he american journal of - lightning warriors ... disclosures the authors who contributed to this...
TRANSCRIPT

Expanding the Influenza Vaccination Season:A New Paradigm for Increasing Immunization Rates
GUEST EDITOR
William Schaffner, MDProfessor and Chair
Department of Preventive MedicineProfessor of Medicine, Division of Infectious Diseases
Vanderbilt University School of MedicineNashville, Tennessee
President-ElectNational Foundation for Infectious Diseases
Bethesda, Maryland
This supplement is supported by an unrestricted educational grant to the National Foundation for Infectious Diseases fromSanofi Pasteur Inc. Editorial support was provided by Alembic Health Communications, Inc., New York, New York.
Statement of Peer Review: All supplement manuscripts submitted to The American Journal of Medicine for publication arereviewed by the Guest Editor(s) of the supplement, by an outside peer reviewer who is independent of the supplement project,and by the Journal’s Supplement Editor (who ensures that questions raised in peer review have been addressed appropriately andthat the supplement has an educational focus that is of interest to our readership).
Author Disclosure Policy: All authors contributing to supplements in The American Journal of Medicine are required to fullydisclose any primary financial relationship with a company that has a direct fiscal or financial interest in the subject matter orproducts discussed in the submitted manuscripts, or with a company that produces a competing product. These relationships(e.g., ownership of stock or significant honoraria or consulting fees) and any direct support of research by a commercial companymust be indicated on the title page of each manuscript. This information will be published in the frontmatter of each supplement.
Editor-in-Chief: Joseph S. Alpert, MDEditor, Supplements: William H. Frishman, MD
Executive Supplements Editor: Brian JenkinsSenior Production Editor: Mickey Kramer
Publishing Director: Pamela Poppalardo
THE AMERICANJOURNAL ofMEDICINE ®
July 2008
Volume 121
Number 7B

Expanding the Influenza Vaccination Season: A New Paradigm for IncreasingImmunization Rates
Guest Editor
William Schaffner, MDVanderbilt University School of MedicineNashville, Tennessee
Faculty
David R. Johnson, MD, MPHSanofi Pasteur Inc.Swiftwater, Pennsylvania
Kim Lipczynski, PhDAdelphi Research by DesignPhiladelphia, Pennsylvania
Kristin L. Nichol, MD, MPHVA Medical CenterUniversity of MinnesotaMinneapolis, Minnesota
Walter A. Orenstein, MDEmory Vaccine CenterAtlanta, Georgia
Gregory A. Poland, MDMayo ClinicRochester, Minnesota
Patricia K. Stinchfield, RN, CS, CPNPChildren’s Hospitals and Clinics of MinnesotaSt. Paul, Minnesota

Faculty Disclosures
The authors who contributed to this publication have disclosed the following industry relationships:
David R. Johnson, MD, MPH, is a full-time employee of Sanofi Pasteur Inc.
Kim Lipczynski, PhD, is a full-time employee of Adelphi Research by Design; and has served as a consultant to SanofiPasteur Inc.
Kristin L. Nichol, MD, MPH, has served as a consultant to Sanofi Pasteur Inc., MedImmune, Novartis, GlaxoSmithKline,and CSL Biotherapies; and received research funding from GlaxoSmithKline and Sanofi Pasteur Inc.
Walter A. Orenstein, MD, has received grant support for clinical trials and research from Merck & Co., Sanofi Pasteur Inc.and Novartis; and serves on two data safety monitoring boards for clinical vaccine trials, Encorium (formerly Dynport) forbioterrorism threats and GlaxoSmithKline for pneumococcal vaccine.
Gregory A. Poland, MD, provided consulting advice and/or performed clinical research trials for Novavax, Merck & Co.,Protein Science, GlaxoSmithKline, Novartis Vaccines, CSL Limited, PowderMed, and Avianax.
William Schaffner, MD, serves as a consultant to GlaxoSmithKline, MedImmune, Merck & Co., Novartis, Sanofi PasteurInc. and Wyeth Pharmaceuticals; and is a member of a data safety evaluation committee for experimental vaccines for Merck& Co.
Patricia K. Stinchfield, RN, MS, CPNP, has no financial arrangement or affiliation with a corporate organization or amanufacturer of a product discussed in this supplement. She currently serves as a voting member on the Advisory Committeeon Immunization Practices for the Centers for Disease Control and Prevention.

S
I
ImNatotaivahiscp
aotdCtsflnnTottaraamsia
s
Div
0d
upplement issue
ntroduction: Expanding the Influenza Vaccination Season
mpesb
pbdnitt
Jisedtstnmrfbewovmoar
Spricoa�
nfluenza immunization remains the best defense against theorbidity and mortality associated with influenza infection.ational influenza immunization guidelines are in place and
re updated annually to identify the groups of individualshat should be vaccinated each year and to provide counseln how and when vaccine should be administered.1 Despitehis specific guidance to clinicians, community immunizers,nd public health workers, there is broad-based evidence ofnfluenza vaccine underutilization in all groups for whomaccination is warranted,2 resulting in potentially prevent-ble illness and complications of influenza (pneumonia,ospitalization, and death).3 One of the contributions tommunization rates that fall far below target levels is aizable number of missed opportunities throughout the vac-ination season (i.e., healthcare visits during which at-riskatients are not vaccinated).
The Centers for Disease Control and Prevention (CDC)nd other health experts have slightly differing definitionsf the influenza vaccination season. Although administra-ion of influenza vaccine in October and November is tra-itional, it has become clear that full implementation ofDC recommendations cannot be accomplished if vaccina-
ion occurs only in the fall, in advance of the influenzaeason. The CDC and others advocate broadening the in-uenza vaccination season, such that patients are immu-ized even after influenza activity has begun in a commu-ity. To maintain consistency throughout this supplement tohe American Journal of Medicine, we are using terminol-gy based on CDC influenza recommendations and defininghe influenza disease season as October through May andhe influenza vaccination season as October into Januarynd beyond.1 This shift in the vaccination timing paradigmequests all healthcare professionals to recognize the valuend medical need of vaccines given throughout the seasonnd to vaccinate at-risk patients at every opportunity. Ineeting public health vaccination goals, healthcare profes-
ionals are also called upon to increase their own influenzammunization rates. Healthcare professionals should viewnnual influenza vaccine as a professional responsibility for
Statement of author disclosure: Please see the Author Disclosuresection at the end of this article.
Requests for reprints should be addressed to William Schaffner, MD,epartment of Preventive Medicine, Vanderbilt University School of Med-
cine, Village at Vanderbilt, Suite 2600, 1500 21st Avenue South, Nash-
cille, Tennessee 37212.002-9343/$ -see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.amjmed.2008.05.001
any reasons: it make us positive role models for ouratients, it minimizes the likelihood that we will get influ-nza and be unable to work at a time when the healthcareystem needs us most, and it will help us avoid doing harmy infecting patients in our care.
Given the emphasis on influenza immunization in USublic health policy, a series of articles on the topic haveeen published together in this supplement. The subjectsiscussed in these articles are as follows: missed vacci-ation opportunities, practice-proven interventions thatncrease immunization rates, the delicate balance be-ween vaccine supply and demand, and adult immuniza-ion barriers.
In the first article, Drs. Gregory A. Poland and David R.ohnson set the stage by discussing the substantial burden ofnfluenza infection on affected individuals, the healthcareystem, and society at large. Given the availability of anffective and safe vaccine, the authors then review in someetail the rationale for the current CDC recommendationhat at-risk patients be vaccinated throughout the influenzaeason, beginning when vaccine first becomes available tohe time when supply is exhausted. They develop the ratio-ale that vaccination throughout the influenza season isedically relevant and feasible. The authors also present
esults from a newly released study in which patients at riskor influenza saw a healthcare provider on average 2.2 timesetween November and February, yet did not receive influ-nza vaccine. These findings underscore the frequency withhich missed vaccination opportunities contribute to sub-ptimal vaccination levels. With the supply of influenzaaccine now plentiful, efforts must be focused on reducingissed vaccination opportunities such that national target
bjectives are achieved. Healthcare providers are encour-ged to use all opportunities to vaccinate, which now rep-esents best practice.
In the second article, Nurse Practitioner Patricia K.tinchfield presents a literature-based review of practice-roven interventions that increase influenza immunizationates and extend the vaccination season. In this regard,nterventions that increase patient demand and vaccine ac-ess and overcome practice-related barriers (e.g., standingrders, reminder and recall efforts, vaccination-only clinics)re discussed. It is suggested that sites select and implement1 intervention that addresses site-specific needs, with
hoices based on necessary resources and other factors to

oaeo
AcipwWyci
tcc(vvlnnptp
t
vt
ATt
GSmm
R1
2
3
S2 The American Journal of Medicine, Vol 121, No 7B, July 2008
ptimize the reach of vaccination. By way of example, theuthor provides case studies of practices that deliver influ-nza vaccine efficiently and effectively to a large proportionf their target patients.
The focus of the third article, coauthored by Dr. Walter. Orenstein and me, is the delicate balance between vac-
ine supply and demand and its impact on the realization ofnfluenza immunization goals. The complexities of vaccineroduction and distribution, and financing are reviewed,ith a particular focus on the implications for the provider.ith substantial growth in supply expected over the coming
ears, demand for the influenza vaccine should be in-reased. A number of strategies are discussed to promotemproved vaccine uptake.
In the final article, Dr. Johnson and colleagues presenthe results of a structured telephone survey, which wasonducted to determine the attitudes and knowledge ofonsumers and healthcare providers about adult vaccinesinfluenza, pneumococcal, and tetanus). Factors affectingaccination decisions were assessed. According to the sur-ey responses, immunization rates for adults are muchower than target rates established by national guidelines. Ofote, the reasons consumers gave for not receiving vacci-ations were not consistent with those given by healthcareroviders. The researchers provide us with a sampling ofhese reasons, which can be used to inform and refineolicies to increase immunization rates in adults.
It is the hope of the authors that these articles will help
o shape new viewpoints and practices, culminating in theaccination of all persons at risk for influenza illness andransmission of influenza to others.
William Schaffner, MDDepartments of Preventive Medicine and Medicine
Vanderbilt University School of MedicineNashville, Tennessee, USA
E-mail address: [email protected].
UTHOR DISCLOSUREShe author of this article has disclosed the following indus-
ry relationships:William Schaffner, MD, serves as a consultant to
laxoSmithKline, MedImmune, Merck & Co., Novartis,anofi Pasteur, Inc., and Wyeth Pharmaceuticals; and is aember of a data safety evaluation committee for experi-ental vaccines for Merck & Co.
eferences. Centers for Disease Control and Prevention (CDC). Prevention and
control of influenza: recommendations of the Advisory Committee onImmunization Practices (ACIP), 2007. MMWR Recomm Rep. 2007;56(RR6):1-54.
. Centers for Disease Control and Prevention (CDC). Estimates of influenzavaccination target population sizes in 2006 and recent vaccine uptake levels[CDC Website]. Available at: www.cdc.gov/flu/professionals/vaccination/pdf/targetpopchart.pdf. Accessed December 5, 2007.
. Atkinson W, Hamborsky J, McIntyre L, Wolfe S, eds, for the Centersfor Disease Control and Prevention (CDC). Epidemiology and Preven-tion of Vaccine-Preventable Diseases. 10th ed. Washington, DC: Public
Health Foundation, 2007.
S
ItGa
S
Acflpmpraewtpvec
s
M2
0d
upplement issue
ncreasing Influenza Vaccination Rates: The Needo Vaccinate Throughout the Entire Influenza Seasonregory A. Poland, MD,a David R. Johnson, MD, MPHb
Mayo Vaccine Research Group, Mayo Clinic, Rochester, Minnesota, USA; and bScientific and Medical Affairs,
anofi Pasteur Inc., Swiftwater, Pennsylvania, USA.Tsagcotidibaa©
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ABSTRACT
he burden of influenza on affected individuals and the healthcare system, as well as on society, isubstantial. Although the supply of an effective and safe influenza vaccine was limited in previous years,dvances in manufacture and distribution have alleviated such shortages. In most seasons, millions of doseso unused, and large numbers of unvaccinated, at-risk persons are left vulnerable to infection and itsomplications. According to insurance claims data, high-risk patients are seen by their healthcare providersn average 2.2 times between the peaks in vaccination (November) and in disease activity (February), yethey remain unvaccinated. The current 2- to 3-month time frame over which patients are traditionallymmunized is too short to fully implement immunization recommendations and inconsistent with theuration of influenza activity. Both healthcare providers and patients should reevaluate their approach tonfluenza vaccination and recognize the need to extend the immunization time period into January andeyond. To increase influenza immunization rates, the Centers for Disease Control and Prevention (CDC)nd other professional societies recommend an expanded immunization season, with vaccination offeredt every opportunity between October and May. 2008 Elsevier Inc. All rights reserved. • The American Journal of Medicine (2008) 121, S3–S10
KEYWORDS: Immunization; Influenza; Influenza season; Vaccination
npha
vtttafieetM
IIti
nnual influenza vaccination of persons at risk for eitheromplications of influenza infection or for transmitting in-uenza virus is the most important component of the USublic health strategy for preventing influenza-associatedorbidity and mortality.1 Historically, most healthcare
ractitioners have offered influenza vaccination to their at-isk patients each year from September to about November,nd vaccination rates decrease precipitously before year’snd. This approach to vaccination was conceived at a timehen fewer individuals were in target groups for vaccina-
ion and when the vaccine supply was limited, necessitatingrioritization of doses to the most vulnerable persons. Theaccine supply is now plentiful,2 and target groups havexpanded to include approximately 3 of every 4 Ameri-ans.3 The most recent expansion calls for universal vacci-
Statement of author disclosure: Please see the Author Disclosuresection at the end of this article.
Requests for reprints should be addressed to Gregory A. Poland, MD,ayo Vaccine Research Group, Mayo Clinic, Guggenheim Building 611,
00 First Street SW, Rochester, Minnesota, 55905.
n: [email protected].ront matter © 2008 Elsevier Inc. All rights reserved.ed.2008.05.002
ation of all children through 18 years of age.4 Some haveostulated that widespread pediatric vaccination may yield aerd immunity affect. Current evidence is modest, though,nd herd immunity, though possible,5–7 needs further study.
Adoption of a new paradigm that includes a much longeraccination period—starting in the autumn and continuinghrough the entire influenza season—is critical to protectinghe large number of at-risk persons. According to the Cen-ers for Disease Control and Prevention (CDC), vaccinedministered after the influenza season has begun is bene-cial. As a consequence, current CDC recommendationsmphasize that immunization providers should offer influ-nza vaccine and even schedule immunization clinicshroughout the entire influenza season, from October to
ay.
NFLUENZA: THE ILLNESS AND ITS IMPACTnfluenza is an acute and potentially serious viral infectionhat affects 1 or 2 of every 10 Americans annually.8 Classicnfluenza, generally an uncomplicated and self-limited ill-
ess, is characterized by respiratory as well as constitutional
sctdrsbecircatc
vtrwhiwmc
dSmovpdtb
shdcd$brh(dS
VMdt(ov
tatmv
i9wsdpt
ibrIpi8h
(Lwcatmcewc
iowmdvsvaifr
VBmiyvg
S4 The American Journal of Medicine, Vol 121, No 7B, July 2008
igns and symptoms (e.g., nonproductive cough, high fever,hills, headache, sore throat, myalgia, and malaise).9 Addi-ional symptoms unique to children include abdominal pain,iarrhea, and vomiting. Influenza infection can lead to se-ious sequelae, including secondary bacterial pneumonia,inusitis, bronchitis, and myocarditis, as well as croup,ronchiolitis, and acute otitis media in children.1,8,10 Influ-nza can also exacerbate underlying medical conditions; itan trigger acute myocardial infarction or stroke11,12 andncrease the rate of death from coronary heart disease (oddsatio, 1.3).13 Complications of the acute infection are mostommon in young children, the elderly, and persons ofny age with underlying medical conditions that placehem “at risk” (e.g., diabetes mellitus, asthma, cardiovas-ular disease).14
Influenza has a substantial impact on both affected indi-iduals and society. A typical case of influenza results in 3o 4 days of bed rest and an additional 5 to 6 days ofestricted activity.15 Absenteeism from work and schoolas attributed to influenza in a study of �12,000 US house-olds with �1 school-aged child reporting influenza-likellness.16 Influenza-associated “presenteeism” (ill but still atork or school) has been shown to decrease job perfor-ance,17,18 and infection is associated with functional de-
line in older adults.19
An average of �200,000 hospitalizations and 36,000eaths due to influenza occurred annually in the Unitedtates during the 1990s.20,21 The current hospitalization andortality rates attributable to influenza are even higher
wing to increased numbers of at-risk persons (e.g., indi-iduals who are elderly, have diabetes, or are immunocom-romised). To provide perspective, the number of influenzaeaths in the United States is on the same order of magni-ude as the number of deaths from colorectal cancer andreast cancer.22
The economic impact of annual influenza epidemics isubstantial. Based on 2003 data, which included �334,000ospitalizations (3.1 million hospitalization days), 41,000eaths, and 31.4 million outpatient visits, Molinari andolleagues23 estimated direct medical costs (in 2003 USollars) of $10.4 billion (95% confidence interval [CI],4.1-$22.2 billion) and projected lost earnings of $16.3illion (95% CI, $8.7-$31.0 billion). Adding indirect costselated to death (lost productivity and intrinsic value ofuman life), the total economic burden was $87.1 billion95% CI, $47.2-$149.5 billion). This exceeds the combinedirect and indirect annual costs of arthritis in the Unitedtates ($82 billion).24
ACCINE SAFETY AND EFFICACYultiple studies, in multiple settings, have consistently
emonstrated the safety and efficacy of both trivalent inac-ivated influenza vaccine (TIV) and live attenuated vaccineLAIV) in mitigating clinical illness and decreasing the riskf associated complications. Influenza vaccines, like all
accines, are not 100% effective. Efficacy varies based on hhe antigenic match between circulating and vaccine strainsnd the age and immune status of vaccine recipients. Fur-her, clinical study findings vary based on the outcomeeasured (e.g., culture-confirmed influenza infection, pre-
ention of medically attended acute respiratory illness).Estimates of TIV efficacy against laboratory-confirmed
nfluenza in healthy adults �65 years range from 70% to0% when the antigenic match is good25–28 to 50%-77%hen the antigenic match is suboptimal.25,27,28–31 In this
ame population, LAIV provides significant reductions inays of illness, days of work lost, days with healthcarerovider visits, and use of prescription antibiotics and over-he-counter medications.
Efficacy against laboratory-confirmed infection is lowern older persons (for whom only TIV is currently approved),ut the true benefit of vaccination for this group is theeduction in risk of serious complications and death.nfluenza vaccination (TIV) is 30% to 70% effective inreventing hospitalization for pneumonia and influenzan community-dwelling elderly persons32,33 and up to0% effective in preventing death among elderly nursingome residents.34 –37
Studies have also confirmed vaccine efficacy in childrenTIV is approved for use in all children aged �6 months;AIV is approved for use in children aged �24 monthsithout asthma). In a 5-year study, TIV reduced laboratory-
onfirmed influenza A infection by 77% to 91% in childrenged 1 to 15 years.38 During a season marked by a subop-imal antigenic match, TIV was 51% effective in children 6onths to 8 years of age against medically-attended, clini-
ally-diagnosed pneumonia or influenza.39 Across 2 influ-nza seasons, 1 marked by a drifted influenza strain, LAIVas 92% effective against laboratory-confirmed influenza in
hildren 60 to 71 months of age.40,41
Both types of influenza vaccine are contraindicated inndividuals with a history of hypersensitive reaction to eggsr egg proteins. The most frequent side effect associatedith TIV is soreness at the vaccination site.42 For LAIV, theost frequent side effect is runny nose. Guillain-Barré syn-
rome (GBS) was associated with the 1976 swine influenzaaccine, but evidence of a connection between GBS andubsequent vaccines has been inconsistent.1 The CDC ad-ises that it is “prudent” to avoid vaccinating persons withhistory of GBS who are not at high risk for severe
nfluenza complications. However, the potential risk of in-ection may outweigh concerns about GBS for those at highisk.
ACCINATION RECOMMENDATIONSased on the available evidence, the CDC has recom-ended that certain groups of persons should receive annual
nfluenza vaccination (Table 1).1,4 In sharp contrast to priorears in which only high-risk persons were targeted foraccination, the most current CDC recommendations sug-est influenza vaccination of any person wanting to reduce
is or her risk of influenza or the potential of transmitting
ttommmim
pFrciryvft
phc
scidivv
gnaVul
SVAirHbpdsashiiwu
CSacctmocibntttv(
A
S5Poland and Johnson Increasing Influenza Vaccination Rates
he illness. The current target groups for influenza vaccina-ion include approximately 218 million Americans, or 73%f the US population.3 In 2006, the CDC’s Advisory Com-ittee on Immunization Practices signaled its intent toove toward a universal influenza immunization recom-endation43 and in early 2008 voted to recommend extend-
ng pediatric recommendations to all children from 6onths through 18 years.4
Despite these recommendations from the CDC and otherrofessional organizations (eg, the American Academy ofamily Physicians [AAFP], American Academy of Pediat-ics [AAP], American College of Obstetricians and Gyne-ologists, American College of Physicians, American Med-cal Association [AMA]), influenza vaccination ratesemain low (Figure 1).1 Approximately 60% of adults �65ears and only 10% to 40% of other target groups wereaccinated in 2005.1 The current level of vaccination fallsar short of the Healthy People 2010 national health objec-
Table 1 Recommendations for Influenza Vaccination
nnual influenza vaccination is recommended for:● Any person, including a school-aged child, who wishes to
reduce the likelihood of becoming ill or of transmittingthe infection to others
● Any person at risk for influenza complications:— Children aged 6–59 mo*†— All persons aged �50 yr— Children and adolescents on long-term aspirin therapy— Pregnant women— All persons (adults and children) with a chronic disease
(e.g., asthma, diabetes mellitus, cardiovascular disease)excluding hypertension
— All persons (adults and children) who areimmunosuppressed
— All persons (adults and children) with a condition thatcan compromise respiratory function, handling ofsecretions, or increase the risk for aspiration (e.g.,cognitive dysfunction, spinal cord injury, seizuredisorder, other neuromuscular disorder)
— Residents of nursing homes and other chronic-carefacilities
● Any person at risk of transmitting influenza:— Healthcare personnel— Healthy household contacts (including children) and
caregivers of:X Children aged �59 mo†X Adults aged �50 yrX Persons (adults and children) with a medical
condition that increases their risk for severecomplications of influenza
Adapted from Centers for Disease Control and Prevention.1,4
*On February 27, 2008, the Centers for Disease Control and Preven-tion (CDC) Advisory Committee on Immunization Practices voted toexpand its recommendations for annual influenza vaccination to includeall children 6 months through 18 years.
†Children aged �6 months cannot be vaccinated and should beprotected through vaccination of close contacts.
ives of 90% for persons �65 years and 60% for younger s
ersons who have risk factors.44 Worse, the majority of USealthcare workers themselves fail to get the influenza vac-ine each year.45
Most persons recommended for influenza vaccinationhould receive a single dose each year. The exception ishildren 6 months to 9 years of age who are receivingnfluenza vaccine for the first time. They should receive 2oses administered �1 month apart.14 No influenza vaccines currently licensed for children aged �6 months; theseulnerable infants should be protected indirectly throughaccination of close contacts.
In 2006, approximately 150 million Americans in targetroups lacked the protection conferred by influenza vacci-ation. This was at a time when the supply was abundant,nd millions of vaccine doses were ultimately discarded.2
accine doses left over after one influenza season cannot besed during the following season due to changes in circu-ating strains (i.e., antigenic drift) and vaccine expiration.14
TRATEGIES TO INCREASE INFLUENZAACCINATIONs the number of people for whom influenza immunization
s recommended has increased, so has the challenge ofeaching them all. The US Public Health Service (USPHS)ealthy People 2010 influenza immunization goals will note achieved without a change in the influenza immunizationaradigm. This requires efforts on 3 fronts: (1) consumeremand for influenza immunization needs to be high andustainable from season to season; (2) there must be andequate vaccine supply; and (3) the healthcare systemhould use all opportunities to vaccinate (e.g., at routineealthcare visits, during hospitalizations) throughout thenfluenza season. Although the influenza season often peaksn February (Figure 2),1 it can last for many months after-ard in the United States. Therefore, vaccination into Jan-ary and beyond is beneficial.
onsumer Demandurveys show that many Americans have misperceptionsbout their risk of influenza, whether they should get vac-inated, vaccine efficacy, and the safety of influenza vac-ines. For instance, in a randomized, nationally representa-ive sample of unvaccinated Medicare beneficiaries, theost common explanations were that they were “unaware
f vaccination’s need” and “concerned that the vaccineauses influenza” and “could cause side effects.”46 Approx-mately half of adult respondents to a survey conductedefore the 2006 to 2007 influenza season indicated they didot plan to be immunized. Their reasons included thinkinghat influenza is not serious enough to warrant immuniza-ion (43%), that they are not at risk for influenza/complica-ions (37%), that the vaccine is not effective (19%), and thataccination in a prior year makes revaccination unnecessary15%).47
Healthcare providers can influence their patients’ deci-
ions regarding vaccination. A first step is to set a good
etstesdtvs
tMvv(tSta
y targe
S6 The American Journal of Medicine, Vol 121, No 7B, July 2008
xample for their patients by vaccinating themselves andheir staff.48,49 Getting an annual influenza vaccinationhould be viewed as a professional responsibility. Vaccina-ion reduces the risk that healthcare workers will get influ-nza and be unable to work at a time when the healthcareystem’s needs are greatest. Even more importantly, it re-uces the risk that healthcare workers will transmit a po-entially deadly virus to the patients in their care. Onceaccinated, healthcare workers are in a better position to
Figure 1 Self-reported influenza vaccination levels b
Figure 2 Peak influenza activity in the United SRecomm Rep.1)
trongly recommend influenza vaccination to all at-risk pa- b
ients.50,51 In this supplement to The American Journal ofedicine, Johnson and colleagues52 report that many un-
accinated persons (54%) have never discussed influenzaaccination with their healthcare provider. Yet most adults79%) are likely to follow their physician’s recommenda-ion that they be vaccinated. As reviewed in detail bytinchfield,53 influenza vaccination rates also may be posi-
ively affected by other interventions that increase vaccineccess, increase demand, and overcome practice-related
t population. (Reprinted from MMWR Recomm Rep.1)
y month, 1976 to 2006. (Reprinted from MMWR
tates barriers.

ptsptpPtMnmAtepe
VAttraAgspcaw2
urbHvd
p(pictmwrog
EOc
vcaoyo
o2tctcetihtpiiCcdneytz
nisdaebf
rcptboec
syicfc
S7Poland and Johnson Increasing Influenza Vaccination Rates
Communication between healthcare providers and at-riskatients may be especially important for influenza vaccina-ion later in the season. Fishbein and associates54 found thatpecific inquiries or discussion of vaccination status withatients led to vaccination rates in December and afterwardhat were comparable to rates earlier in the season, whenatients tended to be self-motivated to seek vaccination.hysician-to-patient education about the importance of get-
ing vaccinated throughout the season (October throughay) is increasingly being supported by consumer aware-
ess campaigns sponsored by the CDC and a variety ofedical groups (e.g., American Lung Association [ALA],MA, Childhood Influenza Immunization Coalition, Na-
ional Foundation for Infectious Diseases, National Influ-nza Vaccine Summit). All of these groups’ Web sitesrovide information about influenza vaccination to consum-rs and healthcare providers.55–57
accine Supplymple influenza vaccine should be available now and for
he foreseeable future in the United States. Althoughhere have been fluctuations in supply (and 1 large dis-uption during the 2004 to 2005 season), shortages camet a time when there were fewer vaccine manufacturers.s a consequence, production problems involving a sin-le manufacturer had a larger relative impact on overallupply than they would now that several additional com-anies are manufacturing and distributing influenza vac-ine. A record 121 million influenza vaccine doses werevailable for the US market in 2006; 130 million dosesere expected to be produced in 2007 and 150 million in008.2
While total vaccine supply continues to grow and man-facturers strive to deliver vaccine as early as possible, theealities of the production process prevent all doses fromeing delivered at once or before the start of the season.ealthcare providers should begin vaccinating as soon asaccine is available and continue until no more vaccine isistributed for the season.
Inherent complexities in the manufacture of a biologicalroduct like influenza vaccine mean that many doses�30%) are delivered in November and later.58 Becauserotection is achieved very quickly (within 2 weeks) aftermmunization,59,60 it is medically relevant to continue vac-ination into January and beyond. In fact, vaccinationhroughout the entire influenza season, not just in the earlyonths as has been the practice in recent years, is the onlyay to fully utilize all available vaccine and to meet the
ecommendations of the CDC, AAFP, AAP, AMA, andther groups, as well as to meet the Healthy People 2010oals.
xtending the Vaccination Seasonne way to meet the challenge of protecting more Ameri-
ans from influenza is to recognize the need for and the D
alue of vaccination throughout the influenza season.61 Ac-ording to data gathered by the CDC, the peak in influenzactivity between 1976 and 2006 occurred well after the startf the year (Figure 2).1 Half of all cases (up to 30 million aear) occur after the peak, which usually occurs in Februaryr later.
These findings are corroborated in the following studyf influenza vaccination and diagnosis visits from 2004 to007. Data for the study were obtained from the elec-ronic healthcare claims submitted by �240,000 physi-ians in practice across the United States to all types ofhird-party payers (i.e., Medicare, Medicaid, commer-ial). A longitudinally stable identifier was assigned toach patient to protect his or her anonymity and was usedo track patients over time. The source data are geograph-cally representative and well characterized, providing aigh degree of precision and accuracy in projections tohe entire US population. Data were monitored at theractitioner level to ensure completeness and consistencyn reporting. Multiple outside sources were used to val-date estimates from the model. The number of timesDC-defined high-risk patients1 were seen in a physi-ian’s office between September 1 and March 31 wasetermined for 2004 to 2005 and 2005 to 2006, as was theumber of patients immunized and the number of influ-nza diagnosis visits over the same months during the 3ears from 2004 to 2005 through 2006 to 2007. Takenogether, these data provide insight into missed immuni-ation opportunities for high-risk patients.
Data show an early surge in uptake of influenza vacci-ation with rates peaking around Thanksgiving, and thenmmunization rates decrease dramatically for the rest of theeason (Figure 3). The early peak in immunization is likelyriven by patients who seek out immunization and by mediattention during the fall. Healthcare visits resulting in influ-nza diagnoses peak much later in the season. The gapetween the 2 peaks—for vaccination and diagnosis—is aull 16 weeks.
Although many believe the drop off in immunizationesults from poor access to at-risk patients, such is not thease. Approximately 25 million unimmunized, high-riskatients visit their healthcare providers a total of 55 millionimes, or on average 2.2 times each, during the periodetween peaks in immunization and disease activity. If thesepportunities to vaccinate were used throughout the influ-nza season, significant improvements in vaccination ratesertainly could be made.
More recent data for the 2007 to 2008 influenza seasonhow no deviation from the pattern of the previous severalears. With record amounts of influenza vaccine distributedn the United States, an even greater surge in vaccinationlaims took place during October and most of November,ollowed by a very similar and precipitous decrease in thoselaims beginning in late November and running through
ecember.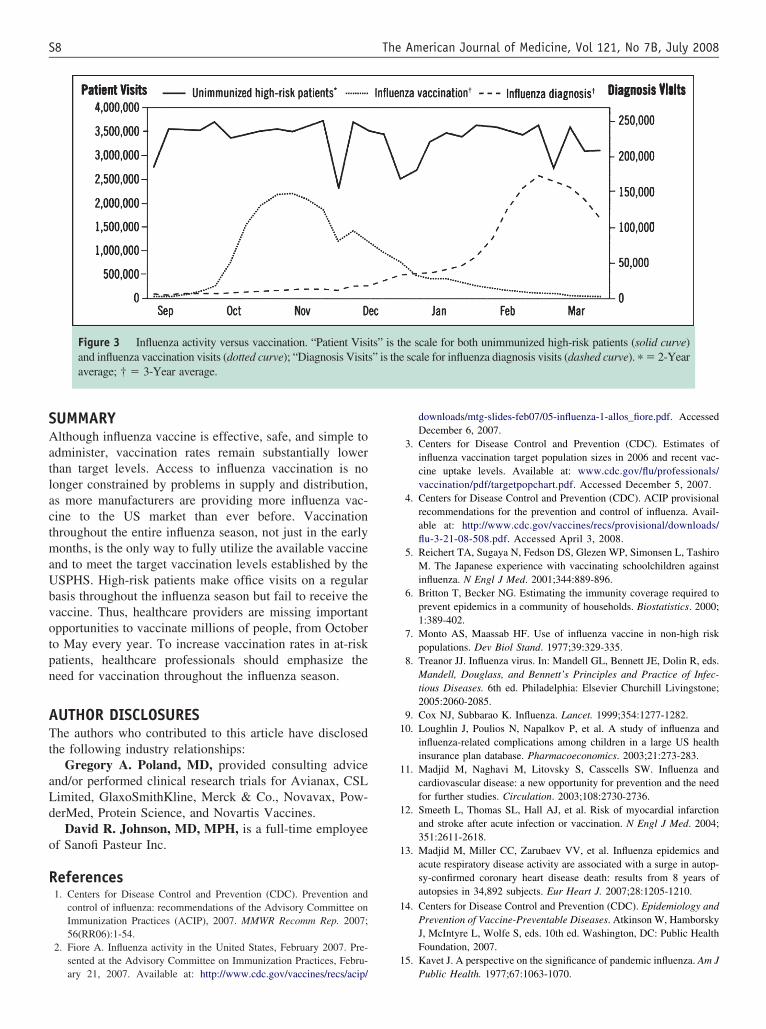
SAatlactmaUbvotpn
ATt
aLd
o
R
1
1
1
1
1
1
S8 The American Journal of Medicine, Vol 121, No 7B, July 2008
UMMARYlthough influenza vaccine is effective, safe, and simple to
dminister, vaccination rates remain substantially lowerhan target levels. Access to influenza vaccination is noonger constrained by problems in supply and distribution,s more manufacturers are providing more influenza vac-ine to the US market than ever before. Vaccinationhroughout the entire influenza season, not just in the earlyonths, is the only way to fully utilize the available vaccine
nd to meet the target vaccination levels established by theSPHS. High-risk patients make office visits on a regularasis throughout the influenza season but fail to receive theaccine. Thus, healthcare providers are missing importantpportunities to vaccinate millions of people, from Octobero May every year. To increase vaccination rates in at-riskatients, healthcare professionals should emphasize theeed for vaccination throughout the influenza season.
UTHOR DISCLOSUREShe authors who contributed to this article have disclosed
he following industry relationships:Gregory A. Poland, MD, provided consulting advice
nd/or performed clinical research trials for Avianax, CSLimited, GlaxoSmithKline, Merck & Co., Novavax, Pow-erMed, Protein Science, and Novartis Vaccines.
David R. Johnson, MD, MPH, is a full-time employeef Sanofi Pasteur Inc.
eferences1. Centers for Disease Control and Prevention (CDC). Prevention and
control of influenza: recommendations of the Advisory Committee onImmunization Practices (ACIP), 2007. MMWR Recomm Rep. 2007;56(RR06):1-54.
2. Fiore A. Influenza activity in the United States, February 2007. Pre-sented at the Advisory Committee on Immunization Practices, Febru-
Figure 3 Influenza activity versus vaccination. “Patient Visiand influenza vaccination visits (dotted curve); “Diagnosis Visitsaverage; † � 3-Year average.
ary 21, 2007. Available at: http://www.cdc.gov/vaccines/recs/acip/
downloads/mtg-slides-feb07/05-influenza-1-allos_fiore.pdf. AccessedDecember 6, 2007.
3. Centers for Disease Control and Prevention (CDC). Estimates ofinfluenza vaccination target population sizes in 2006 and recent vac-cine uptake levels. Available at: www.cdc.gov/flu/professionals/vaccination/pdf/targetpopchart.pdf. Accessed December 5, 2007.
4. Centers for Disease Control and Prevention (CDC). ACIP provisionalrecommendations for the prevention and control of influenza. Avail-able at: http://www.cdc.gov/vaccines/recs/provisional/downloads/flu-3-21-08-508.pdf. Accessed April 3, 2008.
5. Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, TashiroM. The Japanese experience with vaccinating schoolchildren againstinfluenza. N Engl J Med. 2001;344:889-896.
6. Britton T, Becker NG. Estimating the immunity coverage required toprevent epidemics in a community of households. Biostatistics. 2000;1:389-402.
7. Monto AS, Maassab HF. Use of influenza vaccine in non-high riskpopulations. Dev Biol Stand. 1977;39:329-335.
8. Treanor JJ. Influenza virus. In: Mandell GL, Bennett JE, Dolin R, eds.Mandell, Douglass, and Bennett’s Principles and Practice of Infec-tious Diseases. 6th ed. Philadelphia: Elsevier Churchill Livingstone;2005:2060-2085.
9. Cox NJ, Subbarao K. Influenza. Lancet. 1999;354:1277-1282.0. Loughlin J, Poulios N, Napalkov P, et al. A study of influenza and
influenza-related complications among children in a large US healthinsurance plan database. Pharmacoeconomics. 2003;21:273-283.
1. Madjid M, Naghavi M, Litovsky S, Casscells SW. Influenza andcardiovascular disease: a new opportunity for prevention and the needfor further studies. Circulation. 2003;108:2730-2736.
2. Smeeth L, Thomas SL, Hall AJ, et al. Risk of myocardial infarctionand stroke after acute infection or vaccination. N Engl J Med. 2004;351:2611-2618.
3. Madjid M, Miller CC, Zarubaev VV, et al. Influenza epidemics andacute respiratory disease activity are associated with a surge in autop-sy-confirmed coronary heart disease death: results from 8 years ofautopsies in 34,892 subjects. Eur Heart J. 2007;28:1205-1210.
4. Centers for Disease Control and Prevention (CDC). Epidemiology andPrevention of Vaccine-Preventable Diseases. Atkinson W, HamborskyJ, McIntyre L, Wolfe S, eds. 10th ed. Washington, DC: Public HealthFoundation, 2007.
5. Kavet J. A perspective on the significance of pandemic influenza. Am J
e scale for both unimmunized high-risk patients (solid curve)scale for influenza diagnosis visits (dashed curve). � � 2-Year
ts” is th” is the
Public Health. 1977;67:1063-1070.

1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
S9Poland and Johnson Increasing Influenza Vaccination Rates
6. Li S, Leader S. Economic burden and absenteeism from influenza-likeillness in healthy households with children (5–17 years) in the US.Respir Med. 2007;101:1244-1250.
7. Keech M, Scott AJ, Ryan PJ. The impact of influenza and influenza-like illness on productivity and healthcare resource utilization in aworking population. Occup Med (Lond). 1998;48:85-90.
8. Smith AP, Thomas M, Brockman P, et al. Effect of influenza B virusinfection on human performance. BMJ. 1993;306:760-761.
9. Barker WH, Borisute H, Cox C. A study of the impact of influenza onthe functional status of frail older people. Arch Intern Med. 1998;158:645-650.
0. Thompson WW, Shay DK, Weintraub E, et al. Mortality associatedwith influenza and respiratory syncytial virus in the United States.JAMA. 2003;289:179-186.
1. Thompson WW, Shay DK, Weintraub E, et al. Influenza-associatedhospitalizations in the United States. JAMA. 2004;292:1333-1340.
2. Miniño AM, Heron MP, Murphy SL, Kochanek KD. Deaths: final datafor 2004. National Vital Statistics Reports, vol. 55, no. 19. Hyattsville,MD: National Center for Health Statistics, 2007. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr55/nvsr55_19.pdf. Accessed Janu-ary 31, 2008.
3. Molinari NA, Ortega-Sanchez IR, Messonnier ML, et al. The annualimpact of seasonal influenza in the US: measuring disease burden andcosts. Vaccine. 2007;25:5086-5096.
4. Centers for Disease Control and Prevention (CDC). National Centerfor Chronic Disease Prevention and Health Promotion. Costs ofchronic disease. November 2005. Available at: http://www.cdc.gov/nccdphp/overview.htm#2. Accessed February 9, 2008.
5. Bridges CB, Thompson WW, Meltzer MI, et al. Effectiveness andcost-benefit of influenza vaccination of healthy working adults: arandomized controlled trial. JAMA. 2000;284:1655-1663.
6. Demicheli V, Rivetti D, Deeks JJ, Jefferson TO. Vaccines for prevent-ing influenza in healthy adults. Cochrane Database Syst Rev. 2004;(3):CD001269.
7. Nichol KL, Lind A, Margolis KL, et al. The effectiveness of vaccina-tion against influenza in healthy, working adults. N Engl J Med.1995;333:889-893.
8. Campbell DS, Rumley MH. Cost-effectiveness of the influenza vac-cine in a healthy, working-age population. J Occup Environ Med.1997;39:408-414.
9. Ohmit SE, Victor JC, Rotthoff JR, et al. Prevention of antigenicallydrifted influenza by inactivated and live attenuated vaccines. N EnglJ Med. 2006;355:2513-2522.
0. Keitel WA, Cate RT, Couch RB, et al. Efficacy of repeated annualimmunization with inactivated influenza virus vaccines over a five yearperiod. Vaccine. 1997;15:1114-1122.
1. Herrera GA, Iwane MK, Cortese M, et al. Influenza vaccine effective-ness among 50-64-year-old persons during a season of poor antigenicmatch between vaccine and circulating influenza virus strains: Colo-rado, United States, 2003-2004. Vaccine. 2007;25:154-160.
2. Nichol KL, Wuorenma J, von Sternberg T. Benefits of influenzavaccination for low-, intermediate-, and high-risk senior citizens. ArchIntern Med. 1998;158:1769-1776.
3. Mullooly JP, Bennett MD, Hornbrook MC, et al. Influenza vaccinationprograms for elderly persons: cost-effectiveness in a health mainte-nance organization. Ann Intern Med. 1994;121:947-952.
4. Jefferson T, Rivetti D, Rudin M, et al. Efficacy and effectiveness ofinfluenza vaccines in elderly people: a systematic review. Lancet.2005;366:1165-1174.
5. Patriarca PA, Weber JA, Parker RA, et al. Efficacy of influenzavaccination in nursing homes: reduction in illness and complicationsduring an influenza A (H3N2) epidemic. JAMA. 1985;253:1136-1139.
6. Arden NH, Patriarca PA, Kendal AP. Experiences in the use andefficacy of inactivated influenza vaccine in nursing homes. In: KendalAP, Patriarca PA, eds. Options for the Control of Influenza. New York:
Alan R. Liss, Inc., 1986.7. Monto AS, Hornbuckle K, Ohmit SE. Influenza vaccine effectivenessamong elderly nursing home residents: a cohort study. Am J Epide-miol. 2001;154:155-160.
8. Neuzil KM, Dupont WD, Wright PF, Edwards KM. Efficacy of inacti-vated and cold-adapted vaccines against influenza A infection, 1985 to1990: the pediatric experience. Pediatr Infect Dis J. 2001;20:733-740.
9. Ritzwoller DP, Bridges CB, Shetterly S, et al. Effectiveness of the2003–2004 influenza vaccine among children 6 months to 8 years ofage with 1 vs. 2 doses. Pediatrics. 2005;116:153-159.
0. Belshe RB, Mendelman PM, Treanor J, et al. The efficacy of liveattenuated, cold-adapted, trivalent, intranasal influenzavirus vaccine inchildren. N Engl J Med. 1998;338:1405-1412.
1. Belshe RB, Gruber WC, Mendelman PM, et al. Efficacy of vaccinationwith live-attenuated, cold-adapted, trivalent, intranasal influenza virusvaccine against a variant (A/Syndney) not contained in the vaccine.J Pediatr. 2000;136:168-175.
2. Margolis KL, Nichol KL, Poland GA, Pluhar RE. Frequency of ad-verse reactions to influenza vaccine in the elderly: a randomized,placebo-controlled trial. JAMA. 1990;264:1139-1141.
3. Centers for Disease Control and Prevention (CDC). National Immu-nization Program: record of the meeting of the Advisory Committee onImmunization Practices, February 21–22, 2006. Available at: http://www.cdc.gov/vaccines/recs/acip/downloads/min-feb06.pdf. AccessedFebruary 29, 2008.
4. US Department of Health and Human Services. Healthy people [HealthyPeople 2010 Web site]. Available at: http://www.healthypeople.gov. Ac-cessed March 3, 2008.
5. Poland GA, Ofstead CL, Tucker SJ, Beebe TJ. Receptivity to manda-tory influenza vaccination policies for healthcare workers among reg-istered nurses working on inpatient units. Infect Control Hosp Epide-miol. 2008;29:170-173.
6. Adler GS. Influenza vaccination and self-reported reasons for notreceiving influenza vaccination among Medicare beneficiaries aged�65 years: United States, 1991-2002. MMWR Morb Mortal Wkly Rep.2004;53:1012-1015.
7. National Foundation for Infectious Diseases. Public perception ofinfluenza, vaccination and treatment options: national consumer surveysponsored by the National Foundation for Infectious Diseases (NFID).Available at: http://www.connectlive.com/events/infectiousdiseases/presskit2006/Survey%20Results%20Fact%20Sheet%20092706.pdf. Ac-cessed February 9, 2008.
8. Tucker SJ, Poland GA, Jacobson RM. Requiring influenza vaccinationfor health care workers. Am J Nurs. 2008;108:32-34.
9. Poland GA, Jacobson RM. Protecting patients from harm: legislatingvaccinations for healthcare workers. Am J Prev Med. 2007;32:544-546.
0. Lin CJ, Nowalk MP, Zimmerman RK, et al. Beliefs and attitudes aboutinfluenza immunization among parents of children with chronic medicalconditions over a two-year period. J Urban Health. 2006;83:874-883.
1. Lewis-Parmar H, McCann R. Achieving national influenza vaccinetargets: an investigation of the factors affecting influenza vaccineuptake in older people and people with diabetes. Commun Dis PublicHealth. 2002;5:119-126.
2. Johnson DR, Nichol KL, Lipczynski K. Barriers to adult immunization.Am J Med. 2008;121:S28–S35.
3. Stinchfield PK. Practice-proven interventions to increase vaccination ratesand broaden the immunization season. Am J Med. 2008;121:S11–S21.
4. Fishbein DB, Fontanesi J, Kopald D, et al. Why do not patients receiveinfluenza vaccine in December and January? Vaccine. 2006;24:798-802.
5. American Medical Association. The National Influenza Vaccine Sum-mit home page. Available at: http://www.ama-assn.org/ama/pub/category/13732.html. Accessed December 4, 2007.
6. American Lung Association. Faces of influenza: vaccination recommen-dations [American Lung Association Web site factsheet]. Available at:http://www.facesofinfluenza.org/resources/2007/Recommendations_FactSheet_2007.pdf. Accessed December 4, 2007.
7. National Foundation for Infectious Diseases. Influenza overview/in-troduction. Available at: http://www.nfid.org/influenza. Accessed
December 4, 2007.
5
5
6
6
S10 The American Journal of Medicine, Vol 121, No 7B, July 2008
8. Wallace GS. Vaccine supply. Presented at the Advisory Committeeon Immunization Practices, February 27, 2008; Atlanta, Georgia. Avail-able at: http://www.cdc.gov/vaccines/recs/acip/downloads/mtg-slides-feb08/23-vac-supply.pdf. Accessed December 7, 2007.
9. Brokstad KA, Cox RJ, Olofsson J, et al. Parenteral influenza vaccina-tion induces a rapid systemic and local immune response. J Infect Dis.
1995;171:198-203.0. Gross PA, Russo C, Dran S, et al. Time to earliest peak serum antibodyresponse to influenza vaccine in the elderly. Clin Diagn Lab Immunol.1997;4:491-492.
1. Centers for Disease Control and Prevention (CDC). Breaking fromyour comfort zone: extending the influenza vaccination season[PowerPoint slide presentation]. Available at: www.cdc.gov/vac-
cines/ed/ciinc/calls/flucall.htm. Accessed December 6, 2007.
S
PRPIM
Iehdcc
bt9tc
s
RIS
0d
upplement issue
ractice-Proven Interventions to Increase Vaccinationates and Broaden the Immunization Season
atricia K. Stinchfield, RN, MS, CPNPnfectious Disease, Immunology, Rheumatology and Infection Control, Children’s Hospitals and Clinics of Minnesota, St. Paul,
innesota, USATtsopatiSciIprf©
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ABSTRACT
he Centers for Disease Control and Prevention (CDC) recommends that most (73%) persons residing inhe United States be vaccinated against influenza each year. The actual rate of influenza vaccination isubstantially below target levels: about 60% of persons �65 years (target is 90%) and only 10% to 40%f other groups (target is 60% for younger persons who have risk factors and 60% for healthcareersonnel). Vaccinating patients throughout the influenza vaccination season (from October into Januarynd beyond)—providing access beyond the traditional “fall immunization season” —is an important stepoward meeting the substantial need for influenza vaccination. Vaccination rates may also be increased bynterventions that increase patient demand and access to vaccine and overcome practice-related barriers.uch interventions include vaccination-only clinics, standing orders, strong recommendations from health-are providers, as well as reminder and recall efforts. For maximum impact on immunization rates,nterventions should be combined into a multifaceted immunization program rather than used alone.nterventions that address site-specific needs, taking resources into account, should be implemented on aractice-by-practice basis. With supply of influenza vaccine now plentiful, efforts need to be focused oneducing missed vaccination opportunities and promoting vaccination beyond the traditional fall timerame to protect as many Americans as possible from serious and potentially deadly influenza infection. 2008 Elsevier Inc. All rights reserved. • The American Journal of Medicine (2008) 121, S11–S21
KEYWORDS: Best practices; Influenza; Interventions; Vaccination; Immunization season
8lsiht5Iewcntfuapg
n the United States, most persons in need of annual influ-nza vaccination are seen, at least periodically, in theealthcare system.1 Thus, those who remain unvaccinatedo so, in part, because of missed opportunities (i.e., health-are encounters in which persons who are eligible for vac-ination are not completely vaccinated).
The magnitude of missed vaccination opportunities haseen documented in diverse practice settings. In a prospec-ive cohort study of 4 pediatric practices in Colorado (N �26 children aged 6 to 72 months with �1 chronic condi-ion), missed opportunities for influenza vaccination oc-urred at 68% of visits during October and November and at
Statement of author disclosure: Please see the Author Disclosuresection at the end of this article.
Requests for reprints should be addressed to Patricia K. Stinchfield,N, MS, CPNP, Infectious Disease, Immunology, Rheumatology and
nfection Control Division, Children’s Hospitals and Clinics of Minnesota,t. Paul, Minnesota 55102.
ront matter © 2008 Elsevier Inc. All rights reserved.ed.2008.05.003
6% of visits during the next 2 months.2 Parents reportedack of a physician recommendation and low perceivedusceptibility to influenza as the primary reasons for notmmunizing their children, underscoring the need for strongealthcare provider recommendations and patient educa-ion. In another urban setting, in California, approximately0% of opportunities to immunize were missed (Figure 1).3
n a health maintenance organization, Kramarz and cowork-rs determined that only 9% or 10% of �100,000 childrenith asthma were immunized against influenza during 2
onsecutive years (1995 to 1997), and 61% of the unvacci-ated children had made �1 outpatient clinic visit duringhe influenza season (October through May).4 Extrapolationsrom a large medical claims database indicated that millions ofnimmunized patients visited their healthcare providers onverage 2.2 times between the peak in immunization and theeak in disease activity.5 This underimmunization of high-riskroups was part of the rationale for approving a new policy for
niversal influenza vaccination annually for all children 6
mnm
ntemcvfsott
SIto
qnig(im(g
e2panc
BBvavtfTcsptirct
CPtsp
S12 The American Journal of Medicine, Vol 121, No 7B, July 2008
onths to 18 years.6 With a simple message, “All childreneed an influenza vaccine,” the hope is that morbidity andortality will be prevented in all children.Sustainable systems are needed that support high immu-
ization rates of all at-risk persons targeted for immuniza-ion. This article describes various strategies designed toliminate missed vaccination opportunities and increase im-unization levels. These strategies, especially when used in
ombination, can result in an effective and long-lastingaccine delivery program. The interventions that prove use-ul may differ from practice to practice and over time. Casetudies, which differ in geography, population served, sizef practice, and resources, showcase how these interven-ions have led to meaningful gains in influenza immuniza-ion coverage in day-to-day clinical practice.
UCCESSFUL TYPES OF INTERVENTIONSnfluenza vaccination rates may be improved by interven-ions that increase vaccine access, increase demand, andvercome practice-related barriers (Table 1).7,8
Stone and associates8 conducted a meta-analysis of high-uality studies designed to determine the relative effective-ess of diverse approaches for improving adherence to adultmmunization. They found that interventions involving or-anizational changes in staffing and clinical procedurese.g., vaccine-only clinic, use of a planned care visit formmunization, designation of a nurse or allied health staffember to administer vaccine) were the most effective
adjusted odds ratio [OR], 16.0 vs. usual care or control
Figure 1 Missed vaccination opportunMed.3)
roup). Other effective interventions were provider remind- v
rs (adjusted OR, 3.8) and patient reminders (adjusted OR,.5). A physician recommendation to a patient in a high-riority target group (not assessed in the meta-analysis) haslso been shown to dramatically increase influenza vacci-ation rates.9,10 These and other techniques are briefly dis-ussed below.
roaden the Influenza Vaccinationeginning in 2007, the Centers for Disease Control and Pre-ention (CDC) emphasized the need to offer influenza vaccinend schedule immunization clinics throughout the influenzaaccination season (October into January and beyond). Thus,he period of vaccination now extends beyond the traditionalall immunization season of October through November.11
his message needs to get out to practitioners, because itlearly differs from previous practice. A cross-sectional surveyent to a national, random sample of internists and generalractitioners (N � 1,606) before this change in recommenda-ion revealed that 43% of the respondents stopped vaccinatingn December, and only 27% continued vaccinating into Feb-uary and beyond. Furthermore, 43% of the physicians indi-ated that they were either neutral or hesitant to vaccinate afterhe onset of influenza activity in their community.12
ase Study. In a busy private practice in Clarks Summit,ennsylvania, 1 physician and 2 nurses provide healthcare
o about 5,000 children during 12,000 visits each year. Aeason-long approach achieves high vaccination rates. Theroviders communicate their strong recommendation for
re common. (Reprinted from Am J Prev
ities aaccination at all visits during the influenza vaccination

sad
IHTthilcTo
ow
tesfaovbchc
I
●
●
●
and Ann
S13Stinchfield Practice-Proven Interventions to Increase Vaccination Rates
eason. Educational posters placed in the waiting room urgennual vaccination. Vaccine-only clinics are offered weeklyuring the influenza vaccination season.13
mmunize at Every Opportunity/Extendedours/Vaccine-Only Dayshe CDC recommends that healthcare providers offer vaccine
o their patients at every opportunity, including during routineealthcare visits and during hospitalization, whenever vaccines available. Given the constraints of a busy practice andimited hours of operation, healthcare providers can use spe-ific strategies to increase vaccine access for their patients.hey can direct patients to clinics dedicated to vaccine delivery
Table 1 Strategies to increase influenza vaccination coverage
ntervention Description
Increase vaccine access—Vaccinate in January and beyond Deliver vaccine to
months of the s—Vaccinate at all visit types Assess patient nee
routine visits, s—Vaccine-only clinics—“Express-lane” vaccination
service
Reduce waiting timvaccination-only
—Extend office hours Increase or makeprovided
—Provide vaccination services atalternative, nontraditional
sites
Deliver vaccination
Increase demand—Clinic-based patient education Provide informatio
or public healthposters, booklet
—Community-wide education Deliver informatiotechniques inclubooklets) and co
—Patient reminder/recall systems Send alerts that vtechniques inclu
Overcome practice-related barriers—Standing orders Empower medical
by protocol with—Provider reminders/recall Settings include c
vaccinations thavaccination. Delnotifications.
—Assessment and feedback forvaccination provider
Perform a retrospepatients) and realso involve othstandard)
—Addition of influenza vaccinationto quality-care checklists
Formalize influenzquality patient c
—Provider education andrecommendation
Provide informatioattitudes; techneducation progr
Adapted from the Centers for Disease Control and Prevention (CDC)7
r provide vaccination services during extended office hours or b
n days when the office is typically closed (e.g., vaccine-onlyeekends during the influenza season).Vaccine clinics have become an integral component of
he influenza vaccination program in many practices. Week-nd, evening, or parallel-track daytime “flu vaccine only”essions and walk-in or same-day appointments are use-ul.14 Eliminating the need for making an appointment indvance and avoiding excessive waiting time during a clinicr office visit are factors that encourage some people to seekaccination.15,16 The immunization rate approximately dou-led when a pharmacy team based out of a primary carelinic designed and implemented vaccine-only clinics forigh-risk patients.17 Scheduling vaccine-only or walk-inlinics in January and beyond is 1 way that practices can
ts throughout the influenza season rather than just in the early(October and November)nfluenza vaccination at all types of healthcare visits, includingfollow-up visits, and during hospitalization
d to make an appointment to obtain vaccination throughes
onvenient the hours during which vaccination services are
ettings in which they were not previously provided
rding vaccination to target patients served in a specific medicall setting; techniques include mass mailings, workshops,televisions in the waiting roomding vaccination to a target population in a geographic area;dia campaign (television, radio, newspapers, posters, leaflets,r-based programsions are due (reminders) or late (recall) to patients; deliveryephone calls, letters, postcards, and e-mails
nel to prescribe or deliver vaccinations to patient populationsrect physician involvement at each interactionhospitals, and nursing homes. Inform those who administeridual patients are due (reminder) or overdue (recall) forechniques include flag patient charts, and computer or e-mail
valuation of provider performance (vaccination of at-risksults to providers to motivate higher vaccination rates; canvities (e.g., benchmarking; comparing performance to a goal or
ination into routine practices that form the basis of high-
accination providers to increase their knowledge or changenclude written materials, videos, lectures, continuing medicalnd computer-based learning programs
Intern Med.8
patieneasond for i
ick ande/neeservic
more c
s in s
n regaclinica
s, andn regarde mempute
accinatde tel
personout dilinics,t indivivery t
ctive eport reer acti
a vaccaren to viques iams, a
roaden their influenza vaccination season.
Cfidiamdo
VVbdBsbiaswisea
vAld(
(dbsctphea
cayMtpmocci
dpeaate
S14 The American Journal of Medicine, Vol 121, No 7B, July 2008
ase Study. Mountain Park Health Centers, a federallyunded, full-service pediatric clinic with 4 satellite locationsn and around Phoenix, Arizona, offers influenza vaccineuring extended hours at “no appointment necessary” clin-cs. Children who received influenza vaccine in prior yearsre eligible to come to these clinics. The practice also holdsass influenza vaccine-only clinics on several Saturdays
uring the influenza season. The clinics are publicized byn-site fliers and posters and through postcard mailings.18
accination in Nontraditional Settingsaccines, including influenza vaccines, have historicallyeen administered in traditional medical settings (e.g., pe-iatric clinics and other offices, and health departments).ut these traditional settings may not have sufficient infra-
tructure to handle increasing levels of vaccination. It wille necessary to use every opportunity and setting to delivernfluenza vaccine. Delivery of the 130 million or more dosesvailable during the influenza season requires additionalites and universal understanding that vaccine is beneficialhen administered even after influenza activity has begun
n a community. Development of alternative sites, such aschools, also establishes the infrastructure that will be nec-ssary to address increased vaccine demand in the event ofn influenza pandemic.
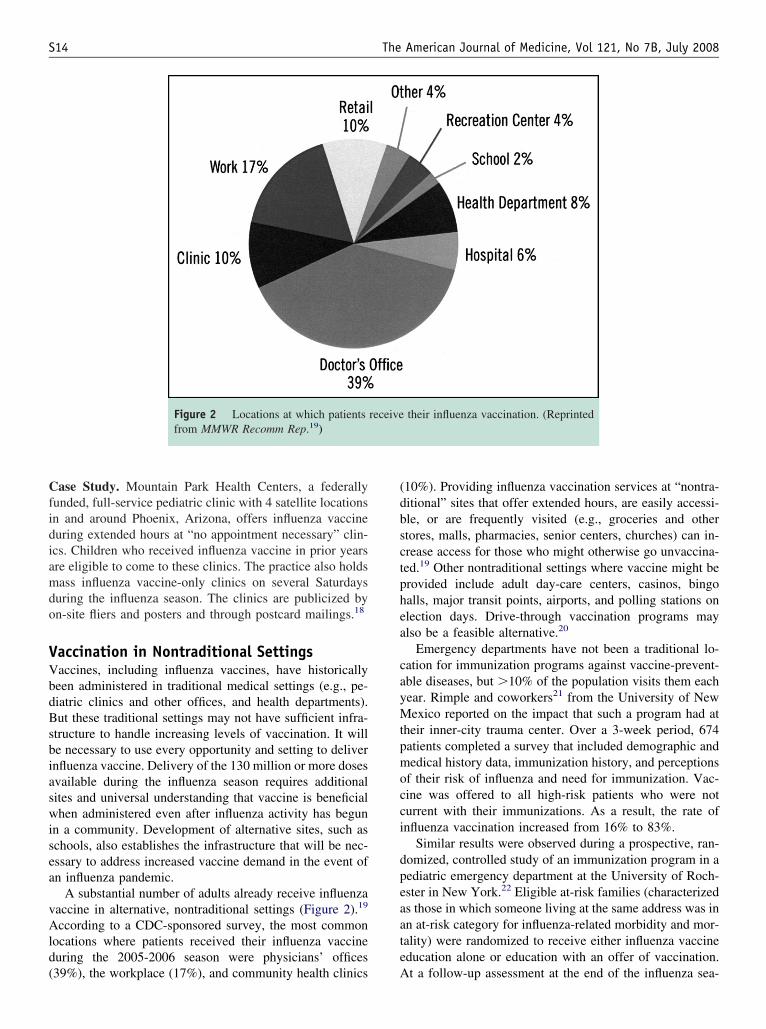
A substantial number of adults already receive influenzaaccine in alternative, nontraditional settings (Figure 2).19
ccording to a CDC-sponsored survey, the most commonocations where patients received their influenza vaccineuring the 2005-2006 season were physicians’ offices
Figure 2 Locations at which patientsfrom MMWR Recomm Rep.19)
39%), the workplace (17%), and community health clinics A
10%). Providing influenza vaccination services at “nontra-itional” sites that offer extended hours, are easily accessi-le, or are frequently visited (e.g., groceries and othertores, malls, pharmacies, senior centers, churches) can in-rease access for those who might otherwise go unvaccina-ed.19 Other nontraditional settings where vaccine might berovided include adult day-care centers, casinos, bingoalls, major transit points, airports, and polling stations onlection days. Drive-through vaccination programs maylso be a feasible alternative.20
Emergency departments have not been a traditional lo-ation for immunization programs against vaccine-prevent-ble diseases, but �10% of the population visits them eachear. Rimple and coworkers21 from the University of Newexico reported on the impact that such a program had at
heir inner-city trauma center. Over a 3-week period, 674atients completed a survey that included demographic andedical history data, immunization history, and perceptions
f their risk of influenza and need for immunization. Vac-ine was offered to all high-risk patients who were noturrent with their immunizations. As a result, the rate ofnfluenza vaccination increased from 16% to 83%.
Similar results were observed during a prospective, ran-omized, controlled study of an immunization program in aediatric emergency department at the University of Roch-ster in New York.22 Eligible at-risk families (characterizeds those in which someone living at the same address was inn at-risk category for influenza-related morbidity and mor-ality) were randomized to receive either influenza vaccineducation alone or education with an offer of vaccination.
their influenza vaccination. (Reprinted
receivet a follow-up assessment at the end of the influenza sea-

sv(attb
tplft
icditfaoctcrdvt
PPpwvplstwmt
knpiaeswptCas
sibbflttea
ptiampsf
RDtlttwwTHa
phmd
SHdvinwsqdua
vrtmh
S15Stinchfield Practice-Proven Interventions to Increase Vaccination Rates
on, the immunization rate was higher among those offeredaccine in the emergency department for pediatric patients57% vs. 36% for those provided education only) and theirccompanying family members (75% vs. 34%, respec-ively). These experiences provide examples of a nontradi-ional setting in which a vaccination program was proved toe feasible and successful.
When developing immunization programs in nontradi-ional settings, healthcare providers should consider theotential role of all forms of influenza vaccine. The newerive attenuated vaccine formulation does not need to berozen and the volume of the dose administered is smallerhan the older formulation.
One issue of concern with widespread influenza vaccinationn nontraditional settings is the resulting fractioning of health-are services and generation of multiple charts that make itifficult to know which of several specialists or generalists hasmmunized the patient. Optimally, all vaccinations should beracked in national immunization information systems (IIS). Inact, a national health objective for 2010 is for 95% of childrenged �6 years to participate in a fully operational IIS.23 Untilptimal IIS use is achieved, however, providers will have toontinue to do a verbal check of vaccination status by askingheir patients if they have received influenza vaccine in theurrent season. Such immunization information systems, oregistries, are especially important for newly vaccinated chil-ren under the age of 9 years who require 2 doses of influenzaaccine in the same season, particularly those who may gethem from different providers.
rovider and Patient Educationersons responsible for administering vaccine, includinghysicians, nurse practitioners, and their staff who interactith patients must be knowledgeable about influenza, theaccines available, and vaccination scheduling. Althoughrovider education is certainly important, in isolation it hasittle impact on immunization rates.24 Yet, it stands to rea-on that when providers are up to date in their knowledge,hey are more likely to establish appropriate standardsithin their practices, and medical and support staff areore likely to be immunized themselves, to communicate
he need for vaccine, and to recommend it to patients.Consistent evidence of provider shortcomings in the
nowledge of persons at risk of influenza25-28 highlights theeed for healthcare providers to take a proactive role inatient education. Survey responses show that many Amer-cans have basic misperceptions about their risk of influenzand its complications, their need for vaccination, and thefficacy and safety of vaccine, and that these misunder-tandings lead to low vaccination rates among those forhom vaccine is recommended. For instance, in a sample ofersons obtained through random-digit dialing, 50% ofhose at high risk of complications from influenza based onDC criteria did not know about their own high-risk statusnd, therefore, were not vaccinated.26 In a national con-
umer survey conducted before the 2006-2007 influenza weason, 48% of respondents said they did not plan to bemmunized and cited various reasons, many of which wereased on misconceptions. Among the explanations was theelief that the vaccine can cause influenza (46%), that in-uenza was not a severe enough illness to justify vaccina-
ion (43%), that they were not at risk of infection (37%), andhat vaccination does not prevent influenza (23%).27 Patientducation should focus on changing misconceptions thatffect vaccination decisions.29
In addition to direct recommendations from their healthcarerovider, patients can receive education about influenza andhe vaccine through other channels. Some examples are prom-nently displayed posters in waiting rooms, brochures, e-mails,nd Web site resources. Public service educational program-ing delivered by mass media (television, radio) also has a
lace in the education of patients, as well as healthcare per-onnel. Direct communication by e-mail or letter to providersrom recognized, local influenza vaccine experts is also helpful.
ecommendation by a Healthcare Professionalirect recommendations from healthcare providers to pa-
ients increase vaccination rates.10 This is especially trueater in the season.30 Among patients with a negative atti-ude about vaccination, Nichol and associates31 noted thathe influenza vaccination rate was 3-fold higher for thosehose physician recommended vaccination than for thoseho did not receive a recommendation from their physician.he impact was even greater in a study by Brewer andallman,26 who found a physician’s recommendation to bestatistically significant predictor of influenza vaccination.Children are more likely to be vaccinated if a healthcare
rofessional recommends it to the parent or guardian. Thisas been demonstrated for healthy children aged 6 to 23onths (OR, 5.5)32 and children with chronic medical con-
itions (OR, 2.6 to 6.0).9,33
tanding Ordersealthcare providers should make operational changes to re-uce barriers and to promote more efficient delivery of routineaccination services.8 One operational change with substantialmpact has been standing orders, or protocols, which allowurses and other allied health personnel to vaccinate personsithout direct physician supervision. In office settings where
tanding orders are in place, the front-office staff can initiateuestions about vaccination status, and designated staff caneliver vaccine; medical intervention is necessary only fornvaccinated patients who decline vaccine or who need anssessment for a true medical contraindication.
Standing orders (Figure 3) have been implemented inarious settings, such as clinics, hospitals, emergencyooms, and nursing homes. Based on their beneficial effect,he Advisory Committee on Immunization Practices recom-ends the use of standing order programs in outpatient and
ospital settings to increase immunization levels.34
Standing orders, whether used alone24,35 or combined
ith other targeted strategies,36 have increased immuniza-
ttn(Tetfitrs
mc
u9audiT
S16 The American Journal of Medicine, Vol 121, No 7B, July 2008
ion rates among adults. In a study of 6 community hospi-als, standing order programs led to a 40% influenza vacci-ation rate, which was superior to both physician reminders17%) and educational programs for physicians (10%).24
he influence of standing orders on vaccine status wasvaluated in a 14-month study conducted at an urban, publiceaching hospital.35 The hospital’s computer system identi-ed inpatients eligible for influenza vaccination, who were
hen randomized to 2 groups: vaccine standing order (di-ected to nurses at the time of patient discharge) and phy-
Figure 3 Sample influenza vaccination standCoalition.)
ician reminder. Standing orders resulted in significantly o
ore patients being vaccinated (42% vs. 30% with physi-ian reminders, P �0.001).
It appears that standing orders for influenza vaccination aresed more commonly for inpatients than outpatients (76% vs.%) and in acute compared with nonacute care settings (prev-lence ratio 1.7).37 Few long-term care facilities (�10%) havesed standing orders to improve vaccination rates of resi-ents,38 which is unfortunate given the sustained benefit real-zed by those facilities that have standing vaccination orders.39
here are ample opportunities for increased use of standing
rder form. (Courtesy of Immunization Action
ing order programs to improve influenza vaccination coverage.

RPcmcn(
iCeirether(
mtTrltrnVr
mcumalws
AEaPaePpl1o
MAdp
aVMwodfCvc
Cgtnpvvtcavwovpm
CHucfCsviwvvamtuevp1s5
C2i4t
S17Stinchfield Practice-Proven Interventions to Increase Vaccination Rates
eminder/Recall Systemsatient and provider reminder/recall systems increase vac-ine coverage.40 For instance, use of a computerized re-inder/automatic telephone recall system in a pediatric
linic in Texas increased the frequency of influenza vacci-ation of children with asthma or reactive airway diseasecohort N � 925) by about 6-fold (from 5% to 32%).41
The effectiveness of patient reminder/recall systems inmproving influenza immunization rates was assessed in aochrane Database systematic literature review.42 Remind-rs were effective for both childhood (OR, 2.87) and adultnfluenza vaccinations (OR, 1.66), increasing immunizationates by 1% to 20% across studies. Reminders were highlyffective in a variety of settings, including academic insti-utions (OR, 3.33), private practice (OR, 1.79), and publicealth clinics (OR, 2.09).43 All types of reminders wereffective: telephone calls (OR, 4.25), patient/practitionereminders (OR, 3.99), postcards (OR, 2.15), autodialer callsOR, 1.51), and letters (OR, 1.50).44
Healthcare professionals can implement their own re-inder/recall systems to facilitate the identification of pa-
ients for whom immunization is due or past due (Figure 4).he form of the reminder will vary based on the needs and
esources of the practice. For example, computer-generatedists can be run to notify a provider of patients to be seenhat day who are in need of vaccination. Alternatively, aeceptionist or nurse can stamp the charts of patients whoeed vaccination with a message such as “No Influenzaaccine on Record” or clip an “Immunization Due” note to
elevant charts.By whatever method, reminder/recalls can decrease
issed vaccination opportunities, especially when they areombined with other strategies with a similar objective. Ifsed consistently by knowledgeable medical staff, a re-inder system can be an aid in promoting immunization of
t-risk patients.1 Sending reminder/recalls in December andater to patients who have not already been vaccinated is aay for practices to broaden their influenza vaccination
eason, in accordance with CDC recommendations.
udit and Feedbackvaluation (audit) and feedback to vaccine providers isnother intervention that can increase immunization rates.rovider performance (i.e., how many at-risk patients are/re not vaccinated) is retrospectively evaluated, and provid-rs are told the results to motivate higher vaccination rates.rovider performance can also be benchmarked or com-ared with a goal or standard. In a systematic review of theiterature, Bordley and colleagues45 found that the results of2 of 15 studies suggested audit and feedback, either aloner in combination, might improve vaccination rates.
ultifaceted Approachlthough each of the aforementioned interventions mayecrease missed vaccination opportunities, a comprehensive
rogram that uses multiple interventions is often the best dpproach. For instance, in a 10-year study conducted at aeterans Administration Medical Center in Minneapolis,innesota, Nichol36 showed that standing orders combinedith physician education, an annual mailing to patients, andther organizational strategies (walk-in clinics, use of stan-ardized, preprinted documentation forms) led to a success-ul and durable influenza vaccination program (Figure 5).ombining any of the above interventions with an expandedaccination season will likely have even greater impact onompliance with CDC recommendations.
ase Study: Private Pediatric Clinic. A private pediatricroup practice in Nashville (12 pediatricians; 26,000 pa-ients) combines many interventions, with a goal of immu-izing all children in recommended categories and any otheratient desiring the vaccine.46 Parents are educated aboutaccination for preventable diseases at all well and sickisits. A patient reminder is mailed in September. Duringhe influenza season, the practice’s “on-hold” message in-ludes information about influenza vaccination, which canlso be found on the practice’s Web site. To streamlineaccine delivery, multiple vaccine clinic days are offered,ith nurses administering vaccine according to a standingrder; the clinics allow for 10 appointments per hour. Theaccination program is evaluated at the end of every season,otential areas for improvement are discussed, and adjust-ents are made.
ase Study: Large Healthcare System. The Geisingerealth System, with �40 clinics throughout Pennsylvania,ses a multifaceted approach to identify, remind, and vac-inate high-risk patients (e.g., those with diabetes, heartailure, or end-stage renal disease).47 As part of Proven-are,SM a program designed to change the way the medical
ystem delivers care, at-risk patients in need of influenzaaccination are identified by searching the electronic med-cal database. These patients receive a reminder letter,hich notes that they are due for their annual influenzaaccine and provides a telephone number to schedule aaccination appointment. A medical staff member contactsll persons who do not schedule a visit. In addition, theedical information system initiates a warning flag each
ime unvaccinated, at-risk persons make a visit for a reasonnrelated to influenza vaccine. Delivery of vaccine is madeasier by a standing order, allowing nurses to administeraccine to patients without a provider preorder. With thisrogram in place, the majority of high-risk patients (75% of6,000) were vaccinated during the 2006-2007 influenzaeason, including 69% of patients with diabetes (up from7% in the previous year).
ase Study: University-Based Clinic. During the 2007-008 influenza season, Arizona State University increasednfluenza vaccination among students, faculty, and staff by1% (from 2,343 to 3,980 vaccine doses), compared withhe previous year.48 The improved vaccination rate occurred
espite an increase in price from $10 per vaccination in
2mnaeitr
vp
CCPc
S18 The American Journal of Medicine, Vol 121, No 7B, July 2008
006 to $18 for students and $20 for employees in 2007. Aultifaceted program included convenient access to vacci-
ations and increasing demand through education and give-ways. Vaccine was made available during 2 week-longvents at the student union. In addition, nurses visited res-dence halls. Education and awareness were enhancedhrough signage, advertising in the student newspaper and
Figure 4 Sample provider reminderClinics of Minnesota.)
adio station, and free T-shirts given to persons who were h
accinated. Next season, a vaccination event is beinglanned during parents’ weekend.
ase Study: Hospital-Based Ambulatory Pediatriclinic. Children’s Hospitals and Clinics of Minnesota–St.aul (Children’s–St. Paul) has a multispecialty ambulatorylinic associated with the 150-bed, tertiary care children’s
(Courtesy of Children’s Hospitals and
form.ospital. Approximately 29,000 outpatient visits are con-
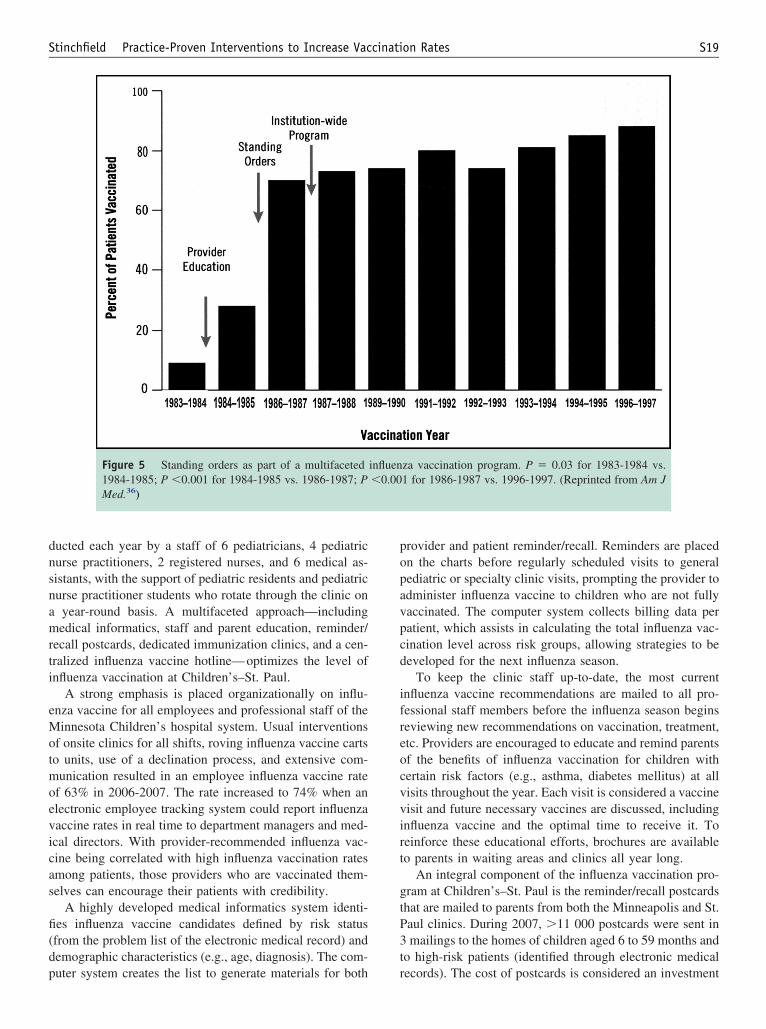
dnsnamrti
eMotmoevicas
fi(dp
popavpcd
ifreocvvirt
gtP3t
S19Stinchfield Practice-Proven Interventions to Increase Vaccination Rates
ucted each year by a staff of 6 pediatricians, 4 pediatricurse practitioners, 2 registered nurses, and 6 medical as-istants, with the support of pediatric residents and pediatricurse practitioner students who rotate through the clinic onyear-round basis. A multifaceted approach—includingedical informatics, staff and parent education, reminder/
ecall postcards, dedicated immunization clinics, and a cen-ralized influenza vaccine hotline—optimizes the level ofnfluenza vaccination at Children’s–St. Paul.
A strong emphasis is placed organizationally on influ-nza vaccine for all employees and professional staff of theinnesota Children’s hospital system. Usual interventions
f onsite clinics for all shifts, roving influenza vaccine cartso units, use of a declination process, and extensive com-unication resulted in an employee influenza vaccine rate
f 63% in 2006-2007. The rate increased to 74% when anlectronic employee tracking system could report influenzaaccine rates in real time to department managers and med-cal directors. With provider-recommended influenza vac-ine being correlated with high influenza vaccination ratesmong patients, those providers who are vaccinated them-elves can encourage their patients with credibility.
A highly developed medical informatics system identi-es influenza vaccine candidates defined by risk statusfrom the problem list of the electronic medical record) andemographic characteristics (e.g., age, diagnosis). The com-
Figure 5 Standing orders as part of a multifaceted1984-1985; P �0.001 for 1984-1985 vs. 1986-1987; PMed.36)
uter system creates the list to generate materials for both r
rovider and patient reminder/recall. Reminders are placedn the charts before regularly scheduled visits to generalediatric or specialty clinic visits, prompting the provider todminister influenza vaccine to children who are not fullyaccinated. The computer system collects billing data peratient, which assists in calculating the total influenza vac-ination level across risk groups, allowing strategies to beeveloped for the next influenza season.
To keep the clinic staff up-to-date, the most currentnfluenza vaccine recommendations are mailed to all pro-essional staff members before the influenza season beginseviewing new recommendations on vaccination, treatment,tc. Providers are encouraged to educate and remind parentsf the benefits of influenza vaccination for children withertain risk factors (e.g., asthma, diabetes mellitus) at allisits throughout the year. Each visit is considered a vaccineisit and future necessary vaccines are discussed, includingnfluenza vaccine and the optimal time to receive it. Toeinforce these educational efforts, brochures are availableo parents in waiting areas and clinics all year long.
An integral component of the influenza vaccination pro-ram at Children’s–St. Paul is the reminder/recall postcardshat are mailed to parents from both the Minneapolis and St.aul clinics. During 2007, �11 000 postcards were sent inmailings to the homes of children aged 6 to 59 months and
o high-risk patients (identified through electronic medical
za vaccination program. P � 0.03 for 1983-1984 vs.1 for 1986-1987 vs. 1996-1997. (Reprinted from Am J
influen�0.00
ecords). The cost of postcards is considered an investment

ipocwhTr
ih2vwewpwb
sncc
lenfnDivtvpac
pohl1wt2
hatniiah
SDtmfhtddmilTuzciram
ATt
co
R
S20 The American Journal of Medicine, Vol 121, No 7B, July 2008
n reaching the highest risk patients. For cost-effectiveness,ostcards were mailed in the 2007 season late in Decembernly to those high-risk patients who had not yet been vac-inated. Data are tracked based on high-risk patients whoere sent postcards as identified through the data ware-ouse, compared with those billed for influenza vaccine.his does not take into account vaccine that may have been
eceived elsewhere.To increase the efficiency of administration and access to
nfluenza vaccine, 4 half-day vaccination-only clinics wereeld on Saturdays in October and November of the 2006-007 season. In 2007-2008, these “flu-vaccine-clinic–onlyisits” were integrated into the day and evening hours,ith 2 medical assistants vaccinating up to 6 patients
very 15 minutes (most had appointments, but walk-insere accepted as well). All relevant paperwork and sup-lies were prepared in advance and placed in a roomhere the vaccinators remained and the patients wererought to them.
An influenza vaccine hotline complements direct profes-ional-to-patient/parent education. Updated daily or aseeded with new information, this centralized resource in-ludes the latest influenza news, any alerts about supplyhanges, flu clinic details, and similar information.
The 2006-2007 influenza season in Minnesota startedate with infections beginning in earnest in January. How-ver, late in January there were 6 pediatric deaths in Min-esota in a 4-week period. This created huge public demandor vaccination later in the season. With 48 hours of plan-ing, Children’s–St. Paul collaborated with the Minnesotaepartment of Health and the county to vaccinate �1,000
ndividuals, mostly insured children from neighboring pri-ate clinics in a 4-hour Saturday clinic and another 1,100he following Saturday morning. There were 30 rooms andaccinators available, but the vaccinations were accom-lished with 21 rooms and vaccinators active at the peaknd another 10 support staff (working the front desk, crowdontrol, etc.).
The memory of the pediatric deaths remained fresh inarents’ minds in 2007 and 2008, resulting in a high uptakef vaccine early in the season. Because vaccine uptake wasigh early in the season, there was barely a surge in demandate in the season when an influenza-related death of a2-year-old with asthma and a staphylococcal pneumoniaas well publicized. Data are being analyzed at this writing
o compare rates from the 2006-2007 season with the 2007-008 season.
Provider education, both formal and informal in 2008,as emphasized starting to vaccinate as soon as vaccine isvailable and through the influenza season. In 2007-2008,he late onset of the season was a good reminder that “it isot too late to vaccinate,” and this was a constant messagen the clinics, hospital, and in the media. Emphasis to keepmmunizing well past the winter holidays through Januarynd February will slowly be helpful in “unlearning” an old
abit and learning a new practice.UMMARYespite the documented beneficial effects of several prac-
ice-proven interventions, meaningful proportions of pri-ary care physicians (14%) and medical specialists (25%)
ail to strongly recommend influenza vaccinations to theirigh-risk and elderly patients, according to a self-adminis-ered questionnaire.49 Likewise, many physicians (�70%)o not use other effective strategies for promoting vaccineelivery (e.g., special clinics, standing orders, patient re-inders). Taken together, these findings suggest areas for
mprovement if all vaccination opportunities are to be uti-ized and national immunization goals are to be reached.he case studies described above illustrate the techniquessed in a range of practice settings to broaden the immuni-ation season and increase influenza vaccination rates. Byombining relevant aspects of these approaches with othernterventions that are based on the particular needs andesources of the practice, healthcare providers should beble to extend the benefits of vaccination to all recom-ended patients.
UTHOR DISCLOSUREShe author of this article has disclosed the following indus-
ry relationships:Patricia K. Stinchfield, RN, MS, CPNP, has no finan-
ial arrangement or affiliation with a corporate organizationr a manufacturer of a product discussed in this article.
eferences1. Atkinson W, Hamborsky J, McIntyre L, Wolfe S, eds, for the Centers
for Disease Control and Prevention (CDC). Epidemiology and Pre-vention of Vaccine-Preventable Diseases. 10th ed. Washington, DC:Public Health Foundation, 2007.
2. Daley MF, Beaty BL, Barrow J, et al. Missed opportunities for influ-enza vaccination in children with chronic medical conditions. ArchPediatr Adolesc Med. 2005;159:986-991.
3. Prislin R, Sawyer MH, De Guire M, et al. Missed opportunities toimmunize: psychosocial and practice correlates. Am J Prev Med.2002;22:165-169.
4. Kramarz P, DeStefano F, Gargiullo PM, et al. Influenza vaccination inchildren with asthma in health maintenance organizations: VaccineSafety Datalink Team. Vaccine. 2000;18:2288-2294.
5. Poland GA, Johnson DR. Increasing influenza vaccination rates: theneed to vaccinate throughout the entire influenza season. Am J Med.2008;[this issue].
6. Centers for Disease Control and Prevention (CDC). ACIP provisionalrecommendations for the prevention and control of influenza [CDCWeb site]. Available at: http://www.cdc.gov/vaccines/recs/provisional/downloads/flu-3-21-08-508.pdf. Accessed April 4, 2008.
7. Centers for Disease Control and Prevention (CDC). Vaccine-prevent-able diseases: improving vaccination coverage in children, adoles-cents, and adults: a report on recommendations of the Task Force onCommunity Preventive Services. MMWR Morb Mortal Wkly Rep.1999;48(RR08):1-16.
8. Stone EG, Morton SC, Hulscher ME, et al. Interventions that increaseuse of adult immunization and cancer screening services: a meta-analysis. Ann Intern Med. 2002;136:641-651.
9. Lin CJ, Nowalk MP, Zimmerman RK, et al. Beliefs and attitudes aboutinfluenza immunization among parents of children with chronic med-ical conditions over a two-year period. J Urban Health. 2006;83:
874-883.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
S21Stinchfield Practice-Proven Interventions to Increase Vaccination Rates
0. Lewis-Parmar H, McCann R. Achieving national influenza vaccinetargets—an investigation of the factors affecting influenza vaccineuptake in older persons and people with diabetes. Commun Dis PublicHealth. 2002;5:119-126.
1. Centers for Disease Control and Prevention (CDC). Prevention andcontrol of influenza: recommendations of the Advisory Committee onImmunization Practices (ACIP), 2007. MMWR Recomm Rep. 2007;56(RR06):1-54.
2. Davis MM, McMahon SR, Santoli JM, et al. A national survey ofphysician practices regarding influenza vaccine. J Gen Intern Med.2002;17:670-676.
3. National Foundation for Infectious Diseases. Kids need flu vaccinetoo! Case study: solo pediatric practice. Available at: http://kidsneedfluvaccinetoo.nfidinitiatives.org/pdf/solocasestudies.pdf. AccessedFebruary 13, 2008.
4. Britto MT, Schoettker PJ, Pandzik GM, et al. Improving influenzaimmunisation for high-risk children and adolescents. Qual Saf HealthCare. 2007;16:363-368.
5. Hinman AR. Immunizations in the United States. Pediatrics. 1990;86:1064-1066.
6. Orenstein WA, Atkinson W, Mason D, Bernier RH. Barriers to vac-cinating preschool children. Am J Public Health. 1991;81:1057-1059.
7. Van Amburgh JA,Waite NM, Hobson EH, Migden H. Improved in-fluenza vaccination rates in a rural population as a result of a phar-macist-managed immunization campaign. Pharmacotherapy. 2001;21:1115-1122.
8. National Foundation for Infectious Diseases. Kids need flu vaccinetoo! Case study: group pediatric practice. Available at: http://kidsneedfluvaccinetoo.nfidinitiatives.org/pdf/groupcasestudies.pdf.Accessed February 13, 2008.
9. Centers for Disease Control and Prevention (CDC). Adult immunizationprograms in nontraditional settings: quality standards and guidance forprogram evaluation. MMWR Recomm Rep. 2000;49(RR01):1-13.
0. Carrico R. Influenza vaccine program: a drive-thru immunization pro-cess [abstract]. Am J Infect Control. 1999;27:191.
1. Rimple D, Weiss SJ, Brett M, Ernst AA. An emergency department-basedvaccination program: overcoming the barriers for adults at high risk forvaccine-preventable diseases. Acad Emerg Med. 2006;13:922-930.
2. Pappano D, Humiston S, Goepp J. Efficacy of a pediatric emergencydepartment-based influenza vaccination program. Arch Pediatr Ado-lesc Med. 2004;158:1077-1083.
3. Centers for Disease Control and Prevention (CDC). IIS: frequentlyasked questions [CDC Web site]. Available at: http://www.cdc.gov/vaccines/programs/iis/providers.htm. Accessed April 4, 2008.
4. Crouse BJ, Nichol K, Peterson DC, Grimm MB. Hospital-based strategiesfor improving influenza vaccination rates. J Fam Pract. 1994;38:258-261.
5. Adler GS. Influenza vaccination and self-reported reasons for not receiv-ing influenza vaccination among medicare beneficiaries aged �65 years:United States, 1991-2002. MMWR. 2004;53(43):1012-1015.
6. Brewer NT, Hallman WK. Subjective and objective risk as predictorsof influenza vaccination during the vaccine shortage of 2004-2005.Clin Infect Dis. 2006;43:1379-1386.
7. National Foundation for Infectious Diseases. Public perception ofinfluenza, vaccination and treatment options: national consumer sur-vey sponsored by the National Foundation for Infectious Diseases(NFID) [NFID Web site]. Available at: http://www.connectlive.com/events/infectiousdiseases/presskit2006/Survey%20Results%20Fact%20Sheet%20092706.pdf. Accessed February 13, 2008.
8. Jones TF, Ingram LA, Craig AS, Schaffner W. Determinants of influ-enza vaccination, 2003-2004: shortages, fallacies and disparities. ClinInfect Dis. 2004;39:1824-1828.
9. Zimmerman RK, Nowalk MP, Raymund M, Tabbarah M, HallDG, Wahrenberger JT, Wilson SA, Ricci EM. Tailored interven-tions to increase influenza vaccination in neighborhood health centersserving the disadvantaged. Am J Public Health. 2003;93:1699-1705.
0. Fishbein DB, Fontanesi J, Kopald D, et al. Why do not patientsreceive influenza vaccine in December and January? Vaccine. 2006;
24:798-802.1. Nichol KL, Mac Donald R, Hauge M. Factors associated with influ-enza and pneumococcal vaccination behavior among high-risk adults.J Gen Intern Med. 1996;11:673-677.
2. Nowalk MP, Zimmerman RK, Lin CJ, et al. Parental perspectives oninfluenza immunization of children aged 6 to 23 months. Am J PrevMed. 2005;29:210-214.
3. Gnanasekaran SK, Finkelstein JA, Hohman K, et al. Parental perspec-tives on influenza vaccination among children with asthma. PublicHealth Rep. 2006;121:181-188.
4. Centers for Disease Control and Prevention (CDC). Use of standingorder programs to increase adult vaccination rates: recommendationsof the Advisory Committee on Immunization Practices. MMWRRecomm Rep. 2000;49(RR01):15-26.
5. Dexter PR, Perkins SM, Maharry KS, et al. Inpatient computer-basedstanding orders vs physician reminders to increase influenza and pneu-mococcal vaccination rates: a randomized trial. JAMA. 2004;292:2366-2371.
6. Nichol KL. Ten-year durability and success of an organized programto increase influenza and pneumococcal vaccination rates among high-risk adults. Am J Med. 1998;105:385-392.
7. Pentakota SR, Halperin W. Prevalence and trend in the use of hospital-based standing orders programs for influenza and pneumococcal vac-cination. Infect Control Hosp Epidemiol. 2007;28:899-904.
8. Shefer A, McKibben L, Bardenheier B, et al. Characteristics of long-term care facilities associated with standing order programs to deliverinfluenza and pneumococcal vaccinations to residents in 13 states.J Am Med Dir Assoc. 2005;6:97-104.
9. Stevenson KB, McMahon JW, Harris J, et al. Increasing pneumococcalvaccination rates among residents of long-term–care facilities: provid-er-based improvement strategies implemented by peer-review organi-zations in four western states. Infect Control Hosp Epidemiol. 2000;21:705-710.
0. Briss PA, Rodewald LE, Hinman AR, et al. Reviews of evidenceregarding interventions to improve vaccination coverage in children,adolescents, and adults: the Task Force on Community PreventiveServices. Am J Prev Med. 2000;18(suppl):97-140.
1. Gaglani M, Riggs M, Kamenicky C, Glezen WP. A computerizedreminder strategy is effective for annual influenza immunization ofchildren with asthma or reactive airway disease. Pediatr Infect Dis J.2001;20:1155-1160.
2. Jacobson VJ, Szilagyi P. Patient reminder and patient recall systems toimprove immunization rates. Cochrane Database Syst Rev. 2005;(3):CD003941.
3. Szilagyi P, Vann J, Bordley C, et al. Interventions aimed at improvingimmunization rates. Cochrane Database Syst Rev. 2002;(4):CD003941.
4. Szilagyi PG, Bordley C, Vann JC, et al. Effect of patient reminder/recall interventions on immunization rates: a review. JAMA. 2000;284:1820-1827.
5. Bordley WC, Chelminski A, Margolis PA, et al. The effect of audit andfeedback on immunization delivery: a systematic review. Am J PrevMed. 2000;18:343-350.
6. National Foundation for Infectious Diseases. Case studies: modelsand strategies for increasing influenza vaccination rates in childrenwith asthma [NFID Web site]. Available at: http://influenzaasthma.nfidinitiatives.org/privatepractice.html. Accessed February 13, 2008.
7. Fallik D. Models in quality: new system gives patients and practitio-ners a heads up [AAMC Web site]. Available at: http://www.aamc.org/newsroom/reporter/may07/quality.htm. Accessed February 13, 2008.
8. Markus AL. Influenza vaccination: challenges for adolescent and col-lege healthcare. Available at: http://www.medscape.com/viewarticle/568193. Accessed February 13, 2008.
9. Nichol KL, Zimmerman R. Generalist and subspecialist physicians’knowledge, attitudes, and practices regarding influenza and pneumo-coccal vaccinations for elderly and other high-risk patients: a nation-
wide survey. Arch Intern Med. 2001;161:2702-2708.
S
LDPWa
o
Idatoetnof
s
E3
0d
upplement issue
essons Learned: Role of Influenza Vaccine Production,istribution, Supply, and Demand—What It Means for therovideralter A. Orenstein, MD,a William Schaffner, MDb
Emory Vaccine Center, Atlanta, Georgia, USA; and bDepartments of Preventive Medicine and Medicine, Vanderbilt University School
f Medicine, Nashville, Tennessee, USAT(rpdgtFdtpwdtfna©
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ABSTRACT
he Advisory Committee on Immunization Practices of the Centers for Disease Control and PreventionCDC) has been increasing the size of the population for whom influenza vaccine is recommended toeduce the substantial and persistent annual health burden of influenza. Realization of current and futureublic health influenza immunization goals requires assuring vaccine supply will be adequate to meetemand. This has posed distinct challenges for the many stakeholders in the influenza vaccine program—overnment agencies, federal, state, and local policymakers, vaccine manufacturers and distributors, andhe medical community— each of whom must make critical decisions in a constantly shifting environment.actors such as the yearly changes in influenza virus strains, the complicated vaccine production andistribution process, revisions in vaccination recommendations, and changing demographics can all affecthe delicate balance between supply and demand. While vaccine shortages and delays have been well-ublicized concerns in the recent past, there has been a marked increase in supply in the past several years,ith substantial growth in supply expected in the future. The primary issue today is to strengthen theemand for the influenza vaccine, which would in turn help ensure the continued availability of the vaccineo reduce disease burden. A number of strategies are discussed, including increased efforts to publicize andully implement current CDC recommendations and to offer influenza vaccine beyond the typical vacci-ation season of October and November, because in the great majority of years, vaccination into Januarynd beyond will still provide health benefits. 2008 Elsevier Inc. All rights reserved. • The American Journal of Medicine (2008) 121, S22–S27
KEYWORDS: Demand; Influenza; Supply; Vaccine production
mc2wwtawtvm
bia
nfluenza causes the greatest vaccine-preventable burden ofisease in the United States, accounting for an estimatednnual average of 36,000 deaths and 226,000 hospitaliza-ions.1,2 To decrease this burden, the Advisory Committeen Immunization Practices (ACIP) of the Centers for Dis-ase Control and Prevention (CDC) gradually has increasedhe size of the population recommended for annual vacci-ation, which now covers about 73% of the US population,r 218 million people.3 This includes persons at high riskor complications from influenza and the individuals who
Statement of author disclosure: Please see the Author Disclosuresection at the end of this article.
Requests for reprints should be addressed to Walter A. Orenstein, MD,mory Vaccine Center, 1462 Clifton Road NE, Suite 446, Atlanta, Georgia0322.
ront matter © 2008 Elsevier Inc. All rights reserved.ed.2008.05.004
ight transmit the virus to them, such as their householdontacts and healthcare workers. Starting no later than the009-2010 influenza season, vaccination recommendationsill be extended to include all children 5 to 18 years of age,4
hich will add approximately 30 million children (�10% ofhe US population) to the group who should be vaccinatednnually. In addition, the ACIP encourages anyone whoants to avoid influenza to obtain the vaccine. Thus, almost
he entire US population is either recommended to beaccinated annually or is covered by a permissive recom-endation.Influenza vaccine is different from all other vaccines
ecause it is administered annually to persons for whom its recommended. More doses of influenza vaccine are usednnually than of any other vaccine.5 Nevertheless, the bur-
ens of providing influenza vaccine have left many provid-
ergtwt
esemtrchwrturaydimga
sfpaC(y2CitirfpadewKpetarmTia
pncnlav
PAvivbarvsi(rwcvmctpf
aogztibscsmstpetpuiegvTsb
S23Orenstein and Schaffner Factors Influencing Influenza Vaccine Availability
rs frustrated. The purpose of this article is to explain theeasons why there may be problems in vaccine supply in aiven season and to outline potential steps providers canake to help their patients avoid the burdens of influenzahile at the same time enhancing production and distribu-
ion capacity to meet present and future demands.In the United States, the major stakeholders in the influ-
nza immunization program include government agencies,tate, federal, and local policymakers, vaccine manufactur-rs, distributors, and clinicians, including community im-unizers as well as those who provide influenza vaccine at
he workplace.6 These participants must make decisionsegarding the vaccine composition, the assessment of vac-ine potency and purity, the amount of vaccine to produce,ow many doses to order, how to distribute, how to finance,hen to administer the vaccine and to whom, and how to
each patients. Numerous factors come into play, many ofhem subject to change. For example, influenza virusesndergo frequent mutations. Thus, the vaccine must beeformulated each year to include new strains experts thinkre likely to circulate the following season. In any givenear, availability of vaccine may be affected by low pro-uction yields, higher-than-expected demand, and changesn vaccine recommendations. Longer-term factors (e.g., de-ographic), such as the increase in the elderly population, a
roup at high risk for influenza-related complications, maylso influence future supply and demand.
There have been several influenza supply disruptionsince the 2001-2002 season.7,8 Disruptions have occurred,or example, when manufacturers have exited the market-lace or when manufacturers’ products became availablefter the traditional influenza vaccination season, which theDC had previously defined as October through November
now considered to be October into January and be-ond).3,9,10 A highly publicized shortage occurred in 2004-005, when contamination forced the vaccine manufacturerhiron to suspend production of its anticipated 46 million
nfluenza doses at its facility in Liverpool, England. At theime, Chiron was 1 of only 3 companies providing thenfluenza vaccine to the US market, and these lost dosesepresented about half of the anticipated US vaccine supplyor 2004-2005. Although federal agencies moved quickly torioritize who should receive the vaccine, concern eventu-lly focused on the country’s inability to administer alloses of even this limited supply.11,12 With the subsequentntry of additional manufacturers into the marketplace,hich now includes sanofi pasteur, Novartis, GlaxoSmith-line, MedImmune, and CSL Biotherapies, the vaccineroduction capacity appears to be less vulnerable. It isstimated that a record 130 million doses were produced forhe 2007-2008 influenza season,13 and in the future, a steadynd plentiful supply of vaccine is expected. Thus, the over-iding issue today involves complying with ACIP recom-endations to prevent the influenza burden each season.his requires increasing consumer demand and providing
ncentives to providers to ensure sufficient supply. For ex-
mple, annual coverage for persons �65 years, 1 of the wriority groups for vaccination, is typically �70%, whenational targets call for �90%.14 This article discusses theurrent system of vaccine production, distribution, and fi-ancing in the context of supply and demand. It also high-ights new developments and approaches that may helpchieve immunization goals to the benefit of all influenzaaccine stakeholders.
RODUCTION OF THE INFLUENZA VACCINElthough a larger manufacturing base will help to avertaccine supply shortages, some degree of uncertainty isnevitable, given the inherent complexities of the influenzaaccine production process. Unlike manufactured drugs,iologics are natural products and therefore are less predict-ble.15 The lack of predictability begins with influenza vi-uses themselves. One or more of 3 strains of influenzairuses are responsible for seasonal influenza epidemics–2trains of type A influenza (A/H1N1 and A/H3N2) andnfluenza type B. These viruses undergo antigenic changesantigenic drift), resulting in new strains that may not beecognized by the body’s immune system.16 To keep upith these changes and remain effective, the influenza vac-
ine is reevaluated each year and reformulated when newariants appear to be emerging. Even if there is no refor-ulation, vaccine must be produced anew each year be-
ause it is not until March that the strains to be included inhe following season’s vaccine are decided upon. Thus, therevious year’s vaccine expires and must be discarded be-ore the next influenza vaccination season.
Vaccine production takes about 8 or 9 months, but isctually an ongoing process if one considers the importancef year-round global influenza surveillance.17 Based onlobal surveillance data collected by World Health Organi-ation (WHO) Collaborating Centers, including the CDC,he US Food and Drug Administration (FDA) selects 3nfluenza strains (type B, A/H1N1, and A/H3N2) thought toe the likely cause of influenza epidemics in the upcomingeason. The efficacy of the vaccine depends in part upon alose match between the vaccine strains and circulatingtrains. However, even when the vaccine is not optimallyatched to the predominant viruses, it usually still affords
ome protection, inasmuch as antibodies made in responseo the vaccine can protect against related strains (cross-rotection).18 In January, the CDC provides influenza “ref-rence” viruses to the FDA, which distributes them, in turn,o the manufacturers.17 It should be noted that at this earlyoint in the production process, well in advance of thepcoming influenza season, manufacturers must considerssues of both supply and demand. For example, they muststimate demand, taking into account “prebookings” fromovernment, large public/private purchasers, and small pri-ate purchasers, as well as the previous year’s demand.15,17
hey must consider the “yield,” or growth potential, of eachtrain, because this dictates the amount of vaccine that cane produced, while also estimating the number of doses that
ill be produced by other manufacturers.
wcefisatnsovaavtadtleu
DP(puust
itsOltbctud
woatiordes
GSPipr3
S24 The American Journal of Medicine, Vol 121, No 7B, July 2008
The vaccine production cycle extends through August,hen completed lots become available.17 During this pro-
ess, the FDA tests vaccines multiple times for purity andfficacy. Indeed, the testing and approval process accountsor a substantial proportion of production time. For bothnjectable and nasal vaccines, the 3 strains are producedeparately in embryonic eggs. The monovalent concentratesre harvested and combined into the trivalent form, which ishen used to fill vaccine delivery devices (vials, syringes,asal sprayers).17 Injectable vaccines undergo additionalteps after harvesting including inactivation and disruptionf the lipid envelope of the virus resulting in split or sub-irion products.19 Live attenuated vaccines for intranasaldministration are produced by reassortment of cold-dapted, temperature-sensitive parent virus strains with wildiruses to produce a virus containing the 6 internal genes ofhe parent attenuated strain and the hemagglutinin and neur-minidase of the wild virus.20 Vaccines are packaged foristribution and kept at appropriate temperatures to guaran-ee potency. Each lot must be approved separately for re-ease by the FDA before shipment. Thus, no matter howfficiently vaccine is produced, it will generally be distrib-ted in stages over time.
ISTRIBUTIONrivate practices, public clinics, and other small and largee.g., pharmacy chains and supermarkets) immunizationroviders may order vaccine either directly from the man-facturers, or from a distributor. Orders are taken by man-facturers and distributors as early as January of the prioreason. Distribution normally begins in September and con-
0
20
40
60
80
100
Cum
ulat
ive
Perc
ent o
f Dos
es
Aug Sep O
6%
30%
71%
Cumulative percent of ireleased by manufacturTraditional seasonal dem
Figure 1 Influenza vaccine suppl2004 to 2007; †Based on influenza vseason. (Adapted from “Vaccine Stions”21 and Clin Infect Dis.22)
inues for as long as vaccine supplies are available. t
The timing of vaccine production as well as distributionssues generally results in vaccine supply reaching providershroughout the fall months. During the last 3 influenzaeasons, about 70% of the vaccine supply was delivered byctober.21 In previous seasons, when total supply was
ower, early demand usually outpaced early supply. Givenhe recent increases in supply, this will hopefully no longere the case. However, a substantial number of doses willontinue to be delivered after the current peak in vaccina-ion (Figure 1).21,22 Extending vaccination efforts into Jan-ary and beyond will harmonize supply-demand discor-ance and provide protection for more at-risk individuals.
The existence of multiple vaccine producers coupledith numerous distribution channels also affects the timingf vaccine delivery, thereby creating real or perceived short-ges and delays. Thus, there may be temporary shortages athe local level, even when the national supply is adequate. Its also possible that providers in the same local area whordered from different manufacturers or distributors mayeceive their vaccine supply at different times. Indeed, theseisparities in vaccine delivery at the local level, particularlyarly in the vaccination season, continue to be a substantialource of confusion and concern among physicians.
ROWING THE DEMAND TO ENSURE THEUPPLYublic (federal, state, and local) and private (health plans,
nsurers, providers) stakeholders have an important role tolay in increasing the demand for the influenza vaccine toeach the �80% of the US population (which includes the0 million children recommended to be vaccinated no later
Nov Dec Jan
96% 99% 100%
vaccine
influenza vaccine†
Vaccine Demand
us demand. *Composite data fromtion pattern–Tennessee, 2003-2004Update & Programmatic Implica-
ct
nfluenza ers*
and for
y versaccinaupply
han the 2009-2010 season) who should be vaccinated an-

nivsttudf
sgwepCcaFipaoibpm
htfisnmcpivwoeo
rstfmipiddsTit
aitwetplscc
WHdsaJcivtt
otcappavllopnc
(ditftTlts
eisas
S25Orenstein and Schaffner Factors Influencing Influenza Vaccine Availability
ually. Driving the demand up would not only ensure thatndividuals and populations who would benefit from theaccine actually receive it, but would also help to mitigateome of the risks, thereby encouraging the continued par-icipation of manufacturers, distributors, and providers inhe system.7 The willingness of manufacturers and distrib-tors to participate in the program depends, to a largeegree, on demand for the vaccine and adequate returnsrom sales.10,15
The financing of immunizations is 1 component of as-uring vaccine availability. In the case of children, theovernment shares the burden for immunization coverageith the private insurance industry and private payers/par-
nts.23 Two sources of federal funds are the Section 317rogram, administered by the CDC, and the Vaccines forhildren program. Since 1993, Medicare has reimbursed theosts of the influenza (and pneumococcal) vaccine for thoseged �65 years without applying a copay or deductible.23
or other adults, the government has only a modest role, andnfluenza vaccines are purchased and administered in therivate sector. Gaps and fragmentation of insurance cover-ge are areas of concern. Limited insurance coverage notnly increases the stress placed on the public sector but alsoncreases the burden on private providers. These financialarriers for patients and providers may lead to missed op-ortunities for immunization, depressing demand and ulti-ately supply.24
Addressing financing issues is only part of the solution,owever. Influenza vaccination rates have remained subop-imal even in vulnerable populations (e.g., Medicare bene-ciaries �65 years old) that have coverage. According to 1tudy, Medicare recipients cited lack of knowledge of theeed for immunization and the belief that the vaccine itselfight cause disease as reasons for avoiding influenza vac-
ine.25 Demand may also wane when the influenza season iserceived to be of “mild” severity, while demand mayncrease in seasons where influenza is perceived to be se-ere or occurs early.7 This applies to healthcare workers asell. The CDC recommends that all healthcare providersbtain yearly vaccinations. By so doing, healthcare provid-rs set an example for their patients, while protecting notnly their own health but also that of their patients.
Efforts should also be directed at following the CDC’secommendations to make use of the entire vaccinationeason (October into January and beyond) and take advan-age of all opportunities to vaccinate patients, which wouldurther bolster demand and ensure supply.3 Typically, de-and is high in the fall and then subsides. The reason
nfluenza vaccine ideally is administered in the fall is torotect against potential early influenza seasons. However,nfluenza activity peaked in February for 45% of the seasonsuring the period 1976-2006.3 In only 16% of the seasonsid influenza disease peak before January, and in someeasons disease activity peaked as late as April or May.hus, in the great majority of years, influenza vaccination
nto January and beyond is beneficial. The CDC has urged
hat healthcare providers make the influenza vaccine avail- oble throughout the entire vaccination season.3 This shouldncrease demand beyond the traditional fall immunizationime frame, and ensure that vaccines do not remain unusedhen they can still confer benefit. To take advantage of
very opportunity, healthcare workers are advised to offerhe vaccine during routine healthcare visits or during hos-italization. Although physician offices and clinics willikely remain the primary sites of vaccination, the CDC alsoupports immunizing patients in nontraditional settings, in-luding the workplace, retail stores, and senior citizenenters.3
HAT THIS MEANS FOR THE PROVIDERealthcare providers are in a unique position to strengthenemand by educating their patients about the serious con-equences of influenza and the benefits of immunization,nd by making the vaccine available from October intoanuary and beyond. Providers can play a key role in en-ouraging and facilitating patients’ receipt of routine annualnfluenza immunizations. In following this approach, pro-iders will not only be providing an important service toheir patients but also will be minimizing potential risks tohemselves.26
Healthcare providers must decide how much vaccine torder, when to administer, and to whom. At the same time,hey must incur the costs (which have increased) of pur-hasing the vaccine, and of storage, insurance against loss,nd administration. In estimating how many doses to order,hysicians have traditionally reviewed their records fromrevious years to purchase a supply sufficient to cover theirt-risk patients. They have been reluctant to purchase moreaccine than they can use, out of concern that they would beeft with unused (and unreturnable) doses and the financialoss that this entails.7 When supplies run out, physiciansften refer their patients to other locations.27 However,atients may not always avail themselves of these opportu-ities, thus remaining exposed to infection and itsomplications.
A factor that should enter into providers’ calculationsFigure 2) in the present context is the CDC’s recommen-ation that vaccination take place throughout the entirenfluenza vaccination season, beginning in October and con-inuing into January and beyond. Taking advantage of theull season will give providers added flexibility, enablinghem to better deal with the vagaries of the vaccine market.hus, if vaccine doses are delayed or distributed over a
onger period, providers will have more opportunities to useheir entire supply over the course of a longer vaccinationeason.
Providers should continue to administer the vaccinearly, to immunize as many persons as possible beforenfluenza activity begins. Physicians should avail them-elves of all opportunities to vaccinate in December, Janu-ry, and later. Those working in other healthcare settings,uch as public clinics, can schedule vaccine clinics through-
ut the season. In addition to providing a benefit to patients
ittv2
FNvprdmetp
ibpdidsTrmosbue
avinc
SIbptrtttpslataiatd
ATt
f
Center
S26 The American Journal of Medicine, Vol 121, No 7B, July 2008
n the great majority of years, this approach will minimizehe chances of financial loss. Providers should also be awarehat the Centers for Medicare and Medicaid Services raisedaccine-administration payments beginning in the 2005-006 season.
UTURE DEVELOPMENTSew strategies and technologies that affect the influenzaaccine production system at various points are being ex-lored. These may ultimately be beneficial in terms ofeducing production time and ensuring a steady supply. Asiscussed, influenza vaccine preparation takes about 8 to 9onths; vaccine testing and approval at the FDA is an
ssential part of the process. The FDA is considering wayso accelerate the vaccine review and approval process asart of an effort to expedite the production process.27
Numerous alternatives to egg-based vaccine manufactur-ng technology are also being developed.28,29 Although egg-ased technology has been used since the 1950s, and hasroduced billions of safe, efficacious influenza vaccineoses, other newer technologies may prove to be beneficialn shortening the manufacturing process and perhaps easingelivery constraints by allowing the vaccine to be availableooner.30 Just how beneficial remains to be determined.wo technologies in development are cell culture10,17 and
everse genetics.30 In contrast to traditional manufacturingethods, cell culture offers the possibility of faster startup
f vaccine production, although this may represent timeavings of only a few weeks, perhaps even days, at theeginning of the process.17 Reverse genetic technology issed to prepare reference virus strains and is applicable to
Figure 2 Decision matrix. CDC �
ither egg-based or cell culture production.17 This approach a
llows scientists to alter the virus in an effort to produce aaccine that better matches the new strain of influenza andncreases production yield.30 It is worth noting that theseew technologies may prove to be more expensive andonsequently may increase vaccine costs.
UMMARYnfluenza vaccination is the best defense against the mor-idity and mortality associated with influenza, and meetingublic health immunization goals is a top priority. To ensurehat all those who would benefit actually receive the vaccineequires achieving a balance between supply and demand inhe vaccine marketplace. In the past, the focus has been onhe supply side, as persistent supply shortages and distribu-ion delays dominated the news. Today there is ample sup-ly, and those involved in the overall influenza vaccineystem, including government agencies, federal, state, andocal policymakers, vaccine manufacturers and distributors,nd healthcare providers, have a role to play in making surehat demand is sufficient to make optimal use of the avail-ble supply to decrease the substantial health burden ofnfluenza. It will also help to guarantee the continued avail-bility of the influenza vaccine in the future and minimizehe residual risks associated with vaccine production andistribution.
UTHOR DISCLOSUREShe authors who contributed to this article have disclosed
he following industry relationships:Walter A. Orenstein, MD, has received grant support
or clinical trials and research from Merck & Co., Novartis,
s for Disease Control and Prevention.
nd Sanofi Pasteur, Inc.; and serves on 2 data safety mon-

imK
GSmm
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
S27Orenstein and Schaffner Factors Influencing Influenza Vaccine Availability
toring boards for clinical vaccine trials, Encorium (for-erly Dynport) for bioterrorism threats and GlaxoSmith-line for pneumococcal vaccine.William Schaffner, MD, serves as a consultant to
laxoSmithKline, MedImmune, Merck & Co., Novartis,anofi Pasteur, Inc, and Wyeth Pharmaceuticals; and is aember of a data safety evaluation committee for experi-ental vaccines for Merck & Co.
eferences1. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated
with influenza and respiratory syncytial virus in the United States.JAMA. 2003;289:179-186.
2. Thompson WW, Shay DK, Weintraub E, et al. Influenza-associatedhospitalizations in the United States. JAMA. 2004;292:1333-1340.
3. Centers for Disease Control and Prevention (CDC). Prevention andcontrol of influenza: recommendations of the Advisory Committee onImmunization Practices (ACIP), 2007. MMWR Recomm Rep. 2007;56(RR06):1-54.
4. Centers for Disease Control and Prevention (CDC). CDC’s advisorycommittee recommends influenza vaccination for children 6 monthsthrough 18 years of age [press release]. Available at: http://www.cdc.gov/media/pressrel/2008/r080227.htm. Accessed May 29, 2008.
5. Mason D. A vaccine supply update for the US market. Presented at theNational Vaccine Advisory Committee Meeting; Washington, DC: June3, 2003 [PowerPoint slide presentation]. Available at: www.hhs.gov/nvpo/meetings/jun2003/mason-s.ppt. Accessed February 22, 2008.
6. Orenstein WA, Douglas RG, Rodewald LE, Hinman AR. Immuniza-tions in the United States: success, structure, and stress. Health Aff(Millwood). 2005;24:599-610.
7. Layton C, Robinson T, Honeycutt A. Influenza Vaccine Demand: TheChicken and the Egg, Issue Brief, 2005. Prepared for the AssistantSecretary for Planning and Evaluation, US Dept of Health and HumanServices, under Contract No. 100-03-0001 [report]. Research TrianglePark, NC: RTI International. RTI Project No. 0208665.001. Availableat: http://aspe.hhs.gov/pic/fullreports/06/8476-4.doc. Accessed March6, 2008.
8. Rodewald LE, Orenstein WA, Mason DD, Cochi SL. Vaccine supplyproblems: a perspective of the Centers for Disease Control and Pre-vention. Clin Infect Dis. 2006;42 (suppl 3):S104-S110.
9. Centers for Disease Control and Prevention (CDC). Prevention andcontrol of influenza: recommendations of the Advisory Committeeon Immunization Practices (ACIP). MMWR Recomm Rep. 2002;51(RR03):1-31.
0. Danzon PM, Pereira NS, Tejwani SS. Vaccine supply: a cross-nationalperspective. Health Aff (Millwood). 2005;24:706-717.
1. Gerberding JL. US influenza supply and preparations for the future.Testimony before the Committee on Government Reform, US Houseof Representatives; February 10, 2005. Available at: http://www.hhs.gov/asl/testify/t050210b.html. Accessed.
2. Fishbein DB, Fontanesi J, Kopald D, et al. Why do not patients receiveinfluenza vaccine in December and January? Vaccine. 2006;24:798-802.
3. Fiore A. Influenza activity in the United States, February 2007. Presentedat the Advisory Committee on Immunization Practices, October 23, 2007,Atlanta, Georgia. Available at: http://www.cdc.gov/vaccines/recs/acip/
downloads/mtg-slides-Oct07/93-flu.pdf. Accessed May 28, 2008.4. US Department of Health and Human Services. Healthy People 2010influenza immunization goals. Available at: http://www.healthypeople.gov/document/html/objectives/14-29.htm. Accessed March 5, 2008.
5. Coleman M, Sangrujee N, Zhou F, Chu S. Factors affecting USmanufacturers’ decision to produce vaccines. Health Aff (Millwood).2005;24:635-642.
6. Betts RF. Influenza virus. In: Mandell GL, Bennett JE, Dolin R, eds.Mandell, Douglass, and Bennett’s Principles and Practice of Infec-tious Diseases. 4th ed. New York: Churchill Livingstone, 1994:1546-1567.
7. Layton C, Lenfestey N. Influenza Vaccine Manufacturing, Issue Brief,October 2005. Prepared for the Assistant Secretary for Planning andEvaluation, US Dept of Health and Human Services, under ContractNo. 100-03-0001 [report]. Research Triangle Park, NC: RTI Interna-tional. RTI Project No. 0208665.001. Available at: http://aspe.hhs.gov/pic/fullreports/06/8476-2.doc. Accessed March 6, 2008.
8. Bridges CB, Thompson WW, Meltzer MI, et al. Effectiveness andcost-benefit of influenza vaccination of healthy working adults: arandomized controlled trial. JAMA. 2000;284:1655-1663.
9. Bridges CB, Katz JM, Levandowski RA, Cox NJ. Inactivated influenzavaccines. In: Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines. 5thed. Philadelphia: Elsevier, 2008:259-290.
0. Belshe RB, Walker R, Stoddard J, et al. Influenza vaccine-live. In:Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines. 5th ed. Philadel-phia: Elsevier, 2008:291-309.
1. Wallace GS. Vaccine supply update & programmatic implications.Presented at the Advisory Committee on Immunization Practices, Febru-ary 27, 2008; Atlanta [PowerPoint slide presentation]. Available at:http://www.cdc.gov/vaccines/recs/acip/downloads/mtg-slides-feb08/23-vac-supply.pdf. Accessed May 28, 2008.
2. Jones TF, Ingram LA, Craig AS, Schaffner W. Determinants of influ-enza vaccination, 2003-2004: shortages, fallacies and disparities. ClinInfect Dis. 2004;39:1824-1828.
3. Hinman AR, Orenstein WA, Rodewald L. Financing immunizations inthe United States. Clin Infect Dis. 2004;38:1440-1446.
4. Institute of Medicine. Financing Vaccines in the 21st Century: AssuringAccess and Availability. Washington, DC: The National Academies Press,2003. Available at: http://www.iom.edu/?id�14451&redirect�0. Ac-cessed March 5, 2008.
5. Adler GS. Influenza vaccination and self-reported reasons for notreceiving influenza vaccination among Medicare beneficiaries aged�65 years: United States, 1991-2002. MMWR Morb Mortal Wkly Rep.2004;53:1012-1015.
6. Poland GA, Tosh P, Jacobson RM. Requiring influenza vaccination forhealth care workers: seven truths we must accept. Vaccine. 2005;23:2251-2255.
7. National Influenza Vaccine Summit. Minutes of meeting; January24-25, 2006; Atlanta, GA. Available at: http://www.ama-assn.org/ama1/pub/upload/mm/36/summit_minutes.pdf. Accessed March 5,2008.
8. Belshe RB. Translational research on vaccines: influenza as an exam-ple. Clin Pharmacol Ther. 2007;82:745-749.
9. Cox MM. Progress on baculovirus-derived influenza vaccines. CurrOpin Mol Ther. 2008;10:56-61.
0. Abramson JS, Neuzil KM, Tamblyn SE. Annual universal influenza
vaccination: ready or not? Clin Infect Dis. 2006;42:132-135.
S
BDa
UP
ADactocrh
batyii
p
s
M1
0d
upplement issue
arriers to Adult Immunizationavid R. Johnson, MD, MPH,a Kristin L. Nichol, MD, MPH,b Kim Lipczynski, PhDc
Scientific and Medical Affairs, sanofi pasteur Inc., Swiftwater, Pennsylvania, USA; bMedicine Service, VA Medical Center andniversity of Minnesota, Minneapolis, Minnesota, USA; cProject Management, Adelphi Research by Design, Philadelphia,
ennsylvania, USAOittvArprria©
E-mail address
002-9343/$ -see foi:10.1016/j.amjm
ABSTRACT
ur aim was to provide a better understanding of why many adults fail to receive recommendedmmunizations. Consumers (N � 2,002) and healthcare providers (N � 200) completed structuredelephone interviews concerning their attitudes and knowledge about adult vaccines and factors affectingheir vaccination decisions. Self-reported immunization rates for tetanus, influenza, and pneumococcalaccines (which were emphasized in the surveys) were lower than goal rates set by national guidelines.mong the most common reasons consumers gave for not receiving immunizations were lack of physician
ecommendations and mistaken assumptions (e.g., healthy people do not need immunizations). Healthcareroviders tended to cite concerns such as side effects, fear of needles, and lack of insurance coverage aseasons consumers forego vaccination. Providers also cited practice issues, such as lack of an effectiveeminder system, as barriers to increasing adult immunization rates. We conclude that a better understand-ng of why adults do not get vaccinated is important for efforts to increase immunization rates in this broadge group. 2008 Elsevier Inc. All rights reserved. • The American Journal of Medicine (2008) 121, S28 –S35
KEYWORDS: adult immunization; barriers; consumer; provider surveys
yir5yprf1
nasea
MTsTf
t the beginning of the new millennium, the Centers forisease Control and Prevention (CDC) listed immunization
s 1 of the top 10 public health achievements of the 20thentury.1 The Advisory Committee on Immunization Prac-ices (ACIP) of the CDC, along with other professionalrganizations, recommends immunization schedules forhildren and adolescents2 and for adults3 and updates themegularly. The recommendations are available to bothealthcare professionals and the general public.
Although the US childhood immunization program haseen very successful, the same level of success has not beenchieved in adults. For example, annual influenza vaccina-ion has long been recommended for everyone aged �65ears and for any adult with certain chronic conditions. Yetn a recent year in which vaccine availability was not anssue, only 65% of noninstitutionalized adults aged �65
Adelphi Research by Design was supported by a grant from sanofiasteur Inc. to conduct this research.
Statement of author disclosure: Please see the Author Disclosuresection at the end of this article.
Requests for reprints should be addressed to David R. Johnson, MD,PH, Sanofi Pasteur Inc., One Discovery Drive, Swiftwater, Pennsylvania
8017.
t: [email protected].ront matter © 2008 Elsevier Inc. All rights reserved.ed.2008.05.005
ears and 30% of younger high-risk adults reported receiv-ng influenza vaccine.4 Pneumococcal vaccination also isecommended in these populations, but in the same year just7% of noninstitutionalized men and women aged �65ears and 17% of younger high-risk adults received theneumococcal vaccine.4 In 1999, the last year that the CDCeported rates for tetanus vaccination in adults, rates rangedrom 36% in females aged �65 years to 71% in males aged8 to 49 years.5
To learn why adults do not receive recommended immu-izations, we conducted surveys of �2,000 adult consumersnd 200 healthcare professionals in the United States. Theurveys focused on general vaccination attitudes and knowl-dge of 3 specific vaccines recommended for routine use indults: tetanus, influenza, and pneumococcal vaccines.
ETHODShe surveys were designed and conducted by Adelphi Re-earch by Design, a healthcare marketing research firm.here were 2 distinct populations and survey instruments, 1
or healthcare professionals and 1 for other people (hereaf-
er called “consumers”). Structured telephone interviews
ub
cmoctfmdwddpiawcp
rprpgassdsb
ntCecwpn
dilehSl
R
CPtw1
1pw1
emtdmss
paAcot
dstt
VMtpte8CpvwC(t5p
vbncttn
kwsttm
S29Johnson et al Barriers to Adult Immunization
sing these survey instruments took place between Septem-er 15, 2006 and October 15, 2006.
Consumers were contacted by random digit dialing. Thealler asked to speak to the person aged �19 years with theost recent birthday. The respondent was given the option
f conducting the interview in Spanish. The response rate,alculated as the percentage of those contacted who agreedo participate, was 3.1%, resulting in a population of 2,002or the consumer study. The survey, which lasted approxi-ately 25 minutes, solicited information about the respon-
ent’s personal immunization history, barriers or reasonshy the respondent did not receive vaccines, the respon-ent’s relationship with healthcare providers, and personalemographics. Questions about personal immunization em-hasized 3 vaccines recommended for all adults or for thosen particular age groups: tetanus vaccine, which should bedministered routinely every 10 years; influenza vaccine,hich is recommended annually for those �50 years or in
ertain high-risk groups; and pneumococcal vaccine, foreople �65 years or in certain high-risk groups.3
In addition, 200 healthcare providers were randomlyecruited from a national database of �16,000 primary careractices. They were contacted by e-mail or fax, and theesponse rate was 3.5%. This population consisted of 100rimary care physicians (50 internists, 50 family physicians/eneral practitioners), 34 registered nurses, 33 physicianssistants, and 33 nurse practitioners. They completed atructured telephone interview lasting about 45 minutes thatolicited information about their practice, their recommen-ations for adult patients regarding vaccines (again empha-izing tetanus, influenza, and pneumococcal vaccines), andarriers to vaccination.
To ensure that the consumer survey results reflected aationally representative sample, iterative proportional fit-ing was used to weight the consumer data to match USensus Bureau data for 2000 on age, ethnicity, sex, income,ducation, and region of the continental United States. Be-ause differences between weighted and unweighted dataere minimal, unweighted consumer survey data are re-orted in this article. Data from healthcare providers wereot weighted.
Statistical significance was determined by the indepen-ent t-test for means (assuming equal variances) and thendependent Z-test for proportions. At the 95% confidenceevel, calculated using a standard formula, the margin ofrror for the consumer survey was �2.2%. The smallerealthcare provider sample had a margin of error of �9.8%.ignificant differences are indicated at the 95% confidence
evel (2-tailed P �0.05).
ESULTS
onsumer Surveyopulation Characteristics. The consumer survey popula-
ion was almost equally divided between men (48%) andomen (52%). Age distribution was 17% aged 19 to 34,
6% aged 35 to 44, 20% aged 45 to 54, 20% aged 55 to 64, t5% aged 65 to 74, and 13% aged �75. Of the 2,002ersons in the consumer survey, 74% were non-Hispanichite, 7% were non-Hispanic black, 9% were Hispanic and0% were other or gave no report.
Most respondents (82%) rated their health as good-to-xcellent, but 20% reported having a serious or chronicedical condition. The most common conditions men-
ioned were obesity (12%), diabetes mellitus (12%), heartisease (10%), and chronic lung disease (9%). In the 12onths before the survey, 20% of respondents had not
een a physician for a well-care visit and 29% had had aingle routine care visit; 46% had not had a sick visit.
About half (48%) of respondents worked full-time orart-time, and 19% felt that their job put them at above-verage risk of injury (e.g., construction, law enforcement).pproximately 1 of 4 consumers (24%) said their job in-
reased their risk of acquiring a vaccine-preventable illnessr brought them into contact with people who were ex-remely susceptible to illness.
Household income was �$35,000 for 30% of respon-ents and �$75,000 for 21%. Most consumers (84%) hadome type of health insurance; 25% received their coveragehrough Medicare, 4% through Medicaid, and 4% throughhe military or the Veterans Administration.
accine Awareness and Personal Vaccination History.ost consumers were aware of the influenza (96%) and
etanus (90%) vaccines. Only 65% were aware of theneumococcal vaccine, although awareness was higher inhe groups for whom this vaccine is recommended. Forxample, 85% (95% confidence interval [CI], 82% to8%) of respondents aged �65 years versus 50% (95%I, 46% to 53%) of those �50 years knew about theneumococcal vaccine (P �0.001). Awareness of thisaccine was 79% (95% CI, 75% to 83%) among peopleith chronic health conditions compared with 62% (95%I, 59% to 64%) among those without chronic conditions
P �0.001), and 67% (95% CI, 61% to 73%) amonghose with increased occupational risk compared with3% (95% CI, 49% to 58%) among those without occu-ational risks (P �0.001).
Although most consumers were aware of the tetanusaccine, only 36% knew that adults should receive aooster every 10 years. Just 27% knew when they wereext due for a tetanus immunization. Among the 533onsumers who had received a pneumococcal vaccina-ion, 147 were aged �65 years and had a chronic condi-ion, and 46% of these individuals were not aware theyeeded a booster.
Most consumers (82%) believed that it is important toeep up-to-date with immunizations, yet 34% said theyere skeptical about receiving any type of vaccine. The
kepticism may reflect misunderstandings about vaccina-ion; for example, 26% of respondents who were aware ofhe influenza vaccine but did not receive it as recom-ended were concerned about getting the disease from
he vaccine.

ethmwasg
R(wvswiw5Akazf
w6wta
vmwoisdt
fratfdr$aiAmv
HA2
npl
RvgivnucpC
atltiim6ti
smsMaOez
Psc(pami
oamktptr(4c
S30 The American Journal of Medicine, Vol 121, No 7B, July 2008
Of the 3 vaccines surveyed, the 1 that the most consum-rs (70%) recalled having received as an adult was theetanus vaccine. In all, 62% of respondents reported havingad an influenza vaccination as an adult. Rates for pneu-ococcal vaccination for those in recommended groupsere low: 61% among people aged �65 years and 52%
mong those with chronic illness. For all 3 vaccines, theelf-reported rates of vaccination were higher among at-riskroups for whom each vaccine is recommended (Figure 1).
easons for not Receiving Vaccines. Most consumers79% to 85%, depending on the vaccine) indicated that theyere likely to receive a vaccination if their healthcare pro-ider recommended it. However, when given a list of pos-ible reasons for not being immunized, 51% of consumersho were aware of the tetanus vaccine but had not received
t, chose: “Doctor hasn’t told me I need it.” This explanationas selected by 38% with regard to the influenza vaccine and7% with regard to the pneumococcal vaccine (Figure 2).mong consumers who knew of the vaccines, “Don’tnow when to get it” was cited as a reason for not havingvaccination by 37% of consumers for tetanus immuni-
ation, by 21% for influenza immunization, and by 26%or pneumococcal immunization.
The most consistent reason for not receiving a vaccineas the belief that a healthy person does not need it (60% or1%, depending on the vaccine). Concern about side effectsas cited by 22% of consumers as a reason for avoiding
etanus immunization, by 43% for influenza immunization,nd by 40% for pneumococcal immunization.
Other frequently selected explanations for not receivingaccinations were specific to the particular vaccine. Theost common reason for not having a recent tetanus vaccineas the belief that it was necessary only when an injuryccurred, an explanation chosen by 74% of respondents. Fornfluenza vaccination, 59% cited a short supply whichhould be used by others who need it more—despite widelyisseminated predictions of ample vaccine supply at theime of the survey.
Financial concerns were not a deterrent to immunizationor most consumers. “No, this is not a reason” was theesponse to “Costs too much” by 80% to 82% of consumerss an explanation for not having each of the 3 immuniza-ions. Only 14% to 17% of respondents stated that theyailed to receive 1 of the 3 vaccines because their insuranceid not cover it. When asked whether they would probablyeceive a vaccine if their out-of-pocket costs were $25 to30, 72% of consumers said they were willing to pay thatmount of money for the tetanus vaccine, 67% for thenfluenza vaccine, and 76% for the pneumococcal vaccine.n immunization costing $25 to $30 that could preventissed days from work or hospitalization would be highly
aluable, according to 83% of consumers.
ealthcare Providers Surveymong the 100 physician practices included in the survey,
3% were urban, 57% suburban, and 20% rural. For the 100 aonphysician providers (a mix of physician assistants, nurseractitioners, and registered nurses [PA/NP/RN]), the practiceocations were 25% urban, 38% suburban, and 37% rural.
ecommendations to Patients. Almost all healthcare pro-iders (90% of physicians and 94% of the PA/NP/RNroup) believed that all of their adult patients should bemmunized. They also claimed to discuss recommendedaccinations with their adult patients, especially during an-ual exams or well-care office visits. Physicians in partic-lar were less likely to discuss immunizations during acute-are or sick visits, with only 29% (95% CI, 20% to 38%) ofhysicians reporting this practice compared with 42% (95%I, 32% to 52%) of the PA/NP/RN group (P � 0.03).
When asked about specific vaccines, 85% of physiciansnd 88% of the PA/NP/RN group said they recommend theetanus vaccine to all adults. Recommendations were muchess frequent for influenza and pneumococcal immuniza-ions, as shown in Table 1. The responses in this tablendicate that healthcare providers are not routinely follow-ng recommended immunization practices for adults. Someay not even be aware of the recommendations, as only
0% of physicians and 56% of the PA/NP/RN group statedhat the official guidelines were their personal sources ofnformation about adult immunizations.
Most healthcare professionals indicated that they haveystems in place to ensure that patients receive recom-ended vaccines. These systems include an immunization
heet or reminder in patient charts and office protocols.any practices post fliers in waiting rooms and exam rooms
nd instruct staff to remind patients about immunizations.nly �33% of providers had ever conducted an objective
valuation, such as a chart review, of their adult immuni-ation rates.
erceived Barriers to Immunization. Healthcare profes-ionals were presented reasons why patients might not re-eive tetanus, influenza, and pneumococcal immunizationsTable 2). According to healthcare providers, failure ofatients to come for regular well-care visits and lack ofn effective reminder system were among the more com-on reasons that adults do not receive recommended
mmunizations.Healthcare providers also indicated that patients’ dislike
f needles, fear of adverse effects, and lack of knowledgebout disease prevention were frequently responsible forissed immunizations. Yet �50% of the providers ac-
nowledged that they do not always inform patients abouthe consequences of missing vaccinations. The PA/NP/RNroviders were significantly more likely than physicianso always talk to patients about the consequences of noteceiving recommended vaccines: 56% versus 34%P �0.001), 61% versus 47% (P � 0.02), and 59% versus0% (P � 0.004) for tetanus, influenza, and pneumococ-al vaccines, respectively.
Additionally, healthcare providers frequently cited in-
dequate insurance coverage and, to a lesser extent, con-
S31Johnson et al Barriers to Adult Immunization
Figure 1 (A-C) Immunization rates reported in consumer survey, by riskfactor (Vaccinations ever received as adults, as reported by 2,002 consum-
�
ers). P �0.05 vs. nonrisk groups.
cfp
pt
eived
S32 The American Journal of Medicine, Vol 121, No 7B, July 2008
ern about the cost of vaccines as reasons adults mightorgo immunizations. Depending on the vaccine and the
Figure 2 (A-C) Reasons consumers acknowtype. Scale shown is the percent of consumeagreed that this is a reason they have not rec
rofessional group, between 61% and 79% of healthcare t
rofessionals thought their adult patients would be likelyo receive a vaccine if their out-of-pocket costs were $25
for not receiving immunizations, by vaccinewere aware of the immunization and who
it or will not receive it.
ledgers who
o $30.

DOibeaSttpIir
necaadnt
ttnlmhwvcio
irtog
rioiHip
bvacpcftd
pMvteitg
P
AAACDHCCWRACSC
S33Johnson et al Barriers to Adult Immunization
ISCUSSIONur surveys confirmed that many adults do not receive
mmunizations as recommended. This is not the first timearriers to adult immunization have been examined. How-ver, many studies are a decade old,6-8 and attitudes, beliefs,nd knowledge about immunization may have changed.ome previous studies were limited to particular popula-
ions, such as the elderly6,9,10 or economically disadvan-aged,11 whereas the sample in our consumer survey coverseople in all economic groups and the entire adult age span.n general, our study confirms findings from previous stud-es and adds to our understanding about why adults do noteceive immunizations.
False assumptions, such as a belief that healthy people doot need immunizations, are important reasons that consum-rs fail to receive vaccinations. Efforts to inform and edu-ate the public occasionally misfire. For example, publicitybout past influenza vaccine shortages appears to have hadlasting negative effect. In our survey, consumers cited theesire to save a vaccine in short supply for others whoeeded it as a reason to skip influenza immunization, al-hough there was no shortage at the time.
The Medicare Current Beneficiary Survey has consis-ently found that people fail to receive influenza vaccina-ions because they do not know they should be immu-ized.12 Most of the consumers in our study said they wereikely to follow their physician’s recommendations for im-unization, echoing earlier research.7 Both groups of
ealthcare providers in our study acknowledged that theyere more likely to discuss immunization during well-careisits than during sick visits. Similarly, Szilagyi and asso-iates13 found that the most significant practice barrier tommunization was other urgent concerns that dominated the
Table 1 Healthcare provider recommendations for influenza an
atient Type
Influenza Va
Physicians(n � 100)
ll adults 39%ged �50 yr 28*ged �65 yr 37hronic lung disease 45iabetes mellitus 31eart disease 20hronic liver disease 22hronic kidney disease 22eak immune system 17adiation/chemotherapy 14splenia —omplications or risk from other illness 25moker —lose contact with someone at high risk 24
NP � nurse practitioner; PA � physician assistant; RN � registered*Significantly greater (P �0.05) than other provider group.
ffice visit. However, a mild acute illness, even a febrile s
llness, is not a contraindication for immunization.14 Inecognition of this missed opportunity, hospitals have es-ablished standard operating procedures and protocols toffer vaccinations to inpatients and those treated in emer-ency rooms.15,16
A comprehensive review of the literature found patienteminder/recall systems to be 1 of the strongest ways toncrease community demand for immunizations.17 A reviewf 41 studies looking exclusively at patient reminder/recallnterventions also found this to be an effective strategy.18
owever, �70% of the providers in our survey noted theneffectiveness of their reminder systems for tetanus andneumococcal immunizations.
Although responses from our 2 different surveys shoulde compared with caution, it appears that healthcare pro-iders and consumers do not always agree on reasons thatdults go unvaccinated, especially those reasons related toonsumer attitudes and beliefs. For example, �66% ofroviders thought that consumers avoid vaccinations be-ause of concern about side effects, dislike of needles, orear that the vaccine would make them ill. Consumers men-ioned these concerns far less frequently as reasons that theyid not receive immunizations.
Economic factors were another area where providers’erception of barriers differed from consumers’ concerns.ost consumer respondents had insurance coverage for
accinations, and only 13% to 15% stated that immuniza-ions cost too much. But 50% to 66% of healthcare provid-rs thought that monetary concerns were a major barrier tommunization. Some providers may not have been awarehat immunizations are covered under Medicare. The pro-ram has been paying for pneumococcal immunization
umococcal vaccinations by patient type
Pneumococcal Vaccine
PA/NP/RNs(n � 100)
Physicians(n � 100)
PA/NP/RNs(n � 100)
59%* — —15 4% 18%*28 65 5540 68 5525 44* 2611 29* 1216 27 2012 25 1720 24 299 17 10
— 27* 817 28 23— 13 1122 11 10
d pne
ccine
nurse.
ince 1981 and for influenza immunization since 1993.19

wtwm
icsmiTbdn
k
sEmcivi
fv
SFhih
E
PvCwLpNFINrUCvTNrVTCBcNdTCmTVNw
S34 The American Journal of Medicine, Vol 121, No 7B, July 2008
Lack of knowledge on the part of healthcare providersas a surprising finding in this study. Almost 50% of
hose surveyed did not rely on the CDC/ACIP guidelines,hich are widely available in both print and electronicedia.Our surveys have several limitations. The response (will-
ngness to participate) rates in both surveys were low, whichould bias the findings. The healthcare provider sample wasmall. Although the consumer sample was large, it wasostly non-Hispanic whites. Studies have found differences
n barriers to immunization among other ethnic groups.20,21
he immunization history in the consumer survey wasased completely on patient recall. Finally, survey respon-ents often underreport behaviors that may be perceivedegatively and overestimate behaviors perceived as good.
Although patient and provider education is needed to fill
Table 2 Healthcare providers’ explanations for why adults may
xplanation
Tetanus Vaccine
Physicians(n � 100)
PA/NP(n � 1
atient does not make regular wellisits
85% 80%
oncern about side effects, that itill cause illness
65 68
ack of knowledge about illnessrevention
73 76
o effective reminder system 73 77ear of needles 71 68nadequate insurance coverage 66 71ot going to same physicianegularly
65 73
naware of vaccination schedule 64 70onfused about recommendedaccination schedule
63 61
hink healthy people don’t need it 49 55ot receiving physician’secommendation
59 55
accine too expensive 51 46hink won’t work if sick 38 33ould worsen current conditions 31 28elieve lifetime protection fromhildhood vaccines
49 45
ot enough time in office visit toiscuss it
40 30
hink it’s ineffective 24 22ould interact with currentedications
25 29
hink only for elderly — —accine shortage — —eed only when injury or openound
80 82
NP � nurse practitioner; PA � physician assistant; RN � registered*Percent of providers who agreed when presented a list of reasons a†Significantly greater (P �0.05) than other provider group.
nowledge gaps and misunderstandings, knowledge by it- l
elf is not sufficient to improve immunization practices.22
fforts should be made to make administration of recom-ended immunizations a routine part of all healthcare en-
ounters. Based on the evidence in 118 studies involving 17ntervention strategies, the Task Force on Community Pre-entive Services recommended a variety of strategies toncrease immunization rates in adults.23
The National Vaccine Advisory Committee has calledor identification and minimization of barriers to receivingaccines.24
UMMARYindings from the consumer and provider surveys reportedere may help distinguish the real reasons adults foregommunizations from the presumed barriers. This knowledgeas the potential to further inform and refine policies estab-
ceive tetanus, influenza, and pneumococcal vaccines*
Influenza Vaccine Pneumococcal Vaccine
Physicians(n � 100)
PA/NP/RN(n � 100)
Physicians(n � 100)
PA/NP/RN(n � 100)
83% 73% 88%† 77%
87 87 65 77
62 75† 73 83
62 63 71 7271 68 69 6761 67 68 7959 65 62 71
50 56 70 6850 45 68 62
66 63 68 6853 54 58 60
52 43 62 5458 58 46 5258 53 37 4328 29 35 31
37 27 39 30
48 46 31 3026 33 21 37†
56 57 68 7387 83 — —— — — —
ients might not receive the vaccine.
not re
/RN00)
nurse.dult pat
ished to increase adult immunization rates.

ATt
o
SR
tNf
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
S35Johnson et al Barriers to Adult Immunization
UTHOR DISCLOSUREShe authors who contributed to this article have disclosed
he following industry relationships:David R. Johnson, MD, MPH, is a full-time employee
f Sanofi Pasteur Inc.Kim Lipczynski, PhD, has served as a consultant to
anofi Pasteur Inc.; and is a full-time employee of Adelphiesearch by Design.
Kristin L. Nichol, MD, MPH, has served as a consul-ant to CSL Biotherapies, GlaxoSmithKline, MedImmune,ovartis, and Sanofi Pasteur Inc; and has received research
unding from GlaxoSmithKline and Sanofi Pasteur Inc.
eferences1. Centers for Disease Control and Prevention (CDC). Ten great public
health achievements—United States, 1900-1999. MMWR Morb Mor-tal Wkly Rep. 1999;48(RR12):241-243.
2. Centers for Disease Control and Prevention (CDC). Recommendedimmunization schedules for persons aged 0-18 years—United States,2007. MMWR Morb Mortal Wkly Rep. 2007;55(RR51):Q1-Q4.
3. Centers for Disease Control and Prevention (CDC). Recommendedadult immunization schedule—United States, October 2006–Septem-ber 2007. MMWR Morb Mortal Wkly Rep. 2006;55:Q1-Q4.
4. US Department of Health and Human Services. Healthy People 2010[CDC Web site]. Available at: http://wonder.cdc.gov/data2010/obj.htm. Accessed July 23, 2007.
5. Centers for Disease Control and Prevention (CDC). Statistics andsurveillance [CDC Web site]. Available at: http://www.cdc.gov/vaccines/stats-surv/downloads/general-99.pdf. Accessed July 23, 2007.
6. Centers for Disease Control and Prevention (CDC). Reasons reportedby Medicare beneficiaries for not receiving influenza and pneumococ-cal vaccinations—United States, 1996. MMWR Morb Mortal WklyRep. 1999;48:886-890.
7. Nichol KL, MacDonald R, Hauge M. Factors associated with influenzaand pneumococcal vaccination behavior among high-risk adults. J GenIntern Med. 1996;11:673-677.
8. Mieczkowski TA, Wilson SA. Adult pneumococcal vaccination: areview of physician and patient barriers. Vaccine. 2002;20:1383-1392.
9. Santibanez TA, Nowalk MP, Zimmerman RK, et al. Knowledge andbeliefs about influenza, pneumococcal disease, and immunizationsamong older people. J Am Geriatr Soc. 2002;50:1711-1716.
0. Zimmerman RK, Santibanez TA, Janosky JE, et al. What affectsinfluenza vaccination rates among older patients? An analysis frominner-city, suburban, rural, and Veterans Affairs practices. Am J Med.
2003;114:31-38.1. Zimmerman RK, Nowalk MP, Raymund M, et al. Tailored interven-tions to increase influenza vaccination in neighborhood health centersserving the disadvantaged. Am J Public Health. 2003;93:1699-1705.
2. Adler GS. Influenza vaccination and self-reported reasons for notreceiving influenza vaccination among Medicare beneficiaries aged�65 years—United States, 1991-2002. MMWR Morb Mortal WklyRep. 2004;53:1012-1015.
3. Szilagyi PG, Shone LP, Barth R, et al. Physician practices and attitudesregarding adult immunization. Prev Med. 2005;40:152-161.
4. Centers for Disease Control and Prevention (CDC). Adult immunizationprograms in nontraditional settings: quality standards and guidance forprogram evaluation. A report of the National Vaccine Advisory Commit-tee. MMWR Morb Mortal Wkly Rep. 2000;49(RR01):1-13.
5. Middleton DB, Fox DE, Nowalk MP, et al. Overcoming barriers toestablishing an inpatient vaccination program for pneumococcus usingstanding orders. Infect Control Hosp Epidemiol. 2005;26:874-881.
6. Rimple D, Weiss SJ, Brett M, Ernst AA. An emergency department-based vaccination program: overcoming the barriers for adults at highrisk for vaccine-preventable diseases. Acad Emerg Med. 2006;13:922-930.
7. Shefer A, Briss P, Rodewald L, et al. Improving immunization cov-erage rates: an evidence-based review of the literature. Epidemiol Rev.1999;21:96-142.
8. Szilagyi PG, Bordley C, Vann JC, et al. Effect of patient reminder/recall interventions on immunization rates: a review. JAMA. 2000;284:1820-1827.
9. Centers for Disease Control and Prevention (CDC). Missed oppor-tunities for pneumococcal and influenza vaccination of Medicarepneumonia inpatients—12 Western states, 1995. MMWR. 1997;46:919-923.
0. Hebert PL, Frick KD, Kane RL, McBean AM. The causes of racial andethnic differences in influenza vaccination rates among elderly Medi-care beneficiaries. Health Serv Res. 2005;40:517-537.
1. Chen JY, Fox SA, Cantrell CH, et al. Health disparities and preven-tion: racial/ethnic barriers to flu vaccinations. J Community Health.2007;32:5-20.
2. Prislin R, Sawyer MH, De Guire M, et al. Missed opportunities toimmunize: psychosocial and practice correlates. Am J Prev Med.2002;22:165-169.
3. Centers for Disease Control and Prevention (CDC). Vaccine-prevent-able diseases: improving vaccination coverage in children, adoles-cents, and adults: a report on recommendations of the Task Force onCommunity Preventive Services. MMWR Morb Mortal Wkly Rep.1999;48(RR08):1-16.
4. Poland GA, Shefer AM, McCauley M, et al, for the National VaccineAdvisory Committee, Ad Hoc Working Group for the Development ofStandards for Adult Immunization Practices. Standards for adult im-
munization practices. Am J Prev Med. 2003;25:144-150.