head trauma - miami county ems become non--reactive or sluggish.reactive or sluggish. • central...
TRANSCRIPT
1
HEAD TRAUMAHEAD TRAUMA
2
Head and Brain TraumaHead and Brain Trauma
••
~ 4 million head injuries in US per ~ 4 million head injuries in US per year.year.
••
~ 450, 000 require hospitalization.~ 450, 000 require hospitalization.––
Most are minor injuries.Most are minor injuries.
––
Major head injury most common cause Major head injury most common cause of trauma deaths in trauma centers of trauma deaths in trauma centers (>50%).(>50%).
3
••
Leading cause of death and disability Leading cause of death and disability from birth to age 44.from birth to age 44.
••
Cause of death in 25% of trauma Cause of death in 25% of trauma patients.patients.
••
Cause of death in half of fatality Cause of death in half of fatality MVCsMVCs..••
Significant long term disability.Significant long term disability.
••
Prompt recognition and treatment can Prompt recognition and treatment can improve outcome.improve outcome.
Head and Brain Trauma

4
••
Every year, 142,000 Americans are Every year, 142,000 Americans are killed as the result of head injury and killed as the result of head injury and another 50,000 another 50,000 ––
70,000 are severely 70,000 are severely
disabled.disabled.••
Almost 30% of all childhood injury Almost 30% of all childhood injury deaths result from a head injury.deaths result from a head injury.
Head and Brain Trauma

5
Causes of Head InjuryCauses of Head Injury
••
MVC 50%MVC 50%••
Falls 21%Falls 21%
••
Assaults and Violence 12%Assaults and Violence 12%••
Sports and Recreation 10%Sports and Recreation 10%
••
Other 7%Other 7%
6
Head and Brain TraumaHead and Brain Trauma
••
Risk GroupsRisk Groups––
Highest risk, males 15 Highest risk, males 15 --
24 yrs of age.24 yrs of age.
––
Very young children from 6 months to Very young children from 6 months to 2 years of age.2 years of age.
––
Young school age children.Young school age children.––
Elderly.Elderly.
••
As EMS providers, what can we do As EMS providers, what can we do in our communities to reduce the in our communities to reduce the incidence of head injuries?incidence of head injuries?

7
LectureLecture Overview Overview
••
Review the anatomy of skull and brain.Review the anatomy of skull and brain.••
Discuss the pathophysiology of head Discuss the pathophysiology of head injury.injury.
••
Review of specific head injuries.Review of specific head injuries.••
Describe the assessment of head Describe the assessment of head trauma and the head injured patient.trauma and the head injured patient.
••
Outline treatment strategies and Outline treatment strategies and describe the management of head describe the management of head trauma.trauma.

8
Skull Anatomy ReviewSkull Anatomy Review
••
Cranium Cranium ––
Double layer of solid (flat) bone which Double layer of solid (flat) bone which surrounds a spongy middle layer.surrounds a spongy middle layer.
––
Frontal, occipital, temporal, parietal, Frontal, occipital, temporal, parietal, sphenoid, and sphenoid, and ethmoidethmoid
bones form the bones form the
cranium.cranium.
9
••
Noteable Noteable Features of the Cranium:Features of the Cranium:––
Middle Middle meningealmeningeal
artery.artery.
••
Important feature due to potential for injury.Important feature due to potential for injury.••
Lies under temporal bone.Lies under temporal bone.••
Common source of an epidural hematoma secondary to Common source of an epidural hematoma secondary to a blow to the temporal region.a blow to the temporal region.
––
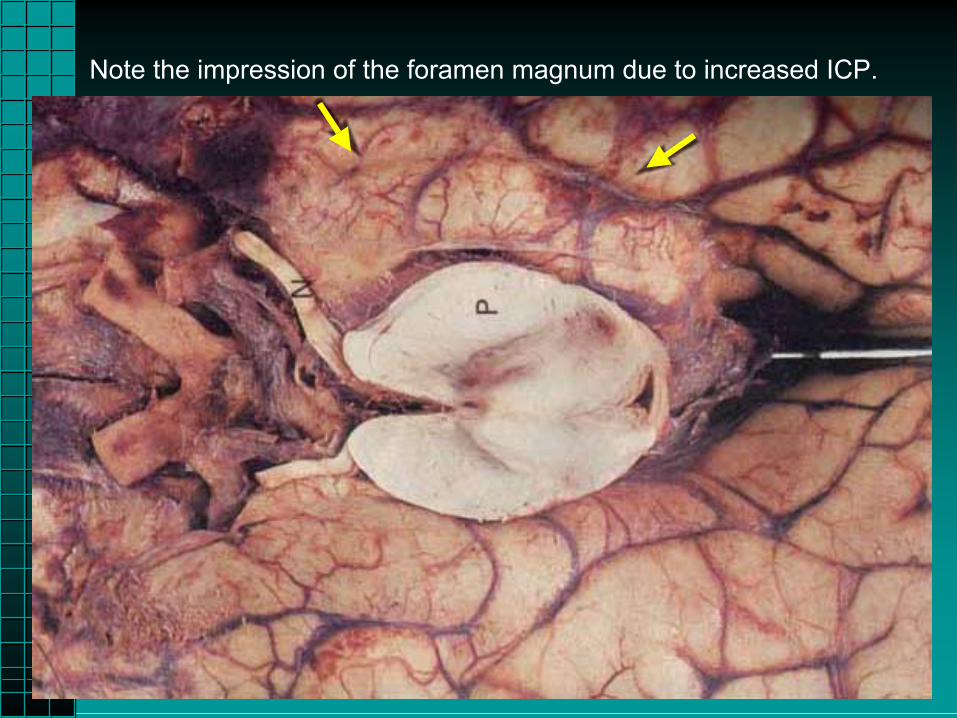
Foramen magnum.Foramen magnum.••
Only opening of significant size in the cranium. (There Only opening of significant size in the cranium. (There are smaller openings for blood vessels, the auditory are smaller openings for blood vessels, the auditory canal, etc.)canal, etc.)
••
As pressure inside the cranial vault increases, pressure As pressure inside the cranial vault increases, pressure is applied to brain tissue as contents are pushed toward is applied to brain tissue as contents are pushed toward the opening.the opening.
Skull Anatomy ReviewSkull Anatomy Review

10
Skull Anatomy

11

12
FontanellesFontanelles
13
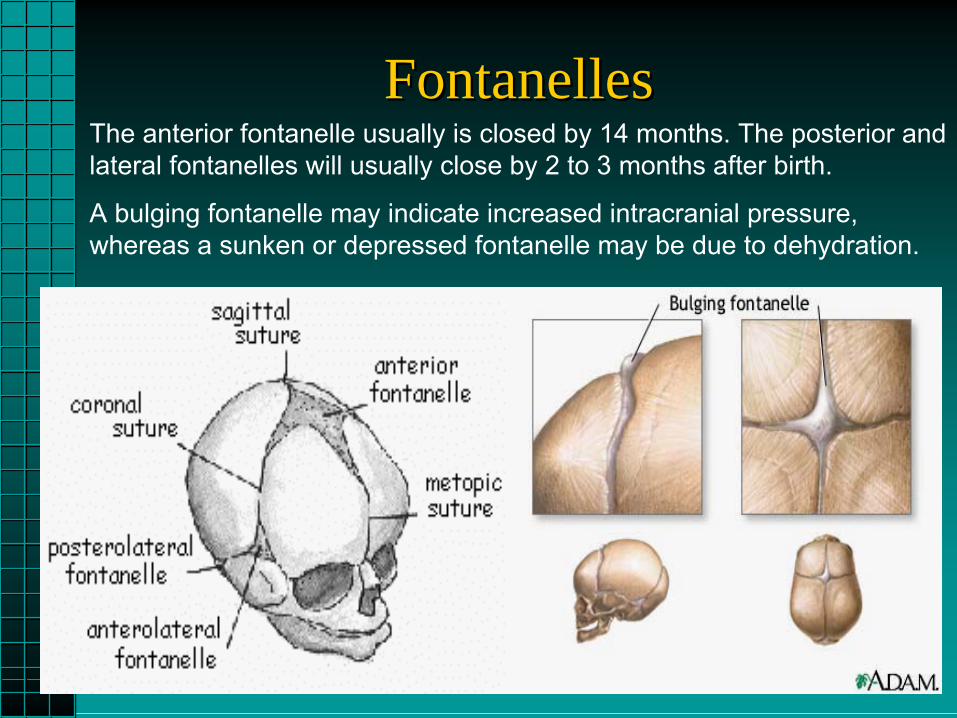
FontanellesFontanellesThe anterior fontanelle usually is closed by 14 months. The posterior and lateral fontanelles will usually close by 2 to 3 months after birth.
A bulging fontanelle may indicate increased intracranial pressure, whereas a sunken or depressed fontanelle may be due to dehydration.

14
Facial BonesFacial BonesEthmoid bone
Lacrimal bone
Nasal bone
Zygomatic bone
Maxilla
Mandible
Vomer
Inferior nasal concha
Palatine

15
AnatomyAnatomy
16
Brain AnatomyBrain Anatomy
••
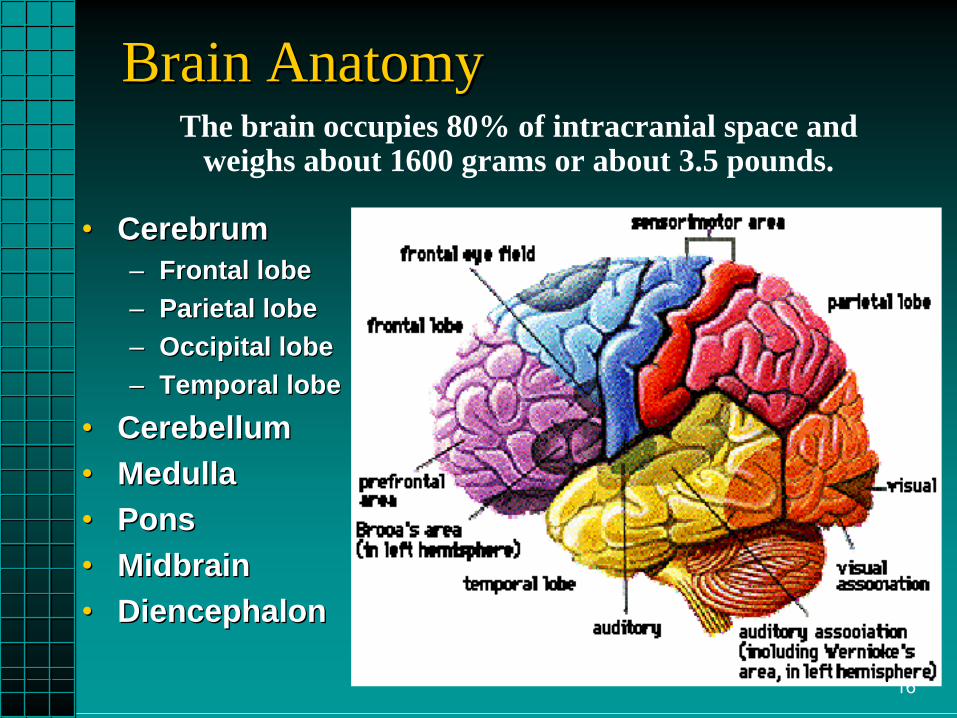
CerebrumCerebrum––
Frontal lobeFrontal lobe––
Parietal lobeParietal lobe––
Occipital lobeOccipital lobe––
Temporal lobeTemporal lobe••
CerebellumCerebellum
••
MedullaMedulla••
PonsPons
••
MidbrainMidbrain••
DiencephalonDiencephalon
The brain occupies 80% of intracranial space andweighs about 1600 grams or about 3.5 pounds.
17
Brain Anatomy ReviewBrain Anatomy Review
••
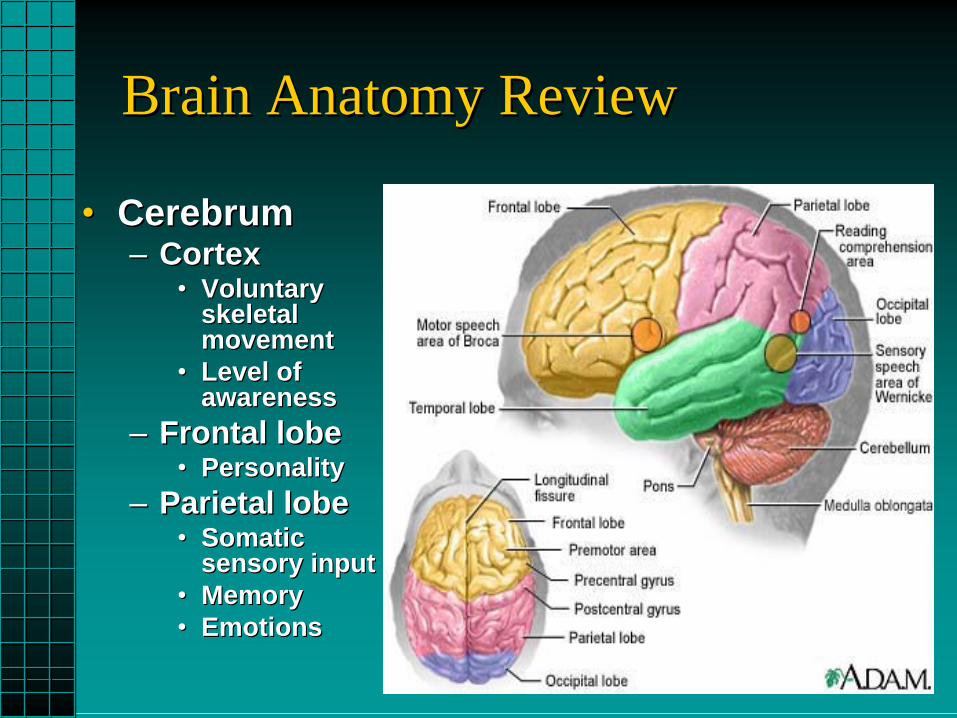
CerebrumCerebrum––
CortexCortex
••
Voluntary Voluntary skeletal skeletal movementmovement
••
Level of Level of awarenessawareness
––
Frontal lobeFrontal lobe••
PersonalityPersonality––
Parietal lobeParietal lobe
••
Somatic Somatic sensory inputsensory input
••
MemoryMemory••
EmotionsEmotions

18
Brain Anatomy ReviewBrain Anatomy Review
••
CerebrumCerebrum––
Temporal lobeTemporal lobe
••
Speech centerSpeech center••
Long term Long term memorymemory
••
TasteTaste••
SmellSmell
––
Occipital lobeOccipital lobe••
Origin of optic Origin of optic nervenerve

19

20
HemoculusHemoculus
21
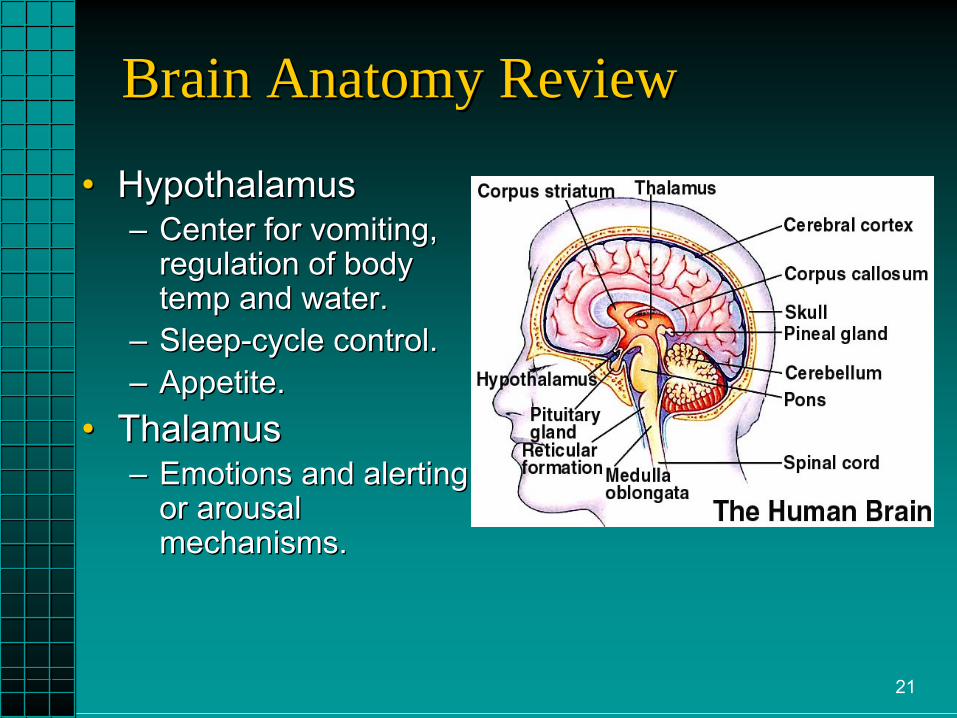
Brain Anatomy ReviewBrain Anatomy Review
••
HypothalamusHypothalamus––
Center for vomiting, Center for vomiting, regulation of body regulation of body temp and water.temp and water.
––
SleepSleep--cycle control.cycle control.––
Appetite.Appetite.
••
ThalamusThalamus––
Emotions and alerting Emotions and alerting or arousal or arousal mechanisms.mechanisms.

22
23
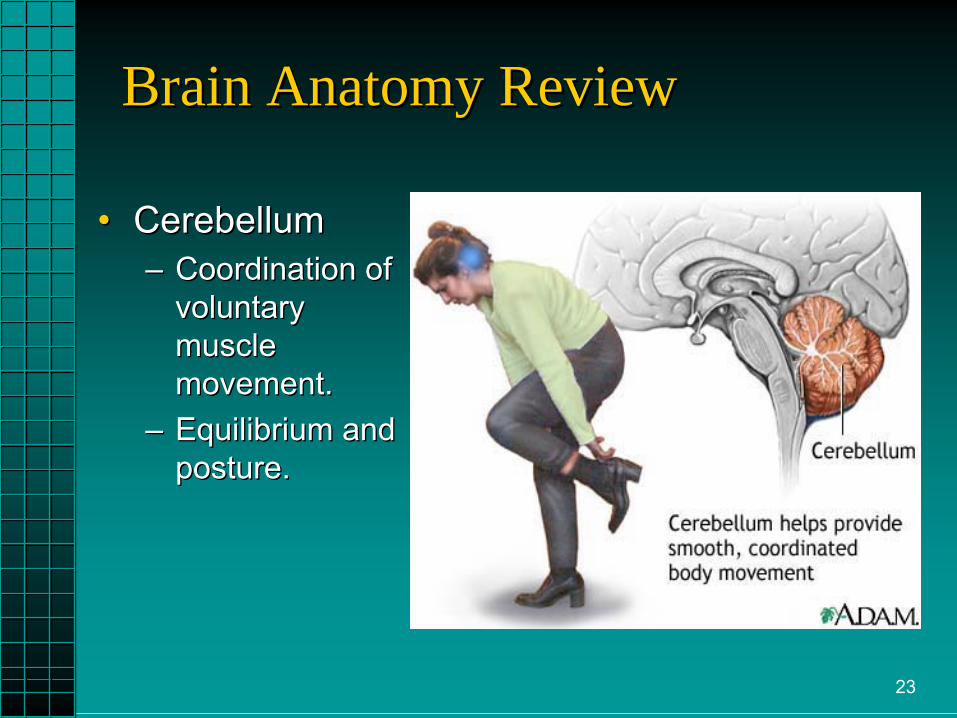
Brain Anatomy ReviewBrain Anatomy Review
••
CerebellumCerebellum––
Coordination of Coordination of voluntary voluntary muscle muscle movement.movement.
––
Equilibrium and Equilibrium and posture.posture.
24
••
Brain Stem:Brain Stem:––
Connects hemispheres, cerebellum and spinal cord.Connects hemispheres, cerebellum and spinal cord.
––
Responsible for vegetative functions and VS.Responsible for vegetative functions and VS.––
Midbrain is the relay point for visual and auditory Midbrain is the relay point for visual and auditory impulses.impulses.
––
Pons Pons is the conduction pathway between brain and is the conduction pathway between brain and other regions of body.other regions of body.
––
Medulla oblongataMedulla oblongata••
cardiac, respiratory, and vasomotor control centers.cardiac, respiratory, and vasomotor control centers.••
control of vomiting and coughing.control of vomiting and coughing.
Brain Anatomy ReviewBrain Anatomy Review

25
26
Brain Anatomy ReviewBrain Anatomy Review
••
Brain Stem:Brain Stem:––
Origin of the 12 Cranial Nerves.Origin of the 12 Cranial Nerves.
––
Reticular Activating System.Reticular Activating System.••
Level of arousal (level of consciousness).Level of arousal (level of consciousness).
––
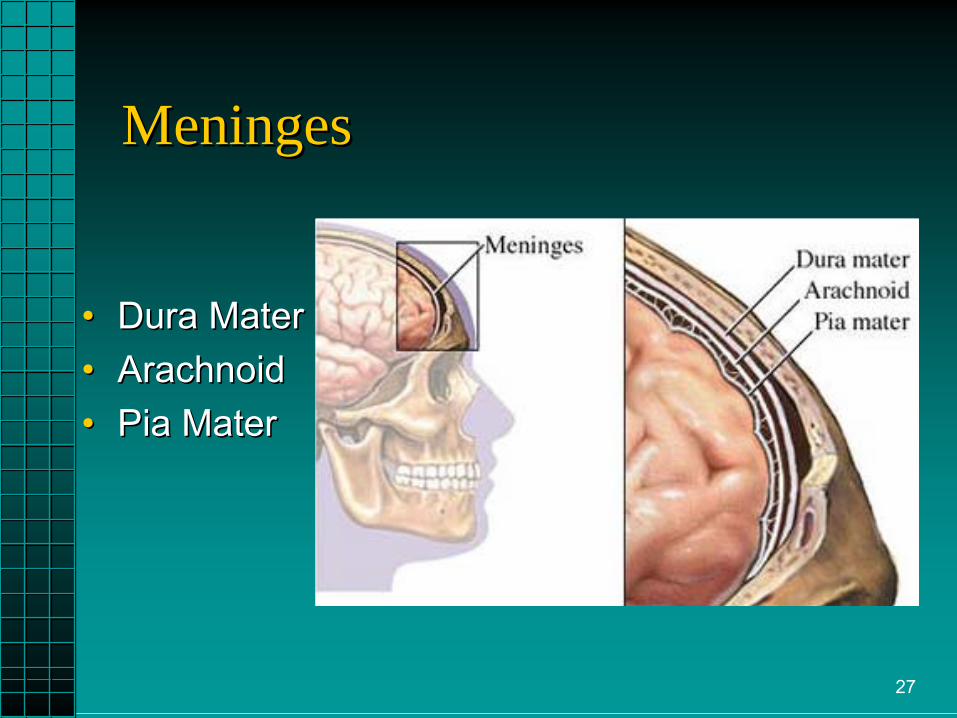
Meninges:Meninges:••
Dura mater. The tough outer layer, separates Dura mater. The tough outer layer, separates cerebellum from cerebral structures, landmark for cerebellum from cerebral structures, landmark for lesions.lesions.
••
Arachnoid. The webArachnoid. The web--like middle layer that contains like middle layer that contains venous vessels that reabsorb CSF.venous vessels that reabsorb CSF.
••
Pia mater. Directly attached to brain tissue.Pia mater. Directly attached to brain tissue.
27
MeningesMeninges
••
Dura MaterDura Mater••
ArachnoidArachnoid
••
Pia MaterPia Mater
28

29

30
31
32

33
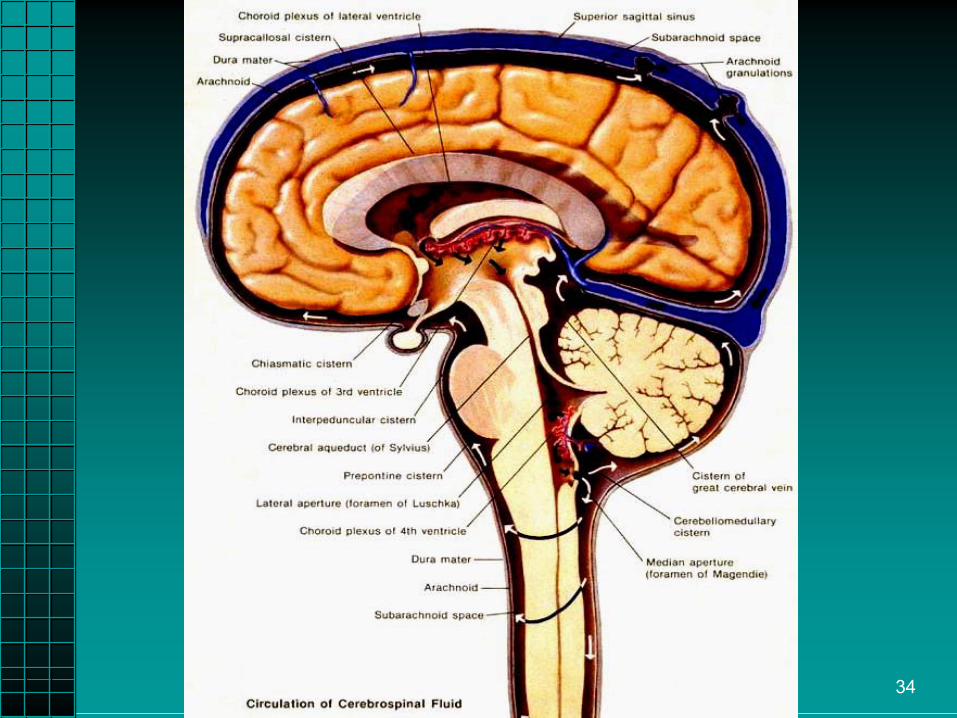
Brain Anatomy ReviewBrain Anatomy Review••
Brain StemBrain Stem––
Cerebral Spinal Fluid (CSF)Cerebral Spinal Fluid (CSF)••
Produced by the cells of the Produced by the cells of the choroidchoroid
plexus.plexus.
••
Clear, colorless, oily liquid.Clear, colorless, oily liquid.••
Circulates through brain and spinal cord.Circulates through brain and spinal cord.
••
Cushions, cleans, and protects.Cushions, cleans, and protects.••
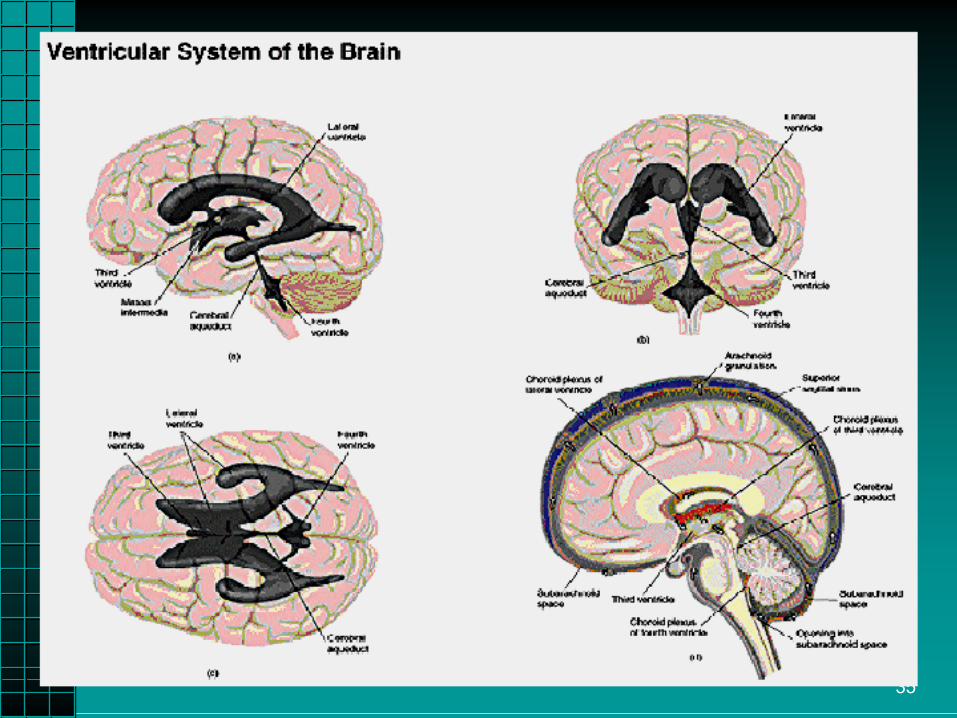
Ventricles:Ventricles:
––
Located in the center of brain.Located in the center of brain.––
Secrete CSF by filtering blood.Secrete CSF by filtering blood.––
Cells of the ventricles form the bloodCells of the ventricles form the blood--brain barrier.brain barrier.
34
35

36
Brain Metabolism & PerfusionBrain Metabolism & Perfusion••
High metabolic rate.High metabolic rate.––
Receives 15% of total cardiac output.Receives 15% of total cardiac output.
––
Consumes 20% of body’s oxygen.Consumes 20% of body’s oxygen.––
25% of glucose utilization (largest user).25% of glucose utilization (largest user).
––
Requires thiamine.Requires thiamine.––
Cannot store nutrients.Cannot store nutrients.
••
Blood SupplyBlood Supply––
Vertebral arteries supply posterior brain Vertebral arteries supply posterior brain (cerebellum and brain stem).(cerebellum and brain stem).
––
Carotid arteries supply most of cerebrum.Carotid arteries supply most of cerebrum.

37

38

39
Brain Metabolism & PerfusionBrain Metabolism & Perfusion••
PerfusionPerfusion––
Cerebral Blood Flow (CBF)Cerebral Blood Flow (CBF)••
Dependent upon CPP.Dependent upon CPP.
••
Flow requires pressure gradient.Flow requires pressure gradient.––
Cerebral Perfusion Pressure Cerebral Perfusion Pressure (CPP)(CPP)••
Pressure moving the blood Pressure moving the blood through the cranium.through the cranium.
••
AutoregulationAutoregulation
allows BP change allows BP change to maintain CPP.to maintain CPP.
••
CPP = Mean Arterial Pressure CPP = Mean Arterial Pressure (MAP) (MAP) --
Intracranial Pressure Intracranial Pressure
(ICP).(ICP).

40
Brain Metabolism & PerfusionBrain Metabolism & Perfusion••
PerfusionPerfusion––
Mean Arterial Pressure (MAP)Mean Arterial Pressure (MAP)••
Largely dependent on cerebral vascular Largely dependent on cerebral vascular resistance (CVR) since diastolic is main resistance (CVR) since diastolic is main component.component.
••
Blood volume and myocardial contractility.Blood volume and myocardial contractility.••
MAP =[(2 x diastolic) + systolic] / 3 .MAP =[(2 x diastolic) + systolic] / 3 .
••
Usually requires MAP of at least 60 mmHg to Usually requires MAP of at least 60 mmHg to perfuse brain (50 perfuse brain (50 ––
70 mmHg).70 mmHg).
––
Intracranial Pressure (ICP)Intracranial Pressure (ICP)••
Increases with edema or hemorrhage.Increases with edema or hemorrhage.
••
ICP usually 10ICP usually 10--15 mm Hg.15 mm Hg.

41
Brain InjuryBrain Injury
By definition:By definition:“a traumatic insult to the brain “a traumatic insult to the brain
capable of producing physical, capable of producing physical, intellectual, emotional, social and intellectual, emotional, social and vocational changes”vocational changes”
42
••
Three broad categories:Three broad categories:––
Focal injuryFocal injury••
Cerebral contusionCerebral contusion
••
Intracranial hemorrhage Intracranial hemorrhage ••
Epidural hemorrhageEpidural hemorrhage
––
SubarachnoidSubarachnoid/subdural hemorrhage/subdural hemorrhage––
Diffuse Axonal InjuryDiffuse Axonal Injury••
Concussion (mild and classic form)Concussion (mild and classic form)
Brain InjuryBrain Injury

4/30/2009 43
Any patient with head or Any patient with head or facial injuries, has a cervical facial injuries, has a cervical
spine injury until proven spine injury until proven otherwise.otherwise.
44
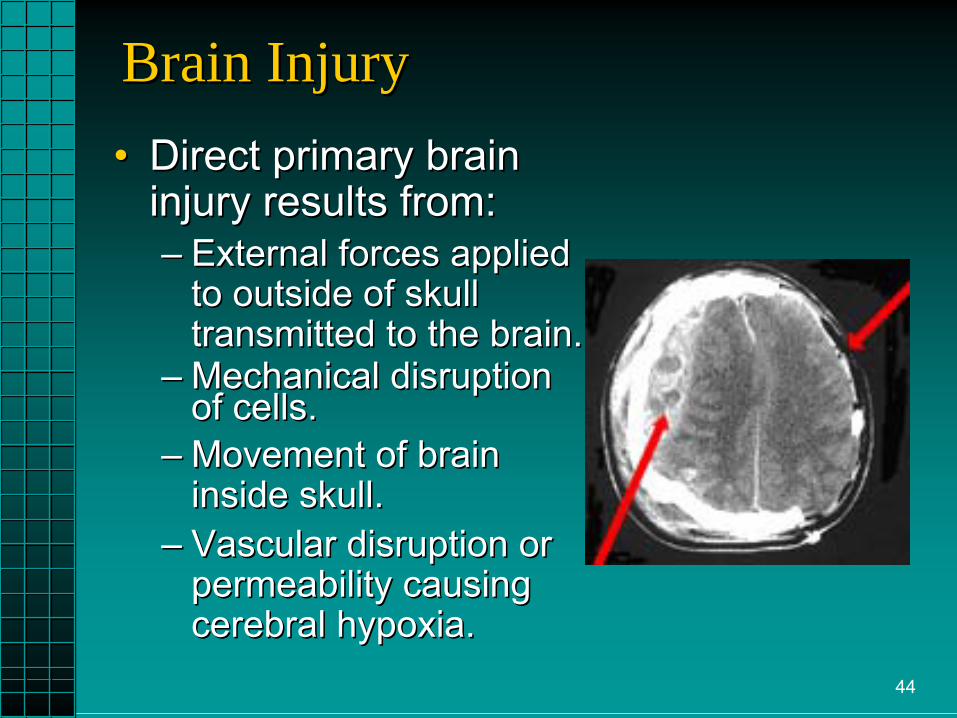
Brain InjuryBrain Injury••
Direct primary brain Direct primary brain injury results from:injury results from:––
External forces applied External forces applied to outside of skull to outside of skull transmitted to the brain.transmitted to the brain.
––
Mechanical disruption Mechanical disruption of cells.of cells.
––
Movement of brain Movement of brain inside skull.inside skull.
––
Vascular disruption or Vascular disruption or permeability causing permeability causing cerebral hypoxia.cerebral hypoxia.

45
••
Indirect (secondary or tertiary) brain Indirect (secondary or tertiary) brain injury may be due to:injury may be due to:––
SecondarySecondary••
Edema, hemorrhage, infection, inadequate Edema, hemorrhage, infection, inadequate perfusion, tissue hypoxia, pressure.perfusion, tissue hypoxia, pressure.
––
TertiaryTertiary••
Apnea, hypotension, pulmonary resistance, Apnea, hypotension, pulmonary resistance, ECG changes.ECG changes.
Brain InjuryBrain Injury
46
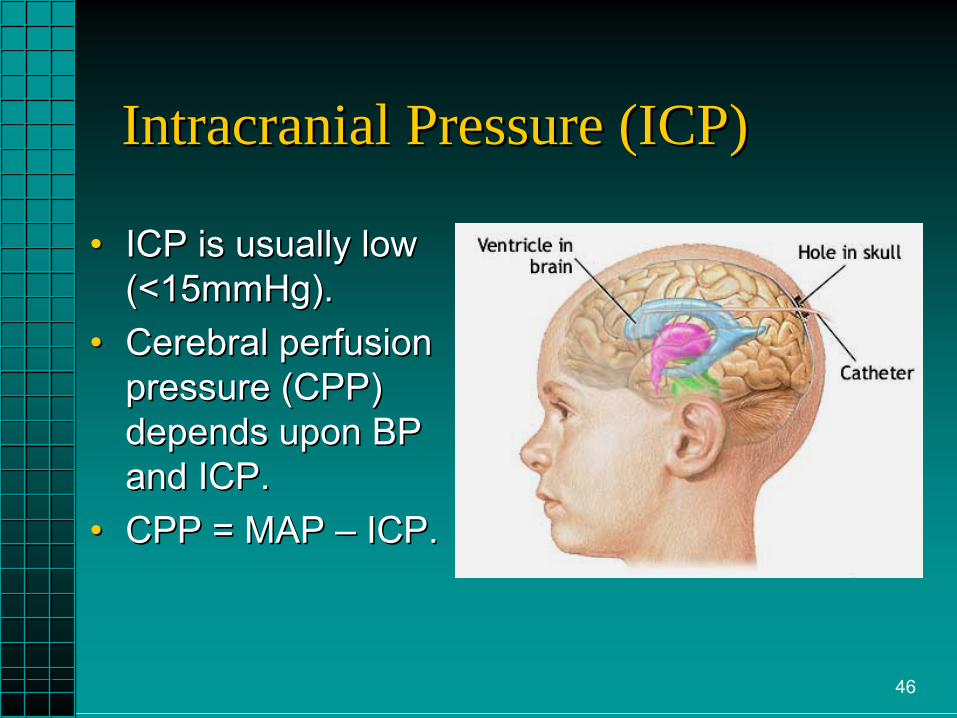
Intracranial Pressure (ICP)Intracranial Pressure (ICP)
••
ICP is usually low ICP is usually low (<15mmHg).(<15mmHg).
••
Cerebral perfusion Cerebral perfusion pressure (CPP) pressure (CPP) depends upon BP depends upon BP and ICP.and ICP.
••
CPP = MAP CPP = MAP ––
ICP.ICP.
47
••
As ICP increases and approaches MAP, As ICP increases and approaches MAP, cerebral blood flow will decrease.cerebral blood flow will decrease.
••
This results in decreased CPP.This results in decreased CPP.••
Compensatory mechanisms attempt to Compensatory mechanisms attempt to compensate and increasecompensate and increase
MAP by MAP by
increasing blood pressure.increasing blood pressure.••
As CPP continues to decreaseAs CPP continues to decrease, cerebral , cerebral vasodilation occurs as an attempt to vasodilation occurs as an attempt to increase increase blood volume and cerebral blood volume and cerebral perfusion.perfusion.
••
This further increases ICP, which leads to This further increases ICP, which leads to decreased CPP and so on . . .decreased CPP and so on . . .
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
48
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
••
A decrease in pH or an accumulation of A decrease in pH or an accumulation of carbon dioxide (carbon dioxide (hypercarbiahypercarbia) causes ) causes cerebral cerebral vasodilation vasodilation that results in that results in blood volume blood volume ICP ICP CPP. CPP. CCompensatory mechanisms attempt to ompensatory mechanisms attempt to
MAP as CPP MAP as CPP , cerebral vasodilation , cerebral vasodilation occurs to occurs to blood volume blood volume and, the cycle and, the cycle continues . . .continues . . .

49
••
Or Or baroreceptorsbaroreceptors
sense an initial drop sense an initial drop in blood pressure (hypotension) that in blood pressure (hypotension) that results in results in CPP CPP cerebralcerebralvasodilationvasodilation that that results in results in blood blood volume volume ICP ICP CPP and, the CPP and, the cycle continues . . .cycle continues . . .
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
50
Pathophysiology of Brain InjuryPathophysiology of Brain Injury••
As the pressure increases, pressure is exerted As the pressure increases, pressure is exerted downward on the brain and brain stem. The increasing downward on the brain and brain stem. The increasing pressure:pressure:––
On the cerebral cortex or RAS causes an altered level of On the cerebral cortex or RAS causes an altered level of consciousness.consciousness.
––
On the hypothalamus stimulates vomiting reflex center.On the hypothalamus stimulates vomiting reflex center.––
On the brain stem:On the brain stem:••
Increases BP and bradycardia secondary to vagal Increases BP and bradycardia secondary to vagal stimulation.stimulation.
••
Irregular respirations or tachypnea.Irregular respirations or tachypnea.••
Unequal/unreactive pupils secondary to oculomotor nerve Unequal/unreactive pupils secondary to oculomotor nerve paralysis.paralysis.
••
Posturing, decorticate or Posturing, decorticate or decerebratedecerebrate..––
Seizures dependent on location of injury.Seizures dependent on location of injury.––
Herniation Herniation will occur if the pressure continues to climb.will occur if the pressure continues to climb.

51
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
••
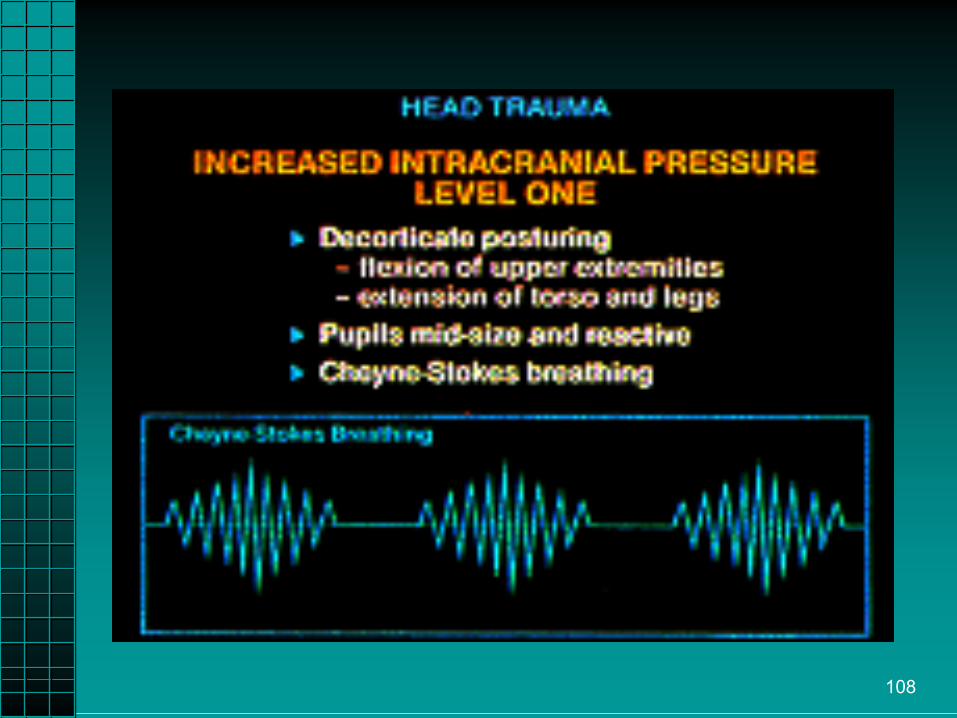
Levels of increasing ICP.Levels of increasing ICP.––
Cerebral cortex and upper brain stem.Cerebral cortex and upper brain stem.••
BP rising and pulse rate slowing.BP rising and pulse rate slowing.
••
Pupils reactive.Pupils reactive.••
CheyneCheyne--Stokes respirations.Stokes respirations.
••
Initially try to localize the pain and remove Initially try to localize the pain and remove painful stimuli.painful stimuli.
••
As it progresses, decorticate posturing.As it progresses, decorticate posturing.
52
••
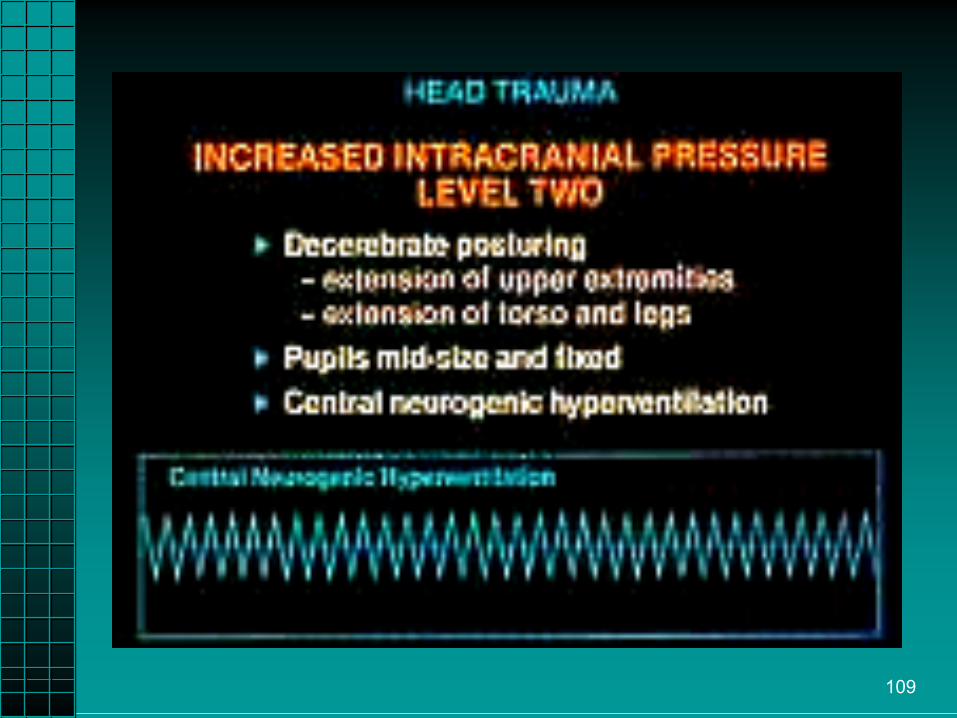
Levels of increasing ICP.Levels of increasing ICP.––
Middle brain stem.Middle brain stem.••
Wide pulse pressure and bradycardia.Wide pulse pressure and bradycardia.
••
Pupils become nonPupils become non--reactive or sluggish.reactive or sluggish.••
CentralCentral
neurogenicneurogenic
hyperventilation.hyperventilation.
••
Extension orExtension or
decerebratedecerebrate
posturing.posturing.
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
53
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
••
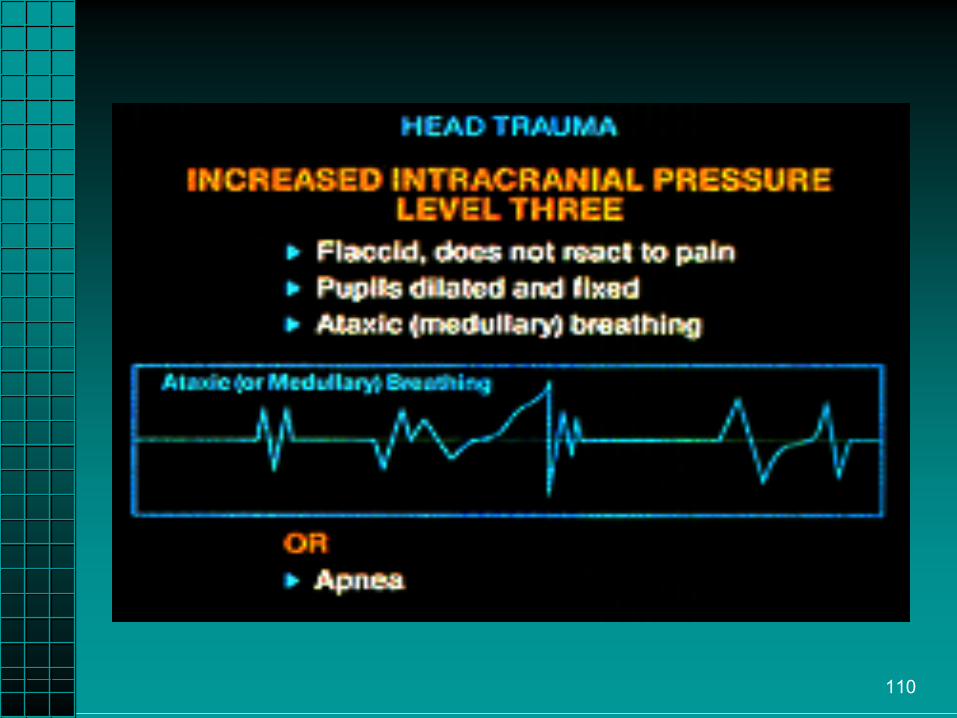
Levels of Increasing ICP.Levels of Increasing ICP.––
Lower Brain Stem / Medulla.Lower Brain Stem / Medulla.••
Pupil blown (both or on the side of injury).Pupil blown (both or on the side of injury).
••
Ataxic or absent respirations. Ataxic or absent respirations. ••
Flaccid.Flaccid.
••
Irregular or changing pulse rate.Irregular or changing pulse rate.••
Decreased BP.Decreased BP.
••
Usually not survivable.Usually not survivable.
54
HerniationHerniation SyndromeSyndrome••
Increased ICP.Increased ICP.
••
Coma.Coma.••
Dilatation of Dilatation of ipsilateralipsilateral
or both pupils.or both pupils.
••
Contralateral hemiparesisContralateral hemiparesis..••
Decreasing respiration.Decreasing respiration.
••
Cushing’s Reflex.Cushing’s Reflex.––
Hypertension.Hypertension.
––
Bradycardia.Bradycardia.––
Central Central neurogenicneurogenic
hyperventilation.hyperventilation.
55
Pathophysiology of Brain InjuryPathophysiology of Brain Injury
••
HerniationHerniation––
TranstentorialTranstentorial
or or tentorial herniationtentorial herniation
••
Downward displacement of the brain due to ICP.Downward displacement of the brain due to ICP.••
Signs include severe headache, fever, alterations in Signs include severe headache, fever, alterations in consciousness, both pupils may dilate or become sluggish.consciousness, both pupils may dilate or become sluggish.
––
UncalUncal
herniationherniation••
““Downward displacement through the tentorial notch by a Downward displacement through the tentorial notch by a supratentorial mass exerting pressure on underlying supratentorial mass exerting pressure on underlying structures including the brain stem.structures including the brain stem.””
••
Placing pressure on the third cranial nerve, dilating the Placing pressure on the third cranial nerve, dilating the pupil on the affected side.pupil on the affected side.

56
57
Note the impression of the foramen magnum due to increased ICP.
58
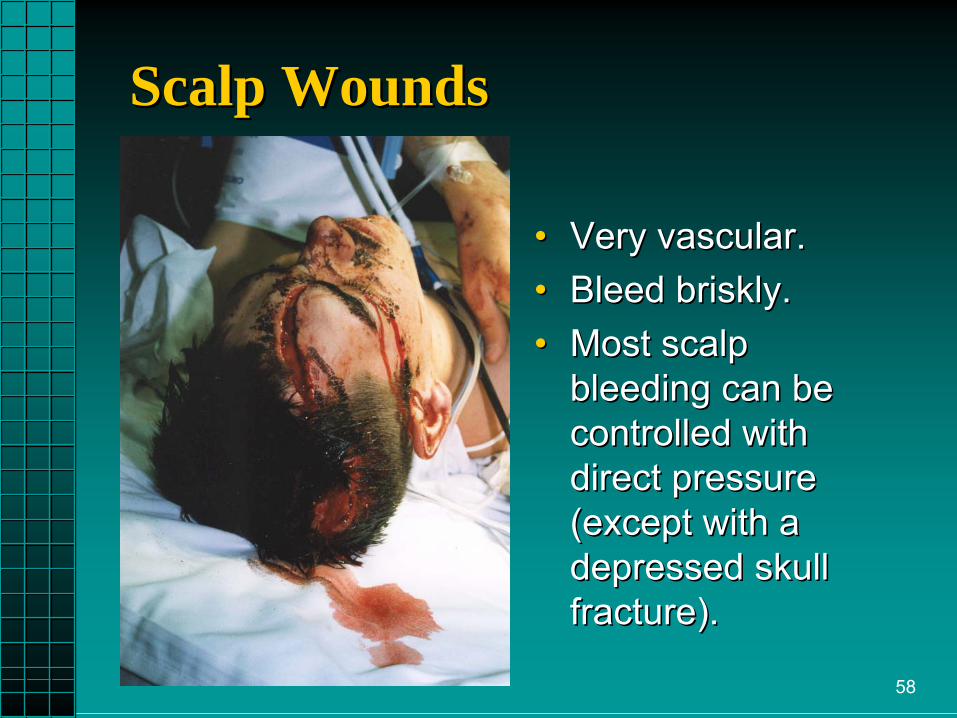
Scalp WoundsScalp Wounds
••
Very vascular.Very vascular.••
Bleed briskly.Bleed briskly.
••
Most scalp Most scalp bleeding can be bleeding can be controlled with controlled with direct pressure direct pressure (except with a (except with a depressed skull depressed skull fracture).fracture).

59

60
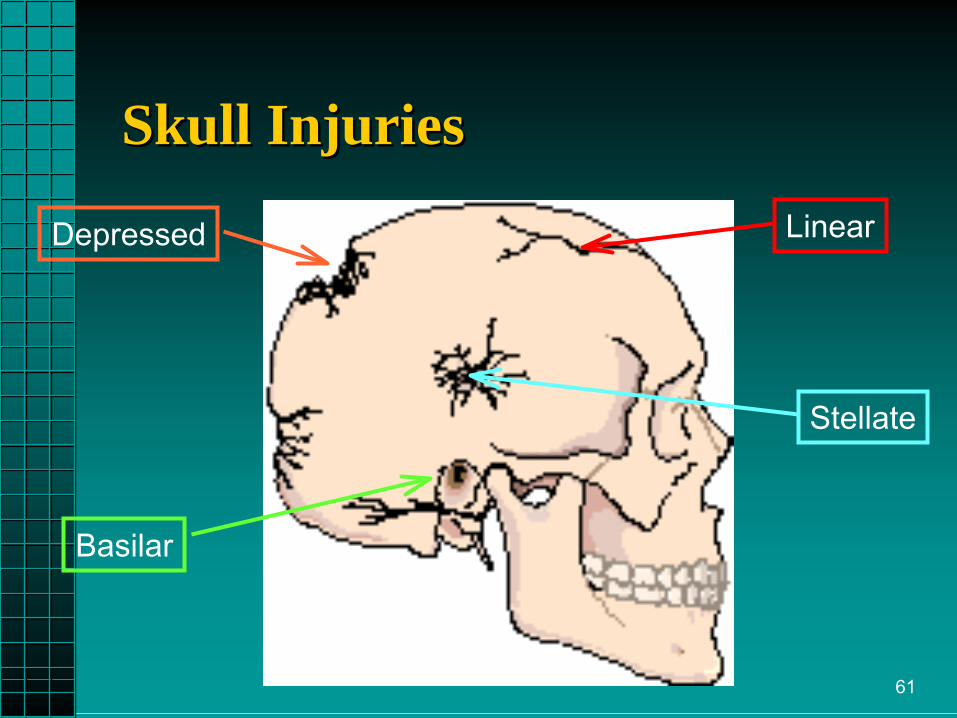
Skull InjuriesSkull Injuries
61
Skull InjuriesSkull Injuries
Depressed Linear
Stellate
Basilar

62
••
Linear FractureLinear Fracture––
Usually not identified in field.Usually not identified in field.••
80% of all skull fractures are linear.80% of all skull fractures are linear.
––
Suspect a linear fracture based on: Suspect a linear fracture based on: ••
Mechanism of injury.Mechanism of injury.
••
Overlying soft tissue trauma.Overlying soft tissue trauma.
––
Temporal region = ~Epidural hematoma.Temporal region = ~Epidural hematoma.
Skull InjuriesSkull Injuries

63
Skull InjuriesSkull Injuries
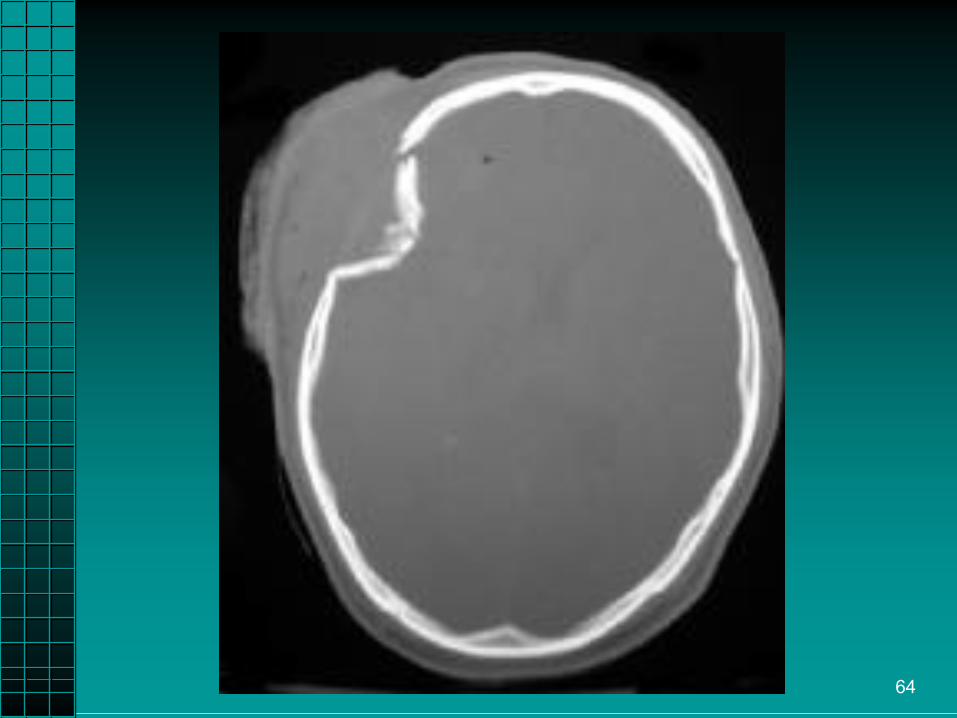
••
Depressed Skull Depressed Skull FractureFracture––
Segment pushed Segment pushed inward.inward.
––
Pressure on brain Pressure on brain may cause further may cause further brain injury.brain injury.
––
Avoid pressure when Avoid pressure when trying to control trying to control bleeding. Use loose bleeding. Use loose dressings.dressings.
64

65
Skull InjuriesSkull Injuries
••
Stellate Stellate skull skull fracture is most fracture is most commonly due commonly due to a blow or to a blow or blunt trauma to blunt trauma to the head.the head.Can also occur Can also occur with penetrating with penetrating trauma.trauma.

66
••
Basilar Skull Fracture:Basilar Skull Fracture:––
May be difficult to detect in the field. A basilar May be difficult to detect in the field. A basilar skull fracture is difficult to detect on xskull fracture is difficult to detect on x--ray.ray.
––
Signs and symptoms depend on amount of Signs and symptoms depend on amount of damage.damage.
––
Suspicion is based on clinical findings:Suspicion is based on clinical findings:••
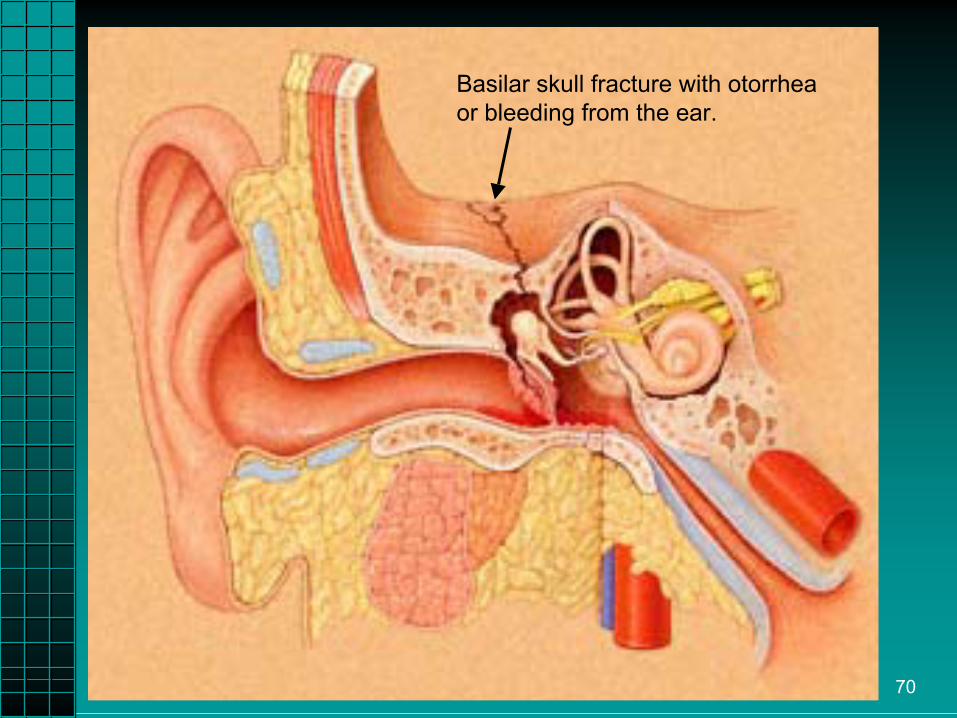
CSF CSF otorrhea otorrhea ––
drainage from the eardrainage from the ear••
CSF CSF rhinorrhea rhinorrhea ––
drainage from the nosedrainage from the nose••
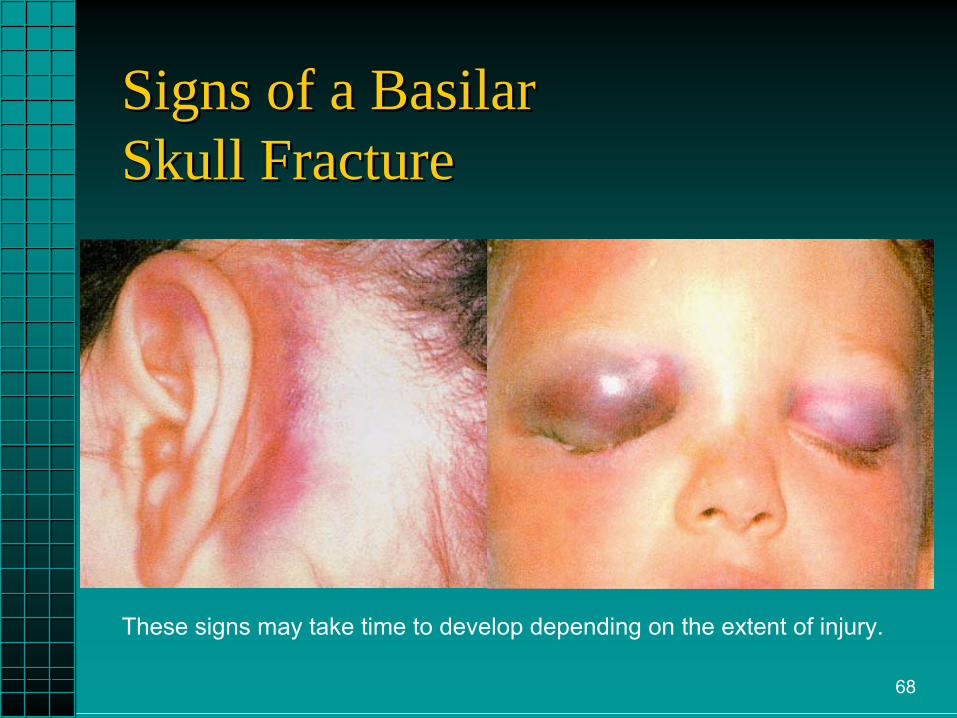
Periorbital ecchymosisPeriorbital ecchymosis••
Battle’s signBattle’s sign
Skull InjuriesSkull Injuries
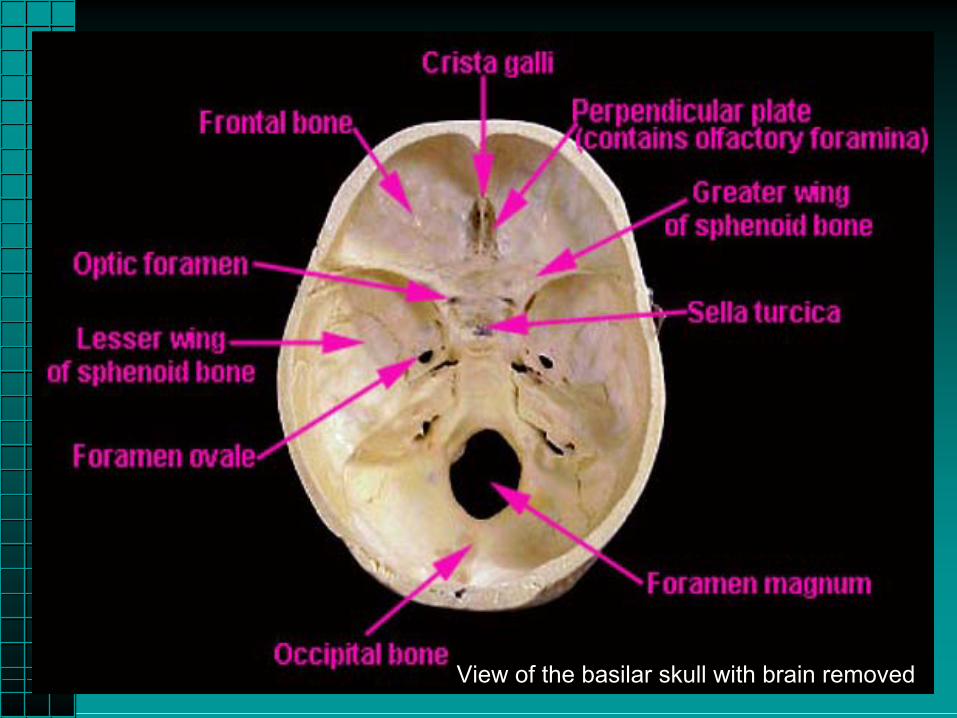
67View of the basilar skull with brain removed
68
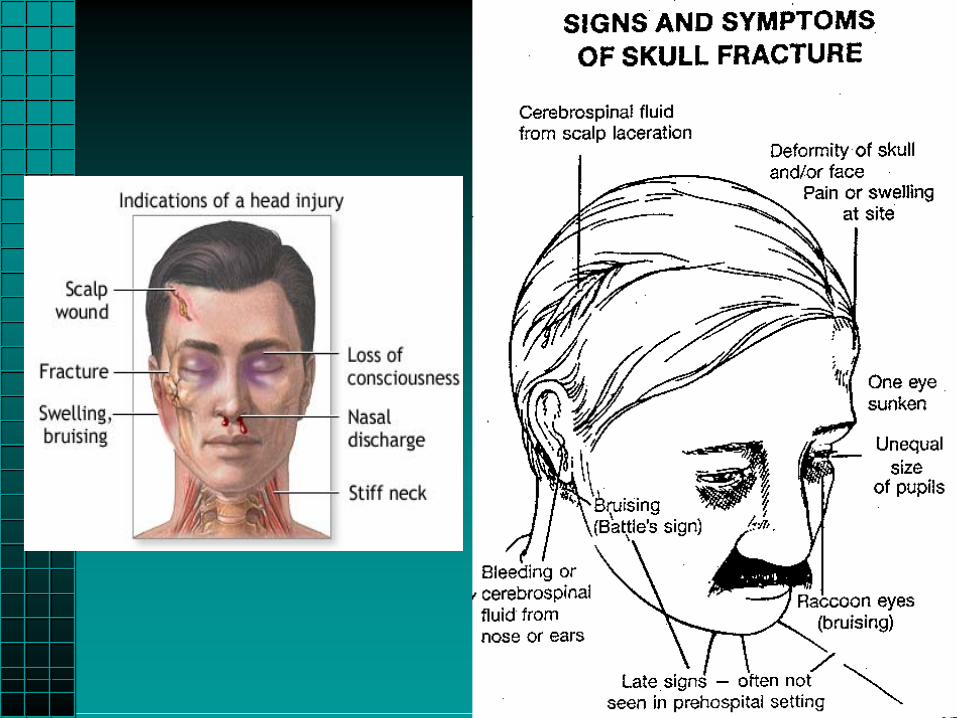
Signs of a BasilarSigns of a Basilar Skull FractureSkull Fracture
These signs may take time to develop depending on the extent of injury.

69
••
Cerebrospinal Fluid.Cerebrospinal Fluid.––
Delays blood clotting.Delays blood clotting.
––
Halo sign present on 4x4.Halo sign present on 4x4.––
Does not crust on drying.Does not crust on drying.
––
Positive blood sugar with Positive blood sugar with DextrostickDextrostick..••
CSF glucose level usually 50 CSF glucose level usually 50 ––
80 mg/dl.80 mg/dl.••
2/3’s the value of normal blood glucose.2/3’s the value of normal blood glucose.••
Nasal fluid not contaminated by blood is Nasal fluid not contaminated by blood is positive for CSF if glucose is positive for CSF if glucose is ≥≥
30 mg/dl.30 mg/dl.••
Not a good diagnostic indicator.Not a good diagnostic indicator.
Skull InjuriesSkull Injuries
70
Basilar skull fracture with otorrhea
or bleeding from the ear.
71
••
Basilar Skull FractureBasilar Skull Fracture––
Do not pack the ears, allow for drainage.Do not pack the ears, allow for drainage.
––
Do not suction fluid.Do not suction fluid.––
Do not put anything in the nose.Do not put anything in the nose.••
No No nasotrachealnasotracheal
intubation.intubation.
••
No No nasogastricnasogastric
tubes.tubes.
Skull InjuriesSkull Injuries

72
Skull InjuriesSkull Injuries••
Open Skull FractureOpen Skull Fracture––
Cranial contents Cranial contents exposed.exposed.
––
Manage like an Manage like an evisceration.evisceration.
––
Protect exposed tissue Protect exposed tissue with moist, clean with moist, clean dressing.dressing.
––
Neurologic signs and Neurologic signs and symptoms evident.symptoms evident.
73
74
Specific Brain InjuriesSpecific Brain Injuries
••
Injury to the Injury to the Cerebral Cerebral Parenchyma.Parenchyma.
••
Diffuse axonal Diffuse axonal injury.injury.
••
Anoxic brain Anoxic brain injury.injury.
75
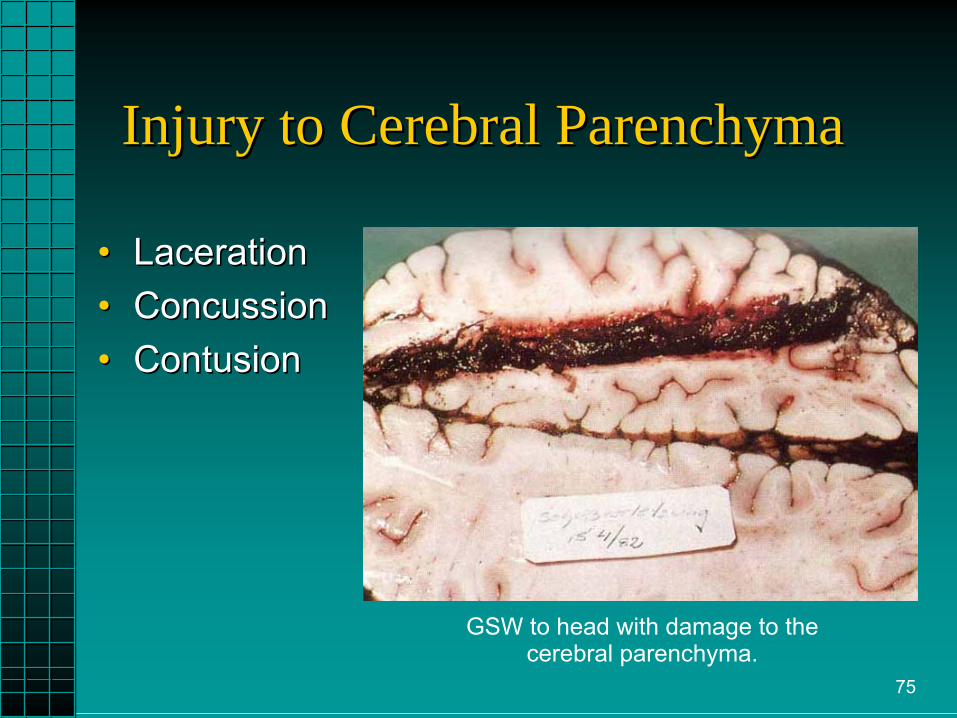
Injury to Cerebral ParenchymaInjury to Cerebral Parenchyma
••
LacerationLaceration••
ConcussionConcussion
••
ContusionContusion
GSW to head with damage to thecerebral parenchyma.
76
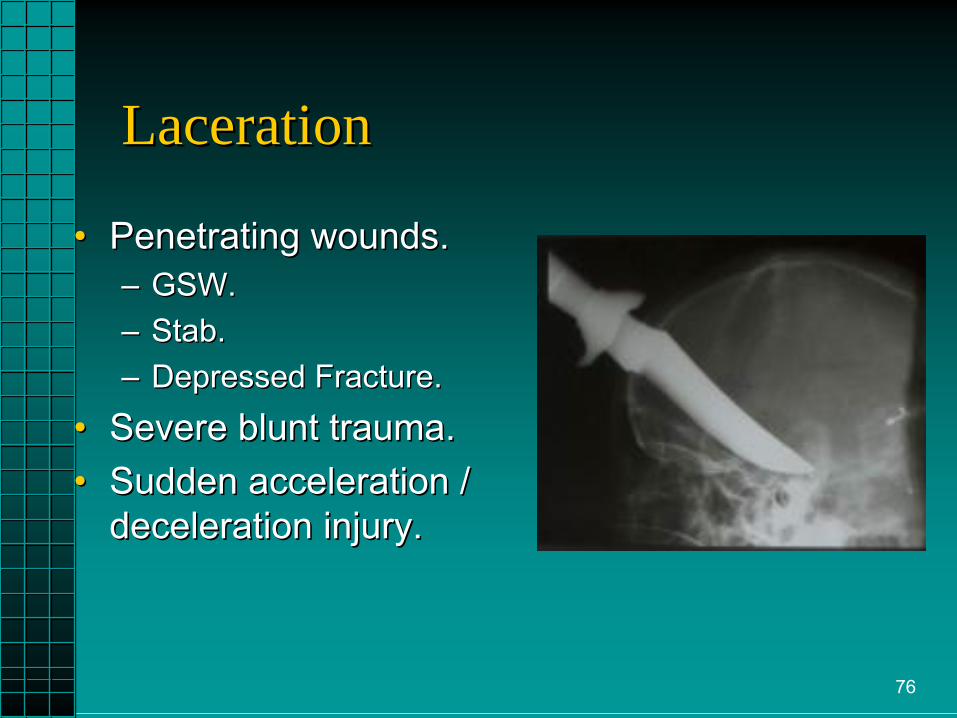
LacerationLaceration
••
Penetrating wounds.Penetrating wounds.––
GSW.GSW.
––
Stab.Stab.––
Depressed Fracture.Depressed Fracture.
••
Severe blunt trauma.Severe blunt trauma.••
Sudden acceleration / Sudden acceleration / deceleration injury.deceleration injury.

77
ConcussionConcussion••
Grade 1Grade 1 The mild concussion occurs when the person does not The mild concussion occurs when the person does not lose consciousness (pass out) but may seem dazed. lose consciousness (pass out) but may seem dazed.
••
Grade 2Grade 2 The slightly more severe form occurs when the person The slightly more severe form occurs when the person does not lose consciousness but has a period of confusion does not lose consciousness but has a period of confusion and does not recall the event.and does not recall the event.
••
Grade 3Grade 3 The classic concussion, which is the most severe form, The classic concussion, which is the most severe form, occurs when the person loses consciousness for a brief occurs when the person loses consciousness for a brief period of time and has no memory of the event. Evaluation period of time and has no memory of the event. Evaluation should be performed as soon as possible after the injury. should be performed as soon as possible after the injury.

78
CoupCoup--ContrecoupContrecoup InjuriesInjuries
•• “4 collision” “4 collision” concept with head concept with head injuries:injuries:1.1.
Auto strikes tree.Auto strikes tree.
2.2.
Head strikes Head strikes windshield.windshield.
3.3.
Brain strikes inside Brain strikes inside of frontal skull.of frontal skull.
4.4.
Brain rebounds Brain rebounds and hits inside of and hits inside of occipital skull.occipital skull.
79
••
Coup injuryCoup injury––
Directly posterior to point of impact.Directly posterior to point of impact.
––
More common when front of head struck.More common when front of head struck.••
ContrecoupContrecoup injuryinjury––
Directly opposite the point of impact.Directly opposite the point of impact.
––
More common when back of head struck.More common when back of head struck.
CoupCoup--ContrecoupContrecoup InjuriesInjuries

80
Cerebral ContusionCerebral Contusion

81

82
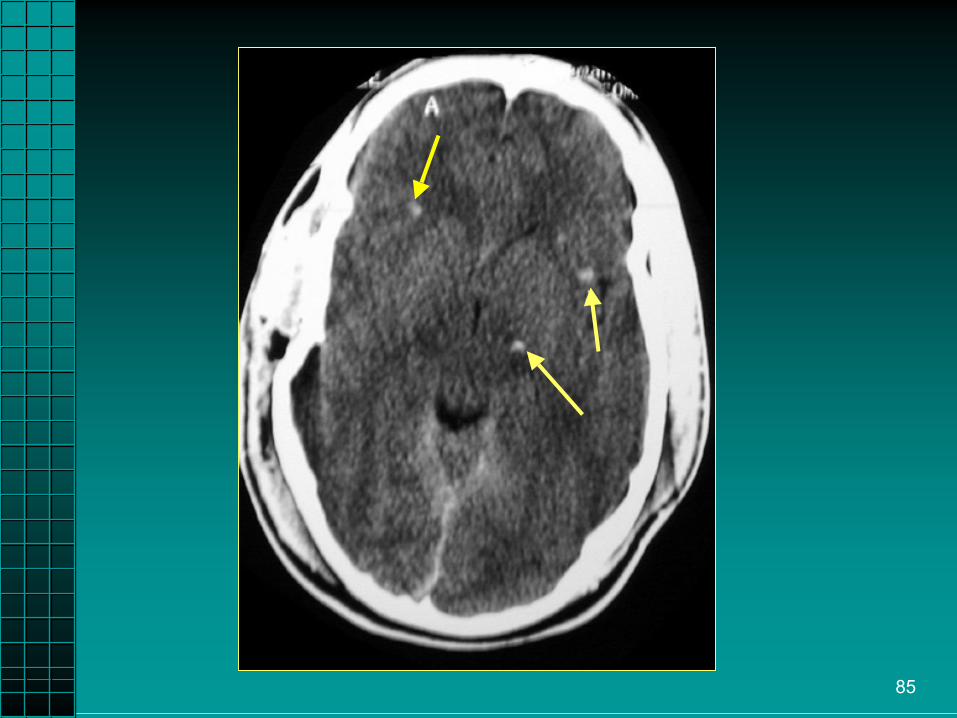
Diffuse Axonal InjuryDiffuse Axonal Injury
••
A type of brain injury A type of brain injury caused by shearing caused by shearing forces that occur forces that occur between different parts between different parts of the brain as a result of of the brain as a result of rotational acceleration. rotational acceleration. The corpusThe corpus
callosumcallosum
and and
the brainstem are often the brainstem are often affected. DAI most affected. DAI most commonly occurs in commonly occurs in motor vehicle crashes.motor vehicle crashes. Petechial hemorrhages
83
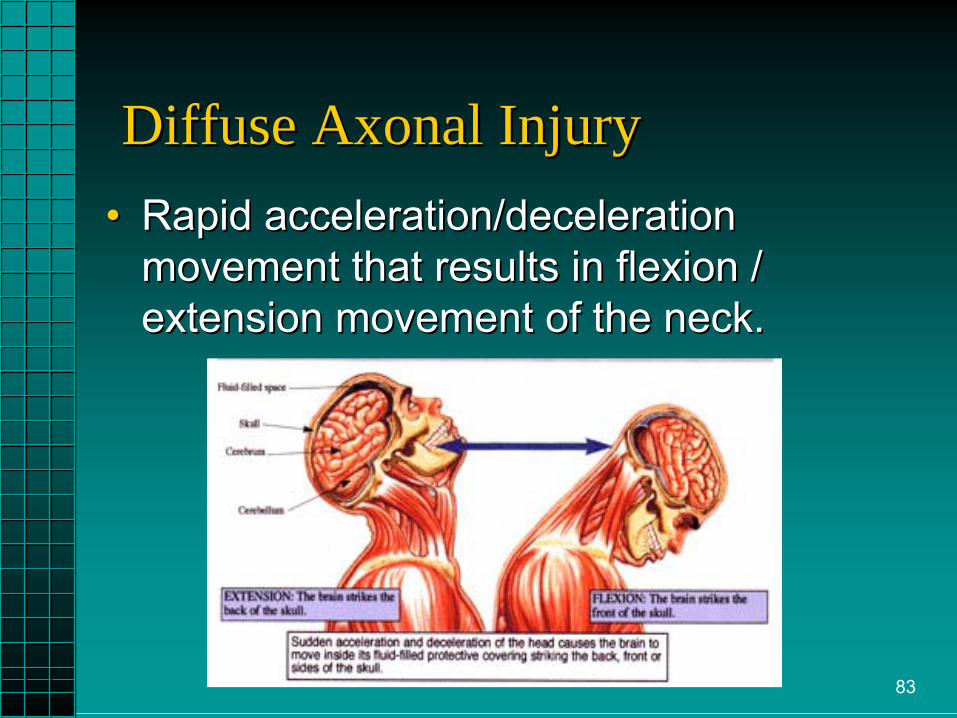
••
Rapid acceleration/deceleration Rapid acceleration/deceleration movement that results in flexion / movement that results in flexion / extension movement of the neck.extension movement of the neck.
Diffuse Axonal InjuryDiffuse Axonal Injury

84
Axons extend across Axons extend across the different layers of the different layers of the brain and are the brain and are stretched and torn stretched and torn causing nerve damage causing nerve damage andand
petechialpetechial
hemorrhages located hemorrhages located at the grayat the gray--white white matter junction, within matter junction, within the corpusthe corpus
callosumcallosum, ,
and in the brainstem.and in the brainstem.
Diffuse Axonal InjuryDiffuse Axonal Injury

86
EpiduralEpidural HematomaHematoma

87
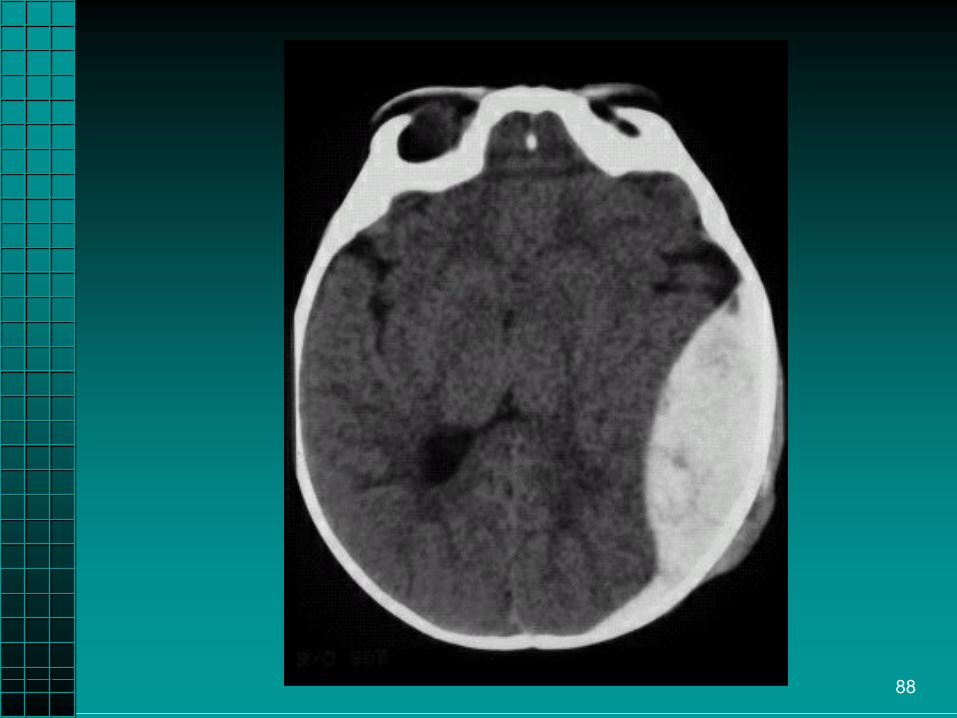
EpiduralEpidural HematomaHematoma
••
Blood between Blood between skull and dura.skull and dura.
••
Usually arterial Usually arterial tear from the tear from the middle middle meningealmeningeal
artery.artery.••
Causes increase Causes increase in intracranial in intracranial pressure.pressure.
88
89
Epidural HematomaEpidural Hematoma
••
Unconsciousness followed by lucid interval.Unconsciousness followed by lucid interval.••
Rapid deterioration.Rapid deterioration.
••
Decreased LOC, headache, nausea, Decreased LOC, headache, nausea, vomiting.vomiting.
••
HemiparesisHemiparesis, , hemiplegiahemiplegia..••
Unequal pupils (dilated on side of clot).Unequal pupils (dilated on side of clot).
••
Increase BP, decreased pulse (Cushing’s Increase BP, decreased pulse (Cushing’s reflex).reflex).
90
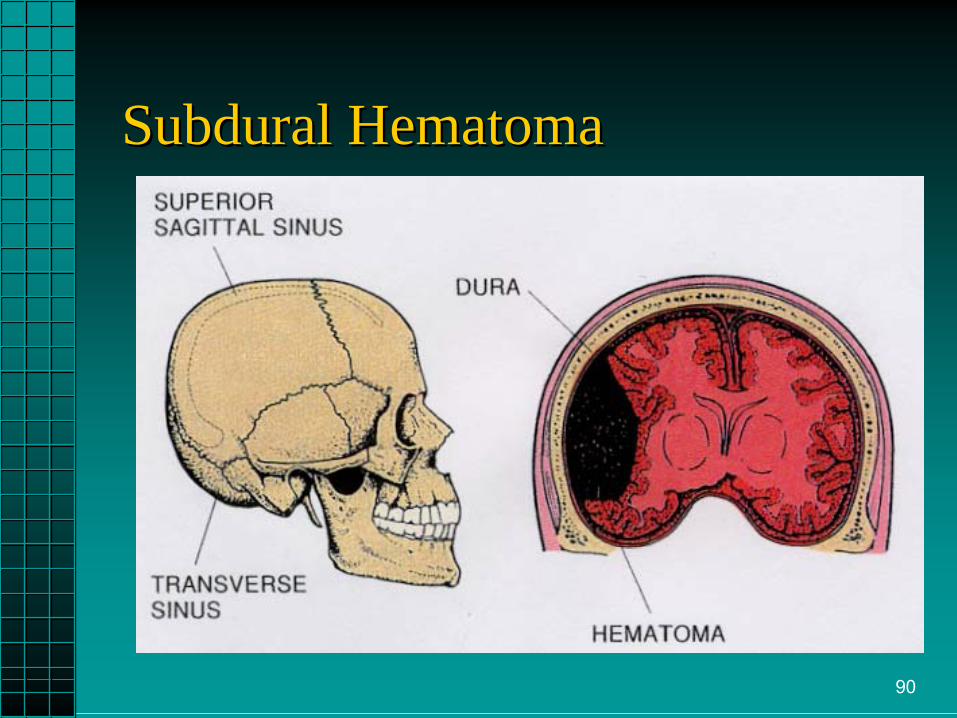
Subdural HematomaSubdural Hematoma

91
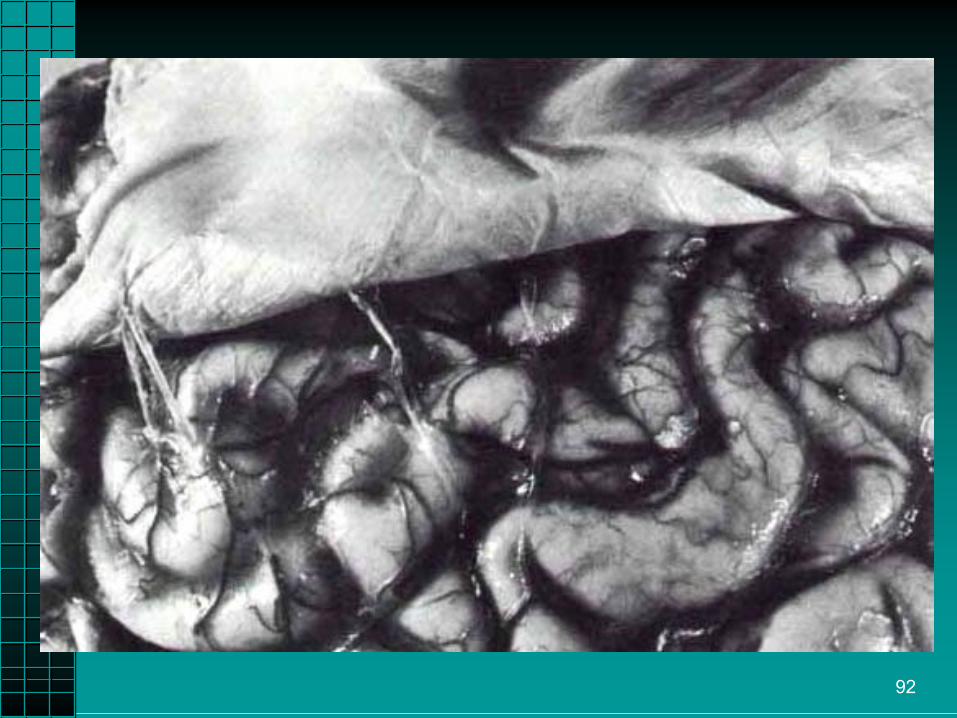
Subdural HematomaSubdural Hematoma
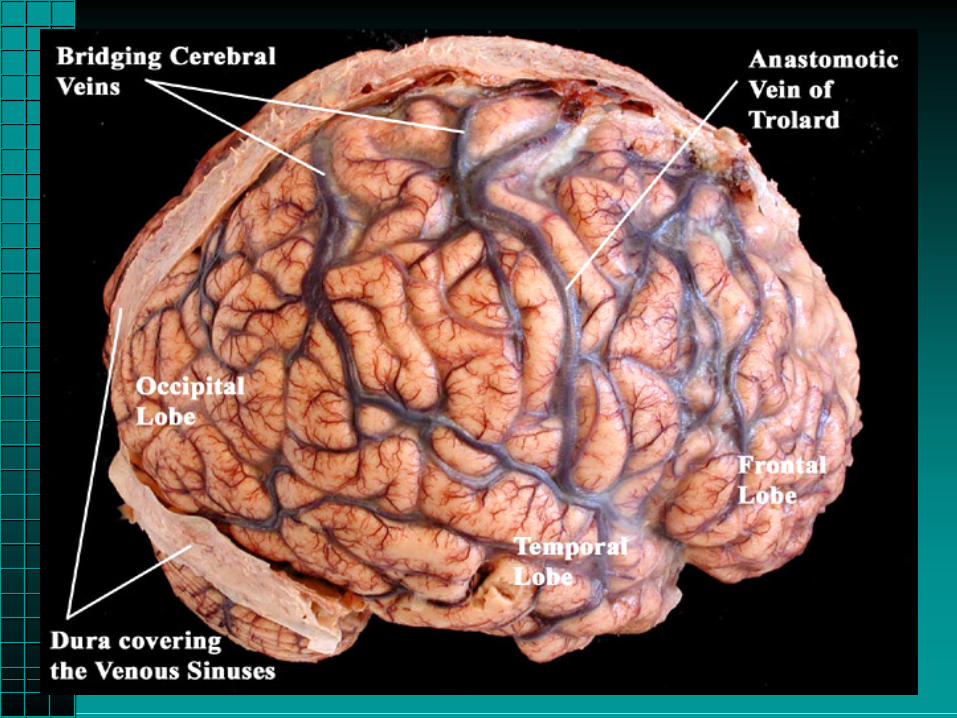
••
Between dura Between dura mater and mater and arachnoid.arachnoid.
••
More common.More common.••
Usually venous.Usually venous.––
Bridging veins Bridging veins between cortex between cortex and the dura.and the dura.
••
Causes increased Causes increased intracranial intracranial pressure.pressure.
92
93

94
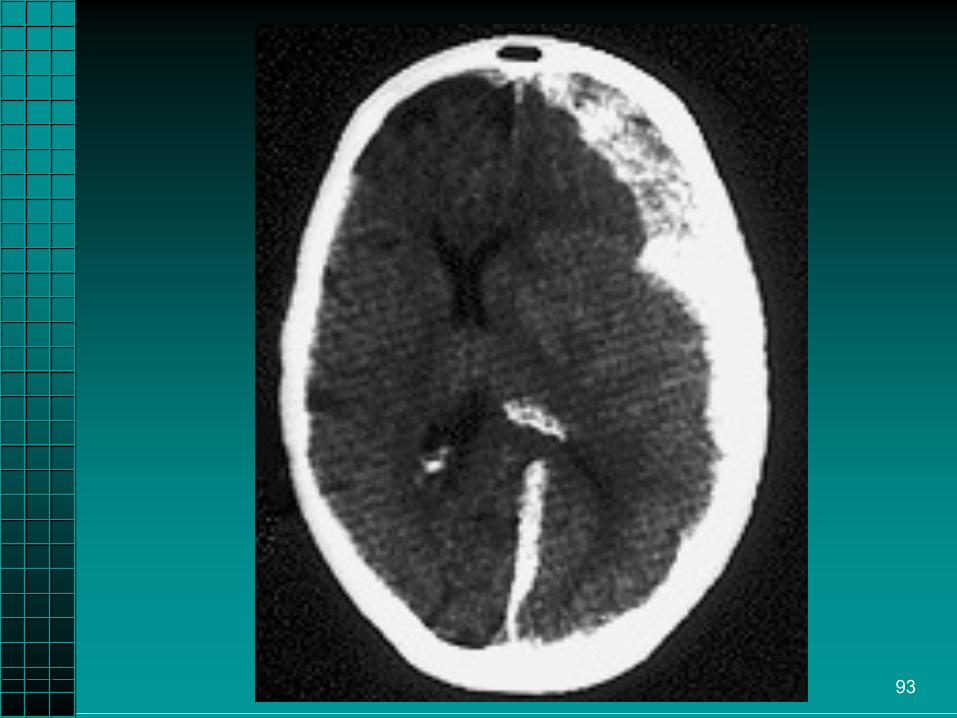
Subdural HematomaSubdural Hematoma
••
Slower onset.Slower onset.••
Increased ICP.Increased ICP.
••
Headache, decreased LOC, unequal Headache, decreased LOC, unequal pupils. pupils.
••
Increased BP, decreased pulse.Increased BP, decreased pulse.••
HemiparesisHemiparesis, , hemiplegiahemiplegia..
95
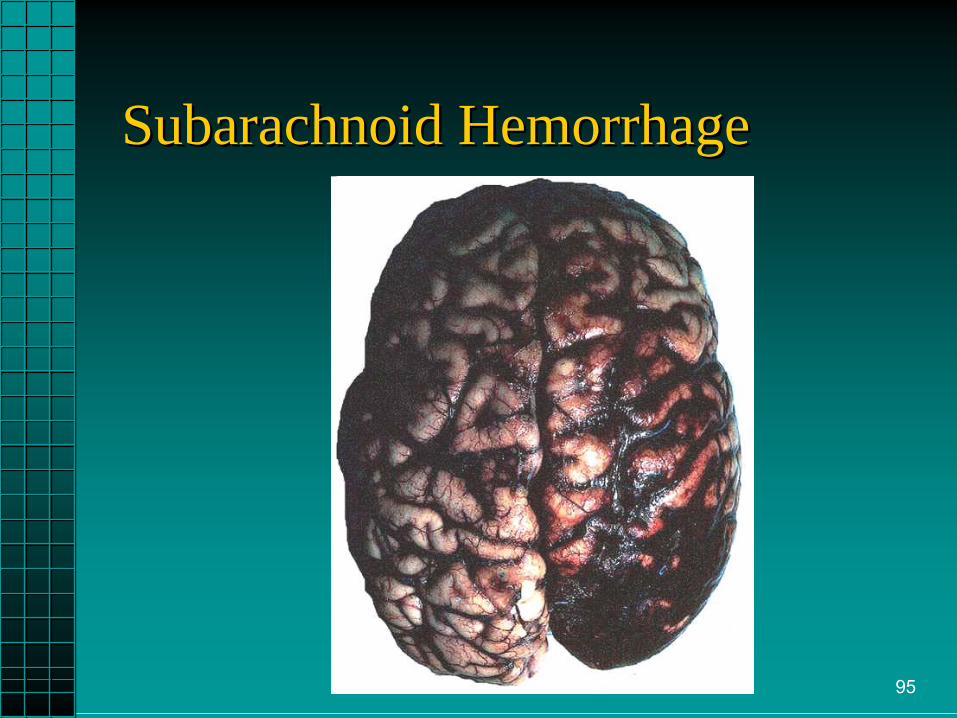
Subarachnoid HemorrhageSubarachnoid Hemorrhage

96
Intracranial HemorrhageIntracranial Hemorrhage

97
IntracerebralIntracerebral HematomaHematoma••
Usually due to Usually due to laceration of the laceration of the brain.brain.
••
Bleeding into Bleeding into cerebral substance.cerebral substance.
••
Associated with Associated with other injuries such other injuries such as DAI.as DAI.
••
Neuro deficits Neuro deficits depend on region depend on region involved and size.involved and size.––
Repetitive w/frontal Repetitive w/frontal lobe.lobe.
••
Increased ICP.Increased ICP.

98
4/30/2009 99
Head Trauma AssessmentHead Trauma Assessment

100
Common Signs and SymptomsCommon Signs and Symptoms of Head Injuriesof Head Injuries
••
Nausea and vomiting.Nausea and vomiting.••
Altered LOC, changing LOC, possibly Altered LOC, changing LOC, possibly combative. Be prepared!combative. Be prepared!
••
Headache.Headache.••
Diplopia or blurred vision.Diplopia or blurred vision.
••
Slurred speech.Slurred speech.••
Raccoon's eyes and / or Battle’s sign.Raccoon's eyes and / or Battle’s sign.
••
CSF and / or blood from the nose or ears.CSF and / or blood from the nose or ears.••
Cushing’s Triad.Cushing’s Triad.
101
Trauma Assessment Trauma Assessment Rapid Trauma SurveyRapid Trauma Survey
••
Note LOC (AVPU), secure airway and protect Note LOC (AVPU), secure airway and protect cc--spine.spine.
••
Assess breathing and oxygenation.Assess breathing and oxygenation.––
Do not allow the patient to become hypoxic.Do not allow the patient to become hypoxic.
••
Assess circulation.Assess circulation.––
Control major bleeding.Control major bleeding.
––
Maintain cerebral perfusion.Maintain cerebral perfusion.••
Transport decision and interventions.Transport decision and interventions.
••
Complete a brief Complete a brief neuroneuro
exam and GCS if exam and GCS if altered LOC.altered LOC.
102
Glasgow Coma ScaleGlasgow Coma Scale
••
Eye Opening:Eye Opening:––
4 = Spontaneous4 = Spontaneous
––
3 = To voice3 = To voice––
2 = To pain2 = To pain
––
1 = Absent1 = Absent
103
••
Verbal response:Verbal response:––
5 = Oriented5 = Oriented
––
4 = Confused4 = Confused––
3 = Inappropriate words3 = Inappropriate words
––
2 = Moaning, Incomprehensible2 = Moaning, Incomprehensible––
1 = No response1 = No response
Glasgow Coma ScaleGlasgow Coma Scale

104
••
Motor function:Motor function:––
6 = Obeys commands6 = Obeys commands
––
5 = Localizes pain5 = Localizes pain––
4 = Withdraws from pain4 = Withdraws from pain
––
3 = Decorticate (Flexion)3 = Decorticate (Flexion)––
2 = Decerebrate (Extension)2 = Decerebrate (Extension)
––
1 = Flaccid1 = Flaccid
Glasgow Coma ScaleGlasgow Coma Scale

105
Head Trauma AssessmentHead Trauma Assessment••
Respiratory Patterns:Respiratory Patterns:––
Cheyne Stokes.Cheyne Stokes.••
Diffuse injury to cerebral hemispheres.Diffuse injury to cerebral hemispheres.
––
Central neurological hyperventilation.Central neurological hyperventilation.••
Injury to midInjury to mid--brain.brain.
––
ApneusticApneustic..••
Injury to theInjury to the
ponspons..

106
••
Respiratory Patterns:Respiratory Patterns:––
BiotBiot
(Cluster).(Cluster).
••
Injury to upper medulla.Injury to upper medulla.––
Ataxic.Ataxic.••
Injury to lower medulla.Injury to lower medulla.
Head Trauma AssessmentHead Trauma Assessment

107
108
109
110

111
PupilsPupils

112
113
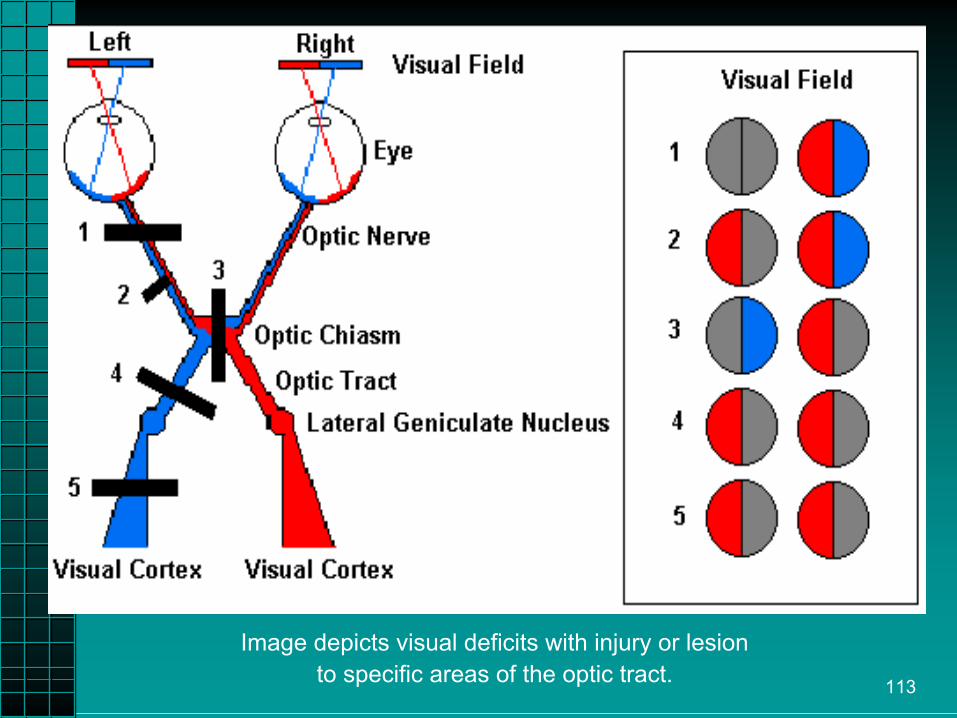
Image depicts visual deficits with injury or lesionto specific areas of the optic tract.
114
••
Pupil exam.Pupil exam.––
Window to the CNS.Window to the CNS.
––
Check pupil size, equality, and response to Check pupil size, equality, and response to light.light.••
Unequal pupils + decreased LOC = Unequal pupils + decreased LOC = compression of compression of oculomotoroculomotor
nerve (CN III).nerve (CN III).
••
Unequal pupils + alert patient = Unequal pupils + alert patient = ––
Direct blow to eye, or Direct blow to eye, or ––
OculomotorOculomotor
nerve injury, ornerve injury, or––
Normal inequality.Normal inequality.
Head Trauma AssessmentHead Trauma Assessment
115
Head Trauma AssessmentHead Trauma Assessment
••
Motor ResponseMotor Response––
Is patient able to move all extremities?Is patient able to move all extremities?
––
How do they move?How do they move?••
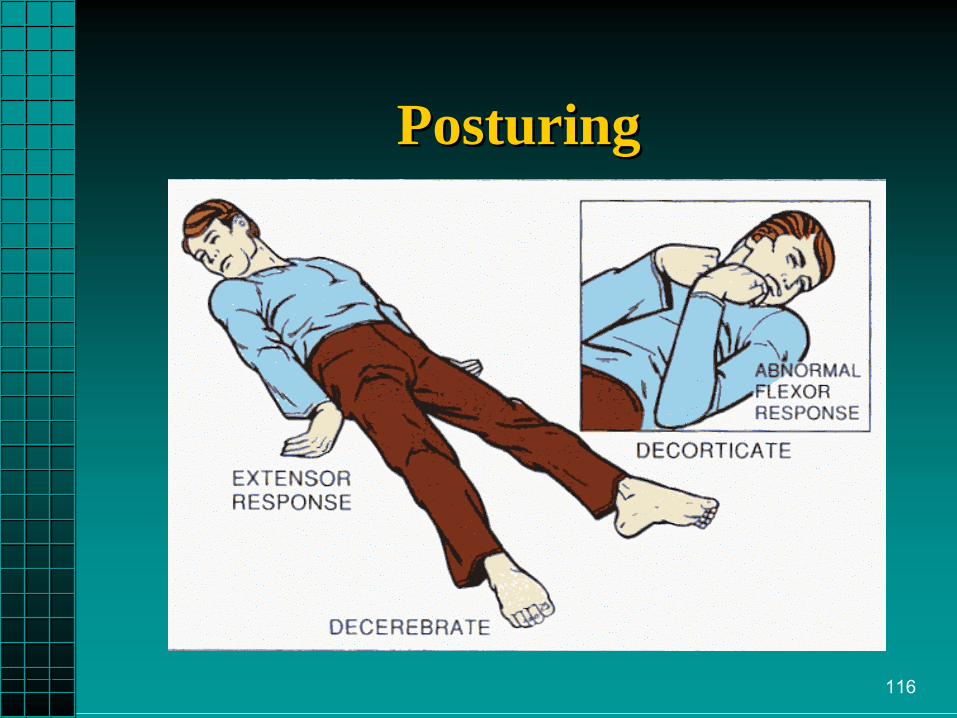
Decorticate.Decorticate.
••
DecerebrateDecerebrate..••
Hemiparesis or Hemiparesis or hemiplegiahemiplegia..
••
Paraplegia or Paraplegia or quadraplegiaquadraplegia..
116
PosturingPosturing
117
••
Motor Response:Motor Response:––
Lateralized/focal signs = lateralized or Lateralized/focal signs = lateralized or focal deficits.focal deficits.
––
Altered motor function may be due to Altered motor function may be due to fracture/dislocation.fracture/dislocation.
Head Trauma AssessmentHead Trauma Assessment
118
••
Vital signs.Vital signs.••
SAMPLE history.SAMPLE history.
••
HeadHead--toto--toe exam, including toe exam, including neurological and GCS.neurological and GCS.
••
Further bandaging and splinting.Further bandaging and splinting.••
Continuous observation.Continuous observation.
Trauma Assessment Trauma Assessment Detailed ExamDetailed Exam

119
Head Trauma AssessmentHead Trauma Assessment
••
Vital Signs:Vital Signs:––
Cushing’s Triad suggests increased Cushing’s Triad suggests increased intracranial pressure.intracranial pressure.••
Increased BPIncreased BP
••
Decreased pulseDecreased pulse••
Irregular respiratory patternIrregular respiratory pattern
120
Head Trauma AssessmentHead Trauma Assessment••
Vital SignsVital Signs––
Isolated head injury will Isolated head injury will NOTNOT cause cause hypotension in adult.hypotension in adult.
––
If hypotension is present, look for another If hypotension is present, look for another life threatening injury of the:life threatening injury of the:••
Chest.Chest.
••
Abdomen.Abdomen.••
Pelvis.Pelvis.
••
Multiple long bone fractures.Multiple long bone fractures.
121
Scene SizeScene Size--UpUp
••
Note mechanism of injury.Note mechanism of injury.••
If the patient is unconscious:If the patient is unconscious:––
Has the patient been moved?Has the patient been moved?
––
Did the patient move on his/her own?Did the patient move on his/her own?––
Has patient LOC or condition changed Has patient LOC or condition changed prior to your arrival?prior to your arrival?
––
Any seizures or posturing?Any seizures or posturing?
122
Management of theManagement of the Head Trauma PatientHead Trauma Patient
••
Stabilize the cStabilize the c--spine.spine.••
Secure and maintain the airway.Secure and maintain the airway.
••
Ventilate at 12 Ventilate at 12 --
15 breaths/min. If available, 15 breaths/min. If available, utilize etCOutilize etCO22
and maintain at 35 mmHg.and maintain at 35 mmHg.••
Prevent hypoxia.Prevent hypoxia.
••
Controlled hyperventilation only with signs of Controlled hyperventilation only with signs of herniationherniation
syndrome:syndrome:
––
Coma, Coma, ↑↑BP, BP, ↓↓Respiration, bradycardia.Respiration, bradycardia.––
Maintain etCOMaintain etCO22
between 32 between 32 ––35 mmHg.35 mmHg.

123
AIRWAY CONTROL CANNOT AIRWAY CONTROL CANNOT BE OVEREMPHASIZEDBE OVEREMPHASIZED
124
HYPERVENTILATION IS HYPERVENTILATION IS NOT RECOMMENDED FOR NOT RECOMMENDED FOR TREATING HEAD INJURY TREATING HEAD INJURY EXCEPT IN THE CASE OF EXCEPT IN THE CASE OF
HERNIATION SYNDROME.HERNIATION SYNDROME.
Maintain mainstream endMaintain mainstream end--tidal tidal carbon dioxide levels carbon dioxide levels
between 32 between 32 --
35 mmHg.35 mmHg.

125
Head Trauma ManagementHead Trauma Management
••
HyperventilationHyperventilation----Benefits Benefits ––
Decreased PaCODecreased PaCO2.2.
––
Vasoconstriction.Vasoconstriction.––
Decreased ICP.Decreased ICP.
••
HyperventilationHyperventilation----RisksRisks––
Decreased cerebral blood flow.Decreased cerebral blood flow.
––
Decreased oxygen delivery to tissues.Decreased oxygen delivery to tissues.––
Increased edema.Increased edema.

126
Patient HistoryPatient History••
May only be able to be obtained from May only be able to be obtained from family or bystanders.family or bystanders.
••
Was there a loss of consciousness?Was there a loss of consciousness?••
Any vomiting? Drugs or alcohol?Any vomiting? Drugs or alcohol?
••
Underlying medical problems?Underlying medical problems?••
Time of accident?Time of accident?
••
Name, age, doctor preference?Name, age, doctor preference?••
SAMPLE.SAMPLE.
127
••
Record baseline exam.Record baseline exam.––
NeuroNeuro, GCS & pupils., GCS & pupils.
––
Vital signs.Vital signs.
••
Maintain good circulation, cerebral perfusion.Maintain good circulation, cerebral perfusion.––
BP 110 mmHg systolic or MAP above 80 mmHg.BP 110 mmHg systolic or MAP above 80 mmHg.
••
Continually monitor and record observations.Continually monitor and record observations.––
DO NOT treat bradycardia.DO NOT treat bradycardia.
••
Prompt transport.Prompt transport.––
Elevate head of Elevate head of spineboardspineboard
15 15 °°..
Head Trauma ManagementHead Trauma Management

128
••
Monitor for hyperthermia. Monitor for hyperthermia. ––
Vasoconstriction.Vasoconstriction.
––
Heat retention. Heat retention. ––
Increased cerebral 0Increased cerebral 022
demand.demand.••
Induced hypothermia may be indicated.Induced hypothermia may be indicated.––
Begin cold (3Begin cold (3°°--
66°°
C)C)
IV fluid bolus at 30 ml/kg to a IV fluid bolus at 30 ml/kg to a
maximum of 2 liters.maximum of 2 liters.––
Place ice packs to head, neck, groin, Place ice packs to head, neck, groin, axillaaxilla, and torso., and torso.
––
Maintain core temperature at 32Maintain core temperature at 32°°
--
3434°°
C.C.––
Secure airway with intubation or advanced airway.Secure airway with intubation or advanced airway.
––
Use Use Etomidate Etomidate and and Norcuron Norcuron to control shivering.to control shivering.––
Dopamine to maintain systolic pressure at 110 mmHg Dopamine to maintain systolic pressure at 110 mmHg or MAP above 80 mmHg. or MAP above 80 mmHg.
Head Trauma ManagementHead Trauma Management
129
••
Drug Therapy Considerations.Drug Therapy Considerations.••
Only after: Only after: ––
Management of ABC’s. Management of ABC’s.
––
Controlled hyperventilation.Controlled hyperventilation.
Head Trauma ManagementHead Trauma Management

130
••
Drug Therapy Considerations.Drug Therapy Considerations.––
Benzodiazepines such as Diazepam Benzodiazepines such as Diazepam (Valium), (Valium), Midazolam Midazolam (Versed), or (Versed), or Lorazepam Lorazepam ((AtivanAtivan).).
••
Anticonvulsant.Anticonvulsant.••
Give if patient experiences seizures.Give if patient experiences seizures.
••
May mask changes in LOC.May mask changes in LOC.••
May depress respirations. May depress respirations.
••
May worsen hypotension.May worsen hypotension.
Head Trauma ManagementHead Trauma Management
131
••
Drug Therapy Considerations.Drug Therapy Considerations.––
Glucose.Glucose.••
Assess blood glucose.Assess blood glucose.
••
Administer only if hypoglycemic.Administer only if hypoglycemic.••
Consider thiamine in malnourished.Consider thiamine in malnourished.
Head Trauma ManagementHead Trauma Management

132
Pitfalls and ProblemsPitfalls and Problems
••
Anticipate cAnticipate c--spine injuries.spine injuries.••
Protect the airway Protect the airway --
prevent aspiration.prevent aspiration.
••
Prevent hypoxia.Prevent hypoxia.••
Prevent shock. Prevent shock. ––
IV fluids to maintain cerebral perfusion.IV fluids to maintain cerebral perfusion.
––
Maintain ventilation and oxygenation.Maintain ventilation and oxygenation.
133
Pitfalls and ProblemsPitfalls and Problems
••
Be prepared for seizures or combative Be prepared for seizures or combative behavior.behavior.
••
Rapidly deteriorating condition requires Rapidly deteriorating condition requires rapid transport.rapid transport.
••
Assess for other causes of altered LOC:Assess for other causes of altered LOC:––
Hypoglycemia.Hypoglycemia.
––
Alcohol.Alcohol.––
Drugs.Drugs.

134
Questions?Questions?