health action in crises global health cluster response to the 2007 iawg call for action dr nevio...
Post on 22-Dec-2015
217 views
TRANSCRIPT

Health Action in Crises
Global Health Cluster response to the 2007 IAWG call for action
Dr Nevio ZagariaRecovery and Transition Programs
Health Action in CrisesWHO
Cairo, November 2008

Health Action in Crises
Structure of the presentation
Normative work Build the case / advocacy Strategic issues for discussion

Health Action in Crises
Normative work

Health Action in Crises
Level of Care
CommunityCare
Primary Care
Secondary & Tertiary Care
General Clinical Services
Child Health
Nutrition
Communicable Diseases
STI & HIV/AIDS
Maternal & Newborn Health
Sexual Violence
Non CommunicableDiseases
Environmental Health
Sub Sectors Initial Key Services
Key Services – Sub Sectors and Level of Care
Rep
rod
uct
ive
Hea
lth
OPD
Vaccinations
TF
EWARS
MISP
Injury Care & Mass Casualty Management
Water Quality Control

Health Action in Crises
Key health services at primary level, by sector

Health Action in Crises
Key health services at community level, by sector

Health Action in Crises
Key health services at secondary level, by sector

Health Action in Crises
Build the case / advocacy

Health Action in Crises

Health Action in Crises
HeRAMS - North Darfur - Health System AnalysisHealth Services Availability (%) in Maternal & Newborn Health, March 2008
Maternal & Newborn HealthAvailability of Services (%) at Primary Care Level in ND
84.3
72.3 72.3
51.8
28.9 31.3
93.596.8 96.8
90.3
48.4 48.4
78.8
57.7 57.7
28.8
17.321.2
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Family Planning * Antenatal Care Postnatal Care Clean & Safe NormalDelivery *
Basic EssentialObstetric Care (BEOC)
Essential NewbornCare
All
Partners
SMoH
Source: State MoH, WHO

Health Action in Crises
* None of the Primary Care Facilities (RH, PHCC, PHCU and Mobile Clinics) of the Admin Unit provides the Service or Package of Services
Maternal & Newborn HealthService monitored: BEOC
Identification of Gaps* in the provision of Key Services & Sub Sectors at the level of Administrative Units
i-HeRAMS – Health Sub Sectors and Key Services Gap Analysis

Health Action in Crises
HeRAMS - North Darfur - Health System AnalysisHealth Services Availability (%) in Sexual Violence, March 2008
Sexual ViolenceAvailability of Services (%) at Primary Care Level in ND
36.1
80.7
18.1 15.7
67.7
90.3
29.0 29.0
17.3
75.0
11.57.7
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Clinical Management ofRape Survivors
Emergency contraception Post Exposure Prophilaxisfor STI&HIV infections
Sexual Violence Package
All
Partners
SMoH
Source: MoH, WHO

Health Action in Crises
* None of the Primary Care Facilities (RH, PHCC, PHCU and Mobile Clinics) of the Admin Unit provides the Service or Package of Services
Sexual ViolencePackage monitored :- Clinical Management of Rape Survivors- Emergency Contraception- PEP for STI & HIV Infections
Identification of Gaps* in the provision of Key Services & Sub Sectors at the level of Administrative Units
i-HeRAMS – Health Sub Sectors and Key Services Gap Analysis

Health Action in Crises
Average number of Staff per Facility Type
1.6
3.7
15.9
0.0
3.4
0.41.6
0.5
2.1 2.0
0.3
1.70.9 0.4
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
MO MA Nurse PHO MW Vacc. LabPerson
Rural Hospitals
PHCC
Rural Hospitals vs PHCCs PHCCs vs PHCUs
HeRAMS - North Darfur - Health System AnalysisStaffing Patterns based on Health Facilities Type, March 2008
Source: State MoH, WHO

Health Action in Crises
Access to Emergency Obstetric Care
Proportion of Caesarean Sections over Expected Births (%) during 2007 North Darfur - March 08
Source: State MoH, WHO
Health Action in Crises
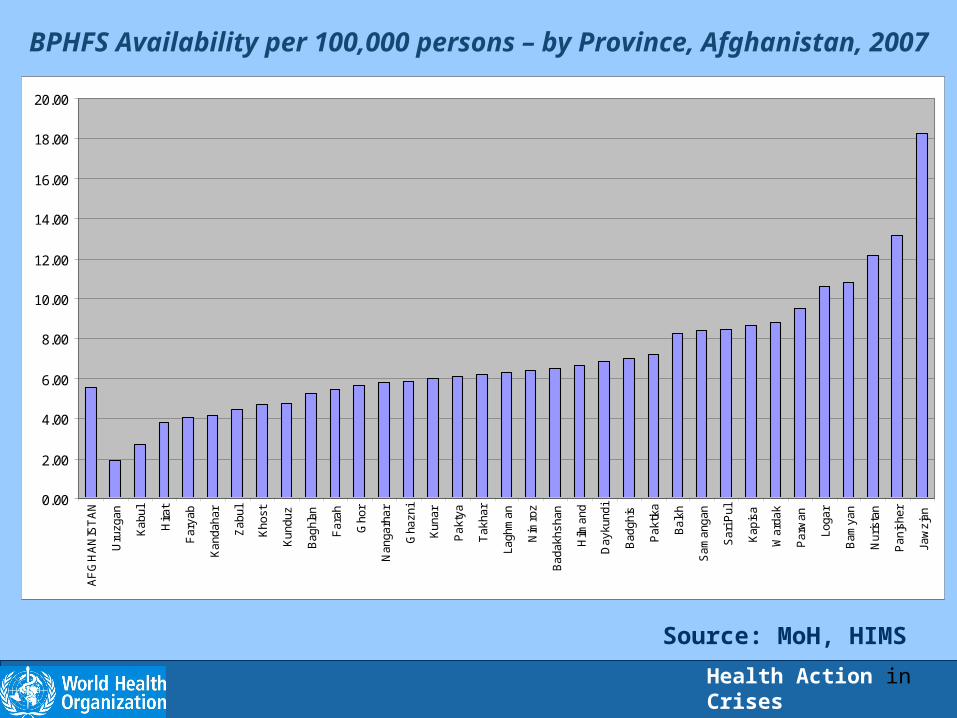
BPHFS Availability per 100,000 persons – by Province, Afghanistan, 2007
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
18.00
20.00A
FG
HA
NIS
TA
N
Uru
zgan
Kab
ul
Hira
t
Far
yab
Kan
daha
r
Zab
ul
Kho
st
Kun
duz
Bag
hlan
Far
ah
Gho
r
Nan
garh
ar
Gha
zni
Kun
ar
Pak
tya
Tak
har
Lagh
man
Nim
roz
Bad
akhs
han
Hilm
and
Day
kund
i
Bad
ghis
Pak
tika
Bal
kh
Sam
anga
n
Sar
i Pul
Kap
isa
War
dak
Par
wan
Loga
r
Bam
yan
Nur
ista
n
Pan
jshe
r
Jaw
zjan
Source: MoH, HIMS
Health Action in Crises
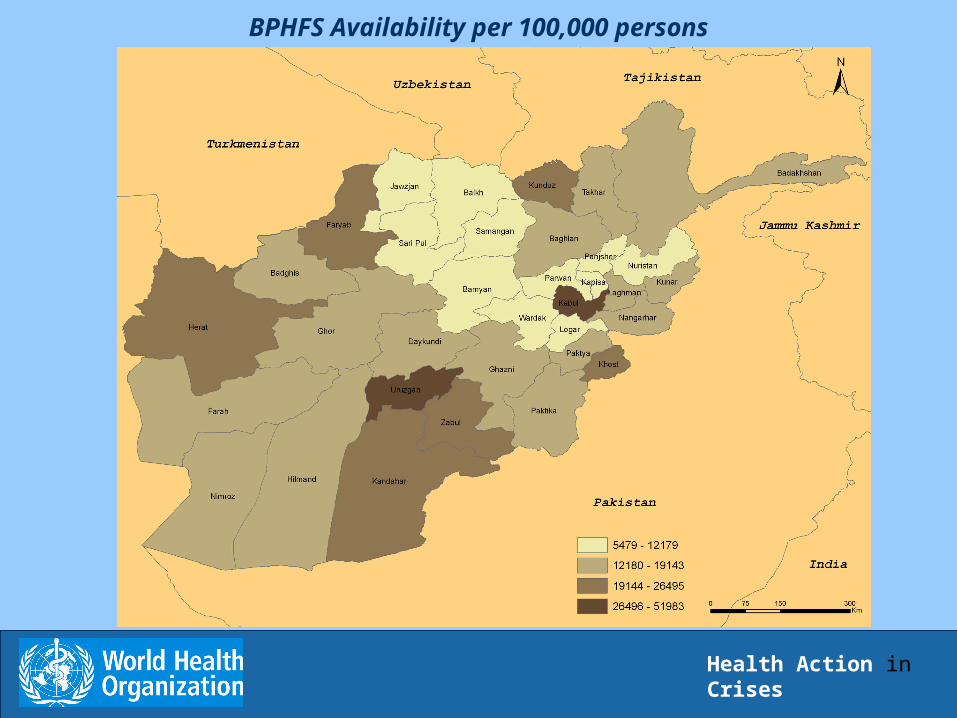
BPHFS Availability per 100,000 persons

Health Action in Crises
District Hospitals Availability per 100,000 persons – by Province
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1.40
AF
GH
AN
IST
AN
Nim
roz
Par
wan
Kho
st
Kun
ar
Uru
zgan
Lagh
man
Nur
ista
n
Kan
daha
r
Kun
duz
Bad
akhs
han
Nan
garh
ar
Gho
r
Kab
ul
Hira
t
Gha
zni
Sar
i Pul
Far
ah
Far
yab
Bad
ghis
Hilm
and
Day
kund
i
Bag
hlan
Kap
isa
Sam
anga
n
Tak
har
Zab
ul
Pak
tya
Bam
yan
Pak
tika
War
dak
Loga
r
Bal
kh
Pan
jshe
r
Jaw
zjan
Source: MoH, HIMS
Health Action in Crises
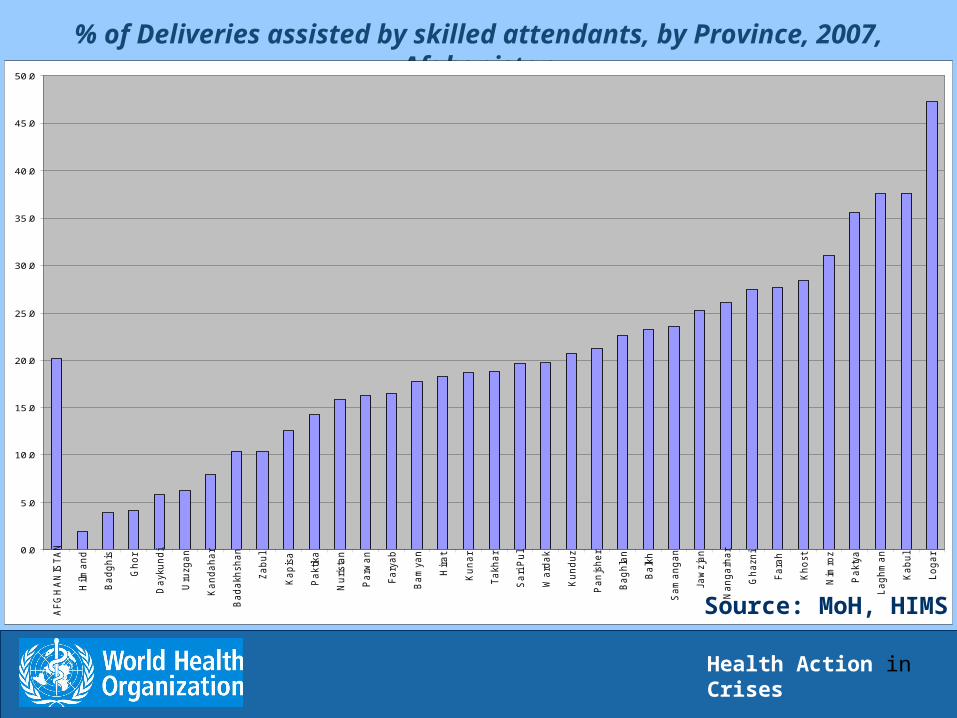
% of Deliveries assisted by skilled attendants, by Province, 2007, Afghanistan
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
AF
GH
AN
IST
AN
Hilm
an
d
Ba
dg
his
Gh
or
Da
yku
nd
i
Uru
zg
an
Ka
nd
ah
ar
Ba
da
kh
sh
an
Za
bu
l
Ka
pis
a
Pa
ktika
Nu
rista
n
Pa
rwa
n
Fa
rya
b
Ba
mya
n
Hir
at
Ku
na
r
Ta
kh
ar
Sa
ri P
ul
Wa
rda
k
Ku
nd
uz
Pa
njs
he
r
Ba
gh
lan
Ba
lkh
Sa
ma
ng
an
Ja
wzja
n
Na
ng
arh
ar
Gh
azn
i
Fa
rah
Kh
ost
Nim
roz
Pa
kty
a
La
gh
ma
n
Ka
bu
l
Lo
ga
r
Source: MoH, HIMS

Health Action in Crises
% of CS performed over Expected Deliveries in 2007, by Province, Afghanistan
0.00
0.50
1.00
1.50
2.00
2.50
3.00
AF
GH
AN
IST
AN
Hilm
an
d
Nim
roz
Nu
rista
n
Ka
pis
a
Gh
or
Pa
kty
a
Ba
dg
his
Uru
zg
an
Da
yku
nd
i
Pa
rwa
n
Sa
ri P
ul
Ku
na
r
Ja
wzja
n
La
gh
ma
n
Fa
rya
b
Za
bu
l
Ka
nd
ah
ar
Pa
njs
he
r
Ba
da
kh
sh
an
Ba
gh
lan
Ba
mya
n
Ku
nd
uz
Na
ng
arh
ar
Gh
azn
i
Sa
ma
ng
an
Lo
ga
r
Wa
rda
k
Fa
rah
Kh
ost
Ta
kh
ar
Ba
lkh
Pa
ktika
Hir
at
Ka
bu
l
Source: MoH, HIMS

Health Action in Crises
% of Caesarean Sections over Expected Deliveries, by Province, Afghanistan 2007
Source: MoH, HIMS

Health Action in Crises
Strategic issues for discussion

Health Action in Crises
Crisis-affected areas
Humanitarian Space:
Defined by political and security considerations
("potential humanitarian coverage")
Access to beneficiaries:
Defined by security considerations, resource availability and programme management capacities
("operational humanitarian coverage")
Affected area, humanitarian space, access to beneficiariesand access to services
movingmoving
Beneficiaries' access to assistance/services:
•Geographical
•Functional
•Cultural
•Financial
("service coverage")
(its extension is a sectoral objective)

Health Action in Crises
KEY CHALLENGE FOR HEALTH SECTOR IN PROTRACTED CRISIS AND IN RECOVERY
Need for simultaneously:– protect lives and reduce disease, malnutrition and disabilities
among the vulnerable populations in the affected areas (the humanitarian imperative),
– strengthen the institutional capacity to pursue longer term health development goals including the health and nutrition related MDGs, to discharge the essential public health functions, to provide critical health services and to extend social protection in health (the developmental imperative).

Health Action in Crises
Basic Premises
The impact of purely humanitarian health and nutrition relief interventions approaches its limits
Need for intensifying actions of institutional capacity building among national counterparts (including non State actors where relevant) in order scale up the priority public health interventions that need to be put in place

Health Action in Crises
Development
Before After
Emergency Response
Reconstruction
RecoveryDevelopment
A thinking shift is needed?

Health Action in Crises
Health System Building Blocks
(Taken from: Strengthening
Health Systems to Improve Health
Outcomes: WHO's Framework for Action, WHO,
2007).

Health Action in Crises
Leadership and Governance Humanitarian principles, negotiation of humanitarian access
Shadow alignment: key stakeholders' role in supporting structures, institutions or systems that are compatible with the existing or potential organization of the state
Decentralization, building back better
New environment generated by the Humanitarian Reform and the Cluster Approach in particular: new coordination or partnership relationships across the stakeholders ?
Contracting health services to non state actors

Health Action in Crises
Service Delivery
Basic Health Packages: how to move from MISP to comprehensive RH services and achieve high coverage?
Inclusive design and planning of "transitional" standards for service delivery: present agreed standards do not meet the challenges, how to reach high coverage of all MISP component in areas with disrupted health systems?
Health Action in Crises
Issues for discussion on RH in crisis
Take into account the implications of the adoption of the cluster approach in areas in crisis, and adapt the MISP accordingly
Identify common problem in scaling up MISP in protracted crisis before moving to comprehensive RH
RH support to field actors within Health Cluster Coordinator’s functions