHD TRM Relapse
OS
KIR mismatchKIR mismatch
KIR matchKIR match
Huang XJ, et al. Biol Bone Marrow Transplant, 2008,14(3)

Strategy-3 Conclusion
• KIR ligand mismatch is associated with higher aGVHD, a greater relapse rate, and inferior survival in our haploidentical GIAC protocol---Donor Slection ?
3. Unmanipulated Haploidentical HSCT

70.0060.0050.0040.0030.0020.0010.000.00
Months posttransplant
1.0
0.8
0.6
0.4
0.2
0.0Prop
ortio
ns o
f pat
ient
s (%
)
300/ul-小于censored
300/ul-大于等于censored
300/ul小于
300/ul大于等于
Cutoff ?按照 值 划分
70.0060.0050.0040.0030.0020.0010.000.00
Months posttransplant
1.0
0.8
0.6
0.4
0.2
0.0Prop
ortio
ns o
f pat
ient
s (%
)
300/ul-小于censored
300/ul-大于等于censored
300/ul小于
300/ul大于等于
Cutoff ?按照 值 划分
ALC-30 >300/ul
ALC-30 >300/ul
ALC-30≤300/ul
ALC-30≤300/ul
P<0.001P<0.001 n=206n=206
Strategy-4 Immune Reconstitution
Huang XJ, et al. Bone Marrow Transplant, 2009,43: 29-36
TRM
3. Unmanipulated Haploidentical HSCT
70.0060.0050.0040.0030.0020.0010.000.00
Months posttransplant
1.0
0.8
0.6
0.4
0.2
0.0
Leuk
emia
-fre
e su
rvival
300/ul-censored小于
300/ul-大于等于censored
300/ul小于
300/ul大于等于Cutoff ?按照 值 划分
70.0060.0050.0040.0030.0020.0010.000.00
Months posttransplant
1.0
0.8
0.6
0.4
0.2
0.0
Leuk
emia
-fre
e su
rvival
300/ul-censored小于
300/ul-大于等于censored
300/ul小于
300/ul大于等于Cutoff ?按照 值 划分
ALC-30>300/ulALC-30>300/ul
ALC-30≤300/ulALC-30≤300/ul

0
200
400
600
800
1000
1200
1400
1600
1800
2000
30 60 90 120 180 270 360
CD3+
cel
ls/u
l
Days f rom transpl antati on
HLA matchHLA mi smatchNormal
**
The counts of reconstituted CD3+ cells (cells/μl ) were significantly lower in HLA-mismatched patients at days 30 than those in HLA-matched patients, which reached normal level at days 60 in both HLA-matched and -mismatched patients. ** P < 0.001
The counts of reconstituted CD3+ cells (cells/μl ) were significantly lower in HLA-mismatched patients at days 30 than those in HLA-matched patients, which reached normal level at days 60 in both HLA-matched and -mismatched patients. ** P < 0.001
HuangXJ, J Cli Imm Online Publication
Comparison of Reconstituted T cells subgroup between HLA match and mismatch

0
100
200
300
400
500
600
700
800
30 60 90 120 180 270 360Days af ter transpl antati on
CD4+
cel
ls/u
lHLA matchHLA mi smatchNormal
** * ***
The counts of reconstituted CD4+ cells (cells/μl ) were significantly lower in HLA-mismatched patients at days 30, 60, 90, and 120 than those in HLA-matched patients, which did not reached normal level until 360 in both HLA-matched and mismatched patients, respectively. * P < 0.05, ** P < 0.001
The counts of reconstituted CD4+ cells (cells/μl ) were significantly lower in HLA-mismatched patients at days 30, 60, 90, and 120 than those in HLA-matched patients, which did not reached normal level until 360 in both HLA-matched and mismatched patients, respectively. * P < 0.05, ** P < 0.001
HuangXJ, J Cli Imm Online Publication
Comparison of Reconstituted T cells subgroup between HLA match and mismatch
Strategy-4 Conclusion
Novel approach to improve the recovery of immune reconstitution are greatly required. IL-2 after HSCT ?
A Randomized Clinical Trial Is Undergoing For Evaluing IL-2 After Haplo-identical HSCT In PUIH
3. Unmanipulated Haploidentical HSCT

Acknowledgements
Stem cell collection centerHai-Yin ZhengHong XuQing ZhaoSu Wang
Department of Bone Marrow Transplant Dai-Hong LiuFeng-Rong WangHuan ChenJing-Zhi WangKai-Yan LiuLan-Ping XuWei HanXiao-Hui ZhangYu-Hong ChenYu Wang
Laboratory of PUIHDan LiYa-Zhen QinYan-Rong LiuYue-Yun Lai