hcv can be cured- friday.ppt - learning stream · chronic hepatitis c virus infection: developing...
TRANSCRIPT
6/15/2017
1
Harlan WrightMedical Director; Liver Director, Liver Transplant/Hepatology
Oklahoma Transplant Center

6/15/2017
2
• Discover the increasing burden of HCV
• Understand that HCV is a curable disease
• Consider your role in screening, diagnosing, and referring patients
Today’s Meeting Goals
• To use the keypad, simply press the button that corresponds with the option that you wish to choose
• There is no Enter button; simply press the voting button
• If you make a mistake, you can correct it by pressing the button that correlates with your response before polling ends
• Your last selection is the one that counts
Keypad Instructions
6/15/2017
3
In the past month, how many patients did you screen for HCV using an HCV antibody test?
1. 02. 1-53. 6-104. 11-195. 20+
In the past month, for how many patients did you order an HCV RNA testto confirm diagnosis?
1. 02. 1-53. 6-104. 11-195. 20+
6/15/2017
4
What percentage of your HCV-diagnosed patients are currently under the care of a specialist?
1. 0%2. ~25%3. ~50%4. ~75%5. 100%
Do you currently prescribe therapy for HCV?
1. Yes2. No

6/15/2017
5
What is HCV?

6/15/2017
6
• An RNA virus that used to be known as non-A, non-B hepatitis until it was discovered in 19881
• No vaccine available
• First therapy approved in 19912
• Before 2011, HCV treatment could last as long as a year, with cure* (SVR) rates of 40%–50% for the most common genotype in the US3
• Since that time, scientific advances have made HCV treatment shorter and more effective
• There are interferon-free treatment options available that have shown cure (SVR) rates of 90% and greater in clinical studies4
*Cure, also known as sustained virologic response (SVR), is defined as no detectable HCV in the blood at 12 or more weeks after therapy is complete4,5
HCV History
1. CDC. MMWR Morb Mortal Wkly Rep. 1998;47(RR-19):1-39. 2. Swartz ML. Gastroenterol Nurs. 1991;14(1):40-43. 3. Ghany MG et al. Hepatology. 2011;54(4):1433-1444. 4. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed December 7, 2015. 5. US Department of Health and Human Services, Center for Drug Evaluation and Research. Draft Guidance for Industry. Chronic Hepatitis C Virus Infection: Developing Direct-Acting Antiviral Drugs for Treatment. October 2013.
HCV History

6/15/2017
7
• 6 HCV genotypes1
• Genotypic prevalence varies by geography1
• Genotype 1 is the most common in the US and accounts for approximately 79% of HCV infections1
HCV Genotypes
1. Zein NN et al. Ann Intern Med. 1996;125:634-639.
Impact of HCV
6/15/2017
8
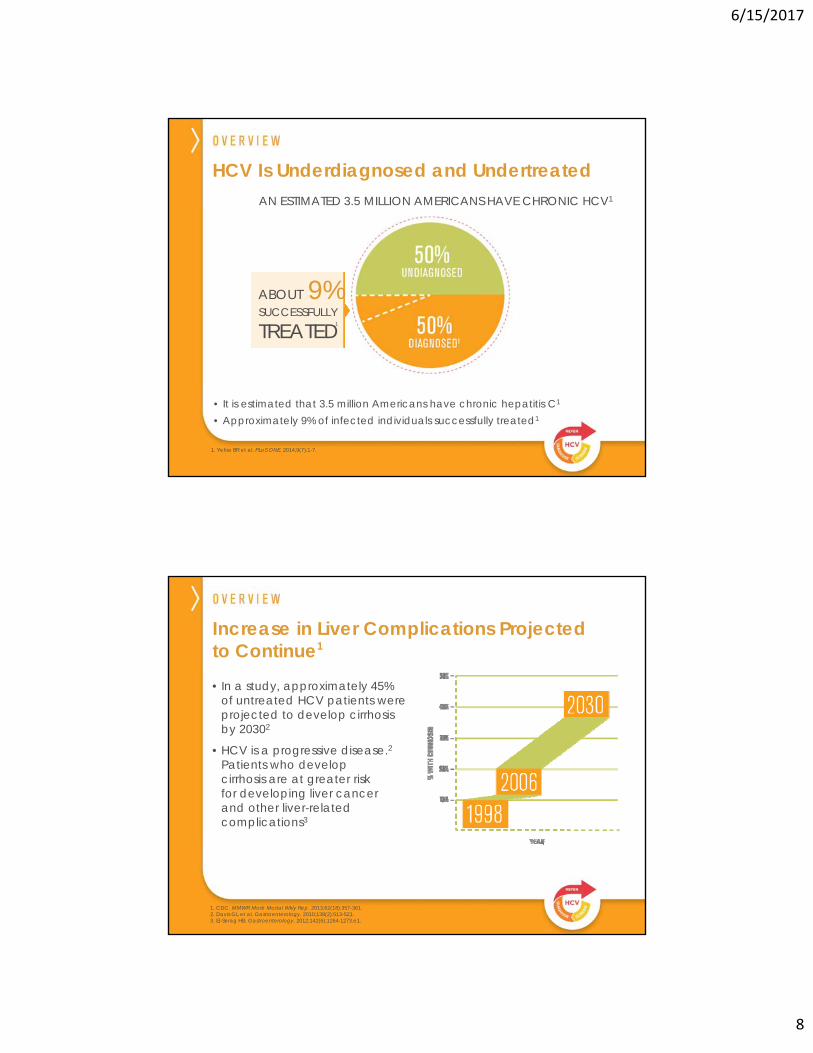
HCV Is Underdiagnosed and Undertreated
1. Yehia BR et al. PLoS ONE. 2014;9(7):1-7.
• It is estimated that 3.5 million Americans have chronic hepatitis C1
• Approximately 9% of infected individuals successfully treated1
AN ESTIMATED 3.5 MILLION AMERICANS HAVE CHRONIC HCV1
1
ABOUT 9%SUCCESSFULLY
TREATED
Increase in Liver Complications Projected to Continue1
1. CDC. MMWR Morb Mortal Wkly Rep. 2013;62(18):357-361. 2. Davis GL et al. Gastroenterology. 2010;138(2):513-521.3. El-Serag HB. Gastroenterology. 2012;142(6):1264-1273.e1.
30% of untreated HCV patients will
progress to cirrhosis by 20159
• In a study, approximately 45% of untreated HCV patients were projected to develop cirrhosis by 20302
• HCV is a progressive disease.2Patients who develop cirrhosis are at greater risk for developing liver cancer and other liver-related complications3

6/15/2017
9
Liver Complications in HCV Patients Contribute to a Shorter Lifespan3
In the US, HCV is the Leading Cause of Liver Transplantation1 and Liver Cancer2
1. Kim WR et al. Am J Transplant. 2014;14(suppl 1):69-96.2. CDC. http://www.cdc.gov/nchhstp/newsroom/docs/HCV-TestingFactSheetNoEmbargo508.pdf. Accessed December 7, 2015.3. Smith BD et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.
1. Ly KN et al. Ann Intern Med. 2012;156(4):271-278.2. Holmberg S, Ly KN, Xing J, Moorman AC. Rising mortality from hepatitis C virus in the United States, 2002-2013. Paper presented
at: American College of Gastroenterology Annual Scientific Meeting and Postgraduate Course; October 16-21, 2015; Honolulu, HI.
HCV Has a Mortality Rate That Exceeds HIV1,2,a
aExtended from: Ly KN et al. Ann Intern Med. 2012;156(4):271-278.
6/15/2017
10
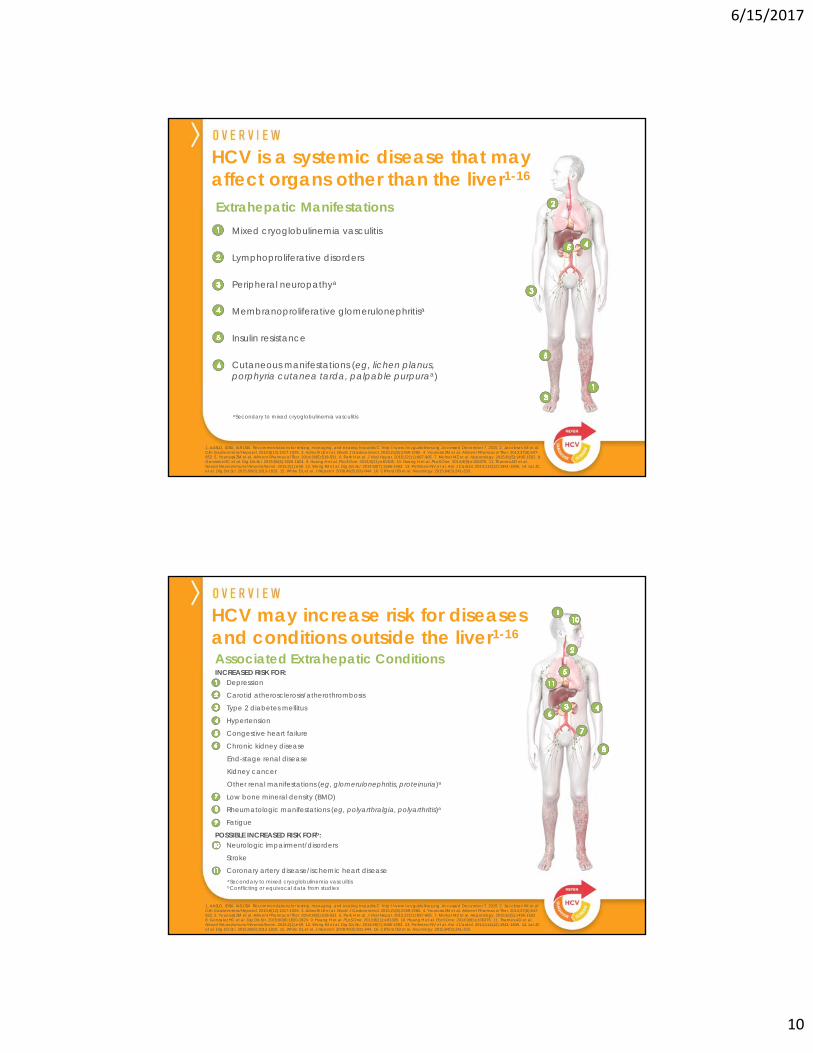
Mixed cryoglobulinemia vasculitis
Lymphoproliferative disorders
Peripheral neuropathya
Membranoproliferative glomerulonephritisa
Insulin resistance
Cutaneous manifestations (eg, lichen planus,porphyria cutanea tarda, palpable purpuraa)
aSecondary to mixed cryoglobulinemia vasculitis
HCV is a systemic disease that may affect organs other than the liver1-16
1. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed December 7, 2015. 2. Jacobson IM et al. Clin Gastroenterol Hepatol. 2010;8(12):1017-1029. 3. Adinolfi LE et al. World J Gastroenterol. 2015;21(8):2269-2280. 4. Younossi ZM et al. Aliment Pharmacol Ther. 2013;37(6):647-652. 5. Younossi ZM et al. Aliment Pharmacol Ther. 2014;39(5):518-531. 6. Park H et al. J Viral Hepat. 2015;22(11):897-905. 7. Molnar MZ et al. Hepatology. 2015;61(5):1495-1502. 8. Gonzalez HC et al. Dig Dis Sci. 2015;60(6):1820-1824. 9. Huang H et al. PLoS One. 2013;8(11):e81305. 10. Huang H et al. PLoS One. 2014;9(9):e106376. 11. Thames AD et al. Neurol Neuroimmunol Neuroinflamm. 2015;2(1):e59. 12. Wong RJ et al. Dig Dis Sci. 2014;59(7):1586-1593. 13. Pothineni NV et al. Am J Cardiol. 2014;114(12):1841-1845. 14. Lai JC et al. Dig Dis Sci. 2015;60(6):1813-1819. 15. White DL et al. J Hepatol. 2008;49(5):831-844. 16. Clifford DB et al. Neurology. 2015;84(3):241-250.
Extrahepatic Manifestations
Associated Extrahepatic Conditions INCREASED RISK FOR:
Depression
Carotid atherosclerosis/atherothrombosis
Type 2 diabetes mellitus
Hypertension
Congestive heart failure
Chronic kidney disease
End-stage renal disease
Kidney cancer
Other renal manifestations (eg, glomerulonephritis, proteinuria)a
Low bone mineral density (BMD)
Rheumatologic manifestations (eg, polyarthralgia, polyarthritis)a
Fatigue
POSSIBLE INCREASED RISK FORb: Neurologic impairment/disorders
Stroke
Coronary artery disease/ischemic heart disease
HCV may increase risk for diseases and conditions outside the liver1-16
1. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed December 7, 2015. 2. Jacobson IM et al. Clin Gastroenterol Hepatol. 2010;8(12):1017-1029. 3. Adinolfi LE et al. World J Gastroenterol. 2015;21(8):2269-2280. 4. Younossi ZM et al. Aliment Pharmacol Ther. 2013;37(6):647-652. 5. Younossi ZM et al. Aliment Pharmacol Ther. 2014;39(5):518-531. 6. Park H et al. J Viral Hepat. 2015;22(11):897-905. 7. Molnar MZ et al. Hepatology. 2015;61(5):1495-1502. 8. Gonzalez HC et al. Dig Dis Sci. 2015;60(6):1820-1824. 9. Huang H et al. PLoS One. 2013;8(11):e81305. 10. Huang H et al. PLoS One. 2014;9(9):e106376. 11. Thames AD et al. Neurol Neuroimmunol Neuroinflamm. 2015;2(1):e59. 12. Wong RJ et al. Dig Dis Sci. 2014;59(7):1586-1593. 13. Pothineni NV et al. Am J Cardiol. 2014;114(12):1841-1845. 14. Lai JC et al. Dig Dis Sci. 2015;60(6):1813-1819. 15. White DL et al. J Hepatol. 2008;49(5):831-844. 16. Clifford DB et al. Neurology. 2015;84(3):241-250.
aSecondary to mixed cryoglobulinemia vasculitisbConflicting or equivocal data from studies

6/15/2017
11
HCV Can Be Cured
Unlike Some Chronic Conditions, HCV Can Be Cured
Hypertension
Diabetes
HCV
MANAGEABLE
CURABLE

6/15/2017
12
HCV does not integrate into the nuclei of infected cells, while HBV and HIV DNA are incorporated into the nucleus of the cell1
Why Is Cure Possible?
1. Soriano V et al. J Antimicrob Chemother. 2008;62(1):1-4.
*HBV cccDNA (covalently closed circular DNA): accumulates in hepatocyte nuclei, acting as a template for viral messenger RNA transcription.†HIV proviral DNA: integrates into the chromatin of infected cells, acting as the template for the transcription of viral genes.
Nucleus Host Cell Host DNA
Cure, also known as sustained virologic response (SVR), is defined as no detectable HCV in the blood at 12 or more weeks after therapy is complete1,2
What Defines HCV Cure?
1. US Department of Health and Human Services, Center for Drug Evaluation and Research. Draft Guidance for Industry. Chronic Hepatitis C Virus Infection: Developing Direct-Acting Antiviral Drugs for Treatment. October 2013.
2. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed December 7, 2015.
3. Swain MG et al. Gastroenterology. 2010;139(5):1593-1601.
• In some instances, HCV treatment does not result in cure, or SVR, because the virus does not reach undetectable levels or because it does not stay undetectable after therapy completion
• In one study, of those patients who reached SVR, 99% had undetectable levels of HCV RNA more than 4 years after treatment end3
• These patients do not experience viral recurrence and may be considered to be cured3

6/15/2017
13
• Cure, or SVR, is associated with improvements in disease complications, such as rates of hepatocellular carcinoma, ascites, hepatic encephalopathy, and variceal bleeding1,2
Cure Can Lead to Improvements in Disease Complications1,2 and Mortality3
1. Bruno S et al. Hepatology. 2007;45(3):579-587.2. Singal AG et al. Clin Gastroenterol Hepatol. 2010;8(3):280-288.e1.3. van der Meer AJ et al. JAMA. 2012;308(24):2584-2593.
SVR is also associated with reduced risk of all-cause mortality3*
*These data are from an international, multicenter, long-term follow-up study from 5 large tertiary care hospitals in Europe and Canada. Patients with chronic HCV infection started an interferon-based treatment regimen between 1990 and 2003 (n=530).
Give your HCV patients access to treatment and a potential cure
6/15/2017
14
1. Elevated liver enzymes2. Symptoms3. Behavioral risk factors4. HIV infection5. Age cohort6. I currently do not screen
Currently, what is your primary HCV screening criterion?
6/15/2017
15
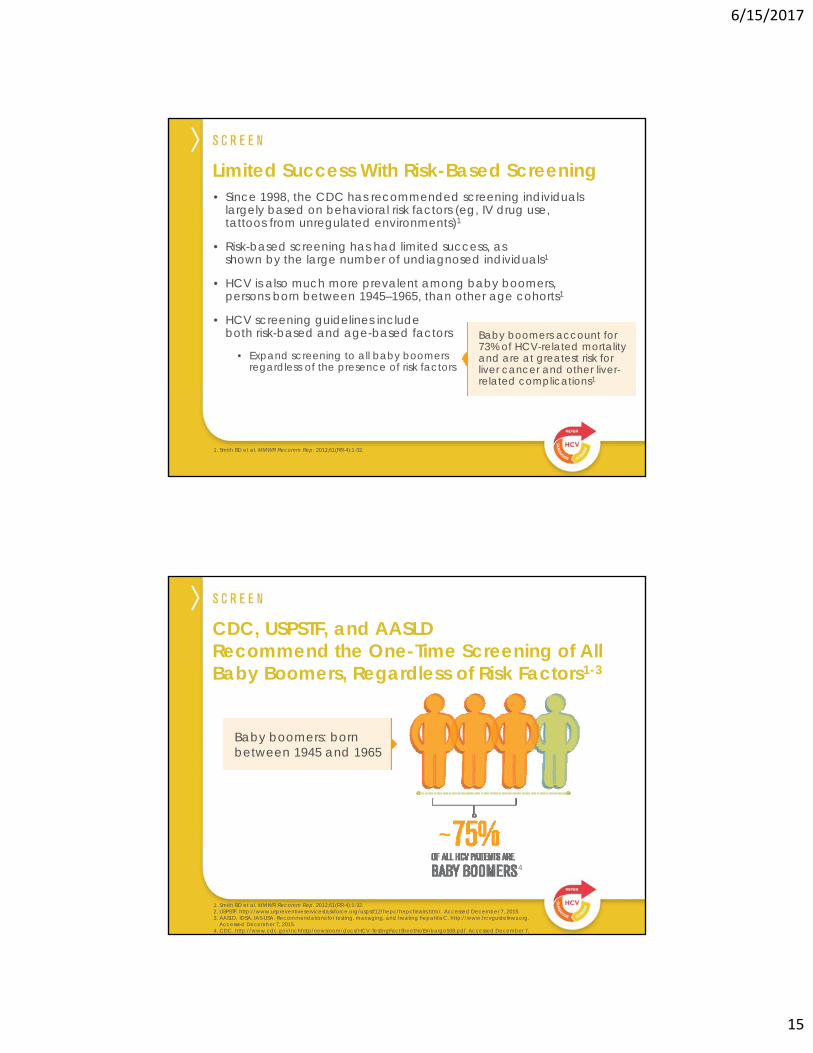
• Since 1998, the CDC has recommended screening individuals largely based on behavioral risk factors (eg, IV drug use, tattoos from unregulated environments)1
• Risk-based screening has had limited success, as shown by the large number of undiagnosed individuals1
• HCV is also much more prevalent among baby boomers, persons born between 1945–1965, than other age cohorts1
• HCV screening guidelines include both risk-based and age-based factors
• Expand screening to all baby boomers regardless of the presence of risk factors
Limited Success With Risk-Based Screening
1. Smith BD et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.
Baby boomers account for 73% of HCV-related mortality and are at greatest risk for liver cancer and other liver-related complications1
CDC, USPSTF, and AASLD Recommend the One-Time Screening of All Baby Boomers, Regardless of Risk Factors1-3
1. Smith BD et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.2. USPSTF. http://www.uspreventiveservicestaskforce.org/uspstf12/hepc/hepcfinalrs.htm/. Accessed December 7, 2015.3. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org.
Accessed December 7, 2015.4. CDC. http://www.cdc.gov/nchhstp/newsroom/docs/HCV-TestingFactSheetNoEmbargo508.pdf. Accessed December 7, 20
Baby boomers: born between 1945 and 1965
4
~
6/15/2017
16
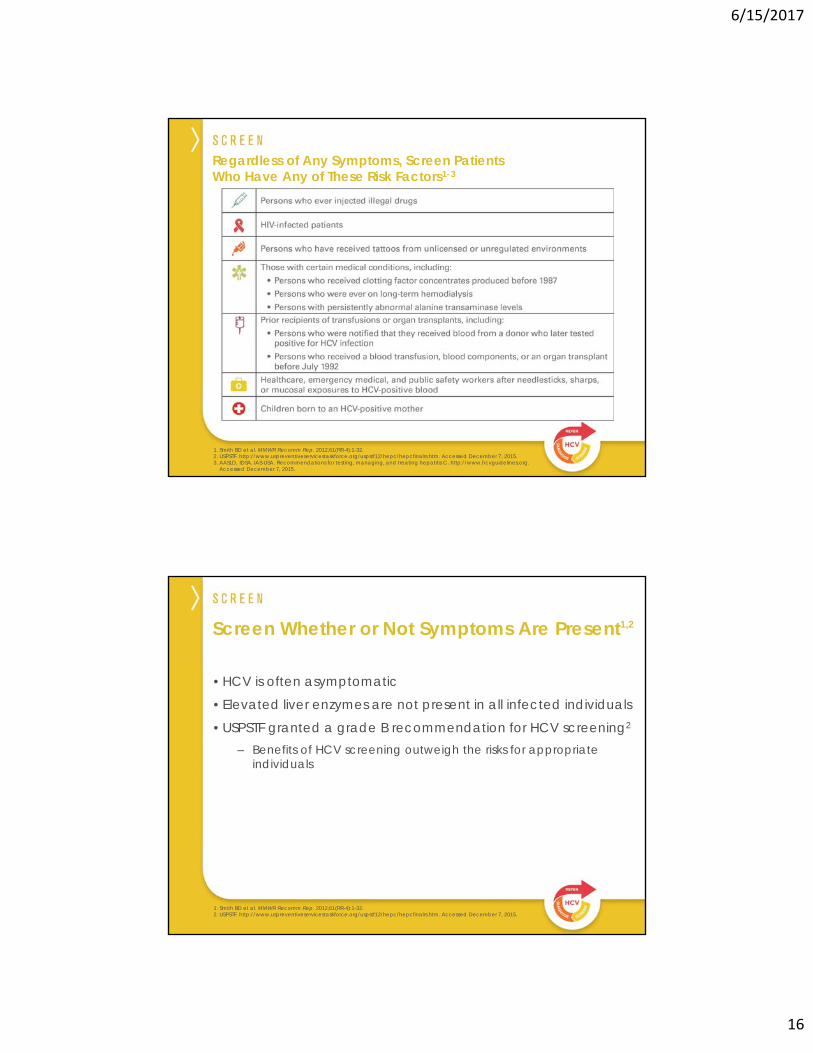
Regardless of Any Symptoms, Screen Patients Who Have Any of These Risk Factors1-3
1. Smith BD et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.2. USPSTF. http://www.uspreventiveservicestaskforce.org/uspstf12/hepc/hepcfinalrs.htm. Accessed December 7, 2015.3. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org.
Accessed December 7, 2015.
Screen Whether or Not Symptoms Are Present1,2
1. Smith BD et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.2. USPSTF. http://www.uspreventiveservicestaskforce.org/uspstf12/hepc/hepcfinalrs.htm. Accessed December 7, 2015.
• HCV is often asymptomatic
• Elevated liver enzymes are not present in all infected individuals
• USPSTF granted a grade B recommendation for HCV screening2
– Benefits of HCV screening outweigh the risks for appropriate individuals

6/15/2017
17
Which test do you typically use to screen for HCV?
1. Liver enzyme panel2. Acute hepatitis panel3. HCV antibody test4. Liver biopsy5. Abdominal ultrasound6. HCV RNA test7. I currently do not screen for HCV
• HCV is screened using a simple blood test to detect the presence of antibodies against HCV
• A positive antibody test is an indicator of exposure to HCV
– Elevated liver enzymes are not present in all infected individuals
• Talk with the patient before screening
– Explain why he/she should be screened
– Tell the patient that HCV is a progressive disease1
– Describe the screening process
How to Screen
Enable an EHR flag or standing order as a reminder to screen, diagnose, and refer patients.Such reminders have proven helpful in improving outcomes.2
1. Davis GL et al. Gastroenterology. 2010;138(2):513-521.2. Feldstein A et al. J Am Geriatr Soc. 2006;54(3):450-457.
Consider selecting a lab’s “reflex-testing” option at the screening step so an HCV RNA test will be run automaticallyif the antibody test is positive. (CPT CODE 86804)

6/15/2017
18
Antibody Negative– Patient not exposed to HCV
– No further action needed, unless exposure suspected in past 6 months
– If suspected, consider re-testing for HCV antibodies or running an HCV RNA test
Antibody Positive– Patient exposed to HCV
– An HCV RNA test is needed to confirm the chronic HCV diagnosis
– If the reflex option was ordered for the screening test, the antibody and HCV RNA results will be returned at the same time
Next Steps After HCV Antibody Test Results

6/15/2017
19
• Not everyone exposed to HCV becomes chronically infected– Approximately 20%–50% of patients clear HCV spontaneously
and do not develop a chronic HCV infection1
• Only by confirming the diagnosis can you be sure the patient has a chronic infection
Diagnosis Must Be Confirmed
1. AASLD, IDSA, IAS-USA. Recommendations for testing, managing and treating hepatitis C. http://www.hcvguidelines.org.Accessed December 7, 2015.
Consider selecting a lab’s “reflex-testing” option at the screening step so an HCV RNA test will be run automaticallyif the antibody test is positive. (CPT CODE 86804)
How to Diagnose• To test for a chronic HCV infection, an HCV RNA test
is used to detect HCV RNA in the blood
• Talk with your patients before diagnosis• Explain to the patient why an HCV RNA test is necessary
• Describe how the diagnostic test is performed
Positive results from HCV antibody test
Consider selecting a lab’s “reflex-testing” option at the screening step so an HCV RNA test will be run automatically if the antibody test is positive. (CPT CODE 86804)

6/15/2017
20
• Patient is not chronically infected with HCV
• No further medical evaluation for HCV infection is required
• Discuss the results with the patient
• Tell patient that he/she is not chronically infected, and no further testing or treatment is needed
• Confirm he/she understands how the virus is spread and the situations in which he/she could be exposed
• Explain that he/she will always test positive for HCV antibodies1
What to Do If HCV RNA Is Not Detected
1. CDC. http://www.cdc.gov/hepatitis/HCV/PDFs/HepCGettingTested.pdf. October 2013. Accessed December 7, 2015.
What to Do If HCV RNA Is Detected
• Patient is infected with HCV
• Consider ordering an HCV genotype test (optional)
• Refer patient to an HCV specialist for additional tests and treatment evaluation
• Discuss the diagnosis with the patient• Tell your patient that he/she is infected with HCV and will
be referred to a specialist for more tests and possible treatment
• Explain that HCV is a progressive disease that can lead to serious complications
• Emphasize that HCV can be curable, and treatment options are available

6/15/2017
21
CPT/HCPCS Codes
Hepatitis C antibody screening, for individual at high risk and other covered indication(s) G0472
Hepatitis C antibody 86803
Hepatitis C antibody, confirmatory test (with reflex) 86804
Collection of venous blood by venipuncture 36415
Hepatitis C, RNA, direct probe technique (qualitative) 87520
Hepatitis C, RNA, amplified probe technique (qualitative) 87521
Hepatitis C, RNA, quantification with reflex to genotype 87522
HCV genotype test 87902
FOR SCREENING
FOR DIAGNOSIS
FOR DIAGNOSIS ONCE CHRONIC INFECTION IS CONFIRMED
ICD-10 CodesCarrier (includes suspected carrier) of viral hepatitis C Z22.52
Carrier (includes suspected carrier) of unspecified viral hepatitis Z22.50
Carrier (includes suspected carrier) of other viral hepatitis Z22.59
Contact with and (suspected) exposure to viral hepatitis Z20.5
Contact with and (suspected) exposure to other viral communicable diseases Z20.828
Encounter for screening for other viral diseases Z11.59
Encounter for screening for infectious and parasitic diseases, unspecified Z11.9
Personal history of other infectious and parasitic diseases Z86.19
Other psychoactive substance dependence, uncomplicated F19.20
Other problems related to lifestyle Z72.89
Unspecified viral hepatitis C without hepatic coma B19.20
Unspecified viral hepatitis C with hepatic coma B19.21
Chronic persistent hepatitis, not elsewhere classified K73.0
Chronic viral hepatitis C B18.2
Sources:CPT Code/Relative Value Search: https://ocm.ama-assn.org/OCM/CPTRelativeValueSearch.doHCPCS HCV Codes: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM8871.pdfICD-10 Code Lookup: http://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx
Use these codes to order the appropriate screening or diagnostic test for your patient.
Use these codes to indicate why you are ordering the HCV test.
Select billing codes for HCV-related testsThis is a select list of CPT®, HCPCS, and ICD-10 codes that may be used for ordering tests related to screening and diagnosing potential patients with HCV.
OTHER HCV TESTS

6/15/2017
22
When do you typically refer a patient with HCV to a specialist?
1. At the point of diagnosis2. When the patient starts experiencing symptoms3. When liver enzymes become elevated4. When fibrosis is detected5. I do not currently refer
• Historically, treatment has been prioritized for patients with advanced liver disease or those at high risk for disease progression in part because of the benefit versus risk profile of therapies
• However, treatment has been shown to be most effective at early-stage disease1
– Patients with cirrhosis show a lower response to treatment1
– Progression of fibrosis is unpredictable2
• A prompt referral is important to ensure the patient is evaluated for treatment by a specialist. Treatment decisions may be made based on several factors including:
– The risks and benefits of treatment
– Patient's disease status compared with treatment tolerability
– Patient motivation
Prompt, Quality Referral Is Crucial
1. Bruno S et al. Hepatology. 2010;51(2):388-397.2. Poynard T et al. Lancet. 1997;349(9055):825-832.

6/15/2017
23
• Refer patients immediately, regardless of viral load or liver enzyme levels1
– Liver damage is possible in the presence of low viral loads and normal ALT or AST levels1,2
– Disease progression may not be reliably assessed by liver function tests2
Refer HCV Patients to an HCV Specialist for Treatment Evaluation
1. Heller T, Seeff LB. Hepatology. 2005;42(6):1261-1263. 2. Healey CJ et al. Gut. 1995;37(2):274-278.
• Between 25% and 50% of referred HCV patients miss their first specialist appointment1
• Many HCV patients do not follow up on their HCV referral for a variety of reasons, such as:
– Patients’ unwillingness to treat a largely asymptomatic disease
– Lack of insurance coverage
– Social rejection and stigmatization
Patient Follow-Up After Referral
1. McGowan CE, Fried MW. Liver Int. 2011;32(suppl 1):151-156.

6/15/2017
24
A Quality Referral Can Help Overcome Barriers
What Makes a Quality Referral?
• Confirmed diagnosis with an HCV RNA test
• Referring to a specialist with experience treating HCV
• Arranging the appointment for the patient
• Following up with the patient to ensure he/she attended the appointment
• Explain why referral is necessary
• Describe the liver complications that can arise from delaying treatment
• Tell your patient what to expect
• Make it clear that therapy may lead to cure
• Let your patient know that you are available for questions
Discuss Referral With Your Patient

6/15/2017
25
• HCV screening criteria have been expanded to include screening of all baby boomers, those born between 1945 and 19651-3
• Treatment options have evolved
• Before 2011, HCV treatment could last as long as a year, with cure rates of 40%-50% for the most common genotype in the US4
• Since that time, scientific advances have made HCV treatment shorter and more effective
• There are interferon-free treatment options that have shown cure rates of 90% or greater in clinical studies3
• Rethink HCV: Screen, Diagnose, and Refer
HCV Management Has Evolved, Making Cure More Possible for Patients
1. Smith BD et al. MMWR Recomm Rep. 2012;61(RR-4):1-32.2. USPSTF. http://www.uspreventiveservicestaskforce.org/uspstf12/hepc/hepcfinalrs.htm. Accessed December 7, 2015.3. AASLD, IDSA, IAS-USA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org.
Accessed December 7, 2015.4. Ghany MG et al. Hepatology. 2011;54(4):1433-1444.
For more HCV resources, register on HCVcanbecured.com to receive:• Your complete HCV Toolkit• Educational videos
• Patient discussion guides • Select CPT®, HCPCS, and ICD-
10 codes
Visit HCVcanbecured.com

6/15/2017
26
Prompt, Quality Referral Is Crucial
• Treatment is most effective before the onset of fibrosis26
– Progression of fibrosis is unpredictable, so all patients should be evaluated by a treating specialist5
• Patients with advanced liver damage show a lower response to treatment26
• Referral can lead to cure, reducing the risk of HCV-related morbidity and mortality27
5. Holmberg SD, Spradling PR, Moorman AC, Denniston MM. Hepatitis C in the United States. N Engl J Med. 2013;368(20):1859-1861.26. Davis G, Lau J. Factors predictive of a beneficial response to therapy of hepatitis C. Hepatology. 1997;26(3):122S-127S.27. McCombs J, Matsuda T, Tonnu-Mihara I, et al. The risk of long-term morbidity and mortality in patients with chronic hepatitis C. Results from an analysis of data from a Department of Veterans Affairs clinical registry. JAMA Intern Med. 2013.
GILEAD and the GILEAD logo are trademarks of Gilead Sciences, Inc., or its related companies. All other trademarks referenced herein are the property of their respective owners. ©2016 Gilead Sciences, Inc. All rights reserved. UNBP2128 02/16