health care failure mode and effect analysis (hfmea) of...
TRANSCRIPT
Health Care Failure Mode and Effect
Analysis (HFMEA) of Continuous
Renal Replacement Therapies
(CRRT): a tool to improve the
patients´ safety on the everyday
health treatment
D. Esteban Molano Álvarez, Dr. Jose Ángel Sánchez-Izquierdo Riera, Dr. Juan Carlos Montejo,
Dª Amelia Guirao Moya, Dª Estrella García Delgado, Dr. Pedro Ruiz López, Dª Teresa Núñez

Introduction
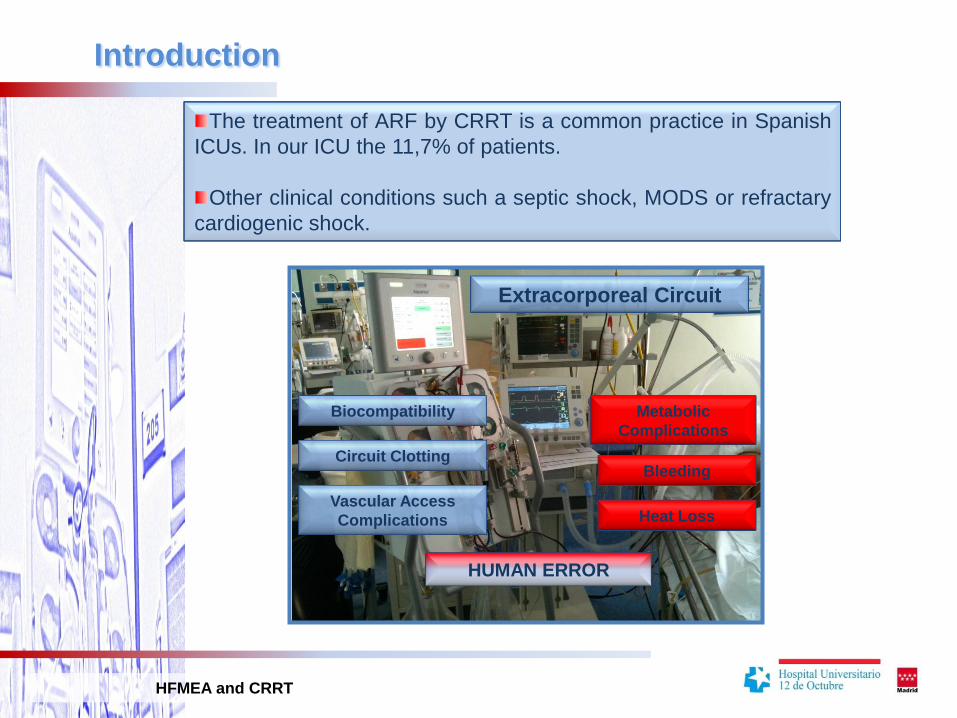
The treatment of ARF by CRRT is a common practice in Spanish
ICUs. In our ICU the 11,7% of patients.
Other clinical conditions such a septic shock, MODS or refractary
cardiogenic shock.
Extracorporeal Circuit
Biocompatibility
Circuit Clotting
Metabolic
Complications
Bleeding
Heat Loss
HUMAN ERROR
Vascular Access
Complications
HFMEA and CRRT
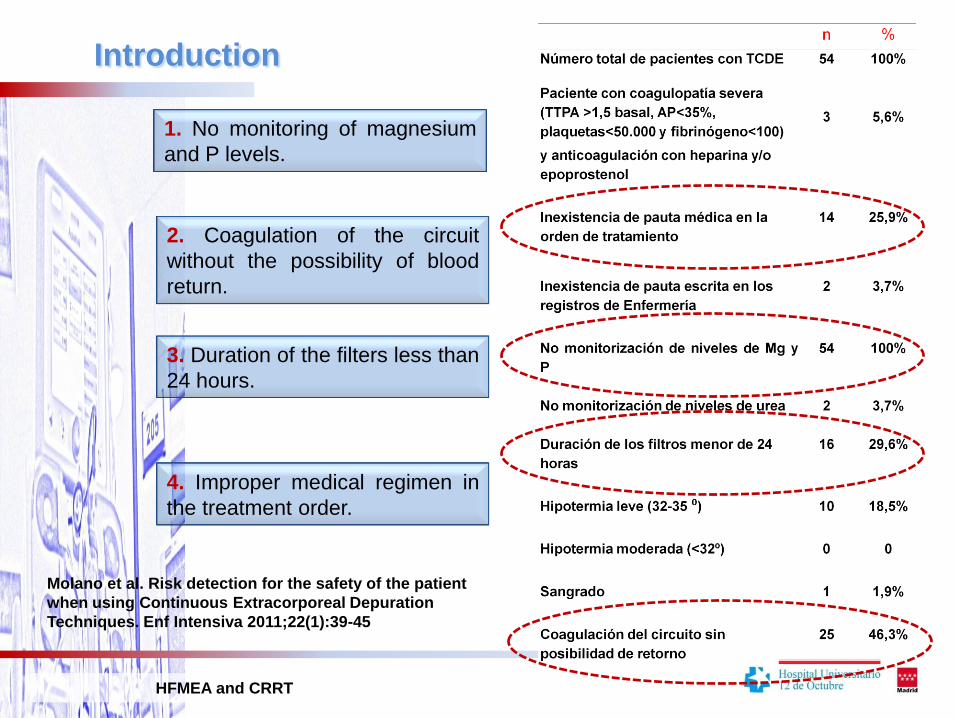
1. No monitoring of magnesium
and P levels.
2. Coagulation of the circuit
without the possibility of blood
return.
3. Duration of the filters less than
24 hours.
Introduction
HFMEA and CRRT
4. Improper medical regimen in
the treatment order.
Molano et al. Risk detection for the safety of the patient
when using Continuous Extracorporeal Depuration
Techniques. Enf Intensiva 2011;22(1):39-45

Health Care Failure Mode and Effect Analysis (HFMEA) of the CRRT
in ICU of the Doce de Octubre Hospital .
Tool to identify and evaluate potential failures of processes, their causes and
possible effects.
Process HFMEA vs Design HFMEA and Media HFMEA.
AIM: To identify safety problems in continuous renal replacement therapy
(CRRT) in order to implement actions to reduce their effects.
HFMEA and CRRT
Introduction
Material and Methods
HFMEA and CRRT
HFMEA PROCESS PHASES
Definition of the object of analysis.
CRRT implementation process in the intensive care unit of Doce de Octubre
Hospital.
HFMEA Team
Dr. Pedro Ruiz López. Head of Quatity Unit of Doce de Octubre Hospital.
.
Dr. Juan Carlos Montejo González. Chiel of Intensive Care Unit Medicine of Doce de Octubre
Hospital.
Dr. Jose Ángel Sanchez-Izquierdo Riera. Medical Assistant of Intensive Care Unit Medicine of
Doce de Octubre Hospital.
D. Esteban Molano Álvarez. Supervisor of ICU Polyvalent of Doce de Octubre Hospital.
Dª Estrella García Delgado. Nursing of the ICU Doce de Octubre Hospital.
Dª Amelia Guirao Moya. Nursing of the ICU Doce de Octubre Hospital.
Dª Teresa Núñez Jiménez. Nurse. Specialist in CEDT of BAXTER Company.

FASESIndication and
treatment regimen
Installation andConnection
Maintenance
Inadequate indicationInadequate therapy indicationTranscript inadequate treatment orderDelayed startWrong patient
Venous Canalization
Improper catheterInadequate venous accessCanalization Problems
Aseptic failureImproper primingIncorrect assembly linesFailed catheter flowConnecting to the wrong patient Inadequate treatment
Equipment failureCoagulation circuitsInadequate monitoring of the patientLack of asepsisAccidental disconnectionIncorrect catheter maintenanceEarly withdrawal
Late WithdrawalIncorrect removal procedureIncorrect catheter removal
Treatment Withdrawal
Graphic Description of the
ProcessMaterial and Methods
HFMEA and CRRT
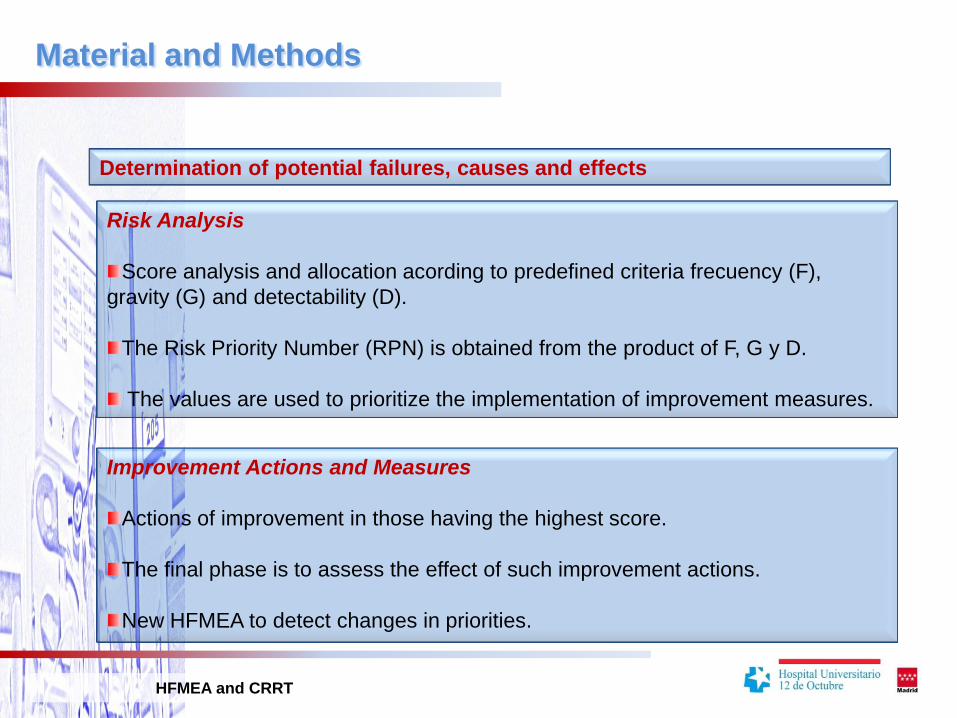
Determination of potential failures, causes and effects
Risk Analysis
Score analysis and allocation acording to predefined criteria frecuency (F),
gravity (G) and detectability (D).
The Risk Priority Number (RPN) is obtained from the product of F, G y D.
The values are used to prioritize the implementation of improvement measures.
Improvement Actions and Measures
Actions of improvement in those having the highest score.
The final phase is to assess the effect of such improvement actions.
New HFMEA to detect changes in priorities.
HFMEA and CRRT
Material and Methods

Material and Methods
HFMEA and CRRT
HFMEA and CRRT
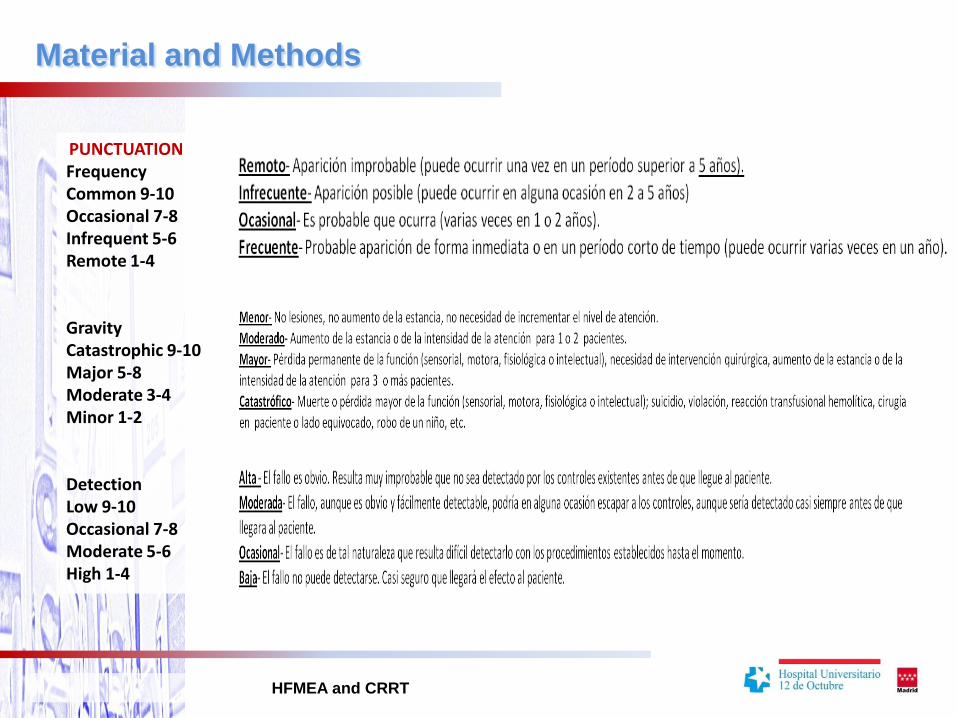
PUNCTUATIONFrequencyCommon 9-10Occasional 7-8Infrequent 5-6Remote 1-4
GravityCatastrophic 9-10Major 5-8Moderate 3-4Minor 1-2
DetectionLow 9-10Occasional 7-8Moderate 5-6High 1-4
Material and Methods

Results
HFMEA and CRRT
MAJOR POTENTIAL FAILURES DETECTED
Lack of asepsis in the maintenance of therapies
Inadequate treatment indication.
Improper connection to the patient.
Inadequate treatment.
Actual dosage lower than scheduled.
Incorrect treatment withdrawal.
ALL OF THEM ASSOCIATED TO THE LACK OF TRAINING AND PROTOCOLS.
Early coagulation of the circuits related to BLOOD CIRCUIT DESIGN AND
FAILURE OF THE CATHETER.

Results
HFMEA and CRRT
PROPOSED IMPROVEMENT ACTIONS
Development of a protocol for CRRT.
Training.
Enhance awareness of asespis. Introduction of assembly check list, including
aseptic handling.
Improve equipment and consumables in order to prevent circuit clotting.
Results
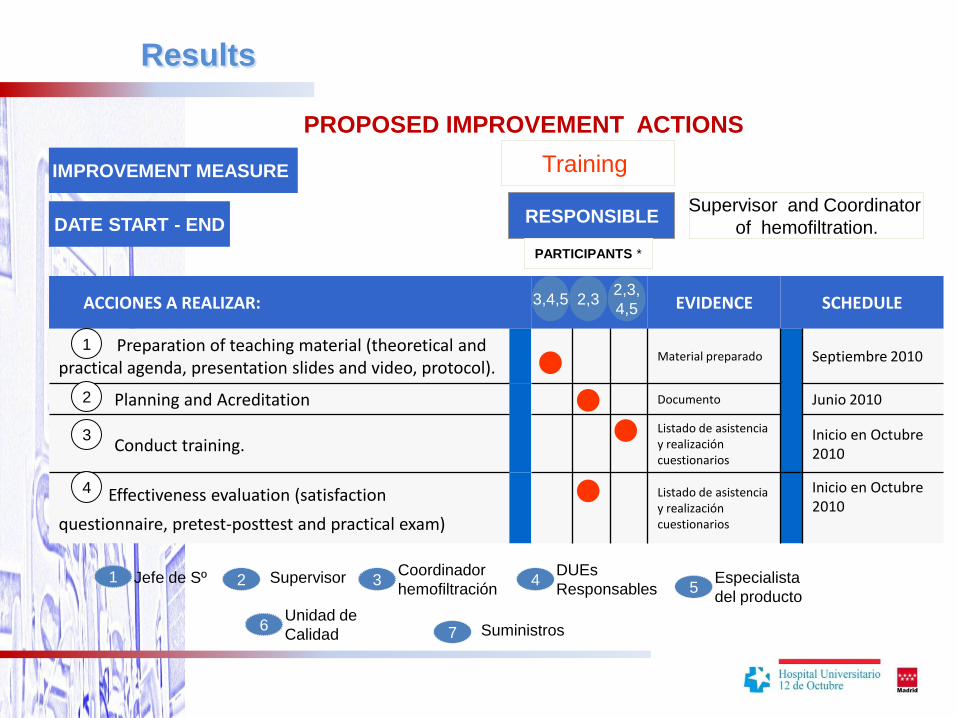
PROPOSED IMPROVEMENT ACTIONS
Training
Supervisor and Coordinator
of hemofiltration.
IMPROVEMENT MEASURE
DATE START - END
ACCIONES A REALIZAR: EVIDENCE SCHEDULE
Preparation of teaching material (theoretical and practical agenda, presentation slides and video, protocol).
Material preparado Septiembre 2010
Planning and Acreditation Documento Junio 2010
Conduct training.Listado de asistencia y realización cuestionarios
Inicio en Octubre 2010
Effectiveness evaluation (satisfaction
questionnaire, pretest-posttest and practical exam)
Listado de asistencia y realización cuestionarios
Inicio en Octubre 2010
3,4,5
RESPONSIBLE
PARTICIPANTS *
2,32,3,
4,5
1
2
3
1 Jefe de Sº 2 Supervisor 3Coordinador
hemofiltración4
DUEs
Responsables 5Especialista
del producto
7 Suministros6Unidad de
Calidad
4

Results
HFMEA and CRRT
MONITORING INDICATORS
CRRT TRAINING
Attendance level:
Pre-and post-training knowledge assessment.
Attending the meeting
Unit Staff
CRRT PROTOCOL DEVELOPMENT
Compliance with protocol guidelines.
Detection of errors in each patient.
Adverse events.

Results
HFMEA and CRRT
MONITORING INDICATORS
ENHANCE AWARENESS OF ASEPSIS
Completion of check list.
Decreased bacteraemia rates for hemofiltration catheters.
Direct observation of hand washing and the use of clean gloves when
handling the circuit.
PREVENTION OF EARLY COAGULATION OF THE CIRCUIT (BEFORE 24 HS)
Evaluate the application of the recommended improvements.
Measure the percentage of clotted circuits before 24 hours.
Results
HFMEA and CRRT
Conclusions
HFMEA and CRRT
The HFMEA is a useful tool to prioritize potential problems for any process.
It facilitates an ordered distribution of possible improvement actions.
We won’t be able to determine the true effectiveness of this tool until the
development of phase 3, in which the indicators will be valued.

Conclusiones
Detección de riesgos en TCDE
Se precisa monitorización protocolizada del Mg y P
P = ATP
Hipofosfatemia (60% de pacientes en estudio
RENAL )
Debe corregirse el defecto en la cumplimentación de la
pauta terapéutica en las órdenes de tratamiento, con una
normalización de la misma
Se precisa optimizar la técnica para prolongar su
duración y evitar pérdidas hemáticas.