health and human services transformation · identified on the basis of a claim with a behavioral...
TRANSCRIPT

Health and Human Services Transformation
Medicaid Waiver Advisory Council
Behavioral Health Transformation
May 23, 2018

DRAFT Confidential – Proprietary and Pre-decisional 1
FY2015 members and spend1,2
Medicaid individuals with diagnosed behavioral health needs make up ~25% of the population, but ~56% of the total spend
44%
48%
8%
7%6%
62%
25%
0%
Individuals with diagnosedbehavioral health needs5
Spend
10.53.1
Members
Medical spend4
Behavioral health core spend3
Individuals with only carecoordination fee spend6
Spend for non-behavioralhealth members
Individuals with no claims
Individuals with no diagnosedbehavioral health needs5
100% =
Spend for members with onlycare coordination fee spend6
1 Annualized members (not unique members) shown here with no exclusions made on population or spend. Annualized member count = Sum of member months/12 2 Most inclusive definition of behavioral health population used here of members who are diagnosed and treated, diagnosed but not treated, and treated but no diagnosis
present. Behavioral health core spend defined as all spend with a behavioral health primary diagnosis or behavioral health-specific procedure, revenue, or HIC3 pharmacy code.
3 Behavioral health core spend is defined as spend on behavioral health care for individuals with behavioral health needs4 Medical spend is defined as all other spend for individuals with behavioral health needs. See appendix for additional methodology notes5 Behavioral health diagnosis is defined as a behavioral health diagnosis in any of the first 18 diagnosis fields of any claim during the year. Behavioral health treatment is
identified on the basis of a claim with a behavioral health primary diagnosis or a behavioral health-specific procedure, revenue, of HIC3 drug code during the year6 Annualized members with only spend for care coordination fees. Care coordination fee is identified by HCPCS codes - G9002, G9008
Annualized members (millions), dollars (billions)
SOURCE: FY15 State of Illinois DHFS claims data

DRAFT Confidential – Proprietary and Pre-decisional 2
Behavioral healthcore spend
109
Medical spend
11294988483
157
121387
80829087
8483
5581778784 86
90
36100
Each bar represents5% of customers: ~18K customers
Distribution of Medicaid behavioral health primary population1 by behavioral health core spend rank
Total spend = $2,550M
5% most costly customers bybehavioral health core spend
5% least costly customers by behavioral health core spend
In Illinois, the costliest 10% of Medicaid members account for 72% of behavioral health spend
SOURCE: FY15 State of Illinois DHFS claims data
The top 10% highest spend behavioral health customers account for:▪ 72% of core behavioral health spend▪ 30% of the total Medicaid spend of
the behavioral health population
1 Distribution of unique members shown here2 Primary population defined as Medicaid members with behavioral health needs minus those who have been treated but not diagnosed and those who have been diagnosed but not treated.
It also excludes those with dual eligibility or non-continuous eligibility or third-party liability, It also excludes those who died during their inpatient stays

DRAFT Confidential – Proprietary and Pre-decisional 3
Informed by stakeholders and customer archetypes, Illinois envisions a member-centric behavioral health system enabled by ten key elements
Data inter-operability
and transparency
High intensity assessment,
care planning, and care
coordination / integration
6
Low-intensity assessment,
care planning, and care
coordination / integration
7
8
Structure, budgeting, and policy
support
10
Integrated, digitized
member data
2
Enhanced identification, screening &
access
1
Best practice vendor and
contract management
9
The nation’s leading member-
centric behavioral
health strategy
Core and preventive behavioral
health services
3
Behavioral health support
services
4
Workforce and system
capacity
5

DRAFT Confidential – Proprietary and Pre-decisional 4
Rebalance the behavioral health ecosystem, reducing overreliance on institutional care and shifting to community-based care 1
Promote integrated delivery of behavioral and physical health care for behavioral health members with high needs2
Promote integration of behavioral health and primary care for behavioral health members with low needs3
Support the development of robust and sustainable behavioral health services that provide both core and preventative care to ensure that members receive the full complement of high-quality treatment they need
4
Invest in additional support services to address the larger needs of behavioral health patients, such as housing and employment services5
Create an enabling environment to move behavioral health providers toward outcomes- and value-based payments 6
Illinois has identified 6 goals it hopes to achieve through this waiverA

DRAFT Confidential – Proprietary and Pre-decisional 5
Other demon-strationgrants
1115waiver
Other waivers
Advance Planning
Documents
State Plan Amendments
General revenue
funds

DRAFT Confidential – Proprietary and Pre-decisional 6
STATE PLAN AMENDMENTS
DESCRIPTION PROPOSED EFFECTIVE DATE
Medication Assisted Treatment January 2017
Mobile Crisis Response Summer 2018
Crisis Stabilization Summer 2018
Uniform Child and Adolescent Needs and Strengths (CANS) and Adult Needs and Strengths Assessment (ANSA)
Summer 2018
Integrated Physical and Behavioral Health Homes October 2018
DRAFT Confidential – Proprietary and Pre-decisional 7
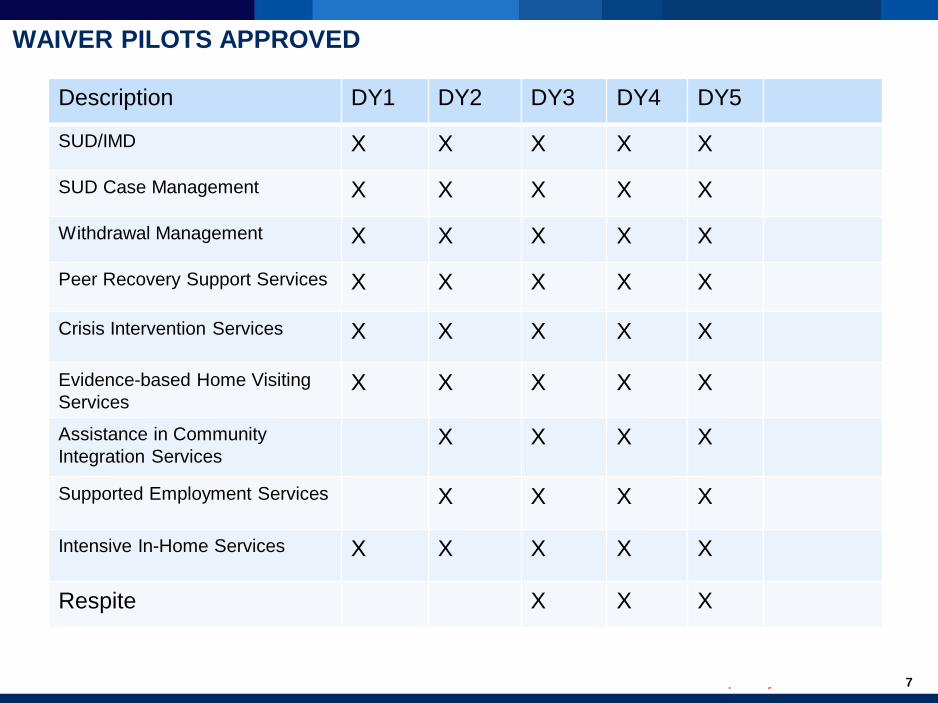
WAIVER PILOTS APPROVED
Description DY1 DY2 DY3 DY4 DY5
SUD/IMD X X X X X
SUD Case Management X X X X X
Withdrawal Management X X X X X
Peer Recovery Support Services X X X X X
Crisis Intervention Services X X X X X
Evidence-based Home Visiting Services
X X X X X
Assistance in Community Integration Services
X X X X
Supported Employment Services X X X X
Intensive In-Home Services X X X X X
Respite X X X
DRAFT Confidential – Proprietary and Pre-decisional 8
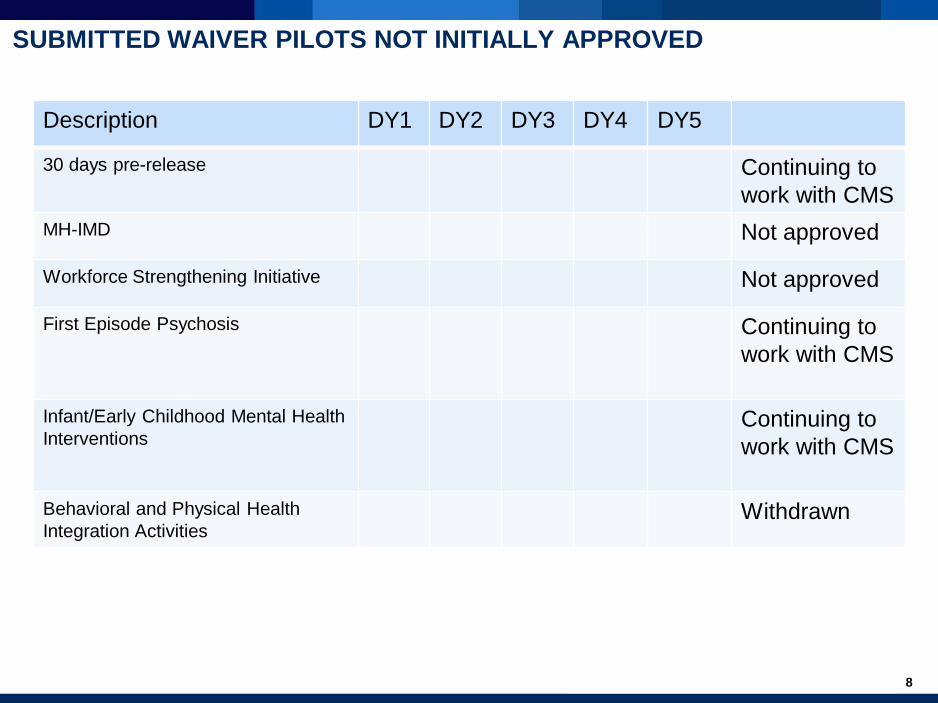
SUBMITTED WAIVER PILOTS NOT INITIALLY APPROVED
Description DY1 DY2 DY3 DY4 DY5
30 days pre-release Continuing to work with CMS
MH-IMD Not approved
Workforce Strengthening Initiative Not approved
First Episode Psychosis Continuing to work with CMS
Infant/Early Childhood Mental Health Interventions
Continuing to work with CMS
Behavioral and Physical Health Integration Activities
Withdrawn

DRAFT Confidential – Proprietary and Pre-decisional 9
WAIVER PILOTS
Description EligibilityGeographic Recipient
SUD/IMD X
SUD Case Management X
Withdrawal Management X
Peer Recovery Support Services X
Crisis Intervention Services X
Evidence-based Home Visiting Services X
Assistance in Community Integration Services X
Supported Employment Services X
Intensive In-Home Services X
Respite X

DRAFT Confidential – Proprietary and Pre-decisional 10
INTEGRATED HEALTH HOMES

DRAFT Confidential – Proprietary and Pre-decisional 11
Integrated Health Homes in Illinois are: Integrated Health Homes in Illinoisare NOT:
… and NOT on the provision of all services▪ Provider of all services for members▪ A gatekeeper restricting a member’s choice of
providers▪ A physical place where all Integrated Health
Home activities occur▪ A care coordination approach that is the
same for all members regardless of individual needs
Primary focus is on coordination of care…▪ Integrated, individualized care planning and
coordination resources, spanning physical, behavioral and social care needs
▪ An opportunity to promote quality in the core provision of physical and behavioral health care
▪ A way to encourage team-based caredelivered in a member-centric way
▪ A way of aligning financial incentives around evidence-informed practices, wellness promotion, and health outcomes
For members with the highest needs:▪ A means of facilitating high intensity,
wraparound care coordination▪ An opportunity to obtain enhanced match for
care coordination needs▪ Identifying enhanced support to help these
members and their families manage complex needs (e.g., housing, justice system)
What an Integrated Health Home is and is not

DRAFT Confidential – Proprietary and Pre-decisional 12
Managed Care Organizations
Payment streams, in response to Integrated Health Homes meeting requirements and improving outcomes
Higher-intensity Integrated Health Homes
Lower intensity Integrated Health Homes
Integrated Health Homes
Higher-needs population1 Lower-needs population1
1 Actual tiering of intensity of care coordination may not be binary
JaneBrice Mike Mia Stephen DarnellAshley Tom William JennGreg CynthiaConnorJerry
Population health
management
Member engagement
and education
Physical/ maternal
health provider
engagement
Behavioral health provider
engagement
Integrated care planning and monitoring
Supportive service
coordination
Reporting of quality and efficiency of care (i.e., member outcomes)
Enhanced access, screening, and assessment
Integrated Health Homes will deliver improvements in care delivery across a range of areas
DRAFT Confidential – Proprietary and Pre-decisional 13
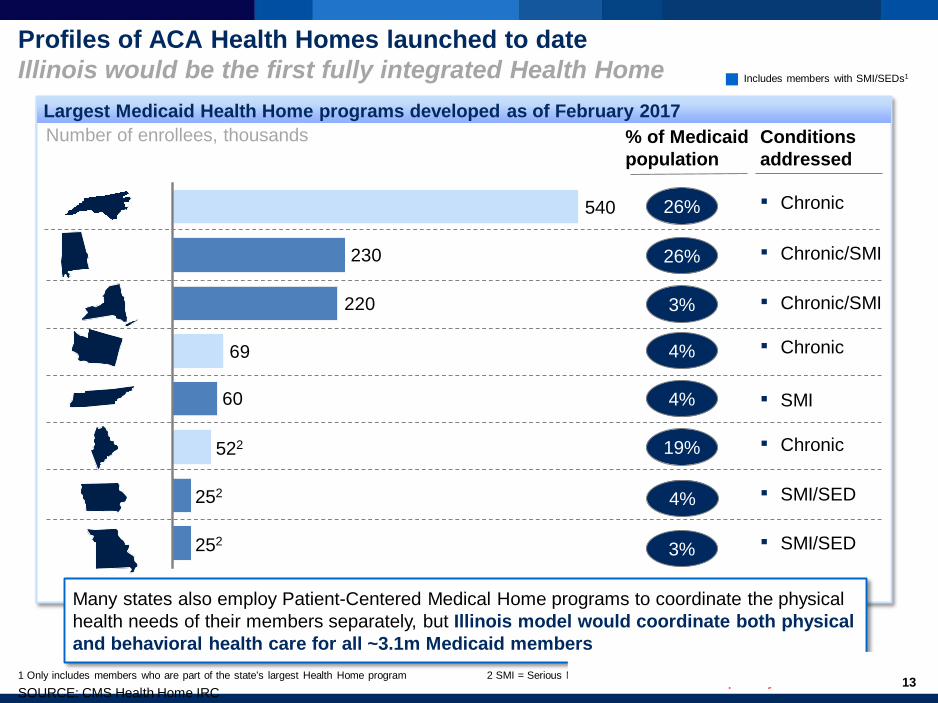
Profiles of ACA Health Homes launched to dateIllinois would be the first fully integrated Health Home
Largest Medicaid Health Home programs developed as of February 2017
60
69
220
230
252
252
522
540 26%
26%
3%
19%
4%
3%
Number of enrollees, thousands
Many states also employ Patient-Centered Medical Home programs to coordinate the physical health needs of their members separately, but Illinois model would coordinate both physical and behavioral health care for all ~3.1m Medicaid members
Conditions addressed
▪ Chronic
▪ Chronic/SMI
▪ Chronic/SMI
▪ SMI
▪ Chronic
▪ SMI/SED
% of Medicaid population
1 Only includes members who are part of the state’s largest Health Home program 2 SMI = Serious Mental Illness; SED = Serious Emotional Disturbance
4%
4%
▪ SMI/SED
▪ Chronic
Includes members with SMI/SEDs1
SOURCE: CMS Health Home IRC

DRAFT Confidential – Proprietary and Pre-decisional 14
Principles for developing care delivery model
Develop a person- and family-centered care delivery model for the whole Medicaid population, regardless of match status, that encourages member and family engagement
Craft a flexible care delivery approach that reflects the diverse needs of members in Illinois and recognizes that member needs change over time
Evolve toward full clinical integration of behavioral, physical, and social healthcare
Acknowledge and accommodate geographical variation in provider capabilities, readiness, and priorities
Strike an appropriate balance between provider flexibility and accountability to enable capabilities and readiness
Prioritize economic sustainability of care delivery model at both the systemic and provider levels

DRAFT Confidential – Proprietary and Pre-decisional 15
Overview of potential approach to IHH member stratification
Level of physical health needs
Level of behav-ioralhealth needs
Low
High
High Low
High behavioral health needs,Low physical health needs
High-estneeds
Low behavioral
health needs, high physical health needs
Low needs members
Moderate needs members
ILLUSTRATIVE
Full Medicaid population will be included in the model, with exception of those receiving duplicative care coordination, in LTC facilities after 90 days, or with MMAI dual, partial eligibile, or TPL status
Approach to tiering adopted to ensure members with similar needs receive comparable care coordination support, and to focus resources on those members who need greatest support
A