health care coverage for louisiana individuals &...
TRANSCRIPT

This brochure is not a contract. It is intended solely to provide you with a general overview of ourhealth insurance products. Complete details of benefits, terms and exclusions that apply to yourhealth care coverage are governed by the Individual Membership Agreement filed with the State ofLouisiana. CoventryOne is underwritten by Coventry Health Care of Louisiana, Inc.
CoventryOneCoventry Health Care of Louisiana, Inc.
3838 N. Causeway Blvd.Suite 3350
Metairie, LA 70002
Health Care Coverage for Louisiana Individuals & Families
...the One making health insurance more affordable.
37966_PktFldr 10/30/06 3:45 PM Page 1
CoventryOne is health insurance for
individuals offered through Coventry Health Care of
Louisiana, Inc., an affiliate of Coventry Health Care, Inc.
a Fortune 500 company which delivers affordable health
coverage to over 3.7 million members nationwide.
Coventry Health Care of Louisiana has been delivering
quality, affordable health coverage to residents of the
New Orleans and Baton Rouge metropolitan areas for over
twenty years.
CoventryOne is ideal for self-employed individuals, part-time
employees, singles or families. We offer several plans to
choose from, including low-cost, high-deductible plans which
can be used with a Health Savings Account (HSA).
37966_PktFldr 10/30/06 3:45 PM Page 2

About the PlansCoventryOne gives you direct access to specialists without requiring referrals. All plans allow youto choose, each time you need medical services, whether or not you use a health care providerthat participates in Coventry Health Care of Louisiana’s ProviderNetwork. By using a network provider you significantly reduceyour out-of-pocket costs and avoid the paper work involved withfiling claims. To verify if your doctor or hospital is in our network,simply visit our website at www.chclouisiana.com and click on“Search for Provider”, located on the upper right corner of the page and then click on “CHC of LA Provider Search”
EligibilityEligible persons are healthy individuals between the ages of 30 days and 64 years, 11 months,who reside in participating Louisiana parishes. Spouses and children are considered as independent applicants and all applicants must reside in the service area. Please refer to theservice area map located in the back pocket of this brochure.
Covered services*
QQuuaalliittyyhealth care
• Hospital and surgical care
• Routine gynecological exams
• Prescription drug coverage
• Pap tests and mammograms
• Emergency room care
• Home health care
• Urgent care centers
• Routine eye exams
• Ambulance services
• Immunizations for adults and children
• Durable medical equipment and supplies
• Doctor’s office visits
• Diagnostic services
• Routine physicals
• Specialist visits
• Preventative Care
*Copays, deductible, coinsurance and limitations may apply.
37966 Coventry Txt 11/21/06 5:34 PM Page 1

Coverage cost andpremium paymentsYou choose the deductible and coinsurance level that best meets your needs and budget, fromthe enclosed product grids. Use the enclosed rate cards and calculation sheet to determine yourmonthly premium.
Premium can only be paid via automatic debit from either your checking or savings account.Premium is deducted on the 10th day of each month. Your first premium payment will not bededucted from your bank account until the 10th day following the effective date of coverage.
Signing upFully complete, sign and date theApplication/Health StatementForm (application is valid for 60days from the signature date on theapplication). Indicate the plan youhave selected by checking off theappropriate box or boxes on the PlanSelection Sheet and signing it.
Fax the completedApplication/Health Statement Form and the Plan Selection Sheet to:CoventryOne Individual Underwriting Dept.Fax toll-free: (866) 560-6328
When coverage beginsThe earliest coverage can begin is the first of the month following underwriting review and written acceptance of theapplication. Allow a minimum of 15 days to review and process your application. Applications for coverage may be denied based upon the health status of the applicant.
AAffffoorrddaabblleepremiums
Coventry One Individual Point-of-Service Plan Selection Sheet� STEP 1: Choose a Point-of-Service (POS) Plan and place a check mark next to that item.
� STEP 2: Choose Pharmacy Plan A or Plan B and place a check mark next to that item.
� Pharmacy Plan A: $0 Deductible, $10 Tier One Copay; $35 Tier Two Copay; $60 Tier Three Copay; $100 Self-Administered Injectables Copay
� Pharmacy Plan B: $250 Calendar Year Deductible, $10 Tier One Copay; $35 Tier Two Copay; $60 Tier Three Copay; $100 Self-
Administered Injectables Copay
� POS Plan $500 20%: Office Visits $40, Emergency Room
$200, Deductible $500, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $1,500; Out-of-Network: Deductible
$1,000, Coinsurance 40%, Out-of-Pocket Maximum $3,000
� POS Plan $750 20%: Office Visits $40, Emergency Room
$200, Deductible $750, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $1,750; Out-of-Network: Deductible
$1,500, Coinsurance 40%, Out-of-Pocket Maximum $3,500
� POS Plan $1,000 20%: Office Visits $40, Emergency Room
$200, Deductible $1,000, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $2,000; Out-of-Network: Deductible
$2,000, Coinsurance 40%, Out-of-Pocket Maximum $4,000
� POS Plan $1,500 20%: Office Visits $40, Emergency Room
$200, Deductible $1,500, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $2,500; Out-of-Network: Deductible
$3,000, Coinsurance 40%, Out-of-Pocket Maximum $5,000
� POS Plan $2,500 20%: Office Visits $40, Emergency Room
$200, Deductible $2,500, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $3,500; Out-of-Network: Deductible
$5,000, Coinsurance 40%, Out-of-Pocket Maximum $7,000
� POS Plan $5,000 20%: Office Visits $40, Emergency Room
$200, Deductible $5,000, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $6,000; Out-of-Network: Deductible
$10,000, Coinsurance 40%, Out-of-Pocket Maximum $12,000
� POS Plan $500 50%: Office Visits $40, Emergency Room
$200, Deductible $500, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $3,000; Out-of-Network: Deductible
$1,000, Coinsurance 50%, Out-of-Pocket Maximum $6,000
� POS Plan $750 50%: Office Visits $40, Emergency Room
$200, Deductible $750, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $3,250; Out-of-Network: Deductible
$1,500, Coinsurance 50%, Out-of-Pocket Maximum $6,500
� POS Plan $1,000 50%: Office Visits $40, Emergency Room
$200, Deductible $1,000, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $3,500; Out-of-Network: Deductible
$2,000, Coinsurance 50%, Out-of-Pocket Maximum $7,000
� POS Plan $1,500 50%: Office Visits $40, Emergency Room
$200, Deductible $1,500, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $4,000; Out-of-Network: Deductible
$3,000, Coinsurance 50%, Out-of-Pocket Maximum $8,000
� POS Plan $2,500 50%: Office Visits $40, Emergency Room
$200, Deductible $2,500, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $5,000; Out-of-Network: Deductible
$5,000, Coinsurance 50%, Out-of-Pocket Maximum $10,000
� POS Plan $5,000 50%: Office Visits $40, Emergency Room
$200, Deductible $5,000, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $7,500; Out-of-Network: Deductible
$10,000, Coinsurance 50%, Out-of-Pocket Maximum $15,000
Name Printed
Signature Date
Notes:
• Annual Deductible and Out-of-Pocket Maximum coincide
with your contract year.
• Lab and X-rays are covered in full in Network.
• Out-of-Pocket Maximum includes copays, Deductible
and Coinsurance.
• Family Deductible and Out-of-Pocket = 2x Individual.
• Coinsurance reflects member responsibility.
• Payment for covered services received Out-of-Network is
based upon Coventry’s Out-of-Network reimbursement rates.
In addition to your Coinsurance, you are responsible for
paying Out-of-Network providers the difference between the
Out-of-Network rate and their actual charges for
non-emergency services.
37966 Coventry Txt 11/21/06 5:34 PM Page 2
Online servicesOur website makes managing your health easy. Besides searching for providers, CoventryHealth Care members can download forms, order ID cards, review claim status, ask questionsand check the status of new prescription requests. Or they can simply call Member Services toreceive prompt, one-on-one attention.
Policy LimitationsServices that are not covered include, but are not limited to:
We may also exclude coverage for pre-existing medical conditions for a period of 12 months from the effective date of the policy. A pre-existing condition is a condition for which medical advice, diagnosis,care, treatment, or prescribed drug was recommended or received within the 12-month period prior to youreffective date of coverage. All pre-existing condition exclusions may be reduced for time served under aprior plan’s coverage as per state and federal regulations.
Canceling coverageYou may cancel your coverage for any reason by written notice to us. Such cancellation would beeffective the last day of the month in which we received notice.
We may terminate your coverage for non-payment of premium, fraud, material misrepresentation,loss of eligibility, relocation outside of our service area, repeatedly refusing to accept procedures ortreatment recommended by a Participating Physician and/or impairing the physician’s ability tocoordinate your care, failure to cooperate in the coordination of benefits, and if we discontinue theproduct through which your coverage is provided.
For more informationContact your authorized CoventryOne agent or email us at [email protected].
• Maternity care• Treatment of mental disorders or alcohol
and/or drug abuse• Cosmetic services & surgery• Eyeglasses & corrective lenses• Services not medically necessary• Family planning, sterilization & infertility
• Experimental procedures or treatments• Corrections for refractive errors of the eye• Food or food supplements• Custodial care• Dental services• Treatment for obesity• Foot care
RReelliiaabblleecoverage
37966 Coventry Txt 11/21/06 5:34 PM Page 3

VViissiioonnscreening & discounts
Vision Benefitsavailable through Avesis Incorporated,Vision Provider ServiceCore Benefit – Services to be provided to members covered under a CoventryOne POS or HDHP plan
Eye ExaminationsEye exams (one per year) to include a comprehensive exam with dilation, which includes, but isnot limited to, the following:
• Case History
• External and Internal eye health examinations to include direct and/or indirect
ophthalmoscopy
• Neurological Integrity – oyoillary reflexes and extra ocular muscle assessment
• Biomicroscopy
• Visual Field screening
• Tonometry (glaucoma testing)
• Refractive analysis (determining prescriptions
for eyewear)
• Dilation BIO, and/or Volk fundus lenses
• Binocular Function tests
• Diagnosis and Treatment Plan
$15 CopayProviders agree to provide a 20% discount off of UCR to Members for frames, lenses and allother noncovered eye care services/materials
For Provider updates, please check the Avesis website at: www.avesis.com
37966 Coventry Txt 11/21/06 5:34 PM Page 4

Value-Added ProgramsAs a CoventryOne member, you will receive valuable discounts on health care products andservices through the following programs:
United Networks of America Nutritional Supplements
• Save up to 40% on nutritional supplements through www.qmd-una.com• Save up to 33% on retail prices when you check out by entering your ID information
United Networks of America Smoking Cessation• Save up to 45% on retail FDA-approved cessation devices• Free Stop Smoking Program
Doctor On-Call• Save 50% on membership, which gives you access to 240
board-certified physicians to answer your medical questions, 24/7
United Networks of America Discount Drug Card
• With a United Networks of America Discount Drug Card, you can save up to 75% on drugs NOT covered by your health plan. Pharmacies such as Rite-Aid, CVS, Phar-Mor, Wal-Mart, Eckerd, Publix, Winn Dixie, Kroger, Safeway, Medicine Shoppe and Target participate in the program.
LLoouuiissiiaannaalagniappe
37966 Coventry Txt 11/21/06 5:34 PM Page 5
Value-Added Programscontinued
Louisiana Dental Plan (LDP)• Save up to 70% on LDP Provider fees for dentistry and orthodontics• Discounts apply to routine procedures, restorative, crowns & bridge work, endodontics,
oral surgery, prosthetics, periodontics and orthodontics
USVisionPlan.comThe following discounts are in addition to your benefits offered by Avesis:
• Save up to 60% on eye exams, glasses, contact lenses, LASIK surgery, sunglasses & accessories
• Ophthalmologists & optometrists featured in a Discount Preferred Provider Network (DPPN)
United Networks of America Hearing Benefits• Free UNA hearing tests, office visits and evaluations plus a 20% discount on all hearing
devices purchased through an authorized provider
American Cosmetic SurgeryNetwork
• Save 20% on provider physicians’ fees including breast augmentation, liposuction, laser surgery, facelift, tummy tuck and more
United Networks of America Massage Therapy• Save up to 55% on UNA provider fees• Save up to 15% on products
37966 Coventry Txt 11/21/06 5:34 PM Page 6
As a CoventryOne member, you will have access to the CoventryWellBeing Program ePhit. ePhit is an onlinepersonal health improvement training program to enhance your overall WellBeing.
37966 Coventry Txt 11/21/06 5:35 PM Page 7

37966 Coventry Txt 11/21/06 5:35 PM Page 8
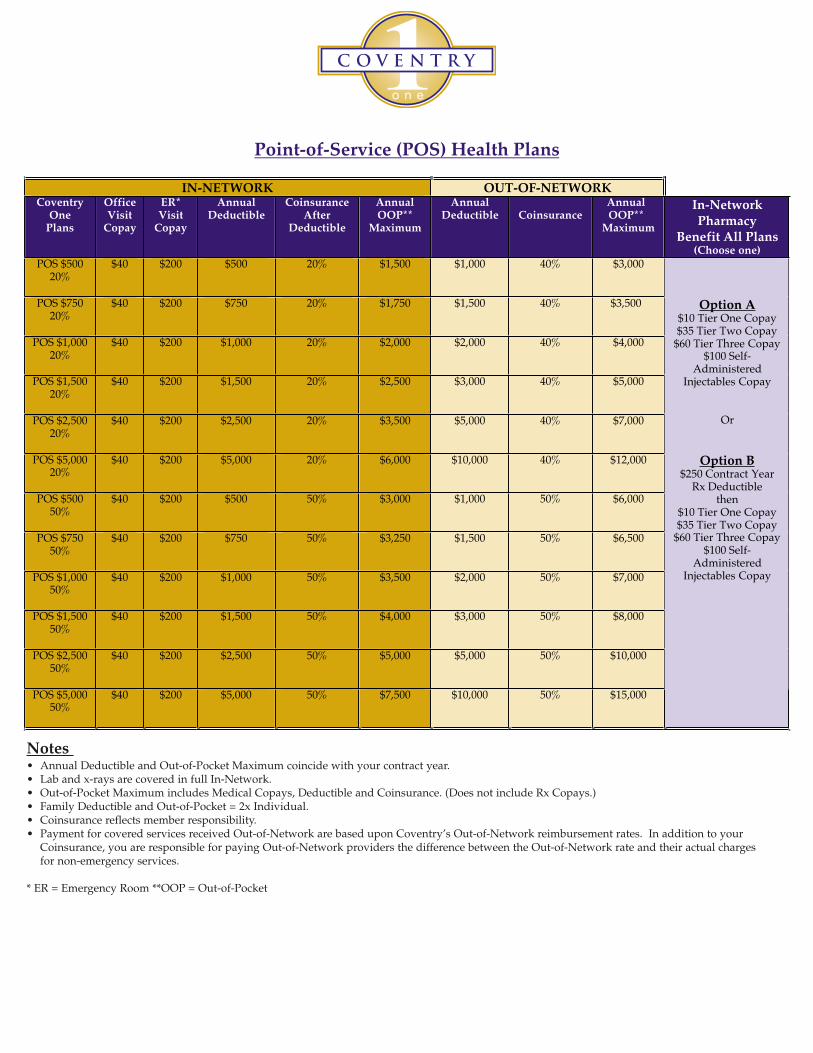
Point-of-Service (POS) Health Plans
IN-NETWORK OUT-OF-NETWORKCoventry
OnePlans
OfficeVisit
Copay
ER*Visit
Copay
AnnualDeductible
CoinsuranceAfter
Deductible
AnnualOOP**
Maximum
AnnualDeductible Coinsurance
AnnualOOP**
Maximum
In-NetworkPharmacy
Benefit All Plans(Choose one)
POS $50020%
$40 $200 $500 20% $1,500 $1,000 40% $3,000
POS $75020%
$40 $200 $750 20% $1,750 $1,500 40% $3,500
POS $1,00020%
$40 $200 $1,000 20% $2,000 $2,000 40% $4,000
POS $1,50020%
$40 $200 $1,500 20% $2,500 $3,000 40% $5,000
POS $2,50020%
$40 $200 $2,500 20% $3,500 $5,000 40% $7,000
POS $5,00020%
$40 $200 $5,000 20% $6,000 $10,000 40% $12,000
POS $50050%
$40 $200 $500 50% $3,000 $1,000 50% $6,000
POS $75050%
$40 $200 $750 50% $3,250 $1,500 50% $6,500
POS $1,00050%
$40 $200 $1,000 50% $3,500 $2,000 50% $7,000
POS $1,50050%
$40 $200 $1,500 50% $4,000 $3,000 50% $8,000
POS $2,50050%
$40 $200 $2,500 50% $5,000 $5,000 50% $10,000
POS $5,00050%
$40 $200 $5,000 50% $7,500 $10,000 50% $15,000
Option A$10 Tier One Copay$35 Tier Two Copay
$60 Tier Three Copay$100 Self-
AdministeredInjectables Copay
Or
Option B$250 Contract Year
Rx Deductiblethen
$10 Tier One Copay$35 Tier Two Copay
$60 Tier Three Copay$100 Self-
AdministeredInjectables Copay
Notes • Annual Deductible and Out-of-Pocket Maximum coincide with your contract year. • Lab and x-rays are covered in full In-Network. • Out-of-Pocket Maximum includes Medical Copays, Deductible and Coinsurance. (Does not include Rx Copays.)• Family Deductible and Out-of-Pocket = 2x Individual. • Coinsurance reflects member responsibility. • Payment for covered services received Out-of-Network are based upon Coventry’s Out-of-Network reimbursement rates. In addition to your
Coinsurance, you are responsible for paying Out-of-Network providers the difference between the Out-of-Network rate and their actual charges for non-emergency services.
* ER = Emergency Room **OOP = Out-of-Pocket
37966-1 Cov POS 11/1/06 2:07 PM Page 1

Point-of-Service (POS) Health Plans Schedule of BenefitsBenefit In-Network Payment Out-of-Network
PaymentLimitation
Lifetime Maximum Benefit $5,000,000 $5,000,000 In & Out-of-Network combined.
Physician Office Visit(no referrals required)
$40 Copay Deductible &Co-insurance.
Routine Eye Exam (Through Avesis Provider) $15 Copay Not a covered benefit.
Routine Mammogram, Lab & X-ray No Copay necessary. Covered in full. Deductible &Co-insurance.
Urgent Care Facility or Urgent Care at aPhysician’s Office
$40 Copay $40 Copay
Hospital Emergency Room Visit $200 Copay(Waived if admitted)
$200 Copay(Waived if admitted)
Chiropractic Care Visit $40 Copay Deductible & Co-insurance.
After initial evaluation, treatment planmust be approved by Coventry Health
Care to authorize additional visits.Inpatient & Outpatient Hospital and
Professional Services, Home Health Care,Hospice Care, Ambulance Services, Outpatient
Facility Services, and Diagnostic Imaging
Deductible & Co-insurance. Deductible &Co-insurance.
Short Term Rehabilitative Therapy, DurableMedical Equipment, and Skilled Nursing
Facility Services
Deductible & Co-insurance. Deductible &Co-insurance.
Short Term Rehabilitative Therapy is limitedto 20 visits per contract year per episode.
Durable Medical Equipment limited to anmaximum benefit of $5,000 per contract year.
Skilled Nursing Facility care is limited to 30inpatient days per contract year.
Maternity Services Not a covered benefit except forcomplications.
Not a covered benefit.
Inpatient & Outpatient Mental Health Services Not a covered benefit. Not a covered benefit.
Inpatient & Outpatient Alcohol and DrugAbuse Services
Not a covered benefit. Not a covered benefit.
Infertility, Custodial Care, Dental Services Not a covered benefit. Not a covered benefit.
Rx OutpatientBenefit (Option A)
Retail Purchase
Mail Order(90 day supply)
$10 Tier One Copay$35 Tier Two Copay
$60 Tier Three Copay$100 Self Administered Injectables Copay
$20 Tier One Copay$70 Tier Two Copay
$120 Tier Three Copay$200 Self Administered Injectables Copay
Not a covered benefit
Not a covered benefit
Rx Outpatient Benefit (Option B)Retail Purchase
Mail Order (90-day supply)
$250 contract year deductible then:$10 Tier One Copay$35 Tier Two Copay
$60 Tier Three Copay$100 Self Administered Injectables Copay
$250 contract year deductible then:$20 Tier One Copay$70 Tier Two Copay
$120 Tier Three Copay$200 Self Administered Injectables Copay
Not a covered benefit
Not a covered benefit
Payment for covered services received out of network are based upon Coventry Health Care’s out of network reimbursement rates. In addition to yourcopay or coinsurance , you are responsible for the difference between our out of network rate and the actual charge for non emergency services. Thissummary is designed as a partial description of the coverage being offered and in no way details all benefits, limitations, exclusions, terms, or conditions.Complete details of the exact terms, conditions, and scope of coverage including all limitations and exclusions governed by the Coventry Health CareIndividual Membership Agreement.
37966-1 Cov POS 11/1/06 2:07 PM Page 2
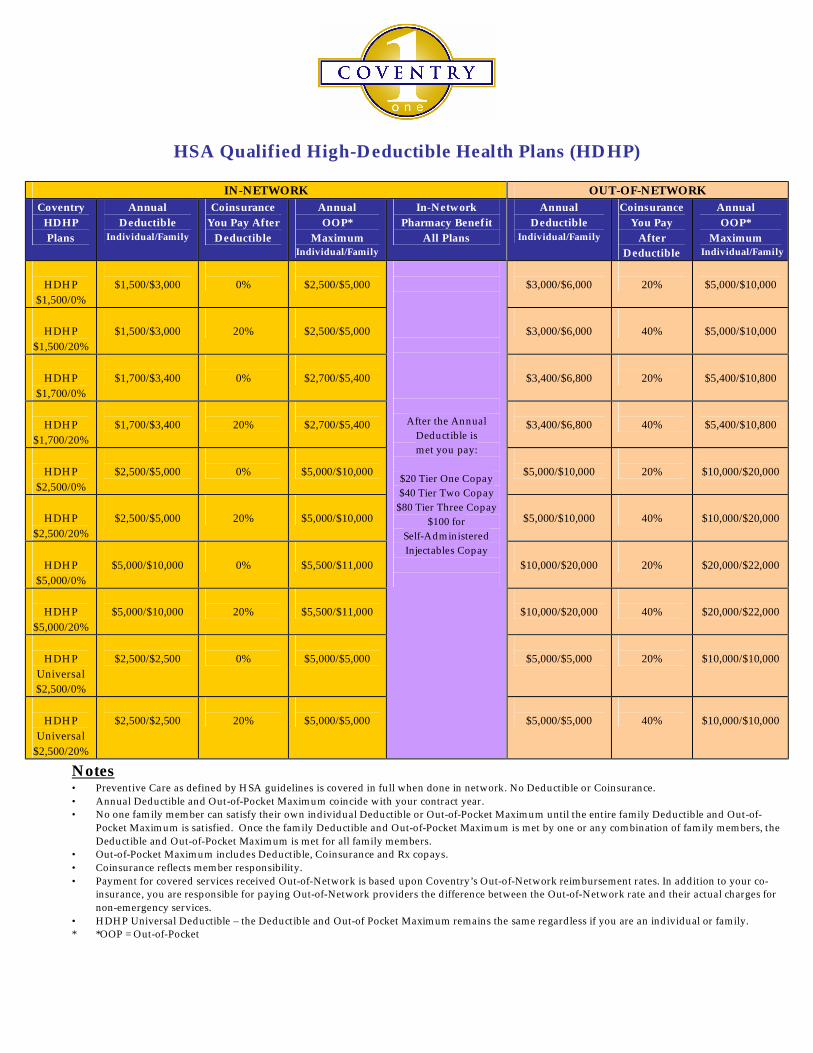
HSA Qualified High-Deductible Health Plans (HDHP)
IN-NETWORK OUT-OF-NETWORK Coventry
HDHP Plans
Annual Deductible
Individual/Family
Coinsurance You Pay After
Deductible
Annual OOP*
Maximum Individual/Family
In-Network Pharmacy Benefit
All Plans
Annual Deductible
Individual/Family
Coinsurance You Pay
After Deductible
Annual OOP*
Maximum Individual/Family
HDHP
$1,500/0%
$1,500/$3,000
0%
$2,500/$5,000
$3,000/$6,000
20%
$5,000/$10,000
HDHP
$1,500/20%
$1,500/$3,000
20%
$2,500/$5,000
$3,000/$6,000
40%
$5,000/$10,000
HDHP
$1,700/0%
$1,700/$3,400
0%
$2,700/$5,400
$3,400/$6,800
20%
$5,400/$10,800
HDHP
$1,700/20%
$1,700/$3,400
20%
$2,700/$5,400
$3,400/$6,800
40%
$5,400/$10,800
HDHP
$2,500/0%
$2,500/$5,000
0%
$5,000/$10,000
$5,000/$10,000
20%
$10,000/$20,000
HDHP
$2,500/20%
$2,500/$5,000
20%
$5,000/$10,000
$5,000/$10,000
40%
$10,000/$20,000
HDHP
$5,000/0%
$5,000/$10,000
0%
$5,500/$11,000
$10,000/$20,000
20%
$20,000/$22,000
HDHP
$5,000/20%
$5,000/$10,000
20%
$5,500/$11,000
$10,000/$20,000
40%
$20,000/$22,000
HDHP
Universal $2,500/0%
$2,500/$2,500
0%
$5,000/$5,000
$5,000/$5,000
20%
$10,000/$10,000
HDHP
Universal $2,500/20%
$2,500/$2,500
20%
$5,000/$5,000
After the Annual
Deductible is met you pay:
$20 Tier One Copay $40 Tier Two Copay
$80 Tier Three Copay $100 for
Self-Administered Injectables Copay
$5,000/$5,000
40%
$10,000/$10,000
Notes • Preventive Care as defined by HSA guidelines is covered in full when done in network. No Deductible or Coinsurance. • Annual Deductible and Out-of-Pocket Maximum coincide with your contract year. • No one family member can satisfy their own individual Deductible or Out-of-Pocket Maximum until the entire family Deductible and Out-of-
Pocket Maximum is satisfied. Once the family Deductible and Out-of-Pocket Maximum is met by one or any combination of family members, the Deductible and Out-of-Pocket Maximum is met for all family members.
• Out-of-Pocket Maximum includes Deductible, Coinsurance and Rx copays. • Coinsurance reflects member responsibility. • Payment for covered services received Out-of-Network is based upon Coventry’s Out-of-Network reimbursement rates. In addition to your co-
insurance, you are responsible for paying Out-of-Network providers the difference between the Out-of-Network rate and their actual charges for non-emergency services.
• HDHP Universal Deductible – the Deductible and Out-of Pocket Maximum remains the same regardless if you are an individual or family. * *OOP = Out-of-Pocket

HSA Qualified High-Deductible Health Plans (HDHP) Schedule of Benefits
Benefit In-Network Payment Out-of-Network Payment
Limitation
Lifetime Maximum Benefit
$5,000,000 $5,000,000 In & Out-of- Network combined.
Preventive Care Covered in full.
No deductible. Co-insurance only.
As defined by HSA guidelines.
Routine Mammogram, Routine Gynecological Exam and Pap Test
Covered in full.
No deductible. Co-insurance only.
Childhood Immunizations Covered in full.
No deductible. Co-insurance only.
Up to age 21
Physician Office Visit (no referrals required)
Deductible & Co-insurance. Deductible & Co-insurance.
Lab & X-ray Deductible & Co-insurance.
Deductible & Co-insurance.
Urgent Care Facility or Urgent Care at a Physician’s Office
Deductible & Co-insurance. Deductible & Co-insurance.
Hospital Emergency Room Visit Deductible & Co-insurance. Deductible & Co-insurance.
Chiropractic Care Visit Deductible & Co-insurance. Deductible & Co-insurance.
After initial evaluation, treatment plan must be approved by Coventry Health Care to authorize
additional visits. Inpatient & Outpatient Hospital and
Professional Services, Home Health Care, Hospice Care, Ambulance Services, Outpatient
Facility Services, and Diagnostic Imaging
Deductible & Co-insurance. Deductible & Co-insurance.
Short-Term Rehabilitative Therapy, Durable Medical Equipment, and Skilled Nursing Facility
Services
Deductible & Co-insurance. Deductible & Co-insurance.
Short-Term Rehabilitative Therapy is limited to 20 visits per contract year per episode.
Durable Medical Equipment limited to an
maximum benefit of $5,000 per contract year.
Skilled Nursing Facility care is limited to 30 inpatient days per contract year.
Maternity Services Not a covered benefit except for complications.
Not a covered benefit.
Inpatient and Outpatient Mental Health Services
Not a covered benefit. Not a covered benefit.
Inpatient and Outpatient Alcohol and Drug Abuse Services
Not a covered benefit. Not a covered benefit.
Infertility, Custodial Care, Dental Services
Not a covered benefit. Not a covered benefit.
Rx Outpatient Benefit Retail Purchase
Mail Order (90-day supply)
Deductible then:
$20 Tier One Copay $40 Tier Two Copay
$80 Tier Three Copay $100 Self Administered Injectables Copay
Deductible then:
$40 Tier One Copay $80 Tier Two Copay
$160 Tier Three Copay $200 Self Administered Injectables Copay
Not a covered
benefit
Not a covered
benefit
Payment for covered services received out of network are based upon Coventry Health Care’s out of network reimbursement rates. In addition to your copay or coinsurance, you are responsible for the difference between the out of network rate and the actual charge for non emergency services. This summary is designed as a partial description of the coverage being offered and in no way details all benefits, limitations, exclusions, terms, or conditions. Complete details of the exact terms, conditions, and scope of coverage including all limitations and exclusions governed by the Coventry Health Care Individual Membership Agreement.
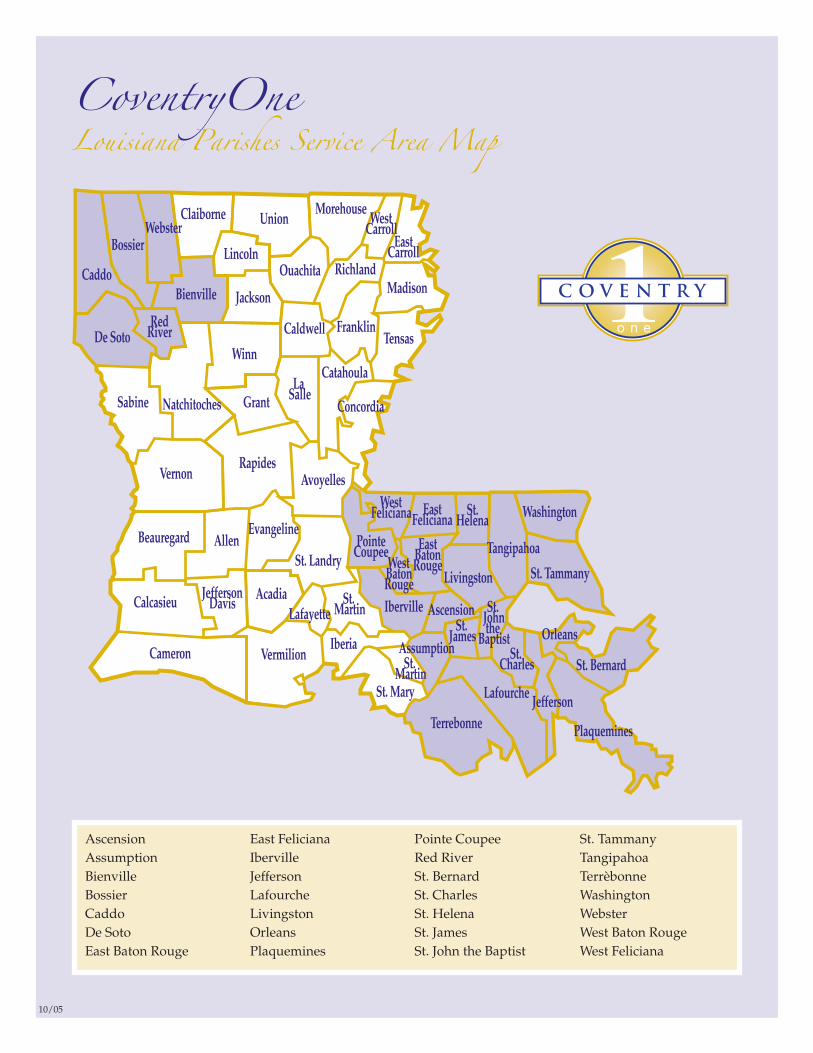
Ascension East Feliciana Pointe Coupee St. Tammany Assumption Iberville Red River TangipahoaBienville Jefferson St. Bernard TerrèbonneBossier Lafourche St. Charles WashingtonCaddo Livingston St. Helena WebsterDe Soto Orleans St. James West Baton RougeEast Baton Rouge Plaquemines St. John the Baptist West Feliciana

Coventry One Individual Point-of-Service Plan Selection Sheet� STEP 1: Choose a Point-of-Service (POS) Plan and place a check mark next to that item.
� STEP 2: Choose Pharmacy Plan A or Plan B and place a check mark next to that item.
� Pharmacy Plan A: $0 Deductible, $10 Tier One Copay; $35 Tier Two Copay; $60 Tier Three Copay; $100 Self-Administered Injectables Copay
� Pharmacy Plan B: $250 Calendar Year Deductible, $10 Tier One Copay; $35 Tier Two Copay; $60 Tier Three Copay; $100 Self-
Administered Injectables Copay
� POS Plan $500 20%: Office Visits $40, Emergency Room
$200, Deductible $500, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $1,500; Out-of-Network: Deductible
$1,000, Coinsurance 40%, Out-of-Pocket Maximum $3,000
� POS Plan $750 20%: Office Visits $40, Emergency Room
$200, Deductible $750, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $1,750; Out-of-Network: Deductible
$1,500, Coinsurance 40%, Out-of-Pocket Maximum $3,500
� POS Plan $1,000 20%: Office Visits $40, Emergency Room
$200, Deductible $1,000, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $2,000; Out-of-Network: Deductible
$2,000, Coinsurance 40%, Out-of-Pocket Maximum $4,000
� POS Plan $1,500 20%: Office Visits $40, Emergency Room
$200, Deductible $1,500, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $2,500; Out-of-Network: Deductible
$3,000, Coinsurance 40%, Out-of-Pocket Maximum $5,000
� POS Plan $2,500 20%: Office Visits $40, Emergency Room
$200, Deductible $2,500, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $3,500; Out-of-Network: Deductible
$5,000, Coinsurance 40%, Out-of-Pocket Maximum $7,000
� POS Plan $5,000 20%: Office Visits $40, Emergency Room
$200, Deductible $5,000, Coinsurance after Deductible 20%,
Out-of-Pocket Maximum $6,000; Out-of-Network: Deductible
$10,000, Coinsurance 40%, Out-of-Pocket Maximum $12,000
� POS Plan $500 50%: Office Visits $40, Emergency Room
$200, Deductible $500, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $3,000; Out-of-Network: Deductible
$1,000, Coinsurance 50%, Out-of-Pocket Maximum $6,000
� POS Plan $750 50%: Office Visits $40, Emergency Room
$200, Deductible $750, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $3,250; Out-of-Network: Deductible
$1,500, Coinsurance 50%, Out-of-Pocket Maximum $6,500
� POS Plan $1,000 50%: Office Visits $40, Emergency Room
$200, Deductible $1,000, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $3,500; Out-of-Network: Deductible
$2,000, Coinsurance 50%, Out-of-Pocket Maximum $7,000
� POS Plan $1,500 50%: Office Visits $40, Emergency Room
$200, Deductible $1,500, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $4,000; Out-of-Network: Deductible
$3,000, Coinsurance 50%, Out-of-Pocket Maximum $8,000
� POS Plan $2,500 50%: Office Visits $40, Emergency Room
$200, Deductible $2,500, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $5,000; Out-of-Network: Deductible
$5,000, Coinsurance 50%, Out-of-Pocket Maximum $10,000
� POS Plan $5,000 50%: Office Visits $40, Emergency Room
$200, Deductible $5,000, Coinsurance after Deductible 50%,
Out-of-Pocket Maximum $7,500; Out-of-Network: Deductible
$10,000, Coinsurance 50%, Out-of-Pocket Maximum $15,000
Name Printed
Signature Date
Notes:
• Annual Deductible and Out-of-Pocket Maximum coincide
with your contract year.
• Lab and X-rays are covered in full in Network.
• Out-of-Pocket Maximum includes copays, Deductible
and Coinsurance.
• Family Deductible and Out-of-Pocket = 2x Individual.
• Coinsurance reflects member responsibility.
• Payment for covered services received Out-of-Network is
based upon Coventry’s Out-of-Network reimbursement rates.
In addition to your Coinsurance, you are responsible for
paying Out-of-Network providers the difference between the
Out-of-Network rate and their actual charges for
non-emergency services.
31319_1 Cov SS 11/2/06 8:13 PM Page 1

Qualified High-Deductible Plan Selection SheetThe following plans qualify for the establishment of a Health Savings Account (HSA). Health Savings Accounts are tax-advantaged accounts
the future, tax-free.
� Pharmacy Benefit All Plans: After the Annual Deductible is met, you pay: $20 Tier One Copay; $40 Tier Two Copay, $80 Tier
Three Copay, $100 Self-Administered Injectables Copay
� Choose a Qualified High-Deductible (HDHP) Plan.
Notes:
• Preventive Care as defined by HSA guidelines is covered in full when done in network. No Deductible or Coinsurance.
•
• Out-of-Pocket Maximum includes Deductible and Coinsurance and RX copays.
• Coinsurance reflects member responsibility.
• Payment for covered services received Out-of-Network is based upon Coventry’s Out-of-Network reimbursement rates. In addition to
your Coinsurance, you are responsible for paying Out-of-Network providers the difference between the Out-of-Network rate and
their actual charges for non-emergency services.
� HDHP $1,500/0%: Annual Deductible Individual/Family
$1,500/$3,000, In-Network Coinsurance You Pay After
Deductible 0%, Pharmacy $20/40/80/100, Out-of-Pocket
Maximum Individual/Family $2,500/5,000; Out-of-Network:
Annual Deductible Individual/Family $3,000/$6,000,
Coinsurance You Pay After Deductible 20%, Out-of-Pocket
Maximum Individual/Family $5,000/$10,000
� HDHP $1,500/20%: Annual Deductible Individual/Family
$1,500/$3,000, In-Network Coinsurance You Pay After
Deductible 20%, Pharmacy $20/40/80/100, Out-of-Pocket
Maximum Individual/Family $2,500/$5,000; Out-of-Network:
Annual Deductible Individual/Family $3,000/$6,000,
Coinsurance You Pay After Deductible 40%, Out-of-Pocket
Maximum Individual/Family $5,000/$10,000
� HDHP $2,500/0%: Annual Deductible Individual/Family
$2,500/$5,000, In-Network Coinsurance You Pay After
Deductible 0%, Pharmacy $20/40/80/100, Out-of-Pocket
Maximum Individual/Family $5,000/$10,000; Out-of-Network:
Annual Deductible Individual/Family $5,000/$10,000,
Coinsurance You Pay After Deductible 20%, Out-of-Pocket
Maximum Individual/Family $10,000/$20,000
� HDHP $2,500/20%: Annual Deductible Individual/Family
$2,500/$5,000, In-Network Coinsurance You Pay After
Deductible 20%, Pharmacy $20/40/80/100, Out-of-Pocket
Maximum Individual/Family $5,000/10/000; Out-of-Network:
Annual Deductible Individual/Family $5,000/$10,000,
Coinsurance You Pay After Deductible 40%, Out-of-Pocket
Maximum Individual/Family $10,000/$20,000
� HDHP Universal* $2,500/0%: Annual Deductible
Individual/Family $2,500/$2,500, In-Network Coinsurance You
Pay After Deductible 0%, Pharmacy $20/40/80/100, Out-of-
Pocket Maximum Individual/Family $5,000/$5,000; Out-of-
Network: Annual Deductible Individual/Family $5,000/$5,000,
Coinsurance You Pay After Deductible 20%, Out-of-Pocket
Maximum Individual/Family $10,000/$10,000
� HDHP Universal* $2,500/20%: Annual Deductible
Individual/Family $2,500/$2,500, In-Network Coinsurance You
Pay After Deductible 20%, Pharmacy $20/40/80/100, Out-of-
Pocket Maximum Individual/Family $5,000/5,000; Out-of-
Network: Annual Deductible Individual/Family $5,000/$5,000,
Coinsurance You Pay After Deductible 40%, Out-of-Pocket
Maximum Individual/Family $10,000/$10,000
Name Printed
Signature Date
Coventry One
(similar to IRAs). By coupling a Coventry One Qualified High-Deductible Health Plan (HDHP) with an HSA account, you’re saving money for
Annual Deductible and Out-of-Pocket Maximum coincide with your contract year. •
*HDHP Universal Deductible: The Deductible and Out-of-Pocket Maximum remains the same regardless if you are an individual or family.
No one family member can satisfy their own individual Deductible or Out-of-Pocket Maximum until the entire family Deductible
combination of family members, the Deductible and the Out-of-Pocket Maximum is met for all members.and Out-of-Pocket Maximum is satisfied. Once the family Deductible and Family Out-of-Pocket Maximum is met by one or any
31319_1 Cov SS 11/2/06 8:13 PM Page 2
This brochure is not a contract. It is intended solely to provide you with a general overview of ourhealth insurance products. Complete details of benefits, terms and exclusions that apply to yourhealth care coverage are governed by the Individual Membership Agreement filed with the State ofLouisiana. CoventryOne is underwritten by Coventry Health Care of Louisiana, Inc.
CoventryOneCoventry Health Care of Louisiana, Inc.
3838 N. Causeway Blvd.Suite 3350
Metairie, LA 70002
Health Care Coverage for Louisiana Individuals & Families
...the One making health insurance more affordable.
37966_PktFldr 10/30/06 3:45 PM Page 1
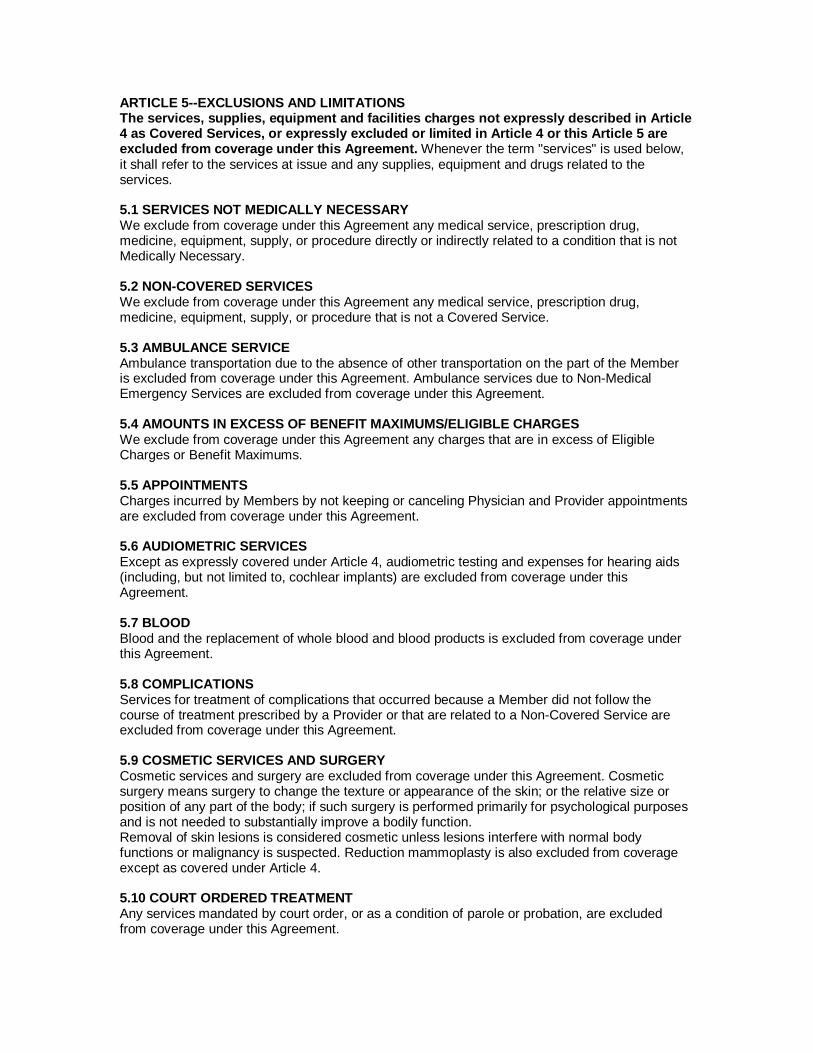
ARTICLE 5--EXCLUSIONS AND LIMITATIONS The services, supplies, equipment and facilities charges not expressly described in Article 4 as Covered Services, or expressly excluded or limited in Article 4 or this Article 5 are excluded from coverage under this Agreement. Whenever the term "services" is used below, it shall refer to the services at issue and any supplies, equipment and drugs related to the services. 5.1 SERVICES NOT MEDICALLY NECESSARY We exclude from coverage under this Agreement any medical service, prescription drug, medicine, equipment, supply, or procedure directly or indirectly related to a condition that is not Medically Necessary. 5.2 NON-COVERED SERVICES We exclude from coverage under this Agreement any medical service, prescription drug, medicine, equipment, supply, or procedure that is not a Covered Service. 5.3 AMBULANCE SERVICE Ambulance transportation due to the absence of other transportation on the part of the Member is excluded from coverage under this Agreement. Ambulance services due to Non-Medical Emergency Services are excluded from coverage under this Agreement. 5.4 AMOUNTS IN EXCESS OF BENEFIT MAXIMUMS/ELIGIBLE CHARGES We exclude from coverage under this Agreement any charges that are in excess of Eligible Charges or Benefit Maximums. 5.5 APPOINTMENTS Charges incurred by Members by not keeping or canceling Physician and Provider appointments are excluded from coverage under this Agreement. 5.6 AUDIOMETRIC SERVICES Except as expressly covered under Article 4, audiometric testing and expenses for hearing aids (including, but not limited to, cochlear implants) are excluded from coverage under this Agreement. 5.7 BLOOD Blood and the replacement of whole blood and blood products is excluded from coverage under this Agreement. 5.8 COMPLICATIONS Services for treatment of complications that occurred because a Member did not follow the course of treatment prescribed by a Provider or that are related to a Non-Covered Service are excluded from coverage under this Agreement. 5.9 COSMETIC SERVICES AND SURGERY Cosmetic services and surgery are excluded from coverage under this Agreement. Cosmetic surgery means surgery to change the texture or appearance of the skin; or the relative size or position of any part of the body; if such surgery is performed primarily for psychological purposes and is not needed to substantially improve a bodily function. Removal of skin lesions is considered cosmetic unless lesions interfere with normal body functions or malignancy is suspected. Reduction mammoplasty is also excluded from coverage except as covered under Article 4. 5.10 COURT ORDERED TREATMENT Any services mandated by court order, or as a condition of parole or probation, are excluded from coverage under this Agreement.

5.11 CUSTODIAL CARE Custodial care, nursing home care, rest cures and domiciliary care, along with all related services, are excluded from coverage under this Agreement. Care is considered custodial if it is primarily for meeting personal needs. For example, custodial care includes, but is not limited to, help in walking, getting in and out of bed, bathing, dressing, shopping, eating and preparing meals, performing general household services, taking medicine, or furnishing other home services mainly to help people in meeting personal, family or domestic needs. Custodial care is excluded from coverage regardless of the location or setting. All services provided to persons confined to long-term care facilities and boarding homes are excluded from coverage under this Agreement. 5.12 DENTAL AND ORAL SURGICAL SERVICES Except as expressly covered under Article 4, oral services are excluded from coverage under this Agreement, including but not limited to: • Services and supplies related to dental care, dental appliances, dental implants, or dental Xrays. • Orthodontics, periodontics, endodontics, prosthodontics, preventive, cosmetic or restorative dentistry. • Oral Surgery that is required as part of an orthodontic treatment program. • Oral Surgery that is required for correction of an occlusal defect. • Oral Surgery that encompasses orthognathic, prosthodontics or prognathic surgical procedures. • Treatment of temporomandibular joint syndrome or temporomandibular joint disorders. • A charge for Physicians' services or X-ray examinations involving one or more teeth, the tissue or structure around them, the alveolar process or the gums is an excluded benefit. This applies even if a condition requiring any of these services involves a part of the body other than the mouth, such as the treatment of temporomandibular joint disorder or malocclusion involving joints or muscles by methods including, but not limited to: crowning, wiring, or repositioning of teeth. • Orthodontia and related services. • Tooth extractions other than those required for the path of the beam used for radiation therapy. • Removal of asymptomatic, non-impacted third molars. 5.13 EMERGENCY FACILITY SERVICES Non-Medical Emergency Services provided in an emergency facility are excluded from coverage under this Agreement. 5.14 EXAMS Physical or psychological examinations for employment, school, camp, sports, licensing, insurance, adoption or marriage, or other examinations ordered by a third party are excluded from coverage under this Agreement. Eye exams for refractive correction are excluded from coverage under this Agreement. 5.15 EXPERIMENTAL OR INVESTIGATIONAL PROCEDURES OR TREATMENTS Other than products or services covered as part of Patient Cost incurred as part of a Clinical Trial, a health product or service is deemed experimental or investigational and excluded from coverage under this Agreement if one or more of the following conditions are met: (i) any drug not approved for use by the FDA;(ii) any drug that is classified as IND (investigational new drug) by the FDA; (iii) any drug requiring Pre-Authorization that is proposed for off-label prescribing; (iv) any health product or service that is subject to Investigational Review Board (IRB) review or approval; (v) any health product or service that is the subject of a clinical trial that meets criteria for Phase I, II or III as set forth by FDA regulations; or (vi) any health product or service that does not have a demonstrated value based on clinical evidence reported by peer-review medical literature and by generally recognized academic experts.

5.16 EYEGLASSES AND CORRECTIVE LENSES Eyeglasses and corrective lenses are excluded from coverage under this Agreement except as expressly listed in Article 4. 5.17 FAMILY PERFORMING SERVICES EXCLUSION Services or supplies furnished by a person who ordinarily resides in the Member's household or a family member are excluded from coverage under this Agreement. 5.18 FAMILY PLANNING, STERILIZATION, AND INFERTILITY Any medical service, prescription drugs, medicine, supplies or procedures directly or indirectly related to the following are excluded from coverage under this Agreement: reversal of voluntarily induced sterilization, services related to sex transformation, artificial insemination with donor semen, in vitro fertilization and embryo transport procedure, drug therapy for infertility, and home delivery for childbirth. Drugs prescribed or given for or in connection with artificial insemination, in-vitro fertilization or any other artificial reproductive technology or whose primary purpose is for treatment of Infertility, whether oral, inhalants, or Injectable are excluded from coverage under this Agreement, including, but not limited to, Pergonal, Follistim, Clomid and other drugs meant to serve the same purpose as Pergonal, Follistim and Clomid. The following items are excluded from coverage under this Agreement: Artificial insemination of any kind, Artificial insemination elected by a patient prior to a medical diagnosis of Infertility; artificial insemination using donor sperm and all other artificial reproductive technology including, but not limited to, in-vitro fertilization (IVF), gamete intrafallopian transfer (GIFT), zygote intrafallopian transfer (ZIFT), ovum harvest, embryo transplants and similar procedures, and related services, cost of donor sperm or donor ova. Unless expressly covered under Article 4, family planning services are excluded from this Agreement, including but not limited to, pregnancy reduction procedures, and abortion services unless Medically Necessary or in the case of rape or incest. All services and supplies associated with surrogate motherhood, including, but not limited to, all services and supplies relating to the conception and pregnancy of a Member acting as a surrogate mother are excluded from coverage under this Agreement. 5.19 FELONY COMMISSION, ETC. Any services or supplies that are required to treat an Injury a contributing cause of which was the Member's: (i) commission of, or attempt to commit a felony or misdemeanor, (ii) engagement in an illegal occupation; or (iii) driving while intoxicated or under the influence of narcotics, are excluded from coverage under this Agreement. 5.20 FOOD OR FOOD SUPPLEMENTS Food (except for low protein food products, as described in Article 4), food supplements, vitamins (except prenatal vitamins), and any other nutritional or over-the-counter electrolyte supplements are excluded from coverage under this Agreement. 5.21 FOOT CARE Foot care is excluded from coverage under this Agreement, except as specifically covered under Article 4. Foot care includes but is not limited to the removal or reduction of corns and calluses, clipping of the nails, treatment of flat feet, fallen arches, and chronic foot strain. 5.22 GENERAL EXCLUSION Services or supplies that are not authorized in accordance with Our Utilization Management Program or that are not received in accordance with the terms and conditions of this Agreement are excluded from coverage under this Agreement. 5.23 GENETIC COUNSELING Genetic counseling and genetic studies that are not needed for diagnosis or treatment of genetic
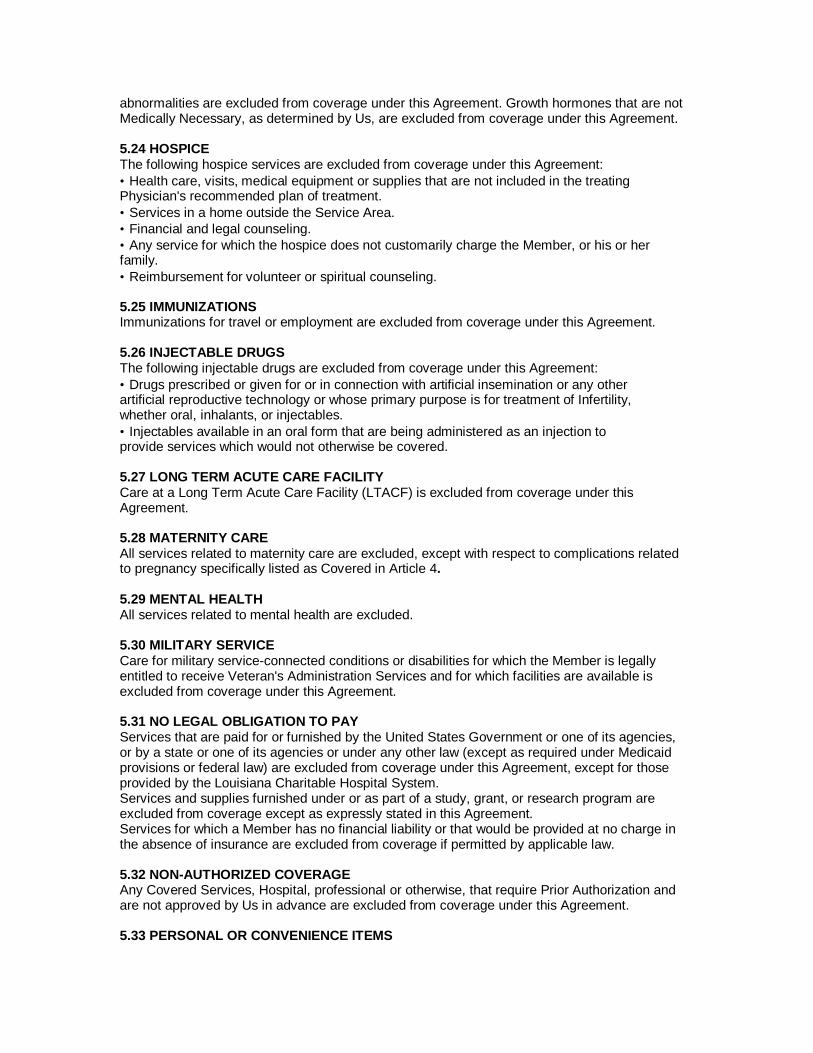
abnormalities are excluded from coverage under this Agreement. Growth hormones that are not Medically Necessary, as determined by Us, are excluded from coverage under this Agreement. 5.24 HOSPICE The following hospice services are excluded from coverage under this Agreement: • Health care, visits, medical equipment or supplies that are not included in the treating Physician's recommended plan of treatment. • Services in a home outside the Service Area. • Financial and legal counseling. • Any service for which the hospice does not customarily charge the Member, or his or her family. • Reimbursement for volunteer or spiritual counseling. 5.25 IMMUNIZATIONS Immunizations for travel or employment are excluded from coverage under this Agreement. 5.26 INJECTABLE DRUGS The following injectable drugs are excluded from coverage under this Agreement: • Drugs prescribed or given for or in connection with artificial insemination or any other artificial reproductive technology or whose primary purpose is for treatment of Infertility, whether oral, inhalants, or injectables. • Injectables available in an oral form that are being administered as an injection to provide services which would not otherwise be covered. 5.27 LONG TERM ACUTE CARE FACILITY Care at a Long Term Acute Care Facility (LTACF) is excluded from coverage under this Agreement. 5.28 MATERNITY CARE All services related to maternity care are excluded, except with respect to complications related to pregnancy specifically listed as Covered in Article 4. 5.29 MENTAL HEALTH All services related to mental health are excluded. 5.30 MILITARY SERVICE Care for military service-connected conditions or disabilities for which the Member is legally entitled to receive Veteran's Administration Services and for which facilities are available is excluded from coverage under this Agreement. 5.31 NO LEGAL OBLIGATION TO PAY Services that are paid for or furnished by the United States Government or one of its agencies, or by a state or one of its agencies or under any other law (except as required under Medicaid provisions or federal law) are excluded from coverage under this Agreement, except for those provided by the Louisiana Charitable Hospital System. Services and supplies furnished under or as part of a study, grant, or research program are excluded from coverage except as expressly stated in this Agreement. Services for which a Member has no financial liability or that would be provided at no charge in the absence of insurance are excluded from coverage if permitted by applicable law. 5.32 NON-AUTHORIZED COVERAGE Any Covered Services, Hospital, professional or otherwise, that require Prior Authorization and are not approved by Us in advance are excluded from coverage under this Agreement. 5.33 PERSONAL OR CONVENIENCE ITEMS
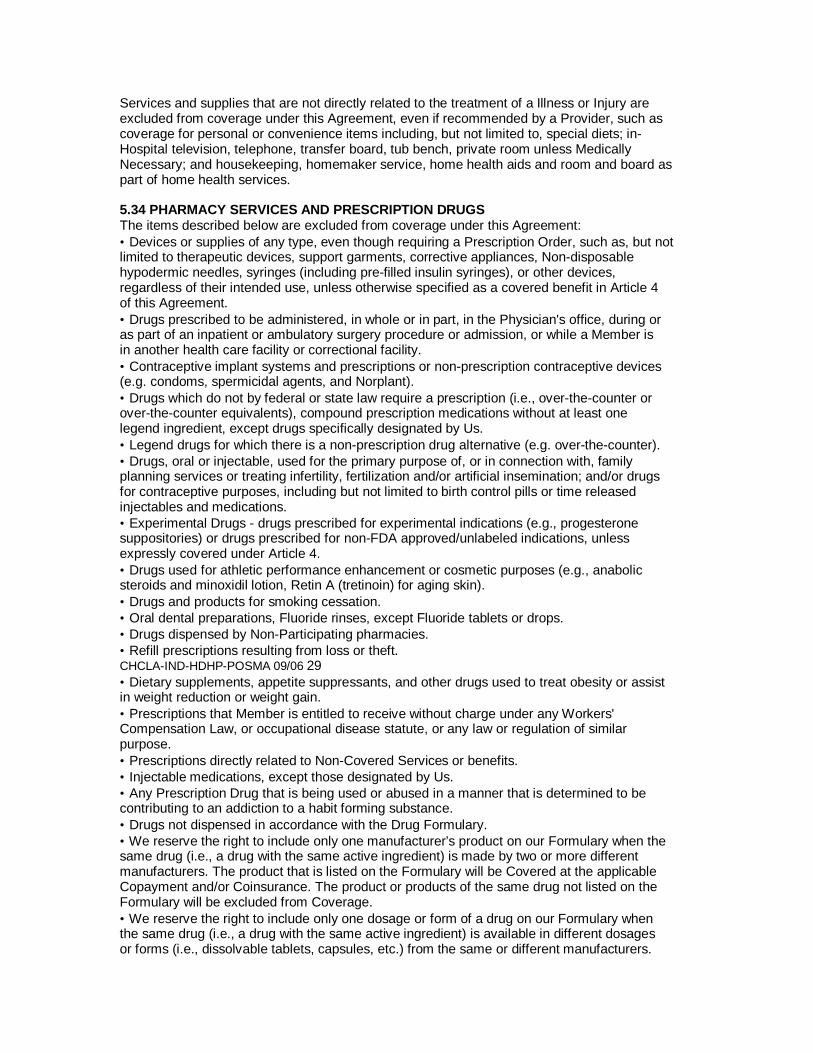
Services and supplies that are not directly related to the treatment of a Illness or Injury are excluded from coverage under this Agreement, even if recommended by a Provider, such as coverage for personal or convenience items including, but not limited to, special diets; in- Hospital television, telephone, transfer board, tub bench, private room unless Medically Necessary; and housekeeping, homemaker service, home health aids and room and board as part of home health services. 5.34 PHARMACY SERVICES AND PRESCRIPTION DRUGS The items described below are excluded from coverage under this Agreement: • Devices or supplies of any type, even though requiring a Prescription Order, such as, but not limited to therapeutic devices, support garments, corrective appliances, Non-disposable hypodermic needles, syringes (including pre-filled insulin syringes), or other devices, regardless of their intended use, unless otherwise specified as a covered benefit in Article 4 of this Agreement. • Drugs prescribed to be administered, in whole or in part, in the Physician's office, during or as part of an inpatient or ambulatory surgery procedure or admission, or while a Member is in another health care facility or correctional facility. • Contraceptive implant systems and prescriptions or non-prescription contraceptive devices (e.g. condoms, spermicidal agents, and Norplant). • Drugs which do not by federal or state law require a prescription (i.e., over-the-counter or over-the-counter equivalents), compound prescription medications without at least one legend ingredient, except drugs specifically designated by Us. • Legend drugs for which there is a non-prescription drug alternative (e.g. over-the-counter). • Drugs, oral or injectable, used for the primary purpose of, or in connection with, family planning services or treating infertility, fertilization and/or artificial insemination; and/or drugs for contraceptive purposes, including but not limited to birth control pills or time released injectables and medications. • Experimental Drugs - drugs prescribed for experimental indications (e.g., progesterone suppositories) or drugs prescribed for non-FDA approved/unlabeled indications, unless expressly covered under Article 4. • Drugs used for athletic performance enhancement or cosmetic purposes (e.g., anabolic steroids and minoxidil lotion, Retin A (tretinoin) for aging skin). • Drugs and products for smoking cessation. • Oral dental preparations, Fluoride rinses, except Fluoride tablets or drops. • Drugs dispensed by Non-Participating pharmacies. • Refill prescriptions resulting from loss or theft. CHCLA-IND-HDHP-POSMA 09/06 29 • Dietary supplements, appetite suppressants, and other drugs used to treat obesity or assist in weight reduction or weight gain. • Prescriptions that Member is entitled to receive without charge under any Workers' Compensation Law, or occupational disease statute, or any law or regulation of similar purpose. • Prescriptions directly related to Non-Covered Services or benefits. • Injectable medications, except those designated by Us. • Any Prescription Drug that is being used or abused in a manner that is determined to be contributing to an addiction to a habit forming substance. • Drugs not dispensed in accordance with the Drug Formulary. • We reserve the right to include only one manufacturer’s product on our Formulary when the same drug (i.e., a drug with the same active ingredient) is made by two or more different manufacturers. The product that is listed on the Formulary will be Covered at the applicable Copayment and/or Coinsurance. The product or products of the same drug not listed on the Formulary will be excluded from Coverage. • We reserve the right to include only one dosage or form of a drug on our Formulary when the same drug (i.e., a drug with the same active ingredient) is available in different dosages or forms (i.e., dissolvable tablets, capsules, etc.) from the same or different manufacturers.
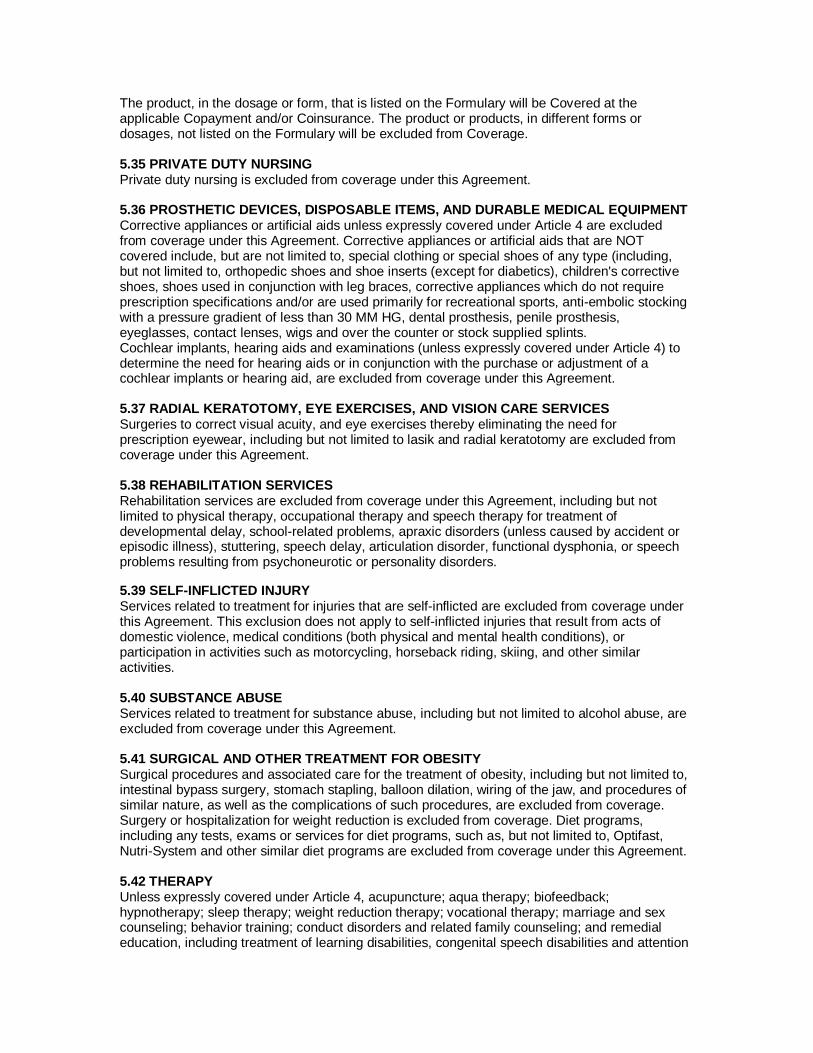
The product, in the dosage or form, that is listed on the Formulary will be Covered at the applicable Copayment and/or Coinsurance. The product or products, in different forms or dosages, not listed on the Formulary will be excluded from Coverage. 5.35 PRIVATE DUTY NURSING Private duty nursing is excluded from coverage under this Agreement. 5.36 PROSTHETIC DEVICES, DISPOSABLE ITEMS, AND DURABLE MEDICAL EQUIPMENT Corrective appliances or artificial aids unless expressly covered under Article 4 are excluded from coverage under this Agreement. Corrective appliances or artificial aids that are NOT covered include, but are not limited to, special clothing or special shoes of any type (including, but not limited to, orthopedic shoes and shoe inserts (except for diabetics), children's corrective shoes, shoes used in conjunction with leg braces, corrective appliances which do not require prescription specifications and/or are used primarily for recreational sports, anti-embolic stocking with a pressure gradient of less than 30 MM HG, dental prosthesis, penile prosthesis, eyeglasses, contact lenses, wigs and over the counter or stock supplied splints. Cochlear implants, hearing aids and examinations (unless expressly covered under Article 4) to determine the need for hearing aids or in conjunction with the purchase or adjustment of a cochlear implants or hearing aid, are excluded from coverage under this Agreement. 5.37 RADIAL KERATOTOMY, EYE EXERCISES, AND VISION CARE SERVICES Surgeries to correct visual acuity, and eye exercises thereby eliminating the need for prescription eyewear, including but not limited to lasik and radial keratotomy are excluded from coverage under this Agreement. 5.38 REHABILITATION SERVICES Rehabilitation services are excluded from coverage under this Agreement, including but not limited to physical therapy, occupational therapy and speech therapy for treatment of developmental delay, school-related problems, apraxic disorders (unless caused by accident or episodic illness), stuttering, speech delay, articulation disorder, functional dysphonia, or speech problems resulting from psychoneurotic or personality disorders. 5.39 SELF-INFLICTED INJURY Services related to treatment for injuries that are self-inflicted are excluded from coverage under this Agreement. This exclusion does not apply to self-inflicted injuries that result from acts of domestic violence, medical conditions (both physical and mental health conditions), or participation in activities such as motorcycling, horseback riding, skiing, and other similar activities. 5.40 SUBSTANCE ABUSE Services related to treatment for substance abuse, including but not limited to alcohol abuse, are excluded from coverage under this Agreement. 5.41 SURGICAL AND OTHER TREATMENT FOR OBESITY Surgical procedures and associated care for the treatment of obesity, including but not limited to, intestinal bypass surgery, stomach stapling, balloon dilation, wiring of the jaw, and procedures of similar nature, as well as the complications of such procedures, are excluded from coverage. Surgery or hospitalization for weight reduction is excluded from coverage. Diet programs, including any tests, exams or services for diet programs, such as, but not limited to, Optifast, Nutri-System and other similar diet programs are excluded from coverage under this Agreement. 5.42 THERAPY Unless expressly covered under Article 4, acupuncture; aqua therapy; biofeedback; hypnotherapy; sleep therapy; weight reduction therapy; vocational therapy; marriage and sex counseling; behavior training; conduct disorders and related family counseling; and remedial education, including treatment of learning disabilities, congenital speech disabilities and attention

deficit disorders or minimal brain dysfunction are excluded from coverage under this Agreement. Therapy through behavior modification is excluded from coverage under this Agreement. Coverage for educational and other Non-medical treatments for mental retardation is excluded from coverage under this Agreement. 5.43 TRANSPLANTS Services relating to an excluded transplant, that would not be performed except in association with the transplant, are excluded from coverage under this Agreement. Any medical and surgical complications resulting from Non-covered transplants are excluded from coverage under this Agreement. We will not cover the cost of any care arising from an organ donation by a Member if the recipient is not a Member. We will not cover the cost of any care arising from an organ donation by a Non-Member except as set forth in Article 4. No coverage is provided under this Agreement, for a transplant procedure that; (1) is not approved for coverage by Us, based on Our established criteria; or (2) is performed in a facility that is not a member of the Coventry Transplant Network. 5.44 TRAVEL All travel expenses, other than expressly covered under this Agreement, are excluded from coverage under this Agreement. 5.45 WAR OR ACT OF WAR Services resulting from war or acts of war are excluded from coverage under this Agreement. 5.46 APPROVAL OF EXCLUDED SERVICES We reserve the right to authorize payment for a service, supply, equipment or benefit that is otherwise not covered or is limited or excluded under this Agreement. Coverage of a service, supply, equipment, or benefit not otherwise authorized does not waive Our right to deny coverage for the same in the future or obligate Us to cover the same for the same Member in the future or for any other Member at any time. 5.47 PRE-EXISTING MEDICAL CONDITION We may exclude Coverage for Pre-existing Medical Conditions. This exclusion applies only to a condition of a Member for which medical advice, diagnosis, care, or treatment was recommended by, or received from, an individual licensed or similarly authorized to provide such services under applicable state law within the twelve (12) month period prior the Member’s Effective Date. This exclusion period shall last for a period of twelve (12) months, which shall begin on the Enrollment Date. The exclusion period for Pre-Existing Medical Conditions will be reduced by Your prior period of Creditable Coverage; provided that there is no break in Creditable Coverage of more then 63 consecutive days. A prior period of Creditable Coverage is the number of days credited to a Member that operates to reduce or eliminate the Health Plan’s Pre-existing Medical Condition exclusion period. Note: The Health Plan will not impose a Pre-existing Medical Condition exclusion period for pregnancy or on a newborn, a child under eighteen (18) years of age who is adopted, placed for adoption, or placed for foster care, provided the child is Covered under this Agreement within thirty-one (31) days of birth, adoption, placement for adoption, or placement for foster care. However, if the child has a break in Creditable Coverage or at least sixty-three (63) consecutive days, the Health Plan may impose a Pre-existing Medical Condition exclusion period on the child. For purposes of this Section 5.47 “Pre-Existing Medical Condition” means any medical condition for which medical advice, diagnosis, care or treatment was recommended by, or received from, a licensed Provider within the twelve (12) months immediately preceding the Member’s Effective Date under the Agreement. Certain health services related to a Pre-existing Medical Condition may be subject to a Copayment or not covered at all. Members may contact the Health Plan to find out to which procedures a Copayment applies.

We retain the discretion to waive any Pre-Existing Medical Condition exclusion for any Pre- Existing Medical Condition properly disclosed in Your and/or Your Dependents’ Enrollment Application. 5.48 MEDICARE Services paid or payable under Medicare Parts, A,B,C and D when you have Medicare coverage. 5.49 COMPLICATIONS RELATED TO PREGNANCY All services related to complications from or related to pregnancy, except for ectopic pregnancies and spontaneous abortions (miscarriages).